
10
Health Care
Racial and ethnic minorities may face challenges in having access to medical care in the United States. When they receive it, their care may not be equivalent to that for other groups. Why this is so, however, is a complex issue involving not only possible differences in ability to pay and provider behavior, but also in such factors as patient preferences, differential treatment by providers, and geographical variability.
INSURANCE COVERAGE
Blacks, Hispanics, and some Asian populations, when compared with whites, appear to have lower levels of health insurance coverage, with Hispanics facing greater barriers to health insurance than any other group (Institute of Medicine, 2002). However, Hispanics and Asians are considerably heterogeneous in insurance coverage, as Table 10-1 shows for the adult population under 65 (Collins et al., 2002; Doty and Ives, 2002; Hughes 2002). Uninsured rates are much higher for Mexicans and Central Americans than for Puerto Ricans. Among Asians, Chinese, Japanese, Filipinos, and Indians have uninsured rates that are comparable to or lower than those of whites, while Koreans and Vietnamese have higher uninsured rates than blacks.
Blacks and Hispanics are less likely to have insurance coverage from a private employer, whether directly or through a spouse, and more likely to have public health insurance coverage than whites (Blendon et al., 1989; Hogue et al., 2000; National Institutes of Health, 1998). Blacks and His-
TABLE 10-1 Health Insurance Coverage for U.S. Adults Aged 18-64, 2001
|
|
Percent Uninsured |
|
|
Population |
Currently |
In Past Year |
|
Total United States |
16 |
24 |
|
White |
12 |
20 |
|
Black |
22 |
30 |
|
Hispanic |
35 |
46 |
|
Mexican |
39 |
49 |
|
Central American |
47 |
55 |
|
Puerto Rican |
16 |
35 |
|
Asian |
14 |
21 |
|
Chinese |
12 |
16 |
|
Korean |
52 |
55 |
|
Vietnamese |
32 |
37 |
|
Filipino |
6 |
15 |
|
Indian |
13 |
18 |
|
Japanese |
1 |
4 |
|
SOURCES: Collins et al. (2002); Doty and Ives (2002); Hughes (2002). Data are from the Commonwealth Fund 2001 Health Care Quality Survey. |
||
panics are also more likely than whites to receive care in nonoptimal organizational settings (such as emergency rooms) and to lack continuity in health care. Analyses of racial and ethnic differences in access to and the use of health services between 1977 and 1996 show that the black-white gap has not narrowed over time, and the gap between Hispanics and whites has widened (Weinick et al., 2000). Moreover, this study found that, even if income and health insurance coverage were equal, racial and ethnic differences in having a usual source of care and in receiving ambulatory care in the previous year would not have been eliminated, because one-half to three-quarters of the differences on these indicators were not accounted for by income and insurance coverage.
In 1965, the Medicare program was established to reduce financial barriers to hospital and physician services for persons aged 65 and older. To participate in this program, hospitals had to comply with Title VI of the Civil Rights Act of 1964, which requires that no one be excluded from federal benefits based on race, color, or national origin. This requirement played a large role in desegregating hospitals (Quadagno, 2000).
Medicare has indeed improved the situation for older adults. For instance, Decker and Rapaport (2002) show that turning 65 increases the chances of having a mammogram among black women, particularly uneducated black women. However, there is also evidence that racial differences remain among older adults in access to health services (Gornick, 2000).
TABLE 10-2 Health Care Coverage for Persons 65 Years of Age and Over, 1998 (in percent)
|
Insurance Type |
White |
Black |
Hispanic |
|
Private insurance |
72.3 |
40.5 |
29.1 |
|
Private, work-based |
38.8 |
27.6 |
17.8 |
|
Medicaid |
5.4 |
18.0 |
27.2 |
|
Medicare only |
20.9 |
37.9 |
38.4 |
|
SOURCE: Data from National Center for Health Statistics (2001). |
|||
Table 10-2 shows the level of health care coverage for black, white, and Hispanic older adults (National Center for Health Statistics, 2001). Almost all of these persons have Medicare. However, in comparison with whites, black and Hispanic older adults are considerably less likely to have private insurance and more likely to receive Medicaid or to have Medicare as their only insurance.
