
Chapter 4
The Role of Adaptive Behavior Assessment
NATURE AND DEFINITION OF ADAPTIVE BEHAVIOR
Adaptive behavior has been an integral, although sometimes unstated, part of the long history of mental retardation and its definition. In the 19th century, mental retardation was recognized principally in terms of a number of factors that included awareness and understanding of surroundings, ability to engage in regular economic and social life, dependence on others, the ability to maintain one’s basic health and safety, and individual responsibility (Brockley, 1999). Today, fulfillment of these personal and social responsibilities, as well as the per-
This chapter contains material drawn from an unpublished paper commissioned by the committee from Sharon Borthwick-Duffy, Ph.D., University of California, Riverside.
formance of many other culturally typical behaviors and roles, constitutes adaptive behavior.
By the close of the 19th century, medical practitioners diagnosing mental retardation relied on subjective or unsystematic summaries of such factors as age, general coordination, number of years behind in school, and physiognomy (Scheerenberger, 1983). These practices persisted over that century because of the absence of standardized assessment procedures. And many individuals who would currently be considered to have mild mental retardation were not included in these early definitions.
Professionals voiced early caution about diagnosing mental retardation solely through the use of intelligence testing, especially in the absence of fuller information about the adaptation of the individual. In addition, mitigating current circumstances (not speaking English) or past history (absence of schooling) were often ignored in the beginning years of intelligence testing (Kerlin, 1887; Wilbur, 1882). At the turn of the century, intelligence assessment placed primary emphasis on moral behavior (which largely comports with the current construct of social competence) and on the pragmatics of basic academics. (Chapter 3 provides details on the development of intelligence assessment.)
Alternative measures to complement intelligence measures began to appear as early as 1916. Edger Doll produced form board speeded performance tests, which were analogues to everyday vocational tasks. During the 1920s, Doll, Kuhlmann, and Porteus sought to develop assessment practices consistent with a definition of mental retardation that emphasized adaptive behavior and social competence. Their work in this area sparked broadened interest in measurement of adaptive behavior among practitioners serving people with mental retardation (Doll, 1927; Kuhlman, 1920; Porteus, 1921; Scheerenberger, 1983).
Doll emerged as a leader in the development of a psychometric measure of adaptive behavior, called social maturity at that time. His work emphasized social inadequacy due to low intelligence that was developmentally arrested as a cardinal indication of mental retardation
(Doll, 1936a, p. 35). Doll objected to the definition of mental retardation in terms of mental age, which had proven problematic in IQ testing (because it resulted in classification of a significant proportion of the population). In 1936, he introduced the Vineland Social Maturity Scale (VSMS—Doll, 1936b), a 117-item instrument. The VSMS, which measured performance of everyday activities, was the primary measure used to assess adaptive behavior, social competence, or social maturity for several decades. One concern that emerged over time was that it was developed and normed for use with children and youth. It did not cover adults and had a limited range of items tapping community living skills (Scheerenberger, 1983).
The assessment of adaptive behavior became a formal part of the diagnostic nomenclature for mental retardation with the publication of the 1959 manual of the American Association of Mental Deficiency (Heber, 1959, distributed in 1961). The 1961 manual (Heber, 1961) discussed adaptive behavior with respect to maturation, learning, and social adjustment. This framework, reiterated in 1983, described adaptive behavior limitations consisting of “significant limitations in an individual’s effectiveness in meeting the standards of maturation, learning, personal independence, or social maturity that are expected for his or her age level and cultural group, as determined by clinical assessment and, usually, standardized scales” (Grossman, 1983, p. 11).
The 1983 manual characterized the tasks or activities encompassed by adaptive behavior (and, plausibly social competence) as:
-
In infancy and early childhood: sensorimotor development, communication skills, self-help skills, socialization, and interaction with others;
-
In childhood and early adolescence: application of basic academic skills in daily life activities, application of appropriate reasoning and judgment in mastery of the environment, and social skills—participation in group activities and interpersonal relations; and
-
In adolescence and adult life: vocational and social responsibilities.
During the 1960s, a wider variety of adaptive behavior measures was developed and disseminated (e.g., Allen et al., 1970; Balthazar & English, 1969; Leland et al., 1967). Indeed, by the late 1970s, the number of available adaptive behavior measures, largely interview or
observational in format, had burgeoned, including checklists pertaining to vocational behaviors (Walls & Werner, 1977). Measures developed in the 1960s have typically been updated in subsequent editions with enhanced psychometric characteristics and scoring (e.g., Sparrow & Cicchetti, 1985).
Over the past 25 years there has also been further refinement of the parameters and structure of tests of adaptive behavior and social competence. This refinement was based on large samples of research participants and data from service registries (McGrew & Bruininks, 1990; Siperstein & Leffert, 1997; Widaman et al., 1987, 1993). Novel frameworks for conceptualization of adaptive behavior have been proposed (American Association on Mental Retardation, 1992), and conventional frameworks have been endorsed for application in differential diagnosis and classification practices (Jacobson & Mulick, 1996). Finally, the difficulties and complexities of differentiating mild mental retardation from its absence or from other disabling conditions (e.g., Gresham et al., 1995; MacMillan, Gresham, et al., 1996; MacMillan, Siperstein, & Gresham, 1996) have remained an enduring concern in both professional practice and policy formulation.
Differing Conceptualizations
In Chapter 1 we summarized the history of definitions of mental retardation and discussed their relevance to the Social Security Administration’s definition. At first glance, current definitions seem to be quite similar; however, there are subtle differences in the conceptualization of adaptive behavior that may affect the outcomes of diagnostic decisions for individuals with mental retardation, particularly those in the mild range.
In the recent Manual of Diagnosis and Professional Practice in Mental Retardation (Jacobson & Mulick, 1996), Division 33 of the American Psychological Association put forth a definition of mental retardation that emphasizes significant limitations in intellectual functioning and adaptive behavior. The definition also views adaptive behavior as
a multidimensional construct, in that the definition is expanded to include “two or more” factor scores below two or more standard deviations. In describing mild mental retardation, there is minimal reference to adaptive behavior problems, except for the inclusion of “low academic skill attainment.”
It is important to note that the Division 33 definition places equal importance on the constructs intellectual functioning and adaptive behavior. The definition speaks to the presence of significant limitations in intellectual functioning and significant limitations in adaptive behavior, which exist concurrently. The term “concurrently” suggests an interdependent relationship in which both constructs are equally important. In this definition, the order of the constructs can be switched without affecting the validity of the definition.
The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), published by the American Psychiatric Association (1994), definition of mental retardation also has a cutoff of two standard deviations below the mean for intelligence, making an IQ cutoff of 70 to 75 acceptable for a diagnosis of mental retardation. In contrast, there is no mention of a standardized score or cutoff point for operationalizing any “significant limitations in adaptive behavior,” even though it is suggested that one or more instruments be used to assess different domains from “one or more reliable independent sources” (p. 40). The implicit rationale for not providing any statistical criteria for adaptive behavior testing is based on the existing limitations in instruments that measure adaptive behavior, specifically in terms of the comprehensiveness of measuring all domains and the reliability of measuring individual domains. Furthermore, issues are raised about the degree to which existing instruments are able to take into account the cultural context in assessing an individual’s adaptive behavior. One of the key themes throughout the DSM-IV definition is the cultural aspect of adaptive behavior. For example, adaptive behavior is defined in terms of effectively coping with common life demands and the ability to meet the standards of personal independence for a particular age group with a specific sociocultural background.
The DSM-IV definition identifies four levels of mental retardation based on IQ: mild, moderate, severe, and profound. No mention is made of the degree of severity of adaptive deficits for each of these levels, nor of the number or types of impaired adaptive behavior domains at each level. The DSM-IV definition places a greater emphasis than the Division 33 one on intelligence than on adaptive behavior, defining mental retardation as “significantly sub-average general intellectual functioning accompanied by significant limitations in adaptive functioning” (p. 39). In using the term “accompanied,” the definition suggests that adaptive behavior is a supplementary variable to intelligence, although both criteria must be present.
The World Health Organization (1996) also includes a definition of mental retardation in its International Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10). ICD-10 views the relationship between intellectual functioning and adaptive behavior as causal, with deficits in adaptive behavior resulting from deficits in intellectual functioning.
In describing the different severity levels of mental retardation, the ICD-10 guide presents IQ levels not as strict cutoffs but as “guides” to categorizing individuals with mental retardation. There is no mention of any standardized cutoffs for adaptive ability, except for mention of the use of “scales of social maturity and adaptation” in the measurement of adaptive behavior.
In the characterization of mild mental retardation, the ICD-10 guide points out that, “some degree of mild mental retardation may not represent a problem.” It goes on to state that the consequences will only be apparent “if there is also a noticeable emotional and social immaturity.” This statement implies that for individuals with mild mental retardation, intellectual deficits are apparent only when represented by problems in adaptive behavior (emotional and social immaturity). Furthermore, “behavioral, emotional, and social difficulties of the mildly mentally retarded . . . are most closely akin to those found in people of normal [range of] intelligence.” It is important to note that the terminology used in the ICD-10 is international English rather than North American English, and that, as a result, word usage in ICD-10 is
not entirely consistent with contemporary North American terminology with respect to functional limitations or depiction of social performance.
The most cited definition in the field is that of the American Association on Mental Retardation (AAMR). In their most recent classification system (American Association on Mental Retardation, 1992), AAMR defines mental retardation as subaverage intellectual functioning existing concurrently with limitations in adaptive skills. These limitations in adaptive skills are operationally defined as limitations in two or more of ten applicable adaptive skill areas (e.g. self-care, home living, social skills, self-direction, health and safety, etc.). The definition also includes the notion that adaptive skills are affected by the presence of “appropriate supports” and with “appropriate supports over a sustained period, the life functioning of the person with mental retardation will generally improve.”
AAMR departs significantly from other organizations by eliminating the grouping of individuals with mental retardation into levels of severity. AAMR no longer differentiates, either qualitatively or quantitatively, differences in intellectual or adaptive functioning of individuals with mild, moderate, severe, and profound mental retardation. Instead, they differentiate individuals with mental retardation based on the supports they need. The result is that the unique aspects and characterization of individuals with mild mental retardation are no longer the basis for differentiating them from more moderately and severely involved individuals. In so doing, AAMR ignores the substantial theoretical and empirical foundation that validates the difference between individuals with mild mental retardation and other individuals with mental retardation (MacMillan et al., in press).
Among these four definitions, there is little variation in the intelligence construct for individuals with mental retardation. The differences occur rather in their consideration of the contributing role of adaptive behavior. In some definitions (Division 33 and AAMR), adaptive behavior is construed as distinct from intellectual functioning and of equal importance, while in other definitions it is considered a result of deficits in intellectual functioning. The definitions also
vary as to whether they consider adaptive behavior to be made up of a single factor or to have multiple factors or domains. In the definitions that imply a multifactor construct, deficits in adaptive behavior must be specified in a certain number of areas/domains. With regard to identifying decision-making criteria, Division 33 presents the only definition that employs a statistical cutoff based on standard norms. In contrast, the other definitions employ more qualitative terms, which are open to interpretation in describing deficits and limitations in adaptive behavior.
Dimensions of Adaptive Behavior
Structure
Multidimensional or Unidimensional? Answers to this question have been mixed. Meyers et al. (1979) concluded from their review of factor analytic studies that adaptive behavior was definitely multidimensional and that the use of a total score would be inappropriate to indicate a general level of adaptation. Their view has been both supported and disputed in the past two decades, and there are currently firm adherents on each side of this issue. McGrew and Bruininks (1989) and Thompson et al. (1999) have concluded, for example, that the number of factors emerging from factor analyses depends on whether data were analyzed at the item, parcel, or subscale level, with fewer factors found for subscale-level data than item- or parcel-level data.
They also found that it was not the selection of the instrument that determined the number of factors. This important finding has direct implications for definitions that require limitations to be observed in a specific number of areas. If there is actually one underlying domain that “causes” behaviors in all different conceptual domains, and there is relatively little unique variance found in each domain, then a total score with a single cutoff point could reliably distinguish those with and without significant limitations. If not, diagnosticians would have to consider a profile of adaptive behavior deficits that takes all domain scores into account. Widaman et al. (1991) and Widaman and
McGrew (1996) concluded that evidence supported a hierarchical model with four distinct domains: (1) motor or physical competence; (2) independent living skills, daily living skills, or practical intelligence; (3) cognitive competence, communication, or conceptual intelligence; and (4) social competence or social intelligence. Widaman and McGrew (1996) further argued that agreement on a common set of terms for domains of adaptive behavior (in contrast to the use of “or” as above) would contribute to a better consensus on the structure of adaptive behavior.
