
A
Methods
This appendix describes the methods used by the committee to collect information for its review, assessment, and consideration. Four types of data collection were undertaken: a literature review, invited presentations, a survey of selected medical schools, and a modified Delphi process for prioritizing topics (see Chapter 3). Each activity is described below.
LITERATURE REVIEW
The committee’s initial literature search (Figure A-1) concentrated on journals found in the MEDLINE database. A second, expanded literature search (Figure A-2) included multiple databases. As noted throughout this report, these searches yielded a relatively small number of articles specific to the inclusion of the behavioral and social sciences in medical education. Broad search terms were used to cast as wide a net as possible. The articles obtained by the search terms were reviewed for their relevance to the committee’s charge. To be viewed as relevant for this report, an article had to be in English and meet one of the following criteria: (1) describe or review medical school curriculum content identified as relevant to the behavioral and social sciences; (2) describe or review medical school curricula or curriculum change; or (3) include a discussion of undergraduate medical school education.
Systematic reviews or descriptions of behavioral and social science content in undergraduate medical school curricula were not found. Articles describing the rationale or goals of a behavioral and social science program, including examples of course content, were obtained. However, these articles did not provide enough information to allow a review of the approaches that have been or are successful
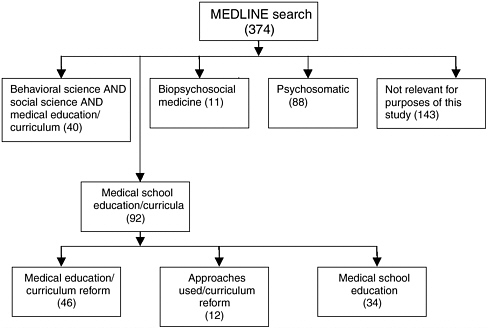
FIGURE A-1 MEDLINE search results. The numbers in parentheses indicate the number of articles found in each category; some articles fall under more than one category. The search was limited by language (English), species (human), and year (1970–2003).
in teaching the behavioral and social sciences in medical school or an evaluation of the effectiveness of current programs. The majority of the articles describing or reviewing curriculum change were not specific to the behavioral and social sciences, but were deemed to address overarching principles and strategies applicable to these disciplines.
INVITED PRESENTATIONS
The committee held multiple open sessions at which invited speakers representing interested organizations, associations, and medical schools provided information. During the sessions, the committee was able to discuss the information presented and gain additional insight from different perspectives regarding the inclusion of the behavioral and social sciences in medical school curricula. A list of the associations, organizations, medical schools, and respective institutions represented by the invited speakers appears in Box A-1.
MEDICAL SCHOOL SURVEY
To obtain additional information on the current status of behavioral and social science content in medical school curricula, the committee surveyed a lim-
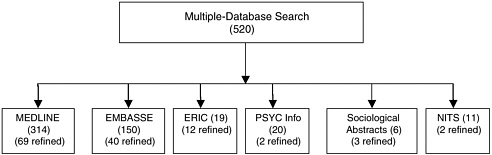
FIGURE A-2 Results of electronic multiple-database search. The numbers in parentheses indicate the number of articles found in each database. The second number in parentheses (refined) indicates the number of articles that remained after nonrelevant articles had been eliminated. The following search terms were used: Medical, Faculty, Education, Undergraduate, Behavioral Sciences, and Social Sciences. Articles with the following terms as a primary focus were eliminated from the search to create the refined results: Distance Education, Informatics, Forensic/Autopsy, Residency, Health Professions other than physician, Medical Subspecialties, Career Planning, Nuclear Medicine, Master of Business Administration, and Bioterrorism. The search was limited by language (English) and year (1995–2003).
ited number of medical schools using a two-step data collection method. Four schools were selected and surveyed based on initial information that indicated their behavioral and social science program could serve as an example of current approaches being used. The survey consisted of two parts: a brief questionnaire completed by an official of the medical school, followed by a telephone interview with that individual. The four schools surveyed were Ohio State University College of Medicine; University of California, San Francisco, School of Medicine; University of Rochester Medical Center; and University of North Carolina School of Medicine.
MODIFIED DELPHI PROCESS
The committee used a modified Delphi process to establish the priority topics delineated in Chapter 3. The initial step was to establish a list of all possible topics in the behavioral and social sciences that could be included in a curriculum for medical students (see Box A-2). The topics on this list varied in subject area, specificity of material, and level of relevance to undergraduate medical school education. Background materials that aided in establishing the original list encompassed (1) relevant, evidence-based articles and reports in the literature; (2) presentations to the committee by content experts and medical school representatives; (3) literature and other material from the Association of American Medical Colleges and the Liaison Committee on Medical Education; (4) considerations related to the health of the public, driven mainly by root causes of morbidity and
|
BOX A-1 Association of American Medical Colleges Association for the Behavioral Sciences and Medical Education Brody School of Medicine, East Carolina University Liaison Committee on Medical Education National Board of Medical Examiners Society of Behavioral Medicine The Society of Teachers of Family Medicine University of California, San Francisco University of Rochester Medical Center |
mortality; and (5) the gap between what is known and what is actually done in practice.
