
I Introduction
I.A STUDY RATIONALE AND SCOPE
From 1945 through 1962, the United States conducted atmospheric tests of nuclear weapons. Hundreds of thousands of military personnel participated in the conduct of those tests, and many of the participants were exposed to ionizing radiation. The effects of that radiation on military personnel first became of interest in the middle 1970s, and since 1981 Congress has passed numerous laws concerning compensation of veterans who were exposed to radiation and later claimed health effects. In recent years, there has been renewed concern regarding the efficacy of those laws and, in particular, the use of dose reconstruction to assess radiation doses received by participants. In April 1998, the Senate Committee on Veterans Affairs held a hearing that focused on dose reconstruction and on issues regarding compensation for “atomic veterans.”
In August 1998, the committee released its hearing report and asked the General Accounting Office (GAO) to review all available information related to dose reconstruction to determine its reliability for measuring veterans’ radiation exposures and to assess the completeness of historical records used to assign radiation doses. GAO completed its review in January 2000 and found that dose reconstruction was a valid method of estimating veterans’ doses for compensation claims and no better method was known, but that the program lacks an independent review process. GAO recommended that the Department of Defense (DOD) establish an independent review process for its dose reconstruction program. Section 305 of Public Law 106-419, which implemented the Senate Committee on Veterans Affairs legislation, called for the DOD to enter into a contract
with the National Academy of Sciences for a review of the dose reconstruction program of the Defense Threat Reduction Agency (DTRA).
In response to the congressional mandate, the Academy formed a committee in the Board on Radiation Effects Research of the Division on Earth and Life Studies to conduct a review of the DTRA dose reconstruction program. Because dose reconstruction is a multidisciplinary science, the committee consisted of members with expertise in radiation physics, pathway analysis, biomedical ethics, health physics, biostatistics, and epidemiology. The study began in December 2000.
The task set before the committee is described in the following scope of work:
The committee will conduct a review which will consist of the selection of random samples of doses reconstructed by the Defense Threat Reduction Agency (DTRA) in order to determine: 1) whether or not the reconstruction of the sample doses is accurate; 2) whether or not the reconstructed doses are accurately reported; 3) whether or not the assumptions made regarding radiation exposure based on the sampled doses are credible; and 4) whether or not the data from nuclear tests used by DTRA as part of the reconstruction of the sampled doses are accurate. The committee will produce a report that will include a detailed description of the activities of the committee. If appropriate, the committee will make recommendations regarding a permanent system of review of the dose reconstruction program of DTRA. If after a year the committee has concluded that its findings differ from the previously published and congressionally directed studies or that significant changes are required to the existing dose reconstruction procedures and methodology, it will issue an interim letter report summarizing its findings and will make appropriate recommendations for any changes warranted.
In this report, the committee is transmitting the results of the review of the DTRA dose reconstruction program that the committee conducted in fulfillment of its task.
I.B BACKGROUND AND HISTORY
I.B.1 The US Nuclear-Weapons Testing Program
The US nuclear-weapons testing program began during World War II with Shot TRINITY, the first test of an atomic bomb. TRINITY, a plutonium implosion device, was detonated at 5:30 a.m. on July 16, 1945, from a 100-ft tower in the Journada del Muerto (Journey of Death) Desert, in the Alamogordo bombing range in New Mexico (Malik, 1985). It had a yield equivalent to 21 kilotons of TNT.
Thunderstorms and rain squalls had threatened to postpone the test, but the weather improved and the test was allowed. Radiation monitoring of fallout
material was accomplished by joint teams of Los Alamos Scientific Laboratory and military personnel, who searched the most probable fallout areas with radiation-detection instruments, questioned residents, and took soil samples for laboratory analyses and comparison with original radiation-monitor readings.
Residents of the village of Bingham, New Mexico, some 18 miles from ground zero, were startled by a brilliant flash of light that awakened them and their families, as recounted to monitoring teams in interviews a few hours after the detonation (Hoffman, 1947). Those interviews were the first of civilians who had witnessed an atomic-bomb explosion. A previous story had been arranged regarding an explosion of store ammunition at the Alamogordo bombing range to answer questions for national security purposes.
The first test was followed by the detonation over Hiroshima, Japan, on August 6, 1945, of the bomb named LITTLE BOY because it was small (10 ft long, 28 in. in diameter, and weighing 9,000 lb) compared with FAT MAN (12 ft long, 60 in. in diameter, weighing 10,800 lb, and having fins), which was detonated over Nagasaki, Japan, on August 9, 1945, and resulted in ending the war with Japan. Unlike TRINITY, LITTLE BOY was a gun-type device containing uranium-235 (235U) and had not been previously tested; FAT MAN was identical with TRINITY except for added tail fins and associated hardware to convert it from a test device to a weapon.
The end of World War II was followed by two nuclear tests at Bikini Atoll in the Pacific Ocean during Operation CROSSROADS, in July 1946. The devices detonated, Shots ABLE and BAKER, each had a yield of 21 kilotons; they were essentially the same as the device detonated at Shot TRINITY and the bomb dropped over Nagasaki. The mostly military participants in CROSSROADS numbered about 43,000.
Operations SANDSTONE in 1948, GREENHOUSE in 1951, IVY in 1952, and CASTLE in 1954—all in the Pacific—were interspersed with Operations RANGER in January-February 1951, BUSTER-JANGLE in October-November 1951, TUMBLER-SNAPPER in 1952, and UPSHOT-KNOTHOLE in 1953 at what came to be called the Nevada Test Site (NTS) (it was called the Nevada Proving Ground, or NPG, until December 1954). Test yields at the Pacific tests increased to 15.3 megatons (MT) of TNT for CASTLE BRAVO in 1954, and yields at NTS tests increased to 74 kilotons with Shot HOOD during Operation PLUMBBOB in 1957, which was the highest atmospheric yield on the continent.
Additional atmospheric test series in the Pacific were WIGWAM in 1955, HARDTACK Phase I in 1958, and DOMINIC Phase I in 1962. Additional atmospheric test series in Nevada were TEAPOT in 1955, HARDTACK Phase II in 1958, and DOMINIC Phase II in 1962. Another test operation was ARGUS, consisting of three nuclear detonations on rockets, each 1-2 kilotons in yield, hundreds of miles above the Atlantic Ocean—far enough above the ocean surface that no detectable exposures of test participants occurred. Overall, the United
TABLE I.B.1 US Atmospheric Nuclear-Weapons Test Seriesa
|
Test Series |
Dates |
Location |
No. Tests |
|
TRINITY |
July 1945 |
Alamogordo, NM |
1 |
|
CROSSROADS |
June-July 1946 |
Bikini |
2 |
|
SANDSTONE |
April-May 1948 |
Enewetak |
3 |
|
RANGER |
January-February 1951 |
NTS |
5 |
|
GREENHOUSE |
April-May 1951 |
Enewetak |
4 |
|
BUSTER |
October-November 1951 |
NTS |
5 |
|
JANGLE |
November 1951 |
NTS |
2 |
|
TUMBLER-SNAPPER |
April-June 1952 |
NTS |
8 |
|
IVY |
October-November 1952 |
Enewetak |
2 |
|
UPSHOT-KNOTHOLE |
March-June 1953 |
NTS |
11 |
|
CASTLE |
February-May 1954 |
Bikini, Enewetak |
6 |
|
TEAPOT |
February-May 1955 |
NTS |
14 |
|
WIGWAM |
May 1955 |
Pacific |
1 |
|
REDWING |
May-July 1956 |
Bikini, Enewetak |
17 |
|
PLUMBBOB |
May-October 1957 |
NTS |
25 |
|
HARDTACK-I |
April-August 1958 |
Enewetak, Bikini |
31 |
|
HARDTACK-II |
September-October 1958 |
NTS |
19 |
|
DOMINIC-I |
April-November 1962 |
Christmas Island, Johnston Island |
31 |
|
DOMINIC-II |
July 1962 |
NTS |
4 |
|
aHigh-altitude rocket tests that did not result in exposure to veterans are not included. Details of individual tests (names, dates, types, yields) can be found in DOE (2000), which is available at http://www.nv.doe.gov/news&pubs/publications/historyreports/default.htm. |
|||
States conducted about 200 atmospheric weapons tests with a total fission yield of about 80 MT.