The review by Thompson et al. (1999) is the most recent summary of studies using factor analysis; it concludes that adaptive behavior is a multidimensional construct. The three most common dimensions found were in these broad categories: (1) personal independence, (2) responsibility, i.e., meeting expectations of others or getting along with others in social contexts, and (3) cognitive/academic. Physical/developmental and vocational/community dimensions were found less often. Thompson et al. concluded: “No single adaptive-maladaptive behavior assessment instrument completely measures the entire range of adaptive and maladaptive behavior dimensions. . . It is clear that different scales place different levels of emphasis on different adaptive behavior domains. No one instrument produced a factor structure that included all of the domains” that were identified by the American Association on Mental Retardation (1992).
Breadth of Domains. The domains assessed by adaptive behavior scales, and thus the individual items included on them, depend in part on the context, target age group, and purpose of the measure. Thus, considerable variation has been found in the content covered by different scales (Holman & Bruininks, 1985; Thompson et al., 1999). Measures used in schools may not need a work domain, for example, if students are too young for employment or the school does not have a work experience program. Conversely, adult scales would not need items on school-related behaviors (Kamphaus, 1987a). In their review, Thompson et al. (1999) suggest that this incongruity reflects the problem noted by Clausen (1972) and Zigler et al. (1984), that adaptive behavior lacks
a unifying theoretical foundation. A consequence of this, according to Thompson et al., is the inability to develop precise measures of adaptive behavior that would objectively differentiate individuals by disability. An alternative explanation is that adaptive behavior must be understood in the context of the individual’s relevant daily and social life, which is determined by age, culture, and context (Thompson et al., 1999).
Independence of Domains. The 1992 AAMR definition requires that an individual show significant limitations in at least 2 of the 10 adaptive skill areas. A danger of accepting “erroneous domains that are not truly distinct from one another” (Thompson et al., 1999, p. 17) is that it can lead to the inconsistent application of eligibility criteria and unequal treatment across groups of people. Thus, characteristics of the factor structure of a measure of adaptive behavior have important implications for diagnosis.
Thompson et al. (1999) reviewed studies that reported factor analyses of adaptive behavior measures. They made two important points before summarizing their findings: (1) highly correlated factors may indicate that they do not represent independent dimensions and (2) different methods of factor analysis can support different factor structures.
Domains Missing from Adaptive Behavior Scales
Greenspan (1999) noted that a drawback to the factor analytic approach to determining the dimensional structure of adaptive behavior is that this statistical method cannot determine whether some domains do not make conceptual sense (i.e., items should not have been included on tests in the first place) or whether missing content domains should have been included.
Social Skills Dimension of Social Competence. Most adaptive behavior scales contain factors addressing interpersonal relationships or social skills, but they do not address overall social competence. For indi-
viduals whose diagnosis is most in question because their measured IQs are near the cutoff, this vital area may determine the presence or absence of mental retardation. Gresham and Elliott (1987) and Greenspan (1999) have argued that social competence has received too little attention in the conceptualization and measurement of adaptive behavior (Figure 4-1). Their model divides social competence into two overall dimensions: (1) adaptive behavior, which includes the factors contained on most adaptive behavior scales (independent functioning, self-direction, personal responsibility, vocational activity, functional academic skills, physical development) and (2) social skills, including domains that are likely to be most key to identifying mental retardation at the borderline levels (interpersonal behaviors, self-related behaviors, academic-related skills, assertion, peer acceptance, communication skills). The dimensions of adaptive behavior and social skills in the Gresham and Elliott model are surprisingly similar to the 10 adaptive skill areas in the 1992 AAMR definition of mental retardation.
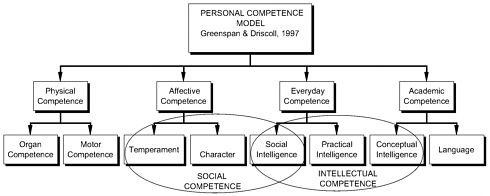
Gullibility/Credulity Component of Social Competence. Greenspan and colleagues (Greenspan, 1999; Greenspan & Driscoll, 1997; Greenspan & Granfield, 1992) have argued that social intelligence, some aspects of which are not contained on any current scales of adaptive behavior or social skills (e.g., credulity, gullibility), should be a key determinant of a diagnosis of mental retardation for adults (Figure 4-2). Greenspan and Driscoll (1997) proposed a “dual nature of competence.” They suggest that intelligence, as measured by IQ, is typically viewed as an independent variable that predicts outcomes, whereas personal competence is the combination of what individuals “bring to various goals and challenges as well as their relative degree of success in meeting those goals and challenges” (p. 130).
Greenspan (1999) argues that the victimization of people with mental retardation, observed in social and economic exploitation, is “a more central (and generally more subtle) problem that goes to the heart of why people with mental retardation are considered to need the protections (ranging from in-home services to conservators) associated
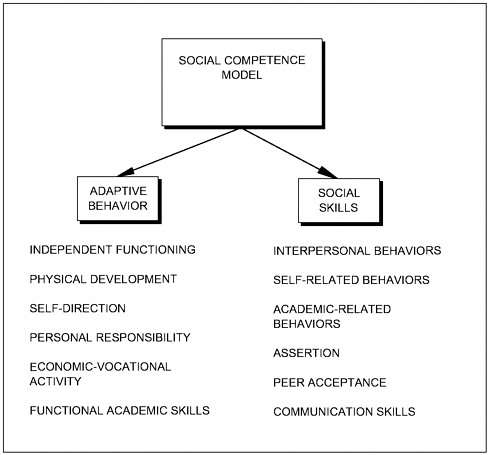
FIGURE 4-1 Social competence model. SOURCE: Gresham & Elliott (1987). Copyright 1987 by PRO-ED, Inc. Reprinted with permission.
with the label” (p. 69). Very recently Greenspan (1999) proposed ideas for assessing vulnerability in a comprehensive assessment of adaptive behavior or social competence. As there is no research yet on credulity in people with mental retardation, these proposals for assessment are unlikely to be found in practice in the next several years. Nevertheless, there is merit to the idea of considering these subtle indicators of social competence, i.e., vulnerability, gullibility, and credulity, as important indicators of adaptive behavior in people with mild cognitive impairments.
Maladaptive Behavior
Many adaptive behavior scales contain assessments of problem or maladaptive behavior, but relationships between domains of adaptive and maladaptive behavior are generally low, with correlations tending to be below .25 (and a tendency to be higher in samples of persons with severe or profound retardation—Harrison, 1987). Division 33 makes it clear that the presence of clinically significant maladaptive behavior does not meet the criterion of significant limitations in adaptive functioning (Jacobson & Mulick, 1996). Hill (1999) also emphasized that behaviors that interfere with a person’s daily activities, or with the activities of those around him or her, should be considered maladaptive behavior, not the lack of adaptive behavior. Refusal to perform a task that a person is capable of doing is also a reflection of problem behavior and should not be considered in relation to adaptive behavior. The classroom form of the Vineland Adaptive Behavior Scales (Sparrow & Cicchetti, 1985) does not include a section on maladaptive behavior, which also suggests that these authors viewed measures of problem behavior as irrelevant to diagnosis or eligibility. Greenspan (1999) also has argued for many years that the presence of maladaptive behavior, or mental illness, is irrelevant for the purpose of diagnosing of mental retardation.
If it is assumed that maladaptive behavior ratings should not contribute to diagnostic decisions about adaptive functioning, then problems in their measurement need not affect this process. However, because several adaptive behavior scales contain maladaptive components, it is worth noting important challenges to reliable measurement. Specifically, several roadblocks to meaningful ratings of maladaptive behavior were noted after publication of the original AAMD Adaptive Behavior Scales (ABS). Scales developed subsequently improved on the simple rating format found in the ABS, which contained a finite list of problem behaviors rated according to the frequency of occurrence. These improvements notwithstanding, the complexity of balancing frequency and severity of problem behavior occurrence will continue to pose problems of score interpretation.
ASSESSMENT OF ADAPTIVE BEHAVIOR
Assessment Dimensions
The assessment of adaptive behavior is complex. One must consider not only general competencies across relevant domains but also the level, quality, and fluency of those behaviors. In addition, there is the issue of the ability to perform behaviors (i.e., can do) versus the actual performance of those skills (i.e., does do). In order for the assessment to be clinically and scientifically meaningful, it is important that the assessor be sufficiently trained in using and interpreting appropriate instruments. A high level of training is necessary in order to capture and distinguish the level, quality, and pattern of adaptive behavior displayed by a given subject, as viewed by the eyes of the respondent (parent, teacher, or caregiver).
The frequency of performance can be classified along a dimension from “never” to “usually or always.” The number of choice points varies by specific instrument or by the variation in the clinical interpretation of the assessor when a formal assessment instrument is not used. The quality of performance may be somewhat more subjective, but a key feature is the appropriateness of a given level of adaptive behavior performance. For example, one needs to distinguish between an individual’s deficit in a specific adaptive behavior skill, as opposed to a deficit in a larger domain.
Assessment Methods
There are a number of ways to assess the level, quality, and pattern of adaptive functioning, each with its own strengths and weaknesses. These include clinical assessment by interview methods (unstructured, structured, semistructured, direct observation), usually with the aid of clinical instruments that are completed by the evaluator during the interview, and the use of checklists that are completed either by an observer or by the individual being assessed.
In an unstructured interview, the clinician applies personal, experience-based clinical norms to the adaptive behavior assessment. The advantage of the method is that it frees the clinician from using a set of criteria that may be perceived as restrictive. The disadvantage is that each clinician imposes his or her own subjective criteria, a process that threatens both the reliability and the validity of the assessment.
Both structured and semistructured interviews, when performed by well-trained and experienced clinicians, appear to be the best available safeguard against threats to the reliability and the validity of adaptive behavior assessment. These procedures, however, need to be employed using an instrument that is reliable, has valid criteria for evaluating adaptive behavior, and uses empirically based norms. In fact, semistructured interviews require the highest level of professional expertise, as the questioning and interpretation of answers requires a high level of training.
Since the adaptive behaviors that need to be assessed are those found in the context of a broad range of everyday living situations displayed across a wide variety of settings, an assessment of adaptive functioning by direct observation is usually not practical. It would be difficult to set up situations in which individuals can demonstrate their ability to perform a wide variety of social, communicative, and daily living behaviors.
Checklists completed by teachers, parents, or other caregivers are often used to rate individuals’ behavior for a broad variety of suspected conditions (e.g., mental retardation, autism, other pervasive developmental disorders, attention deficit disorder). However, the simplicity and lack of reliability or validity of many such procedures render them less useful than more complex measures administered professionally. Checklists may add valuable information and insights, but they are seldom solely sufficient for diagnostic purposes. In order to make reliable and valid judgments about the presence or absence of many behaviors, the items may need such extensive clarification as to obscure the meaning of such behaviors for many respondents.
The issues of cross-cultural, racial, ethnic, and subcultural biases
are of concern to some who view many aspects of adaptive functioning as culturally determined (Boyle et al., 1996; Valdivia, 1999—for a general discussion see the section “Sociocultural Biases”). The issue of sociocultural bias also arises in the context of the adaptive behavior interview. Administration of adaptive behavior scales generally follows one of two possible formats. One is an interview with a professionally trained interviewer and a respondent who knows the individual being assessed well. The other consists of a person who also knows the individual being assessed well but who independently completes a checklist of specific items without assistance. Other scales permit someone to help the person answer questions that cannot be answered without assistance. Some scales can be administered either way. When trained professionals use an interview format, the phrasing of items contained in the record booklet is not used. In this format, the professional has the opportunity to ask questions that are at the appropriate level of sophistication and also appropriate to the cultural group of the respondent.
Adaptive behavior is generally not a mental health issue, since the focus is on developing positive behaviors, rather than deficits. Thus, some of the concerns about cultures that are less accepting of mental illness labels than the majority culture are much less relevant to adaptive behavior assessment.
