
4
Sociodemographic and Community Factors Contributing to Preterm Birth
ABSTRACT
A number of maternal sociodemographic characteristics are associated with an increased risk for preterm birth. Young maternal age, maternal age over 35, and pregnancy for single mothers and those cohabitating outside of marriage (except in countries where cohabitation is common) are associated with an increased risk. As discussed in preceding chapters, there are significant inter- and intragroup variations in the rates of preterm birth. Proposed explanations include socioeconomic condition, maternal behaviors, stress, and infections, and racial differences in genetics. However, these factors do not fully account for the disparities in the rates of preterm birth. In addition to disparities by race and ethnicity, disparities by socioeconomic condition, independent of race-ethnicity, are well documented. Nutrition, cigarette smoking, substance use or abuse, work and physical activity, prenatal care, infection, psychological factors and multiple gestations have been explored but do not fully explain these differences. Examining the context of neighborhoods may be a promising avenue of exploration for explaining disparities in preterm birth because of clear patterns of residential segregation that result in unequal exposures to adverse neighborhood conditions. Although the evidence suggests that after adjustment for individual-level attributes, neighborhood conditions are independently and significantly associated with a risk of low birth weight, evidence regarding the relationship between
neighborhood context and preterm birth specifically is lacking. Further examination of the social contribution to preterm birth may contribute to an understanding of the disparities in the rates of preterm birth among different segments of the U.S. population.
The preceding chapter reviewed the association between individual-level health behaviors and psychosocial characteristics and the risk of preterm birth. In general, studies have not revealed the individual-level risk factors that are strongly and consistently associated with the risk of preterm birth. However, the literature on racial and ethnic disparities in the rates of preterm birth suggests other individual-level characteristics that may be associated with preterm birth and that should be considered. For example, African American women are disproportionately affected by many individual-level conditions that may be associated with preterm birth, such as the higher likelihood of being unmarried, of having lower levels of income and education, and of having poorer prepregnancy health than white women. Thus, it is important to also consider sociodemographic characteristics in relation to preterm birth. These individual-level factors do not occur in isolation. They are embedded in a social context, which also has implications for preterm birth. This chapter addresses both of these issues. The first section addresses sociodemographic characteristics, such as maternal age, marital status and cohabitation, race and ethnicity, and socioeconomic condition. The second section discusses the association between neighborhood conditions and the potential mechanisms through which the neighborhood context may influence reproductive outcomes.
SOCIODEMOGRAPHIC FACTORS
A number of maternal sociodemographic characteristics are associated with an increased risk for preterm birth. This section evaluates the relationships between maternal age, marital status and cohabitation, race and ethnicity, and socioeconomic condition and preterm birth. Possible causes of racial-ethnic and socioeconomic disparities in preterm birth are also explored.
Maternal Age
Several studies have identified young maternal age as an important risk factor for preterm birth (Amini et al., 1996; Branum and Schoendorf, 2005; Fraser et al., 1995; Hediger et al., 1997; Satin et al., 1994; Scholl et al., 1992, 1994). Hediger et al. (1997) found that young adolescents (less than
16 years of age at the time of their last menstrual period), especially those of young gynecological age (within 2 years of menarche), had a twofold greater risk for preterm delivery compared with the risk for older women (ages 18 to 29 years). Using U.S. natality data, Branum and Schoendorf (2005) also found a nearly twofold greater risk of very preterm delivery (less than 33 weeks gestation) among young adolescents (16 years of age or younger) compared with that among young adults (ages 21 to 24 years); the risk decreased with an increase in the age of the adolescent mothers. It is not known at present whether the increased risk of preterm birth among young adolescents is due to their biological immaturity or to an increased prevalence of other risk factors associated with their generally poor socioeconomic condition (Branum and Schoendorf, 2005; Mitchell and Bracken, 1990; Olausson et al., 2001; Scholl et al., 1992).
Women ages 35 and over are also at increased risk for preterm delivery (Astolfi and Zonta, 2002; Cnattingius et al., 1992). Astolfi and Zonta (2002) found in a population sample of Italian women a 64 percent increased odds of preterm delivery among mothers 35 years of age or older compared with that among mother less than 35 years of age when education, birth order, and fetal gender were controlled for. The risk was particularly striking among mothers over 35 years of age delivering their first-born child. The reasons for the increased risk for preterm delivery among older women are not known. By using pooled data for the 1998 to 2000 U.S. birth cohorts from the National Center for Health Statistics (NCHS), the committee identified a similar U-shaped curve that characterizes the relationship between maternal age and preterm delivery (Figure 4-1).
As shown in Figure 4-1, the association between maternal age and the risk of preterm birth is not consistent across racial and ethnic groups. It is observed that the preterm birth rate begins to rise at a younger age for non-Hispanic African Americans (ages 27 to 29) than for non-Hispanic whites (ages 33 to 35), and the slope of the rise with increasing age is greater for African Americans than for whites. Geronimus (1996) attributes this differential rise with increasing age to “weathering.” According to the “weathering” hypothesis, the effects of social inequality on health compound with age, leading to growing gaps in health status between African American and white women through young and middle adulthood that can affect their reproductive outcomes. However, evidence supporting the weathering hypothesis remains inconclusive, as most studies that use cross-sectional data cannot adequately control for potential cohort effects. Further studies on the interaction effects of maternal age and race-ethnicity on preterm birth are needed.
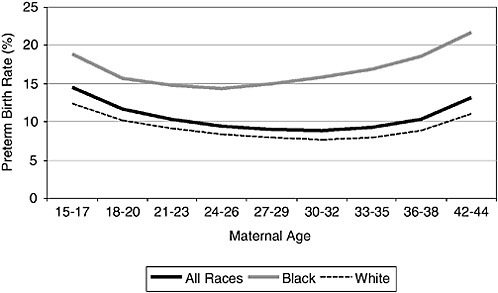
FIGURE 4-1 Relationship between maternal age and preterm birth, by race, 1998 to 2000, U.S. birth cohorts.
SOURCE: NCHS (unpublished data).
MARITAL STATUS AND COHABITATION
Pregnancy in unmarried women has been associated with a higher risk of preterm birth (Blondel and Zuber, 1988; Holt et al., 1997; Luo et al., 2004; Olsen et al., 1995b; Peacock et al., 1995; Raatikainen et al., 2005; Wen et al., 1990; Zeitlin et al., 2002). The rates of preterm birth for unmarried and married women were determined by using NCHS data for the 1998 to 2000 U.S. birth cohorts. As shown in Table 4-1, preterm birth rates are higher for unmarried women than for married women across all racialethnic and age groups.
