
Appendix E
Human Resource Requirements for Scaling-up Antiretroviral Therapy in Low-Resource Countries1
INTRODUCTION
As drug costs have fallen sharply inrecent years anddonor funding has risen, ambitious programs are now underway to make the widespread availability of antiretroviral (ARV) treatment for AIDS patients a reality. Through these efforts, the immense benefits of antiretroviral therapy (ART) for individuals and societies alike are becoming within reach. But as the financial barriers to scaling up are relaxed, greater attention is being focused on other potential obstacles to ART expansion.
Against this background, the implications of human resource shortages for the President’s Emergency Plan for AIDS Relief (PEPFAR) and other global AIDS initiatives are now receiving increased attention. ART is a new and complicated intervention that is being expanded in settings where there may be only one doctor for every 10 or 20,000 people. It also requires other personnel—nurses, laboratory technicians, pharmacists, and counselors—as well as a capacity to provide supporting services such as voluntary counseling and testing (VCT) and the treatment of opportunistic infections (OIs). Difficulties in developing and retaining a sufficient number of skilled health workers is by no means a new problem, but the sheer scale of the HIV/AIDS epidemic, and its impact on human resources through an array of both supply and demand-side factors, has made the problem much worse.
Furthermore, while HIV/AIDS is a devastating epidemic, it is not the only source of morbidity and mortality faced by the PEPFAR countries. Drawing personnel into ARV provision will mean that fewer workers are available to address other priority health problems. In short, it is possible that in many settings the human resource constraint will be a greater obstacle to program expansion than the financial constraint.
The purpose of this chapter is to provide illustrative estimates of the human resource requirements for achieving the PEPFAR goal of treating 2 million patients with ARVs.2 There is a rapidly growing literature on the impact of HIV/AIDS on human resources for health, touching on both the complex nature of the problem as well as possible solutions (Aitken and Kemp, 2003; USAID, 2003). The objective here is more narrowly defined: to make a first step toward quantifying the human resource needs for PEPFAR. This exercise can help answer questions such as: How do needs compare with existing capacity? Which countries face the greatest challenge? Which categories of health personnel are in shortest supply? The analysis will also help point the way to potential solutions, although these are not discussed in detail. These issues are most appropriately addressed at the country level, where better data are available and policies can be tailored to local circumstances. The broad approach and illustrative estimates presented here will ideally serve as a starting point for more detailed country-specific work.
In the discussion that follows, the term “human resource requirements” refers to the number of people required to deliver ART-related health services. Making sure that they have the appropriate training to do so is another key aspect of the human capacity development issue that is not addressed here. More broadly still, there is a whole range of critical institutional components to a well functioning health care system—including governance structures, financing arrangements, logistics and information systems, and other issues—that are beyond the scope of this study. The difficulties that many public health systems have experienced in addressing less expensive and less labor-intensive health problems than ART should serve as a reminder that no amount of resources per se, whether financial or human, can guarantee program success in the all-too-frequent absence of these broader “architectural” health system inputs.
|
BOX E-1
|
The paper is organized as follows. First, the paper outlines the estimation approach and discusses methodological issues related to coverage targets for VCT and OI treatment. Second, it presents the results with respect to two major scenarios, discusses Zambia as a specific country example, and also addresses issues of sustainability. Finally, the paper offers concluding remarks and proposed next steps.
APPROACH
Estimation Approach
The basic calculation undertaken in this paper is to estimate human resource requirements by multiplying the number of patients receiving care by the per-patient time requirements for service delivery, and then dividing by the amount of time that each health worker can spend seeing patients in a year. This is shown in Box E-1. The provision of VCT and OI treatment is also included in the calculations. The result is then compared to the current stock of health workers available in each country.3 This subsection provides a short discussion of each of the inputs to this equation.
