
Page 17
1
Introduction
Nancy Mairs was barely aware she had developed a limp.* It had come on so gradually and she had been so busy over the past months that she had given it little heed. She had just moved with her husband and two young children from Boston to Tucson to start a new life as a graduate student in English literature. During the past year, she had had countless bouts of exhaustion, but what working mother of young children doesn't? Indeed, she was startled and somewhat offended when a fellow graduate student asked her why she was limping. Had she hurt herself? It was that question that finally jarred her enough to consult her family doctor who then referred her to a neurologist.
Readers of this report will immediately suspect that this woman has multiple sclerosis (MS). She does, but like so many other people with MS, it was the last thing she suspected. Multiple sclerosis sneaks up on people. The earliest symptoms are usually mild enough to be blamed on temporary causes such as fatigue or stress. It is often only after someone is diagnosed that they recall their history of episodic clumsiness, deep fatigue, or blurred vision.
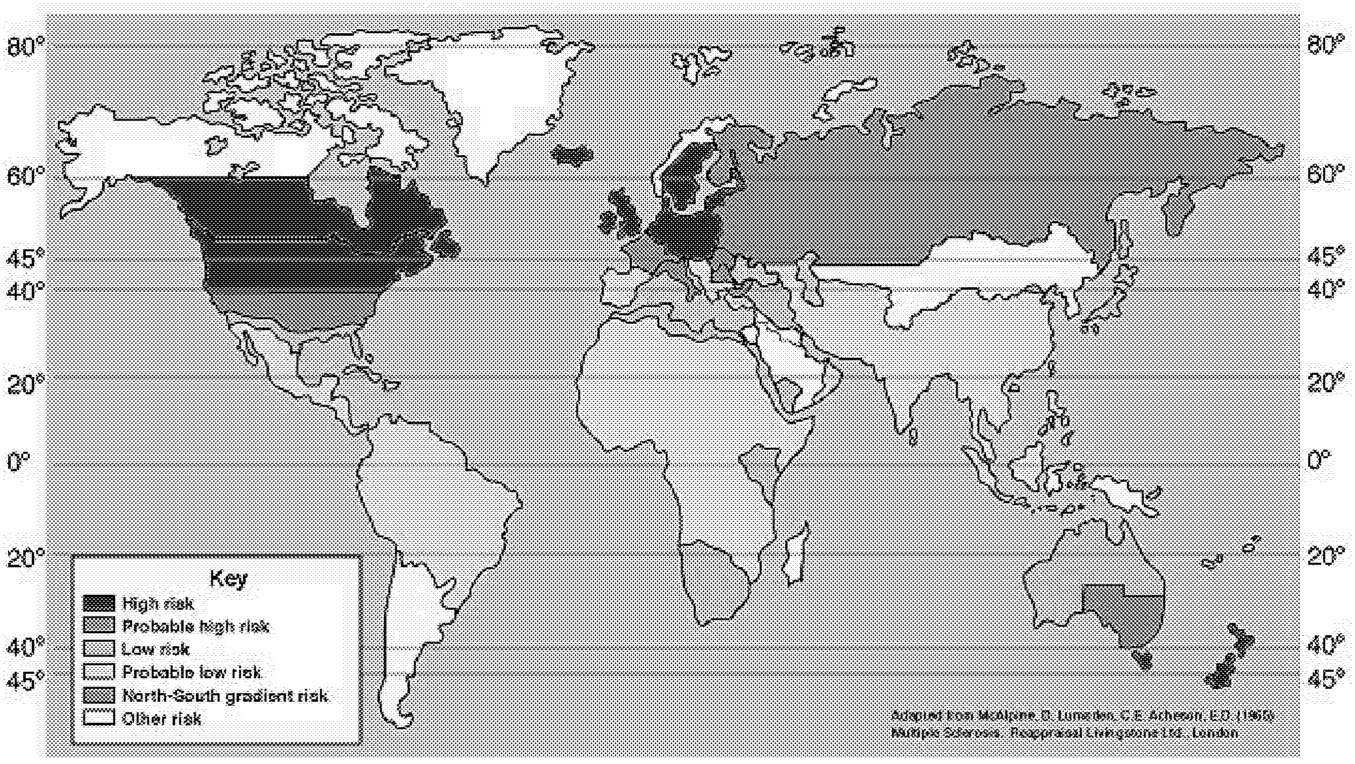
Although multiple sclerosis sneaks up on individuals, it is fairly predictable in populations. Approximately 1 in 1,000 people develop MS, usually in their late twenties, and about two-thirds of them are women. It is more common among people of Northern European heritage and more common among people who live in the high latitudes during childhood (Figure 1.1). Genetic factors can increase
*Taken with Nancy Mairs' permission from her autobiographical book on life with multiple sclerosis, Waist High in the World.3
Page 18
~ enlarge ~
FIGURE 1.1 MS distribution map. SOURCE: Adapted from McAlpine D, Lumadan CE, Acheson ED. 1967. Multiple Sclerosis a Reappraisal. Livingstone Ltd., London. Courtesy of John Rose and the Knowledge Weavers, University of Utah.
