
Page 199
6
Dissemination: Increasing the Use and Availability of New Technologies
A positive coverage decision from Medicare or private insurers does not guarantee adoption of new technologies. Even after the hurdles of approval, coverage, and reimbursement have been cleared, the adoption and dissemination of new technologies will ultimately depend on whether consumers and providers find them acceptable. Many factors can influence the extent to which new devices or procedures are used. For example, health care providers must be educated about the new technology and are unlikely to use it unless they believe that it will be beneficial for their patients. Providers also need to be reimbursed at a level that will allow them to recover the costs of using the technology. In this regard, “big-ticket” technologies may have a more difficult time with adoption than low-price items.
It is essential to educate women about new screening and diagnostic technologies as well. Women are not likely to undergo medical procedures unless they believe that the potential benefits outweigh the potential risks. Medical technologies must also be readily available in their own communities if women are to take advantage of them. Even in the case of a highly accurate breast cancer screening tool, it would be truly effective only if it was widely available and acceptable to women and used routinely by them.
The developers of new technologies will undoubtedly face questions about each of these issues during the adoption process. Much is already known about the adoption and dissemination of film-screen mammography, and this knowledge may prove instructive for the developers of other developing technologies. Experience from current mammography
Page 200
programs suggests that outreach to women, education of women and providers, and access to facilities and services may be as important as technical factors in saving lives.
HISTORY OF DISSEMINATION OF MAMMOGRAPHY
Mammography provides a good example of how social, cultural, and political factors, in addition to experimental data, can influence the dissemination of medical technologies into clinical practice because even the best scientific information is subject to interpretation (reviewed by Lerner, 2001).
Although the use of X-ray imaging for the detection of breast cancer was first suggested in the early years of the 20th century, mammography did not begin to emerge as an accepted technology until the 1960s (see Figure 1-1). Between 1930 and 1960 a number of technical innovations were introduced to produce higher-quality images that were more reproducible and easier to interpret. Subsequently, the developers of the technology promoted its use, and some physicians began ordering mammograms to help with the diagnosis of complicated cases in which the physical examination was inconclusive.
The early reports of mammography's ability to detect small cancers coincided with increased public education efforts on the part of organizations like the American Cancer Society (ACS), which had launched a “war on breast cancer.” Before the introduction of mammography, ACS encouraged women to perform breast self-examinations and to seek medical attention for any breast lumps that they found. The advent of mammography was seen as a potentially powerful new weapon in this war. Even in the absence of clinical trials to test the value of breast self-examination or mammography, earlier detection was intuitively thought to be a good thing.
As the results of the first randomized controlled trial for the assessment of mammography as a screening tool were published over a number of years, the real potential of mammography to reduce breast cancer mortality seemed to have been realized (about 30 percent fewer deaths among screened women than among unscreened controls for women over age 50). The screening technology then began to diffuse more widely, in large part because of a demonstration project (a noncontrolled study) organized by the National Cancer Institute (NCI) and ACS. When preliminary results suggested that screening resulted in breast cancer detection at an earlier stage, the press and anticancer organizations like ACS enthusiastically spread the news. Anecdotal stories of women, both famous and unknown, whose cancers had been detected by mammography added to
Page 201
the belief that screening was a great success. Women finally felt that they had some control over a terrifying disease.
By the late 1970s, mammography had diffused more widely into common clinical practice, but it had also become a source of considerable controversy. Advocates of the technology were enthusiastic about its ability to detect smaller, potentially more curable cancers, but critics questioned whether mammography, particularly for women age 50 and younger, actually caused more harm than benefit. Initial fears about the potential dangers of radiation exposure have largely been put to rest (although some questions remain for specific groups of women [see Chapter 1]), but concerns continued to build about the lead-time and length biases of screening and the possibility of overdiagnosis due to screening mammography (see Chapter 1). Most importantly, the analysis of the data from the original screening trial showed that the decreased death rate was statistically significant only among women age 50 and older. Many statisticians and some clinicians had recommended additional randomized trials for women between the ages of 40 and 50 rather than the demonstration project, but the organizers of the project had rejected this suggestion. Now it was the controversy over screening of women in this age group that received considerable attention from the press.
In an effort to help resolve the debate about the use of mammography in younger women, the National Institutes of Health (NIH) convened an expert panel for a consensus conference in 1977. The panel agreed that annual screening mammography of women over age 50 was appropriate but recommended that women ages 40 to 49 receive a screening mammogram only if they had previously had breast cancer or had a strong family history of breast cancer.
In the 1980s NCI, the American College of Radiology, and 11 other medical organizations followed the lead of ACS in recommending routine screening mammograms for younger women based on the findings of the demonstration project. Dissent reemerged in 1993, however, when NCI withdrew its support for this policy because of the growing amount of data available from a series of randomized controlled trials of mammography that included women in their 40s. Another NIH consensus panel was convened in 1997 in an attempt to resolve the issue. The panel again concluded that there was not enough evidence to support routine screening mammography for women in their 40s, but the controversy only escalated and many organizations continued to recommend screening for women in their 40s (see below and Table 6-1). Even the U.S. Senate joined in the fray, voting 98 to 0 to encourage NCI's National Cancer Advisory Board to reject the consensus panel's conclusions.
