
Appendix N
Preliminary Results from CDC’s Estimate of the National Capacity for Colorectal Cancer Screening and Follow-Up Laura C.Seeff, M.D.
SLIDE 1
SLIDE 1 NOTES: In this presentation, I will briefly show preliminary results of CDC’s capacity assessment. I will touch on the methods and results of the study listed above.
We hope to have the final results published in the late Spring (Seeff et al., 2004).
SLIDE 2
SLIDE 2 NOTES: We assessed the national capacity to perform endoscopic procedures in three steps. We first implemented the National Survey of Endoscopic Capacity, or SECAP, to estimate the current volume of lower endoscopic procedures currently being performed. We then designed a forecasting model to estimate the unmet need for a lower endoscopy. Finally, we compared the two to make our capacity assessment.
SLIDE 3
SLIDE 3 NOTES: We used a sampling frame based on endoscope sales made to medical practices between 1996 and 2000.
We asked survey recipients, among many other questions, what is the current and maximum potential weekly volume of both flexible sigmoidoscopy and colonoscopy, given the current resources without making any additional investments or changes? “Current resources refers” to personnel, though in other parts of the survey we asked about equipment.
SLIDE 4
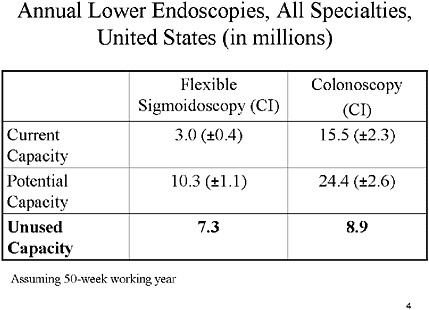
SLIDE NOTES 4: These results are collapsed across all specialties. (We do have results by specialty; they will be included in our final study report.) The results are also scaled up from the weekly assessments to annual estimates assuming a 50-week working year.
Respondents indicated that in a year, about 3 million flexible sigmoidoscopies are being done, and 15.5 million colonoscopies are being done. We are currently referring to that as “current capacity”; though, it might better be called “current utilization.”
Then the potential capacity is the number that the respondents said they could do with their current resources. That estimate gives 10.3 million sigmoidoscopies and 24.4 million colonoscopies.
Note, however, that the questions about potential capacity were asked independently for each modality. Therefore, we cannot be certain that the respondents could reach the estimated potentials for both sigmoidoscopy and colonoscopy simultaneously.
SLIDE 5
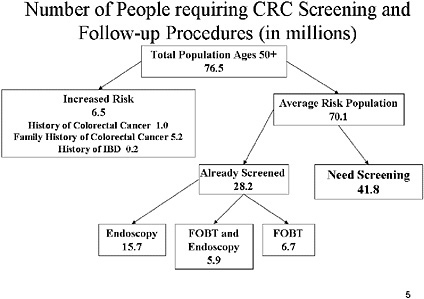
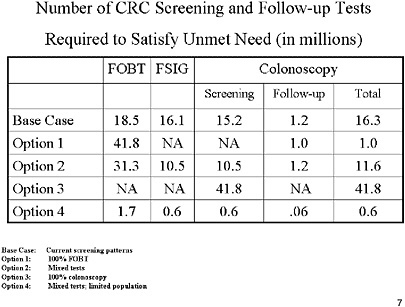
SLIDE 5 NOTES: We attempted to determine the size of the U.S. population that has not been screened and the number of tests needed under a series of scenarios to screen those people.
From the 76.5 million individuals in the U.S. age 50 or greater, we removed 6.5 million persons who would be deemed “high risk” from these categories. High-risk is based on family history of colorectal cancer or history of pre-disposing conditions. Those data come from SEER (NCI), National Health Interview Survey (CDC), and National Institute of Diabetes and Digestive and Kidney Diseases (NIH) databases.
The average-risk population is 70 million. We used NHIS data to determine which of those individuals would already have been screened, which eliminates 28.2 individuals. Thus, almost 42 million people ages 50 and older have not been screened according to current screening guidelines.
SLIDE 6
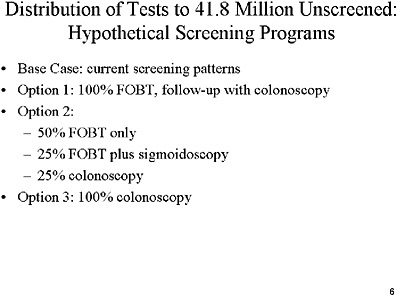
SLIDE 6 NOTES: We looked at how to distribute the current endoscopy capacity among the 42 million unscreened individuals. Several options are available. First, we examined how capacity would compare with unmet screening need if the unscreened population were to follow current screening patterns. We assume that those 42 million people would be screened in the same proportions as is currently observed through the National Health Interview Survey (NHIS).
Option 1 assumes that all those people would get FOBT first, followed by a followup colonoscopy for those individuals with a positive FOBT.
Option 2 assumes that half of the individuals would get an FOBT, one-quarter would get FOBT plus flexible sigmoidoscopy, and one-quarter would get colonoscopy.
Option 3 assumes that all such individuals would be screened via colonoscopy.
SLIDE 8
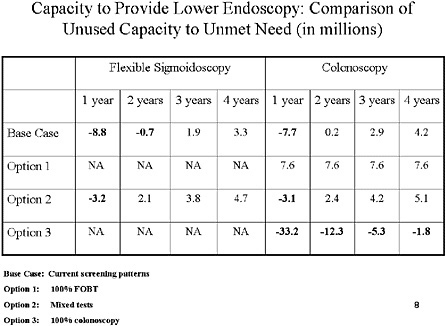
SLIDE 8 NOTES: This table shows how the unused capacity (resulting from the SECAP) survey compares to the unmet need results if we were to distribute tests over 1, 2, 3, or 4 successive years. It would, of course, be difficult to do all tests in the first year.
As you can see, in the base case scenario, distributing the tests over a single year would leave a capacity deficit of almost 9 million sigmoidoscopies and almost 8 million colonoscopies. However, under option 1, we would have enough colonoscopy capacity to screen all individuals immediately.
If we were to try to offer colonoscopy to the entire unscreened population (option 3), it would take 5 years in all.
SLIDE 9
SLIDE 9 NOTES: Assuming that the current met need continues to be met, the endoscopic capacity for the general population is immediately available if we were to use an FOBT-only strategy. Any of the other options would require more than one year for completion.
REFERENCES
Seeff LC, Nadel MR, Klabunde CN, Thompson T, Shapiro JA, Vernon SW, Coates RJ. 2004. Patterns and Predictors of Colorectal Cancer Test Use in the Adult U.S. Population. Cancer. 100(10):2093–2103.