the risk of developing MS, but the precipitating event that somehow results in the immune system's attack on the nervous system remains unknown. The attacks may be few and far between with little or no impact on a person's ability to function, or they may cause a rapid progression toward severe disability. Most people with MS fall between these extremes and, on average, live only a few years less than the general population.
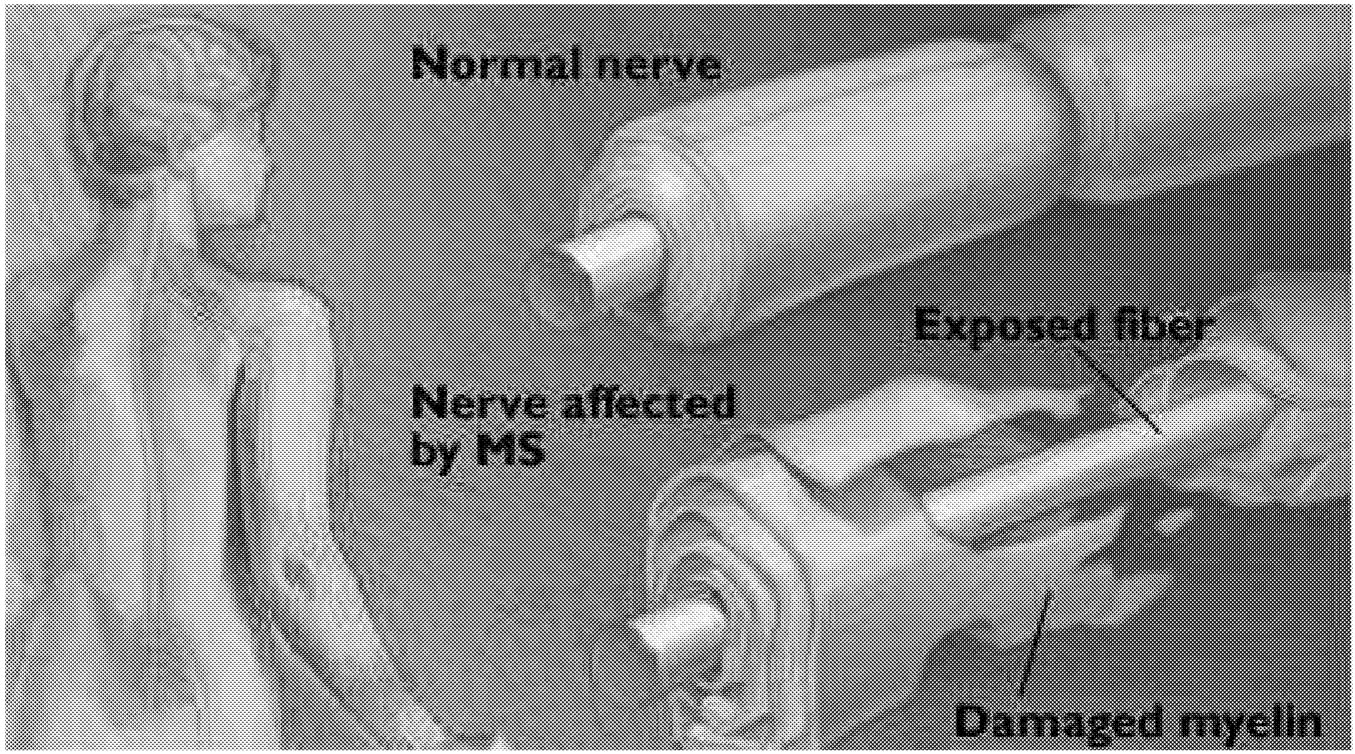
MS is probably an autoimmune disease, meaning that the body's natural defenses are turned against itself. Instead of destroying foreign cells, the immune system destroys the body's native cells. For example, in the autoimmune disease, Type 1 diabetes, the insulin-producing cells of the pancreas are destroyed. In MS, the myelin sheath that insulates nerve cells is destroyed (see Figure 1.2). Without the myelin sheath, nerve cells lose their ability to conduct nerve impulses. As the number of damaged nerve cells increases, the body loses its ability to perform the functions controlled by these cells.
This attack on the myelin sheath is believed to be orchestrated by blood-borne immune cells that invade the brain through the blood-brain barrier, the physical-chemical barrier that surrounds the brain and normally protects it from foreign and toxic substances circulating in the blood. The brain is thus normally resistant to infections that afflict the rest of the body. MS is one of the few diseases in which the blood-brain barrier is breached.
Page 19
~ enlarge ~
FIGURE 1.2 The nerve fiber in multiple sclerosis. SOURCE: Mayo Clinic Health Letter. Multiple Sclerosis: New leads into its cause and treatment. November 1995. Reprinted with permission of Mayo Foundation for Medical Education and Research.
THE U.S. NATIONAL MULTIPLE SCLEROSIS SOCIETY
The National MS Society (the MS Society) was founded in 1946 by Sylvia Lawry “to end the devastating effects of multiple sclerosis.” Her brother had been diagnosed with MS and doctors told her there was nothing they could do for him. In response, she established a foundation that would be devoted to research