In retrospect, several commentators have pointed out that the experts on opposing sides of the screening debate have not really disagreed about what the data showed (a 16 to 18 percent reduction in breast cancer mor-
Page 202
|
Organization |
||||
|
Age |
ACS |
ACR |
AMA |
NCI |
|
20-39 |
Monthly BSE; CBE every 3 years. |
Same as ACS |
Same as ACS |
No recommendation |
|
Women at higher risk should consult with their physician about beginning mammography screening before age 40. |
Women at higher risk should consult with their physician about beginning mammography screening before age 40. |
|||
|
40-49 |
Monthly BSE; begin annual mammography and CBE at age 40. Women at higher risk should consult with their physician to determine their mammography schedule in their 40s. |
Same as ACS |
Same as ACS |
Mammography every 1–2 years for women in their 40s at average risk of breast cancer. Women at higher risk should consult with their physician to determine their mammography schedule in their 40s. CBE every 1–2 years. |
|
50+ |
Annual mammography and CBE, monthly BSE. |
Same as ACS |
Same as ACS |
Mammography every 1–2 years for women ages 50 and older |
Page 203
|
AAFP |
USPSTF |
ACOG |
ACP |
|
Monthly BSE, CBE every 1–3 years for women ages 30–39 |
Insufficient evidence to recommend for or against routine mammography or CBE or the teaching of BSE. |
Same as ACS |
No recommendation |
|
Monthly BSE, annual CBE |
Insufficient evidence to recommend for or against routine mammography or CBE or the teaching of BSE. |
Monthly BSE, annual CBE, mammography every 1–2 years |
Recommends against screening for women under age 50 |
|
Monthly BSE, annual CBE, and mammography |
Mammography with or without CBE every 1–2 years. Insufficient evidence to recommend for or against routine mammography or CBE for women ages 70 and older. |
Monthly BSE, annual CBE, and mammography |
Mammography every 2 years for women ages 50–74. Recommends against screening for women over age 75. |
NOTE: Abbreviations: ACS, American Cancer Society; ACR, American College of Radiology; AMA, American Medical Association; NCI, National Cancer Institute; AAFP, American Academy of Family Physicians; USPSTF, United States Preventive Services Task Force; ACOG, American College of Obstetricians and Gynecologists; ACP, American College of Physicians; BSE, breast self-examination; CBE, clinical breast examination.
SOURCE: U.S. Preventive Services Task Force (1996).
Page 204
tality, about half as great as that among older women) but, rather, how the data should be interpreted and acted upon. Opponents argued that 2,500 healthy women under age 50 would have to receive regular screening to extend one life, leading to many unnecessary interventions in women without any actual breast disease. They also were concerned by the lag time (10 years or more) between screening initiation and decreased mortality in women under age 50. The controversy continues today, even though mammography has been more thoroughly evaluated than any other screening test.
EVIDENCE ON USE AND ACCEPTANCE OF MAMMOGRAPHY BY WOMEN
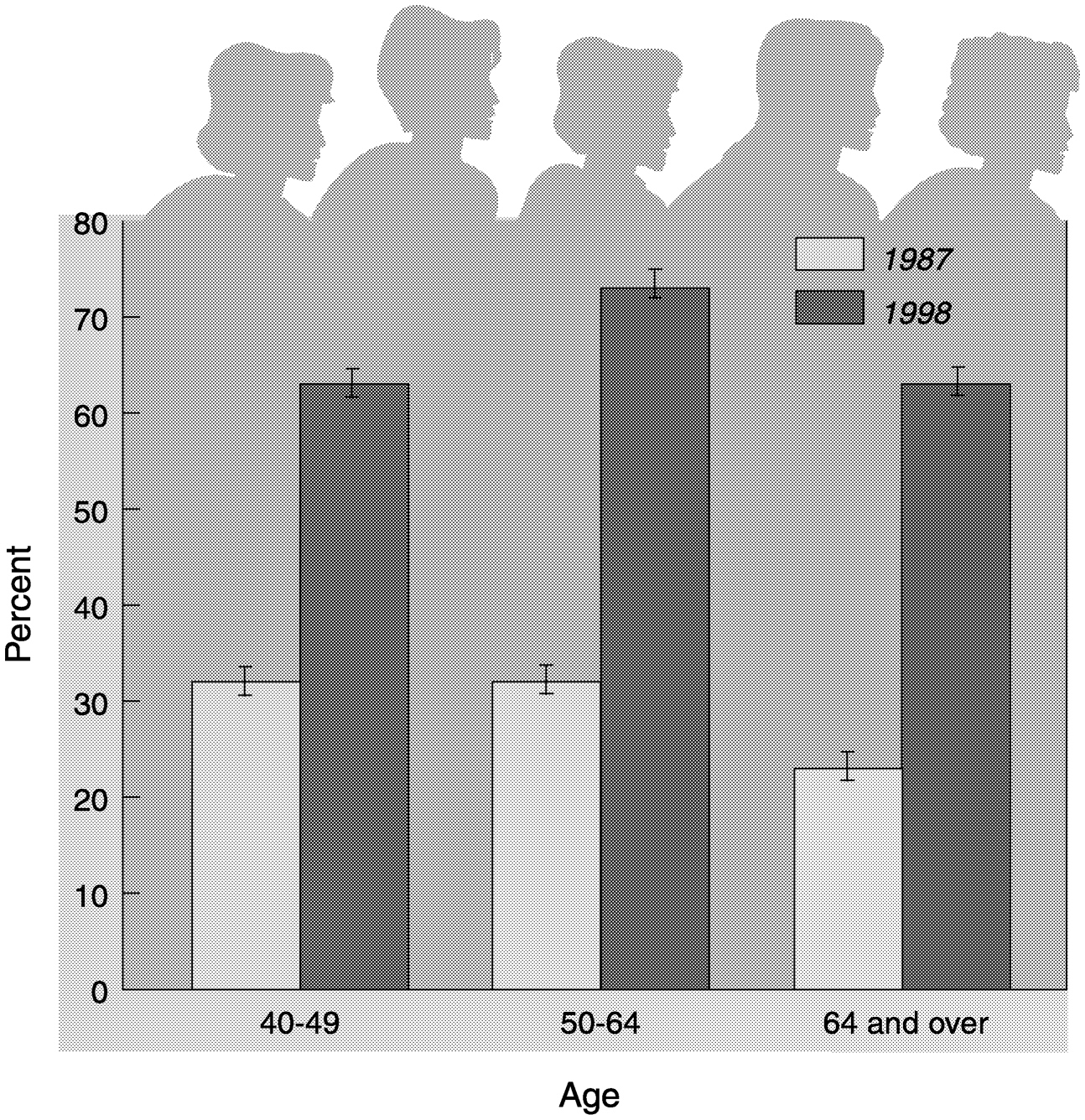
The use of screening mammography has increased greatly over the past decade (Blackman et al., 1999; Makuc et al., 1999; U.S. Department of Health and Human Services, 2000) (Figure 6-1). The percentage of women age 50 and over who reported having a recent mammogram rose to 69 percent in 1998, up from 61 percent in 1994 and 27.4 percent in 1987 (U.S. Department of Health and Human Services, 2000). However, despite this overall increase, many women do not follow the screening guidelines advocated by a variety of medical institutions by getting mammograms at the recommended intervals. One recent study found that 27 percent of women had the age-appropriate number of