
Pain and Distress Caused by Experimental Procedures—Is It Time for a Reality Check?
Alicia Karas
Assistant Professor of Anesthesiology, Department of Clinical Sciences
Tufts University School of Veterinary Medicine
North Grafton, Mass.
As a veterinary anesthesiologist, I often speak about pain in clinical patients as well as laboratory animals. My experience is predominantly with pain caused by surgical interventions. Many years ago, at the time when we began to worry about having an IACUC, I was a laboratory animal technician. I am now an IACUC member and an investigator, so I am very aware of the problem of adding work or regulatory burden.
UP-FRONT REPORTING
In relation to whether the pain and distress classification systems are adequate, I think there is a different problem than just the wording. The problem I see is in the way people are complying with the policies and the regulations. I also believe that we are in some cases, as the HSUS contends, underreporting pain and distress and not adequately treating it because of the way we do things.
I think that most institutions probably suffer from an up-front reporting bias in actually recording the category, the number of animals, and the pain and distress category ahead of time. If you conducted a survey, you would find that most institutions probably use that information for their numbers at the end of the year, and it infrequently becomes altered.
Predictability
When the IACUC and the attending veterinarian decide ahead of time whether a given procedure should be in a pain category, the process suffers from limitations of predictability. I might know, for example, that a given type of
surgical procedure causes a particular amount of pain, but because this is science, we are not always doing exactly the same thing. We might be drilling a hole in the femur this week and putting in something that causes more pain than in previous experiments.
In addition, as mentioned in the HSUS April 2000 report, there is no category for procedures that cause pain and distress that were partially but not fully alleviated with drugs. Of course, pain medicine specialists will tell you that you are very seldom going to actually get rid of every single iota of pain felt post-operatively by a subject having surgery. As someone mentioned earlier this morning, a few investigators might give aspirin to their subjects and consider it to qualify as “giving analgesics”; however, these cases do not address the concern of whether pain and distress are adequately alleviated.
Another problem of up-front reporting is that it blinds people to reality: because a study is assigned to Category D, it therefore will remain in Category D. None of my colleagues in the institutions where I have worked have thought we should go back and reclassify a study after a pilot run.
We should ask whose responsibility it is to validate the category assignment. As Dr. Rowan asked, is it a lot of pain? Is it a little pain? Is it the responsibility of the IACUC, the investigator, the attending veterinarian?
Planning for Optimal Animal Care
With regard to study design, anyone who has been involved in research knows that it is not possible to write a protocol that is 100% accurate. You can try your best to decide what you are going to do, how you are going to do it, how you are going to treat pain, and how you are going to assess pain; but you may have to change it. Pain can last longer than predicted. Events happen. Problems happen. Sometimes a procedure takes longer than is predicted. It is less possible than predicted. Because of those things, flexibility in the way the IACUC views the investigator's protocol is an absolute necessity for optimal animal care.
HSUS also states, and others today have mentioned, the following: “Animal pain, distress, and suffering are not easy to recognize or measure unambiguously. There is considerable opportunity for legitimate disagreement among scientists.” I agree that pain, distress, and suffering are not easy to recognize. As stated in the Guide (NRC 1996), it is necessary to understand species-specific indicators of well-being. Pain and distress can be very difficult to predict and sometimes difficult to recognize; however, when we look at the animal, we are often going to find that it is necessary to revisit either the plan or the category assignment.
An example of this difference is the fact that two people can disagree. In my experience with a dog that had had a laparotomy to biopsy her liver, I worked with a gentleman who was a 20-year veterinary technician. He walked by this dog in the recovery room and said, “She looks great! ” He was referring to the fact that she was sitting up, I think. She was not screaming or making any noise, and he thought the dog was doing very well. I strongly disagreed and thought the dog was showing evidence of severe pain and/or distress. In fact, she was responsive to an additional dose of analgesic, and I saw a behavior change.
TABLE 1 Type of Pain Expected from Surgical Procedures
|
Mild to Moderate |
Moderate to Severe |
|
|
Based on my experience, I can tell you what types and what amount of pain are expected from certain surgical procedures (Table 1), but I sometimes have to rethink these expectations. Last week, I advised a student not to do an epidural on a dog to fix a lower limb fracture because I thought it would not be very painful. In fact, however, I was wrong. Again, flexibility is essential.