The key variable underlying the number of health personnel required to achieve the PEPFAR treatment goal will be how long different categories of workers spend with each ARV patient to deliver services. In broad terms, the identification of time requirements must balance the limited available
|
3 |
The allocation of the 2 million patient target across the 14 countries has not yet been identified under PEPFAR. (Note also that at the time of writing, a 15th PEPFAR country had yet to be identified). It will be assumed here that each country will contribute to the overall target using the number of HIV-infected adults as the weight (data were drawn from Appendix E of the PEPFAR strategy paper [2004]). For example, a country accounting for 10 percent of all HIV infections in the 14 countries would have a target to treat 200,000 of the 2 million patient total. Of course it is unlikely to be this simple in practice, and indeed the issue of human resource constraints is arguably a reason unto itself for expanding services more rapidly in some countries than in others. |
stock of health workers (for HIV/AIDS and other health services) with the importance of delivering quality care. There is no “ideal” model of care, but rather a wide range of service delivery options, both with regard to who delivers care (doctors, nurses, community lay workers, etc.) and for how long (per contact as well as the frequency of visits). Existing pilot programs may offer some guidance, but these models of care may not be appropriate for expansion to a national scale. This paper draws on some existing work on time requirements as well as the author’s own discussions with providers. Due to the range of options available, two alternative scenarios will be explored. These will be presented in detail in the results section.
The second input is the number of hours per year that health personnel have available to treat patients. To estimate this parameter, the contractual level of effort must be modified to take into consideration holidays, vacation, sick leave, and training activities (all of which will cause absences from the workplace), as well as waiting time, administrative duties, cleaning and maintenance tasks, and other activities that curtail time available to spend with patients even while at work. Especially in high-prevalence countries there is a link between time availability and the epidemic itself, since many health care workers may miss time because they are HIV-positive themselves, because they are the caregiver for someone else who is HIV-positive, or because they are attending the funerals of those who have died from the disease (Aitken and Kemp, 2003).
For all these reasons, the amount of time available to spend with patients may be substantially lower than nominal hours worked. For example, Aitken and Kemp (2003) cite a study that found that laboratory technicians in Malawi work on average about 24 hours per week instead of the expected 44 hours. Kurowski and colleagues (2003) found that in Tanzania less than 40 percent of health worker time was actually spent with patients. Current productivity levels can likely be improved upon through a range of policy interventions (e.g., better remuneration or other measures to improve health worker motivation), and ARV expansion itself implies more patients to treat and therefore possibly less time between patients for providers. However, it should also be recognized that heavy workloads could increase the rate of workforce attrition.
In this paper it will be assumed that all categories of health workers spend 1000 hours per year with patients. This could reflect, for example, an average of about 4 days at work each week (with an average of 1 day per week attributed to holiday, vacation, sick leave, training, etc.) and 5 hours per day spent providing care to patients (with the remaining hours performing other tasks or waiting). Either a greater or smaller number of hours per year could also be justified.
The final major data input used in the analysis, to which the estimation of human resource requirements will be compared, is the current stock of
health workers. Up-to-date, internationally comparable data on human capacity for health is virtually nonexistent. The analysis here draws from the World Health Organization’s WHOSIS database (WHO, 2004), which relies on country sources. The database states that “estimates of health personnel are extremely difficult to obtain, and those listed here are all that we have available.” The data on doctors and nurses may or may not adequately reflect emigration, or the possibility that some qualified personnel hold management or research positions that curtail their time for practice. The extent to which private providers are reflected in the data is also not clear.4 Finally, information on laboratory technicians is not available.
Even at the national level, accurate data are often very difficult to find. Aitken and Kemp (2003) identified eight different sources of data (mostly government documents) on human resources for health in Malawi, none of which could be fully reconciled with the others. To make matters more difficult, for the purposes of this analysis, the weak information on current stocks of health personnel must also be projected forward to 2008 when PEPFAR goals are to be achieved. The detailed work in Tanzania by Kurowski et al. (2003) predicted some increase in the numbers of doctors and nurses by 2015. However, the reality that in many countries the size of the health workforce has declined in recent years should temper expectations of any sharp increases (Liese et al., 2003). In this paper it is conservatively assumed that there will be no change through 2008 from current data on the number of health workers available.5
Supporting Services: VCT and OI Treatment
The expansion of ART requires a capacity to provide supporting services as well, and these will require human resources of their own. The estimates presented in this paper include human resources for VCT and OI treatment. However, unlike for ARV provision, there are no explicit targets for program coverage of these services. This subsection therefore briefly discusses some related methodological issues.