screening examinations, whereas 59 percent of women had been screened within the previous 2 years (Phillips et al., 1998). For 1998, the estimated number of U.S. civilian noninstitutionalized women over age 40 who reported that they had not received a mammogram within the past 2 years was 19.4 million, representing 33 percent of that population (Table 6-2). In comparison, the number of women in this age group who reported that they had not received a Pap test as a screen for cervical cancer in the past 3 years (the recommended screening interval) was 14.5 million, or 24.7 percent of that population. The percentage of women who had “recently” received a Pap test may be higher because of the longer screening interval, but other factors could also contribute to the difference. For example, Pap testing can be performed during a physical examination and thus does not require an additional visit, as mammography does. Notably, women between the ages of 40 and 49 are more likely to undergo screening for cervical cancer than for breast cancer, whereas the opposite is true for women over age 65.
Despite the generally positive attitude of most women toward screening mammography (Baines et al., 1990; Gram et al., 1990), some barriers clearly exist. Many reasons have been cited for the lack of breast cancer screening at recommended intervals, including limited access to health
Page 205
~ enlarge ~
FIGURE 6-1 Use of mammography by women 40 years of age and over, 1987 and 1998. Percent of women having a mammogram within the last two years. SOURCE: U.S. Department of Health and Human Services, 2000 (www.cdc/gov/nchs/products/pubs/pubd/hus/hus/htm). Data are based on the National Vital Statistics System, National Center for Health Statistics..
care and health insurance, lack of education and physician referral, pain or discomfort from the procedure, fear of what could be found, beliefs that mammograms are necessary only when symptoms arise, and inconvenience because of the location of the test facility (Baines et al., 1990; Rimer et al., 1989; Vernon et al., 1990). Some women with disabilities have also found mammography facilities to be inaccessible to them (Haran, 2000), and a report by the Centers for Disease Control and Prevention (CDC) found that women over age 65 with functional limitations were
Page 206
|
Age Group |
Number of women without a Pap test in the last 3 years, in millionsa (percent) |
Number of women without a mammogram in the last 2 years, in millionsa,b (percent) |
Estimates of the total civilian noninstitutionalized female population, in millions |
|
|
40 and older |
14.5 (24.7) |
19.4 |
(33.0) |
58.8 |
|
40–49 |
3.1 (15.1) |
7.5 +/− 0.25 |
(36.6) |
20.5 |
|
50–64 |
4.0 (20.3) |
5.2 +/− 0.20 |
(26.4) |
19.7 |
|
65 and older |
7.5 (40.3) |
6.7 +/− 0.22 |
(36.0) |
18.6 |
aThe screening interval for the given type of cancer that is recommended by USPSTF (with the exception of mammography for women aged 40 and over, which is not currently recommended by USPSTF)
bValues are means +/− standard errors.
SOURCE: Diane Makuc, Ph.D., Director, Division of Health and Utilization Analysis National Center for Health Statistics, 1998 data.
less likely than other women their age to have ever had a mammogram (Centers for Disease Control and Prevention, 1998).
Some of the major issues pertaining to the use of mammography are discussed below and were described in more detail in a recent Institute of Medicine (IOM) report, Ensuring Quality Cancer Care (Institute of Medicine, 1999). The authors of that report concluded that the underuse of screening mammography to detect breast cancer early, in conjunction with lack of adherence to diagnostic standards and treatment regimens, leads to reduced survival rates and, in some cases, compromised quality of life.