There seems to be little evidence that adaptive behavior assessment is as prone to cultural, racial, and ethnic bias as other areas of psychological testing. For example, adaptive behavior tests are not as culturally or ethnically bound as tests of intelligence (Hart, 2000; Hart & Risley, 1992; Sparrow et al., 1984a; Walker et al., 1994). However, a recent surgeon general’s report (U.S. Department of Health and Human Services, 2001) focuses on the miscommunication that may exist when the interviewer and the respondent speak different languages. The report notes that “several studies have found that bilingual patients are evaluated differently when interviewed in English as opposed to Spanish.” It is also possible that different subcultural expectations about independence or religious or medical causes for certain behav-
iors may affect the validity of reports. In such instances, if a same-language or same-culture interviewer is not available, the clinician needs to be very aware of such possible miscommunications in order to obtain a valid interview. The surgeon general’s report emphasizes that more research is needed to better understand how, when, and if culture affects interview-based assessments.
Psychometric Concerns in Using Adaptive Behavior Scales
The primary use of adaptive behavior scales in the classification of mental retardation has frequently been confirmatory (i.e., to confirm that a low IQ is associated with delayed acquisition or manifestation of everyday personal and social competencies). This use may result from concerns among clinicians about the robustness of adaptive behavior measures. For the most part, such concerns result from considerations of the structure of measures (e.g., as related to items and other factors mentioned in this section), procedures for obtaining information used to complete the protocols, and issues surrounding informant bias.
Such concerns arise in part because intellectual performance, the other criterion associated with mental retardation, is measured by comprehensive intelligence tests that are the most thoroughly researched forms of psychological assessment (Neisser et al., 1996). Research studies in the past decade that employ adaptive behavior measures have used them as outcome measures or to study the structure or dimensions of adaptive behavior, rather than behavioral development. Clinicians may consequently believe adaptive behavior to be less well understood than intelligence. Nonetheless, there is a rich literature documenting differential outcomes for quality of life, autonomy, and clinical decision making for adaptive behavioral development as measured by existing assessment instruments (Jacobson & Mulick, 1996). Newer adaptive behavior scales evidence more robust psychometric properties than older scales. In this section, we discuss a variety of psychometric features of adaptive behavior scales that have implications for decision making about mental retardation.
Floor and Ceiling Effects
The initial, and probably primary, application of adaptive behavior scales in clinical practice has been to assess the behavioral development of children thought to have mental retardation. Thus, most norming samples, item development, and scale selection have been targeted at groups ages 3 to 18 or 21. This facilitates the early identification of preschool children at risk of mental retardation and permits confirmation of persisting developmental delays. Adult norming samples are often included as well, but they tend to consist of people with already identified disabilities. Thus, adaptive behavior scales have particular relevance in application with preschoolers and with teens, who are often participants in Supplemental Security Income (SSI) determinations or redeterminations. However, depending on the age range of adult participants without disabilities sampled during norming studies, the ceiling (i.e., the highest level of behavioral performance assessed) may differ across scales and may affect the characterization of the degree of delay manifested. Measures of behavioral functioning or responsiveness of children younger than 36 months have not been strengths of many adaptive behavior measures. Infants and toddlers may more appropriately be assessed with more specialized measures in most cases.
Developmental Range Effects
Floor and ceiling effects are also evident as developmental range effects. Scales typically include items that permit behavioral assessments for young children and adolescents without disabilities (i.e., superior behavioral development or skill). For older adolescents, ages 18 to 21, the difficulty level of items often permits identification of either delayed or typical skills. Thus, to the extent that a young adult with mild mental retardation has selected skills that are well developed relative to others, it may not be accurate to describe those skills in developmental terms. Instead, it may be possible to establish only that their skills are superior to those achieved by other young adults with
mild mental retardation, and they may sometimes fall in the normal range of performance of similar age peers. Some data suggest that ceiling and developmental range effects hinder the full description of skill assets for some individuals with mild mental retardation. In unpublished data on some 27,000 people with mild mental retardation, between 75 and 100 percent of participants obtained perfect scores (100 percent) on three of five indices of one scale (J.W. Jacobson & C.S. Brown, personal correspondence, June 17, 2001).
Item Sampling in Relation to Age-Typical Behavior and Settings
Because adaptive behavior scales are designed with applicability for a wide age range but with primary emphasis on childhood and adolescence, some items may not be suitably worded or may not reflect a performance that is age-relevant. For example, an item may tap skills associated only with childhood (e.g., performing a specific activity or completing a task with adult assistance in an age-typical manner) or with adulthood (e.g., menstrual care for an adult or adolescent woman). Some scales contain provisions for alternative items or alternative performance of items. However, depending on the nature of these provisions, they may reduce the comparability of measures of the related skills from different adaptive behavior scales.
In other instances, scales may be constructed such that they are relevant to only certain age groups (e.g., the motor scale in the Vineland ABS), or different versions of the same scale may be used in different settings (e.g., school versus residential and community settings). For example, the Adaptive Behavior Assessment System (Harrison & Oakland, 2000a) is available in four forms: parent, teacher, adult self-report, and adult reported by others. The two versions of the AAMR ABS differ with respect to the age groups emphasized and the settings about which items are structured and weighted in item selection. For example, in relation to the AAMR school-age scales, “items were selected in part based on discrimination among institutionalized individuals and community dwelling individuals previously classified at
different adaptive behavior levels, and among adaptive behavior levels in public school populations” (Lambert et al., 1993b).
Item Density
Adaptive behavior scales are structured to be comprehensive without being cumbersome (Adams, 2000). Consequently, several features must be balanced. A number of factors and descriptive categories of behavioral development must be represented adequately in order to ensure comprehensiveness and documentation of both strengths and limitations for clinical and diagnostic purposes. The number of items associated with each descriptive category must be sufficient to provide a scale and to be applicable across age ranges. A relatively wide age range must be represented. In balancing these factors, item density, that is, the inclusion of multiple items reflecting age-typical performance at a range of ages, must be maintained at a fairly uniform level. This means that within any one subscale of an adaptive behavior scale, for example, there may be only one or two items typical of performance for a 10-year-old. When subscale scores are aggregated into summary scores, this results in a meaningful number of age-relevant items, although the items sampled in each subscale are limited. For this reason, some manuals recommend that clinicians fully explore the nature of tasks that the focal person performs that may be age typical (e.g., Sparrow et al., 1984a). Nonetheless, it should always be recognized that items in adaptive behavior measures represent a sampling of items that have passed reliability and validity screens, rather than a complete characterization of adaptive behavior.
Reliability of Informant Judgments
Because adaptive behavior scales are typically completed through interview of informants or direct responses (marking of a protocol by the informant), the reliability and the validity of informant responses have been particular concerns. These concerns are heightened when
informants have a stake in the outcome of the assessment (e.g., when responses may affect eligibility for services). Developers have addressed this issue through several strategies: (1) assessing the interrater and test-retest reliabilities of measures, (2) providing instructions to raters for coding items (e.g., Sparrow et al., 1984a), and (3) specifying training for clinicians and preparation of raters (e.g., Bruininks et al., 1996). Reliabilities are initially assessed at the item level and then at the scale and factor levels. Current measures evidence acceptable interrater and test-retest reliability, with consistency scores at levels of .90 and above (seldom at a level below .80) for clinical and normative subgroups, partitioned by age and clinical variables. Similarly, adequate internal consistency of subscales or domains is documented using split-half or alpha coefficients. Full details on standardization and reliabilities are provided in the manuals associated with the major adaptive behavior scales (Adams, 2000; Bruininks et al., 1996; Harrison & Oakland, 2000b; Lambert et al., 1993b; Sparrow et al., 1984b; see also Harrington, 1985). Additional discussion is provided in Chapter 3.
Validity of Informant Judgments
Validity can be categorized in terms of: (1) content validity (evidence of content relevance, representativeness, and technical quality); (2) substantive validity (theoretical rationale); (3) structural validity (the fidelity of the scoring structure); (4) generalization validity (generalization to the population and across populations); (5) external validity (applications to multitrait-multimethod comparison); and (6) consequential validity (bias, fairness, and justice; the social consequence of the assessment to the society—Messick, 1995). Technical manuals present analyses of data gathered in the process of test development that addresses content validity (in terms of representativeness and inferences from age norms), substantive validity (in that they present either a theoretical or empirically derived model of adaptive behavior to which the scale conforms), generalization validity (with respect to differing age or disability groups), external validity (in terms of concurrence with previous or contemporary adaptive behavior measures
and intellectual measures), and consequential validity (in terms of evidence of bias or procedures utilized to reduce bias). As previously noted, primary concerns in the use of adaptive behavior scales in eligibility determination decisions center on informant bias.
Manuals for the major adaptive behavior scales encourage the use of multiple informants, for example, teachers and parents. This allows the rater to obtain a complete picture of the adaptive functioning of the person being assessed. It also allows for reconciliation of ratings among these informants. Both legislative action and judicial decisions at the federal level have focused on concerns that parents may misinform clinicians regarding their children’s skills in order to obtain SSI benefits. Federal review of the SSI program has indicated that such deception is an uncommon occurrence.
Adequacy of Normative Samples
Another psychometric concern is whether the norming samples are adequate. Although normed on smaller samples than comprehensive intelligence tests use, current adaptive behavior measures typically have adequate norming samples in relation to both representation of people with and without mental retardation and representation of age groups in the population in relation to the age span of the measure.
-
For the Adaptive Behavior Assessment System (Harrison & Oakland, 2000a), the norming groups for 5- to 21-year-olds included 1,670 (parent form) to 1,690 (teacher form) children; for 16- to 89-year-olds, the norming groups included 920 (rated by others) to 990 (self-report) adults without disabilities throughout the United States.
-
For the Scales of Independent Behavior-R (Bruininks et al., 1996), the norming sample included 2,182 people ages 3 years 11 months to 90 years, with a sampling frame based on the general population of the United States stratified for gender, race, Hispanic origin, occupational status, occupational level, geographic region, and community size.
-
For the AAMR Adaptive Behavior Scale-School scales (Lam-
-
bert et al., 1993a) the norming group included 2,074 students (ages 3-21) with mental retardation living in 40 states, and a sample of 1,254 students (ages 3-18) without mental retardation from 44 states.
-
For the Vineland Adaptive Behavior Scales (Sparrow et al., 1984a) the standardization sample was representative of the U.S. population. It consisted of 3,000 children ages birth through 18 years 11 months of age, including 99 children in special or gifted education among the 2,500 who were of school age.
-
For the Comprehensive Test of Adaptive Behavior-R (Adams, 2000), the norming sample represented four of five U.S. regions (excluding the West) and included a nonschool sample of 4,456 people with mental retardation ages 10 to 60+ years and a school sample of 2,094 children and adolescents with mental retardation ages 5 to 22, and a sample of 4,525 children and adolescents without mental retardation ages 5 to 22.
Sociocultural Biases
Bias refers to a consistent distortion of scores that is attributed to demographic factors, principally nonmodifiable personal characteristics such as age, gender, race, and ethnic or cultural membership. In the United States there have been significant concerns about the relationship between ethnicity or racial origin and performance on intelligence tests (Neisser et al., 1996). This has generalized to adaptive behavior measures. As the importance of adaptive behavior measures in classification of mental retardation has increased, this concern has been heightened as disproportionate numbers of minority children have been identified as having mental retardation, primarily because of low-income status and the overrepresentation of individuals with mental retardation among low-income people (Boyle et al., 1996).
Some (e.g.,Valdivia, 1999) have suggested that age norms are arbitrary and reflect white, middle-class childrearing standards, and that developmental attainments are affected by culturally different skills and expectations. The result is an overidentification of skill limita-
tions among minority children. However, research that indicates a causal relationship between the childrearing practices of minority families in North America and developmental delay is very limited. Comparative research examining the relationship between minority status and pronounced delays that are not accounted for by socioeconomic factors is also limited. However, available data are sufficient to raise concerns that such issues should be studied further (Bryant et al., 1999; Craig & Tasse, 1999).
To some extent, inclusion of participants representative of the general population, including racial and ethnic minorities, in norming samples should mitigate against biases in scoring of adaptive behavior scales. To the extent that low income or very low income is more common among certain ethnic minority groups, however, differences in developmental trajectories for children may reflect differences in childrearing practices and stimulation that are associated with economic and social class and related levels of parental education (Hart, 2000; Hart & Risley, 1992; Walker et al., 1994).
