
2
Context and Content of the CDC Quarantine Station Expansion Plan
During the late1960s, more than 500 people staffed the 55 federal quarantine stations then active at U.S. seaports, airports, land-border crossings, consulates, territories, and territorial waters (Cetron, 2004; DGMQ, 2003a). Yet many leaders of the American medical community during those years believed it was “time to close the book on infectious diseases, declare the war against pestilence won, and shift national resources to such chronic problems as cancer and heart disease.” This statement, attributed by legend to U.S. Surgeon General William Stewart (Office of the Public Health Service Historian, 2002), reflected the public’s confidence in the power of antibiotics and vaccines to eradicate such dreaded communicable diseases as yellow fever, plague, cholera, and especially smallpox, which the quarantine stations had worked to barricade from entering the U.S. population for nearly a century.
The perception that humans had effectively controlled microbial threats led to the dismantling of most of the federal border quarantine system in the 1970s; by the end of that decade, fewer than a dozen active stations remained (Cetron, 2004).
THE EMERGENCE OF NEW INFECTIOUS DISEASES AND THE THREAT OF BIOTERRORISM
At the same time that the border quarantine system was being largely dismantled, new and long-absent infectious diseases were emerging, reemerging, and spreading in human populations. Nearly 40 newly emerging
infectious diseases were identified during the 30 years between 1973 and 2003 (GAO, 2004). The convergence of multiple interrelated factors is responsible for this phenomenon (IOM, 2003). Important factors include
-
rapid, high-volume international and transcontinental travel, commerce, and human migration;
-
mass relocation of rural populations to cities and the prevalence of overcrowded, unsanitary conditions there;
-
exponential growth of population and the number of individuals susceptible to infectious disease;
-
widespread changes in climate, ecology, and land use;
-
more frequent contact between people and wildlife;
-
reduced global investment in public health infrastructure;
-
development of antimicrobial resistance.
Numerous scientists, physicians, and public health officers in national and international organizations have voiced concern about these trends and their relationship to such naturally occurring public health threats as West Nile virus, SARS, and pandemic influenza. Also within the past two decades, terrorism in general and bioterrorism in particular have become grave concerns to the U.S. government and its citizens. Consequently, in the late 1990s, DGMQ began to explore ways that the quarantine stations at U.S. ports of entry might help protect U.S. citizens from the unintentional or intentional importation of dangerous infectious agents (Personal communication, D. Kim, DGMQ, October 13, 2004).
EXPANSION PLAN FOR CDC QUARANTINE STATIONS AT U.S. PORTS OF ENTRY
U.S. Government Increases Investment in Quarantine Stations at Ports of Entry
The outbreak of SARS in 2002 and 2003 dramatically demonstrated the need for strong, well-coordinated national and international systems for disease surveillance, detection, and response (DGMQ, 2003b). In the short term, the outbreak led to a modest addition of nine contract employees at the CDC quarantine stations (Personal communications: D. Kim, DGMQ, October 13, 2004; M. Remis, DGMQ, October 21, 2004).
Coupled with the microbial threats described above, SARS reinvigorated interest within the federal government to commit funding to biosecurity initiatives. A portion of the fiscal year 2004 budget appropriation went to DGMQ for the development of three new CDC quarantine stations at U.S. ports of entry: Houston Intercontinental Airport; the Mexico–
U.S. land border crossing in El Paso, Texas; and Dulles International Airport, located 26 miles from Washington, D.C. These three new stations are partially staffed as of this writing (Personal communications: J. Barrow and M. Remis, DGMQ, December 28, 2004; M. Remis, DGMQ, May 11, 2005).
Further expansion of the quarantine stations in number and scope of work was proposed under the biosecurity umbrella of the Administration’s fiscal 2005 budget request to Congress (OMB, 2004). This proposal called for expansion to a total of 25 CDC quarantine stations at U.S. ports of entry (Figure 2.1).
Congress allocated $80 million for fiscal 2005 biosecurity activities to the Office of the Secretary of the Department of Health and Human Services (U.S. Congress, 2004), which distributed $10.2 million to DGMQ’s Quarantine and Border Health Services Branch, 92% of which was applied to salaries and other personnel expenses (Personal communication, M. Remis, DGMQ, March 21, 2005). The Administration’s fiscal 2006 budget request to Congress includes $15.1 million for the quarantine station expansion (Personal communication, M. Remis, DGMQ, March 21, 2005). CDC Director Julie Gerberding forecast that the expansion will be complete by the end of fiscal 2006 if the requested funds are allocated to DGMQ (Gerberding, 2005).
DGMQ’s Vision for the Expanded Quarantine System
With its new mandate, DGMQ wants the CDC quarantine stations to do more than respond to and evaluate travelers with suspect or probable illness. It envisions playing an active, anticipatory role in nationwide biosurveillance (DGMQ, 2003b; DGMQ, 2004a). This move may be broadly viewed as a significant step back to the robustness of the U.S. border quarantine station system before 1970, as well as a step forward toward national biosecurity based on today’s technology and knowledge of microbial threats to human heath.
