
4
The HIV/AIDS Epidemic, Kin Relations, Living Arrangements, and the African Elderly in South Africa
M. Giovanna Merli and Alberto Palloni
INTRODUCTION
Although the effects of HIV/AIDS on individuals who contract it have been relatively well known for sometime (Quinn, Mann, Curran, and Piot, 1986), the understanding of the plethora of indirect effects and their pervasiveness in many realms of individual and social life is much less complete. Age selectivity, together with the disease’s relatively long periods of incubation and the associated morbidity and lethality, may affect a number of social relations and social organizations that are either unique or distinctly more powerful than those observed for other diseases in Africa or anywhere else. In particular, the levels and age patterns of the incidence of HIV and future increases in prevalence are likely to have a large impact on kin relations, residential patterns, household organization, and the well-being of family members. Faced with the escalating burden of excess morbidity leading to the disruption of normal activities and functions, families and households are likely to adopt coping strategies to contain the damaging effects of the epidemics. An interesting issue is the magnitude and nature of the costs borne by individuals and families as a consequence of the adoption of these strategies and whether or not they will be put into place without threatening the very fabric of family relations as they are known today.
Ten years ago, Palloni and Lee (1992) reviewed the potential effects of the HIV/AIDS epidemic on mortality levels at various ages that would affect household and family organization. The main idea is that when levels of widowhood and orphanhood rise as much as they could due to the HIV/ AIDS effects on mortality alone (excluding effects on fertility and migration), the material basis of traditional kin relations (kin availability) and of
household organization (residential patterns) will weaken or cease to operate. In their place, one could expect to see the emergence of new forms of social relations. In addition to projecting high levels of widowhood and orphanhood, the authors anticipated the collapse of traditional family organization, kin networks, and the erosion of the foundations of typical household arrangements. They also predicted increasing prevalence of households in which children live with grandparents in the absence of their parents.
In this paper, we update the work of Palloni and Lee and use a modified version of their model to calculate the demographic impact of HIV/AIDS on the elderly. Our evaluation rests on newly available data for South Africa.
The AIDS epidemic is far worse in Southern Africa than it is in Central and Eastern Africa, where it first began. With its 5.3 million cases (Department of Health, 2003), South Africa is the country with the largest number of people infected with HIV. The rapidity with which HIV has spread is exceptional. In less than a decade, adult HIV prevalence from antenatal surveys increased from 1 percent in 1990, to 7.6 percent in 1994, to 27.9 in 2003 (Department of Health, 2003). On the basis of a combination of vital registration data and estimates derived from AIDS modeling, Dorrington, Bourne, Bradshaw, Laubscher, and Timaeus (2001) attributed to AIDS a significant increase in mortality at young and middle adult ages since the late 1980s, estimating that 40 percent of the deaths of adults ages 15-49 in 2000 were from AIDS. A more recent study estimates the increases in mortality related to HIV between 1996 and 2000-2001 at 7 per 1,000 among children, 2.7 per 1,000 among women ages 30-34, and 2.6 per 1,000 among men ages 35-39 (Groenewald, Nannan, Bourne, Laubscher, and Bradshaw, 2005). This age-specific increase is consistent with an AIDS-related acceleration of mortality in the latter part of the 1990s, estimated from demographic surveillance system data in KwaZulu-Natal (Hosegood, Vanneste, and Timaeus, 2004). Without treatment to prevent the progression from HIV to AIDS, Dorrington et al. (2001) estimate that the cumulative number of AIDS deaths is expected to reach between 5 and 7 million by 2010.
Furthermore, in South Africa, as in much of the rest of Africa, the African elderly have been until very recently primarily supported by intra- and intergenerational familial networks. In particular, coresidence with an adult child is a common form of living arrangement and a form of exchange (Møller and Devey, 1995). Thus what we observe among the African population of South Africa may be replicated in other countries with similar patterns of intergenerational relations.1
Strategies adopted by households and families to cope with the depletion of human and material resources induced by HIV/AIDS may range from changes in household structure, to reorganization of the division of labor in the domestic domain, to shifts in norms regarding female, child, and elderly labor force participation, and depletion of assets and cash reserves. The particular menu of strategies chosen will depend on the social group, and some, though not all, of the changes in household structure introduced by HIV/AIDS will be reflected in observable shifts in the living arrangements of the elderly. Increases in AIDS morbidity and mortality will reduce the availability of members of the young adult generation. Adult children will be sick or disabled for long periods of time and later die. They may lose the capacity to earn the income that would have been otherwise transferred to their aging parents. They may also require additional resources for their own support and medical care. Thus the elderly suffer a double burden with likely implications for their own health status and wellbeing: they become caregivers of the younger generations, first of their adult children and then of the AIDS orphans, and they may find themselves without the income transfers from the middle generations, so that net resource flows may be from rather than to aging parents.
Moreover, the physical and psychological well-being of older persons will be affected not only by the death of adult children and foregone transfers of income, goods, and services, but also by the need to raise additional cash by diluting assets or deploying more hours of work to satisfy the increased burden entailed by the protracted nature of the illness. With its implied long-lasting health impairments on adult individuals, the disease jeopardizes households’ ability to generate resources for the care of their most vulnerable members, namely, children and the elderly, and thus aggravates the social and psychic costs of the illness (Ainsworth and Dayton, 2001).
This damaging consequence of the disease will start long before the time of death of those already infected. This phenomenon is what was referred to early on as the “bottom of the iceberg” (Palloni and Lee, 1992:82). The effects of deterioration of the health status of adults on the well-being of children and the elderly is in all likelihood much larger than those implied by the direct effect via excess mortality.
Our central objective in this paper is rather modest, since we only estimate the effects of HIV/AIDS on residential patterns of the South African elderly and evaluate observable changes in their living arrangements over a decade. We eschew assessment of other effects of the epidemic on the elderly but argue that these may be reflected, at least in part, in changes in residential arrangements. We use information from three data sources collected before and after the onset of the HIV/AIDS epidemic in South Africa: the 1991 census of the Republic of South Africa, the 10 percent sample of
South Africa’s first postapartheid census conducted in 1996, and the 10 percent sample of the 2001 census.
We proceed in two steps. First, we evaluate macromodels of the epidemic through backward and forward projections of HIV incidence and related mortality. The models are based on a backward projection of a current population of elderly people who are then projected forward, subjecting their children to an estimated HIV/AIDS regime. These models yield estimates of the expected availability of adult children for the elderly, lower bounds for the prevalence of sickness among the children born to elderly people, and 10- to 15-year projections of changes in the availability of adult children and the prevalence of sickness. Second, we use the macromodel to contrast some of the epidemic’s expected outcomes derived from the model with observed changes in living arrangements of the elderly over time and across provinces. These contrasts depend on descriptions of observable patterns. We focus on the impact of AIDS mortality as well as the burden of illness associated with the presence of sick adult children. A significant difficulty made evident by these comparisons is that of identifying the direction and magnitude of changes in the living arrangements of the elderly that can be unequivocally associated with the impact of HIV/AIDS.
PREVIOUS RESEARCH ON THE IMPACT OF EPIDEMICS ON FAMILIES AND HOUSEHOLDS
Demographically speaking, the HIV/AIDS epidemic is not far removed from the large shocks suffered by preindustrial populations. In fact, all evidence available to us seems to point to a catastrophe of much larger proportions. Although the parallel suggests that we could learn from the past by examining studies of the population impact of epidemics, famines, and wars, this literature is in general devoid of systematic analysis of the complex effects on family and household organization. Attempts to assess the relation between past crisis mortality and the day-to-day operation of households, families, and social relations are scarce. The effects most successfully examined are those directly related to global excess mortality, deficits in fertility, and increased regional displacement of individuals.2
Only rarely have extant studies of past population crises attempted to identify mechanisms translating raised levels of individual mortality or morbidity into shifts of the size distribution of households and the likelihood of fusion, fission, or outright disappearance of family units. An important exception is Livi-Bacci’s (1978) assessment of the demographic effects of epi-
demics suffered by preindustrial populations on the distribution of families by size.3 We attempt to follow this lead to understand the effects of HIV/ AIDS on the living arrangements of the African elderly in South Africa, but we adopt completely different assumptions to reflect the operation of a unique epidemic, with a distinct age pattern of incidence, a protracted period of incubation and infectiousness, and singular lethality.