The reasons for the higher rates of preterm birth among unmarried mothers are not known but are commonly attributed to their relative lack of social support and resources (Raatikainen et al., 2005; Waldron et al., 1996). The protective effects of marital status, however, are not uniform across racial-ethnic and age groups; the data in Table 4-1 suggest that marital status appears to offer the greatest protection against preterm birth among older (35 years of age or older) women and non-Hispanic African Americans.
Approximately 40 percent of births that occur outside of marriage now occur to cohabiting couples (CDC, 2000), and the rates of cohabitation have been increasing in the United States within the last few decades. Sev-
TABLE 4-1 Preterm Birth Rates (percent) for Married and Unmarried Women, by Maternal Age and Race-Ethnicity, 1998 to2000
|
Age |
Non-Hispanic African American |
Non-Hispanic Whites |
Asians-Pacific Islanders |
Americans Indians |
Hispanics |
|||||
|
Married |
Unmarried |
Married |
Unmarried |
Married |
Unmarried |
Married |
Unmarried |
Married |
Unmarried |
|
|
<20 |
13.7 |
17.6 |
10.4 |
11.5 |
12.4 |
14.3 |
10.3 |
12.8 |
10.6 |
12.7 |
|
20–34 |
13.7 |
16.7 |
7.9 |
10.8 |
8.3 |
11.9 |
10.2 |
12.0 |
9.1 |
11.0 |
|
≥35 |
16.2 |
22.9 |
8.6 |
14.0 |
9.9 |
14.0 |
13.4 |
16.0 |
11.5 |
14.2 |
|
SOURCE: NCHS data for U.S. birth cohorts from 1998 to 2000. |
||||||||||
eral studies have examined the relationship between cohabitation outside of marriage and preterm birth (Blondel and Zuber, 1988; Manderbacka et al., 1992). A collaborative case-control study in 16 European countries found that a significantly elevated risk of preterm birth was associated with cohabitation compared with the risk for those who are married (although the odds of preterm birth were substantially lower for women who cohabit with their partners than for single mothers) in countries where less than 20 percent of births occur outside of marriage. In contrast, no excess risk was associated with marital status in countries where out-of-marriage births were more common (Zeitlin et al., 2002). A population-based study in Quebec (where 44 percent of births were to common-law mothers in 1997) found the preterm birth rate among mothers in common-law unions to be higher than that among mothers in traditional marriage relationships but still lower than that among unmarried mothers living alone (Luo et al., 2004). The adjusted odds ratios for preterm birth were 1.14 and 1.41 for common-law and single mothers living alone, respectively, when individualand community-level characteristics were controlled for. A large hospital cohort study in Finland also found a higher risk of preterm birth among single women than married women (adjusted odds ratio = 1.29), with the risk of cohabiting women being somewhere in between (adjusted odds ratios = 1.15) (Raatikainen et al., 2005).
Race and Ethnicity
Preterm birth rates vary substantially by race and ethnicity in the United States (CDC, 2005i). As discussed in Chapter 1, there are significant interand intragroup variations in the risk of premature birth. For example, in 2003 the preterm birth rates among Hispanics ranged from 11.7 percent for Mexicans to 13.8 percent for Puerto Ricans. Preterm birth rates also varied by nativity and duration of residence. In 2003, the preterm birth rate was 13.9 percent for foreign-born blacks but 18.2 percent for U.S.-born African Americans (CDC, 2005i). Even the duration of residence seems to have an effect on preterm birth rates. A study in California found that long-term Mexican immigrants who had lived in the United States for more than 5 years were more likely to deliver preterm infants than newcomers who had lived in the United States for 5 years or less (Guendelman and English, 1995). In general, the literature examining potential causes of racial and ethnic disparities in preterm births is not well developed. Investigations of the effects of nativity are even less developed.
These racial-ethnic disparities have persisted for decades, although the precise reasons are not clear. A number of explanations have been proposed, including racial differences in socioeconomic condition, maternal
TABLE 4-2 Preterm Birth Rates (percent) by Maternal Race-Ethnicity and Educational Attainment, 1998 to 2000
|
Educational Attainmenta |
Non-Hispanic African Americans |
Non-Hispanic Whites |
Asians-Pacific Islanders |
American Indians |
Hispanics |
|
<8 |
19.6 |
11.0 |
11.5 |
14.8 |
10.7 |
|
8–12 |
16.8 |
9.9 |
10.5 |
11.8 |
10.4 |
|
13–15 |
14.5 |
8.3 |
9.1 |
9.9 |
9.3 |
|
≥16 |
12.8 |
7.0 |
7.5 |
9.4 |
8.4 |
|
aEducational attainment indicates the number of years of school completed. SOURCE: NCHS data for U.S. birth cohorts from 1998 to 2000. |
|||||
behaviors, stress, infections, and genetics (reviewed by Lu and Halfon [2003]).
Conventional wisdom often regards race as a proxy for socioeconomic condition, and some believe that socioeconomic factors (often measured in terms of educational attainment, household income, or occupational status) explain differences in preterm birth rates by race. African American women, on average, are more socioeconomically disadvantaged than non-Hispanic white women (Oliver and Shapiro, 1995), and a poorer socioeconomic condition is associated with an increased risk for preterm birth. However, in most studies the differences in preterm birth rates (McGrady et al., 1992), birth weights (Collins and Hawkes, 1997; Shiono et al., 1997), and infant mortality rates (Schoendorf et al., 1992) between African American and white women persisted after adjustment for (measured) socioeconomic differences. Furthermore, socioeconomic condition does not confer equal protection across racial-ethnic groups, as shown in Table 4-2.
For example, although within each racial-ethnic group the risk of preterm birth decreases with an increasing level of educational attainment, African American women with more than 16 years of education still have substantially higher preterm birth rates than non-Hispanic white women with less than 9 years of education. Although it is possible that the residual disparities result from misclassification error, measurement error, aggregation bias, or some unmeasured aspect of socioeconomic condition (Kaufman et al., 1997), these studies suggest that differences in socioeconomic conditions cannot fully account for racial disparities in preterm birth rates.