“CDC Quarantine Stations are gearing up to make the transition from the current focus on federal inspection services at airports to become a full partner in public health response,” reads a 2003 proposal by DGMQ (DGMQ, 2003b, p.1). “The transformed CDC Quarantine Stations will go beyond evaluating ill passengers to encompass a wide range of responses to infectious disease threats, whether intentional—as in the case of bioterrorism—or related to emerging pathogens…. [They] will bring new expertise to bridge gaps in public health and clinical practice1, emergency
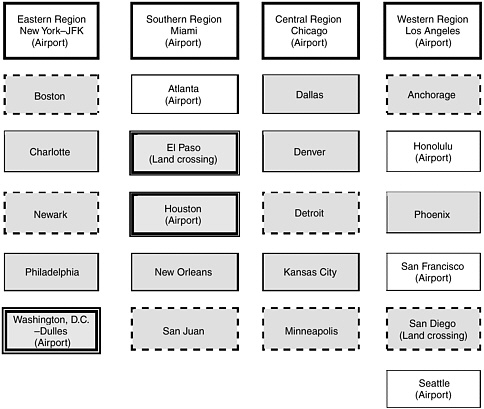
FIGURE 2.1 The proposed geographic distribution of the 25 quarantine stations in the expanded system. The New York, Miami, Chicago, and Los Angeles quarantine stations would have the greatest capacity in both number of people and variety of competences. These staff would support other stations in their geographic region. The white boxes denote the eight cities where quarantine stations have existed prior to 2004. The shaded boxes with a double border identify the 3 cities where the development of new quarantine stations began in 2004; none is fully operational as of this writing. The other shaded boxes represent the 14 cities where DGMQ plans to establish more stations beginning in 2005; those with a dashed border represent the 7 stations slated to open in 2005. The type of port where a quarantine station is or will be located, if known, is indicated in parentheses under the name of each of those cities.
SOURCES: DGMQ, 2004b; personal communication, M. Remis, DGMQ, March 21, 2005.
services, and response management…. Improved communications networks will enable passengers to be notified promptly of potential exposures to infectious diseases. These expanded services will be integrated into bioterrorism and emergency preparation and response plans and will be grounded in strengthened collaboration” with state and local health departments, the travel industry, and the health-care community, as well as other federal agencies.
DGMQ also would like the CDC quarantine stations to provide a stronger continuum of health support for refugees, whom the division helps prepare for migration to the United States, and immigrants. Refugees primarily enter the United States through a port with a quarantine station2, so the stations may be well positioned to monitor the health status of arriving refugees and collaborate with state and local officials on followup health evaluations and treatment. It should be noted that DGMQ does have a program for immigrants and refugees housed in a branch parallel in structure to the branch that houses the quarantine stations staff.
DGMQ’s Self-Reported Goals and Accomplishments—Fiscal 2003
In its program review for fiscal 2003, DGMQ articulated its goals for the expanded number and scope of quarantine stations (DGMQ, 2004a). Reflecting on its experience with SARS, DGMQ highlighted the importance of communication and linkages with partner organizations in both routine and emergency contexts. The program review also noted the importance of risk communication with travelers through travel health recommendations and specific travel alerts. The review presented a long list of the quarantine stations’ accomplishments in fiscal 2003; those that pertain directly to the committee’s findings and conclusions include the following:
-
Met 31 flights arriving from Africa to inspect Liberian and Somali Bantu refugees; met 23 flights with adoptees arriving from China to assess their general state of health and rash illnesses and to facilitate notification of state health departments for medical follow-up.
-
Reviewed or responded to more than 2,000 cases of reported illnesses among travelers arriving in the United States and implemented control measures.
-
Oversaw arrivals of 6,663 immigrants and 36,163 refugees; oversaw shipments of 2,245 nonhuman primates, 1,402 dogs, and 54,268 etiologic agents.
-
Performed or oversaw the performance of 2,077 inspections of maritime vessels for rodent infestation.
Selection of Ports for the New CDC Quarantine Stations
Figure 2.1 illustrates the proposed geographic distribution of CDC quarantine stations at U.S. ports of entry. DGMQ’s plan groups the 25 stations into four regions. Each region will have one station—those in New York, Miami, Chicago, and Los Angeles—with relatively robust capacity. Other stations in the region may draw upon this capacity as needed.
DGMQ used the following criteria to select the cities that have received or will receive a new quarantine station (DGMQ, 2003b):
-
Volume of international human travelers:
-
Airports with >500,000 arriving international air travelers per year.
-
Seaports in major cities with >150,000 arriving international maritime travelers per year.
-
Land crossings in major cities with >10 million arriving international travelers.
-
-
Total volume of human travelers, airports:
-
Airports with >25 million arriving international and domestic air travelers per year.
-
-
Volume of imported wildlife:
-
Major cities that serve as designated or nondesignated ports of entry by the U.S. Fish and Wildlife Service to receive international shipments of wildlife.
-
-
National security considerations:
-
The selected cities are among the 83 so-called Tier 1 U.S. cities, which are believed to be strategic destinations from a national security standpoint (Personal communication, M. Cetron, DGMQ, September 22, 2004).