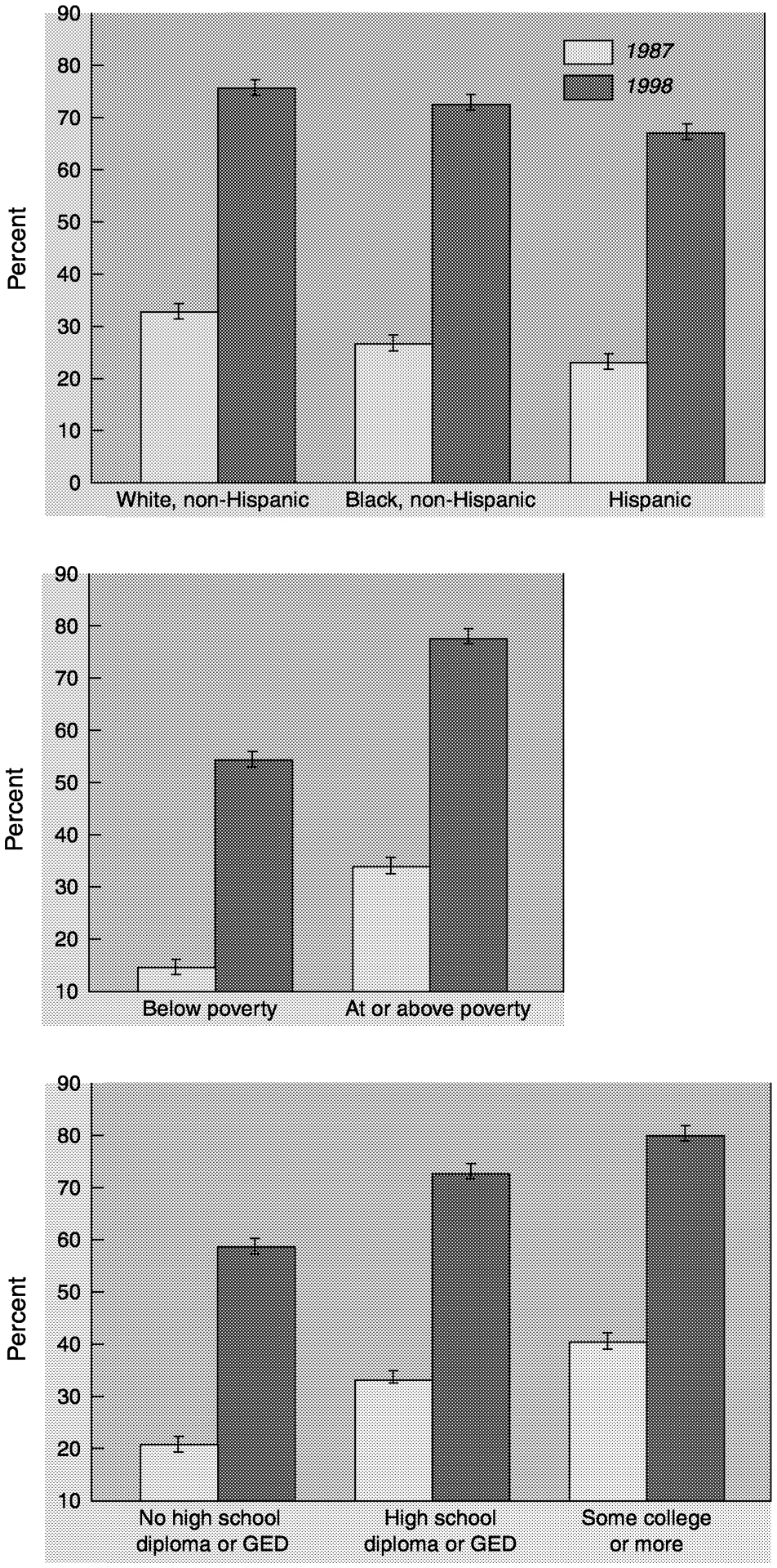
A great variety of interventions targeted toward women have been developed with the intent of increasing breast cancer screening rates, including multimedia educational interventions and peer counseling. Studies have shown that diverse campaign strategies directed toward women are needed to alter the screening behaviors of different groups of women, especially among medically underserved populations (Abbott et al., 1999; Wismar, 1999). The rate of mammography use varies by factors such as age, socioeconomic status, education, and ethnicity (U.S. Department of Health and Human Services, 2000) (Figure 6-2). For example, women between the ages of 50 and 65 are more likely to undergo screening mammography than women over age 65, even though the risk for and incidence of breast cancer are considerably higher among women in the latter age group (Table 6-2; see also Table 1-4).
A higher level of education and higher socioeconomic status are also
Page 207
~ enlarge ~
FIGURE 6-2 Use of mammography by women aged 50 to 64 according to various attributes (1987, 1998). Percent of women having a mammogram within the last two years. SOURCE: U.S. Department of Health and Human Services, 2000. ( www.cdc/gov/nchs/products/pubs/pubd/hus/hus/htm). Data are based on the National Vital Statistics System, National Center for Health Statistics.
Page 208
associated with a more frequent use of mammography (Katz and Hofer, 1994). Investigators have noted sizeable increases in the numbers of poor women as well as women whose family incomes are at or above the federal poverty level who have received screening mammograms. Poor women, however, are still less likely than women with higher incomes to receive screening. Among women whose family incomes were below the poverty threshold in 1998, 53 percent reported that they had recently received a screening mammogram, whereas 72 percent of women whose family incomes were at or above the poverty line reported that they had recently received a screening mammogram.