The key entry point to the provision of antiretroviral treatment is VCT services to determine an individual’s HIV status. To put the required number of people on ART, a much greater number of people must be tested, since many will turn out to be HIV-negative, while others will be HIV-
positive but not yet clinically eligible for treatment. Thus, ambitious targets for ARV provision automatically imply ambitious targets for VCT as well, with important implications for human resource needs. VCT also offers important benefits as a prevention tool, and so human resource requirements for VCT should be seen as contributing to the achievement of PEPFAR’s prevention goal of averting 7 million new infections as well.
What level of VCT service provision should human resource estimates be based upon? Exactly how many VCT contacts will be required to initiate 2 million people on treatment is very uncertain. People are more likely to seek testing if they have reason to believe that they may have been exposed to the virus, or because they are already developing symptoms. Among those who are tested, therefore, the proportion of individuals who are HIV-positive, and within that group the proportion that is clinically eligible for ART, will be higher than the corresponding population-wide rates. It will be assumed here that the diagnosis rate is two to three times higher than the prevalence rate (depending on the country), and that one-third of those diagnosed as HIV-positive are clinically eligible for treatment.6 The result is that over 25 million people would need to be tested across the 14 countries to initiate 2 million people on treatment.7 Human resource requirements for this level of coverage will contribute to both treatment and prevention efforts.
PEPFAR also aims to treat people with opportunistic infections. Since ART provision should reduce a patient’s susceptibility to OIs, on the surface it may seem that as ARV programs expand there will be a significant human resource “savings” with respect to OI care. However, for several reasons this may not occur. First, the absolute number of illness episodes per person may not decline because patients will live much longer and ARVs may merely delay the onset of OIs, rather than eliminate them altogether. Second, as the PEPFAR plan recognizes (Office of the United States Global AIDS Coordinator, 2004:36), the goal of expanding the entire continuum of care for HIV/AIDS patients may increase access to health services among certain population groups not previously presenting for the treatment of OIs. Finally, it is important to note that PEPFAR’s treatment goal of initiating 2 million people on ARVs by 2008 represents perhaps 20 percent of those who over the next 5 years will be reaching the stage of disease at which they become susceptible to OIs. The need for treatment
among the other 80 percent will remain unchanged. In sum, overall demand for OI car—and the resulting need for human resources—is unlikely to decline substantially during the course of PEPFAR.
What level of OI service provision should human resource estimates be based upon? PEPFAR has no explicit coverage target for OIs. The plan aims to provide care to 10 million people, but this includes care of orphans and vulnerable children, symptom management, and end-of-life care, in addition to the treatment of OIs. For the present analysis it will be assumed that OI treatment is provided to everyone receiving ARVs (who are much less susceptible to infection than those not receiving ART), as well as to 20 percent of those who are not. This translates into the treatment of OIs for about 3.5 million non-ARV patients over five years, accounting for about one-third of the broader care goal. Four of the most common OIs will be considered: tuberculosis, pneumonia, oral candidiasis, and cryptococcal meningitis (Kombe and Smith, 2004).
RESULTS
This section presents estimates of the number of personnel required in five different service provider categories—doctors, nurses, laboratory technicians, VCT counselors, and community workers—for delivering ARVs to 2 million people by 2008, including supporting VCT and OI services. Other crucial human resource inputs—such as pharmacists, program managers, and logistical workers—are not included. Two scenarios are discussed: the first does not include community workers, while the second adds this cadre and assigns to them certain tasks normally performed by skilled professionals. The case of Zambia is also analyzed to provide a country-specific illustration of key issues. The topic of sustainability is discussed in the final subsection.