Although research from the 1970s and 1980s found comparable performance on adaptive behavior scales among majority and minority ethnic groups (Bryant et al., 1999; Craig & Tasse, 1999), linguistic factors remain a concern. These include such considerations as interviewing informants in their primary language and dialect, and the comparability of translations of items in adaptive behavior scales to particular languages and dialects, including dialects in English (e.g., American and British). Translation is a concern because the comparability of translations of items has seldom been confirmed through back-translation from the translated content to the initial language, or through confirmatory analysis through further retranslation (Craig & Tasse, 1999). Noncomparability of items may alter norms due to item wording that requires a higher developmental level of performance in the translated item. Also, English language norms may be lower than the typical performance of a same-age child in another culture. Cross-cultural and cultural subgroup studies of adaptive behavior differences among ethnic, racial, or national groups are certainly needed, but evi-
dence for substantial relationships between racial or ethnic group membership and performance on adaptive behavior scales, unmediated by socioeconomic differences, is very limited.
Nonetheless, culturally competent assessment practices require consideration of the developmental impacts of cultural practices or language differences among examiners, examinees, and informants that may affect the validity of the clinical information collected and interpreted. Under ideal circumstances, adaptive behavior measures should be administered in an examinee’s or informant’s primary language. Often, there may be no substitute for assistance by a translator familiar with the informant’s dialect, even for examiners who are fluent in the informant’s primary language. In instances in which the informant is bilingual, it may be appropriate to probe interview responses in both languages.
Adaptive Behavior Scales with Well-Known Properties
There are at least 200 published adaptive behavior instruments that have been used for diagnosis, research, program evaluation, administration, and individualized programming. Some of these scales were developed to serve only one of these purposes; however, several have attempted to include both the breadth required for diagnosis and the depth required for clinical use. Most tests fall short of accomplishing both purposes. Referring to the dual purpose of adaptive behavior scales, Spreat (1999) concluded that it is “unrealistic to think that the same test can be used for program evaluation, diagnosis, classification, and individual programming” (p. 106). Among the very large number of adaptive behavior scales on the market, very few have adequate norms and reliability to diagnose mental retardation in people with IQs in the questionable range (e.g., 60-80). Kamphaus (1987b) reported that the Vineland Adaptive Behavior Scales-Survey Form (Sparrow et al., 1984a) and the Scales of Independent Behavior (Bruininks et al., 1984) had adequate standardization samples. In a national survey of school psychologists, only three scales were found to be in wide use for diagnosis: the Vineland Adaptive Behavior Scales, the Scales of
Independent Behavior, and the AAMR Adaptive Behavior Scale-School Edition (Stinnett et al., 1994). The Adaptive Behavior Assessment System (Harrison & Oakland, 2000a) is quite new and relatively untested, but its psychometric properties and norms extend to age 89.
Each of these scales (except the Adaptive Behavior Assessment System) has been reviewed extensively and compared with others in detailed reports. Readers are referred to the test manuals and to Reschly (1990), Harrison and Robinson (1995), Thompson et al. (1999), Jacobson and Mulick (1996), Spector (1999), Hill (1999), Test Critiques, test reviews in the Journal of Psychoeducational Assessment, and the Mental Measurements Yearbooks for more detailed psychometric information about these and other measures. Although each scale described has both strengths and weaknesses, each has impressive psychometric characteristics and is highly recommended for use in eligibility determination and diagnosis. Decisions about which instrument to use depend on the age of the individual to be tested and available norms, available sources of information, the context in which the individual is known, and the training of the rater.
Vineland Adaptive Behavior Scales
The Vineland Adaptive Behavior Scales (VABS—Sparrow et al., 1984a) have their conceptual roots in the Vineland Social Maturity Scale (Doll, 1936b), although overlap between the original and the new scales is minimal (Kamphaus, 1987b). There are actually three scales, including a survey form (VABS-S) and an expanded form (VABS-E), which uses a conversation data gathering format during interviews with parents or guardians. A psychologist, social worker, or other professional who has appropriate training in interview techniques must complete these forms. Norms on children having no disability are available from birth to 18 years, 11 months, based on a standardization sample of 3,000 cases that were stratified by age, gender, ethnicity, parental education, geographic region, and community size consistent with U.S. census data. The proportion of children from homes with low socioeconomic status was lower than that in the cen-
sus data. The expanded version is designed to meet the requirements of diagnosis and of planning/intervention, and is intentionally longer and more detailed in order to ascertain information on specific skill deficiencies. Data from reliability and validity studies of the survey form are very impressive, especially in light of the flexible conversational procedures used for obtaining information.
The third scale is a classroom form (VABS-C), appropriate for children ages 3-12, and can be completed by the teacher fairly quickly. It does not require specific or graduate training to complete. However, teachers have limited opportunities to observe all behaviors on the VABS-C and must necessarily provide estimates of behaviors that do not occur in the school context. A strength of this scale is that teachers are asked to record when they estimate behaviors, so the resulting threat to reliability and validity can be appraised.
AAMR Adaptive Behavior Scales
There are two versions of the Adaptive Behavior Scales (ABS)–a school version (ABS-S:2—Lambert et al., 1993a) and a residential and community version (ABS-Residential and Community, ABS-RC:2— Nihira et al., 1993). The ABS-S:2 is used to identify students who are significantly below their peers in adaptive functioning for diagnostic purposes. It also determines strengths and weaknesses, documents progress, and assesses the effects of intervention programs. Although it is linked to AAMR by name, the ABS does not provide subscale scores in the 10 adaptive skill areas listed in the 1992 AAMR definition of mental retardation. Stinnett (1997) matched ABS items to the 10 adaptive skill areas in the AAMR definition and found that some skill areas are addressed in depth by the ABS (social skills and self-care domains), while others have too few items to give reliable estimates (home living, health and safety, leisure). Nine behavior domains measure personal independence and personal responsibility in daily living, including prevocational/vocational activity. A second part of the ABS-S relates to social and maladaptive behavior.
The ABS-S was standardized on population samples of people
with and without mental retardation. Standard scores, age-equivalent scores, and percentile rank scores can be converted from raw scores on the adaptive behavior subscales and three factor scores for ages 3-21. The standardization samples have been judged to be excellent, although the fact that the sample of people with mental retardation did not include people in the IQ range 71-75 is likely to overestimate adaptive behavior when using the mental retardation norms (Stinnett, 1997). Since other norms should be used for determining a diagnosis of mental retardation, according to the manual, this should not be a problem in the current SSA context. The ABS-S:2 has excellent interrater reliability.
The ABS-S:2 provides norms only through age 21 and includes some content specifically appropriate for school settings rather than adult environments. The residential and community version, ABS-RC:2, was developed to be appropriate for use with persons through 79 years of age. ABS-RC:2 norms are not available for adults with typical functioning, and most norm-referenced scores provide comparisons only with adults with developmental disabilities. The standardization sample consisted mostly (80 percent) of adults living in residential facilities, and the overall functioning level of the sample may be lower than if other community-dwelling adults had been included (Harrison, 1998). Because standard scores and percentile ranks do not indicate standing relative to people without developmental disabilities, and because the norming sample is probably not representative of the population of adults with developmental disabilities, the ABS-RC:2 may not fit the psychometric criteria used in determining a diagnosis of mental retardation according to AAMR requirements (American Association on Mental Retardation, 1992).
Scales of Independent Behavior
The Scales of Independent Behavior (SIB-R—Bruininks et al., 1984) is a component of the Woodcock-Johnson Psycho-Educational Battery. The SIB provides norms from infancy to adulthood (40+ years), contains 14 adaptive behavior subscales that fall into four ma-
jor clusters, and provides an additional full-scale broad independence score.
The SIB-R manual addresses many of the issues that make the scoring interpretation of adaptive behavior scores challenging, including physical disability, the use of adaptive equipment, alternative communication methods, tasks no longer age appropriate, partial performance of multipart tasks, lack of opportunity due to environment or safety, and cognitive ability to understand social expectations for performing behaviors. In general, individuals are to be rated according to what they actually do (or would do if age appropriate), rather than giving “credit” for these considerations or denying credit if tasks are performed well with the assistance of adaptive equipment, medication, or special technology (Hill, 1999). However, if functional independence is to be considered “within the context of the environments and social expectations that affect his or her functioning” (Hill, 1999), interpreting scores without considering opportunity and societal expectations for a person with physical limitations could be problematic for a diagnosis of mental retardation.
Adaptive Behavior Assessment System
The Adaptive Behavior Assessment System (ABAS—Harrison & Oakland, 2000a) is the newest of the adaptive behavior measures that has sound psychometric properties. Although it had extensive field testing before publication, formal reviews are not yet available. It was developed to be consistent with the 10 AAMR adaptive skill domains, and, depending on the weight placed on using the AAMR definition for diagnosis by a clinician, this may be a relevant characteristic. Moreover, the ABAS is appropriate for use with children (age 5 and older) as well as adults. It includes two adult forms, including a self-report and a report by others, and norms that extend well into adulthood. It appears to have good potential for assessing adaptive behavior for diagnostic purposes. Average reliability coefficients of the adaptive skill areas across age groups range from .86 to .97, with the majority above .90 and corrected reliability coefficients of individuals with clinical di-
agnoses above .98. Norms for age birth to 5 years are expected to be available in 2002.
Battelle Developmental Inventory
The Batelle Developmental Inventory (BDI—Newborg et al., 1984) is a developmental scale, rather than an adaptive behavior scale, and is appropriate for children from birth to age 8 (Spector, 1999). It does not have the problems with floor effects in diagnosing developmental delays at the youngest ages that are present in other adaptive behavior scales. It contains broad domains similar to those found on adaptive behavior scales, which include: personal-social, adaptive, motor, communication, and cognitive. The BDI has well-documented reliability and validity, with norms based on a nationally representative sample of children (Harrington, 1985; Oehler-Stinnett, 1989). Several studies have shown significant and meaningful correlations between the BDI and other measures of cognitive, adaptive, language, and social functioning, with samples of children with and without disabilities (Bailey et al., 1998). The BDI is susceptible to “age discontinuities” (Boyd, 1989) or “differences in norm table layout” (Bracken, 1988) that are relatively common in measures of young children during this period of typically rapid development. This problem, and recommended strategies to avoid errors in diagnosis, are discussed in the section on norms.
Other Scales
The adaptive behavior scales described above have been consistently identified in research and practice reports as meeting criteria of technical excellence in measurement. Several other tests have been widely used and have many positive features but do not have the same reputation. Because clinicians are encouraged to utilize multiple measures in diagnosis, these other measures may be useful in providing supplemental or complementary information.
The Comprehensive Test of Adaptive Behavior (CTAB—Adams
& Hartleben, 1984) has been described as “fairly efficient and inexpensive,” with “excellent reliability, solid validity, and adequate norms” (Reschly, 1990). It is reported to be appropriate for ages 5-22, yet it may not have a sufficient ceiling to discriminate performance levels among children above age 14 (Evans & Bradley-Johnson, 1988). A second limitation of this scale is that the standardization sample was limited to the state of Florida. Because Florida is a large and populous state with a culturally diverse population, it is likely that results can be generalized to the national population. Scores on the revised version of this measure, the CTAB-R, are based on a standardization sample that includes four of five regions of the United States (Adams, 2000).
The Adaptive Behavior Inventory (ABI—Brown & Leigh, 1986) was designed to “reflect the ability of school-age youngsters to meet age-appropriate socio-cultural expectations for personal responsibility” (Smith, 1989). It is appropriate for use with students ages 5 through 18 and is completed by the teacher. The ABI has a normative sample representative of all school-age children, including those with disabilities, and of a sample with mental retardation. The standardization sample was proportional in demographic characteristics to the 1980 census data. However, Smith (1989) notes that, at the low end of the normal intelligence norms, a few raw score points can dramatically change the adaptive behavior “quotient,” and suggests that the norms on students with mental retardation are more useful. An attempt was made to select items that would avoid ceiling effects for the normal population and to ensure basal measures for the population with mental retardation. There is evidence that the ABI has adequate construct, content, and criterion-related validity, as well as internal reliability, but no data were provided on interrater reliability. Smith (1989) cited many problems with the norm tables but concluded the ABI could contribute some information to the determination of mental retardation.