Very few studies have directly examined the breast cancer screening behaviors of immigrant women, but the available data suggest that the rates of screening among first-generation immigrants are significantly lower than the rates among women in other groups of the population (Wismar, 1999). Language and cultural barriers can make it difficult for immigrant women to obtain information about screening tests, and immigrants often have limited access to health care and insurance, a major reason why women are not screened. Having a regular source of health care (with or without insurance) is also significantly correlated with the use of screening mammography, independent of age, ethnicity, sociodemographic status, or other variables (Mandelblatt et al., 1999).
The U.S. Department of Health and Human Services recently set a breast cancer screening goal in the report Healthy People 2010.1 The report suggests that by the year 2010, it is reasonable to expect that 70 percent of all women over the age of 40 will have had a recent mammogram (within the last 2 years).
IMPEDIMENTS OF EFFECTIVE DIFFUSION OF MAMMOGRAPHY
Lack of Provider Compliance with Screening Recommendations
CDC found in a recent study that a significant fraction of women between the ages of 50 and 75 do not receive recommendations for screening mammography from their physicians (May et al., 1999). A review of the medical records for more than 1,000 women (ages 50 to 75) attending three clinics in an urban university medical center found that only 66 percent of the women received a recommendation for screening mam-
1Healthy People is a national health promotion and disease prevention initiative that brings together national, state, and local government agencies; nonprofit, voluntary, and professional organizations; businesses; communities; and individuals to improve the health of all Americans, eliminate disparities in health, and increase the number of years of healthy life and improve the quality of life (see
http://www.health.gov/healthypeople/).
Page 209
mography from their doctors. Another study found that older women reported less physician encouragement for screening than younger women (Grady et al., 1992).
Physician referral is one of the strongest predictors of mammography use, and the most frequently cited reason for not having a mammogram is that a woman's physician did not recommend one (Fox and Stein, 1991; Grady et al., 1992; Lane et al., 1996). Consequently, a number of strategies have been designed and tested for their ability to increase the number of physician-ordered screening mammograms. A recent meta-analysis examined the effectiveness of these various interventions intended to increase the rate of mammography use among women by encouraging physician recommendations for screening (Mandelblatt and Yabroff, 1999). The interventions were divided into three categories: behavioral, cognitive, and sociological. Behavioral interventions included a reminder or office system prompts. Cognitive interventions identified provider attitudes toward screening and breast cancer and provided focused educational material directed at increasing the rate of compliance with ordering of mammography. Sociological intervention strategies included nurse-based interventions or reorganization of the clinic. The results demonstrated that all types of provider-targeted interventions (behavioral, cognitive, and sociological) could increase the rate of mammography use (6 to 21 percent over that for controls) in a fashion similar to what has been observed for patient-targeted interventions (Yabroff and Mandelblatt, 1999). However, most studies analyzed changes in mammography use at only a single point in time, so it is difficult to discern the long-term effects of the interventions. If the programs do not lead to increases in the rates of regular screenings, the observed change in the rates of screening mammography may not translate into reductions in breast cancer mortality.
Contrary to intuition, combined strategies that targeted both patients and providers or that used multiple approaches (e.g., behavioral and cognitive approaches) did not appear to be more effective than single approaches or provider-targeted interventions alone (Mandelblatt and Yabroff, 1999). The reasons for this surprising finding are not known, but may include undefined effects on patient-provider communication and behavior. Alternatively, the results may indicate limitations of the studies and the analysis.
Inconsistent and Conflicting Guidelines
Practice guidelines for screening mammography have been developed by many different scientific and professional organizations (U.S. Preventive Services Task Force, 1996). Although some groups like the U.S. Preventive Services Task Force (USPSTF) use explicit evidence-based methods, in most cases the recommendations for screening have been
Page 210
based on a combination of expert opinion and a review of published studies. As a result, the guidelines vary with respect to the age at which screening should begin, how often a woman should be screened, and when screening should be discontinued (Table 6-1). This has led to some confusion on the part of both patients and providers and has generated considerable controversy. The guidelines have changed over time as new studies have been published, but there is not a universal consensus on the value of screening for women under age 50 or women over age 70 (see Chapter 1). Furthermore, the age range of 50 to 69 years, for which screening recommendations are most uniform, is to a large extent based on artificial boundaries chosen for study purposes. For any individual woman, these boundaries may not represent a real biological point at which the ratio of benefits to risks sharply increases or decreases. Among a population of women, this ratio is likely to change along an age continuum rather than at discrete boundaries. As a result, when interpreting the guidelines, women and their physicians may find it quite challenging to make appropriate, informed decisions about when and how often the woman should be screened for breast cancer.
Health System Issues
A lack of health insurance is clearly linked to lower rates of screening mammography (Hoffman, 1998). The type of insurance coverage that a woman has may also play a role in a woman's decision to undergo screening for breast cancer. For example, individuals covered by managed care plans have higher rates of cancer screening than those covered by fee-for-service plans (Potosky et al., 1998), although the gap may be narrowing. Among Medicare beneficiaries, those with private supplemental insurance are more likely to be screened for cancer than those with Medicare alone (Potosky et al., 1998), even though Medicare provides coverage for screening.
For women with adequate health insurance, screening mammography may still be unavailable if facilities are not readily accessible where they live (Katz and Hofer, 1994; Mandelblatt et al., 1995). Women living in both rural and inner-city settings are less likely to undergo cancer screening than those living in other urban locations, which often have more mammogram facilities.