The limitations of Medicare create economic challenges for blacks and Hispanics. Medicare does not cover such medical needs as prescription drugs, dental care, and long-term care, and it imposes various out-of-pocket medical expenses: an annual deductible for some care, copayments on physician charges, and payment for one day of inpatient care. These expenses may represent a substantial burden for low-income older adults, and minorities are more affected because of lower household incomes. In 1996, two-thirds of white Medicare beneficiaries had incomes of less than $25,000; 90 percent of black and Hispanic beneficiaries had incomes this low (Gornick, 2000). Other data show that black and Hispanic older adults have higher rates of poverty than their white counterparts, as do Asians and American Indians and Alaska Natives (Williams and Wilson, 2001).
Many older adults reduce their out-of-pocket expenses by purchasing supplemental private insurance, but black and Hispanic older adults are a little more than twice as likely as whites not to do so (Wallace et al., 1998). Not surprisingly, although black Medicare beneficiaries report higher levels of morbidity than their white counterparts, they report lower levels of office visits and more inpatient, emergency room, and nursing home visits (Gornick, 2000). In comparison with whites, black beneficiaries also have markedly fewer visits to specialists, and they receive such diagnostic services as mammography and sigmoidoscopy much less often (Gornick, 2000). For some older persons with low incomes and limited assets, Medicaid can cover much of their out-of-pocket medical expenses. However, only about 11 percent of older Medicare beneficiaries also receive Medicaid; these dual eligibles are more likely to be in poor health and over age 85 than other Medicare beneficiaries (Feder et al., 2001).
The situation with regards to American Indians and Alaska Natives is somewhat unique because of the existence of the Indian Health Service (IHS), which operates its own network of inpatient and ambulatory care facilities. While insurance coverage is an issue—24 percent of American Indians do not have health insurance (Brown et al., 2000)—it does not factor into matters of access to care in the same manner as for other subpopulations. The tripartite system of the IHS, tribally operated clinics, and urban Indian clinics represent a unique ecology within which American Indians seek help for physical, mental, alcohol, and drug problems. This is particularly relevant when discussing health care challenges for American Indian elderly since the emphasis of the IHS system is on acute rather than chronic health problems (Baldridge, 2001). Although the IHS is intended, legally, to be a residual provider, a large fraction of the IHS-eligible population depends on it (Cunningham, 1996).
QUALITY OF CARE
Research reveals systematic racial differences in the kind and quality of medical care received by Medicare beneficiaries (Escarce et al., 1993; McBean and Gornick, 1994). In 1992, black Medicare beneficiaries were less likely than their white counterparts to receive any of the 16 most commonly performed hospital procedures (McBean and Gornick, 1994). The differences were largest for referral-sensitive procedures. The Medicare files showed only four nonelective procedures that black Medicare beneficiaries received more frequently than whites—all procedures (such as the amputation of a lower limb and the removal of both testes) that reflect delayed diagnosis or initial failure in the management of chronic disease. Since a greater percentage of black than white Medicare beneficiaries make out-of-pocket payments for deductibles and copayments (McBean and Gornick, 1994), this burden could contribute to less use of ambulatory medical care and to the postponement or avoidance of treatment.