The Independent Living Scales (ILS—Loeb, 1996) were designed to assess the degree to which older adults are capable of caring for themselves (i.e., functional competence). It requires an individual to
demonstrate adaptive skills, rather than using a third-party informant or self-report to gather information on typical behavior. Reviews of the ILS have been generally negative, and it may not be suitable for disability determination purposes.
The Adaptive Behavior Evaluation Scale (ABES—McCarney, 1983) and the Parent Rating of Student Behavior (PRSB—McCarney, 1988) are used to identify mental retardation, learning disabilities, behavior disorders, vision or hearing impairments, and physical disabilities in students ages 5 to 21. Moran (2001) concluded that the information in the manual was not adequate to show how students with mental retardation differed from students with other disabilities. Norms are available to age 18 for the ABES and to age 12 for the parent scale. Reliability is good. High correlations with intelligence tests suggest it may be a duplication of this construct.
The Adaptive Behavior: Street Survival Skills Questionnaire (SSSQ—Linkenhoker & McCarron, 1983) was designed to assess adaptive behavior in youth from age 9 years and adults with mild to moderate mental retardation. The subscales are similar to general adaptive behavior scales, but there is a greater emphasis on skills required to function in community settings than on basic adaptive skills. It also differs from other adaptive behavior scales because it is administered as a test directly to the individual and, as such, does not measure typical performance in “real life.” Haring (1992) found this to be an advantage in terms of its excellent reliability but noted that there were concerns about validity. Another concern was whether one may obtain a comprehensive picture of overall adaptation to the natural environment, because some skills could not be tested using the SSSQ’s multiple-choice picture format. He suggested that the SSSQ could provide useful data when combined with the results of other comprehensive tests. To the extent that SSSQ data can predict entry or retention of competitive, gainful employment among people with mental retardation, it may have utility.
For the Social Skills and Vocational Success, Chadsey-Rusch (1992) described three measurement approaches to operationalize a
definition of social skills, including (1) the perception of others in the workplace, especially employers, (2) the goals and perceptions of the target individual, and (3) performance of social behaviors in natural contexts. Perceptions of others are typically measured by sociometric ratings and behavior rating scales. The Social Skills Rating System, described below, is a behavior rating scale that was developed to provide this information for students. Sociometric ratings provide useful information but are impractical for diagnostic purposes, and the use of nonstandardized rating forms is not recommended for diagnosis of significant limitations in social skills. Direct measures from target individuals involve presenting them with hypothetical situations and conducting direct observations. It is unclear whether individuals with low-normal intelligence or mild mental retardation would be able to respond reliably to hypothetical situations.
The Social Skills Rating Scales (SSRS—Gresham & Elliott, 1987) is probably the best measure available of social skills adaptation in the school context. Although developed for school-age children, this scale may hold promise for adapted use with adults in work settings. In addition to rating skill performance, raters also specify whether each skill is critical to success in the environment in which the child is observed, i.e., school or classroom.
Table 4-1 shows the principal available adaptive behavior measures that are comprehensive in nature and their characterstics, including age range for use, age range of norm groups, date of publication, available versions, examiner requirements, appropriate scores for use in determining presence of adaptive behavior limitations, and assessed reliability of scores.
ASSESSMENT ISSUES IN ELIGIBILITY DETERMINATION
Relation of Principal Adaptive Behavior Scale Content to SSA Criteria
In Chapter 1 we provided the details of SSA’s criteria for a disability determination of mental retardation in terms of both mental capac-
ity and adaptive functioning. Adaptive behavior measures are useful in the identification of limitations concurrent with an IQ significantly below average. They also have utility in documenting delays or functional limitations consistent with marked impairment in motor development, activities of daily living, communication, social functioning, or personal functioning. These measures also may be validly used, with repeated or periodic administrations, for assessment of changes in status. Generally, however, adaptive behavior measures will be less effective in fine-grained analysis and classification of such problems as specific motor disorders or communication disorders and deficiencies in concentration, persistence, or pace.
SSA guidelines further clarify the intent and nature of activities of daily living and social functioning for adults, and personal functioning for younger and older children, closely paraphrased below:
-
Activities of daily living include adaptive activities such as cleaning, shopping, cooking, taking public transportation, paying bills, maintaining a residence, caring appropriately for one’s grooming and hygiene, using telephones and directories, and using a post office, etc. In the context of the individual’s overall situation, the quality of these activities is judged by their independence, appropriateness, and effectiveness. It is necessary to define the extent to which the individual is capable of initiating and participating in activities independent of supervision or direction.
-
The number of activities that are restricted does not represent a “marked” limitation in activities of daily living, but rather the overall degree of restriction or combination of restrictions must be judged.
-
Social functioning refers to an individual’s capacity to interact appropriately and communicate effectively with others. Social functioning includes the ability to get along with others, e.g., family members, friends, neighbors, grocery clerks, landlords, and bus drivers. A history of altercations, evictions, firings, fear of strangers, avoidance of interpersonal relationships, or social isolation may demonstrate impaired social functioning. Strength in social functioning may be docu-
TABLE 4-1 Principal Comprehensive Adaptive Behavior Measures and Their Characteristics
|
Adaptive Behavior Measurea |
Age Range: Use |
Age Range: Norms |
Year Published |
|
AAMR Adaptive Behavior Scale-Residential and Community |
18-79 years |
18.0 to 60+ years N = 4,103 people with DD |
1993 |
|
AAMR Adaptive Behavior Scale-School |
3-18 or 3-21 years |
3.0-18.11 years N = 2,074 students with MR; N = 1,254 students w/o MR |
1993 |
|
Adaptive Behavior Assessment System |
5-89 years |
5-21 years; N = 1,670 &1,690; general population 16-89 years; N = 920 & 990; general population |
2000 |
|
Versions |
Examiner Requirementsb |
Appropriate Scores |
Principal Reliabilities |
|
Children’s version (see below) |
Completion by a professional; or completion by a paraprofessional, with professional supervision (perhaps Class C, not specified) |
-Personal self-sufficiency -Community self-sufficiency -Personal-social responsibility & 10 domain scores |
Test-retest: (N = 45) -Factors: r = .93 to .98 -Domains: r = .88 to .99 Interrater: (N = 16) -Factors: r = .97 to .99 -Domains: r = .83 to .99 |
|
Adult version (see above) |
Completion by a professional; or completion by a paraprofessional, with professional supervision (perhaps Class C, not specified) |
-Personal self-sufficiency -Community self-sufficiency -Personal-social responsibility & 9 domain scores |
Test-retest: (N = 45) -Factors: r = .72 to .79 -Domains: r = .75 to .95 Interrater: (N = 15) -Factors: r = .98 to .99 -Domains: r = .95 to .99 |
|
-Parent form -Teacher form -Adult form |
Completion by a professional; or completion by a paraprofessional, with professional supervision (perhaps Class C, not specified) |
-Global Adaptive Composite (GAC) -10 Domains: communication; community use; functional academics; home/school living; health & safety; leisure; self-care; self-direction; social; work |
(Parent Form) Test-retest: (N = 102) -GAC: r = .96 -Domains: r = .83 to .94 Interrater: (N = 81) -GAC: r = .84 -Domains: r = .57 to .82 |
|
Adaptive Behavior Measurea |
Age Range: Use |
Age Range: Norms |
Year Published |
|
Comprehensive Test of Adaptive Behavior-Revised |
Birth-60+ years |
5-22 years; N = 2,094; students with MR 10-60+ years; N = 4,456; with MR 5-22 years: N = 4,525; students w/o MR |
2000 |
|
Scales of Independent Behavior-Revised |
3 months-90 years |
3 months-90 years; N = 2,182; general population |
1996 |
|
Vineland Adaptive Behavior Scalesc |
1-99 years |
0.1 to 18.11 years N = 3,000 general population |
1984 |
|
Versions |
Examiner Requirementsb |
Appropriate Scores |
Principal Reliabilities |
|
-Normative Adaptive Behavior Checklist-Revised (NABC-R) is composed of a subset of CTAB-R items -Also a parent/guardian form of the CTAB-R |
Completion of NABC-R by a parent or guardian Completion by a professional; or completion by a paraprofessional, with professional supervision (perhaps Class C, not specified) |
-Total score -7 Domains: self-help; home living; independent living; social skills; sensory-motor; language/academics |
(School sample) Test-retest: (N = 58) -Total: r = .99 -Domains: r = .98 to .99 Interrater: (N = 32) -Total: r = .99 -Domains: r = .95 to .99 |
|
-Short form -Early development form -Other related instruments |
Completion by a professional; or completion by a paraprofessional, with professional supervision (possibly Class C for & interpretation of scores) |
-Broad Independence Score (BIS) -4 Cluster scores: motor skills; social interaction & communication skills; personal living skills; community living skills |
(Children w/o MR) Test-retest: (N = 31) -BIS: r = .98 -Clusters: r = .96-.97 Interrater: (N = 26) -BIS: r = .95 -Clusters: r = .88-.93 |
|
-Interview survey form -Expanded form -Classroom edition |
Class C; or completion by social worker or educator |
-AB composite -Communication -Daily living -Motor -Socialization |
(Interview survey form) Test-retest: (N = 484) -Composite r = .88 -Domains r = .81 to .86 Interrater: (N = 160) -Composite r = .74 -Domains r = .62-.78 |
-
mented by an individual’s ability to initiate social contacts with others, communicate clearly with others, interact, and actively participate in group activities. Cooperative behaviors, consideration for others, awareness of others’ feelings, and social maturity also need to be considered. Social functioning in work situations may involve interactions with the public, responding appropriately to persons in authority, e.g., supervisors, or cooperative behaviors involving coworkers.
-
A “marked” limitation is not represented by the number of areas in which social functioning is impaired, but rather by the overall degree of interference in a particular area or combination of areas of functioning.
-
Personal functioning in preschool children pertains to self-care, i.e., personal needs, health, and safety (feeding, dressing, toileting, bathing; maintaining personal hygiene, proper nutrition, sleep, health habits; adhering to medication or therapy regimens; following safety precautions). Development of self-care skills is measured in terms of the child’s increasing ability to help himself or herself and to cooperate with others in taking care of these needs. Impaired ability in this area is manifested by failure to develop such skills, failure to use them, or self-injurious actions. This function may be documented by a standardized test of adaptive behavior or by a careful description of the full range of self-care activities. These activities are often observed not only at home but also in preschool programs.
-
Personal functioning in adolescents pertains to self-care. It is measured in the same terms as for younger children, the focus, however, being on the adolescent’s ability to take care of his or her own personal needs, health, and safety without assistance. Impaired ability in this area is manifested by failure to take care of these needs or by self-injurious actions. This function may be documented by a standardized test of adaptive behavior or by careful descriptions of the full range of self-care activities.
The overall correspondence of several adaptive behavior measures to the content within the functional areas that are considered in ascertaining marked limitations is shown in Table 4-2. Each of the four adaptive behavior measures included in the table collects or assesses information regarding developmental status or performance in the areas of motor development, activities of daily living, communication, social functioning, and personal functioning. This table is a useful means to summarize and illustrate the detailed description of adaptive functioning that meets listing criteria, which are required to establish eligibility for SSI and DI.
Sensitivity of Scales at Ranges in Which Diagnostic Confirmation Is a Priority
Because adaptive behavior scales are targeted either specifically at children and adolescents or at groups ranging from children to young adults, there is a strong developmental component to their structures (Widaman et al., 1987). Such scales sample behaviors that are typically achieved at a range of ages and can indicate strengths and weaknesses in the ability to adapt. However, this also means that most scales are structured in steps that permit sampling of typical developmental tasks at each age. For any given age, it is unlikely that developmental tasks will be oversampled. In fact, as noted above, in the construction of adaptive behavior scales, such oversampling is typically avoided. Therefore, these instruments generally do not have firm cut-
TABLE 4-2 Correspondence Between SSI Classification Domains and Domains or Subdomains in Prominent Adaptive Behavior Measures
|
SSI Classification Domain |
AAMR–ABSa |
ABAS |
SIB-R |
VABS |
|
Motor development |
-Physical development |
-Health & safety |
-Motor skills (gross & fine) |
-Motor skills (gross & fine) |
|
Activities of daily living |
-Independent functioning -Domestic activity |
-Self-care -Home living |
-Eating & meal preparation -Toileting -Dressing -Personal self-care -Domestic skills |
-Personal daily living skills -Domestic daily living skills |
|
Communication |
-Language development -Numbers & time |
-Communication -Functional academics |
-Language comprehension -Language expression |
-Receptive communication -Expressive communication -Written communication |
off points at each age at which adaptive behavior is considered to be substantially or markedly impaired. The determination of whether adaptive deficits are marked in character requires clinical interpretation informed in part by the data provided by the scoring of adaptive behavior measures.
