A
Conceptual Framework for Assessing the Consequences of Uninsurance for Communities
The conceptual framework used in this report, and the variations on this framework described in Chapter 2, are closely related to the conceptual framework introduced in the Committee’s first report, Coverage Matters (IOM, 2001a). In the paragraphs that follow, the Committee’s initial framework is described and its modification for use in this report is clarified.
Figure A.1 depicts the conceptual framework used in Coverage Matters. The framework is based on Andersen’s model of access to health services, which incorporates ideas from the behavioral sciences to understand the process of health services delivery and health-related outcomes for individuals (Andersen and Aday, 1978; Andersen and Davidson, 2001). In addition, it draws on an economic model of insurance status and the impact of out-of-pocket costs on health care demand.
To describe the roles of factors at the individual, family, and community levels (e.g., an individual’s health insurance status) that influence both the process of services delivery and the consequences of health care experiences, the framework uses Andersen’s grouping of variables into three categories: (1) resources that foster or enable the process of obtaining health care; (2) personal or community characteristics that favor or predispose action related to obtaining health care; and (3) needs for health care, as articulated by those in need, determined by health care providers, or identified by researchers and decision makers. Arrows and spatial relationships among the boxes in Figure A.1 indicate hypothesized causal and temporal relationships.
To depict the economic consequences of uninsurance, the Committee creates links within Andersen’s framework among determinants of health insurance and such factors as family economic well-being, the institutional viability of health services, and community-level socioeconomic conditions. This expansion allows
the Committee to assess hypothesized interactions between economics and health. The Committee recognizes that insurance is one of many factors that can influence the physical, social, and economic health of communities and their health care arrangements.
CONCEPTUAL FRAMEWORK INTRODUCED IN COVERAGE MATTERS
The left panel of Figure A.1 addresses the main economic forces affecting the insured or uninsured status of individuals and families. Individual- and family-level characteristics include financial resources, categorical eligibility for public health insurance, labor market determinants of employment-based insurance, and the requisite skills to enroll and maintain coverage. Community-level factors include public program eligibility standards, labor market characteristics that determine the availability of employment-based health insurance, and the commercial market for individual health insurance.
The center panel of Figure A.1 is based almost directly on Andersen’s model of access to health care (Andersen and Davidson, 2001). The boxes labeled “individual and family level” and “community level” contain individual- and aggregate-level variables, respectively, believed to influence how people obtain access to health care. Community-level variables are ecologic or aggregate measures to describe the context or environment within which individuals and their families seek and use health care. For example, the community’s morbidity rate for whooping cough might indicate the need for an immunization campaign. Because health care services are provided and consumed locally, the term community refers to a geographic grouping.
Implicit in the categories of resources, characteristics, and needs are judgments about how much a particular variable may be susceptible to change. Variables labeled “resources” are considered, at least theoretically, to be more open to change. Those termed “characteristics” are considered less flexible or manipulable, and those called “needs” comprise a mixed or heterogeneous grouping, with some needs being more changeable than others.
As a whole, community-level and individual- and family-level variables describe many potential scenarios for accessing health care. The variables within the box labeled “health care” describe how these potentials may be realized, with particular attention to the role of health insurance coverage. The process of health care delivery is characterized in terms of three types of variables: (1) personal health practices (e.g., dietary habits, physical exercise), (2) use of health services (e.g., number and kind of physician visits within a year), and (3) processes of care (e.g., adherence to clinical practice guidelines). The Committee focuses most of its attention on the literature concerning the processes of services delivery and the utilization of health services while recognizing that personal health practices may be influenced by insurance coverage and access to care.
The right panel of Figure A.1 describes the ways in which the committee
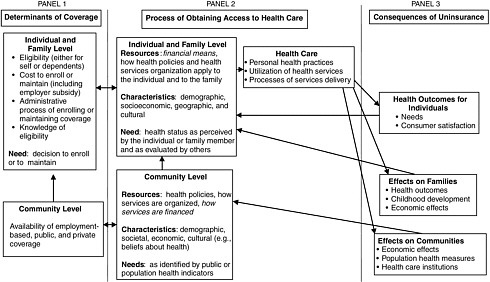
anticipates that health insurance status may affect the health, economic, and social characteristics of individuals, families, and communities by means of access to and the process of health care delivery. These effects of realized access to health care cascade from the smallest unit of analysis, the individual, to increasingly larger units, first the family and then the community. The consequences linked to health insurance influence community-level and individual- and family-level variables that describe the process of obtaining access to health care and also of gaining or losing health insurance coverage. This last panel should make it clear that the process is dynamic with multiple feedbacks. For example, employment status and income affect family insurance status, which affects current and future health status. Health status, in turn, can influence future employment status, bringing us full circle.
CONCEPTUAL FRAMEWORK FOR THIS REPORT
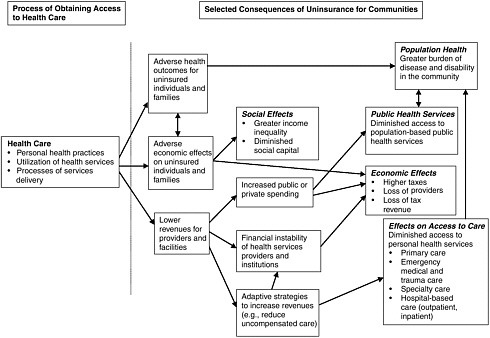
Figure A.2 depicts a version of Figure A.1 modified to reflect the focus of the Committee in this report. The modified version draws on the same theories and conceptual approaches to health insurance as does the initial version in Figure A.1. It focuses on part of the second and third panels of Figure A.1, to emphasize hypothesized community effects and pathways believed to lead to community effects. The left panel of Figure A.2, containing a box labeled “health care” corresponds to the center panel of Figure A.1, while the right panel of Figure A.2 corresponds to both the third panel of Figure A.1 (labeled “consequences of uninsurance”) and the box labeled “community-level determinants of coverage” in the left panel of Figure A.1. Where both frameworks are similar, the text description is shortened in Figure A.2.
The health, social, and economic consequences of delayed or forgone health care for uninsured individuals and families (as depicted in the two boxes labeled “adverse health outcomes for uninsured” and “adverse economic effects”) can result in a greater burden of disease and disability for the community overall as well as erosion of the capacity for timely and appropriate health services delivery in the community. To the extent that uninsured individuals and their families obtain health services, the uncompensated care burden on local providers and facilities (as depicted in the box labeled “lower revenues for providers and facilities”) serves as another pathway to community effects because it is hypothesized to lead to (1) pressures to increase public spending to subsidize care for uninsured persons, (2) increased costs for health care and for health insurance, and (3) financially destabilized local health services. As a result, all members of the community may experience diminished access to and quality of health services, as well as a greater burden of disease and disability.