Table I.B.1 lists the atmospheric nuclear-weapons test series that have been conducted by the United States. The number of tests in each series does not include safety tests and some high-altitude rocket tests. Figure I.B.1 shows the locations of US atmospheric nuclear-weapons detonations where veterans may have been exposed to radiation. Hundreds of underground tests of different weapon designs have since been conducted. There have also been high-altitude, rocket-launched tests and tests of nuclear devices for peaceful uses in a program called PLOWSHARE.
I.B.2 Radiation Exposures of Military Personnel
In understanding the significance of radiation exposures of military personnel that resulted from their participation in the atmospheric nuclear-weapons testing program, it can be helpful to consider that these exposures were in addition to unavoidable exposures to natural background radiation that have been experienced by all personnel throughout their lives. As summarized by the Na
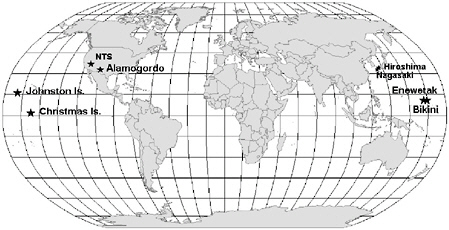
FIGURE I.B.1 Locations of atmospheric nuclear-weapons detonations where military personnel may have been exposed to radiation. A few additional high-altitude air blasts were conducted at sites in the south Atlantic and Pacific oceans, and two underwater tests that resulted in exposures to naval personnel were conducted in the Pacific off the southern California coast (DOE, 2000).
tional Council on Radiation Protection and Measurements (NCRP, 1987a), an average member of the US population receives in each year a total dose from natural background radiation of about 0.3 rem. Exposure to cosmic rays, naturally occurring radionuclides (potassium-40, radium, thorium, and uranium) in rock and soil, and naturally occurring radionuclides incorporated in body tissues (mainly by ingestion) gives a dose in each year of about 0.1 rem, and the remaining 0.2 rem in each year is due to indoor radon. Thus, for example, an average individual who lives for 70 years receives a total lifetime dose from natural background radiation, excluding the contribution from indoor radon, of about 7 rem, and the total lifetime dose, including the contribution from indoor radon, is about 21 rem.
A presentation of information on doses from natural background radiation is not intended to trivialize exposures that military personnel received during their participation in the weapons testing program or to convince individuals that their exposures are of no concern. However, such information can be helpful as each individual judges for himself the significance of his exposures during the testing program.
The types and amounts of ionizing-radiation exposures received by military personnel participating in atmospheric nuclear-weapons test detonations depended on the characteristics of the detonation, the role of the participants, and the proximity of personnel to detonations and fallout of nuclear debris.
When a nuclear explosion occurs, penetrating gamma rays and neutrons are emitted from fission of the fuel (usually 239Pu or 235U or a combination of the two). The gamma rays and neutrons can result in external radiation doses to
unshielded participants at distances up to many kilometers depending on the yield and height of the burst. Emitted neutrons are also absorbed by elements in the soil and air, and this results in radioactive activation products. If the device has a fusion component, as well as a fission component, higher-energy neutrons are emitted that can travel even farther in air before they are absorbed. After the blast, a rapidly rising fireball forms; it contains vaporized fission products and other material, such as unfissioned fuel, debris from the device, and other surrounding material. Depending on the height of the burst, the fireball may also contain soil particles. As the fireball cools, a cloud of radioactive debris is formed. The cloud can extend from a few kilometers above the ground to the stratosphere (in the case of very-high-yield tests), and it expands and diffuses as it is transported away from the test site by the prevailing winds. As the cloud travels through the atmosphere, the radioactive debris begins to fall out, heavier particles first, because of gravitational settling.
Radioactive “fallout” includes hundreds of radioactive fission products with half-lives ranging from fractions of a second to millions of years and unfissioned plutonium and 235U. This debris emits penetrating gamma radiation and less-penetrating beta and alpha particles. Test participants were exposed externally to those kinds of radiation as the debris descended through the atmosphere and after the debris was deposited on the ground and other surfaces. They were also exposed internally by inhaling particles as the fallout descended or was resuspended after being deposited. Because fairly heavy fallout can occur for many hours after a test, even people on ships and islands hundreds of kilometers downwind of a test were exposed. In fact, because the smaller particles can remain in the atmosphere for days, weeks, or even months, almost all the population of the United States was exposed to low levels of fallout from Nevada weapons tests. Debris injected into the stratosphere by the high-yield thermonuclear tests conducted in the Pacific resulted in low levels of fallout over the entire globe (Beck and Bennett, 2002).
Some members of the military participated directly in tests as observers or by conducting maneuvers close to ground zero shortly after a blast. Only a few of the hundreds of thousands of military participants were close enough to be exposed to the initial gamma rays and neutrons emitted in a detonation. The few exposed to neutrons from nuclear-weapon detonations, who were close to the blast, included pilots flying close to detonations to collect samples and volunteer officers in protective trenches at short distances selected to determine safety measures for other military personnel at different distances from detonations during a nuclear confrontation. The number of volunteer officers exposed during atmospheric nuclear-weapons tests was probably less than a few hundred. Most of the exposed military personnel were performing their duties in areas contaminated by fallout from the blasts, either during the fallout period itself or thereafter.
The total number of military and civilian personnel participating in atmospheric weapons tests was about 210,000. In addition to those exposed during the
atmospheric-testing period in the Pacific and within the United States, some 195,000 military personnel were potentially exposed to residual fission products and fissile weapons material while on duty in Japan after and in the area of the bombings of Hiroshima and Nagasaki.
Most radiation exposures of military personnel in the Pacific or within the United States were external exposures to gamma- and beta-emitting fission products deposited on the ground and other surfaces and to activation products produced in soil, water, and other materials by neutrons from nuclear-weapon detonations. Participants were exposed externally to gamma and beta radiation and internally by inhaling descending fallout or resuspended debris. Exposures also resulted from inhalation of fission products and unfissioned plutonium and other fissile material from previous tests; these materials could be resuspended by wind and human activity, as well as by nuclear-blast shock waves, and could have exposed participants to radiation in addition to what they may have received from the tests they were participating in.
In addition to maneuver troops and observers, military personnel were exposed during performance of their support functions and monitoring activities. For example, pilots who took gaseous and particulate samples of clouds from nuclear detonations to be analyzed in determining yields were exposed externally to high levels of gamma radiation from the time they collected the samples until they left their aircraft. These pilots were authorized to receive some of the highest radiation exposures to accomplish their missions. Personnel who removed samples from the aircraft and decontaminated the aircraft were also exposed to radiation. Others were exposed while recovering equipment or decontaminating ships or aircraft. Many participants were exposed to fallout on residence islands or on support ships during tests in the Pacific. Thus, thousands of military participants were exposed to radiation by direct participation in tests, such as during maneuvers or as observers, and thousands more were exposed while performing their routine duties in support of nuclear tests.