Another popular explanation holds maternal risk behaviors responsible for the racial disparities in preterm birth, such as smoking or drug use. However, several studies have found, albeit by self-report, that proportion-
ately fewer African American women than white women smoke cigarettes during pregnancy (Beck et al., 2002; Lu et al., 2005). Similarly, the reported prevalence of alcohol and drug use among pregnant African American women appears to be no greater than that among pregnant white women (Serdula et al., 1991). Although it is possible that studies may not have considered all risk behaviors (e.g., douching) or interactions between race and behaviors, a few studies have concluded that the contributions of behavioral risk factors during pregnancy to racial disparities in birth outcomes such as preterm birth or low birth weight appear to be modest (Goldenberg et al., 1996a).
Similarly, the delayed and inadequate use of prenatal care among African American women has been identified as an important risk factor for the excess adverse birth outcomes among African American infants, including preterm birth. The expectation that increased access to and use of prenatal care will improve birth outcomes and reduce disparities has shaped national policy for nearly 2 decades (IOM, 1985); however, the effectiveness of prenatal care for the prevention of preterm birth has yet to be demonstrated conclusively (Alexander and Kotelchuck, 2001). A recent review concluded that the standard prenatal care provided today does little that could be expected to reduce preterm birth rates (Lu and Halfon, 2003), and the substantial increased use of early and adequate prenatal care over the past decade has not led to a significant decline in preterm birth rates for either African American or white women (CDC, 2005i). By using NCHS data for the 1998 to 2000 birth cohort, it was found that non-Hispanic African American women who initiated prenatal care in the first trimester or who had adequate prenatal care still experienced higher rates of preterm birth than non-Hispanic white women (Table 4-3).
TABLE 4-3 Preterm Birth Rates (percent) by Maternal Race-Ethnicity and Prenatal Care Use by Trimester of Initiation of Prenatal Care, 1998 to 2000
|
Trimester |
Non-Hispanic African Americans |
Non-Hispanic Whites |
Asians-Pacific Islanders |
American Indians |
Hispanics |
|
First |
14.7 |
8.3 |
8.6 |
10.4 |
9.7 |
|
Second |
17.5 |
10.2 |
10.8 |
12.7 |
11.0 |
|
Third |
16.0 |
10.0 |
9.5 |
12.3 |
10.0 |
|
No prenatal care |
33.4 |
21.7 |
19.4 |
24.0 |
19.8 |
|
SOURCE: NCHS data for U.S. birth cohorts from 1998 to 2000. |
|||||
Over the past decade, two risk factors have emerged as promising explanations for the racial disparities in preterm birth rates: stress and infection. As reviewed in Chapter 3, a growing body of research suggests that maternal psychological stress is associated with an increased risk for preterm delivery. Insofar as African American women may experience more stress in their daily lives than white women, it has been suggested that maternal stress may contribute to the disparities in preterm birth rates between African American and white women (James, 1993). For example, Lu and Chen (2004) reported that African American women were significantly more likely to experience stressful life events (e.g., to lose a job or to become separated or divorced) just before or during pregnancy than non-Hispanic white women. As discussed in Chapter 3, African American women are also more likely to experience racism, which can be conceptualized as an additional source of stress (Krieger, 2000).
African American women are more likely than white women to experience a number of infections, including bacterial vaginosis and sexually transmitted infections (Fiscella, 1995; Meis et al., 2000). Insofar as these infections are associated with preterm delivery, they may be responsible for a significant portion of the racial disparities in preterm birth rates (Fiscella, 1995). However, the cause of this increased susceptibility to infections among pregnant African American women remains largely unknown, and to date antibiotic treatment of infections (other than for asymptomatic bacteriuria) during pregnancy has yielded modest or no benefits (Carey et al., 2000; McDonald et al., 2005) (see Chapter 9).
Genetic differences have often been invoked to account for racial disparities in a number of birth outcomes, including preterm birth. Although a woman’s genetic makeup undoubtedly plays a role in the pathogenesis of preterm birth, the potential genetic contribution to racial disparities in preterm birth is unknown. First, it is not known which genes contribute to racial disparities in preterm birth rates. For example, interleukin-6 (IL-6), gamma interferon (IFN-γ), and tumor necrosis factor alpha (TNF-α) have all been implicated in the pathogenesis of preterm birth. Although several population-based studies have shown that African Americans are more likely than whites to carry genotypes that induce a high level of expression of IL-6 (Cox et al., 2001; Hassan et al., 2003; Hoffmann et al., 2002), the findings for IFN-γ and TNF-α are less consistent; in some studies the prevalence of individuals with genotypes that induce high levels of expression of these two proinflammatory cytokines was actually lower among African Americans than whites (Cox et al., 2001; Hassan et al., 2003; Hoffman et al., 2002). Second, it is not known how genes interact with the environment to produce racial disparities in preterm birth. Geneticists recognize that the causes of most common,complex diseases and conditions, including preterm birth, consist of a complicated interaction between genes and the environ-
ment (Macones et al., 2004; Wang et al., 2002). To date, few studies on preterm birth have untangled this interaction in the context of racial disparities (see Chapter 7). Third, it is not known why foreign-born and U.S.-born women of the same racial descent have such disparate rates of preterm birth, given their supposedly common genetic ancestry. The genetic contributions to racial-ethnic disparities in preterm birth are discussed in greater detail in Chapter 7.
In sum, significant racial-ethnic disparities in preterm birth rates exist in the United States. Racial differences in socioeconomic condition, maternal behaviors (including the use of prenatal care), stress, infection, and genetics cannot fully account for the disparities. More research, perhaps performed by the use of a more integrative approach (Lu and Halfon, 2003; Misra et al., 2003; NRC, 2001), is needed to address this persisting problem. As discussed in the introduction, the greatest difference in rates of preterm birth are between African American and Asian/Pacific Islander women. There could be something learned by understanding those differences as well as differences among Asian subgroups. Although the rates among African American women are strikingly high, they have been decreasing in recent years. In contrast, rates among other racial/ethnic groups have been increasing slightly. Examining these trends or differences may potentially help to shed light on racial and ethnic disparities.