Scenario 1: No Community Workers
The assumptions for average per-patient time requirements by personnel category (expressed in annual terms for ARVs and per-episode terms for other services) are shown in Table E-1. Each individual patient in reality will require a different amount of time with health workers depending on a variety of factors. Time requirements for ARV delivery, for example, will be higher for patients who are being initiated on treatment, or for those who are suffering from complications.8 Models of care may also vary
TABLE E-1 Per-Patient Time Requirements in Minutes, Scenario 1
|
|
Doctor |
Nurse |
Lab Technician |
VCT Counselor |
Community Worker |
|
VCT, HIV neg (per service) |
0 |
15 |
0 |
30 |
0 |
|
VCT, HIV pos (per service) |
0 |
30 |
0 |
45 |
0 |
|
ARVs (per year) |
90 |
90 |
90 |
0 |
0 |
|
Tuberculosis (per episode) |
45 |
30 |
60 |
0 |
0 |
|
Oral candidiasis (per episode) |
15 |
0 |
0 |
0 |
0 |
|
Pneumonia (per episode) |
15 |
0 |
20 |
0 |
0 |
|
Meningitis (per episode) |
30 |
0 |
40 |
0 |
0 |
depending on the physical setting (hospital, health center, at home, etc.) in which the service is delivered. But overall human resource requirements will ultimately depend on averages such as those shown in the table.
These estimates are based generally on reserach by Huddart and colleagues (2004), outcomes from a WHO/UNAIDS consensus meeting held in November 2003 (WHO/UNAIDS, 2004),9 and the author’s discussions with providers in Uganda and Zambia. As noted earlier, there is no “ideal” model. A wide range of service delivery options is available and existing models of care may be unrealistic for scaling up to a national level. Note that VCT services are assumed to be performed by a nurse and a VCT counselor but not by a lab technician; in some cases only one person may do everything.10 For ARV delivery, lab technician time will depend on the number and type of tests to be performed, the technology applied, and even the model of equipment being used. Thus a very wide range is possible; here we will assume that 90 minutes of lab technician time is required per patient per year.
Table E-2 shows the total human resource requirements for this sce-
TABLE E-2 Total Human Resource Requirements in FTEs, Scenario 1
|
|
Doctor |
Nurse |
Lab Technician |
VCT Counselor |
Community Worker |
|
Botswana |
61 |
71 |
62 |
25 |
0 |
|
Cote d’Ivoire |
141 |
198 |
144 |
128 |
0 |
|
Ethiopia |
400 |
629 |
411 |
512 |
0 |
|
Guyana |
4 |
9 |
4 |
10 |
0 |
|
Haiti |
50 |
81 |
52 |
68 |
0 |
|
Kenya |
483 |
660 |
497 |
416 |
0 |
|
Mozambique |
215 |
301 |
221 |
205 |
0 |
|
Namibia |
40 |
52 |
41 |
26 |
0 |
|
Nigeria |
650 |
1092 |
665 |
944 |
0 |
|
Rwanda |
88 |
127 |
90 |
86 |
0 |
|
South Africa |
966 |
1246 |
990 |
663 |
0 |
|
Tanzania |
263 |
398 |
269 |
293 |
0 |
|
Uganda |
101 |
184 |
103 |
173 |
0 |
|
Zambia |
206 |
261 |
211 |
133 |
0 |
nario, measured as full-time equivalents (FTEs). Note that because perpatient time requirements for ARV delivery were the same for doctors, nurses, and lab technicians at 90 minutes each per year, the overall requirements for these three cadres are similar as well (differences are due to OI treatment). But since all countries have far more nurses than doctors, and often more doctors than lab technicians, the relative burden falls more heavily on doctors and lab technicians. ARV provision is a relatively complicated intervention, and an important implication is that it places a greater burden on more specialized workers. Table E-2 helps to identify where the shortages are likely to be most severe and also points to the potential solution of delegating as much responsibility to nurses and community workers as possible (as will be seen in Scenario 2).