The committee discussed the use of specific numeric cutoff points at which a marked deficit is present. There are few data on which to base such a decision. In fact, only one adaptive behavior test manual provides data that would be useful for answering this question. As a result, the committee commissioned Monte Carlo simulations to understand better the implications of requiring a specific numeric cutoff point. These data are presented in Chapter 5.
Here we review data from the only adaptive behavior test manual that could provide some guidance about the use of cutoff points for adaptive behavior assessment. Some caution is needed in interpreting these findings, because the study is small and unrepresentative. It may, however, be useful for identifying some of the issues likely to arise in setting a specific numeric cutoff point.
Using IQ as a parallel, it might seem that a reasonable cutoff score on an adaptive behavior scale could be a composite score or several scale scores of two standard deviations below the mean (i.e., –2 SD). However, depending on the functional domain and the measure, many people with a diagnosis of mild mental retardation do not have adaptive delays or limitations to this degree. Table 4-3, adapted from Harrison and Oakland (2000b), shows the percentage of adaptive behavior domain scores for a sample of children with mild mental retardation (N = 66) and controls without mental retardation matched for gender, age, and socioeconomic status (N = 66) that scored below the –2 SD standard on the teacher form of the ABAS. Because the sample for mild mental retardation shown in Table 4-3 was drawn from a school-age sample, some members of the group may have had IQs above 70 (i.e., less than 2 SDs below the mean). It should also be noted, however, that there is no gold standard against which cutoff scores could be appraised, or research from which a “true” proportion of people with observed IQs in the range of approximately 65-75 who
TABLE 4-3 Percentage of People Ages 5-18 Lower Than Two Standard Deviations Below the Mean on the Domains of the Adaptive Behavior Assessment System
manifest adaptive limitations consistent with mental retardation may be directly projected. But it does seem reasonable, based on clinical experience, that any cutoff scores used should classify a majority of people in this IQ range as having adaptive limitations consistent with mental retardation.
Several important conclusions are suggested by this comparison, although the specifics might differ if another adaptive behavior scale with a somewhat different structure were used:
-
One-half of children with mild mental retardation (column 2) had a summary score falling in the marked limitation range (≤ 2 SDs), compared with about 14 percent of children without mental retarda-
-
tion (column 3). One-half of children (and adolescents) with diagnosed mental retardation did not have summary scores falling in this range.
-
About three-quarters of children with mild mental retardation had two or more domain scores falling in the marked limitation range, compared with slightly less than one-third of the children without mental retardation (last row).
-
There is considerable overlap in adaptive behavior attainment among children with mild mental retardation and matched peers. Even in those domains in which the greatest differences in attainment are evident, between 24 and 48 percent of children with mild mental retardation do not have adaptive limitations meeting a standard of marked limitation in those domains (although many may have such limitations in other domains).
-
Children with mild mental retardation were most likely to have adaptive behavior skills consistent with marked limitation (e.g., ≤ –2 SDs) in the domains of functional academics, communication, and community use.
-
Children without mild mental retardation were most likely to have adaptive behavior skills consistent with marked limitation in the domains of communication, health and safety, and self-direction.
-
Based on the ratio of marked deficits in the two groups (column 4), children with mild mental retardation were much more likely to have deficits in functional academics (especially), self-care, and community use and more likely to have deficits in social, self-direction, school living, and communication than children without mental retardation.
These findings are also evident in analyses of other adaptive behavior scale data (Jacobson, 1997) and client registry or population data sets (Jacobson, 1992; Larson et al., 2000; Lubin et al., 1982). Moreover, the findings suggest that eligibility criteria for SSI and DI applicants with IQs in the range of –2 to –2.66 SDs, by including the presence of marked limitations in activities of daily living, communication, social functioning, and personal functioning, will exclude a sub-
stantial number of people with IQs in this range. These score patterns also suggest that if a criterion of –1.0 to –1.5 SD was adopted as a cutoff point for each of several limitations in different domains, a much smaller percentage of people would be excluded from eligibility. Indeed, this latter approach is consistent with guidance already noted from the Social Security Administration.
General Clinical Practice and the Selection and Use of Adaptive Behavior Scales
In a 1990 survey, Archer et al. (1991) found that two adaptive behavior scales ranked 20th and 21st among 29 specific psychological assessment measures used by psychologists serving adolescents, and they were used “frequently” by fewer than 10 percent of practitioners. Adaptive behavior scales were seldom used as components of assessment batteries. A more recent study by Watkins et al. (1995) found that only 13 percent of respondents in the sample of clinical psychologists engaged in ability testing as part of their clinical practice, but 66 percent engaged in intellectual assessment. Adaptive behavior scales were not among the types of measures (or named measures) that respondents identified as important for the training of future practitioners. One particular adaptive behavior scale was ranked 17th in use among 38 scales, but less than 15 percent of respondents reported using this scale frequently. In their review of child assessment practices of psychologists, Kamphaus et al. (2000) mention the utility of adaptive behavior measures as components of multidimensional models of functioning and child psychopathology but did not include any adaptive behavior scales in an extensive listing of prominent measures that are currently used in psychological testing in schools. These findings are generally consistent with other findings regarding service utilization, showing, for example, that people with mental retardation, regardless of age, are less likely than others in need to receive psychological services in the community mental health systems, including assessment services.
In contrast to the studies above, which focus more on general clinical practice, direct surveys of school psychologists have disclosed that adaptive behavior scales are among the measures used most frequently. These studies also show that use of adaptive behavior scales has been growing over time (Hutton et al., 1992; Ochoa et al., 1996; Stinnett et al., 1994). Presumably, these findings reflect the importance of the schools as a setting in which the presence of mild mental retardation is frequently first identified and the use of adaptive behavior scales as a component of this practice. Nonetheless, available research on the clinical use of adaptive behavior scales for diagnosis and treatment-related purposes by either school psychologists or community clinical psychologists appears to be relatively sparse and does not focus on groups of people with mental retardation, as such (i.e., Clinger et al., 1988; McNamara et al., 1994; Pearson & Lachar, 1994; Roberts et al., 1993; Voelker et al., 1990; Wolber et al., 1997).
Taken together, these findings suggest that the primary cadre of psychologists with experience and expertise in the use of adaptive behavior measures, those who are most likely to use them in assessment and classification of mental retardation, consists of school-based practitioners. At the same time, it has been noted that use of adaptive behavior measures in the process of identifying children with mild mental retardation, especially, may be forgone in many schools because the academic failures or behavioral problems that prompt teacher referral of students, in and of themselves, may be considered valid indicators of limitations, deficits, or delays in adaptive behavior (McCullough & Rutenberg, 1988). However, children who do meet intellectual and functional criteria for mental retardation also are classified as having disabilities other than mental retardation in some schools and in some cases, and not necessarily consistently so (McCullough & Rutenberg, 1988). Finally, it has been suggested that adaptive behavior and social competence represent an important facet of adjustment in academic contexts, as important if not more so than intelligence (Forness et al., 1998). It is not evident that adaptive behavior scales efficiently differentiate among individuals with diverse
disabilities that can be described as mild in degree (e.g., mild mental retardation, hyperactivity, specific learning disability) (Gresham & MacMillan, 1997; Zigler et al., 1984).
Although schools may be the service settings in which adaptive behavior measures are most likely to be used, the information derived from these assessments may not be considered meaningful for the purposes of classification by decision makers. It is possible that the use of these measures is diminishing in local educational agencies, with increasing emphasis on specific educational classification in many states. As a result, they may become less available for use in disability determinations. It also appears that community practitioners, aside from those associated with developmental disabilities clinics or centers or with community developmental disabilities services, may not be well versed in the use and interpretation of adaptive behavior measures or prepared to apply different measures in different situations for different purposes.
Clinical Considerations in the Selection and Use of Adaptive Behavior Scales
In the committee’s view, adaptive behavior is an essential component of the mental retardation diagnostic construct, and all agencies contemplating mental retardation diagnoses should give consideration to adaptive behavior. This consensus rests on the accumulated wisdom in the field of mental retardation, including the fact that adaptability in meeting the demands of everyday living was fundamental to conceptions of mental retardation long before effective tests of intellectual functioning were developed. Adaptive behavior has been fundamental to conceptions of mental retardation at least since the early 19th century (Doll, 1936a, 1967).
Choice of Assessment Methods
In the committee’s view, the use of standardized measures of adaptive behavior is potentially valuable in the overall assessment of adap-
tive behavior. The value of such instruments will depend on careful decisions about instrument choice, score interpretation, and consideration of other information that bears on adaptive status. The committee does not recommend any specific list of instruments, but choices should be guided by the reviews of the available instruments in this chapter and the research literature on existing and new instruments.
Instrument Choice
Informed judgments are required about using an adaptive behavior instrument in the evaluation of SSA eligibility based on a diagnosis of mental retardation. For most people, the use of currently available adaptive behavior instruments along with other information on adaptive functioning will improve decisions about mental retardation classification. The decision on which standardized instrument to use must be informed by knowledge of the following characteristics of clients, respondents, and instruments.
-
The instrument must be appropriate to the age of the client and the client’s approximate functioning level. Currently available instruments typically do not provide sufficient coverage of some aspects of adaptive functioning for adolescents and adults who are functioning in the IQ range of 60 to 75, the range in which diagnostic decisions about mental retardation are most difficult. Careful analysis of the appropriateness of the item content and density of specific measures is crucial.
-
An appropriate respondent, knowledgeable about the examinee, is required for most adaptive behavior instruments. If an appropriate respondent is not available, use of the instrument in some other way (e.g., self-report, unless a self-report version of the protocol is available) violates basic standardization procedures, rendering normative comparisons invalid. There are some techniques that extend the range of appropriate respondents. For example, some instruments permit more than one respondent to answer different items, depending on which respondent is most knowledgeable about the behavior (Adams, 2000). Another instrument permits adult client self-report
-
(Harrison & Oakland, 2000a), a promising method that needs further study of its feasibility with clients having IQ scores in the range of 60 to 75 (Millham et al., 1978). Still another way to extend respondent usefulness has been to permit guessing on items involving behaviors that have not been observed (e.g., Harrison, 1984; Harrison & Oakland, 2000a). These results become increasingly unreliable and invalid as the number of guesses increases.
-
Scores from the instrument that are useful in diagnostic decisions must be provided and, in turn, interpretations need to be guided by the structure and organization of the adaptive behavior inventory. Diagnostic decisions about mental retardation nearly always involve normative comparisons using various derived scores. Standard score scales are preferred for these comparisons. Useful score scales and appropriate norms are vital features of adaptive behavior instruments used in diagnostic decisions.
-
The instrument’s structure must guide interpretation. For example, the ABAS is organized into 9 or, depending on age, 10 adaptive skills areas, clearly reflecting the 1992 AAMR manual on classification (American Association on Mental Retardation, 1992), which also identified 10 adaptive skills areas. Factor analysis results do not support the existence of more than one overall ABAS general factor. Interpretation should focus on the composite score or, perhaps, implement the AAMR classification criterion of deficits in two or more adaptive skills areas. Use of 3 to 5 group factor scores, appropriate with the SIB, the VABS, and some other instruments, would not be appropriate with the ABAS.
-
Interpretation of the results of instruments must consider the possible influence of unintentional response sets as well as more deliberate efforts to raise or lower the adaptive behavior results in order to achieve certain outcomes. One important protection against inappropriate adaptive behavior decisions, which is due to respondents intentionally reporting invalidly low adaptive behavior performance, is consideration by the examiner of further information about everyday
-
performance of social roles and related activities that are consistent with presence of adaptive limitations.
Typical Performance Measurement and the Nature of Adaptive Behavior
Perhaps the most fundamental problem with regard to adaptive behavior measurement is the relationship of existing measures to the conceptions of the underlying construct. Is adaptive behavior a set of abilities and skills useful in coping with environmental demands that are mastered by the individual? Is adaptive behavior the consistency with which an individual performs various skills in coping with environmental demands? The former, mastery, suggests assessing what people can do, whereas the latter suggests assessing what people typically do.