From the beginning of the testing period, the primary means of measuring radiation dose to individuals was the film-badge dosimeter. The badges were effective and usually provide reasonable estimates of external gamma-radiation exposure. The accuracy of exposures recorded by film-badge dosimetry has previously been reviewed by the National Research Council (NRC, 1989). However, not all participants wore film badges, especially in the early period of testing, and exposures of most veterans could only be inferred from badges worn by other members of their cohorts or by making assumptions regarding exposure on the basis of radiation readings from the area and the veterans’ locations and times of activities.
Exposures during atmospheric nuclear-weapons tests varied substantially from one veteran to another and depended on many factors. Furthermore, the reconstruction of doses to veterans for the purpose of compensation up to 50 years after the exposures occurred can be complex, tedious, and labor-intensive.
That is the challenge that has confronted DTRA and the Department of Veterans Affairs1 for nearly two decades. The process of dose reconstruction and its validity for the purpose of awarding claims has been questioned by the veterans and by others since its beginning. This report evaluates the process of dose reconstruction for atomic veterans and considers some of the questions that have been raised.
To begin, it is important to have some knowledge of the history of the atomic-veterans compensation program and the laws and objectives that guide it. It is also important to have an understanding of the limits and capabilities of historical dose reconstruction in general. This background information is provided in the sections that follow.
I.B.3 Development of the Nuclear Test Personnel Review Program
Possible radiation exposures of military personnel during observer and maneuver programs at the NTS and during participation in support of testing in the Pacific and at the NTS have been of concern since 1977, when it was first reported that there might be an increase in leukemia among military personnel who participated in Shot SMOKY of Operation PLUMBBOB at the NTS that could be attributed to ionizing-radiation exposure (Caldwell et al., 1980). At that time, exposure to radiation was known to increase the risk of some types of cancer. Additional results reported by Caldwell et al. (1983) expanded observations on the same cohort to incidence of other types of cancer, in addition to mortality from cancers and other causes, and covered a period of 22 years, through 1979.2 However, in this analysis of Shot SMOKY, it was assumed that 3,200 military personnel were exposed during the exercise when in fact only 572 participants were close enough to ground zero to receive exposure.3 The other troops were either at News Nob, an observation point about 12 miles south of Shot SMOKY, or at Camp Desert Rock, about 40 miles south of Shot SMOKY. Because of the incorrect number of participants in the cohort exposed to radiation in Shot SMOKY, the estimate of the number of cases of leukemia might be in error. However, that error is understandable, considering the scarcity of data
available at the time on the activities of participants and the lack of dose information related to atomic tests. It is also important to note that these early studies were the first attempts to investigate effects among the veterans and set the stage for investigations that were to follow.
Concern among military personnel who participated in the testing program continued to grow during the late 1970s. By late 1977, funding was made available by the Energy Research and Development Administration (ERDA; now the Department of Energy, DOE) to begin reorganizing the master file of radiation-exposure records for the US nuclear-testing program. The Defense Nuclear Agency (DNA; now DTRA) had been designated as the responsible DOD agency to address radiation exposure of atomic veterans.
Effects of radiation exposure on military personnel participating in atmospheric nuclear-weapons testing soon became of interest to Congress, which held hearings on the matter. Congress played an important role not only in opening a forum and making sure funding was available to estimate personnel exposure, but also in opening archives to make available documents, many of which had to be declassified. In January 1978, the Nuclear Test Personnel Review (NTPR) program4 was officially initiated as a coordinated effort of the DNA and the Energy Research and Development Administration. Science Applications Incorporated (now Science Applications International Corporation, SAIC) has held a contract to perform dose reconstructions on military personnel almost since the inception of the NTPR program.
One of the first attempts to gather information was a program where veterans were encouraged to call a toll-free number and register data related to their participation. This program was advertised in various military publications. Once a veteran called in, forms were sent to him to provide a written account of his experience in the atmospheric testing program. These data were collected in a database called “File A” that is still retained as part of a veteran’s record. Subsequently, a “File B” was established to collect data from historical documents.
Originally, each branch of the service had an NTPR team to handle its own members’ dose reconstructions. However, that led to disparities between methods and assumptions in estimating personnel doses. In 1983, it was decided to consolidate the teams at DNA and make procedures for dose reconstruction more consistent across the services.
SAIC continued to perform dose reconstructions for DNA and eventually teamed with JAYCOR, which is responsible for confirming a veteran’s status as a participant in the testing program and for developing historical background
information for use by SAIC in estimating doses to the veterans. As of September 30, 2002, 4,048 partial or total dose reconstructions had been performed for specific veterans (Schaeffer, 2002a).
Since the inception of the program, the responsibilities of DTRA (then DNA) and the Department of Veterans Affairs (then the Veterans Administration) have been different. DTRA is responsible for confirming service status and reconstructing doses, and VA is the primary avenue of contact for a veteran and is responsible for determining eligibility for compensation. Each fulfills its role independently of the other, although close interaction is maintained.
I.B.4 Key Laws and Regulations Governing the NTPR Program
About 15 public laws form the basis of regulations that govern the administration of the NTPR program and determine the eligibility of veterans to receive service-connected disability compensation based on their radiation exposure during the nuclear-weapons testing program. Several of the key laws are described below, and then the regulations implementing them are discussed.
The primary law was enacted in 1981: Public Law (PL) 97-72, the Veterans’ Health Care, Training, and Small Business Loan Act. It specified that atomic veterans were entitled to medical care if they could prove that their disease was service-connected, which few could do. The next law was PL 98-542, the Veterans’ Dioxin and Radiation Exposure Compensation Standards Act of 1984, which listed in greater detail how such service connection was to be established. It also listed radiogenic diseases,5 their latent periods,6 and appropriate compensation. When a claim was filed under this law, the veteran had to obtain a dose estimate from the DNA and the estimated dose had to be above a certain level for an award to be made (usually greater than 5 rem).
In 1988, Congress passed PL 100-321, The Radiation-Exposed Veterans Compensation Act. Under this law, referred to as the presumptive law, it is presumed that a veteran’s disease was caused by radiation if the veteran was present at a nuclear detonation, or some associated activities, and if the veteran developed one of the presumptive diseases, regardless of the veteran’s dose. The original presumptive law listed 13 cancers as radiogenic: leukemia, except chronic lymphocytic leukemia; multiple myeloma; lymphoma, except Hodgkin’s disease; primary liver cancer; and cancer of the thyroid, breast, pharynx, esophagus, stomach, small intestine, pancreas, bile duct, and gall bladder. Cancers of the salivary
gland and urinary tract were added in 1992 and bronchiolo-alveolar carcinoma was included in 1999. Finally, in 2002, cancer of the bone, brain, colon, lung, and ovary were added, bringing the total number of cancers considered radiogenic under the presumptive law to 21 (VA, 2002).
The various laws are implemented in Title 38, Code of Federal Regulations, Part 3 (38 CFR Part 3). The regulations authorize the VA to provide medical care and pay compensation benefits to confirmed test participants and dependence and indemnity compensation to certain survivors. A veteran seeking compensation can file a claim with VA. To resolve claims, VA uses one of two processes, depending on the specific type of disease being claimed. Under 38 CFR 3.309, if the veteran was a confirmed participant and has one of the 21 cancers presumed to be radiogenic, the veteran is eligible to receive compensation regardless of dose. Throughout this report, we refer to that situation as “presumptive.”
The second regulation governing the claims process is described in 38 CFR 3.311. It applies to diseases that are not presumed to be caused by radiation exposure but could be linked to radiation if the veteran’s dose was high enough. Alternatively, the veteran can supply evidence that the condition can be caused by radiation, that is, is a radiogenic disease. We refer to that type of claim as “nonpresumptive.” Such a claim is used for veterans with all other forms of cancer and some nonmalignant ailments: tumors of the central nervous system, nonmalignant thyroid disease, posterior subcapsular cataract, and parathyroid adenoma. The process relies on estimating the radiation dose received and evaluating the probability that the disease was caused by the exposure. Under the nonpresumptive regulation, if a veteran’s claim of presence at a nuclear test cannot be verified but the government cannot prove that the veteran was elsewhere at the time, it must be assumed that the veteran was present. The regulation also requires that in assessing a dose, the veteran must be given the benefit of the doubt if information needed to determine the dose is inconclusive or unavailable. The principle of benefit of the doubt is discussed in Section I.C.3.2.
