
1
Introduction
Tuberculosis is a treatable, communicable disease that has two general states: latent infection and active disease.1 With few exceptions, only those who develop active tuberculosis in the lungs or larynx can infect others, usually by coughing, sneezing, or otherwise expelling tiny infectious particles that someone else inhales.
After more than 30 years of declines in reported tuberculosis cases and deaths, the mid-1980s and early 1990s saw a reversal of that trend in the United States. Between 1985 and 1992, reported cases of tuberculosis increased by 20 percent, from 22,201 in 1985 to 26,673 in 1992 (CDC, 2000b).2 The case rate per 100,000 population increased by more than 12 percent, from 9.3 in 1985 to 10.5 in 1992. The number of deaths rose from 1,752 in 1985 to 1,970 in 1989. Especially alarming was the increase in the number of more lethal multidrug-resistant strains of Mycobacterium tuberculosis, the organism that causes the disease. In the early 1980s, about 0.5 percent of new tuberculosis cases were resistant to the two major drug treatments (isoniazid and rifampin). By 1991, the figure stood at 3.5 percent (Edlin, 1992).
Reasons cited for the increasing rates of tuberculosis and drug-resistant disease include the deterioration of public health programs aimed at preventing tuberculosis and encouraging completion of therapy for the disease (IOM, 2000). Incomplete treatment is a major cause of drug resistance. Increasing rates of HIV infection, homelessness, imprisonment, and immigration also contributed to the resurgence of tuberculosis. Depending on region and age group, up to 35 percent of those with tuberculosis were also infected with HIV.
The rise in tuberculosis, particularly multidrug-resistant disease, created considerable public alarm. For example, a 1992 opinion piece in the Washington Post on the combined threat of AIDS, substance abuse, and tuberculosis (headlined as the “three-headed dog from hell”) described tuberculosis as a deadly and highly contagious disease “that you could catch from the person next to you in a movie theater or classroom” (Califano cited in OTA, 1993, p. 28). Transmission of the disease under such conditions is not very likely, but the description illustrates the level of concern being voiced by some commentators at the time.
Figure 1-1 shows both the increase in the number of tuberculosis cases beginning in the mid-1980s and the subsequent decrease in the number of cases starting in 1993. By 1999, the number of cases nationwide had dropped to 17,528 (an all-time low), and the case rate stood at 6.4 per 100,000 population (also the lowest ever). The rate of multidrug-resistant tuberculosis stood at 1.2 percent of reported cases, approximately one-third the level in 1991. In addition, the death rate had dropped to 0.4 per 100,000 population in 1998 (the latest year for which data are available), down from 0.8 per 100,000 population in 1988.
National case rates mask considerable geographic variation in the incidence of tuberculosis. In 1999, case rates varied from less than 1.0 per

FIGURE 1-1. Reported cases of tuberculosis, 1978–1999. Source: IOM (2000) and CDC (2000b).
100,000 population in Vermont and Wyoming to more than 10 per 100,000 population in California (10.9), New York (11.0), and Hawaii (15.5) (CDC, 2000b). Some metropolitan statistical areas have even higher rates. For example, in 1999, case rates per 100,000 population were 17.7 for New York City and 18.2 for San Francisco. In 1998, the case rate in central Harlem was 63.7 per 100,000 population, which is similar to rates seen in developing countries such as Brazil (75 per 100,000 population) although it is far lower than the rates in the most severely affected countries, such as Zimbabwe (540 per 100,000) (Dye et al., 1999).
More than 40 percent of the tuberculosis cases reported in the United States in 1999 involved people born in other countries (IOM, 2000; CDC, 2000b). Individuals from Mexico, the Philippines, and Vietnam accounted for nearly half (45 percent) of these cases, with 151 other countries accounting for the remainder.
