

SLIDE 4
SLIDE NOTES 4: Any discussion of surveillance would be remiss if it did not focus extensively on the National Polyp Study, which I will refer to as the NPS (Winawer et al., 1993).
The NPS was a randomized trial of the timing of surveillance colonoscopy. It included over 1400 patients who had resected adenomas. The seven participating centers were centers of excellence and expertise.
SLIDE 5
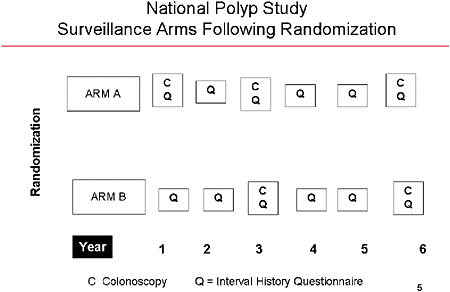
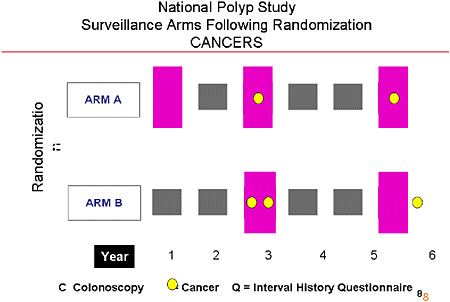
SLIDE 5 NOTES: The basic design involved a comparison of two arms. A patient randomized to Arm A was assigned to a surveillance colonoscopy at 1 year, at 3 years, and at 6 years following the colonoscopy in which the index adenoma was detected. In each of the years between the surveillance procedures, questionnaires were administered.
SLIDE 6
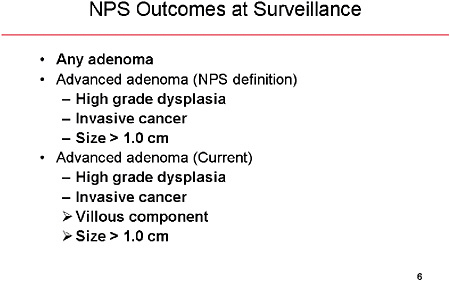
SLIDE 6 NOTES: Outcomes of each surveillance procedures were defined as shown above. An advanced adenoma was defined in the study somewhat differently from that used in today’s conventional current practice and in the guidelines issued by professional societies. Notice the subtle difference in the size criterion. There is some evidence that specifying greater than or equal to, as opposed to greater than, 10 mm can make a real non-trivial difference in the number of lesions subject to surveillance. In addition, a villous component has been recognized as an important risk indicator, but the data from the NPS did not define advanced adenomas using that criterion.
SLIDE 7
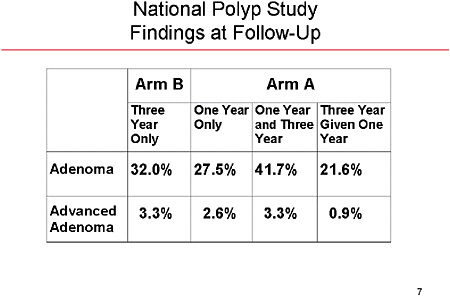
SLIDE 7 NOTES: Here are the results for the two arms. Arm B—the three-year surveillance protocol—had a 32 percent incidence of any adenoma and a 3.3 percent incidence of advanced adenoma. Arm B, on the other hand, had a higher cumulative incidence of adenomas (41.7 percent). However, the risk of advanced adenoma at three years is identical between the two arms (3.3 percent).
At the end of 6 years, the cumulative risk of any adenoma was 52 percent for Arm A and 48 percent for Arm B.
SLIDE 12
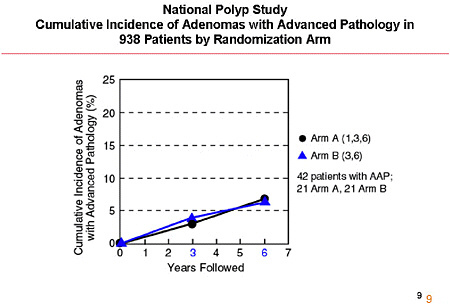
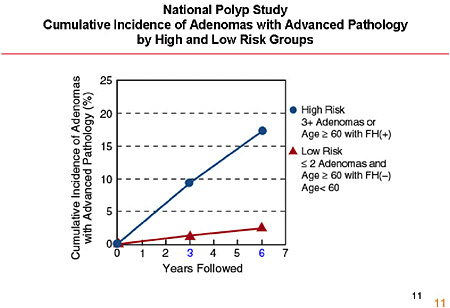
SLIDE 12 NOTES: On the basis of these findings, the NPS researchers concluded that surveillance intervals lengthened to six or more years are reasonable for low-risk adenoma patients. (Winawer et al., 1993; Zauber and Winawer, 1997).
The data are currently being reanalyzed with the current definition of high-risk adenoma. It is unlikely, however, that the reanalysis will affect the conclusions.