It has happened that a claim was filed under the presumptive regulation but the veteran’s presence at a nuclear test could not be verified, so the veteran was not eligible for compensation under that regulation. In such a case, however, the veteran’s claim can be evaluated under the nonpresumptive regulation.
The laws governing compensation for atomic veterans have continued to change over nearly two decades. There have been advances in the science and tools available for administering the program and for estimating doses. Additional records have also come to light over the years. These changes are reflected in changes to the dose reconstruction process noted by the committee during its review.
I.B.5 Objectives of the NTPR Program
DTRA continues to administer the NTPR program for DOD. VA is responsible for making decisions about awarding claims. The primary function of the
NTPR program is to provide participation data and radiation-dose information to VA and to the veterans.
As described on its Web site (http://www.dtra.mil/press_resources/fact_sheets/display.cfm?fs=ntpr), the NTPR program has four primary objectives, which are summarized below:
-
Providing participant and radiation-dose information to support medical and compensation programs administered by VA and the Department of Justice. The NTPR program also ensures that veterans can obtain access to relevant documents and records about their involvement in US atmospheric nuclear tests or in the occupation forces of Hiroshima and Nagasaki.
-
Conducting historical-records research. Over 100 archives nationwide have been researched for relevant information. More than 40 historical volumes and 25 analytical reports have been developed to provide details on each test and operation. The program has located, retrieved, declassified as necessary, and preserved records pertaining to US atmospheric nuclear tests. The documentation includes service and medical records, film-badge records, pocket-dosimeter logs, special orders, muster rolls, unit memoranda, ship logs, morning reports, flight logs, personal accounts, diaries, and papers.
-
Performing outreach service to veterans and their families and appointed representatives. The outreach includes personal contact with veterans and mass-media announcements to find veterans and publicize the availability of services and of VA’s health-care and entitlement programs.
-
Supporting independent scientific studies to determine whether US atmospheric nuclear-test participants have adverse health effects as a result of their participation. Some of the studies are described in the next section.
I.B.6 Previous National Research Council Studies on Military Personnel Exposed to Radiation in Atmospheric Nuclear-Weapons Tests
The National Research Council has conducted studies related to exposures of participants in atmospheric nuclear-weapons tests. The first report, Mortality of Nuclear Weapons Test Participants (NRC, 1985a), selected participants in five nuclear test series. Numbers of actual test participants were not well known during that study with the result that thousands of test participants were inadvertently omitted and thousands more military personnel who were not participants were included. An additional problem was the illness occurrences in the general populations as a comparison cohort, causing a “healthy soldier effect” that may have obscured illness in atomic veterans. As a consequence, the results of that study were later questioned and a second five-series study of atomic veterans was conducted (IOM, 2000).
The second report, Review of the Methods Used to Assign Radiation Doses to Service Personnel at Nuclear Weapons Tests (NRC, 1985b), was prepared to
advise DNA on whether the methods used in the NTPR program to assign radiation doses were comprehensive and scientifically sound and to recommend improvements if needed. The committee was not charged to conduct audits of the dose assignments or reconstructions for specific veterans. The committee concluded that “the procedures used to estimate external radiation doses were reasonably sound.” It also concluded that “if bias exists in the dose estimates, it is probably a tendency to overestimate the most likely dose, especially for internal emitters.” Further discussion of the findings on methods of estimating dose from internal emitters is given in Section V.C.2. However, the National Research Council committee had difficulty in finding information that summarized the procedures being followed in the dose reconstruction process and recommended that DTRA develop a comprehensive report addressing the methods and procedures being used.
The third report, Film Badge Dosimetry in Atmospheric Nuclear Tests (NRC, 1989), was an in-depth evaluation of film-badge practices used during the weapons-testing period, of recording of dosimetric data, and of overall uncertainties associated with the film-badge dosimeter readings. The report concluded that “it is feasible to estimate dose for participants with reasonable certainty.” The report included methods of addressing uncertainties in film-badge readings and of converting film-badge readings to doses received by organs that are important in assessing the biological significance of exposure.
In 1996, the Institute of Medicine published Mortality of Veteran Participants in the CROSSROADS Nuclear Test (IOM, 1996). The report described a cohort epidemiological study that investigated mortality in US Navy personnel who participated in Operation CROSSROADS, a 1946 atmospheric nuclear-test series in the Pacific. The study did not use dosimetry information for cases, because this information was not considered suitable to support an epidemiological analysis. The report stated that “the findings do not support a hypothesis that exposure to ionizing radiation was the cause of increased mortality among CROSSROADS participants.”
As discussed above, a second five-series study (IOM, 2000) was undertaken to address problems associated with the 1985 report (NRC, 1985a). That project was a mortality study of about 70,000 military personnel who participated in at least one of five selected atmospheric nuclear-weapons test series. The study carefully confirmed the status of each participant and used nonparticipant military personnel as a comparison group. The analysis considered effects among participants for all tests and within each specific test series. The study found that, overall, participants and controls had similar risks of death from all causes. It originally intended to use specific dosimetry information on veterans to determine whether a dose-response analysis could be carried out, and a special working group was formed to investigate the feasibility of using doses generated by the NTPR program. The working group was specifically charged to determine whether the doses recorded for veterans could be used for epidemiological pur
poses and it considered four factors in forming its evaluation: consistency in technical approach, nondifferential methods in dose assignments, quality assurance, and consideration of uncertainties. The working group concluded that the available dose information did not meet the criteria for epidemiology, so dose-response analyses were not performed.
I.B.7 General Accounting Office Reports on the NTPR Program
GAO published two reports related to exposures of veterans in the atmospheric nuclear-weapons testing program. The first, Nuclear Health and Safety: Radiation Exposures for Some Cloud-Sampling Personnel Need to be Reexamined (GAO, 1987), was undertaken at the request of the chairman of the Senate Committee on Veterans Affairs. It addressed the concern expressed by a public-interest group (the Environmental Policy Institute) that radiation exposures of about 300 Air Force personnel associated with flying and decontaminating aircraft had been substantially underestimated in the NTPR program. The report concluded that the doses were indeed underestimated and needed to be re-examined. The NTPR program took actions to address the report’s conclusions.
A second GAO report, Veteran’s Benefits: Independent Review Could Improve Credibility of Radiation Exposure Estimates (GAO, 2000), responded to veterans’ concerns about the methods being used in dose reconstructions performed under the nonpresumptive regulation. GAO’s conclusion was that although studies appeared to validate DOD’s dose reconstruction program for deciding claims, “the agency is not providing independent oversight of the program.” The report noted that VA did not believe that it was responsible for overseeing the DOD program. The GAO report recommended that the dose reconstruction program be continued as a means for deciding claims but also recommended that independent oversight of the NTPR program be considered. The present National Research Council report responds to the issue of independent oversight and to other questions raised by Congress.
I.C PRINCIPLES AND PROCESS OF DOSE RECONSTRUCTION
I.C.1 Introduction to the Process of Dose Reconstruction
Dose reconstruction refers to the process of estimating radiation doses that were received by individuals or populations in the past as a result of particular exposure situations of concern. For example, this report is concerned with radiation exposure of military personnel (the atomic veterans) who were prisoners of war in Japan or were stationed in Hiroshima or Nagasaki after the atomic bombings of 1945 or who participated in various activities during atmospheric testing of nuclear weapons at the Trinity site in New Mexico, at the Nevada Test Site (NTS), and in the Pacific in 1945-1962.