RISKS TO HEALTH CARE AND OTHER WORKERS
The resurgence of tuberculosis in the mid-1980s and early 1990s also affected health care workers and others employed in settings that served patients, inmates, or clients with tuberculosis. A number of high-profile outbreaks of tuberculosis—including cases of multidrug-resistant disease—were documented in hospitals, nursing homes, prisons, homeless shelters, and other settings (see, e.g., CDC [1994a], Dooley and Tapper [1997], and Garrett et al. [1999]). Most such outbreaks have been linked to lapses in infection control practices, delays in diagnosis and treatment of infectious individuals, and the presence of high-risk populations including people with HIV infection or AIDS and recent immigrants from countries with high rates of tuberculosis.
In 1999, of the 16,223 cases of tuberculosis for which occupational data were reported (92.5 percent of all reported cases), unemployed individuals accounted for nearly 60 percent of reported tuberculosis cases (CDC, 2000b). Such individuals accounted for less than 5 percent of the total workforce (BLS 2000a, 2000b). Health care workers accounted for about 2.6 percent or 422 of the cases in 1999. In 1998, health care workers accounted for about 9 percent of employed persons and 8 percent of tuberculosis cases among employed persons (Amy Curtis, CDC, 2000, personal communication) and about 5 percent of the total workforce. As discussed in Chapter 5, it can be difficult to determine whether tuberculosis in health care and other employed workers is due to workplace or community exposure.
Several health care and correctional workers have died of tuberculosis following documented work-related exposure to the disease (Dooley and Tapper, 1997), but no comprehensive mortality figures are available. Most of these workers as well as patients or inmates who died suffered
from poorly functioning immune systems related to medical conditions such as HIV infection or AIDS or to medical treatments such as cancer chemotherapy.
Newly reported outbreaks of tuberculosis in health care facilities have dropped off since the mid-1990s, but recent outbreaks have been reported in correctional facilities (see Chapter 5). Reports on facilities that experienced tuberculosis outbreaks in the late 1980s and early 1990s describe lapses in tuberculosis control measures followed by the implementation of new protective measures, and the subsequent reduction of worker exposures and new infections.
OVERVIEW OF REPORT
In 1999, the U.S. Congress requested that the National Academy of Sciences undertake a short-term study of occupational tuberculosis (P.L. 106–113, Conference Report 196–749). A committee of the Institute of Medicine (IOM), which is the health policy arm of the Academy, prepared this report. Consistent with legislative conference language, the committee focused on three questions:
-
Are health care and selected other categories of workers at a greater risk of infection, disease, and mortality due to tuberculosis than others in the community within which they reside? If so, what is the excess risk due to occupational exposure? Can the risk of occupational exposure be quantified for different work environments and different job classifications?
-
What is known about the implementation and effects of the 1994 Centers for Disease Control and Prevention (CDC) guidelines for the prevention of tuberculosis in health care facilities?
-
What will be the likely effects on tuberculosis infection, disease, or mortality of an anticipated Occupational Safety and Health Administration (OSHA) standard to protect workers from occupational exposure to tuberculosis?
The committee’s charge from Congress from this limited study did not include the development of recommendations for regulatory policy. It also did not include an evaluation of the costs or cost-effectiveness of the implementation of a standard.
According to the congressional request, work on this report was not to delay the issuing of the final rule, nor was the IOM study to be delayed pending the rule’s publication. When the study committee officially began work on April 1, 2000, publication of the rule was expected in July 2000. When the committee met for the final time in September 2000, the final standard had not been issued, and its status was uncertain following the change in control of the Executive Branch in January 2001. As explained
in Chapter 7, in the absence of the final standard, the committee focused on the conditions that a standard would need to meet to be effective.
The rest of this chapter briefly reviews responses to resurgent tuberculosis and proposed strategies for the elimination of tuberculosis in the United States and worldwide. Chapter 2 provides a basic review of tuberculosis transmission, infection, and disease. Chapter 3 discusses the proposed OSHA rule in the larger context of regulatory and other strategies used to protect worker health and safety. It also examines the statutory, judicial, and administrative frameworks within which the rule was developed. Chapter 4 summarizes the 1994 CDC guidelines and describes how the 1997 proposed OSHA rule differs from the guidelines. Chapter 5, 6, and 7 are organized around the three questions posed to the committee: the extent of occupational exposure to tuberculosis, the effects of the CDC guidelines, and the likely effects of an OSHA rule, respectively.