on MS. It was an optimistic era. Fatal diseases were being conquered in rapid succession. In the late 1920s, it was discovered that vitamin B12 could both prevent and cure pernicious anemia. By 1940, insulin was being used to control diabetes. Also, with the discovery of the curative powers of penicillin and streptomycin in the 1930s and 1940s, a major revolution in public health and medicine had been launched—the “age of antibiotics.” Each of these triumphs, marked by Nobel prizes, inspired the search for clear-cut cures.
However, much has changed since 1946. Many diseases, including MS, have disappointed those hoping to discover simple answers. Nevertheless, the study of MS has led to many improvements, in both quality and longevity, in the lives of people with MS. For the first time ever, treatments that can slow the progress of the disease are available, but still no cause or cure for MS has been found. MS remains a mysterious disease.
Page 20
BOX 1.1Recent Research Advances with Far-Reaching Implications for People with MSTHERAPEUTIC DEVELOPMENTS
BASIC RESEARCH DISCOVERIES THAT ARE IMPORTANT FOR NEW THERAPEUTIC STRATEGIES IN MS
|
Page 21
|
RECENT ADVANCES IN MS
In recent years, progress in MS research has accelerated (see Box 1.1). The 1990s saw the development of the first therapies that can modify the course of the disease. Admittedly, these therapies are not a cure, nor do they work equally well for all patients, but they are a major breakthrough. Twenty-five years ago, the possibility that human nerves damaged by disease could be repaired was almost unthinkable. Now, the many years of basic research on the development and function of nerve cells are beginning to bear fruit. A number of therapeutic strategies to repair nerve cells are under serious investigation to treat a variety of diseases and injuries. For the most part, these strategies are still experimental and remain to be proven safe and effective for human use, but they have the potential to revolutionize the treatment of neurological disorders.