In many respects, the process of dose reconstruction is similar to the process of estimating radiation doses to workers at an operating nuclear facility while they are on the job or doses to members of the public who are exposed to continuing releases of radionuclides from a nuclear facility. The principal distinction is that dose reconstruction generally is concerned with estimating doses that resulted from exposures in the past. The terms historical and retrospective often are used to indicate that characteristic of a dose reconstruction. The distinction is made even though the types of information that can be used to estimate doses may be similar. For example, some external doses received by atomic veterans were monitored at the time with film badges (NRC, 1989) in the same way that external doses to workers at an operating nuclear facility are monitored. However, the quantity and quality of historical data used to support a dose reconstruction may be inferior to data that can be used to monitor exposures of workers and the public today.
Many dose reconstructions have been undertaken over the last two decades. In the United States, dose reconstructions have been performed for members of the public who were exposed to fallout from atmospheric testing of nuclear weapons at the NTS, both in regions near the NTS (Anspaugh and Church, 1986; Anspaugh et al., 1990; Simon et al., 1990; Till et al., 1995; Kirchner et al., 1996; Whicker et al., 1996) and throughout the country (NCI, 1997; IOM/NRC, 1999). Dose reconstructions also have been performed for members of the public who were exposed to releases of radionuclides from nuclear facilities of the DOE and its predecessor agencies (Brorby et al., 1994; Farris et al., 1994a; Farris et al., 1994b; Killough et al., 1998; Apostoaei et al., 1999a; Apostoaei et al., 1999b; Grogan et al., 1999; Rood and Grogan, 1999; Rood et al., 2002), and a program of dose reconstruction to address historical exposures of workers at DOE facilities is under way (DHHS, 2002).
The process of dose reconstruction for atomic veterans generally is similar to the process that has been used in other cases. Dose reconstructions may differ substantially in some respects, such as in the radionuclides, radiation types, and exposure pathways of concern; the types, quality, and quantity of information available for estimating doses; the degree to which modeling, rather than relevant measurements, must be used to estimate doses; and the importance of subjective judgment, both scientific and nonscientific, in estimating doses. Nonetheless, all dose reconstructions, if conducted properly, incorporate a few basic principles. The main purpose of this section is to identify and briefly discuss those basic principles and to present examples of how they have been applied in dose reconstructions for atomic veterans. The dose reconstruction process for atomic veterans is discussed in more detail in Chapter IV.
This section also discusses three other aspects of the dose reconstruction process for atomic veterans that are particularly important: dose reconstructions for atomic veterans are used to evaluate claims for compensation by veterans who developed cancers or other diseases that could have been caused by radiation
exposure; regulations governing dose reconstruction specify that atomic veterans will be given the benefit of the doubt in evaluating claims for compensation; and dose reconstructions for atomic veterans have been performed for many years. Proper consideration of those aspects places unusual demands on the dose reconstruction process for atomic veterans.
I.C.2 Elements of Dose Reconstruction Process
Regardless of the purpose of a dose reconstruction, the process has several basic elements, which the committee identifies as follows:
-
Definition of exposure scenarios,
-
Identification of exposure pathways,
-
Development and implementation of methods of estimating dose,
-
Evaluation of uncertainties in estimates of dose,
-
Presentation and interpretation of results,
-
Quality assurance and quality control.
Those elements constitute the basic principles of dose reconstruction. They are summarized in Table I.C.1 and are briefly described on the following pages.7
I.C.2.1 Definition of Exposure Scenarios
As used in this report, the term exposure scenario (or scenario) refers to a set of assumptions about the conditions of exposure of an individual or group of individuals for whom a dose reconstruction is being performed. A properly defined exposure scenario incorporates two kinds of information:
-
A description of assumed locations of the individuals of concern, their activities at those locations, and the time spent at each location,
-
A description of the radiation environment at assumed locations of the individuals during the time spent at those locations.
The dose received is determined by combining information on the radiation environment with information on the locations and activities of an individual or group of individuals.
For example, consider an atomic veteran who was a member of a maneuver unit at a nuclear-weapons test at the NTS. Information about the veteran that would be needed to develop an exposure scenario includes the location of the maneuver unit at the time of detonation (the distance from ground zero), whether
TABLE I.C.1 Summary of Basic Elements of Dose Reconstruction Process
|
Basic element |
Summary description |
|
Definition of exposure scenarios |
Activities of individuals in areas where radiation exposure could occur and characteristics of radiation environment in those areas |
|
Identification of exposure pathways |
Relevant pathways of external and internal exposure |
|
Development and implementation of methods of estimating dose |
Data, assumptions, and methods of calculation used to estimate dose from relevant exposure pathways in assumed scenarios |
|
Evaluation of uncertainties in estimates of dose |
Evaluation of effects on estimated dose of uncertainties in assumed exposure scenarios and uncertainties in models and data used to estimate dose in assumed scenarios, to obtain expression of confidence in estimated dose |
|
Presentation and interpretation of results |
Documentation of assumptions and methods of estimating dose and discussion of results in context of purpose of dose reconstruction |
|
Quality assurance and quality control |
Systematic and auditable documentation of dose reconstruction process and results |
the unit was huddled in trenches at the time of detonation or standing or sitting in an unshielded position, where and for how long the unit marched or was transported after a detonation, the time spent at the objective of the maneuver or at other locations if the objective was not reached, as well as activities undertaken at the objective and whether the veteran used respiratory-protection equipment during any part of the maneuver. A description of the radiation environment could include the height of the weapon above ground at the time of detonation, the amounts of different kinds of radiations and radionuclides produced by and after the detonation, whether radiation emitted in the blast reached the location of the maneuver unit at the time of detonation, whether the maneuver unit was exposed to airborne radionuclides after detonation, whether fallout occurred at locations of the maneuver unit, whether there was fallout from previous tests at those locations, and available data on external exposure rates or concentrations of radionuclides in the air or on the ground at various locations and times after a detonation.
The committee emphasizes that no single approach to defining exposure scenarios is suitable in all cases. If activities of an atomic veteran were simple and indisputable and the radiation environment was well characterized, defining an adequate exposure scenario is usually straightforward. But defining an adequate scenario can be challenging, especially if a veteran engaged in unusual or complex activities or if important information on the veteran’s activities or the
radiation environment is lacking, is quite uncertain, or is a matter of dispute. In its review of dose reconstructions for individual atomic veterans, the committee encountered both extremes of difficulty in scenario development.
The task of defining exposure scenarios is the most important part of the dose reconstruction process for atomic veterans. An assumed exposure scenario provides the basis of an estimate of dose, so the adequacy of an estimated dose for purposes of dose reconstruction can be no better than the validity of the assumed scenario. The validity of an assumed scenario often cannot be determined by objective means alone, such as film-badge measurements of dose or a complete and indisputable record of a veteran’s activities. Rather, a considerable amount of subjective judgment is often required in defining exposure scenarios, and it is often the case that more than one scenario is plausible. Thus, it is critical that all plausible scenarios be investigated, especially when plausible alternatives would result in higher estimates of dose. Veterans themselves can often provide information that can be used to develop plausible scenarios.