Appendix A describes the committee’s activities in more detail. Appendix B discusses the strengths and limitations of the tuberculin skin test, Appendix C reviews the literature on the occupational risk of tuberculosis, and Appendix D reviews the literature on the effects of workplace tuberculosis control measures. Appendix E discusses OSHA from a legal perspective. Appendix F reviews issues related to the use of personal respiratory protection devices and programs in health care and other settings. Appendix G lists the recommendations of another recent IOM report on strategies for the elimination of tuberculosis in the United States, and Appendix H includes brief biographies for members of the committee.
RESPONSES TO RESURGENT TUBERCULOSIS
Responses to Tuberculosis in the Community
The increase in tuberculosis case rates in the mid-1980s and early 1990s prompted public health authorities to revive and adapt traditional strategies to prevent and control tuberculosis in the community. Specific federal funding for tuberculosis control programs, which had virtually disappeared in the 1970s, resumed in the 1980s and increased substantially in the 1990s, as shown in Figure 1-2 (IOM, 2000). States and some cities and counties began to rebuild programs that had been neglected or dismantled in the 1970s and early 1980s.
A particular focus of federal, state, and community efforts was drug-resistant disease, particularly that related to inappropriate or incomplete treatment. One measure, directly observed therapy, targeted the failure of many with active tuberculosis to complete their full, several-month treatment regimen (Addington, 1979; Chaulk et al., 1995; ATS/CDC, 2000a). Physician failure to prescribe the appropriate drugs at the appropriate level and frequency for the appropriate period of time is another problem (Rao
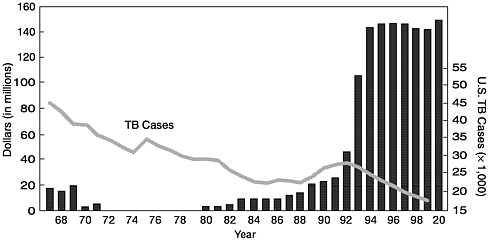
FIGURE 1-2. Trends in tuberculosis funding (CDC, fiscal years 1967–2000) and numbers of tuberculosis cases in the United States (in thousands). SOURCE: IOM (2000), p. 36 and CDC (2000b).
et al., 2000; Iseman, 1999a, 1999b). The development of practice guidelines and physician education programs are partial responses to such treatment errors (see Chapter 4), but physician awareness of and adherence to tuberculosis treatment guidelines remain concerns (DeRiemer et al., 1999; Evans et al., 1999). Other elements of the attack on drug resistant disease have included faster laboratory identification of drug-resistant strains of the disease (Tenover et al., 1993), surgical treatment of resistant disease, and the development of alternative drug regimens (Iseman, 1999a, 1999b).
Responses to Outbreaks in the Workplace
Outbreaks of tuberculosis in several health care and correctional facilities prompted additional actions by public health officials, health care and other managers, and those representing workers in these institutions (see Box 1-1 for a selective chronology). Federal and state investigations of these outbreaks often pointed to lapses in basic infection control protocols including failure to promptly identify and isolate suspected cases and failure to provide, maintain, and properly use negative-pressure isolation rooms designed for patients with infectious tuberculosis.
Beginning in 1990, CDC and other public and private health groups issued guidelines for the prevention and control of workplace transmission of tuberculosis in health care facilities, correctional facilities, and settings that serve homeless people (CDC, 1990a,b, 1992a, 1994b, 1996b). The 1990 CDC guidelines for health care facilities were adapted from earlier infection control guidelines. They did not reflect the changing epidemiology of the disease or the occupational safety and health perspec-
|
Box 1-1 Regulating Occupational Exposure to Tuberculosis: Selective Chronology of Events
|
tives evident in later guidelines (Nardell, 1997). The 1994 revision of the guidelines was a specific response to disease outbreaks in health care facilities and the contributing factors identified during investigations of the outbreaks. In 1995, the National Institute for Occupational Safety and Health, which is part of the CDC, certified a new class of respirator for use in preventing transmission of tuberculosis.