Mastery assessments typically involve direct testing of a person with a set of tasks administered under standardized conditions that permit comparisons to norms or to absolute standards for performance. In the mastery approach, examinees are encouraged to do their best, and testing conditions are designed to elicit maximum performance. Traditional measures of achievement and intellectual functioning are examples of maximum performance tests.
Measures of typical performance involve an attempt to assess what an individual typically does or how a person usually feels (Cronbach, 1990). Individuals or third-party respondents are asked to indicate their usual feelings or behaviors, not their best or most positive feelings or behaviors. Inventories or checklists that attempt to assess vocational interests, emotional status, and personality traits nearly always are typical performance measures.
The adaptive behavior construct has both typical performance and maximum performance elements, a characteristic that complicates measurement operations. The typical adaptive behavior inventory inquires about both the individuals’ skills or abilities (what they can do) and about what they usually do in various circumstances (performance of skills or typical performance). Various measures differ on the degree to which they attempt to assess the can-do and does-do character-
istics of adaptive functioning (Adams, 2000; Sparrow et al., 1984a). This leads to some unique problems with these measures. The skills or abilities items may be readily assessed through direct measures of the individual with behavioral tasks, while performance or does-do features can be assessed only through extensive behavioral observations that often are impractical given the breadth of the adaptive behavior construct and the number of relevant settings. Therefore, the most common method of assessing adaptive behavior is through a third-party respondent, although many difficult measurement issues arise in such assessments.
The distinction between maximum performance and typical performance assessments might be illustrated with some common adaptive behavior items. Use of a telephone is a common item on communication subdomains of many adaptive behavior inventories. Looking up a phone number is a relevant item for that subdomain. This skill could be assessed by giving the individual a local phone directory, asking them to look up a number, and observing the results, yielding a measure of whether the individual can demonstrate this skill. Another method is to ask a third-party respondent (e.g., a parent or teacher) either very general questions about communication skills, a more specific question about telephone use, or a direct question like “Does Edouard find a number by looking it up in a telephone book?” As a general rule, skills can be measured directly with greater accuracy, reliability, and validity than performance. It is, however, performance or typical performance that most adaptive measures address. In addition to the usual considerations attendant on any measure of individuals, special considerations always exist with typical performance measures (Cronbach, 1990).
Some Differences Among Typical Performance Measures
Adaptive behavior measures differ regarding the use of typical or maximum performance methods. The most widely used measures use a typical performance approach involving third-party respondents (Bruininks et al., 1996; Harrison & Oakland, 2000b; Lambert et al.,
1993b; Sparrow et al., 1984b), although several differences exist among the response formats for items in these measures. Adams (2000), in contrast, uses a mixture of typical performance with third-party respondents and maximum performance operations.
This chapter has discussed problems with item and score scale floors and ceilings, item sampling in relation to the behaviors that are most problematic at different developmental periods, item density, reliability of informants, and validity of informants. It is crucial that people conducting or interpreting adaptive assessments take these problems into account.
Structured Versus Unstructured Interviews
There are vast differences in how the third-party respondent reports on the adaptive behaviors of a client, particularly in the structure for the interview. Interview methods recommended for different measures vary from high to low structure. On one instrument, the items are shown to the respondent and the respondent is given responses from which to choose (e.g., Bruininks et al., 1996), while in another the interviewer is required to assess adaptive competencies through a general conversation with prompts such as “Tell me about Thomasina’s language skills” (Sparrow et al., 1984a). The latter measure requires a more skilled interviewer, as well as a relatively verbal respondent who spontaneously offers sufficient information to permit the interviewer to determine scores on items, or evocation of relevant information through prompts for further details. Many of the parents of children suspected of meeting criteria for mild mental retardation may themselves experience cognitive difficulties and are relatively nonverbal (Ramey et al., 1996), making semi- or unstructured interviews much more difficult to conduct in a standardized manner.
Response Sets
Highly structured interviews have unique problems as well. A number of well-known, often unintentional, response sets are espe-
cially applicable to the more structured third-party respondent measures and, to a lesser extent, the less structured approaches (Anastasi & Urbina, 1997; Cronbach, 1990; Sattler, 1988, 1990). Response options such as “never,” “sometimes,” and “always” or Likert-type response formats using a five- or seven-point continuum with anchor statements like “very good,” “good,” “acceptable,” “poor,” and “very poor” are open to a variety of response sets. Some of the more common and relevant response sets are (a) social desirability, involving responses consistent with positive or desirable connotations of the items or behaviors, (b) acquiescence, involving the tendency to say “yes,” “true,” or, in cases in which knowledge is lacking or uncertain, “sometimes,” and (c) halo effects, involving reporting higher adaptive behavior among persons who are more liked by the respondent.
RESEARCH AREAS
Adaptive Behavior: A Social-Cognitive Perspective
In recent years, existing operational definitions of adaptive behavior and techniques for measuring adaptive behavior have been criticized as being inadequate for determining the presence of significant limitations in individuals with mild mental retardation. In particular, criticism has focused on the inadequacy of existing techniques for measuring the social domain of adaptive behavior (MacMillan et al., in press). This attention to and concern about the assessment of social behavior is hardly surprising, given the prominent place that social behavior has historically occupied among the domains of day-to-day life that constitute adaptive behavior for individuals with mental retardation.
The social domain is particularly important to assess for individuals with mild mental retardation because prominent limitations that these individuals experience are often in the domain of interpersonal relationships, rather than in skill domains that are not predominantly social in nature (e.g., activities of daily living, motor skills). Interestingly, individuals with mild mental retardation often face their most
significant obstacles to competitive employment and job retention arising not from task-related skills, but rather from limitations in their social functioning (Bullis & Foss, 1986; Butterworth & Strauch, 1994; Chadsey-Rusch, 1992; Foss & Bostwick, 1981; Greenspan & Shoultz, 1981; Salzberg et al., 1988; Salzberg, Likins et al., 1986).
A major reason why proper assessment of the social domain of adaptive behavior can be a challenge for eligibility examiners is that the limitations in social functioning in individuals with mild mental retardation are often difficult to quantify with available assessment methods. Often, these limitations take the form of poor judgment or social rule violations, rather than markedly maladaptive behavior (Greenspan & Granfield, 1992). As Switzky et al. (1996) put it, “relatively immature, as opposed to deviant, social behavior has always been the central distinguishing feature of this disability” (pp. 7-8). Furthermore, these limitations may be more noticeable in certain settings or circumstances than in others (Greenspan, 1999). For example, an individual with mild mental retardation may be familiar with the routines and may benefit from the supports that staff provide in the supervised apartment program in which he lives. However, he may have difficulty keeping a job because he has difficulties interacting with a changing cast of coworkers or customers who are unfamiliar with his social style.
Clearly, examiners need to be concerned about whether available instruments and practices for assessing adaptive behavior adequately document critical difficulties in social functioning that prevent individuals with mild mental retardation from fulfilling key roles and expectations in society. At present, a variety of assessment instruments have been employed in research and clinical settings that attempt to capture these individuals’ social limitations. The available instruments include indirect assessments, such as rating scales that assess an individual’s typical performance of social behaviors based on information from informants, including teachers, parents, and job coaches, as well as instruments that permit direct assessment of the processes that, according to theoretical models of successful social adaptation, under-
lie the ability to perform situationally appropriate behavior. With regard to the direct assessment of processes, the overarching construct of social cognition has been put forth by developmentalists over the past four decades (e.g., Crick & Dodge, 1994; Dodge, 1986; McFall, 1982; Trower, 1982). Social cognition encompasses such constructs as social problem solving (Spivack & Shure, 1974), decision making (Hickson & Khemka, 1999), and social and emotional learning (Elias et al., 1997). Overall, the construct of social cognition represents the cognitive aspects of social functioning.
As social cognition has matured as a research discipline, researchers have developed methodologies for assessing social-cognitive processes and have demonstrated the usefulness of these methodologies for detecting the limitations that individuals with mild mental retardation exhibit in their ability to adapt to changing social situations. Currently, instruments and interviewing procedures for assessing social-cognitive processes can provide examiners with valuable supplemental information about the social functioning of individuals with mental retardation. This information may otherwise be lacking because of inadequacies in existing adaptive behavior measures. In addition, social-cognitive assessment can also be helpful in establishing that an individual’s social problems are indeed a manifestation of an underlying cognitive impairment (in accordance with standard definitions of mental retardation), rather than primarily reflecting other factors, such as environmental constraints or motivational characteristics. Thus, social-cognitive assessment increases the likelihood of making accurate diagnostic and disability determination decisions by increasing the pool of information available to an examiner regarding an individual’s functional limitations, while simultaneously reducing the risk of “false positive” decisions.
The potential utility of social-cognitive assessment techniques for the evaluation of individuals with mild mental retardation for eligibility determination purposes is evident in focusing on three major skill areas: social perception, the generation of strategies for resolving social problems, and consequential thinking. These three processes oc-
cupy a prominent place in most theoretical models of social cognition (e.g., Crick & Dodge, 1994; Gumpel, 1994; Leffert & Siperstein, in press; McFall, 1982).
Social perception refers to an individual’s ability to interpret or “read” relevant social messages from others (Maheady et al., 1984). These messages, known as social cues, consist of verbal and nonverbal stimuli, such as physical actions, words, facial expressions, tone of voice, and body language, which tell about others’ behaviors, feelings, and intentions. Individuals with mental retardation often demonstrate difficulties at the most basic level of recognizing specific types of social cues (e.g., recognizing a person’s emotional state on the basis of his or her facial expression) (Adams & Markham, 1991; Gumpel & Wilson, 1996; Harris, 1977; Hobson et al., 1989). Research with children and adolescents with mental retardation has found that they also have difficulty integrating information from multiple cues in order to interpret a social situation (Brosgole et al., 1986; Doman, 1967; Gomez & Hazeldine, 1996; Leffert & Siperstein, 1996; Leffert et al., 2000; Maheady et al., 1984).
The assessment of social perception skills in individuals with mild mental retardation has involved a variety of instruments, with subsequent methodological refinements, which have been developed and employed over four decades with children, adolescents, and adults. For example, the Test of Social Inference (TSI—de Jung et al., 1973) employs the technique of presenting an individual with mild mental retardation with illustrations of common social situations and asking him or her, for each illustration, to tell the examiner what the picture is about. Of the various social perception assessment instruments that have been developed, the TSI is the instrument that has been used most widely to assess social perception skills in this population (de Jung et al., 1973; Matthias & Nettelbeck, 1992).
The second social-cognitive process is the generation of strategies for resolving social problems. Through the assessment of strategy generation, researchers have been able to evaluate an individual’s fund of social knowledge (i.e., his or her repertoire of social strategies), as well as the ability to adapt to varied social situations by generating
situationally appropriate strategies. Research with individuals with mental retardation has consistently documented limitations in their performance of both of these components of strategy generation.
Regarding strategy repertoires, for example, researchers have found that children and adults with mental retardation have a limited repertoire of appropriate social strategies to draw from (Herman & Shantz, 1983; Smith, 1986). Their repertoires often exclude certain types of socially adaptive strategies. For example, they rarely employ the strategy of attempting to work out a mutually acceptable compromise solution in instances when one’s interests conflict with another person’s wishes (Hickson & Khemka, 1999; Hickson et al., 1998; Jenkinson & Nelms, 1994; Smith, 1986).
Regarding the ability to adjust one’s social strategies to fit the needs of a particular social situation, children with mild mental retardation often fail to use information from the specific social cues present in the social situation to guide their search for appropriate strategies (Leffert et al., 2000). As a result, they often rely on generic, one-size-fits-all strategies, such as appealing to an authority, rather than adjusting their strategies in accordance with situational demands. At the workplace, for example, overdependence on the strategy of appealing to a supervisor, regardless of the nature of the problem, can be a problem in creating tension with peers or in creating a perception that the person cannot function autonomously in a work setting.
Unlike the area of social perception, there is no single instrument for assessing strategy generation in individuals with mental retardation. Rather, there is a standard clinical methodology that consists of presenting the individual with a hypothetical situation in the form of a story and asking “What would you do if this happened to you?” The Social Problem-Solving Test (Castles & Glass, 1986) is an example of an assessment instrument employing this methodology that was specifically designed for use with individuals with mental retardation. The technique of asking open-ended questions that tap the process of generating strategies for solving problems is widely used in standard assessments of intellectual functioning, such as the Wechsler scales.