How do the requirements in Table E-2 compare with existing capacity? The fraction of each country’s existing doctor workforce required to reach PEPFAR coverage goals under Scenario 1 is shown in Figure E-1. For all countries, approximately 80 percent of the doctor requirements are for ARVs, with the remainder for OI treatment. It is difficult to identify a constraint precisely, since dedicating 100 percent of a country’s doctor workforce to HIV/AIDS is obviously not realistic. For four countries (and nearly a fifth), the requirement exceeds 20 percent.
What about the other health worker categories? The burden on the nursing sector is likely to be less serious than in the case of doctors, rarely exceeding 5 percent of existing capacity. However, it is likely to be more serious for laboratory technicians. International data for lab technicians are scarce, but the illustrative case of Zambia (which faces a severe challenge) is
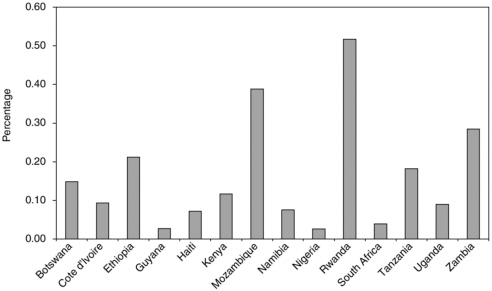
FIGURE E-1 Fraction of existing doctor workforce required under Scenario 1.
discussed below. Finally, there are similarly no international data on existing numbers of VCT counselors. This is the cadre of health workers that could probably be trained most quickly among the four categories, but they may also be subject to the highest burnout rate.
Requirements for all staff categories should be placed in a broader context. As noted earlier, HIV/AIDS is not the only health crisis facing the 14 PEPFAR countries. Devoting personnel to HIV/AIDS will mean fewer are available to contribute, for example, to the reduction in malaria incidence and child and maternal mortality rates as targeted by the Millennium Development Goals (MDGs). Taking a broader view of health sector human resource requirements, Kurowski and colleagues (2003) found that projected human resource availability in Tanzania was “grossly insufficient” for reaching the requirements necessary to scale up priority interventions (including ART) as recommended by the Commission on Macroeconomics and Health (CMH).
Scenario 2: Adding Community Workers
In recognition of the obstacle to scaling-up posed by inadequate human resources, the PEPFAR plan proposes that alternative service delivery models could ease the burden by shifting certain duties to community workers. The onerous requirements of Scenario 1 discussed above help support the rationale for this devolution of responsibilities.
Table E-3 shows the per-patient time requirements of an alternative service delivery model that makes use of community workers. It is assumed that lab technician responsibilities for ART monitoring and OI diagnosis cannot be reassigned to any other health worker category. The only way to reduce requirements for this job category—where the shortages may be most severe—is to reduce the number of tests.
The resulting human resource requirements are shown in Table E-4. Doctor requirements are reduced by roughly 50 percent compared to Scenario 1. Nurse requirements decline by a narrower margin, since the “savings” generated by allocating some of their responsibilities to community workers are partially offset because they simultaneously adopt part of the doctor’s role. Note that in all countries the number of lab technicians required is now higher than the doctor requirement, although many health systems are endowed with more of the latter than the former.
How do these compare to current availability? Figure E-2 shows doctor requirements as a share of existing capacity. For all countries, about 75 percent of the requirements are for ARV provision, while the rest is for OI treatment. Except for Mozambique and Rwanda, all countries are now below the 20 percent threshold. But the requirements in many cases are still substantial. As before, there are no international data on lab technicians and VCT counselors to which comparisons can be made.