Socioeconomic Condition
Disparities in preterm birth rates by socioeconomic condition have been well documented (Kramer et al., 2000) not only in the United States (Parker et al., 1994a but also in countries such as Canada (Wilkins et al., 1991), Sweden (Koupilova et al., 1998), Finland (Olsen et al., 1995b), Scotland (Sanjose et al., 1991), and Spain (Rodriguez et al., 1995), where the rates of poverty are generally lower than elsewhere in the world and women generally have universal access to high-quality prenatal and other medical care. Although the disparities in preterm birth rates by socioeconomic condition are often closely paralleled (and hence confounded) by disparities by racial and ethnic origin, there are notable exceptions. For example, despite their relative socioeconomic disadvantage, Mexican Americans have preterm birth rates comparable to those of non-Hispanic whites (Table 4-2) (CDC, 2005i).
The reasons for socioeconomic disparities in preterm birth rates are unclear and have been relatively unexplored. A number of factors have been implicated, including maternal nutrition, cigarette smoking, substance use or abuse, work and physical activity, prenatal care, genitourinary tract infection, sexually transmitted diseases, psychological factors, and multiple gestations. A general discussion of these risk factors as they relate to preterm
birth is found in Chapters 3 and 5. Kramer and colleagues (2000) reviewed these factors as potential mediators of socioeconomic disparities in preterm birth, and that review is briefly summarized here.
Maternal nutritional status before and during pregnancy may contribute to the risk for preterm birth (WHO, 1995). Women with a low prepregnancy body mass index (BMI) are at increased risk for preterm birth. In the United States, however, BMIs are higher among women who are socioeconomically disadvantaged (Flegal et al., 1988); therefore, the prepregnancy BMI cannot account for socioeconomic disparities in preterm birth rates. Recent evidence suggests that maternal obesity before pregnancy is associated with an increased risk for indicated preterm delivery but with a decreased risk for spontaneous preterm delivery (Hendler et al., 2005); the contribution of maternal obesity to the disparities in preterm birth by socioeconomic condition is not clear. Low gestational weight gain is more common among socioeconomically disadvantaged women (Taffel, 1980); however, because of its modest association with preterm birth, low gestational weight gain is unlikely to be an important mediator of socioeconomic disparities in preterm birth rates (Carmichael and Abrams, 1997). Nutritional intake during pregnancy is generally poorer among socioeconomically disadvantaged women; however, given the weakness of the available evidence linking macro- and micronutrient intakes to preterm birth (Villar et al., 2003a,b), their role in explaining the socioeconomic disparities in preterm birth rates remains unclear.
In the United States, cigarette smoking is more prevalent and heavier among socioeconomically disadvantaged women, and as the adverse effects of smoking during pregnancy have become widely recognized by the general public, the socioeconomic gradient in the rates of cigarette smoking has widened. Cigarette smoking appears to explain some of the socioeconomic disparities in preterm birth, given its higher prevalence among socioeconomically disadvantaged women and its association with preterm birth (Kramer et al., 2000).
Although cocaine use is more common among socioeconomically disadvantaged women and is associated with preterm birth, it has a small etiological effect on preterm birth and thus is unlikely to be an important mediator. In poor, inner-city areas in the United States, however, the prevalence of cocaine use may be high, and in these settings, the mediating role of cocaine use is likely to be more important. Marijuana, alcohol, and narcotic use are also more common among socioeconomically disadvantaged women in the United States, although their independent effects on gestational duration are not clear (Kramer et al., 2000).
Work that is physically demanding, work that requires standing for prolonged periods, shift and night work, or work that creates high levels of cumulative fatigue has been associated with an increased risk for preterm birth (Mozuekewich et al., 2000); and socioeconomically disadvantaged
women are more likely to have jobs with these characteristics. However, the etiological effect of these types of work on preterm birth is not known. Even less clear are the contributions of physically demanding work in the home (Pritchard and Teo, 1994) and the stress associated with unemployment or underemployment (Lu et al., 2005).
The rate of use of prenatal care is lower among socioeconomically disadvantaged women (CDC, 2005i); however, given the serious doubt about the effects of prenatal care on reducing the risk of preterm birth (Alexander and Kotelchuck, 2001; Lu and Halfon, 2003), prenatal care also seems to be an unlikely mediator of socioeconomic disparities in preterm birth rates.
Bacterial vaginosis is more common among socioeconomically disadvantaged women (Hillier et al., 1995; Meis et al., 1995). Given its association with preterm birth, it could be an important mediator of socioeconomic disparities in preterm birth rates. However, clinical trials of screening for and treatment of bacterial vaginosis have yielded conflicting results (Carey et al., 2000; McDonald et al., 2005) (see Chapter 9). The potential role of genitourinary Chlamydia trachomatis infection in spontaneous preterm birth has remained controversial, and studies of this and other sexually transmitted infections have generated conflicting results (Andrews et al., 2006).
Socioeconomically disadvantaged women experience more stressful life events and more chronic stress (Lu et al., 2005; Peacock et al., 1995). Poverty is associated with poor and crowded housing, living without a partner, unsatisfying marital relationships, violence from an intimate partner, and stressful working conditions. Unintended pregnancies are far more common among socioeconomically disadvantaged women. They also have less social support to limit the impacts of those stressors. Thus, psychosocial factors may prove an important mediator of socioeconomic disparities in preterm birth rates, but their etiologic links with preterm birth require further clarification.
Although socioeconomic differences in multiple gestations have not been well studied, Kramer and colleagues speculate that indirect evidence of increased multiple births attributable to infertility treatment among women in high socioeconomic groups, coupled with the growing contribution of multiple births to the overall incidence of preterm birth, will narrow socioeconomic disparities (Kramer et al., 2000).
Summary of Sociodemographic Factors
A number of maternal sociodemographic characteristics are associated with higher rates of preterm delivery. Specifically, maternal age (less than 16 years of age or 35 years of age or older), marital status (unmarried or cohabiting), race or ethnicity (African American or American Indian), and socioeconomic condition (low income or educational attainment) have been
identified as risk factors for prematurity. Most of these sociodemographic factors are closely intertwined with behavioral risk factors, such as smoking and physical activity, and to psychosocial processes, such as stress, discrimination, and social support (see Chapter 3).
Finding 4-1: A particular focus of sociodemographic studies of preterm birth should be on disparities by race-ethnicity and socioeconomic condition, as significant differences in the rates of preterm birth by race-ethnicity and socioeconomic condition continue to exist in the United States. The causes of these persisting disparities remain largely unexplained
COMMUNITY FACTORS
In general, the risks for preterm birth have been individualized; that is, those characteristics of individuals that increase the likelihood of preterm delivery within groups rather than the environmental and social factors that affect the rates of preterm birth among the population as a whole (Goldenberg et al., 1998) are emphasized. However, as discussed in Chapter 3 and the previous section on sociodemographic factors, observational studies do not consistently demonstrate strong associations between the characteristics of the individual and the risk of preterm birth, nor do these individual-level characteristics explain the racial-ethnic differences in the rates of preterm birth.