I.C.2.2 Identification of Exposure Pathways
Radiation doses can be received as a result of external or internal exposure. The term external exposure refers to irradiation of the body by sources outside the body. Only radiation that can penetrate the body surface and irradiate radiosensitive tissues of the skin and deeper organs is of concern with respect to external exposure. For atomic veterans, that radiation includes neutrons and photons (gamma rays and X rays) of any energy produced in a detonation or by decay of radionuclides and higher-energy electrons (beta particles) produced in radioactive decay. Nonpenetrating radiation, such as lower-energy electrons and alpha particles produced in radioactive decay, generally is not of concern in estimating dose from external exposure. External exposure to neutrons and photons usually is assumed to result in nearly the same dose to all body organs and tissues, whereas external exposure to higher-energy electrons results in a dose only to tissues near the body surface, including the skin and lens of the eye.
The term internal exposure refers to irradiation of the body by sources inside the body. Internal exposure can occur as a result of intakes of radionuclides by inhalation, ingestion, or absorption through the skin or an open wound. In cases of internal exposure, all radiation (photons, electrons, and alpha particles) emitted by the radionuclides of concern is important and is taken into account in estimating dose. Internal exposure can result in doses that are nearly the same in all organs or tissues, as when a radionuclide is distributed throughout the body (for example, 3H, 14C, and 137Cs), or doses that are highly nonuniform and occur mainly at sites of radionuclide deposition in the body (for example, irradiation of the thyroid due to intakes of 131I, irradiation of bone surfaces and bone marrow due to intakes of 90Sr, and irradiation of the lungs, bone surfaces, bone marrow, and liver due to inhalation of plutonium).
I.C.2.2.1 Pathways of external exposure
Pathways of external exposure that could be of concern in dose reconstructions for atomic veterans include the following:
-
Direct exposure to radiation emitted in a nuclear detonation,
-
Exposure due to immersion in contaminated air,
-
Exposure due to immersion in contaminated water,
-
Exposure to radionuclides deposited on the ground or other surfaces or to radionuclides distributed in surface soil or water,
-
Exposure to radionuclides deposited on the surface of the body.
The importance of different pathways of external exposure depends on the exposure scenario. For example, external exposure to radionuclides deposited on the ground or other surfaces often is the most important pathway of external exposure at the NTS and in the Pacific.
Direct exposure to radiation (neutrons and higher-energy photons) produced in a detonation occurred only when a veteran was relatively close to ground zero and the radiation was not completely absorbed during transport from the source to the receptor location. This pathway is relevant, for example, to participants at the NTS who observed shots from trenches that were within a few kilometers of ground zero.
Exposure due to immersion in contaminated air occurred in a number of circumstances, such as: when a veteran was at a location of descending fallout; when radioactive materials that had been deposited on the ground, on surfaces of a ship, or on surfaces of equipment were resuspended in the air; or in an aircraft that flew through a contaminated atmospheric cloud. Radioactive material on a surface can be resuspended by natural processes (such as wind), by the blast wave of a detonation, or by such activities as marching or transport through an area where fallout occurred, digging trenches in a contaminated area, handling contaminated equipment, and decontaminating ships with water hoses.
Exposure due to immersion in contaminated water generally is of concern only for nuclear tests in the Pacific. This pathway is important mainly for veterans who undertook diving activities after an underwater test.
Exposure to radionuclides deposited on the ground or other surfaces or to radionuclides distributed in surface soil or water is important in a number of circumstances. At the NTS and in the Pacific, external exposure to a contaminated ground surface is important if a veteran was in an area where fallout occurred. Exposure to other contaminated surfaces occurred, for example, on ships that experienced fallout or in the handling of contaminated equipment. Exposure to radionuclides distributed in surface soil occurred, for example, when a veteran was in an area of the NTS where irradiation by neutrons from a detonation resulted in activation of the nuclei of various elements in soil. Exposure to radionuclides distributed in water occurred in some circumstances in the Pacific,
such as when a veteran spent time on a ship or in a small boat in a contaminated lagoon. This exposure pathway is different from that involving immersion in contaminated water in that the exposed person is above the body of contaminated water.
Exposure to radionuclides deposited on the surface of the body is of concern, for example, if a veteran was in an area of descending fallout or settling of resuspended material or handled contaminated soil or equipment. This pathway was especially important for maneuver troops and close-in observers at the NTS. The primary concern in cases of contamination of the body surface is irradiation of radiosensitive tissues of the skin and lens of the eye by higher-energy beta particles emitted by radionuclides.
I.C.2.2.2 Pathways of internal exposure
Inhalation and ingestion of radionuclides can occur by several pathways. In most cases of internal exposure of atomic veterans, intakes by inhalation probably were the most important. Inhalation exposure occurred, for example, when a person was in descending fallout or in a cloud of airborne radionuclides that were resuspended from a contaminated surface, such as the ground surface, surfaces of ships, or surfaces of equipment. The most likely pathway of ingestion exposure of atomic veterans involved inadvertent ingestion of contaminated material that originated in soil or on surfaces. However, ingestion may have occurred otherwise in unusual circumstances, for example, if a person consumed food or water that had been directly contaminated by fallout, or if a person on a residence island in the Pacific consumed local terrestrial foodstuffs that were contaminated by fallout or root uptake of fallout radionuclides from soil or consumed contaminated seafood obtained from local waters.
Absorption of radionuclides through the skin or an open wound probably is relatively unimportant in exposures of atomic veterans. Skin absorption would be important only if a veteran were in an atmospheric cloud that contained substantial amounts of 3H in the form of tritiated water vapor (ICRP, 1979a). Absorption through an open wound could occur if radioactive materials were deposited on the body surface.
I.C.2.3 Development and Implementation of Methods of Estimating Dose
Once an exposure scenario is defined, including the assumed locations and activities of an atomic veteran at various times and the radiation environment at those locations and times, and relevant exposure pathways are identified, the radiation dose received by the veteran by all pathways can be estimated.
Estimation of dose is based on a combination of available data and modeling. Important data that can be used to estimate dose to an atomic veteran directly include film-badge readings and measured external exposure rates at various
locations and times in the veteran’s exposure environment. Data on humans also are used to estimate dose. For example, models used to estimate dose due to inhalation on the basis of estimates of concentrations of radionuclides in air include an assumption about the breathing rate.
When data that could be used to estimate dose directly are not available, mathematical models that incorporate available information and other assumptions must be used. The extent to which models must be used depends on the particular exposure situation. All estimates of internal dose must be based on models because internal dose cannot be measured directly. The availability of reliable and complete film-badge readings can minimize the need to use models to estimate external dose from exposure to photons. However, models to describe the time and spatial dependence of external dose rates must be used whenever film-badge or other radiation survey data are unavailable or inadequate, and complex models generally must be used to estimate dose from external exposure to neutrons and higher-energy electrons (beta particles).
One simplification in dose reconstructions for atomic veterans, compared with dose reconstructions for members of the public exposed to releases from the NTS or DOE facilities, is that models of radionuclide transport in air or water are not needed. Transport of radionuclides in the environment after a detonation generally was tracked by using cloud sampling and measurements of fallout on the ground or on ships. However, models of the environmental behavior of radionuclides are needed in some cases. For example, estimates of dose to atomic veterans due to inhalation of fallout that was resuspended in the air from the ground or other surfaces must be based on models to estimate concentrations of specific radionuclides on the surface and the extent of resuspension, because radionuclide concentrations on surfaces or in air generally were not measured during periods of exposure.
The dosimetric quantity calculated in dose reconstructions generally is the biologically significant radiation dose to organs and tissues of humans. In the NTPR program, that quantity is called the dose equivalent and is expressed in rem. Dose equivalent is calculated as the average absorbed dose in an organ or tissue, given in rad, modified by a factor that represents the biological effectiveness of the type of radiation that delivers the dose. The modifying factor takes into account that for a given absorbed dose in an organ or tissue of humans, the probability that a cancer or other stochastic radiation effect will result depends on the radiation type and the absorbed dose.8 In this report, however, the biologically significant dose to organs and tissues is called the equivalent dose to conform to the terminology currently used by the International Commission on Radiological Protection (ICRP, 1991a).