Similar issues come into play with regard to monitoring women with abnormal screening results. As discussed in Chapter 1, a screening mammogram alone cannot definitively identify breast cancer. Abnormal findings on a mammogram must be followed up with additional diagnostic tests. In addition, early detection through screening for breast cancer is not beneficial unless appropriate medical interventions can reduce the numbers of deaths from breast cancer. However, many women do not
Page 211
receive appropriate follow-up care in the form of diagnostic tests and treatments for the same reasons noted earlier for a lack of screening (reviewed by the Institute of Medicine, 1999).
In 1990, the Breast and Cervical Cancer Mortality Prevention Act mandated the establishment of the National Breast and Cervical Cancer Early Detection Program because a significant number of women did not have access to screening mammography. Since its inception in 1991, the program has grown to cover all U.S. states and territories and annual funding has increased from $30 million to $167 million. The program targets hard-to-reach women who lack health insurance, with a focus on screening at recommended intervals. Approximately 60 percent of the budget is allocated for screening services, with the remaining 40 percent devoted to education and outreach, including special promotional events, culturally specific brochures, home visits, church-based presentations, and provider education. In all areas of its work, the program seeks to collaborate with a variety of public and private organizations.
The breast cancer screening and diagnostic services available through the program include clinical breast examinations, screening and diagnostic mammograms, breast ultrasound, fine-needle aspiration, and breast biopsy. The program's policy on new technology requires that when new and improved methods of detection become widely available and are shown to be most effective they should replace the methods currently in use. Screening is offered at a myriad of institutions and centers, including local health departments, federally funded community health centers, hospital-based clinics, and mobile mammography vans, but at present, the program serves only 12 to 15 percent of eligible women.
Funding for treatment of cancers detected through the program were initially not included, but federal legislation that results in the provision of funding for such coverage was recently passed.2 The Breast and Cervical Cancer Treatment Act gives states the option of providing Medicaid reimbursement for treatment of cancers detected through the CDC screening program, with federal and state governments sharing the costs. The bill must now be considered by each state legislature for adoption.
Financial Issues
A number of radiologists have raised concerns about reimbursement rates for mammography. Mammography is often seen as a money-loosing activity in radiology departments (Brice, 2000; Feig, 2000a,b; Kolb, 2000), and many believe that the current reimbursement rates do not
2The bill was approved by the U.S. Congress and signed by President Bill Clinton in October 2000.
Page 212
cover the actual total expense of providing the service (see the section on Reimbursement in Chapter 5). Others have argued that more efficient management, at least in high-volume centers, could improve the financial status of mammography facilities (Brice, 2000). If reimbursement does not meet the costs of providing mammography services, it could potentially lead to problems with access because facilities may close if they are not financially solvent. A recent study of seven university-based breast care centers found that all seven had lost money on the professional component of mammography. Other breast-related procedures also lost money, but the high volume of mammography made it more problematic for the centers (Brice, 2000). Likewise, a survey of mobile mammography facilities found that less than half were financially profitable or breaking even (Debruhl et al., 1996).
To date, there have been few documented cases of breast screening facilities closing because of financial difficulties, but some anecdotal cases of breast screening facility closings have recently been reported (Brice, 2000). Even if facilities are not closing, preliminary results from a recent survey of the Society of Breast Imaging (SBI)3 membership suggest that the capacities of screening facilities are not keeping pace with the increasing demand for mammography services. Half of the respondents indicated that waiting times for mammography appointments had increased at their facilities. Nine percent of respondents reported that their facilities will actually decrease their volume of breast imaging in the coming year for a variety of reasons, with reimbursement rates, rising costs, and lack of equipment or personnel topping the list.
Because of the perceived financial difficulties of mammography facilities, several options to make breast imaging more efficient and economically viable have been suggested (Feig, 2000b; Kolb, 2000), including the following:
-
streamlining the appointment processes for screening and follow-up procedures;
-
batch reading of mammograms;
-
making more efficient use of the radiologist's time by shifting all tasks that are not directly related to interpretation or consultation to other personnel;
-
accepting only self-paying patients to avoid reimbursement caps;
-
performing more interventional procedures such as biopsy and aspiration, which have higher reimbursement rates; and
3SBI is a national organization consisting of more than 2,000 radiologists who interpret the results of breast imaging studies. The survey of SBI members was carried out by ACS and the American College of Radiology. The results are based on 635 responses.
Page 213
-
renegotiating hospital contracts to balance losses from mammography with downstream profits from surgery, radiation therapy, and oncology treatment of cancers detected by mammography.
Training Issues
Mammography is one of the most technically challenging radiological procedures (U.S. General Accounting Office, 1998a,b). Ensuring the quality of the image is not easy, and reading the image is difficult because no criteria can absolutely distinguish benign and malignant lesions. As a result, the more experienced radiologists detect a greater percentage of breast cancers (Elmore et al., 1998b). Regulations promulgated under the Mammography Quality Standards Act require each facility to have a training program that meets a set of initial personnel training requirements and to maintain the continuing education and continuing experience of its staff.