The committee’s collective and individual experience in curriculum development and reform in the behavioral and social sciences largely directed the prioritization of the topics on the original list. The rating scale used to prioritize the topics ranged from 0 to 3, with 0 being the lowest score, and included “U” (for unknown) as an option for rating a topic if the level of priority was unknown or could not be determined by a committee member. Each topic was then assigned high, low, or medium priority based on its mean score and standard deviation.
Given the number of topics with large standard deviations, it was determined that a second round of ratings was needed to clarify the appropriate rating for each topic. For the second round of ratings, several decisions were made:
-
Topics ranked as low or with a mean score equal to or less than 1 were removed from the list.
-
Topics added by a committee member were placed as the first item in the appropriate category or subcategory.
-
Committee members were given the opportunity to provide a rationale or clarification for their ratings.
The results of this second round provided additional clarification of topics, and the variance in standard deviations was reduced.
The next step in developing the list was to apply the following set of criteria:
-
Is the content of this topic included in or overlapping with other topics on the list?
-
Is undergraduate medical school the most appropriate level for this topic to be taught?
-
Is the topic of limited value for general physician education?
-
Is the topic part of a core behavioral or social science curriculum?
Based on a combination of the answers to the above questions, mean scores, standard deviations, and the expert opinion of the committee, topics were removed from the list and/or reassigned high, medium, or low priority. The committee reviewed a third ranked list and performed a final rating, this time using a 0 to 5 scale similar to the one discussed previously. This list was refined and finalized using the collective and individual expertise of the committee members in medical school curriculum development and reform in the behavioral and social sciences. The final list of topics is in Chapter 3, Table 3-1. In this list, the 11 items ranked top and the 9 items ranked high were combined into one high-priority group.
|
BOX A-2 Biological Domain Psychological Domain Social Domain Behavioral Domain Economic Domain 1.0 Biological Domain 1.1 Genetic contributions to behavior 1.1.1 Concepts in behavioral genetics 1.1.2 Assessment of genetic contributions to personality and behavior 1.1.3 Principles and strategies of genetic counseling 1.2 Mind–body interactions in health and disease 1.2.1 Brain/behavior/central nervous system/autonomic nervous system 1.2.2 Psychoendocrinology 1.2.3 Psychoneuroimmunology 1.2.4 Pathobiology 1.2.5 Biological basis of illness behavior 1.3 Mind–body interactions in specific disease states 1.3.1 Cardiovascular diseases 1.3.2 Gastrointestinal diseases 1.3.3 HIV/AIDS 1.3.4 Neurological disorders, e.g. Parkinson’s disease, frontal tumors, chronic pain 1.3.5 Mood disorders 1.3.6 Substance abuse 1.3.7 Sleep disorders 1.3.8 Eating disorders 1.3.9 Psychosis 2.0 Psychological Domain 2.1 Psychological models of human behavior 2.1.1 Cognitive psychology: thinking habits, core schemas (Beck), focus of control (Roter), cognitive dissonance (Festinger), “transtheoretical” psychology of change (Prochaska) 2.1.2 Social psychology: roles and expectations, attributions, choice |
|
2.1.3 Dynamic psychology: unconscious conflict, ego defenses 2.1.4 Social–cognitive models: self-efficacy, coping models (Bandura) 2.1.5 Systems theory: family dynamics, functions of the sick member 2.1.6 Humanistic psychology: empathy, warmth, genuineness (Rogers) 2.1.7 Personality development and personality types (Shapiro, Diagnostic and Statistical Manual [DSM]-IV) 2.1.8 Normal development: birth through old age 2.2 The psychology of patients 2.2.1 Expectations, biases, and assumptions about the nature of illness and the roles of doctor and patient: mind–body dualism 2.2.2 The psychology of health risk behaviors: food, tobacco, alcohol and substance abuse, risky sex, risky driving, risky sports behaviors 2.2.3 Normal illness psychology: fear and anxiety, vulnerability, appropriate dependency, humiliation, anger, sadness, and loss 2.2.4 Abnormal illness psychology: denial, pathological dependency, depression, somatization, hypochondriasis 2.2.5 The psychology of somatoform disorders (e.g., lower back pain, irritable bowel syndrome, chronic fatigue syndrome) 2.2.6 The psychology of chronic pain 2.2.7 Psychological issues in chronic diseases and disabilities 2.2.8 Psychopathology—DSM-IV disorders 2.3 The psychology of doctors 2.3.1 Expectations, biases, and assumptions about the nature of illness and the roles of doctor and patient: mind–body dualism 2.3.2 Knowledge availability: memory structures, pattern recognition 2.3.3 The processes of clinical reasoning: reflective and analytic versus gestalt and associative reasoning (“knee-jerk reactions”); hypothetical deductive reasoning, etc. 2.3.4 Shared decision making (clinician–clinician and clinician–patient) |