CATEGORY D
When we say that a study is in Category D and pain and distress will be alleviated by use of anesthetics, analgesics, or by other measures, do we then alleviate the condition? On our IACUC, we have been saying that if investigators do not give analgesics just because they do not know what to give and they do not know how to give it, they must put their study in Category E. Apparently, that course of action is not consistent with the policy.
I think that when animals still experience pain despite analgesic administration, it probably means that it is an ineffective choice of drug agent, or the wrong frequency or dose. It is necessary to change either the method or the category. I believe we need to have another category, that is, pain that was not able to be alleviated: Category D-2. This is simply an idea because I believe that most surgical interventions are not totally pain or distress free, even with medication. Although pain and distress may be largely alleviated, the biggest problem is that the investigator, and in many cases the laboratory animal veterinarian who might be the person who is consulted, is not likely to know how. I believe we need a lot of work in this area.
HSUS also states that “sensitive practical measures to gauge levels of distress in common laboratory animal species do not presently exist. For the most part, animal care staff rely on ad hoc observations or on relatively insensitive measures such as weight loss to ascertain whether animals are experiencing pain and/or distress.” Dr. Bayne made an excellent (albeit heartbreaking) point that things are more complicated than we even suspected. However, I actually take
the opposite view, which is that if we look at animals systematically, we will learn things. There is extensive literature on this subject, and evidence now exists for the behavior changes we see in animals. There is excellent work on how to assess pain in many different animal species, and I think it is possible to recognize much by careful study.
What then do we do? The method is not too difficult. Students scratch their heads and say, “I do not know how to tell if the animal is in pain.” I would respond, “Did you look at him?” “Yes.” “Did you touch him?” “No, I do not want to hurt him,” they say. The fact is, it is simply application of scientific method, and we are, after all, scientists. One can read the available literature (the IACUC will know what is available), make regular observations, evaluate data, draw conclusions, and apply those inputs for the sake of the animals. Those steps are key to developing humane animal care methods.
To record observations, I have borrowed an idea from Dr. David Morton, and I know Dr. Hampshire has done the same thing. Using a laboratory dog assessment form (Figure 1), writing in a graphical or chart format is often better than scribbled notes on a sheet of lined paper. It is possible to see how things are changing over time and to get an idea of how long the animal actually needs to be medicated, have activity restricted, have appetite tempted, and so forth.
PLANNING EXPERIMENTAL METHODS
Planning of experimental methods should take into account that revisions of the methods may be necessary. If you have not used a surgical model before, try a first run-through in a surgical study in a pilot study. Record and use those observations in later studies. Include documentation of assessments and of any revision. If that information is available to the IACUC, and the IACUC wants to look at an investigator 's study, they can request a formal monitoring sheet or assessment sheet such as Figure 1 to help them make their decisions even if they have not been in the laboratory seeing the animal. Documentation will help laboratory care personnel and other scientists and, of course, will benefit future work.
We found last week that we were working with some sheep that were about 100 pounds larger than sheep with which we had previously worked. Our plan simply to hold them, place a catheter, and give them an induction dose of anesthetic was not so easy because they outweighed all of us. We found that changing our method and giving them a premedication sedative, which is not necessarily commonly done, made things much easier on the sheep as well as on the scientists. Everyone benefits from something like that.
The IACUC must understand that assessing pain and distress caused by experimental handling procedures is a learn-as-you-go process in many cases. I have to disagree with Dr. Bayne's statement, that investigators are the experts on their animal models. In my experience, investigators are frequently coming from, for example, a contract research laboratory where they have been experimenting
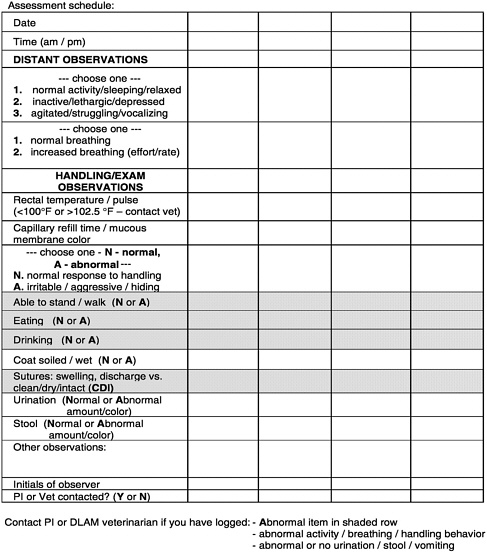
FIGURE 1 Laboratory dog assessment form.
with rats, and they want to use a procedure in a different model. Alternatively, the investigator may actually know the animal from a biochemical and on-paper point of view but not from an observation point of view. In fact, in many situations, investigators may see animals only during procedures, and the animal care staff and the veterinarian are the people who are watching the animals. I therefore disagree with that premise.