With the increased use of mammography during the 1980s, the need for improved training of more radiologists became apparent, and mammography became a separate category on the oral examination of the American Board on Radiology (ABR) in 1989. In the early 1990s the number of breast imaging questions on the written examinations of ABR increased to equal that for each of the other nine subspecialty categories. In 1999, SBI assumed a leadership role in breast imaging education by developing both a residency and a fellowship training curriculum (Feig, 1999b). This undertaking was in response to a request made by the Curriculum Committee of the Association of Program Directors in Radiology that each subspecialty society develop goals and objectives, and a graded curriculum that can be mastered reasonably well by the residents within the allotted training time. The SBI Residency Training Curriculum contains extensive and detailed lists of key concepts in 14 subject areas and recommends that residents be familiar with several texts. The SBI Curriculum Committee concluded that the program should require 3 full-time-equivalent months in breast imaging, interpretation of a minimum of 1,000 mammograms, and performance of breast ultrasound and needle localization.
Despite the increased emphasis on training in mammography, the number of individuals undertaking specialty training may not be sufficient to meet the growing demand for breast screening services (Eklund, 2000). Nationally, the number of mammography fellowships has decreased by about 25 percent over the last 5 years (American College of Radiology survey) (Box 6-1), and a recent survey of radiology residents found that only 4 percent accepted fellowships in women's imaging in 1999 (Goodman et al., 2000). Although the current demand for trained mammographers has not been thoroughly examined or quantified, anec-
Page 214
BOX 6-1
|
Page 215
dotal reports from the field indicate that it is becoming increasingly difficult to fill vacant positions (Brice, 2000). There are similar reports that too few mammography technologists are being trained to meet the demand. According to the American Society of Radiologic Technologists, 1,800 technologists took the national mammography examination4 in 1999, less than half the number who took the test in 1997 (Martinez, 2000).
Legal Issues
A study by the Physician's Insurers Association of America (1995) found that allegation of error in the diagnosis of breast cancer is now the most prevalent reason for medical malpractice lawsuits among all claims against physicians and is associated with the second highest indemnity payment rate5 As mammography use has increased, both the number of malpractice suits filed and the sizes of the awards or settlements have increased. Radiologists are the specialists most frequently sued in malpractice suits involving breast cancer, and within the radiology community, concerns have been raised over trends in malpractice litigation and their potential effect on the practice of radiology (Berlin, 1999). Pathologists who interpret biopsy samples for the diagnosis of breast cancer have also raised similar concerns (Skoumal et al., 1996).
In addition to the increase in the number of claims that results naturally from an increase in the number of mammograms performed, at least two additional factors may contribute to the rise in the number of malpractice claims for failure to diagnose breast cancer. First, the legal doctrine is in the process of change: the advent of the “loss of chance” doctrine (Box 6-2) has lowered the hurdle to a legally acceptable claim. Second, jury verdicts in medical malpractice claims—and insurance settlements based on predictions of jury decisions—may reflect a change in public expectations.
The negligence basis
(Box 6-3) of the medical malpractice system in general is often criticized. There is only a weak correlation between the cases in which a malpractice claim is filed and those in which expert
4This examination was first offered in 1992. In addition to students taking the examination upon completion of their degrees, many of the people taking the examination in the first years in which it was offered were already working in the field. Thus, the noted decrease may be only partially due to the declining number of students enrolling in technologist training programs (Jerry Reid, Executive Director of the American Registry for Radiologic Technologists, personal communication, December 2000).
5The current Medicare reimbursement relative value units do not reflect the higher malpractice costs and risks of mammography compared with those for other radiology procedures (Farria and Feig, 2000). See
Chapter 5 for more detail.
Page 216
BOX 6-2
|
assessment identifies negligence (Brennan, 1996). Because the concept of “standard of care” is quite vague, even “the finest panel of medical reviewers” may not be able to classify “the majority of cases. . . as either due to medical negligence or not due to such negligence” (Rubin, 1997). Furthermore, juries often idealistically believe that medical technologies should be used whenever a patient might possibly benefit, even if the probability is quite low (Havighurst, 1998).
Most medical malpractice claims for breast cancer are due to missed diagnoses. Given that breast cancer is a potentially fatal disease that can strike a relatively young population, the potential severity of any failure to diagnose breast cancer (or the perception thereof) may also increase the likelihood of a favorable verdict or settlement. According to Brennan (1996), the severity of a patient's disability, not the occurrence of an adverse event or an adverse event due to negligence, is predictive of pay-
Page 217
BOX 6-3
|
ment to the plaintiff. Thus, the perceived severity of a “delayed” breast cancer diagnosis may be more predictive of a jury's verdict than the occurrence of a true medical “error” in the initial interpretation of a mammogram.
It is unclear whether the increase in malpractice claims for missed breast cancer diagnosis has had a negative effect on the availability of mammography services, as has been suggested by some. If the risk and financial burden of malpractice claims are deemed too great, some facilities may choose to discontinue their services. Likewise, if young radiologists in training view the field of mammography as too risky with respect to malpractice, they may choose other specialties, with a subsequent decline in the number of trained mammographers. However, to date there is no documented evidence that either of these phenomena is occurring.
POTENTIAL FOR RISK-BASED SCREENING
Since the time of the first randomized clinical trial conducted to evaluate screening mammography, questions have been raised about whether risk stratification could be used to identify populations for which screening would be most beneficial. The goal of risk profiling is to identify groups with a significantly higher or a significantly lower risk for breast cancer than that for the general population and to develop different screening strategies based on that risk. Such an approach could, in theory,
Page 218
increase both the efficacy and the cost-effectiveness of screening programs.