|
2.3.5 The interpretation of evidence 2.3.5.1 Unwarranted variations in health care delivery (Wennberg) 2.3.6 Effects of informatics and other decision support systems 2.3.7 Effects of continuing medical education and recertification on clinical decision making 2.3.8 Dangers of stress and burnout: need for self-awareness, self-care 2.4 The psychology of doctor–patient relationships 2.4.1 Doctor-centered: paternalistic, sole expert, etc. 2.4.2 Patient-centered: activated patient, patient as expert 2.4.3 Relationship-centered 3.0 Social Domain 3.1 Basic concepts 3.1.1 Social stresses and supports as determinants of health 3.1.2 The sick role as a social construct 3.1.3 The professional role and ethics as social constructs 3.1.4 Health care policies 3.1.5 Clinical medicine and public health 3.1.6 High-risk versus population-based approaches 3.1.7 Community health 3.1.8 Levels of organization in health care 3.1.9 Occupational health 3.1.10 Evaluating individual context (e.g., available tangible support); capacity for self-care, making medical decisions, and independent living 3.2 Multicultural medicine 3.2.1 Cultural competence in diagnosis 3.2.2 Cultural competence in patient management 3.2.3 Cultural issues in patient–physician interactions 3.2.4 Folk medicine, alternative medicine, and biomedical treatment 3.3 Social inequalities in health 3.3.1 Social inequalities in health care 3.3.2 Poverty/homelessness 3.3.3 Rural/urban issues and culture |
|
3.4 Gender issues in health care 3.5 Sexual orientation issues in health care 3.6 Domestic abuse, violence 3.7 Social constraints on physician behavior 3.7.1 Health maintenance organization requirements 3.7.2 Insurance carriers 3.7.3 Legal risk and malpractice insurance 3.7.4 Medical jurisprudence 3.7.5 Confidentiality issues 3.8 Social influences on physician behavior 3.8.1 Social accountability and responsibility 3.8.2 Professional norms for referrals, case management, and follow-up 3.8.3 Culture of biomedicine, including cultures of training environments 3.8.4 Medical humanities 3.9 Social change 3.9.1 Communication behavior change (McGuire) 3.9.2 Diffusion of innovation (Rogers) 3.9.3 Social marketing 3.9.4 Social change theories 3.9.5 Economic incentive theories 3.9.6 Public policy and advocacy 3.10 Medical practice organization to ensure optimal care delivery 3.11 Effective use of community resources to enhance care 4.0 Behavioral Domain 4.1 Principles of behavior management: accurate assessment and goal setting, contingent reinforcement and stimulus conditioning 4.2 Maladaptive behavior patterns of patients 4.2.1 Health risk behaviors: abuse of alcohol, nicotine, illegal drugs, legal drugs, unhealthy foods: over- and undereating; risk taking in sexual activities, sports, and driving: deliberate self-harm and self-mutilation; fictitious illness (Munchausen syndrome and malingering) |
|
4.2.2 Maladaptive help-seeking behaviors: high-frequency attendance; nonadherence, including appointment nonattendance; demanding or critical behavior; flattering or seductive behavior; dependent behavior 4.3 Maladaptive behavior patterns of doctors 4.3.1 Poor communication skills: Inattentive listening or failure to check and clarify diagnostic data, failure to elicit psychosocial data, failure to demonstrate empathy and respect or to promote partnership, failure to explore patient’s views about diagnosis and treatment, failure to give adequate explanations of diagnosis and treatment 4.3.2 Lapses in professional role behavior: poor timekeeping, excess formality or informality, failure to maintain professional boundaries in relating to patients, failure to maintain updated knowledge and skills, inadequate attention to psychosocial/behavioral and somatoform problems 4.4 Communication skills for doctors 4.4.1 Basic concepts: process versus content, structure versus function, skills versus attitudes continued 4.4.2 Skills for building a therapeutic relationship, e.g., empathy, respect, support 4.4.3 Skills for eliciting data for a five-domain assessment, e.g., open questions, active listening, checking and clarifying 4.4.4 Skills for educating, advising, and promoting behavior change: e.g., creating links with patient’s knowledge and experience 4.4.5 Advanced communication competencies; giving bad news; dealing with patients’ and families’ anger, diagnosing and counseling for obesity, alcoholism, smoking, substance abuse, risky sexual behaviors, domestic abuse, depression, etc. 5.0 Economic Domain 5.1 Overview of the U.S. health care system 5.1.1 Public insurance 5.1.2 Employer provision of health insurance 5.1.3 Insurance models 5.1.4 Hospital markets |
|