Some scholars argue that the study of discrete risk factors has led to a rather narrow, static view of perinatal risk assessment (Konte et al., 1988; Main and Gabbe, 1987). In practice, individual risk factors tend to cooccur, resulting in dynamic interactive or synergistic processes that may reflect complex biological mechanisms (Casey and MacDonald, 1988; Challis, 1994; Olson et al., 1995; Petraglia et al., 1996; Romero et al., 1994). Such complex processes may render the contribution of a single risk factor somewhat meaningless. Furthermore, analytic problems arise when individual risk factors have different predictive powers for different populations (Geronimus, 1996; James, 1993; Kleinman and Kessel, 1987), making it difficult to make meaningful adjustments for confounders in studies involving multiple racial groups and resulting in potentially biased estimates of effect (Kaufman et al., 1997).
Several theories exist for the reasons that the identified risk factors do not adequately explain the racial-ethnic and social class disparities in rates of preterm birth. Among these is the idea that adverse social contexts, such as neighborhood conditions, may independently affect health or interact with individual-level characteristics to produce an increased risk of preterm
birth. Against this backdrop, some researchers have redirected attention to consideration of the social determinants of reproductive health, calling for new approaches that go far beyond traditional medical risk assessment models and individual-level poverty-driven paradigms to include contextualized research (Holzman et al., 1998; Krieger et al., 1993; Link and Phelan, 1995; Rowley et al., 1993; Susser and Susser, 1996).
Adverse Neighborhood Conditions
The notion that adverse neighborhood conditions influence health outcomes through direct and indirect pathways has recently received increased attention (Robert, 1999). Evidence supporting the contributing role of neighborhood conditions is presented in this section. An important note is that the studies conducted thus far use birth weight as an outcome. A major need in future work is to examine gestational age as well. Neighborhood context may be a fruitful and salient avenue of exploration for explaining differences in preterm birth rates between African American and white women because of clear patterns of residential segregation that result in unequal exposures to adverse neighborhood conditions across racial-ethnic groups. Concentrated poverty and associated neighborhood disadvantages (including a lack of goods and services, health care facilities, and recreational opportunities; poor housing quality; and high crime rates) are more common features of African American neighborhoods than of white neighborhoods (Massey and Denton, 1993; Wilson, 1987). Residents of disadvantaged areas, in turn, not only are at a greater risk of physical injury but also are exposed to higher levels of everyday life stressors.
The social environment, service environment, and physical characteristics of a neighborhood have been hypothesized to affect the health of its residents (Konte et al., 1988). Social environment refers to the level of neighborhood cohesion or disorganization, norms of reciprocity, civic participation, crime, socioeconomic compositions, residential stability, and related attributes. These characteristics are thought to influence health outcomes through pathways such as the availability of social support, the adaptation of coping strategies, and exposure to chronic stress (Casey et al., 1988; Challis, 1994; Geronimus, 1996; Olson et al., 1995; Petraglia et al., 1996; Romero et al., 1994).
The service environment reflects the availability of goods and services, such as access to quality health care, grocery stores, recreational facilities, and police and fire protection. The availability of such services is likely to be affected by the degree of political organization influencing residents’ ability to demand public services and recruit private service providers to their neighborhoods. Poor public and private services may have direct and indirect impacts on an individual’s health by making residents more suscep-
tible to intentional and unintentional injuries; by limiting access to quality health care, healthy foods, and recreational opportunities; and by increasing crime rates (Holzman et al., 1998; James, 1993; Kleinman and Kessel, 1987; Konte et al., 1988; Mercer et al., 1996). One study of the distribution of food stores found significantly fewer (three to four times) supermarkets in poor and African American communities than in more affluent white communities (Kramer, 1987a).
Finally, the quality of the physical environment and the quality of the housing stock and public space could also have direct effects on health (Main et al., 1987; Olson et al., 1995). Factors that affect the quality of the physical environment include toxicants, noise, and air pollution to which a pregnant woman may be exposed
The concentration of adverse neighborhood conditions along all three dimensions discussed above is often closely tied to the clustering of socioeconomic disadvantage. A number of studies have documented a significant association between neighborhood-level socioeconomic disadvantage and birth outcomes (Cramer, 1995; Kaufman et al., 1997; Krieger et al., 1993). Collins and David (1990) documented variations in the rates of low birth weight in Chicago, Illinois, in 1982 and 1983 among neighborhoods classified by the census-tract median family income. Their results show that in univariate comparisons, the risks of low birth weight for the infants of high-risk African American and white women (whose risk was assessed by measurement of age, level of educational attainment, and marital status) were more similar in poor neighborhoods than in more affluent areas. Lowrisk white women had much lower rates of low birth weight than low-risk African American women, no matter where they lived. In a related study of an association between violent crime and low birth weight in Chicago’s low-income neighborhoods, defined as census tracts with a median family income of less than $10,000, the same authors found a significant association between the risk of intrauterine growth retardation and the level of violent crime (Collins and David, 1997).
Using 1990 birth record data for Chicago linked to 1990 census data on community-level measures of socioeconomic condition, residential stability, the racial compositions of neighborhoods, and selected housing characteristics, Roberts (1997) modeled the incidence of low birth weight by including individual-level and community-level characteristics in a multivariate logistic regression analysis. The findings indicated that women living in economically disadvantaged communities were more likely to have a low birth weight baby than women living in better off neighborhoods, when individual characteristics available on the birth certificate were controlled for. Several counterintuitive findings were also noted. For example, the percentage of community residents who were African American was inversely associated with low birth weight, as was the rate of crowded housing units,
when individual-level determinants and community-level economic status were controlled for. Racial differences in the rates of delivery of low-birth-weight infants remained substantial, however, with African American mothers being about twice as likely to deliver a low-birth-weight infant than white mothers, even after individual- and community-level factors were taken into account (Roberts, 1997, Table 2).