With the exception of a few studies on the direct economic costs for individuals and households (Ainsworth and Over, 1999), most research on the effects of the African epidemic focus on particular members of families, such as mothers or children, and on the impact of adult male deaths that raise widowhood and orphanhood. Studies of the impact of HIV/AIDS on widowhood have focused on traditional behaviors, such as the role of widow inheritance, where a widow is inherited by one of her husband’s brothers or other male relatives, in exposing women to HIV infection, and the changes in such traditional arrangements due to the epidemics in Uganda (Mukiza-Gapere and Ntozi, 1995). Ntozi, Ahimbisibwe, Ayiga, Odwee, and Okurut (1999a) found that the stigmatization of AIDS widows upon the loss of their spouse in Uganda influenced their movements. Less healthy widows were more likely to leave their late husbands’ homes and seek care in their natal villages, while healthier AIDS widows were more likely to remarry or form new sexual partnerships.
A review of a series of case studies on the impact of HIV/AIDS on orphanhood by Zaba and Gregson (1998) reveals that in areas with high HIV/AIDS prevalence, the prevalence of paternal orphanhood was higher than that of maternal orphanhood. It was attributed to polygynous unions whereby, at the father’s death, all children born to his widows become orphans. In Tanzania, Urassa and colleagues (1997) found that 8 percent of children under age 15 and 9 percent of children under age 18 had lost one or both parents. In the region of Manicaland in Zimbabwe, the rapid increase in the number of parental deaths posed demands that exceed the capacity of relatives to fulfill their traditional role of caring for orphans and triggered the emergence of child-headed households (Foster, Makufa, Drew, and Kralovec, 1997). In the Kagera region of Tanzania, excess adult deaths not only implied higher levels of orphanhood but severely affected the nutritional status of orphaned children (Ainsworth and Semali, 1998).
Community studies provide evidence for the effects of the epidemic on household organization (Barnett and Blaikie, 1992; Boerma, Urassa,
Senkoro, Klokke, and Ng’weshemi, 1999; Ntozi and Zirimenya, 1999; Urassa et al., 1997). In Uganda’s Rakai district, two or three generations with at least one orphan and individuals living alone were more common in AIDS-affected households than unaffected ones, and in a significant fraction of households containing AIDS victims, grandparents cared for orphans (Barnett and Blaikie, 1992). The burden of AIDS mortality and morbidity for households is shared by their members in a strict hierarchy. In Uganda, care of AIDS orphans was left to the surviving parent, then to grandparents, followed by older orphans, stepparents, and members of the extended family, such as uncles. Paternal orphans were more likely to be fostered by uncles than cared for by their mothers, because children belong to their father’s lineage (Ntozi, Ahimbisibwe, Odwee, Ayiga, and Okurut, 1999b). In a study in Zimbabwe, grandparents were the main care providers to AIDS orphans (Foster et al., 1995). Data from the Kisesa community study show that terminally ill people travel back to rural homes in search of care by the extended family (Urassa et al., 2001). Elderly parents are the most likely caregivers of their infected children, because parents are the most sympathetic and are likely to be informed of their children’s AIDS diagnosis first (Ntozi, 1997). Strikingly, similar patterns of caregiving were found in Thailand (Knodel, VanLandingham, Saengtienchai, and Im-em, 2001), where 27 percent of adults with “symptomatic” AIDS were cared for by a parent. Two-thirds of the adults who died of an AIDS-related disease had lived with or next to a parent by the terminal stage of illness, and a parent, usually the mother, had acted as a main caregiver for about half. For 70 percent, either a parent or other older-generation relative had provided at least some care. The vast majority of parents were age 50 or more and many were 60 or older.
The foregoing summary identifies two important albeit weak regularities. First, most studies underscore transformations of living arrangements to accommodate AIDS orphans and widows, with an increased prevalence of households composed of the elderly with their widowed children and grandchildren, as well as households with grandparents and grandchildren but no member of the intermediate generation. Second, there is a rearrangement of the household to adjust to the needs of caring for sick adult children. These changes may lead to increases in headship among the elderly and to a more influential presence of households composed of elderly parents, their adult children, and grandchildren.
Besides the somewhat elusive evidence connecting HIV/AIDS and concomitant changes in families and households, demographic models that attempt to identify the population-level effects of HIV/AIDS have not succeeded in providing a benchmark against which to evaluate empirical evidence (Zaba and Gregson, 1998). For example, although orphanhood is the most amenable outcome to modeling because it requires assumptions
only about mortality and fertility, modeling the impact of HIV/AIDS on orphanhood is complicated by time lags between the onset of HIV and orphanhood and the difficulties of quantifying pre-HIV/AIDS levels and patterns of orphanhood. Models predicting the impact of HIV on widowhood require additional conjectures about nuptiality and are more complicated to implement, especially in sub-Saharan Africa, where polygyny and remarriage are frequent.4
Changes in household organization in general and in the living arrangements of the elderly in particular have proven to be even less amenable to modeling than orphanhood or widowhood. This is because, in addition to information on demographic determinants, one needs to assess the influence of propensities to coreside and of internal migration flows, both of which may mimic the effects of HIV/AIDS on the availability of kin and confound the epidemic’s independent effect. Efforts to isolate the contribution of each of these factors are rare, as they generally require the combined use of simulation and empirical observations. One study uses microsimulation, in combination with aggregate demographic analysis, to estimate how patterns of coresidence of elderly parents in Thailand would adjust in response to the HIV/AIDS epidemic (Wachter, Knodel, and VanLandingham, 2002). The authors project that 11.9 percent of the present generation of Thai elderly (age 50 and over) will lose one or more children to AIDS, and 13 percent of those who lose at least one child will lose two or more before death. They also estimate that, of the cohort of Thai men and women age 55 in 1995, 1 in 9 could expect to experience the loss of at least one child to AIDS, while 1 in 14 could expect to have lived with a child during illness and have provided care.
The most important lesson emerging from this brief review of previous studies is that even the most direct effects—those working through augmented levels of orphanhood and widowhood—present themselves in a veiled form or not at all in aggregate data. Problems with identification of the proper time lags, imperfect knowledge of relations prevailing in the period preceding the epidemic, and the widespread use of norms typical of most African societies, such as those regulating fosterage and remarriage, tend to mask or dampen the observed effects of the epidemic.
THE IDENTIFICATION PROBLEM
Minimum Identification Conditions
Efforts to estimate empirically the impact of HIV/AIDS on the residential arrangements of the elderly can be successful only if a set of minimum identification conditions are satisfied at the outset. These conditions are associated with processes that either uniquely determine or loosely bound the observable patterns of the elderly’s living arrangements.
Living arrangements of the elderly are determined by two factors. The first is a function of purely demographic forces and influences the availability of kin. Preexisting levels and patterns of mortality, fertility, and migration limit the supply of kin that could reside with older people and therefore affect the ability to observe certain types of living arrangements. The second factor is the set of individual propensities to live with blood kin and other relatives. Residential propensities are a function of culturally bounded patterns of preferences and are likely to vary greatly across social classes and ethnic groups in the same society.
Thus the prevalence of living alone or with a spouse but no children among the elderly age x at time t, P(x,t), is simply the product of D(x,t), a measure of the supply of children available to the elderly age x—the proportion of elderly who have surviving children to live with—and p(x,t), a measure of the conditional probability of residing with one of the surviving children.5 Since excess mortality associated with HIV/AIDS affects D(x,t), one could argue that the difference between estimates of demographic availability in contexts with and without HIV/AIDS is sufficient to identify the effects of HIV/AIDS on living arrangements of the elderly. But this line of thought ignores a number of difficulties.
First, when examining changes in the living arrangements of the elderly, both D(x,t) and p(x,t) need to be identified simultaneously. While changes in D(x,t) can be assessed through a variety of procedures, including micro- and macrosimulations, estimation of p(x,t) is almost always problematic. This difficulty has already confronted scholars who have worked on microsimulation of households and families (Ruggles, 1987; Wachter, Hammel, and Laslett, 1978), but it has been met with no straightforward solution. Furthermore, the relationship among the observed distribution of living arrangements of the elderly, the demographic availability of kin, and individual propensities involves sources of misidentification that, if not properly neutralized, will bias inferences regarding the effects
of HIV/AIDS on the living arrangements of the elderly. While some of these sources of misidentification are unique to South Africa, others apply to broader contexts.