As a final comment on Scenario 2, the issue of quality of care should also be considered. Delegating certain responsibilities from skilled health professionals to trained community workers, and scaling back the laboratory monitoring protocol, does introduce a risk that the quality of care will
TABLE E-3 Per-Patient Time Requirements in Minutes, Scenario 2
|
|
Doctor |
Nurse |
Lab Technician |
VCT Counselor |
Community Worker |
|
VCT, HIV neg (per service) |
0 |
15 |
0 |
15 |
15 |
|
VCT, HIV pos (per service) |
0 |
30 |
0 |
30 |
15 |
|
ARVs (per year) |
45 |
60 |
60 |
0 |
75 |
|
Tuberculosis (per episode) |
30 |
15 |
60 |
0 |
30 |
|
Oral candidiasis (per episode) |
15 |
0 |
0 |
0 |
0 |
|
Pneumonia (per episode) |
15 |
0 |
20 |
0 |
0 |
|
Meningitis (per episode) |
15 |
15 |
40 |
0 |
0 |
TABLE E-4 Total Human Resource Requirements in FTEs, Scenario 2
|
|
Doctor |
Nurse |
Lab Technician |
VCT Counselor |
Community Worker |
|
Botswana |
33 |
52 |
45 |
16 |
55 |
|
Cote d’Ivoire |
77 |
156 |
105 |
72 |
162 |
|
Ethiopia |
221 |
511 |
304 |
279 |
531 |
|
Guyana |
2 |
7 |
3 |
5 |
8 |
|
Haiti |
28 |
66 |
38 |
37 |
68 |
|
Kenya |
267 |
516 |
367 |
235 |
541 |
|
Mozambique |
120 |
238 |
165 |
114 |
249 |
|
Namibia |
22 |
39 |
30 |
15 |
41 |
|
Nigeria |
354 |
895 |
485 |
510 |
926 |
|
Rwanda |
48 |
100 |
66 |
48 |
104 |
|
South Africa |
529 |
956 |
726 |
387 |
1003 |
|
Tanzania |
143 |
318 |
196 |
162 |
331 |
|
Uganda |
55 |
153 |
75 |
92 |
158 |
|
Zambia |
113 |
200 |
155 |
79 |
210 |
suffer. ART offers enormous benefits to AIDS patients, but it is not without risks, especially with regard to the development of drug resistance.
The Case of Zambia
The case of Zambia provides one illustration of the potential human resource challenges that lie ahead. The estimates presented earlier assume that Zambia treats about 110,000 individuals with ARVs by 2008 under PEPFAR, based on its share of HIV-infected persons in the 14 countries. But there is a total of about 850,000 HIV-positive Zambians, about half of whom may be eligible for treatment within the next 5 years (and almost all within the next 10 years). Even at this relatively low level of coverage (roughly 25 percent by 2008), however, the human resource requirements will impose a large burden.
The requirement of 206 doctors by 2008, as indicated in Table E-2, represents close to one-third of the existing doctor workforce in the country. The implications of meeting this requirement for the delivery of other priority health services would be substantial. At the same time, however, the requirement of 261 nurses represents only 2 percent of the existing workforce in that category. This serves to highlight the logic underlying proposals to reassign as much of the doctor’s role to nurses as possible.
Perhaps the most forbidding constraint, however, is with respect to lab personnel: the need for 211 technicians in Scenario 1 represents about 65 percent of Zambia’s 325 public sector lab technicians and technologists (Huddart et al., 2004). The Scenario 2 requirement for lab personnel repre-
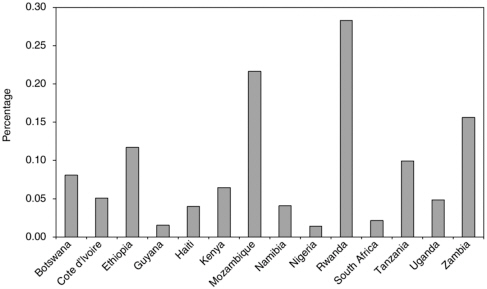
FIGURE E-2 Fraction of existing doctor workforce required under Scenario 2.
sents nearly 50 percent of current capacity. As noted earlier, this job is difficult to reassign to other categories of health personnel or to community workers, and thus the only way to reduce requirements is to reduce the number of tests performed.