I.C.2.4 Evaluation of Uncertainties in Estimates of Dose
Any estimate of dose obtained in a dose reconstruction has some uncertainty because of the variability in relevant measurements or a lack of knowledge of relevant processes or an individual’s exposure scenario. All uncertainties, including uncertainties in exposure scenarios that form the basis of estimates of dose and uncertainties in the data and models used to estimate dose, must be considered and taken into account in a dose reconstruction. The essential purpose of an uncertainty analysis is to provide a credible range within which one can be reasonably confident that the true dose lies. Without proper consideration of uncertainty, the results of a dose reconstruction cannot be regarded as credible.
There are two ways of accounting for uncertainty in a dose reconstruction. An approach that can be used in any dose reconstruction, regardless of its purpose, is to obtain a best (central) estimate of dose and quantify its uncertainty due to uncertainties in the assumptions, data, models, and parameter values used. For example, the uncertainty in an estimate of dose can be represented by a 90% confidence interval giving a range of plausible values.9 Such a confidence interval can be based on a combination of rigorous methods of statistical analysis and the use of subjective scientific judgment, depending on the quantity and quality of information used to estimate dose.
An alternative approach to addressing uncertainty that can be useful, depending on the purpose of a dose reconstruction, is to provide a credible upper bound of the dose (rather than a best estimate and confidence interval) on the basis of an argument that such a value overestimates the actual dose in almost all cases (for example, at least 95% of the time). This approach is particularly appropriate in dose reconstructions for atomic veterans because veterans are to be given the benefit of the doubt in estimating doses used to evaluate claims for compensation for radiation-related diseases (see Section I.C.3.2).
Both approaches to accounting for uncertainty have been used in dose reconstructions for atomic veterans. It is important to recognize that either can involve substantial subjective judgment (in addition to more rigorous methods of statistical analysis) depending on the importance of judgment in developing the assumptions, methods, and data used to estimate dose.
The importance of uncertainty in estimated doses to atomic veterans can depend on the magnitude of the dose. If the estimated dose is very low, the uncertainty can be large and still have no effect on a decision regarding compensation for a radiation-related disease. At higher doses, however, smaller uncertainties can be important to a decision about compensation.
A wide range of plausible estimates of uncertainty may be encountered in dose reconstructions for atomic veterans. For example, uncertainties should be relatively low in scenarios where the dose was due mainly to external exposure and a film badge was worn at all times of exposure, but they can be much higher in scenarios where a veteran might have received a high dose by inhalation of resuspended radionuclides.
I.C.2.5 Presentation and Interpretation of Results
After estimates of dose have been obtained, it is important that the results of a dose reconstruction be presented in a way that can be understood by the veteran in question and others. For example, the assumptions, data, and models used in the dose reconstruction must be clearly identified and explained, and uncertainty in the results must be addressed. Key assumptions and conclusions should be provided, and the work should be signed and dated by the analyst. The analysis must be documented in such a way that other scientists can understand and verify the calculations. Especially in the dose reconstruction program for atomic veterans, proper communication of the analysis and results to the veterans themselves is essential.
It also is important that the results of a dose reconstruction be interpreted properly by discussing the results in the context of the purpose of the analysis. For example, the interpretation of results generally would depend on whether the purpose of the dose reconstruction is to provide best estimates of the dose to a specific person, best estimates of dose to a representative person in a group, upper-bound estimates of dose to persons or groups, or assurance that the dose received by a specific person or representative person did not exceed a specified value. As discussed throughout this report, the proper interpretation of results of dose reconstructions for atomic veterans is in terms of obtaining credible upper-bound estimates of dose to individuals.
Thus, in general, presentation and interpretation of results of a dose reconstruction should provide a reasonably complete, coherent, and understandable picture of the analysis that would allow others to judge the adequacy of the dose reconstruction for its intended purpose. Knowledgeable scientists should be able to reproduce the calculations on the basis of the information documented in the dose reconstruction, and persons or groups whose doses have been estimated should be able to understand the assumptions used in the analysis, especially assumptions about exposure scenarios and exposure pathways, and the results of the analysis.
I.C.2.6 Quality Assurance and Quality Control
Use of proper quality assurance and quality control procedures is an essential aspect of all the other elements of the dose reconstruction process described
above. The essential function of quality assurance and quality control is to ensure that there is a systematic and auditable documentation of the procedures used in dose reconstructions and that the methods of analysis and the calculations themselves are free of important error. Proper documentation must be provided for all data, interpretations of data and other assumptions, and computer codes or other methods of calculation used to estimate dose. Procedures to be used in dose reconstructions and changes in the procedures, including when they occurred, must be properly documented. If complex computer codes are used, they should be verified to ensure that they do not introduce important error. External peer review is an important means of achieving quality assurance.
In general, proper quality assurance and quality control are essential to developing confidence in the dose reconstruction process and the resulting estimates of dose. The issue of quality assurance and quality control is discussed in more detail in Section IV.G.
I.C.3 Special Aspects of Dose Reconstructions for Atomic Veterans
Three other aspects of dose reconstructions for atomic veterans warrant special consideration. First, dose reconstructions have been used to evaluate claims for compensation by specific persons who incurred a disease that could have been caused by exposure to ionizing radiation during the atomic-testing program; in many cases, estimates of dose to a particular organ or tissue in which a cancer or other disease has occurred are compared with a specified dose as part of the process of deciding whether the disease was at least as likely as not to have been caused by radiation exposure (see Section III.E). Second, the claimant is to be given the benefit of the doubt in estimating dose. Third, the NTPR program has been going on for more than two decades, and there have been many advances in the science of dose reconstruction over that time. As discussed below, these considerations have important implications for the dose reconstruction process for atomic veterans.
I.C.3.1 Focus on Specific Persons
Focusing on reconstruction of doses received by specific persons can place considerable demands on the dose reconstruction process, especially with regard to defining exposure scenarios, selection of parameter values for use in models to estimate dose, and treatment of uncertainty. For example, depending on the particular exposure situation, it could be inappropriate to ascribe average exposure conditions in a participant group to a specific person in that group. In its review of dose reconstructions for individual veterans, the committee encountered a substantial number of cases that clearly involved unusual, or even unique, exposure conditions.
Another challenge in dose reconstructions for atomic veterans is that some of the models and supporting data used to estimate dose, especially in cases of intakes of radionuclides by inhalation or ingestion, represent standard assumptions that were developed for purposes of radiation protection. In radiation protection, which is concerned with controlling exposures and evaluating compliance with dose limits for workers or the public, standard models and databases used to estimate internal dose are assumed to apply to everyone, without uncertainty. However, dose reconstructions for atomic veterans focus on estimating actual doses to specific persons. It is important that uncertainties in standard models used in radiation protection be acknowledged and properly taken into account in dose reconstructions for specific veterans in the context of a compensation program.
I.C.3.2 Importance of Benefit of the Doubt
Regulations governing the NTPR program specify that the veteran will be given the benefit of the doubt in estimating dose. Specifically, as stated in 38 CFR 3.102:
When, after careful consideration of all procurable and assembled data, a reasonable doubt arises regarding service origin, the degree of disability, or any other point, such doubt will be resolved in favor of the claimant. By reasonable doubt is meant one which exists because of an approximate balance of positive and negative evidence which does not satisfactorily prove or disprove a claim. It is a substantial doubt and one within the range of probability as distinguished from pure speculation or remote possibility. It is not a means of reconciling actual conflict or a contradiction in the evidence. Mere suspicion or doubt as to the truth of any statements submitted, as distinguished from impeachment or contradiction by evidence or known facts, is not justifiable basis for denying the application of the reasonable doubt doctrine if the entire, complete record otherwise warrants invoking this doctrine. The reasonable doubt doctrine is also applicable even in the absence of official records, particularly if the basic incident allegedly arose under combat, or similarly strenuous conditions, and is consistent with the probable results of such known hardships.