In the foregoing formulation, we assumed that the estimation of past levels and patterns of vital events (including nuptiality and migration) is unproblematic. Although this may be so for fertility, mortality, and nuptiality, it is not so for migration. Migration exerts a severe drag on the supply of adult children. In the absence of proper controls for out-migration flows, one can mistake a decline in P(x,t) for changes in other demographic determinants, particularly mortality. In the absence of direct estimates of the tug of migration, a minimum first condition for the identification of the effects of HIV/AIDS is a comparison of measured effects across areas exposed to similar incidence of HIV/AIDS but experiencing different levels of migration.
The second source of misidentification is peculiar to the nature of HIV/ AIDS. Because the median duration from infection to full-blown AIDS and mortality in sub-Saharan Africa is about 7.5 years (Boerma, Nunn, and Whitworth, 1998), one cannot expect to see large changes in patterns of living arrangements until some time after the onset of the epidemic. In South Africa, the first AIDS cases were reported in 1984-1985 (Sher, 1986), but the full force of the epidemics could not have been felt before 1995. Using a data source for a year before 1995 is tantamount to choosing a baseline against which changes induced by the epidemic can be measured. The selection of a target date is also problematic, for it should be sufficiently distanced from the benchmark to allow time for the effects to accumulate. Thus, a second minimum identifying condition is to examine information on residential arrangements after 1995 relative to those prevailing some time before this benchmark date.
Third, the above formulation rests on a “whopper” assumption—to paraphrase Ruggles’s terminology (Ruggles, 1987)—namely, that changes in demographic forces do not significantly alter individual residential preferences. However, sudden changes in mortality levels could simultaneously shift preferences among kin by decreasing the propensity of the elderly to live with a surviving adult child. If one is unaware of this, one will attribute a larger fraction of changes in P(x,t) to observed changes in mortality levels than one ought to, with an ensuing exaggeration of the effects of exogenous changes in mortality due to HIV/AIDS. Conversely, a sudden rise in adult morbidity may increase the propensity to live with a surviving (and possibly ill) adult child. The resulting increase in p(x,t) will offset the mortality-induced decrease in D(x,t) and yield an error in the opposite direction, namely, an underestimation of the demographic effects of excess mortality. These examples ignore time lags and the precise mechanisms through which demographic availability influences residential preferences, but the main
idea should be transparent: if our mission is to assess the impact of an external event on P(x,t) and to determine how much of this change occurs via changes in D(x,t) alone, identification will be problematic insofar as we do not account for the impact of changes in D(x,t) on p(x,t). It follows that a third minimum condition for the identification of HIV/AIDS effects is the assessment of changes during a period of time short enough to support the assumption that endogenous effects have not significantly altered residential preferences prevailing prior to the onset of HIV/AIDS.
It should be noted, however, that if one is interested in the total effect of HIV/AIDS, the third identification condition is superfluous. Indeed, in this case all we need is a rough measure of change in P(x,t)—whether reflecting changes in D(x,t) or in p(x,t) induced by the epidemic itself. The only caveat is that inconsistent estimates of the effects of the epidemic will obtain if any of the changes in p(x,t) are exogenous to the event of interest. Furthermore, if changes in D(x,t) and p(x,t) offset each other perfectly, no changes in P(x,t) will be observed, leading one to conclude that the HIV/ AIDS epidemic is inconsequential for living arrangements.
Identification Conditions in South Africa
In South Africa, identification problems are exacerbated by the fact that the period of fastest growth of the incidence rates in HIV/AIDS coincided with a period of tumultuous social and demographic transformations that occurred just before and after the collapse of apartheid.
Apartheid and its associated system of separate development imposed restrictions on spatial mobility, education, and employment of black South Africans, by forcibly resettling them to the homelands, four of which were made “independent states” in the 1960s and 1970s (Transkei, Bophuthatswana, Venda, and Ciskei, or the TBVC states). This regime supported a migrant labor system, of circular character, which affected almost every African household. Through the enforcement of influx control laws, African men working in the mining industries, on white farms, and in towns and cities were systematically denied the right to settle there with their families. Single sex hostels were built in all major cities to host rural African laborers. This system encouraged male out-migration but kept families divided by forcing heavy restrictions on residential changes by migrants’ wives, children, and elderly relatives (Murray, 1980, 1987; Russell, 1998). What were once undivided rural households became “stretched households,” that is, spatially divided units connected by kinship and remittances (Spiegel, Watson, and Wilkinson, 1996). After the collapse of apartheid, migration involved broader age groups as well as women (Collinson, Tollman, Kahn, and Clark, 2003; Posel and Casale, 2002). The intensi-
fication of migration resulted in the rapid periurbanization of formerly rural areas bordering large metropolitan areas and the swelling of the population of black townships living in backyard shacks (Kinsella and Ferreira, 1997; Percival and Homer-Dixon, 1995; Spiegel et al., 1996).
If death were the only reason for children to be cared for by grandparents, we would expect a higher proportion of the elderly living in skipped-generation households—which are households composed by grandparents and grandchildren without members of the middle generation, in areas where the prevalence of HIV/AIDS is high. But in South Africa, children may lose a parent to migration as well as death (Bray, 2003), and migration provides a condition for grandparents to take in and support their grandchildren (Smit, 2001). Thus, an increase in the prevalence of grandparents living with their grandchildren without the presence of an adult child may not be due to HIV/AIDS but to high rates of population mobility.
Apartheid and its forced labor migration system also changed the economic function of black South African households, from agricultural production to labor in South Africa’s gold mines and industrial development (Martin and Beitel, 1987; Marwick, 1978). Theories of modernization hold that economic transformations, brought about by industrialization and the establishment of wage labor, have decoupled production from the family division of labor characteristic of traditional agricultural societies. In line with these theories, the changes brought about by apartheid might have led to an erosion of social control over family members and a weakening of emotional ties that sustain traditional adherence to the family and its patriarch. Disintegration of the traditional intergenerational relationships has implications for the living arrangements of the elderly, for whom modernization assumes a shift from a preference for coresidence with adult children and grandchildren to a preference for solitary living. Thus, an observed increase in the prevalence of solitary living among the elderly may be due to forces of modernization rather than the outcome of demographic constraints imposed by HIV/AIDS.
Moreover, in South Africa, there is a distinctive reason for alterations in the living arrangements of the elderly: a pension system that was extended to all South African elderly in 1993, mostly by increasing the benefits received by Africans. With rising rates of unemployment, pension sharing with an elderly relative has become a reason for adult children to join their elderly parents’ households (Burman, 1996; Møller and Sotshongaye, 1996). Nearly 80 percent of age-qualified Africans reported receiving a social pension in 1996 (Case and Deaton, 1998). Similar to the effects of HIV/AIDS, which may draw adult children back to their elderly parents’ homes, the elderly pension system may affect the propensities of adult children to coreside with the elderly, thus introducing another source of misidentification.
Operationalization of Minimum Conditions
In order to partially satisfy the identification conditions, we utilize three different strategies. The first strategy is model-based and consists of estimating expected demographic impacts, that is, changes in D(x,t) associated with mortality increases due to HIV/AIDS. These estimates are obtained through the application of simple multistate models relying on estimated patterns of age-specific HIV incidence, incubation periods, and HIV/AIDS-related mortality. They provide us with a benchmark for the magnitude and direction of expected changes in living arrangements of the elderly (P(x,t)) due to changes in the availability of adult children (D(x,t)) in the absence of changes in p(x,t). They also provide a baseline to evaluate the burden of disease borne by their adult children. Observed data derived from data sources for the period 1991-2001 are then compared with expected (model-based) values. This first strategy contributes to the first and second identification conditions, since it provides us with a sense of the magnitude of the expected changes in availability due to changes in demographic forces in the absence of endogenous or exogenous changes in residential propensities.
Second, for the comparison of model outcomes with empirical data, we choose the period 1991-2001, which brackets the sharp increase in the incidence of HIV/AIDS. Differences in the patterns of living arrangements during this period will give us leverage to detect changes in living arrangements due to changes in D(x,t). Although the interval between 1991 and 2001 is wide enough to capture time lags inherent in the progression of the epidemic and address the second identification condition, it may not be short enough to contribute to the third identification condition. In fact, we may not be able to fend off the threats to identifiability originating in the reciprocal relations between demographic availability and propensities. However, our inability to distinguish changes in living arrangements due to changing propensities from changes due to demographic availability will be a less serious issue if we are interested in assessing the overall effect of HIV/ AIDS. It will be a problem only if the propensities are changing due to exogenous factors (e.g., modernization).