The current breast cancer screening recommendations are already based on age (because the risk of cancer increases with age) and gender (only women are screened).6 Attempts to base screening strategies on more specific characteristics such as family history or age at menarche or first pregnancy have largely been unsuccessful because the known risk factors for breast cancer are associated with comparably low relative risks (2 or less; see Box 1-2 for a definition of relative risk). Investigators have retrospectively evaluated data from clinical trials and case series studies to determine the proportion of cases that would have been identified if women had been selectively screened on the basis of certain risk factors for breast cancer. Unfortunately, these studies found that screening based on risk stratification could not be used to identify the majority of breast cancer cases (reviewed by Smith, 1999).
More recently, new attempts have been made to develop risk-based guidelines to aid the decision-making process for women who fall into age categories for which the general screening guidelines are inconsistent or controversial (Gail and Rimer, 1998). Models for the calculation of risk may help women and their physicians make decisions about the age at which screening should begin (for women under age 50), how often a woman should be screened, and when screening should be discontinued (for women over age 70).
With technological advances in screening and diagnostic methods has come renewed interest in developing specialized screening programs for women at different risk levels. For example, several large studies are under way to evaluate the use of magnetic resonance imaging to screen high-risk women (see
Chapter 2). Much of the effort has focused on women with dense breast tissue, a characteristic associated with an increased risk for breast cancer (Byng et al., 1998), as well as the reduced accuracy of screening mammography (Mandelson et al., 1995). Breast density is highest at menarche and declines with menopause and increasing age, but there is considerable variation in breast density among women at any given age. For example, among postmenopausal women, those on estrogen replacement therapy are likely to have denser breast tissue than those who forego such therapy (Laya et al., 1996). One impediment to the stratification of women on the basis of breast density is a lack of standardization for density classification, in part because of the inability to incorporate volume measurements in standard mammograms. If this difficulty
6Although men can and do develop breast cancer, the incidence among men in extremely low compared with that among women. Thus, screening of men for breast cancer is not recommended.
Page 219
can be overcome, then screening protocols could potentially be optimized by studying different approaches, such as the use of magnetic resonance imaging and ultrasound as adjuncts to mammography or other alternative screening techniques with large screening populations.
NEW ISSUES THAT ARISE WITH ADOPTION OF EMERGING TECHNOLOGIES
New technologies may provide additional choices for women and their physicians, allowing an individualized approach to screening and diagnosis that depends on a woman's specific needs and characteristics. At the same time, new technologies may add layers of complexity to the decision-making processes associated with screening and diagnosis. The current practice guidelines for breast cancer detection and diagnosis are already quite complex (see Figure 1-4), and the incorporation of new technologies will likely make it even more challenging to establish practice guidelines and to define a “standard of care.”
Economic considerations also accompany the adoption of new technologies. For example, if the rate of reimbursement for mammography is artificially low, as has been suggested by some directors of breast screening facilities, cost comparisons with new technologies will unfairly favor mammography. Furthermore, many new technologies may first be introduced as an adjunct to mammography (to improve its sensitivity or specificity, or both) and will therefore be used in a more limited fashion and have a smaller market compared with that for mammography. As more breast cancer detection technologies become available, competition among new technologies and with established technologies will likely increase, in effect further reducing the size of the market and thus limiting the profit expectations of developers. Equal access may also become an issue when new imaging technologies prove to be effective but are also significantly more expensive. If the adoption of expensive new technologies is limited to resource-rich health care settings, many underserved segments of the population may be denied access and disparities in the health of different groups may actually increase after their adoption. The effect that the recent advertising of new imaging technologies to the general public (on television and in print media) will have on patient demand and dissemination is as yet unknown, but it is likely to be significant.
SUMMARY
Use of screening mammography has increased greatly in the last decade, but it has not been universally adopted and accepted by women. Many eligible women have never had a mammogram, and of those who
Page 220
have been screened, a significant number do not undergo screening at the recommended interval. Because mammography is less than an ideal test, women have expressed a variety of concerns about undergoing screening by this procedure, such as discomfort from the procedure and fear of what could be found, including false-positive results.
Much of the controversy over mammography has focused on the recommendation for screening mammographies for women between the ages of 40 and 49, but more lives may be lost because women over age 50 do not get regular mammograms and follow-up care (Aronowitz, 1995). Physician recommendation is the single most important factor that determines whether women are screened, but outreach to and education of women are also important for improving the screening rate. Access to screening facilities, including geographic proximity and payment for the procedure, is an issue for many women as well. Currently, the CDC screening program, established with the intent of improving access for underserved women, reaches only 12 to 15 percent of eligible women.
As the number of women eligible for screening mammography increases (because of the changing age distribution of the U.S. population) and more women adopt the practice of routine screening, there will be increased demand for trained mammographers and certified screening facilities. Whether the medical care system is prepared to meet these needs is not clear, but some concerns have been raised in this regard. Although data are unavailable to confirm or refute such concerns, some suggest that the potential threats to future screening services may include the financial difficulties of some screening facilities, high rates of medical malpractice claims for missed breast cancer diagnosis, and anecdotal reports of a downward trend in the numbers of individuals enrolled in training programs in breast imaging.
Lessons learned from the adoption and dissemination of mammography may be informative as new technologies become available. However, because mammography was a “void-filling” technology, the adoption process for new technologies is likely to be quite different. New technologies may offer novel opportunities for breast cancer detection, but their adoption will ultimately depend on whether they can provide added value to current technologies and survive competition in the marketplace. If they can, screening and diagnostic procedures may become more tailored to individual women's needs, but at the same time, deciding on the appropriate course of action for a particular woman may become more complex.






