One problem faced by CDC in 1990 and then again in 1994 was the lack of rigorous, prospective, controlled studies documenting the effectiveness of individual protective measures in preventing workplace transmission of tuberculosis. Both the lack of research and the expected cost of tuberculosis control measures contributed to the controversy over the revised guidelines for health care facilities that CDC issued in draft form in 1993 and final form in 1994 (Sepkowitz, 1995).
In 1993, the Congressional Office of Technology Assessment observed that none of the measures described in CDC’s 1990 guidelines for health care facilities were thought to have been widely adopted (OTA, 1993, p. 6). Survey data supported these suspicions (see Chapter 6).
Groups representing health care and other workers created the Labor Coalition to Fight TB in the Workplace. In 1992, the coalition petitioned OSHA to issue an “advisory notice” with enforcement guidelines designed to protect workers from occupational exposure to tuberculosis. In 1993, it asked OSHA to issue a permanent standard (Labor Coalition, 1993).3 In addition to citing the 1990 CDC guidelines, the coalition cited enforcement guidelines issued by Region II of the Occupational Safety and Health Administration and by the state of California’s occupational safety and health agency. The Secretary of Labor announced in 1994 that OSHA would initiate a rulemaking process to establish formal standards to prevent workplace transmission of the disease. The U.S. Department of Labor, however, declined to issue the emergency temporary standard sought by labor groups, which had argued that the 1990 CDC guidelines were not being adequately implemented.
In 1993 and 1996, OSHA issued statements that emphasized the statutory obligations of employers to provide a safe workplace, described the applicability of certain existing regulations, and outlined procedures for investigating worker complaints and inspecting workplaces identified by CDC as having a higher incidence of tuberculosis than the general population (OSHA, Fact Sheet No. OSHA 93–43, 1993; OSHA directive CPL 2.106, February 9, 1996). Consistent with those statements, OSHA has cited or fined employers for failure to protect
workers from known hazardous conditions that put workers at risk of exposure to tuberculosis (ACCP/ATS, 1995). Recently, OSHA cited a federal agency, the Immigration and Naturalization Service, for such conditions (OSHA Region 6, 2000). Federal agencies cannot be fined by OSHA (see Chapter 3); the fines for an equivalent private-sector violator would have been $390,000.
In 1997, OSHA published a proposed rule (62 FR 201, October 17, 1997). It requested comments and information from affected groups. The proposed rule generated both support and opposition including lobbying by some groups for Congress to delay or block issuing of a final rule. In 1998, the agency conducted four public hearings. The agency reopened the public comment period in the summer of 1999, specifically requesting information and comments on homeless shelters and the agency’s preliminary risk assessment. Altogether, the agency received approximately 1,500 comments on the proposed rule including testimony at the four hearings and comments submitted when the record was reopened in 1999 (Amanda Edens, OSHA, personal communication, December 6, 2000).
THE BROADER PUBLIC HEALTH CONTEXT: ELIMINATING TUBERCULOSIS IN THE UNITED STATES AND WORLDWIDE
Today, tuberculosis is a largely preventable and curable disease. Nonetheless, it continues to cause disability and death, especially in poor and disadvantaged communities around the world. The combination of HIV infection or AIDS and tuberculosis and the rise of multidrug-resistant disease have refocused policymakers and public health authorities on the goal of eliminating tuberculosis in the United States and worldwide. Workplace programs to prevent the transmission of tuberculosis operate within these broader national and international contexts.
Eliminating Tuberculosis in the United States
In the recently released Institute of Medicine report Ending Neglect: The Elimination of Tuberculosis in the United States, another IOM committee set forth a broad strategy for the elimination of the disease in this country (IOM, 2000). The report argues that the resurgence of tuberculosis in the 1980s was the price exacted from disregard of earlier calls for a drive to eliminate the disease and from neglect of the public health infrastructure needed to control tuberculosis. It then goes on to propose a strategy to prevent a return to complacency and, eventually, to eliminate the disease in this country. The strategy includes five broad tasks:
-
maintaining control in an environment of declining disease incidence and a changing health care system;
-
speeding the decline in disease incidence and moving toward elimination of the disease by focusing on targeted skin testing and treatment of latent infection;
-
developing additional diagnostic, treatment, and vaccination tools;
-
increasing U.S. involvement in efforts to eliminate tuberculosis worldwide; and
-
mobilizing public support and measuring progress toward the goal of tuberculosis elimination.