Nested data structures are common meaning that individuals operate within multiple realities such as the household, the neighborhood, the city or town, and the state. Another classic example of nested date derives from the educational world with students, within classrooms, within schools, within neighborhoods, etc. Following the educational example, we can assume that the students within a certain class share common characteristics such as the teacher and the physical surroundings and therefore they are not independent. In other words, students within a specific class are more alike than a random sample of students drawn from the larger population. Given that many statistical techniques require that observations are independent, nested data poses challenges. Until recently nested data would have to be aggregated or disaggregated prior to analyses so that only one level of the data was being assessed (e.g., students, or classrooms or schools but not students, classrooms, and schools). Now, however, nested data can be analyzed using hierarchical linear models or multilevel models. Multilevel models permit the simultaneous assessment of the association between nested data and an outcome of interest.
O’Campo and colleagues (1997) were among the first scientists to use multilevel models to investigate the effects of maternal characteristics and neighborhood conditions on the risk of low birth weight in Baltimore, Maryland, using data recovered from 1985 to 1989 in a multilevel framework. Controlling for individual-level characteristics, which included maternal age, education, prenatal care use, and health insurance coverage, the authors found that women living in census tracts with per-capita incomes of less than $8,000 had a significantly higher risk of delivering an infant of low birth weight than women who lived in higher-income census tracts. They also found a number of significant interactions between neighbor-hood-level variables and individual-level risk factors for low birth weight. The protective effects of prenatal care, for example, were less strong in neighborhoods with high levels of unemployment, and the elevated risk of low birth weight among women with low levels of schooling was stronger in tracts with higher crime rates. They did not investigate whether these effects varied by race or whether the contextual and individual-level variables explained racial differences in low birth weight.
Pearl and colleagues (2001) conducted a multilevel analysis of the impact of socioeconomic status (SES) on birthweight. SES was measured at the individual level as maternal education, Medi-Cal coverage during preg-
nancy, and family income. Neighborhood SES was measured by dividing the sample into census tracts and blocks, in which they selected poverty, unemployment, and education as specific SES indicators. Latinas and Asian women were subdivided into U.S. and foreign born. Findings suggest that neighborhood SES was unrelated to the birth weights of children born to white women and U.S.-born Latinas, whereas it was related to a decrease in birth weight among blacks and Asians. Furthermore, foreign-born Latinas living in neighborhoods with high unemployment and poverty delivered infants of higher birth weights and had a lower risk of delivering a low birth weight infant. These findings suggest that both individual and neighborhood level pathways are important, as well as their interactions with ethnicity and nativity.
Elo and colleagues (2001) analyzed linked birth and infant death records in Philadelphia, Pennsylvania, to investigate the effects of individual-and contextual-level variables on birth weight (in grams) and the risk of low birth weight using both fixed-effects and random-effects models. The authors also tested whether their results were sensitive to the level of neighborhood aggregation used; that is, block groups, census tracts, or larger neighborhood aggregations. Using fixed-effects models, the authors found that about a third of the racial difference in birth weight and the risk of low birth weight was explained by the neighborhood context and the characteristics shared by women living in the same neighborhood. The difference was further narrowed when the individual-level characteristics of the women and their births were controlled for. The reduction in the racial difference was greater when neighborhoods were conceptualized as block groups and was somewhat less pronounced when neighborhoods were defined as larger aggregates. The fact that the neighborhood context explained a part of the racial difference in birth weights points to the importance of including neighborhood characteristics in models of birth outcomes. Of the neighborhood-level characteristics examined (income, poverty, education, occupation, health status, household composition, migration, housing, crime, and homelessness), indicators of neighborhood economic deprivation and crime were the most consistently associated with birth weight and the risk of low birth weight.
Research in perinatal health demonstrates modest but consistent effects of neighborhood-level socioeconomic disparities in key pregnancy outcomes (Geronimus, 1996; James, 1993; Kleinman and Kessel, 1987). Low birth weights have been associated with a variety of neighborhood-level socioeconomic variables, including poverty (Cramer, 1995; Geronimus, 1992; Kaufman et al., 1997), unemployment (Geronimus, 1992), education and income (Geronimus, 1992; Kaufman et al., 1997; Krieger et al., 1993), and median rent (Kaufman et al., 1997). In addition to single-variable associations, neighborhood indices representing aspects of economic disadvantage
have also been associated with low birth weight. For example, Buka and colleagues (2003) created an index measure of neighborhood economic disadvantage using, among other variables, the percentages of individuals in a neighborhood living below the poverty level according to 1990 census data, receiving public assistance, and being unemployed and found the index to be significantly associated with birth weight. Krieger and colleagues (2003) used multiple indices to assess area-level effects on low birth weight and child lead poisoning, with tract and block group measures of economic deprivation observed to have the strongest effects on low birth weight (odds ratio > 2.0). Although research results have consistently confirmed the effects of neighborhood deprivation on adverse birth outcomes, these findings can be difficult to interpret and compare, owing to the variety of indicators used to measure neighborhood-level deprivation.
Although most studies have documented an association between neighborhood context and health outcomes, whether they are for adults or infants, additional research is needed to more fully specify and test these associations. Future work needs to (1) focus on how best to define context, e.g., whether the context should be administrative or political units or some alternative specifications of neighborhood boundaries; (2) include contextual variables defined at various levels of aggregation on the basis of theoretical considerations, e.g., crime at the block group or smaller levels of aggregation versus service availability at tract or larger levels of aggregation; (3) integrate adequate individual-level information to ensure that neighborhood variables do not reflect individual-level differences; (4) test interactions across levels; and (5) explore various analytical techniques to model the effects of space on health outcomes. In addition, as discussed above, most studies have used birth weight as an outcome, thus confounding with small for gestational age (see Chapter 2). Studies should also use gestational age to investigate prematurity. There are likely different mediators, moderators, and pathways to preterm birth than there are to low birth weight. Using preterm birth as a discrete outcome may not reveal effects. Gestational age should be studied as a continuous variable.
Regardless of how neighborhood-level characteristics are measured, multilevel research has helped to draw attention to the role of social structures in health, particularly with respect to the problem of persistent health disparities. However, as recently reviewed by Oakes (2004), very few such studies have attended to the question of causal inference or recognized that neighborhood effects may not be truly independent effects. Oakes suggests that future multilevel studies make use of social experimental designs to provide a better understanding of the underlying causal processes and to use this understanding to design interventions that more effectively reduce risk and improve public health. Specifically, Oakes suggests that the benefits of studying the independent effect of neighborhood conditions on
health are really only realizable through the design, implementation, and rigorous evaluation of randomized clinical trials where a “community-level” treatment is delivered to a randomly selected set of communities. As examples, Oakes suggests community interventions that alter norms with mass media public health messages, change local policies, add green space or clean existing parks, repair sidewalks, or institute community policing strategies. However, Oakes cautions that these types of interventions are very expensive, are hard to evaluate given the long latency between exposure and disease and, most significantly, are hard to design given our limitations in theories linking neighborhoods to health. Given the complex relationships between health and social conditions, this type of methodology might be very productively applied in the field of perinatal epidemiology.