Third, to address the first identification condition and distinguish the effects of HIV/AIDS on the living arrangements of the elderly from those of migration, our analyses will compare conditions across South African provinces, which differ in levels of HIV/AIDS prevalence and magnitude and direction of migration flows. By contrast, there is no similar strategy to reduce the confounding effects of the pension system on patterns of elderly coresidence. Fortunately, changes in pension laws are more likely to affect certain types of coresidential arrangements than others. While coresidence with adult children could be easily related to the issuance of pension receipts, changes in the coresidence of the elderly with grandchildren (but not
their parents) are less likely to be related to availability of pension payments to the elderly.
DATA ON LIVING ARRANGEMENTS
Data Sources
Our observation of changes in P(x) relies primarily on the analysis of the last apartheid census taken in 1991, the 10-percent public sample of the first postapartheid census taken in 1996, and the 10-percent public sample of the 2001 census.
The 1991 census is well known for its apartheid-induced distortions in coverage, which produced significant underenumeration, especially in the self-governing territories, that is, the six homelands that remained part of South Africa after “independence” was granted to the four TBVCs (Orkin, 2000).6 Even after various adjustments, the underenumeration of the African population was estimated at 17 percent (Zuberi and Khalfani, 1999). The granting of “independence” to the TBVCs further complicates the comparability of data sources in the 1990s, because in 1991 the TBVCs conducted their own censuses.
As the first and second postapartheid censuses, the censuses of 1996 and 2001 were conducted after reintegration of the TBVCs into South Africa. These censuses standardized methodologies of data collection for all areas (Cronje and Budlender, 2004). We use the 10-percent public samples of both censuses, based on a systematic sample of households stratified by district and province.
Statistics South Africa offers users of 2001 census data a combination of two kinds of imputations for the 2001 data: “logical” imputations, in which “a consistent value is calculated or deduced from other information relating to the individual or household” and “hotdeck” imputations (Statis-
tics South Africa, 2001). No imputation of missing data was undertaken to correct the 1996 census data (Kevin Parry, Statistics South Africa, personal communication, April 21, 2005). For the present analysis, we accept the logical imputations but code as missing the observations with values imputed by hotdeck procedure. This approach resulted in comparable fractions of missing values in the 1996 and 2001 censuses on the variables of interest to this analysis.
Issues of Census Comparability
Important issues affect the ability to compare censuses over time. First, the empirical geographic basis of the 1991 census is different from those of the 1996 and 2001 censuses. Whereas the 1996 and 2001 censuses covered the entire country, the 1991 census excluded the former TBVCs. Where needed, we were able to use a version of the 1996 census subsetted to the same geographic areas as the 1991 census, which excludes the population residing in the former TBVC states, to compare the 1991 census population with the 1996 population purged of the fraction of the population enumerated in the former TBVCs. Moreover, because the different sizes of the territory covered and different provincial boundaries complicate the comparison of the population enumerated in the 1991 and 1996 censuses, we use a version of the 1991 census, which allots the population to the same geographic areas of the nine South African provinces in the 1996 census.
Second, all three data sets contain information on the relationship of each household member to the household head. This information is necessary to calculate the distribution of living arrangements of the elderly, widowhood and orphanhood rates, and other indicators pertaining to the residential arrangements of the elderly. But the number of relationships to household head provided in each census varies. The 1991 census has the smallest number (spouse, child, other family, unrelated), with the most notable absence being the category of grandchild. The 1996 and 2001 censuses are richer in details.7
To increase our ability to capture key living arrangements of the elderly by successfully identifying grandchildren in the 1991 census, we imputed the relationship of grandchildren of head in the 1991 census by estimating the proportion of “other family” who are grandchildren of head in a nationally representative survey conducted on a date close to 1991 and apply-
ing this proportion to 1991 data to obtain grandchild status.8 We then degraded the 1996 and 2001 data by ignoring information unavailable in the 1991 census, so that, beside household head, the only relations to head used to construct household types were spouse, child, grandchild, other family, and unrelated.
Third, the definition of what constitutes a household changed over time. A household in the 1991 census was defined as “a person or a group of persons (whether related or not) who usually occupy a dwelling or part thereof and who provide themselves with food and other essentials for living or have made arrangements for such provision” (Republic of South Africa Central Statistical Service, 1991). Live-in domestic workers were classified alongside their employers’ households as unrelated members. In the 1996 and 2001 censuses, a household was “a person or a group of persons who occupy a common dwelling and who provide themselves jointly with food and other essentials for living.” Domestic workers were classified as separate households (Statistics South Africa, 1998a, 2004).
Fourth, each census adopted different procedures to enumerate individuals living in hostels and the institutionalized elderly. In the 2001 census, every individual (or household) living in a workers’ hostel, student residence, residential hotel, or home for the independent elderly was enumerated on a household questionnaire. The 1991 census classified individuals living in hostels and the institutionalized elderly as “unrelated household members,” regardless of whether they were enumerated at these locations along with one or more family member. In the 1996 census, only individuals living in hostels with their families were administered a household questionnaire. Individuals living in hostels as a single family unit were administered a personal questionnaire. Institutionalized elderly were individually enumerated with a special institution questionnaire, which prevents the tracing of household relations between spouses who are enumerated in the same institution.
A PROFILE OF SOUTH AFRICA’S PROVINCES
In order to identify the effects of HIV/AIDS on the living arrangements of the elderly and separate them from those of migration, Table 4-1 displays a profile of South African provinces in the three census years. Most notably this table reports provincial levels of HIV prevalence and of migration. This information permits the assignment of provinces to two distinct regimes of HIV prevalence and migration, the former defined by the severity of HIV infection estimated from antenatal surveillance data, the latter defined by the proportion of households with an absent migrant member,9 the level of urbanization, the sex ratio of the population, and the average per capita income. The most rapid increase in HIV prevalence over the 1990s has been experienced by KwaZulu-Natal, followed by Mpumalanga, Free State, Gauteng, and Northwest Province, while most of the increase of HIV prevalence in Eastern Cape occurred in the latter half of the 1990s. By 2001, six provinces displayed adult HIV prevalence rates higher than 20 percent. The remaining ones, Western Cape, Limpopo, and Northern Cape, displayed low to moderate levels of HIV.
As for migration, Gauteng and Western Cape, with the highest average incomes and levels of urbanization, are major destinations of rural migrants. These two provinces display the smallest fractions of African households with at least one absent migrant worker. In contrast, Limpopo, Eastern Cape, KwaZulu-Natal, Mpumalanga, and Northwest all display very large fractions of households with a migrant worker. Limpopo and Eastern Cape, which contain two of the former four TBVCs, are predominantly rural provinces and among the poorest. They are historically two major sending regions of labor migration. KwaZulu-Natal’s major urban centers also receive migrants from Eastern Cape, especially from the former Transkei region (Percival and Homer-Dixon, 1995). But because of this province’s good road and transportation system, KwaZulu-Natal also experiences significant internal migration flows. Mpumalanga and Northwest Province are predominantly rural but have large periurban settlements near the border, and Gauteng attracts large concentrations of rural migrants from the provinces’ more remote corners (Kok, O’Donovan, Bouare, and van Zyl, 2003).
Despite the value of this provincial categorization for our ability to identify the effects of HIV/AIDS on the living arrangements of the elderly and separate them from those of migration, the association between province and coresidential outcomes is fragile for at least one important reason. This is because we assign the consequences of HIV/AIDS mortality for the living arrangements of the elderly to provinces with high HIV prevalence and neglect to consider the indirect effects on provinces with low to moderate prevalence. Yet some of the consequences of HIV/AIDS are likely to be experienced by the elderly in low-prevalence regions as well as by those living in high-prevalence regions. Consider, for example, the hypothesized increased proportion of the elderly living with grandchildren but no adult children in areas with high HIV prevalence. Because of the well-established relation between mobility and the spread of high-risk sexual behavior leading to HIV infection (Hunt, 1989; Lurie, Harrison, Wilkinson, and Karim, 1997; Nunn, Wagner, Kamali, Kengeya-Kayondo, and Mulder, 1995; Pison, Le Guenno, Lagarde, Enel, and Seck, 1993; Quinn, 1994), migrant husbands may pass on the infection acquired in urban and periurban areas or in mining towns to their wives in rural areas. The death of both parents will entrust children to the care of grandparents in migration sending areas. Under this scenario, HIV mortality would be as likely to increase the proportion of skipped-generation households in low-prevalence areas, which are also sending areas of migration, thus complicating our ability to obtain the first identification condition.