The third social-cognitive process, consequential thinking (i.e., reasoning regarding the consequences of carrying out different social strategies), is also a critical process in the adaptive behavior of individuals with mild mental retardation. Recent studies with these individuals have documented limitations in their reasoning about the consequences of strategies that make it difficult for them to select a social strategy that is appropriate for a given social situation. Rather than weighing the likely outcomes of enacting a particular strategy in a given situation, these individuals tend to render global judgments (e.g., whether a strategy is generally a good thing or bad thing to do) when evaluating behavioral options. Consequently, they have difficulty evaluating which potential strategy is best to enact in a particular situation (Hickson et al., 1998; Jenkinson & Nelms, 1994).
Methodologies for assessing consequential reasoning have existed for several decades. A widely used technique, which was first employed by Spivack and Shure (1974), is to present the individual with a story describing a social problem, as well as a particular strategy that the protagonist might use to resolve the problem. The person is then asked, “What will happen after” the protagonist carries out this strategy? Another, more open-ended assessment technique is to present a social problem and then to ask the interviewee to relate everything that is going through the protagonist’s mind as he or she tries to decide what to do about resolving the problem (e.g., Hickson et al., 1998; Jenkinson & Nelms, 1994). A third approach is to ask individuals with mild mental retardation to select the best strategy for resolving a social problem from among several alternatives. This is the approach that has been utilized in the Test of Interpersonal Competence for Employment (TICE—Foss et al., 1986). The TICE, which is commercially available, consists of two subtests that assess the individual’s ability to evaluate strategies in relation to the situational demands of two distinct social interaction contexts common in work settings: interaction with coworkers and interaction with supervisors. Auty and colleagues (1987) have found positive correlations between subtest scores on the
TICE and supervisor-rated work skills, self-reported job satisfaction, and worker productivity among adults with mild mental retardation.
Social-cognitive assessments have already demonstrated their usefulness as a supplement to standard adaptive behavior rating scales. They have provided valuable information that has informed decision making about interventions to improve the social functioning of individuals with mental retardation. Specifically, instruments such as the TSI, the Social Problem-Solving Test (Castles & Glass, 1986), and the TICE have been successfully employed with this population for the purposes of determining where to begin instruction in social skills and documenting the improvements that have resulted from instructional interventions. These assessment instruments, which have been useful in instructional contexts, can also be valuable for the evaluation of an individual’s eligibility for SSA services.
The social-cognitive processes and the approaches that are used to measure them can also inform and enrich the interviews that examiners conduct with individuals with mild mental retardation and other informants. Table 4-4 presents examples of questions that can guide examiners in eliciting information regarding the three social-cognitive processes reviewed here. By eliciting information about an individual’s performance of these processes, the examiner can increase the likelihood of detecting impairments in social functioning that often characterize this population. Additional measures of social cognition or social skills and issues relevant to social skills assessment of people with mental retardation have been discussed further (Bell-Dolan & Allan, 1998; Blacher, 1982; Blake & Andrasik, 1986; Jackson et al., 1981; Matson et al., 1983; Meyer et al., 1990; Monti, 1983; Smith & Greenberg, 1979; Van Hasselt et al., 1981).
Overall, as a supplement to standardized adaptive behavior assessment scales, social-cognitive assessment has the potential to contribute to the improvement of SSI and DI eligibility determination practices by enriching the pool of relevant information that is available for resolving uncertainty in decisions regarding impairment in the social domain. In this fashion, the assessment of social-cognitive processes can
TABLE 4-4 Question Guide for the Assessment of Social-Cognitive Processes
|
Social perception: encoding of social cues |
Does the person recognize that a social problem has occurred? Can the person accurately describe the problem? Does the person attend to and recognize the specific social cues (e.g., facial expression, tone of voice, body language, sequence of actions) present in social situations that indicate others’ emotions and intentions? |
|
Interpretation of social cues |
Does the person accurately interpret others’ emotions and intentions on the basis of the available cues? |
|
Strategy generation |
Is the person familiar with and able to think of a variety of strategies that are potentially appropriate for resolving social problems? Does the person modify his or her strategy from one situation to another based on the type of social problem, the other person’s intentions, and related considerations? |
|
Strategy evaluation and selection |
Can the person anticipate the consequences of carrying out different strategies for resolving particular social problems in a given social context? In doing so, does the person consider long-term and more abstract consequences of a carrying out a particular strategy (e.g., impact on maintaining interpersonal relationships or keeping one’s job) as well as the immediate and more tangible consequences (e.g., personal gratification, escaping from an immediate problem)? |
become part of a more comprehensive approach to individual assessment that includes information from informants about day-to-day behavior, as well as direct assessment of skills of a social-cognitive nature. The information obtained from this type of evaluation can clarify the
nature and extent of the limitations those individuals with mild mental retardation experience in adapting their behavior to meet the social demands and expectations of the school, workplace, and recreational and residential settings.
Alternative Assessment Instruments
There are a small number of well-normed adaptive behavior scales that are especially suitable for use in initial determinations for children and youth with possible mental retardation. There is a much larger number of scales that do not have extensive norms but may nonetheless be suitable as a means of gathering and summarizing information that can be assessed on a clinical basis. In addition to summarizing adaptive behavior status for the purposes of diagnosis and establishing SSI and DI eligibility, some adaptive behavior scales, such as the AAMR Adaptive Behavior Scales (both school and residential or community versions) and the Scales of Independent Behavior permit the recording of maladaptive behavior. A record of maladaptive behavior may permit an individual to be qualified for SSI by virtue of concurrent IQ in the range of –2 to –2.66 SD and presence of another mental (or behavioral) disorder (Jacobson, 1990; Jacobson & Janicki, 1983).
Whereas situational and functional assessment are appropriate in intervention design for maladaptive behavior or behavior disorders or problems, norm-referenced or criterion-referenced instruments are appropriate for initial assessment (Reschly, 1992). Possibly the most thoroughly researched and well understood instrument to assess both prosocial and problem behavior among children generally is the Achenbach Child Behavior Checklist (CBC—see Achenbach & Edelbrock, 1978). The CBC differentiates between internalizing (e.g., withdrawal, diminished interests, depressive affect) and externalizing (e.g., aggression against peers or adults, property destruction) behavior problems that may be consistent with a mental disorder (see also Borthwick-Duffy et al., 1997; Fidler et al., 2000; Hodapp et al., 1997). Norms for several versions of the CBC, which are age-graded, are available for both clinical and nonclinical child and youth populations.
In addition to the CBC, there are other instruments available to assess overt behavior, affect, or verbal statements consistent with the presence of mental or behavioral disorders among children and youth with mild mental retardation. Generally, these instruments do not have well-established norms but rather have been assessed for their sensitivity with diagnosed cases (e.g., Reiss & Valenti-Hein, 1994), and some scales are more suitable for youth than for children: the Assessment of Dual Diagnosis (Matson & Bamburg, 1998); the Psychopathology Instrument for Mentally Retarded Adults (Balboni et al., 2000; Linaker, 1991; Sturmey & Ley, 1990; Watson et al., 1988); and the Reiss Screen for Maladaptive Behavior (Havercamp & Reiss, 1997; Prout, 1993; Sturmey & Bertman, 1994) For practitioners skilled in clinical interviewing, a field-tested adaptation of a structured clinical interview is available. This scale is the Psychiatric Assessment Schedule for Adults with Developmental Disability or PASS-ADD (Moss et al., 1996, 1998, 2000; Prosser et al., 1998). All of the measures above have demonstrated concordance with psychiatric diagnosis. They can contribute to accurate and appropriate clinical diagnosis of concurrent conditions that may meet listing requirements for SSI and DI as an alternative to assessment of adaptive behavior.
Finally, as this chapter is being written, the World Health Organization (WHO) has completed development of ICIDH-2, the International Classification of Functioning, Disability, and Health (World Health Organization, 2000; see also Post et al., 1999), a functionally based nomenclature. This nomenclature has dimensions of impairments of body functions, impairments of body structures, activity limitations and participation restrictions, and environmental factors. For the purposes of assessment focused on ascertainment of mental and physical conditions, the most salient measurement dimensions of ICIDH-2 are body functions (e.g., mental processes), and activity limitations and participation restrictions. In conjunction with the ICIDH-2, WHO has developed the World Health Organization Disability Assessment Schedule II (WHODAS II), which, in its most extensive form, contains 36 items tapping domains of: (1) understanding and communicating, (2) getting around, (3) self-care, (4) getting along with
others, (5) household and work activities, and (6) participation in society. The utility of the WHODAS II remains to be established as a means to consolidate adaptive or maladaptive behavior information of value in informing the SSI and DI eligibility determination process.
CONCLUSIONS AND RECOMMENDATIONS
Review of the extensive literature on adaptive behavior and its assessment suggests that adaptive behavior is best viewed as a multidimensional construct. That is, current science suggests that there are various domains of behavior that form the construct of adaptive behavior. Factor analyses of existing measures finds consistent domains of functioning. These domains vary by age, consistent with the development of adaptive behavior. The committee therefore, makes two major recommendations to SSA:
Recommendation: Standardized adaptive behavior instruments should be used to determine limitations in adaptive functioning. In general, the cutoff scores for adaptive behavior should be one standard deviation below the mean in two adaptive behavior areas or one and one-half standard deviations below the mean in one adaptive behavior area.
-
Adaptive behavior measures should be used whenever possible, but only when there is an instrument that matches the client’s characteristics and when an appropriate third-party respondent is available.
-
A client can be determined to have a significant limitation in adaptive functioning even with scores that do not meet the above criteria IF there is compelling evidence of adaptive behavior deficits that significantly impair performance of expected behaviors.
Recommendation: Revisions should be made in the adaptive behavior areas or domains emphasized in SSA regulations to con-
form to factor analysis results. The following areas by age should be adopted by SSA:
-
Infancy/early childhood (approximate ages birth to 4): motor/ mobility, social, communication, daily living skills (self-help).
-
Childhood (approximate ages 5 to 17): motor/mobility, social, communication/functional academic skills, daily living skills.
-
Adolescence/adulthood (approximate ages 18 and older): motor/mobility, social, communication/practical cognitive skills, daily living skills, work skills/work-related behaviors.
Current science also suggests that several measures of adaptive behavior tap into these domains. These measures have excellent psychometric properties, with reliabilities of about .90. Also, current measures also evidence strong validity, as described in the chapter. The committee has identified several measures that would be useful in disability determination for mental retardation.
Unlike intelligence tests, which measure maximum performance, adaptive behavior assessment focuses on what the individual typically does. Assessments work best when they document: (a) quantitative level of performance, (b) fluency of performance (e.g., qualitative criterion performance), (c) the extent to which the individual has failed to acquire skills or failed to perform skills already learned, and (d) the inability of the individual to perform skills through lack of opportunity. The committee’s review of the scientific and practice literature also reveals that adaptive behavior is a broadly focused construct. The focus is on the ability of the individual to function independently, with minimal external supports, by adjusting his or her behavior in a self-guided fashion to meet varied situational demands and expectations.
Our review of the practice literature reveals that adaptive behavior scales are in wide use by some groups of clinicians. In our judgment, good clinical practice requires that data from standardized adaptive behavior scales be combined with other clinical or behaviorally oriented information in determining the presence or the absence of adaptive behavior deficits. These other bits of data could include a review
of developmental and social history, direct observation of the individual’s behavior, verbal reports from interviews, and the use of the other structured and semistructured interviews. Best-practice guidelines require that clinicians using adaptive behavior measures employ those that are culturally compatible and have suitably contemporary and age-related norms.
Finally, the committee has identified a number of research areas, focusing on which would improve the measurement of adaptive behavior for mental retardation diagnosis. These areas include social-cognitive and social skill assessment—with a specific focus on social cognitive processes of social perception, strategy generation, and consequential thinking—and vocational and work-related skills assessment with prognostic value. In addition, there is a strong need to fund studies examining the nature and distribution of adaptive behavior deficits among individuals with mental retardation in general and those with mild mental retardation more specifically.



































