Contrasts among different groups are evident if one focuses on a few procedures that alleviate some major sources of morbidity and mortality, procedures supported by strong scientific evidence and practitioner consensus. Jencks et al. (2000) identified 24 such measures that they labeled measures of the quality of care for Medicare beneficiaries, and 21 of these have been compared across racial and ethnic groups (Hebb et al., 2003), including such inpatient measures as warfarin for patients with atrial fibrillation and such outpatient measures as mammograms at least every 2 years. Receipt of appropriate treatment by each racial or ethnic group is compared with the percentage receiving appropriate treatment overall in Figure 10-1. Racial and ethnic minorities appear to be at some disadvantage, particularly for outpatient rather than inpatient procedures. Hispanics
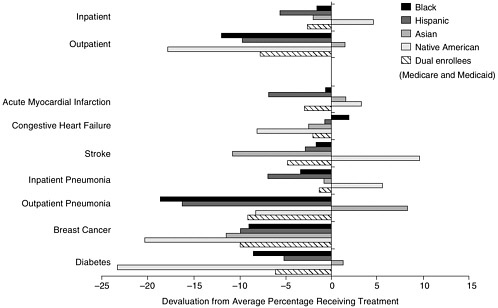
and American Indians and Alaska Natives, overall, may receive care that is as inadequate as that for blacks, though because of small numbers and problems with racial and ethnic identification, the figures must be treated with caution. People enrolled in both Medicare and Medicaid (of any racial or ethnic group) also receive less adequate care than average, suggesting a socioeconomic dimension to poor care. However, their disadvantage is sometimes smaller than that of particular racial and ethnic groups.
Such differences in the receipt of medical procedures are consistent with a larger literature, generally for earlier years, that finds systematic racial and ethnic differences in the receipt of a broad spectrum of therapeutic interventions (Geiger, 2002; Institute of Medicine, 2002; Mayberry et al., 2000). Blacks and sometimes other minorities are less likely to receive a diverse range of procedures, ranging from high-technology interventions to basic diagnostic and treatment procedures, and they experience poorer quality medical care than whites.
Differences in patient preferences and inappropriate use by whites of some procedures may play a role in the differences. For instance, Schneider et al. (2001) show that the black-white difference in angioplasty can be explained by inappropriate or at least questionable use of the procedure for whites. However, they find that this explanation does not fully account for differences in bypass surgery. The pattern of differences between blacks and whites appears robust even when such factors are considered, and it persists in studies that adjust for differences in health insurance, socioeconomic status, stage and severity of disease, comorbidity, and the type of medical facility (Institute of Medicine, 2002).
Weighed against such evidence is one recent study of a nationwide sample of almost 30,000 Medicare patients hospitalized with heart failure in 1998 and 1999 (Rathore et al., 2003). Blacks were slightly more likely than whites to receive appropriate treatment (ACE inhibitors and measurement of left ventricular ejection fraction). They were more likely to be readmitted but had lower mortality rates up to a year after hospitalization. None of these differences, however, was significant after controlling for patient medical history and other patient, physician, and hospital characteristics. This study, drawing on the same database as Hebb et al. (2003) and reaching essentially similar conclusions in the area of treatment of congestive heart failure (see Figure 10-1), shows that even blacks, despite falling short of standard treatment more often than others, are not necessarily disadvantaged in every treatment area.
Some differences in quality of care may reflect the particular institutions and health care providers on which minorities depend. Regardless of insurance coverage, blacks and Hispanics are almost twice as likely as whites to receive care from a hospital-based provider (Institute of Medicine, 2002). In particular, they are almost 1.6 times more likely than whites to be
treated at safety-net urban hospitals. Some evidence also suggests that minority patients are more likely than whites to be treated by less proficient physicians (Mukamel et al., 2000).
GEOGRAPHIC AND INSTITUTIONAL VARIATION
One factor that needs to be more consistently taken into account in studying racial and ethnic differences is the role of geography or residential area. Access to high-quality care varies considerably by area—by state, between rural and urban areas, as well as across smaller communities (Waidmann and Rajan, 2000; Wennberg and Cooper, 1999). Since racial and ethnic groups are unevenly distributed across communities, geographic variation in health care has the potential to explain some health care differences. For instance, states with large proportions of blacks tend to provide less appropriate treatment to all myocardial infarction patients, whether black or not, than states with smaller proportions of blacks (Chandra and Skinner, 2004).