SLIDE 13
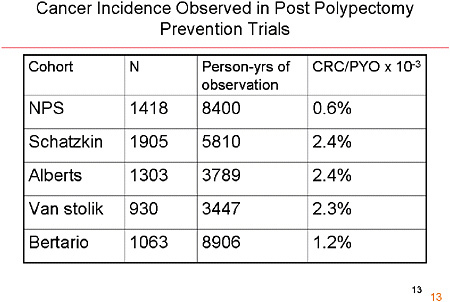
SLIDE 13 NOTES: Is it possible that cancers were missed in the NPS? Some relatively small studies have examined back-to-back colonoscopies. They have shown that the miss rate is inversely related to the size of the tumor. For advanced adenomas, the miss rate is small, so it is unlikely that the clinicians in the NPS missed a high number of tumors.
SLIDE 14
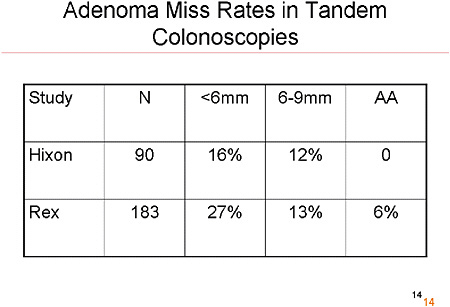
SLIDE 14 NOTE: Is it possible that cancers were missed in the NPS? Some relatively small studies have examined back-to-back colonoscopies. They have shown that the miss rate is inversely related to the size of the tumor. For advanced adenomas, the miss rate is small, so it is unlikely that the clinicians in the NPS missed a high number of tumors.
SLIDE 17
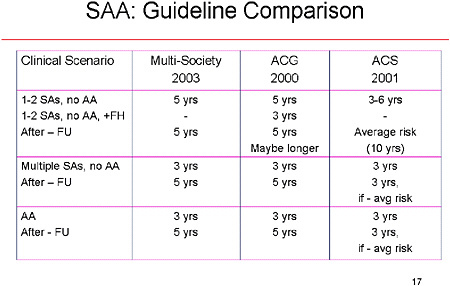
SLIDE 17 NOTES: The three groups are not very different from one another in their recommendations. After two small adenomas, or no adenoma with advanced pathology, most societies recommend surveillance after 5 years. The American Cancer Society gives a greater range—from 3 to 6 years. The groups do differ on what to do after the first negative surveillance examination. Two groups indicate that every-five-years is still warranted, whereas the American Cancer Society recommends that such individuals be considered average risk and returned to a screening pool (with a colonoscopy ever 10 years).
SLIDE 21
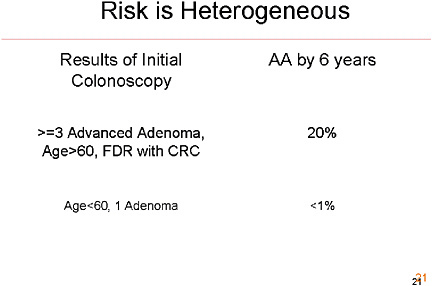
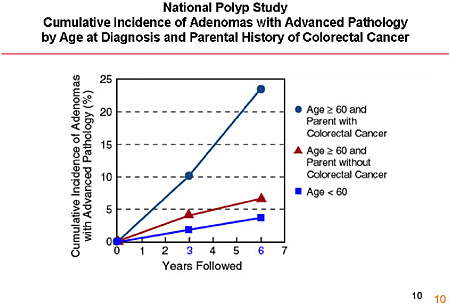
SLIDE 21 NOTES: It is important to remember, when considering adherence data, that risk is heterogeneous. We know from the National Polyp Study, for example, that 20 percent of individuals who are over age 60 and have a first-degree relative with CRC are likely to have an advanced adenoma in the 6 years following the index polypectomy, but only 1 percent under age 60 with a single adenoma and no first-degree relative with CRC will have one. It appears, from the surveys, that physicians actually take those risk differences into account when they decide on what to recommend to their individual patients.
SLIDE 22
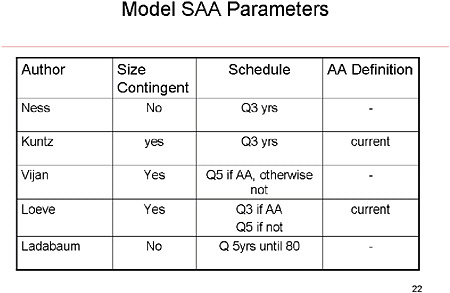
SLIDE 22 NOTES: A brief look at the five models investigated in depth as part of this workshop shows that the surveillance patterns differ substantially. Some base surveillance strategies contingent on the size of the initial adenoma, some don’t. Most use a 3-year surveillance schedule. And they differ as to whether a different surveillance regimen is enacted for advanced adenomas.
What none of the models appear to have is any tailoring of surveillance on the basis of age. But the data suggest that in practice, age is an important determinant of the frequency of surveillance.
REFERENCES
Winawer SJ, Zauber AG, May Nah Ho, O’Brien MJ, Gottlieb LS, Sternberg SS, Waye JD, Schapiro M, Bond JH, Panish JF, Ackroyd F, Shike M, Kurtz RC, Hornsby-Lewis L, Gerdes H, Stewart ET, Lightdale CJ, Edelman M, Fleisher M. 1993. Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med. 329(27):1977–1981.
Zauber AG, Winawer SJ. 1997. Initial management and follow-up surveillance of patients with colorectal adenomas. Gastroenterol Clin North Am. 26(1):85–101.






