THE DEMOGRAPHIC IMPACT OF HIV/AIDS: A SIMPLE MACROMODEL BASED ON BACKWARD AND FORWARD PROJECTIONS
Model
We focus on an elderly woman age x (x ≥ 60) who is alive in a target year, say 1995.10 Hereinafter we refer to this woman as the target or target person, and to the year 1995 as the target year. Our approach consists of back-projecting target women alive in the target year to the time when they
TABLE 4-1 Percentage Distribution of Population by Province and Selected Characteristics, South Africa 1991, 1996, and 2001
|
Census Year |
Western Cape (WC) |
Eastern Cape (EC) |
Northern Cape (NC) |
Free State (FS) |
|
|
Census 1991 |
|||||
|
|
African |
16.6 |
57.3 |
29.8 |
83.3 |
|
|
Urban |
54.3 |
53.5 |
52.2 |
51.4 |
|
|
Nonurban |
45.7 |
46.5 |
47.8 |
48.6 |
|
|
Sex ratio |
1.01 |
0.97 |
1.02 |
1.12 |
|
|
% age 60+ |
7.9 |
8.1 |
7.4 |
5.8 |
|
|
N |
271,654 |
113,463 |
57,214 |
142,398 |
|
|
HIV %a |
0.1 |
0.6 |
0.1 |
1.5 |
|
Census 1996 |
|||||
|
|
African |
21.1 |
86.4 |
33.1 |
84.5 |
|
|
Urban |
88.9 |
36.6 |
70.1 |
68.6 |
|
|
Nonurban |
11.1 |
63.4 |
29.9 |
31.4 |
|
|
Sex ratio |
0.96 |
0.86 |
0.96 |
0.97 |
|
|
% age 60+ |
8.7 |
9.2 |
8.6 |
7.9 |
|
|
N |
361,735 |
563,816 |
70,974 |
240,179 |
|
|
P.c. income 1996b in Rands |
17,880 |
5,479 |
13,398 |
10,628 |
|
|
1996 % Afr hh w/ migr. worker |
1.2 |
28.5 |
6.9 |
12.3 |
|
|
HIV %a |
3.1 |
8.1 |
6.5 |
17.5 |
|
Census 2001 |
|||||
|
|
African |
26.7 |
87.6 |
36.2 |
87.8 |
|
|
Urban |
89.7 |
38.1 |
80.2 |
74.8 |
|
|
Nonurban |
10.3 |
61.9 |
19.8 |
25.2 |
|
|
Sex ratio |
0.93 |
0.86 |
0.95 |
0.92 |
|
|
% age 60+ |
7.9 |
9.1 |
8.0 |
7.3 |
|
|
N |
382,963 |
551,926 |
71,530 |
226,338 |
|
|
P. c. income 2000c in Rands |
20,777 |
7,792 |
12,481 |
12,334 |
|
|
1998 % Afr hh with migr. workerd |
1.0 |
35.3 |
10.5 |
14.9 |
|
|
2001 HIV %e |
8.6 |
21.7 |
15.9 |
30.1 |
|
NOTE: All percentages from the 1991, 1996, and 1998 censuses reflect sampling weights, but the N rows report the unweighted denominators. aSouth Africa Department of Health, cited in Ubomba-Jaswa (2000). bStatistics South Africa (1998b). cBureau of Market Research (2000). |
|||||
started reproduction and then projecting them forward to reproduce their childbearing experience. The forward projection exposes the target’s children to the risk of HIV infection and death due to AIDS. This is done by applying rates of HIV incidence (transition from the healthy state to HIV+), rates of incubation (transition from HIV+ to AIDS), and mortality rates (transitions from any of healthy, HIV+, and AIDS to the absorbing state of
death). Backward projection is carried out using estimates of AIDS-free mortality schedules and childbearing schedules for the period 1900 onward. Throughout we assume that childbearing and mortality are independent events for the subpopulation of target women.
Our goal is to calculate the following quantities: (a) the probability that a target’s female children born alive when the target was age x − y at time
t − y have survived healthy to time t, or have not experienced HIV by time t, SI(y,t); (b) the probability that they have survived to t but contracted HIV along the way and are alive but ill at time t, QI(y,t); and, finally, (c) the probabilities that they have died due to HIV, QID(y,t), or due to other causes, Q(y,t). The time variable y varies from a minimum equal to x − 50 to a maximum equal to x − 15, thus constraining the childbearing period of the target to be within ages 15 and 50.11 The expressions for each of these functions are defined in the appendix to this chapter. With knowledge of the time distribution of children ever born (or the age pattern of fertility to which women age x at time t were exposed during childbearing), ![]() , we can calculate the weighted probabilities of having a child in any of the four statuses defined above. This is achieved multiplying
, we can calculate the weighted probabilities of having a child in any of the four statuses defined above. This is achieved multiplying ![]() , for every permissible value of y, by each of the quantities defined above. These weighted values represent the average probabilities for an elderly woman age x at time t. In particular,
, for every permissible value of y, by each of the quantities defined above. These weighted values represent the average probabilities for an elderly woman age x at time t. In particular, ![]() is the average fraction of all children born to the target person who are infected with HIV at age y at time t;
is the average fraction of all children born to the target person who are infected with HIV at age y at time t; ![]() is the average probability of having a child age y at time t who is healthy; and, finally,
is the average probability of having a child age y at time t who is healthy; and, finally, ![]() is the average probability of having lost a child to either HIV/ AIDS or to mortality due to other causes.
is the average probability of having lost a child to either HIV/ AIDS or to mortality due to other causes.
Outcomes from the Model
The main outcomes from the model track the history of illness and mortality experienced by the target person’s children. Calculations can be fine-tuned to project forward or to assess the target person’s status some years ahead of the initial date of calculation.12 In particular, we estimate the aforementioned quantities for the cohort of the elderly ages 60, 65, and 70 in 1995 and then project these forward 10 years to 2005, thus assessing the experience of these cohorts when they are ages 70, 75, and 80 in 2005. We also estimate the quantities for those ages 60, 65, and 70 in the year
2000, and similarly project these forward to the year 2010. Thus, we are able to trace the experience of those ages 60, 65, and 70 in 1995, through the years 2000, when they are ages 65, 70, and 75, respectively, 2005, when they are ages 70, 75, and 80, respectively, and, 2010, when they attain ages 75, 80, and 85.
Armed with knowledge of the distribution of mothers by survival status of children ever born for a period, we can estimate the probabilities of having a given number of children alive and healthy or a given number of children alive with HIV or dead due to HIV or other causes. This extension is straightforward and relies on the quantities defined before and on the estimated distribution of mothers by number of children ever born. If, for example, we are interested in estimating the probability of r children alive and not affected by HIV for a target age x at time t, we use the following expression:
where C(r,j) is the quantity j!/(r!*(j − r)!), ![]() is the standardized fertility rate (adding up to unity) at age x − y, w(j) is the probability of having exactly j children ever born, and SI(x,t) is as defined before. Simple modifications of this expression lead to the probability of exactly r children alive and infected, and r children dead due to non-HIV/AIDS-related causes or due to HIV/AIDS. Perhaps the most important quantity is the probability of having 0 children alive or 0 children alive and with no HIV. These are direct measures of demographic availability and the potential burden of illness, respectively.
is the standardized fertility rate (adding up to unity) at age x − y, w(j) is the probability of having exactly j children ever born, and SI(x,t) is as defined before. Simple modifications of this expression lead to the probability of exactly r children alive and infected, and r children dead due to non-HIV/AIDS-related causes or due to HIV/AIDS. Perhaps the most important quantity is the probability of having 0 children alive or 0 children alive and with no HIV. These are direct measures of demographic availability and the potential burden of illness, respectively.