Although I believe that planning ahead helps, it cannot provide for all contingencies, no matter how careful you are. There must be some feedback loop, an
internal process for reviewing the pain and distress caused or alleviated and the measures taken. I believe the problem is not so much with the definition (although the regulators will claim to need it for their legal basis) but in the implementation and outcome.
The HSUS report also mentions that laboratory personnel can develop distancing mechanisms that help them cope but that often lead to people overlooking pain and distress. I want to make the point that distancing mechanisms are really a poor substitute for refinement. We could have not cared about how the sheep were doing, but in finding a better sedative for them, everyone was happier.
One major problem is the “disconnect” between the scientific community (including myself and others here from the scientific community), the investigators, and those who are developing and refining techniques. Are the investigators responsible for reading the refinement literature? They will say they have too much to do, and it is an admittedly difficult problem.
I think this disconnect is something that can be helped by training laboratory animal personnel in these methods, ensuring that they have a solid foundation. I actually took aside a college student who was working in our facility for the summer, and in 20 minutes, I was able to teach her to recognize more of pain and distress (pain in particular) than the investigator had led her to understand.
SCIENTIFIC JOURNAL REPORTING
HSUS also states correctly that there is limited published information about animals' experience of pain, distress, and suffering caused by typical laboratory procedures. I believe it was Dr. Zurlo, in a talk last year, who called my attention to a paper by Jane Smith and colleagues (Smith and others, 1997), which surveyed the biomedical literature and found that frequently you cannot tell what was done to animals by reading the published reports. I think that is a real problem because where else are the investigators getting their information?
In reading biomedical journals (which I now do fairly critically), I find many times that things were done and there is no mention of analgesics; there is no mention of whether the study was approved. I looked at one veterinary journal and found a paper written by at least two veterinarians in whose study dogs were anesthetized by mask isofluorane. They may have had very different dogs from those in my experience, because a dog with no premedication is quite difficult to mask down without a struggle. Then the authors had implants placed and to do that, they tunneled them from the neck to the flank and then turned them over, opened the abdomen, and implanted them into organs in the abdomen. Recovery was uneventful. That was it. No mention of analgesics or even whether the animals were euthanized at the end of the study. You can see that there is a big problem with what the authors actually reported doing to the animals. There is no mention of whether a few animals were lost due to problems with the technique in the beginning.
I would like to propose that when you review papers, you look for descriptions of animal care that include anesthesia and analgesia techniques. Look for specifics of acclimation and disposition and things such as whether animals were conditioned to be able to accept certain parts of the study. I believe that if we are not going to have these methods published, if we lack space that is precious in our research publications, then we must find some other place for that information. Many people are developing very interesting techniques to which we have been unable to have access. Our Internet user groups have made a huge difference because we can all speak to each other instead of talking on the telephone. We can speak to each other in large groups (and search previous conversations).
SUMMARY
The question in my mind is whether we should change the practice of up-front reporting of prospective pain and distress categories. I think the limitations of predictability can be overcome by appropriate observation and flexibility. Observation and documentation are key. If significant efforts are not made to assess and document pain and distress, then accurate reporting will never be possible. You will not know. No matter what method is used, we all might as well go home and not bother to redefine things anymore.
I believe that some sort of internal review must take place, and it can provide a reality check. The IACUC or the attending veterinarian, depending on the institution, can assume this role. Validation is achieved by periodic or even random (e.g., USDA inspections) IACUC review and consideration of category assignment. I realize that in proposing this, I am proposing that someone will be required to do more work.
I agree with HSUS that it is not beyond the scope and responsibility of the scientific community to determine underlying principles of pain and distress alleviation in animals, which can then be applied to various models and methods. I think it is not beyond our scope. It is going to take some work, but we can start right now by looking at the animals, at how they are doing, and documenting that information. We cannot say that everything went alright unless we check to see whether it did.
REFERENCES
NRC [National Research Council]. 1996. Guide for the Care and Use of Laboratory Animals. 7th ed. Washington, D.C.: National Academy Press.
Smith J.A., L. Birke, and D. Sadler. 1997. Reporting animal use in scientific papers. Lab Anim 31: 312-317.