The relationship between geographic variation and racial and ethnic differences in health care is complex. Some geographic variation may be due to racial factors related to residential segregation by race. But some variation in care is clearly not geographic, as when variations exist within geographic areas. Several studies have found racial and ethnic differences in care in a single facility (e.g., Baker et al., 1996; Chung et al., 1995; Lowe et al., 2001; Moore et al., 1994; Ng et al., 1996; Peterson et al., 1997; Todd et al., 1993, 2000); a single geographic location (Herholz et al., 1996; Ramsey et al., 1997; Segal et al., 1996); and, in the case of cardiovascular disease, even after a broad range of hospital characteristics are considered (Geiger, 2002).
Health care can also vary within health systems, though some studies show similar treatment for different racial groups. In the Veterans Administration health system, for instance (where differences in insurance coverage are minimized), black-white differences do not appear for the treatment of colorectal cancer (Dominitz et al., 1998) but have been shown in the treatment of heart disease (Oddone et al., 1998; Peterson et al., 1994; Sedlis et al., 1997; Whittle et al., 1993), gall-bladder disease (Arozullah et al., 1999), and mental health (Kales et al., 2000). In Department of Defense medical facilities, no black-white differences were found in the treatment of prostate cancer (Optenberg et al., 1995) or cervical cancer (Farley et al., 2001). Similarly, no differences were found in treatment of acute myocardial infarction through catheterization and revascularization procedures, but whites were more likely than minorities to be considered for future catheterization (Taylor et al., 1997).
To produce overall differences in care, the choice of hospitals or clinics that different groups attend and variations in treatment within those institutions could reinforce each other, or cancel each other out, or one or another factor could be more important. An example of the first possibility is one study of inadequate pain management, which found that all patients treated in settings where the patient population was primarily black or Hispanic were more likely to receive inadequate analgesia than those treated in settings where the patient population was primarily white (Cleeland et al., 1997). In addition, minority patients were more likely to be undermedicated for pain than white patients and more likely to have the severity of their pain underestimated by physicians. In contrast, in a five-state study, Kahn et al. (1994) found that blacks received poorer care in acute care hospitals than whites in the same hospitals, but because more blacks in the study were seen at higher-quality urban teaching hospitals, their overall quality of care was no worse. Finally, focusing on acute myocardial infarction, Skinner et al. (2003) found that, nationwide, blacks received care at lower-quality hospitals, where they tended to make up a larger proportion of the patients. Within groups of hospitals with different proportions of black admissions, however, white patients actually received poorer care than blacks, as reflected in 30-day mortality rates adjusted for various factors.
STEREOTYPING BY PROVIDERS
Some differences in medical care may be due to stereotypes of different groups held by health care providers. The authors of Unequal Treatment (Institute of Medicine, 2002) argue that unconscious or unthinking discrimination based on negative stereotypes, even in the absence of conscious prejudice, may contribute to systematic bias in care.
This argument is based on a chain of reasoning. Stereotypes are common in American society for various racial and ethnic groups. National data show that whites view blacks, Hispanics, and Asians more negatively than they view themselves, with perceptions of blacks being the most unfavorable and perceptions of Hispanics being substantially more negative than perceptions of Asians. For instance, 29 percent of whites agree with the statement that most blacks are unintelligent, while 6 percent of whites say the same of most whites. Similarly, many more whites say that most blacks are prone to violence (51 percent) than those who say the same about most whites (16 percent) (Davis and Smith, 1990; Williams, 2001b). Such stereotypes can be activated, and affect behavior, under conditions of time pressure, when quick judgments must be made on complex tasks, with cognitive overload and in the presence of such emotions as anger and
anxiety (van Ryn, 2002). In the typical health care encounter, some of these conditions are present, particularly cognitive complexity and time pressure.