Interaction Between Neighborhood- and Individual-Level Characteristics
Neighborhood-level characteristics may indirectly exert their influence on reproductive outcomes by patterning individual-level economic opportunities and health behaviors. For example, the neighborhood-level opportunity structure may restrict or facilitate access to schooling, training programs, and employment opportunities and thus influence reproductive outcomes through the socioeconomic condition that a woman has attained (Anderson et al., 1996; Konte et al., 1988). Thus, disparities in birth outcomes according to a woman’s socioeconomic condition may originate in part from the neighborhood context that shape an individual’s life chances.
Furthermore, the social characteristics of neighborhoods, perhaps through shared cultural norms and values, may well influence health behaviors that are linked to reproductive outcomes. For example, individual-level smoking patterns (Cubbin et al., 2000; Diez-Roux et al., 1997), alcohol consumption, and dietary practices (Macintyre et al., 2002; Shepard, 1994; Taylor and Repetti, 1997; Yen and Kaplan, 1999; Yen and Syme, 1999), which seem particularly relevant to this discussion, have been significantly associated with area-level deprivation when individual attributes are controlled for. In addition to health behaviors, adverse conditions such as high crime rates, housing abandonment, and even noise pollution may act as either acute or chronic stressors that exert their influences through stress physiology and are thus potential intervening mechanisms between neighborhood context and reproductive health. Geronimus (1996), for example, has argued that long-term exposure to socioeconomic disadvantage, including residence in socioeconomically disadvantaged neighborhoods, is detrimental to maternal reproductive health and is one of the factors that contributes to more adverse birth outcomes among African American women (O’Campo et al., 1997).
Finally, neighborhood context and individual-level characteristics may
interact such that individual-level characteristics may exert a greater influence in certain neighborhoods or such that the effects of the neighborhood context are more pronounced for subgroups of women stratified by socioeconomic condition, race-ethnicity, or other individual attributes. For example, a recent study in Chicago found that high perceived levels of neighborhood support were positively associated with birth weight only for white infants. A significant negative association between birth weight and neighborhood-level economic disadvantage was documented for African American infants (Buka et al., 2003). This association remained significant even after adjustment for maternal characteristics and other neighborhood conditions (Casey and McDonald, 1988). O’Campo and colleagues (1997) found that the early initiation of prenatal care did not have the same beneficial effect for women living in disadvantaged neighborhoods in Baltimore, raising the possibility that prenatal care in deprived settings is unable to address various risks associated with adverse birth outcomes (Holzman et al., 1998; Kaufman et al., 1997). Evidence also suggests that prenatal care has no effect on preterm birth (see Chapter 9 for a discussion).
Effect modification in multilevel models also occurs. This type of effect modification is perhaps most difficult to conceptualize and test because it implies a kind of cross-level effect by which individual-level effects are moderated by community-level conditions. This would mean, for example, that the effect of cigarette smoking on an individual’s risk of preterm birth would depend on some attribute of the community in which that individual resides. This effect modification would not be explained by interactions with other individual-level psychological or social exposures. In a study of community characteristics and child maltreatment, The Project on Human Development in Chicago Neighborhoods found that neighborhood social networks interacted with Hispanic ethnicity to affect the amount of physical abuse committed by individual families (Molnar et al., 2003). The authors interpreted this finding to make the point that neighborhood-level interventions may be the most effective way to reduce rates of the child abuse in certain populations. Such findings suggest that studies that examine factors at only one level (either the individual level only or the ecological level only) may underestimate the effects of the social environment and potentially miss an opportunity to use interventions to the reduce risk associated with any particular factor.
Biological Mechanisms
Exposure to acute and chronic stress is one of the hypothesized pathways through which neighborhood context may affect birth outcomes. At the individual level, a growing body of empirical evidence, based on methodologically rigorous studies of pregnant women of different racial-ethnic,
socioeconomic, and cultural backgrounds, supports the premise that mothers experiencing high levels of psychological or social stress during pregnancy are at significantly increased risk for preterm birth (relative risk = 1.5 to 2.0), even after adjustment for other biomedical, sociodemographic, and behavioral risk factors (Pearl et al., 2001; Rauh and Culhane, 2001). In addition, adverse neighborhood conditions, such as crime, homelessness, and tax delinquency, were significantly associated with the risk of urogenital tract infection, one of the leading causes of preterm birth (Collins and David, 1997; Roberts, 1997), during pregnancy, even after adjustment for individual-level risk factors (Elo et al., 2001).
Stress both at the individual level and at the neighborhood level may affect preterm birth through physiological pathways (see Chapter 6 for a discussion). The plausibility of the influences of the direct neuroendocrine and the neuroendocrine-immune interaction pathways suggests that stressful exposures may have physiological consequences over and above their possible influences on health-related behaviors. As evidence accumulates that individual-level stressful exposures can become annoying (“get under the skin”), it is not hard to imagine that dangerous and rundown neighborhoods may exert a similar effect. It is therefore possible that neighborhoods can influence health outcomes through direct physiological dysregulation.
Methodological Issues in Modeling Social Context
The inclusion of social conditions in models of cumulative risk depends on the ability to validly measure the various components of social context at appropriate scales of influence. In their simplest form, multilevel studies typically include assessments at the individual and community levels by the use of some standard administrative unit to define community (e.g., health area, zip code, census tract, or block). For example, exposure to poverty or substandard housing may be measured at the individual level (personal income, number of homeless episodes, etc.) and the community level (average income in the census tract, amount of concentrated poverty, proportion of imminently dangerous buildings, etc.).