Required Inputs
Estimation of model outcomes depends on six pieces of information. The first and most important are the yearly HIV incidence rates from the onset of the epidemic until time t. The second is the incubation function that determines the waiting time in the infected state. The third is mortality of healthy individuals, of individuals infected with HIV, and of those with full-blown AIDS. The fourth is the time distribution of children ever born or, equivalently, the fertility function approximating the childbearing experience of the target population. The fifth is the time distribution of targets by number of children ever born, w(j). Finally, we need to have an approximation of the mortality schedule experienced throughout the childbearing period of the target persons. The nature of these inputs is described in the appendix to this paper.
RESULTS FROM THE MODEL
Prevalence and Incidence at the National and Provincial Levels13
Figure 4-1a displays observed, fitted, and “adjusted-fitted” values of cumulated incidence for South Africa. The adjusted-fitted values obtain after correcting the associated post-peak incidence using a model-based procedure outlined in the appendix. Figure 4-1b shows the fitted and adjusted values of annual incidence rates consistent with estimated cumulated prevalence.14 Two points are worth mentioning. First, the fitted cumulated incidence shows a peak of about 0.45, a value lower than those utilized by the Joint United Nations Programme on HIV/AIDS (UNAIDS) (Zlotnik, personal communication). However, after adjusting the post-peak incidence rates we obtain a ceiling of about 0.53, a value more consistent with those imputed by other researchers. Second, although fitted and observed values are hard to distinguish from each other, we downplay this feature since the “observed” values are the result of operations that are of unknown nature to us.
Figure 4-2 shows adjusted incidence for South Africa and contrasts these with two provinces representing high and low HIV prevalence, KwaZulu-Natal and Limpopo. Note that the incidence rates in all three settings peak around the same year but at different levels, suggesting heterogeneity of ceilings and of stable incidence rates but not a different timing for the epidemic.
Households of the Elderly and HIV/AIDS Prevalence
Estimates of HIV prevalence can be used in simple ways to calculate the prevalence of elderly households with at least one HIV-infected adult child. The estimates are calculated by province and obtained as follows:
where k denotes the province, r denotes the number of adult (ages 15-49) members in the household, pk is the observed HIV prevalence among adults
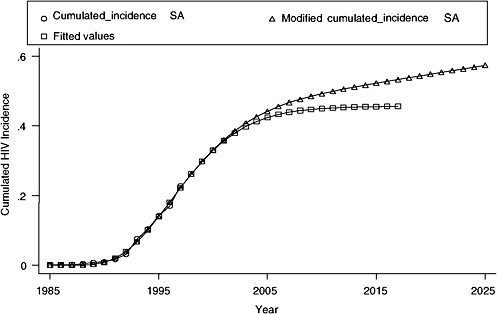
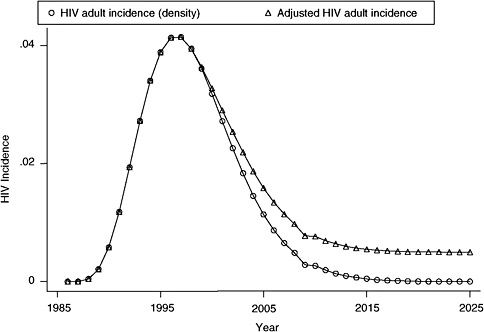
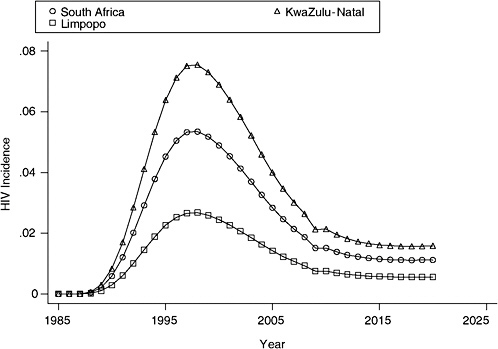
FIGURE 4-2 Estimated adult HIV incidence (density): KwaZulu-Natal, Limpopo, and South Africa.
in the province, and gk(r) is the fraction of all households containing an elderly member that include exactly r adult members. The values of rk are displayed in Table 4-2. Although the table is suggestive, the estimates rest on an assumption of independence that is likely to be violated. To the extent that infection of one adult member of the household is a marker for exposure for all other members of the same households (spouses and children), the quantities in Table 4-2 will overestimate the fraction of households with infected members. A bias in the same direction is possible due to the fact that the epidemic tends to cluster in social and ethnic groups. Since the expression overlooks such heterogeneity, it will generate overestimates of households’ HIV/AIDS prevalence, more so in provinces where heterogeneity of social groups is paramount. Provinces with higher average adult household size will tend to show a higher probability of at least one member’s being infected with HIV/AIDS even if the overall prevalence is relatively low. The figures in Table 4-2 show that in KwaZulu-Natal one should expect about 37 percent of households (with at least one adult member) having at least one infected adult. This is a remarkably high value, even
TABLE 4-2 Estimates of the Proportion of Households Containing at Least One Elderly Person with at Least One HIV-Infected Adult Member (by province, 1996)
|
Province |
HIV Prevalence (1996) |
Proportion |
|
Western Cape |
.031 |
.05 |
|
Eastern Cape |
.081 |
.15 |
|
Northern Cape |
.065 |
.13 |
|
Free State |
.180 |
.28 |
|
KwaZulu-Natal |
.199 |
.37 |
|
NorthWest |
.138 |
.27 |
|
Gauteng |
.155 |
.24 |
|
Mpumalanga |
.158 |
.29 |
|
Limpopo |
.080 |
.14 |
|
Total |
.142 |
.26 |
|
SOURCE: South Africa 1996 census, 10-percent sample. |
||
if upwardly biased. Still, there are provinces that are hardly touched by the epidemic, for example Western Cape.
Children of the Elderly and Their Experience with HIV/AIDS
Figure 4-3a displays the functions SI(y,t) evaluated in 1995 and 2005 (prob_healthy_1995 and prob_healthy_2005). In addition, the figure includes the probabilities of surviving to age y in the absence of HIV/AIDS (prob_survival_1995). The two SI(y,t) curves trace the probabilities that adult children born y years before the target year (values of y in the x-axis: 10, … , 55) are alive and healthy (uninfected) in years 1995 and 2005; the third set of plotted values represents the probabilities that the adult children will be alive in the absence of HIV/AIDS. Note that because all values of SI(y,t) are associated with real cohorts of adult children, they need not be monotonically decreasing. In fact, they should not be, since they must reflect, on one hand, the combined effects of mortality and of HIV incidence on the other. For example, in 2005 slightly more than 40 percent of the adult children age 20 were expected to survive with no HIV infection, whereas about 50 percent of those aged 50 will do so. This is because the burden of HIV weighs more heavily among the younger cohorts than among the older ones. While in the absence of HIV/AIDS an elderly parent could expect that almost 80 percent of her adult children born 30 years before would have survived to target year 2005, only 48 percent will survive healthy, not infected, as a result of the epidemic. This is a formidable load of illness that could potentially translate into reduced transfers of assets and
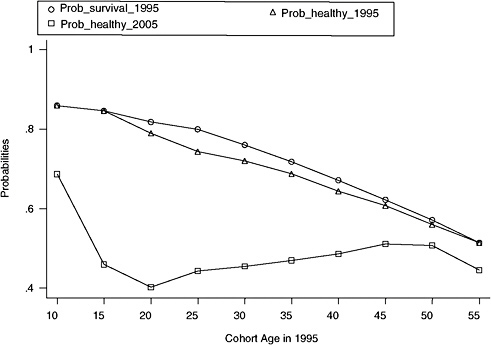
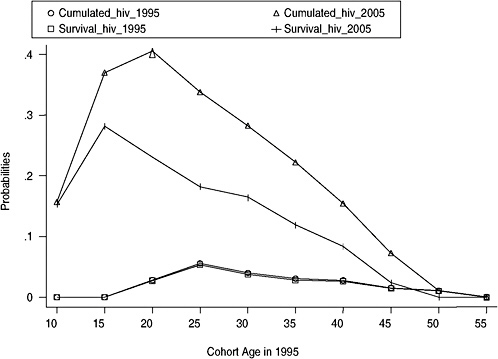
income to the elderly, additional labor, added burden to grandparents in the form of care for adult children and grandchildren, and, finally, reorganization of residential arrangements.