The possibility that some health care providers may hold particular stereotypes is suggested by a few studies in which physicians were found to view their black patients more negatively than white patients (Finucane and Carrese, 1990; van Ryn and Burke, 2000). For instance, van Ryn and Burke (2000) found that—.even after adjusting for patient age, sex, socioeconomic status, sickness or frailty and overall health, and patient availability of social support—physicians viewed black patients, compared with whites, as less kind, congenial, intelligent, and educated, less likely to adhere to medical advice, and more likely to lack social support and to abuse alcohol and drugs. Experimental studies of physicians (Schulman et al., 1999; Weisse et al., 2001) and medical students (Rathore et al., 2000) provide evidence that the experimental manipulation of hypothetical patients’ characteristics such as race can lead to variations in provider perceptions.
But do stereotypes actually affect patient care? There is little evidence on this issue, though one may hypothesize various possibilities. For instance, a health care provider may interpret symptoms in line with beliefs about group differences. These beliefs might be based on generalizations from clinical experience (Satel, 2000, 2001-2002), or a provider may also select treatments based on stereotypical assumptions about patient behavior. Some research tackles this latter possibility. A national sample of AIDS care physicians predicted that, among hypothetical patients, black men would be less likely to adhere to antiretroviral therapy—a generalization that may be right for some therapies but not others (see below). Since potential adherence to therapy is a factor in decisions to start treatment, the inference might be drawn that black men would be less likely to receive such care, but this potential effect of stereotypes was not actually demonstrated (Bogart et al., 2001). Somewhat similarly, van Ryn et al. (1999; cited in van Ryn and Fu, 2003) found that physicians rated black patients, in comparison with white patients, as more likely to be lacking in social support and less likely to participate in cardiac rehabilitation. The likelihood of such participation is a factor in recommending revascularization, but the researchers did not link any difference in recommendations to the stereotype.
Whether medical decisions are actually affected by stereotypes is therefore not known. It would be useful to determine how often stereotypes are activated, in what circumstances, and what medical decisions are indeed affected. In principle, stereotypes would not be a problem if treatment decisions were entirely individualized (as suggested earlier, in the genetics section, as a long-term goal). However, negative stereotypes could still make the provider-patient interaction uncomfortable, which could hamper such individualization by restricting the full exchange of information. Such processes may well be important in particular individual cases but their
overall contribution to less appropriate care for minorities, or to explaining racial and ethnic differences in health in later life, remains uncertain.
PATIENT BEHAVIOR
Differences in patient self-care—a behavior about which stereotypes may exist—are themselves unconfirmed. Patient self-care covers behavior ranging from seeking health care to compliance with prescribed therapies. Compliance with complicated new therapies, such as those to control insulin-dependent diabetes and for HIV, has been shown to be better among those, including older adults, with more education. However, with education controlled, neither blacks nor Hispanics differ significantly from whites in these self-maintenance behaviors (Goldman and Smith, 2002). But other studies have documented differences by race. For instance, persistence with statin therapy among older patients—which tends to decline over time and is also related to socioeconomic status—declines more, regardless of status, among blacks and other nonwhite patients than in white patients. In fact, black subjects had 2.7 times the odds of suboptimal persistence with statin therapy compared with whites, the racial difference being greater than that on any other predictor analyzed (Benner et al., 2002).
Somewhat inconsistent results also have been shown for the use of screening tests. Winkleby and Cubbin (2004) show that, at ages 45-64, black and Hispanic women do not differ from whites with regard to having had a Pap test or a mammogram in the preceding 2 years. However, when the proportions of women having had such tests are adjusted for education and income, blacks and Hispanics are significantly more likely to be screened than whites. This result also holds for Hispanics aged 65-74; for blacks the differences were not significant at that age. However, Medicare reimbursement records tell the opposite story. Black and Hispanic women aged 52-69 less often receive a mammogram paid for under Medicare fee-for-service than the average beneficiary of this program (Figure 10-1; Hebb et al., 2003). In addition, Strzelczyk and Dignan (2002) show that nonwhite women in the Colorado Mammography Project are less likely than whites to adhere to a recommended follow-up screening. Such apparent inconsistencies may have explanations, but they suggest that the role of patient self-care in racial and ethnic differences has not been clearly established.