A recent study (Huddart et al., 2004) of the HIV/AIDS workforce in Zambia identified two other challenges that may be common elsewhere as PEPFAR activities are scaled up. First, it found that the average loss rate of HIV/AIDS service delivery staff was 30 percent annually. High rates of workforce attrition will make program expansion even more challenging. Second, standards of service delivery in existing programs were found to be low, suggesting that quality of care considerations will become increasingly important as population coverage expands.
Sustainability
As Aitken and Kemp (2003) note, “the impact of HIV/AIDS is devastating and will continue for decades—[and] the response must be on a similar scale and timeframe.” As we look further into the future, there will be a greater probability that more health workers can be trained, new interventions and technologies can be developed, or other steps can be taken to ease the human resource constraint.
But the issue of sustainability will remain relevant. PEPFAR aims to treat 2 million patients with ARVs in a group of countries in which about
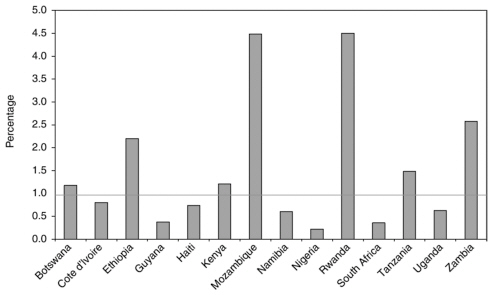
FIGURE E-3 Fraction of existing doctor workforce required for full coverage in 10 years.
20 million HIV-positive individuals currently live. There are millions of people who are seropositive today who still won’t be clinically eligible for treatment by 2008, and ultimately they, too, will require human resources for ARV delivery. Also, there are other global initiatives to expand ARV provision, such as the WHO’s 3 × 5 initiative and the Global Fund to Fight AIDS, Tuberculosis, and Malaria. These are placing similar demands on human capacity in the health sector but were not included in the estimates presented earlier.
Since virtually all of the 20 million HIV-positive individuals in the 14 countries will become clinically eligible for treatment within the next 10 years, it may be asked hypothetically what the human resource requirements would be if every one of them were actually to receive ARVs at that time.11 The resulting doctor requirements, assuming the same model of care as in Scenario 1 above, are shown in Figure E-3. In half of the countries, the requirements exceed the entire existing workforce. Even levels above 50 percent, surpassed by four others, are probably not realistic given other health demands. The number of new human resources that would be available 10 years from now is uncertain, but as noted earlier, many countries have suffered recent declines, and so a sharp increase is unlikely.
A more modest pace of expansion would be to duplicate the goals of PEPFAR during the subsequent 5-year period from 2009 to 2013. The human resource needs would be approximately twice the Scenario 1 and 2 results presented earlier. The number of doctors available by then would also need to double just to keep the ratios in Figures E-1 and E-2 constant. Again, this is unlikely. In sum, the human resource challenge applies not only to treating 2 million patients by 2008, but also to initiating treatment for those who will become clinically eligible beyond that year.
CONCLUSION AND NEXT STEPS
The results of the previous section provide an indication of the human resource needs for PEPFAR and how they differ across countries and across different categories of health workers. These are illustrative estimates. Of necessity they are based on general assumptions about what models of care may ultimately be implemented on the ground, and how the overall target of treating 2 million patients will be achieved across countries. Also, the requirements are compared to imperfect data on existing human resource capacity.
However some key findings do emerge. First, the human resource requirements of PEPFAR are substantial. Even providing 90 minutes of doctor time per year to each of the 2 million ARV patients would require about 20 percent or more of the existing doctor workforce in 5 of the 14 PEPFAR countries. Second, the severity of the human resource constraint varies widely among the 14 countries. It is clear that some countries will be much better positioned to rapidly scale up services than others, and indeed this could inform how the overall target of 2 million patients is achieved. Third, the human resource requirements are much more onerous for doctors and lab technicians than they are for nurses and counselors, and models of care need to be designed accordingly.