Advances in statistical analysis techniques that facilitate the modeling of multilevel influences and the growing interest in the use of geographic information systems have made analyses of community- and regional-level variations more feasible (Bellinger, 2004; Diez-Roux, 1999; Kawachi, 2000; Link and Phelan, 1995). A recent review of articles published before 1998 of the effects of local-area social characteristics on various individual health outcomes in developed countries found that all but 2 of the 25 studies reviewed reported a statistically significant association between at least one measure of the social environment and a health outcome, after adjustment for individual-level socioeconomic condition, despite heterogeneity in study
designs, substitution of local-area measures for neighborhood-level measures, and probable measurement error (Diez-Roux et al., 2003). Although multilevel studies in environmental health science are still relatively rare compared with individual- or ecological-level investigations, the results of these studies nevertheless point to the potential importance of residential context on health.
Multilevel analysis has the capacity to simultaneously assess the effects of individual- and group-level exposures on individual outcomes (Cassel, 1976). Such studies can address the question of whether local-area characteristics have a measurable effect on outcome over and above individual exposures or whether the apparent associations between aggregate measures and outcomes simply reflect the individual-level characteristics of area residents. For example, does the mean income level in some defined community have an effect on the outcome for an individual beyond the effect of the individual’s income, and is the contextual effect independent of a given individual’s income (Von Korff et al., 1992)? If individual and contextual factors both influence outcomes, then models that exclude one or the other set of risk factors are likely to be poorly specified and lead to misinterpretation of the effects of both individual- and contextual-level factors.
At the ecological level, the high correlation among various community characteristics poses problems in estimating the effects of distinct community characteristics. One way to get around this problem is to develop indices of related community-level constructs, but such indices may obscure the roles of their distinct components. For example, this approach could underestimate the association between a chemical exposure of interest and a neurobehavioral outcome, if part of the chemical effect is carried by the association between the community quality index and the neurobehavior. Bellinger (2004) suggests the use of more differentiated measures of complex social constructs to control for only those aspects of community quality that do not reflect exposure opportunities.
Despite progress in this area, problems persist with respect to the conceptualization of and the distinctions between micro- and macrolevel social phenomena. Link and Phelan (1995) have proposed the notion of “fundamental social causes” of disease to explain how resources (such as knowledge, power, money, prestige, and social connections) are linked to disease outcomes through multiple (often shifting) risk-factor mechanisms. The notion is that inequalities in health are a function of persistent social inequalities, regardless of the intervening individual-level exposures, many of which can be shown to vary over time. To date, few studies have managed to successfully differentiate macrolevel from microlevel factors, especially with respect to statistical analysis (Diez-Roux, 1999). So-called mixed models and multilevel approaches are now being used in epidemiological studies, but further refinement is needed. In fact, it seems obvious that the
classification of “levels” into two or even three categories of influence is somewhat crude, because the definition of the higher-level units and the borders between the various levels are frequently unclear.
CONCLUSION
The overall high rate of preterm birth in the United States and the persistent racial-ethnic gap is one of the most significant public health problems today. Despite many years of observational and clinical research, the exposures that place women at risk are not well understood. The substantial intergroup as well as intragroup variabilities in the risk of preterm birth have been shown to be related related to socioeconomic condition, nativity, acculturation, or other maternal characteristics. Although future research should continue to focus on factors that contribute to the high rates of preterm births among African American infants, much can be learned from examinations of racial-ethnic disparities outside the context of the disparities between African American versus white women, as well as disparities within a particular racial or ethnic group. Common measures of socioeconomic status (e.g., income and education) and other potential mediators may not fully capture the magnitude of group differences. For example, the median income of African American families is about 64 percent of the median income of white families, but the median net worth of African American families is only 12 percent of that of white families (Mishel and Bernstein, 2003).
Similarly, a list of stressful life events cannot adequately measure the multiple dimensions of stress, including acute and chronic stressors, stress appraisal, and the environmental (including social and cultural) contexts of stress. For example, racial discrimination disproportionately affects women of color and is associated with preterm birth, yet it often goes unmeasured in studies linking stress to preterm birth. Thus, better measures (both for “exposures,” such as socioeconomic condition and race, and for potential “mediators,” such as stress) are needed in research on these disparities.
The paradox of favorable birth outcomes, despite social disadvantages, among some immigrant groups and the increased rates of preterm birth with increasing length of residence in the United States have been attributed, in part, to the loss of resiliency factors with increasing acculturation. This suggests that research on disparities in the rates of preterm birth needs to pay more attention to protective factors (which include such factors as personal resources, social support, and spirituality).
Current research into the causes of the disparities commonly attempts to isolate the effect of a single risk factor, without accounting for the cooccurrence and potential interactions among multiple protective and risk factors (e.g., age and race or education and race) operating at multiple lev-
els and across the life course to produce disparities in the rates of preterm birth. A more integrative approach to understanding racial-ethnic and socioeconomic disparities in the rates of preterm birth is needed (Lu and Halfon, 2003; Misra et al., 2003). Future research on disparities should aim for longitudinal integration linking a woman’s life history to her vulnerability for preterm delivery, as well as contextual integration linking individual biology and behaviors to the multilevel, multiple determinants of preterm birth.
Although some individual-level risk factors hold modest associations with a risk of preterm birth, individual-level characteristics do not adequately explain the high rate of preterm birth in the United States or the racial-ethnic differences in the rates of preterm birth. The notion that community-level conditions can produce profound effects on disease susceptibility is long-standing (Cassel, 1976). The questions, however, of whether community-level adversity has a deleterious impact on fetal outcomes, independent of individual-level risk factors, and whether the predictive power of these individual-level factors depends on community-level conditions have only recently been subjected to empirical testing. Numerous reports now show, however, that after adjustment for individual-level attributes, neighborhood conditions are in fact independently and significantly associated with a risk of delivering an infant with a low birth weight. Thus, because exposures to adverse neighborhood conditions are much more common for African American women than for their white counterparts, entire groups of women experience distress. There is also a need to examine the relationship between gestational age and adverse neighborhood conditions.
Exploring the social contribution to this important health outcome may contribute to an understanding of the racial-ethnic differential and provide new avenues for remedial strategies to decreasing the rates of preterm birth that move past the narrow biomedical approach. In addition, it is important to give equal consideration to the concept that social conditions are in fact fundamental causes of diseases and syndromes like preterm birth (Link and Phelen, 1995).
Finding 4-2: Independent of the individual-level attributes that are risk factors for preterm birth, adverse neighborhood conditions such as poverty and crime are risk factors for preterm birth. These data suggest that intervention strategies may need to expand from focusing exclusively on the individual to including the contributions of social structural factors to the risk of preterm birth.
