One needs to attend, to begin with, to differences across specific diseases or conditions. Psychosis and substance abuse, for instance, are related to contrasting differences. Blacks with psychotic disorders visit psychiatrists less often than whites. But blacks with substance abuse disorders have more psychiatric visits than whites (Kales et al., 2000). Other factors, from socioeconomic status to differences in cultural beliefs relating to fatalism
(Nelson et al., 2002) also complicate the picture. In addition, blacks and Hispanics are reported to distrust health care providers and expect discriminatory treatment more often than whites (LaVeist et al., 2000; Lillie-Blanton et al., 2000), but whether this affects their acceptance of recommended treatments or compliance with prescribed regimens has not been clearly demonstrated.
NEEDED RESEARCH
Improvements in health care by themselves are unlikely to either eliminate social inequalities in health or achieve optimal levels of population health (House and Williams, 2000; Kaplan et al., 2000).
Some evidence indicates that medical care explains only 10 percent of variation in adult mortality (U.S. Department of Health, Education, and Welfare, 1979), which has led to the widely held view that medical care makes a limited contribution to population differences in health status (Adler et al., 1993). However, medical care may have a greater effect on the health status of vulnerable populations, such as racial and ethnic minorities and low-status groups among older adults, than on the population in general (Williams, 1990). What this effect could be, what differences actually exist beyond those now documented, how they interact with multiple vulnerabilities in the older population, and how health care should be properly structured to address differences are all issues that require attention.
Research Need 14: Identify differences in health care—access, use, and quality—for racial and ethnic minority populations other than blacks.
To date, most research on differences in care has focused on blacks and whites, partly reflecting the absence in the Medicare file of high-quality ethnic identifiers for other groups. The few studies that have identified differences in quality and intensity of care for other groups leave the extent of the differences faced by Hispanics, American Indians and Alaska Natives, and Asians unclear (Institute of Medicine, 2002).
Research Need 15: Determine the reasons for differences in health care quality, focusing on the contributions of geographic variation, characteristics of health care institutions, provider behavior and stereotypes, and patient adherence to recommendations for care.
Multiple factors are almost certainly involved, as they are with differences in health outcomes, and need to be assessed against each other. Medical care may vary because of the health needs of different groups, or the types of care they seek, prefer, or can afford, or because of insurance coverage, provider behavior, or the policies and procedures of hospitals and
health systems. Research attention is desirable across multiple dimensions of health care.
Geographic Variation Why care varies across areas is poorly understood. Some variation may be due to less adequate services in poor areas that are predominantly minority. However, geographic variation that is not rooted in any racial or ethnic factor could still produce racial and ethnic differences in care. Different ways to define geographic areas, different patterns across areas for various medical procedures, and the complex and changing settlement patterns for racial and ethnic groups all complicate the research challenge.
Health Care Institutions The specific characteristics of health care institutions and systems that affect racial and ethnic differences in care require attention. Financial, structural, and institutional factors need consideration, taking into account features of medical procedures, such as their cost, and the degree to which medical consensus exists about particular treatments.
Provider Behavior and Stereotypes Whether, and if so how, provider decisions about treatment are influenced by stereotypes requires consideration. Negative stereotypes and the unrecognized discrimination connected with them could contribute to systematic bias in the delivery of medical care. Evidence that this actually happens, and that medical decisions are sometimes inappropriate for this reason, does not exist.
Patient Compliance Racial and ethnic differences in acceptance of therapies and compliance with prescribed regimens deserve clarification. Differences across groups are unclear and may depend on the specific medical conditions, procedures, and prescriptions. The reasons for any differences also require study—whether they are due to differences in the way patients are treated or advised, in the cultural background of each patient, or in other factors.