The strategy emphasizes the importance of early diagnosis of latent tuberculosis infection and active tuberculosis, especially among immigrants from countries with a high-prevalence of the disease. It also stresses appropriate treatment of latent tuberculosis infection with the use of directly observed therapy, when indicated, to ensure the completion of treatment.
Although workers’ risk of tuberculosis is not explicitly discussed in the earlier IOM report, the success of a national tuberculosis elimination strategy would clearly benefit health care and other workers. Eliminating a hazard is much more effective than trying to control exposure to it a known or suspected danger.
Eliminating Tuberculosis Worldwide
With more than 40 percent of the tuberculosis cases in the United States involving people born in other countries, policymakers and public health authorities cannot ignore the global problem of tuberculosis. As noted above, a key recommendation of the recent IOM report on tuberculosis elimination in the United States was that this country should “expand and strengthen its role in global tuberculosis control efforts” (IOM, 2000, p. 11). Another recommendation was that those applying for immigration visas from countries with high rates of tuberculosis be tested for tuberculosis and that those with positive tests be evaluated and, if indicated, treated before being issued a permanent residency card.
Eliminating tuberculosis in the United States is a challenge that pales beside the challenge of eliminating tuberculosis worldwide. According to the World Health Organization (WHO), approximately one-third of the world’s population is infected with M. tuberculosis (WHO, 1996, 2000b). Each year about 8 million people are newly diagnosed with the disease, and about 95 percent of these people live in developing countries (WHO, 1996, 2000b). Worldwide, tuberculosis kills about 2 million people yearly. It accounts for more deaths among adults than AIDS, malaria, and all other infectious diseases combined.
In 1993, the WHO declared a global tuberculosis emergency, and it has stated that “poorly managed TB programmes are threatening to make
TB incurable” (WHO, 2000a, p. 2). Twenty-two countries4 account for nearly three-quarters of all new cases of the disease, and WHO has targeted them for special attention and assistance (WHO, 2000a).
WHO recently issued guidelines for the prevention of tuberculosis in health care facilities in resource-limited settings (WHO, 1999). The measures emphasize relatively inexpensive control measures involving natural ventilation (e.g., opening windows and providing special open-air areas for people waiting for care or visiting infectious patients). The focus is on firstline district health care facilities that lack the resources to support more expensive measures such as negative-pressure isolation rooms and personal respirators, which are advised only for referral facilities. Tuberculin skin testing is recommended only in research settings and at sites that offer preventive therapy for latent infection. Although these recommendations are aimed at resource-poor countries, they may also, under some circumstances, be relevant for some settings in this country. For example, crowded, underfunded homeless shelters may, when weather permits, have people with suspected tuberculosis wait outside in fresh air until transportation and treatment can be arranged.
CONCLUSION
Although tuberculosis is still a major killer in poor countries, 50 years of effective drug treatment has greatly reduced the toll that the disease takes in the United States. Nonetheless, the resurgence of the disease in the mid-1980s and early 1990s and the rise of multidrug-resistant disease demonstrate that tuberculosis remains a threat that public health programs cannot afford to ignore. Likewise, outbreaks of the disease in hospitals, prisons, and other facilities have underscored the potential for harm to nurses, doctors, guards, and others who work with people at increased risk of tuberculosis.
Will government mandates be effective in protecting health care and other workers from tuberculosis? The final chapter of this report considers this question. The next five chapters provide the foundation for that assessment by reviewing the basic features of the disease and its treatment, describing the legal context for OSHA regulations, comparing the regulations proposed by OSHA in 1997 with the voluntary guidelines published by CDC in 1994, examining the historical and recent occupational risk of tuberculosis, and evaluating the implementation and effects of the 1994 CDC guidelines.