Figure 4-3b shows another face of the impact of the epidemic: the cumulated incidence of HIV by cohort of children (cumulated_hiv_1995 and cumulated_hiv_2005) and the cumulated survival among adult children who experience HIV (survival_hiv_1995 and survival_hiv_2005). The difference between these two sets of curves for each target year is a measure of the bereavement load on the elderly, the cumulated mortality among their adult children due to HIV/AIDS. Note that, as it should be given the youth of the epidemic, the bereavement load is trivial in 1995 (the lowest pairs of curves), but it grows to be as large as 0.20 among those in cohorts ages 20-35 in 2005: this implies that the probability of an adult child dying of HIV/AIDS before attaining ages 20-35 in 2005 is on the order of 0.20 or, equivalently, that a fifth of all daughters belonging to these cohorts will experience mortality due to HIV/AIDS.
Figures 4-4a and 4-4b are analogous to Figures 4-3a and 4-3b but correspond to evaluations in 2000 and 2010, respectively. The cumulated impact of the epidemic is quite visible in Figures 4-4a and 4-4b: only 35 percent of the cohorts born 20-30 years before 2010 will reach the target year without having been infected by HIV/AIDS. The bereavement load for elderly associated with adult children ages 20-30 in 2010 grows from 0.20 in 2005 to a staggering 0.35 in 2010. This means that the probability of an adult child dying of HIV/AIDS before attaining ages 20-35 in 2010 is on the order of 0.35. More than a third of all daughters belonging to these cohorts will die due to HIV/AIDS.
Table 4-3 displays summary measures for South Africa nationwide and two provinces with stark contrasts in the HIV/AIDS epidemic, KwaZulu-Natal and Limpopo. These figures contain the probabilities that the elderly ages 60, 65, and 70 will have children who are alive and healthy, infected, and dead to HIV/AIDS in selected target years. The numerical evaluation is for the pair of years 1995-2005 and for 2000-2010. The table sections associated with 1995 and 2005 trace the experience of the elderly ages 60, 65, and 70 in 1995 over 10 years until 2005. A similar interpretation applies to the sections associated with the years 2000 and 2010.15
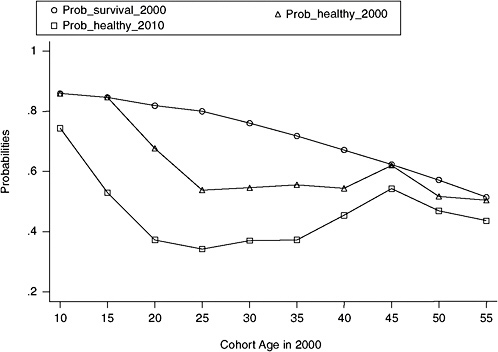
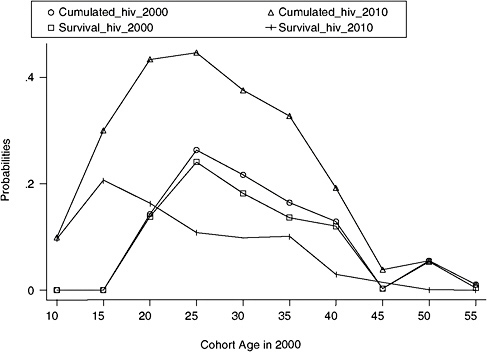
TABLE 4-3 Proportion of the Elderly Ages 60, 65, and 70 Who Will Have an Adult Child Infected with HIV or Dead Due to AIDS, 1995-2010
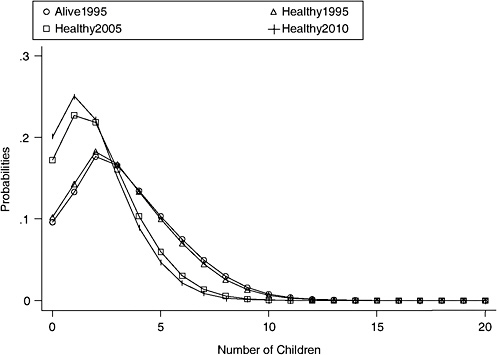
FIGURE 4-5 Problems of adult children alive-healthy, South Africa, 1995-2010.
Constraints on the Availability of Healthy Adult Children Imposed by HIV/AIDS
An outcome computable from the results of the model is the distribution of the elderly by number of children alive and healthy, infected with HIV, or dead due to AIDS. These estimates are indicators of demographic availability and of the potential burden of disease on the elderly. Figure 4-5 displays the estimated distribution of children surviving in 1995 in the absence of HIV/AIDS (alive1995) uninfected and alive in 1995 (healthy1995), and uninfected and alive in 2005 and in 2010 (healthy2005 and healthy 2010) for the elderly between ages 60 and 70 in the target year. The impact of HIV is remarkable: the distributions of healthy children narrows down considerably and drifts toward much lower means. The fraction of elderly with no surviving children (in the absence of HIV) is around 10 percent in 1995 but balloons to 18 and 20 percent in 2005 and 2010, respectively.
But the damage caused by the epidemic may be even larger than what these figures suggest. In fact, although the increase in the number of the elderly with no surviving children is a key determinant of the probability of the elderly living alone (Palloni, 2000; Wolf, 1994), the fall in the mean
number of healthy children may produce effects that are not captured by the results of the model. Indeed, while the model results indicate the magnitude and direction of demographic constraints placed on the elderly, they do not remove the uncertainty associated with endogenous effects, whereby demographic constraints may shift and alter residential propensities. Thus, while in some social settings the drop in the number of healthy children may increase the elderly’s propensities to live with adult children, because joint residential arrangements are a mechanism to cope with a sick adult child, in other settings it may increase the propensity of grandparents to take in their grandchildren to ease the burden on their sick adult children. A third social reaction could be more perverse, as elderly parents shy away from sick adult children to avoid social stigma and preference for coresidence is reduced. If the first mechanism were to prevail, we should expect an increase in the proportion of the elderly living with adult unmarried and widowed children. If instead the second mechanism dominates, we should observe an increase in living arrangements involving skipped-generation households. The third mechanism, together with the sheer pressure on the availability of surviving children produced by HIV/AIDS mortality, should lead to sharp increases in the proportion of the elderly living alone or with their spouse.
Our model results provide only benchmark estimates of the constraints in demographic availability but cannot tell us anything about actual residential arrangements. In order to investigate these, we turn now to results from the 1991, 1996, and 2001 data.
ANALYSIS OF CENSUS DATA
Orphanhood and Widowhood
Before turning to an examination of the observed living arrangements of the African elderly from the three South African censuses, we calibrate our ability to detect gross effects of HIV/AIDS from each data source. We do this by examining patterns of orphanhood and widowhood among African children and women. If the empirical results we obtain are broadly consistent with expected results, we have prima facie evidence that the three data sources reflect the impact of HIV/AIDS and that they can be used to inquire about other outcomes, such as the living arrangements of the elderly. Inconsistency between expected and observed results could mean one of two things: either that the epidemic has not yet gathered enough momentum to produce visible effects or, alternatively, that adjustment mechanisms obscure what should otherwise be clearly observed effects. If the first interpretation is correct, we should not expect to find large effects on residential arrangements, either. If the second explanation is more appropriate, our
ability to observe effects at the level of elderly residential arrangements will be a function of how effective adaptive mechanisms are, such as fosterage in the case of orphanhood and remarriage in the case of widowhood, in offsetting the impact of the epidemic.
To facilitate comparisons with other research (Zaba and Gregson, 1998) and because information on parental survival was not collected in the 1991 census, we estimate linear regressions of the logarithm of the proportion of orphans on the logarithm of prevalence by provinces from 1996 and 2001 census data. The estimated regression coefficients can be interpreted as elasticities or, equivalently, as the proportionate change in orphanhood relative to a proportionate change in HIV prevalence. Each regression is based on nine observations, one for each province.