ORIGIN OF THE STUDY
In December 1998, the National Multiple Sclerosis Society asked the Institute of Medicine (IOM) to undertake a strategic review of MS research on its behalf. The society selected the IOM because, in its words, the IOM offered a uniquely “broad, intellectual perspective.” The selection goes both ways. IOM studies are undertaken only upon approval from the National Research Council (NRC) Governing Board that oversees all studies of the National Academies, which includes the Institute of Medicine. To be approved, a study must be timely and of national significance. While this study is clearly significant for MS patients and the research community, its value also lies in its potential as a model for the development of similarly broadly based strategic research plans for other health fields.
Page 22
By the end of 2000, the MS Society will have spent more than $285 million to support research on MS. People with MS, their families, and friends are understandably discouraged that no cure has resulted from this 50-year effort. During this period, many diseases have succumbed in the face of concerted research efforts. Polio and smallpox are diseases of the past. Where cancer was once diagnosed with a prognosis of “years to live,” many people now recover to live many years after their diagnosis. Neurological diseases, however, are among the most difficult to study, and although beneficial therapies have been developed in the last decades for Parkinson's disease, Alzheimer's disease, and epilepsy, there is still no cure for any of the degenerative neurological diseases. MS is not alone in this regard. This is, nonetheless, a period of tremendous optimism about future therapeutic strategies, due in large part to the accelerating pace of new discoveries about the cellular machinery of the brain and spinal cord, as well as the information explosion emanating from the human genome project.
PREVIOUS REVIEWS OF MS RESEARCH PROGRAMS
Since 1973, various groups have met to review the status of research in multiple sclerosis. Each group had a somewhat different goal and each resulted in different initiatives.
1973 National Advisory Commission on Multiple Sclerosis
This commission laid out a detailed set of recommendations, to the point of recommending how much the MS Society should spend on specific projects.4 Among other proposals, it recommended that
-
$150,000 be spent in 1975, $300,000 in 1976, and $300,000 in 1977 for research on the demyelination and remyelination process of nerve cells in culture;
-
$10,000 be spent to disseminate information to physicians and nurses on the prevention and treatment of bedsores; and
-
$225,000 be spent in 1975, $400,000 in 1976, and $500,000 in 1977 for support of the first comprehensive treatment center devoted to the prevention of complications and disabling effects of MS rather than research on the disease process (all dollars are 1975 dollars).
Other recommendations included the establishment of a dedicated staff member to oversee multiple sclerosis research at the National Institute of Neurological Disease and Stroke (which was implemented and continues to this day), and the integration of MS research across the National Institutes of Health (which was not implemented).
Page 23
1986 IOM Workshop
In the mid-1980s, some members of the MS Society argued that more of the their funds should be spent directly on patient services and less on supporting basic research. At the invitation of the MS Society Board of Directors, the IOM convened a workshop to discuss the question, Should the hard-won dollars of single-disease-oriented voluntary agencies be spent on patient services or on lobbying to obtain a larger NIH budget, rather than on research?1 The participants included leaders of various health care foundations, and they strongly endorsed a continued commitment to the MS Society's support for basic research. They also recommended that the society set funds aside for innovative research projects that might not have enough preliminary data to be considered “safe” enough to risk a large investment. This was the origin of the pilot research program of the MS Society, which awards about 20 small grants (less than $30,000) each year. (Grants to individual investigators are generally funded at about $200,000 to $400,000 for three years.)