-
According to fiscal 2002 data gathered by DGMQ, the 25 cities in the expanded system receive around 75 percent of international air travelers arriving in the United States, or approximately 52 million people, and 48 percent of arriving international sea travelers, or 5.9 million people (DGMQ, 2003b). In addition, more than 78 million people enter the United States through the land-border crossings in El Paso, Texas, and San Diego (DGMQ, 2003b). The 25 cities in the expanded system also receive around 32 percent of the maritime cargo annually imported to the United States; this was equivalent to approximately 275 million short tons of cargo in 2003, as illustrated in Appendix D, Table D.6 (1 short ton = 2,000 pounds).
For a complete description of DGMQ’s methodology and data, see Appendix C.
Proposed Workforce for Expanded Stations
DGMQ has proposed a workforce plan to support the activities of 25 CDC quarantine stations at U.S. ports of entry (DGMQ, 2004c). This plan has changed over time; the version presented here dates to July 2004. It appears that, to some extent, DGMQ has begun to act on the plan. Notably, medical officer-epidemiologists have been hired for many of the existing stations, and the title “quarantine public health advisor” has recently replaced “quarantine inspector.” We decided to use the title “inspector” in this report because, for the most part, it still reflects a principal activity of those workers.
The proposed workforce comprises eight full-time equivalents (FTEs) located at the Quarantine & Border Health Services Branch headquarters and 158 FTEs in the field. Headquarters would have a chief, a deputy chief, an administrative officer, a training coordinator, a technical writer-editor, a lead medical officer-epidemiologist, an epidemiologist, and a mathematical statistician.
The four regional stations (Chicago, Los Angeles, Miami, and New York-JFK) would each have eight FTEs: a regional supervisor, a medical officer-epidemiologist, four public health advisors at the GS-11 or GS-12 level, and two public health advisors at the GS-9 level. The remaining 21 stations would have six FTEs each: a lead public health advisor (the station’s supervisor), a medical officer-epidemiologist, three public health advisors at the GS-11 or GS-12 level, and one public health advisor at the GS-9 level. The field medical officer-epidemiologists would report to the lead medical officer-epidemiologist, and the regional supervisors would report to the chief of the Quarantine & Border Health Services Branch.
Field staff would support operations from 8:00 A.M. to 4:30 P.M. on Mondays through Fridays. One or more FTEs would always be on call after hours to provide around-the-clock coverage. It is unclear how many after-hours officers there would be and where they would be located. DGMQ projected that extending the hours of operation to nearly all day, every day, would require a 25 percent increase, or 39 more FTEs.
REFERENCES
Cetron M. 2004. CDC Division of Global Migration and Quarantine. Presentation at the October 21, 2004, Meeting of the IOM Committee on Measures to Enhance the Effectiveness of the CDC Quarantine Station Expansion Plan for U.S. Ports of Entry, Washington, DC.
DGMQ (Division of Global Migration and Quarantine, National Center for Infectious Diseases, Centers for Disease Control and Prevention). 2003a. CDC–History of Quarantine–DQ. [Online] Available: http://www.cdc.gov/ncidod/dq/history.htm [accessed September 20, 2004].
DGMQ. 2003b. Reinventing CDC Quarantine Stations: Proposal for CDC Quarantine Station Distribution. Proposal, September 16, 2003.
DGMQ. 2004a. Program Review Fiscal Year 2003. Program review, May 7, 2004.
DGMQ. 2004b. Proposed Organization Chart. Organizational chart, July 8, 2004.
DGMQ. 2004c. Proposed Organization Chart Breakout. Organizational chart, July 8, 2004.
GAO (United States Government Accountability Office). 2004. Emerging Infectious Diseases: Review of State and Federal Disease Surveillance Efforts. GAO–04–877. Washington, DC: GAO.
Gerberding J, Director, Centers for Disease Control and Prevention. 2005. A Hearing on the Centers for Disease Control and Prevention. Statement at the Apr. 6, 2005 hearing of the Subcommittee on Labor, Health and Human Services, Education and Related Agencies, Committee on House Appropriations, U.S. House of Representatives.
IOM (Institute of Medicine). 2003. Microbial Threats to Health: Emergency, Detection, and Response. Smolinski MS, Hamburg MA, Lederberg J, Editors. Washington, DC: The National Academies Press.
Office of the Public Health Service Historian. 2002. FAQ’s. [Online] Available: http://lhncbc.nlm.nih.gov/apdb/phsHistory/faqs_text.html [accessed January 10, 2005].
OMB (Office of Management and Budget, The Executive Office of the President of the United States). 2004. Budget of the U.S. Government, Fiscal Year 2005. [Online] Available: http://www.whitehouse.gov/omb/budget/fy2005/budget.html [accessed December 9, 2004].
U.S. Congress, House of Representatives, Committee of Conference. 2004. Making Appropriations for Foreign Operations, Export Financing, and Related Programs for the Fiscal Year Ending September 30, 2005, and for Other Purposes: Conference Report to Accompany H.R. 4818. 108th Cong., 2nd Sess. Report 108-792. November 20, 2004.