5.2 Patient behavior 5.2.1 Risk 5.2.2 Health production 5.2.3 Problems of asymmetric information between doctor and patient 5.3 Health insurance 5.3.1 Demand for health insurance 5.3.2 Welfare loss or excess insurance (moral hazard) 5.3.3 Employer-provided health insurance and job lock 5.4 Provider behavior 5.4.1 Physician-induced demand 5.4.2 Hospital competition 5.5 Trade-offs among efficiency, equity, and selection 5.5.1 Prospective payment 5.5.2 Fee-for-service payment 5.5.3 Risk selection in health plans 5.6 Quantitative methods in health economics 5.6.1 Prediction versus causation in health economics 5.6.2 Randomized controlled trials and the causation problem 5.6.3 Outcomes analyses (natural experiments) 5.7 Health policy 5.7.1 The problem of the uninsured and public insurance crowd-out effects 5.7.2 Mandated health insurance benefits and employment effects 5.7.3 Hospital competition and medical arms race 5.7.4 Racial and educational disparities in health care 5.7.5 Are medical care prices really rising? 5.7.6 Quality report cards and consumer choice 5.7.7 Prescription drug benefits and costs 5.7.8 Direct-to-consumer advertising of pharmaceuticals 5.7.9 Community rating and adverse selection 5.7.10 Price controls in insurance markets |
QUESTIONNAIRE SENT TO MEDICAL SCHOOLS
-
At your school, the primary strategy for teaching behavioral and social science material is: primarily: (Please circle the appropriate letter)
-
Integrated as a content theme across several course in the curricula. Taught as a content theme in more than two courses in the curricula
-
Concentrated in a few courses.
-
-
Please complete the chart below.
|
Please indicate if this information is taught by checking yes or no |
YES |
NO |
Title of course(s) that includes information |
Department(s) responsible for teaching behavioral and social science content |
Circle Year Taught |
Teaching method* (circle all that apply) |
|
Communication Skills |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Community Health |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Cultural Diversity |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
End of Life Care |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Epidemiology |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Family/Domestic Violence |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Please indicate if this information is taught by checking yes or no |
YES |
NO |
Title of course(s) that includes information |
Department(s) responsible for teaching behavioral and social science content |
Circle Year Taught |
Teaching method* (circle all that apply) |
|
Health Care Quality Improvement |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Health Care Systems |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Health Literacy |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Human Development/ Life Cycle |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Medical Social Economics |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Pain Management |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Palliative Care |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Please indicate if this information is taught by checking yes or no |
YES |
NO |
Title of course(s) that includes information |
Department(s) responsible for teaching behavioral and social science content |
Circle Year Taught |
Teaching method* (circle all that apply) |
|
Patient Health Education |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Population based Medicine |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Prevention and Health Maintenance |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
Substance Abuse |
|
|
|
|
1 2 3 4 |
PBL SG L U O |
|
*L = lecture, PBL = problem based learning, SG = small-group, U = unknown, O = other (describe). |
||||||
-
Does your school provide formal faculty development in behavioral and social science content for participation in these courses? (Circle the appropriate letter.)
-
Yes
-
No
-
-
Is there a faculty or staff position that is principally responsible for faculty development? (Circle the appropriate letter.)
-
Yes, please provide the position title __________________
-
No
-
-
What activities are part of your formal faculty development program? (Circle all that apply.)
-
Small group discussions
-
Demonstrating/teaching techniques of problem-based learning
-
Examples of incorporating behavioral and social science into clinical exam
-
-
Career development awards for behavioral and social science
-
Formal didactic sessions teaching faculty behavioral and social science material
-
Other _____________________________________________
-
None
-
What rationale, if any, was stated as the primary reason for including this behavioral and social sciences content in the curriculum? (Circle all that apply.)
-
Meets licensing or accreditation requirement(s)
-
Better prepare medical students to care for patients
-
Communicates belief in multilevel approach to disease
-
Supports mission of the school
-
Meets societal expectations
-
Other ___________________________________________
-
No formal rationale explicitly stated
-
-
There are several other topics of relevance to your behavioral/social science curriculum we would like to explore with a key, knowledgeable person in a telephone appointment of 15-20 minutes’ length. Whom should we contact for this appointment and conversation?
Name __________________________________
Telephone number ________________________
E-mail address ___________________________
THANK YOU
