1996 MS Society Strategic Planning Retreat
The 1996 report reviewed the portfolio of MS Society research programs, which it strongly supported.5 The report recommended that the Society encourage research on gender-related issues and that programs be developed to encourage more physicians to do research. Both recommendations reflected current trends that transcended research in multiple sclerosis. Gender-based differences in immune responses had recently been recognized as more important than previously understood, and the combination of unprecedented levels of medical school debt, low grant funding rates, and changes in the U.S. health care system had all contributed to making a research career a discouraging prospect for potential physician-researchers. Although that report strongly supported the MS Society's research programs, there was some sentiment that it was inherently biased in having been written by a committee that was composed only of MS “insiders,” that is, members of the MS research elite who were unlikely to be critical of a society in whose decisions they were deeply involved and that also supported their own research.
1998 Review of the MS Society of Great Britain and Northern Ireland
The 1998 review identified results from the British MS Society's funding of research in the previous decade, as an accounting of how effectively it had used its resources during that period and, also, as a basis for considering future strategies to support research.2 The three primary recommendations on research funding were that (1) support of investigator-initiated projects should remain the backbone of the research program, (2) training mechanisms should be supported
Page 24
to recruit talented young investigators, and (3) a research advisory group should be established that would be composed of experienced scientists who are less dependent on MS Society funding than the current advisory council and that would include distinguished investigators in cognate fields. Overall, many of that committee's recommendations were that the British MS Society should operate more like its larger counterpart across the Atlantic Ocean, the National MS Society.
THE IOM COMMITTEE AND ITS MANDATE
The IOM committee was asked to review current scientific knowledge and to recommend strategic plans for future research, including laboratory and clinical research. In developing research strategies for the future, the committee was asked to look beyond both national and disciplinary boundaries to identify new ideas and new techniques that can be enlisted in the fight against MS. The committee was also asked to consider the roles played by different types of organizations that sponsor MS research. Private health organizations such as the MS Society, private firms, and the federal government each occupy different niches both in the scientific research community and for health care consumers or caregivers. Identifying how these different organizations can use their resources most productively toward “ending the devastating effects” of MS is important for everyone concerned. Further details of what the committee was asked to do are listed under the “Statement of Task” (see Box 1.2).
The committee was not asked to evaluate the MS Society's research program or grant review process. As noted earlier in this chapter, that has been done before. Indeed, the MS Society's research program has helped to model programs of other voluntary health organizations including the Arthritis Foundation, Cystic Fibrosis Foundation, Hemophilia Foundation, and the British MS Society.
Forming the study committee involved recruiting an intricate balance of a broad range of professional expertise and individual perspectives. The foremost consideration was that all members be considered by their peers to be among the very best in their areas of expertise. A second consideration was to form a committee whose thinking was not limited to the well-established research strategies in MS, but nonetheless included the in-depth knowledge of past and present research in MS and related fields needed to provide a solid foundation upon which new ideas could be weighed. Anyone currently in a policy-setting position at the MS Society was excluded from consideration.
The committee included people whose primary field of expertise is research on multiple sclerosis and those who worked in other fields; it included clinicians and basic researchers; people from academe and industry; those with experience managing research in government and private foundations; and researchers from the United States, Canada, Britain, and Germany (see Appendix A for committee
Page 25
BOX 1.2Statement of TaskThe Institute of Medicine will review current knowledge about the cause and treatment of MS and will develop a strategic plan to guide future investments. The goal of the study is to identify the potentially most productive research strategies for the field of MS as a whole; in particular, to identify the resources and strategies from disciplines not generally considered to be involved in MS research, but that might nonetheless expand the intellectual and technological resources from which researchers might draw in the fight against MS. The IOM will assemble a study committee of outstanding scientists and other experts from academia, industry, and other research and medical organizations that include health care practitioners, who are knowledgeable about the fields relevant to MS research, but whose careers are generally not focused on this disease. The committee will be charged with the following:
|
biographies). Different ways of knowing MS were also represented on the committee: those of someone living with MS, clinicians who treat MS patients, and scientists at the cutting edge of research, ranging from the study of fundamental brain mechanisms to clinical trials of treatments for neurological disease.