The results also highlight some important thematic issues. First, the scale of the problem is such that human resource requirements for HIV/ AIDS should not be viewed in isolation from other health sector human resource needs.12 More health personnel for ARVs will mean less for other priority services. Second, while the delegation of responsibilities to community lay workers is a sensible approach to the human resource constraint, these models should also be scrutinized from a quality of care perspective. Quantifying human resource needs—for example, by identifying the aver-
age number of minutes that an ARV patient spends each year with a doctor—can help inform these discussions. Third, there are millions of people currently infected with HIV who will still not be clinically eligible for ART in 2008, and so issues of sustainability beyond that year should not be ignored.
Ultimately, however, the results presented here should serve as a starting point for detailed country-level work. It is there that the best data and understanding of local circumstances lie. The exercise of quantifying human resource needs by national stakeholders can provide important information before a program expands.13
Most important, it can help to inform policy measures that aim to address the human resource constraint. Potential solutions have been discussed in detail elsewhere.14 They may be pursued on multiple levels simultaneously: within the HIV/AIDS sector, within the health system more broadly, at the national level, or internationally. No single solution will offer a magic bullet to the human resource challenge; countries will need to adopt multipronged strategies to fit local circumstances. But taken together they can help contribute to a more successful program expansion.
REFERENCES
Aitken JM, Kemp J. 2003. HIV/AIDS, Equity and Health Sector Personnel in Southern Africa. Equinet Discussion Paper Number 12. [Online]. Available: http://www.equinetafrica.org/Resources/downloads/discussionpaper12.pdf [accessed August 24, 2004].
Huddart J, Lyons JV, Furth R. 2004. The Zambia HIV/AIDS Workforce Study: Preparing for Scale-up. [Online]. Available: http://www.qaproject.org/pubs/PDFs/ORMZambiaWorkforcel.pdf [accessed September 7, 2004].
Kombe G, Smith O. 2004. The Costs of HIV/AIDS Services within the Basic Health Care Package in Zambia. Unpublished.
Kurowski C, Wyss K, Abdulla S, Yemadji N, Mills A. 2003. Human Resource for Health: Requirements and Availability in the Context of Scaling Up Priority Interventions in Low Income Countries: Case Studies from Tanzania and Chad. London: Health Policy Unit, London School of Hygiene and Tropical Medicine.
Liese B, Blanchet N, Dussault G. 2003. The Human Resource Crisis in Health Services in Sub-Saharan Africa. [Online]. Available: http://econ.worldbank.org/files/30373_29_Bernhard_Liese_The_Human_Resource_Crisis_in_Health_Ser.pdf [accessed September 7, 2004].
Office of the United States Global AIDS Coordinator. 2004. The President’s Emergency Plan for AIDS Relief. [Online]. Available: http://www.state.gov/documents/organization/29831.pdf [accessed September 7, 2004].
PEPFAR strategy paper (2004), Appendix E.
Picazo O. 2003. Deployment and Retention of Health Workers in Africa: A Note on Some Practices and Issues. Mimeo.
USAID (U.S. Agency for International Development). 2003. The Health Sector Human Resource Crisis in Africa: An Issues Paper. [Online]. Available: http://www.dec.org/pdf_docs/PNACS527.pdf [accessed August 24, 2004].
WHO (World Health Organization). 1998. WHO Estimates of Health Personnel. [Online]. Available: http://www3.who.int/whosis/health_personnel/health_personnel.cfm?path=whosis,topics,health_personnel&language=english [accessed September 7, 2004].
WHO. 2004. WHO Statistical Information System. [Online]. Available: http://www3.who.int/whosis [accessed September 2, 2004].
WHO/UNAIDS (World Health Organization and Joint United Nations Programme on HIV/ AIDS). 2004. Report on the Methods Used to Estimate Costs of Reaching the WHO Target of 3 by 5. [Online]. Available: http://www.who.int/3by5/en/Progressreport.pdf [accessed October 21, 2004].

