Thus, if there are matters of dispute or a lack of important information about conditions of exposure, plausible assumptions that give the highest estimates of dose should be used in dose reconstructions for atomic veterans. It is not intended that doses be estimated on the basis of assumptions that are beyond reason. Rather, as stated above, assumptions should be “within the range of probability as distinguished from pure speculation or remote possibility.” Nonetheless, the need to give the veteran the benefit of the doubt can place considerable demands on the definition of exposure scenarios, the selection of parameter values used in models to estimate dose, and the methods used to account for uncertainty in estimates of dose. The demands are greater if a veteran engaged in unusual activities.
The policy on benefit of the doubt in the use of dose reconstructions to evaluate claims for compensation encourages an approach to estimating dose that focuses on obtaining credible upper bounds, rather than best estimates, of possible doses to atomic veterans. However, in attempting to provide credible upper-bound estimates of dose, uncertainties in methods and assumptions used in the analysis must be considered and evaluated, and proper justification that the estimated doses are credible upper bounds must be provided.
I.C.3.3 Conduct of Dose Reconstruction over Time
An unusual aspect of the NTPR program is that it has been going on for 25 years. This can place special demands on the dose reconstruction process with regard to consistency in the technical approach, nondiscriminatory methods of estimating dose, and implementation of changes in methods of estimating dose based on improvements in science.
Ideally, consistent approaches to developing exposure scenarios and consistent methods of estimating doses would be used in dose reconstructions for all atomic veterans. For example, if a bias toward overestimation of dose was deliberately included in some dose reconstructions (for example, on the basis of benefit of the doubt), similar biases should be applied in all cases, consistent with the available information. Likewise, consistent assumptions about models and parameter values should be used in estimating doses to different persons who have been assumed to be exposed in similar ways. It can be difficult to achieve consistency in methods of dose reconstruction when analyses are performed by different people and over an extended period during which the scientific basis of dose reconstruction has been evolving. Preparation of a detailed manual of procedures for the conduct of dose reconstructions can be an important means of achieving the desired degree of consistency among different analysts and over time.
Dose reconstructions for atomic veterans are performed for different purposes. In many cases, as noted previously, dose reconstruction is used to support a claim for compensation. In other cases, however, it is used to inform the veterans about their doses. In general, methods used to estimate dose should not differ on the basis of the purpose of dose reconstruction. An important goal of a dose reconstruction program is to foster a perception that all individuals whose doses are estimated are treated fairly and consistently.
During the 25-year existence of the NTPR program, there have been substantial improvements in the scientific foundations of dose reconstruction and in the tools used to estimate doses and evaluate uncertainties. It is important that these improvements be evaluated and incorporated into the NTPR program as appropriate. Methods of dose reconstruction for atomic veterans do not necessarily need to be changed whenever a new piece of information becomes available, but there must be a deliberate and regular effort to evaluate changes in data and
methods of dose reconstruction and to incorporate improvements in the dose reconstruction process as warranted. For example, given the increased capabilities of computers to process large amounts of data rapidly, it is reasonable to expect that the results of dose reconstructions could be presented as probability distributions or confidence intervals of dose, rather than single values, with uncertainties associated with dose reconstructions taken into account. That approach would give veterans a much clearer idea about uncertainties in their estimated doses than the current practice of emphasizing only upper-bound estimates. Peer review of methods of dose reconstruction and the existence of a detailed manual of standard operating procedures, including proper procedures for document control and updating, are important.
The NTPR program should be cognizant of new techniques for measuring or assessing radiation doses that were received by veterans many years ago. The need to rely on uncertain models is reduced to the extent that doses can be estimated on the basis of measurement. An example (see Section VI.D) that has been recognized by the NTPR program is the development of improved bioassay techniques for estimating prior intakes of plutonium. Similarly, new measurement techniques, such as electron paramagnetic resonance, can be used to estimate accumulated radiation dose in tooth enamel (for example, see Romanyukha et al., 2000, 2002). Such developments should be followed, although they may be limited in their sensitivity to the low radiation doses that were received by most atomic veterans and, thus, may provide only limited data of use in evaluating veterans’ claims for compensation.
I.D CONCERNS OF VETERANS
Veterans have expressed concerns about the atomic veterans compensation program since its beginning. Their concerns have led to hearings by Congress, independent evaluations of the program, and, as described above, studies by the National Research Council and other organizations. Believing that it is important to understand these concerns and, to the extent possible, to address them in its review of the dose reconstruction program, the committee interacted with veterans and provided an opportunity for them to raise issues for consideration. By listening to the veterans and attempting to address their concerns in this report, the committee hopes that it is providing answers to some of their questions and, more important, helping them to understand the process of dose reconstruction and its role in their compensation program.
Veterans expressed their concerns to the committee through correspondence and by participating in the committee’s open meetings. Members of the committee also attended the 2001 annual meeting of the National Association of Atomic Veterans, where a number of questions were asked about the dose reconstruction and claims process.
The following are examples of concerns expressed by the veterans to the committee:
-
The perception of an extraordinarily low rate of successful claims under the nonpresumptive regulation.
-
The validity of dose reconstruction as a basis for compensation.
-
The burden to veterans and their spouses posed by the claims and appeal process.
-
The lack of timeliness of claims resolution and responses from DTRA and VA.
-
Changes in doses assigned by the NTPR program to individual veterans as they continue to make inquiries or seek help from a legislative official.
-
Use of a low-level internal dose screen to eliminate the need for calculation of inhalation dose.
-
Failure to account properly for inhalation dose in some scenarios.
-
Neglect of possible ingestion doses in dose reconstructions.
-
Improper assumptions about scenarios of exposure and failure to consider veterans’ own accounts or accounts of companions.
That is not a comprehensive or ranked list, but several of those concerns seem to be overriding and consistent in importance. A few are discussed below, and others are discussed in more detail throughout this report.
The issue that has appeared to be of most concern to the veterans throughout our interaction during the project is the overall effectiveness of the compensation program under 38 CFR 3.311, the nonpresumptive regulation. Although that concern seemed to be somewhat peripheral to our scope, it is indirectly related because knowledge about the “accuracy” of the doses, as stated in the committee’s charge, could affect decisions about compensation. The veterans have been led to believe that over the course of the compensation program, relatively few claims have been awarded under the nonpresumptive regulation even though more than 4,000 dose reconstructions have been performed. As a consequence, there is an intense distrust and skepticism by the veterans about how dose reconstructions are being performed, and about whether accurate dose reconstruction is even possible, given the lack of historical data and the period of time since exposures occurred. The committee hopes that some of the information provided in this report will be helpful in addressing that issue.
Veterans are also concerned about some of the elements of the dose reconstruction process, including assumptions about scenarios of exposure, improper accounting of internal doses, and the use of a “low-level internal dose screen” that they believe improperly eliminates the need to estimate inhalation doses to some veterans. The concept and use of an internal dose screen is a good example of an issue to which the committee devoted considerable attention in an effort to provide clarification to the veterans. Although DTRA has consistently stated that it does not use an internal dose screen to eliminate the need to estimate inhalation
doses, the issue continues to cause considerable confusion among the atomic veterans, which the committee hopes to alleviate.
Some of the concerns expressed by the atomic veterans are beyond the scope of this study, but the committee has endeavored to answer as many of them as possible in the report and appreciates the veterans’ willingness to express their concerns to us throughout the project.





