Page 26
HOW THE COMMITTEE CARRIED OUT ITS TASK
The committee supplemented its expertise through a series of background papers and three workshops. The background papers were written for the committee by experts on the different complications of MS such as pain, fatigue, and bladder problems (see Appendix B for the list of expert consultants). Each workshop was organized as a combined information-gathering and brainstorming session on one of the following themes: new technologies and research on the mechanism of disease in MS, new opportunities for the treatment of neurological disease, and research toward improving the quality of life for people with MS (see Appendix C for a list of workshop participants). To supplement the committee members' own experience treating MS patients, they also met with several people—some of whom have MS themselves—who work with MS patients in a variety of nonresearch settings, including nursing, outdoor adventures, and the Jimmie Heuga Center, an exercise and life-style management facility for people with MS.
Among the important audiences for this report are the architects and developers of multiple sclerosis research programs. The report covers a broad spectrum of MS research, ranging from strategies to develop treatments that impede the disease process, to treatments for specific symptoms, to research aimed at promoting successful adaptations to the illness including optimizing the abilities of people with MS to function in their daily lives. Throughout the study, the committee sought to identify windows of opportunity for research, such as those created by new discoveries about the self-repair mechanisms of the brain or new disease-specific changes in gene activation. The committee also sought to identify research needs where the windows of opportunity are less transparent, such as the development of evidence-based approaches for addressing the varied information needs of people with MS and for treating the fatigue and pain that so often accompany MS.
Ultimately, however, this report is for people with MS. It represents another chapter in the efforts of the National Multiple Sclerosis Society to conquer MS. Thus, the report also attempts to provide a readable, comprehensive review of what is currently known about MS, what needs to be learned, and the promises that research holds in the near future.
ORGANIZATION OF THE REPORT
Chapter 2 reviews what is known about the clinical and biological aspects of MS, including possible causes of the disease and the destructive mechanisms that leave the brain and spinal cord unable to perform their normal functions. It also reviews the research tools that hold the greatest promise to reveal those underlying disease mechanisms.
Page 27
Chapter 3 reviews what is known about the prevalence, causes, impact, and treatment of specific symptoms of MS such as fatigue, spasticity, and visual disturbances.
Chapter 4 focuses on the lives of people with MS and strategies for adapting to the illness. It also reviews the tools that are most important for research aimed at improving the lives of people with MS, specifically the tools that measure quality of life and functional status.
Chapter 5 looks forward and discusses research strategies and techniques that have the greatest potential to reveal new insights into the biology of the disease, insights that are likely to be crucial in the development of effective treatments.
Chapter 6 also looks forward, in this case reviewing critical issues and research for developing specific therapeutic strategies, with an emphasis on disease-modifying therapies. This chapter includes a discussion of challenges inherent in designing appropriate clinical trials in MS research.
Chapter 7 discusses building and supporting the research enterprise necessary to facilitate the most effective research strategies for MS.
Finally, Chapter 8 collates the key recommendations that emerge from discussions in the preceding chapters.
REFERENCES
1. , . 1987. The role of voluntary agencies in the funding of biomedical research. N Engl J Med.; 316: 1665.
2. , , . 1998. Review and development of a strategic plan of MS research. London, UK: MS Society of Great Britain and Northern Ireland.
3. . 1996. Waist-high in the world. A life among the nondisabled. Boston, MA: Beacon Press.
4. . 1974. Report and Recommendations: An Overview. Bethesda, Maryland: National Institutes of Health; Volume One.
5. . 1996. Strategic Planning Retreat for Research and Training Programs. Washington, DC: National Multiple Sclerosis Society.