To ensure consistency with other research, in each year we focus on three types of orphanhood (maternal, paternal, and dual orphans) in the age groups 0-4, which we regress on contemporaneous HIV prevalence.16 The R-squares fluctuate between 0.004 for paternal orphans in 2001 and 0.59 for maternal orphans in 2001. The elasticities for maternal and paternal orphanhood are 0.17 and -0.11 in 1996, and 0.64 and 0.04 in 2001. Estimates of relative changes in maternal orphanhood obtained from data collected elsewhere in Africa suggest elasticities in the range between 0.10 and 0.90 (Zaba and Gregson, 1998). Thus, our results fall within an expected, albeit fairly liberal, range. The estimated coefficient for maternal orphanhood for 2001 is, as expected, higher than for 1996, and it is statistically significant (p < 0.001). Differential fosterage practices, documented elsewhere in Africa (Ntozi et al., 1999b), may explain the much lower elasticities for paternal than maternal orphanhood. The elasticities of the proportion of dual orphans in 1996 and 2001 are 0.07 and 0.45, respectively: the change is in the expected direction and the higher 2001 coefficient is marginally significant (p = 0.09). These estimates are, respectively, 0.10 lower and 0.25 higher than estimates obtained from macrosimulation models (Palloni and Lee, 1992).
Because of the dynamics of HIV transmission and sex differences in the
age-specific incidence curve of HIV/AIDS, the progression of the HIV/AIDS epidemic is expected to increase first the proportion of women who are widowed. To assess the responsiveness of widowhood to HIV/AIDS, we estimate the elasticity of widowhood among women ages 15-59 with respect to HIV prevalence between 1991 and 2001. The focus on female widowhood in this age group is consistent with the age selectivity of AIDS mortality among men and the documented South African decline in mortality at the older ages over the 1990s (Dorrington et al., 2001). Elasticities for 1991, 1996, and 2001 are −0.006, 0.07, and 0.18, respectively. The increase in the elasticities is in the expected direction, but their values are low and not statistically significant, suggesting a weaker relationship between HIV/AIDS and widowhood than between HIV/AIDS and orphanhood. This may be partly explained by remarriage patterns, but also by the fact that widowhood itself is likely to be of short duration, truncated by the death of the surviving partner, since the infectious status of one of the partners is highly correlated with the infectious status of the other (Palloni and Lee, 1992). Paradoxically, the dynamics of HIV transmission censors the widowhood experience of the surviving partner and weakens one effect of the epidemic.17
In sum, these aggregate results reveal the signature of HIV/AIDS, as the epidemic progresses over time. The magnitude of the elasticity coefficients are also within the bounds of empirical or model-based estimates. However, the observed effects of the epidemic may be dampened by sociocultural responses, especially in the case of paternal orphanhood and female widowhood.
Patterns of Living Arrangements of the African Elderly
The taxonomy of living arrangements of the elderly adopted here is suggested by the outcomes of the macrosimulation model. We focus on four main residential arrangements of the elderly: (1) living alone or with a spouse,18 (2) living with unmarried or widowed adult children with or with-
out grandchildren, (3) living with grandchildren but no adult children, and (4) living with one or more orphaned grandchildren.
Similar to our previous analysis of orphanhood and widowhood, we explore the relationship between living arrangements of the African elderly age 60 and above and HIV prevalence across the nine South African provinces by estimating a linear regression of the logarithm of each type of living arrangement of the elderly in 1991, 1996, and 2001 on the logarithm of HIV prevalence. For each relationship, the data are shown by means of scatterplots of the values of the nine provinces together with the regression line that best fits the data, the estimated regression equation, and the associated R-square. While an increase in the size of the regression coefficient over time implies a stronger relationship between HIV and a given living arrangement, the movements of the regression line along the y axis imply a change in the proportion of the elderly living in a given living arrangement. Besides gauging the responsiveness of each type of living arrangement of the elderly to HIV prevalence, this approach also allows identification of patterns across provinces grouped according to their shared level of HIV prevalence and migration characteristics. 1991 provides the baseline observation for the period before the onset of the HIV/AIDS epidemic in South Africa, while the observations for 1996 and especially 2001 are for a period when the impact of HIV/AIDS should already be felt.19
Figure 4-6 shows the relationship between the fraction of the elderly living alone or with a spouse and HIV prevalence in 1991, 1996, and 2001. Based on model predictions, we expect the proportion of the elderly living alone or with a spouse to increase over the 1990s with increasing levels of HIV prevalence as a result of harsher constraints on the availability of adult children. However, although the fraction of the elderly experiencing solitary living has increased over time in most provinces, the association between this living arrangement and HIV is negative in all years. Rather than by changes in demographic availability of adult children, these patterns may be explained by forces of modernization, which, especially in the most urbanized provinces of Western Cape and Gauteng, may have weakened emotional ties that sustain traditional adherence to coresidence of the eld-
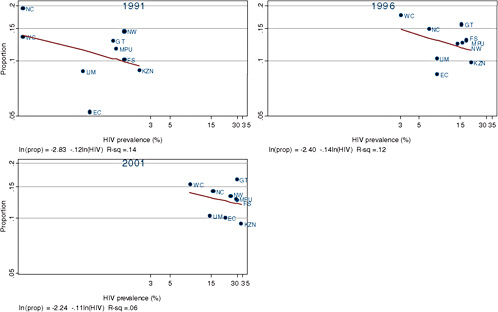
erly with their children and prevent the identification of the effects of HIV/ AIDS.
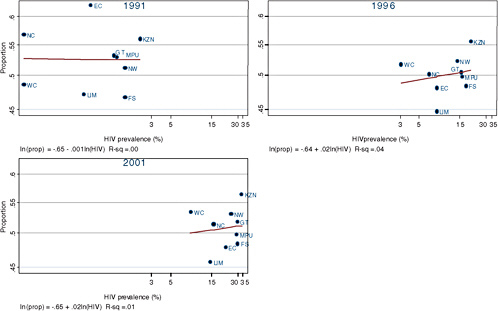
Similarly, in Figure 4-7, although model results predicted that increases in HIV/AIDS will be associated with increasing proportions of the elderly providing care for their sick adult children in the form of coresidence, the data show only very small increases in this type of living arrangement over time with the absence of an association between this type of living arrangement and HIV/AIDS.
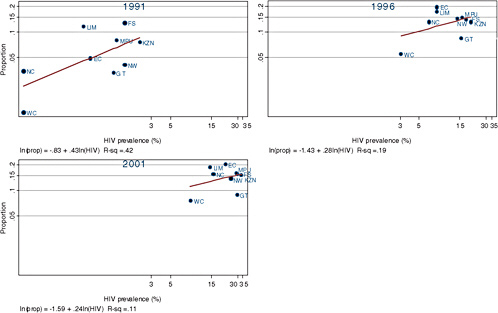
The macromodel further predicted an increase in the number of grandparents who live with a young grandchild to relieve the burden on their sick children or to provide care for their orphaned grandchildren. Indeed, in Figure 4-8 the fraction of the elderly living in skipped-generation households rises over time in all provinces. But if the rise in skipped-generation households were associated with HIV, we would expect to see a strengthening of the association over time. On the contrary, the association is weaker in 2001 and 1996 than it is in 1991. Like HIV/AIDS, migration is likely to provide the conditions for grandparents to take in their grandchildren. In fact, introducing controls for the levels of migration gauged by the proportion of households with at least one migrant worker in 1996 and 2001, the association between prevalence of skipped-generation households and HIV further weakens, while that with migration is strong. In 1996, the HIV coefficient drops to .04, while the coefficient for migration is high (.31) and statistically significant (p < 0.001). In 2001, the HIV coefficient drops to −.10 and the coefficient for migration is .26 (p < 0.001).
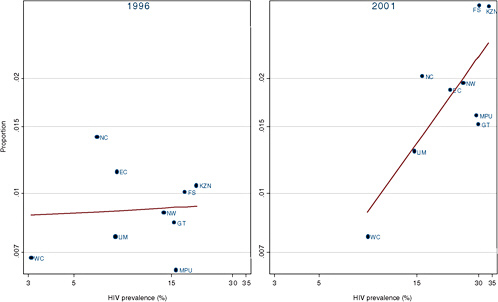
In order to unequivocally associate changes in the living arrangements of the elderly with the impact of HIV/AIDS, Figure 4-9 shows the relationship between HIV and the fraction of the elderly living with a dual orphaned grandchild in 1996 and 2001. The prevalence of this type of living arrangement does indeed rise between 1996 and 2001, and the size of the coefficient in 2001 is much larger than in 1996. In 2001, a 1 percent increase in HIV is associated with a 0.75 percent increase in the proportion of the elderly living with orphaned grandchildren (p < 0.01). The strong relationship between this type of living arrangement and HIV is suggestive of the elderly’s coping mechanisms with increased mortality due to HIV/AIDS.
CONCLUSION
We have focused on the effects of the HIV/AIDS epidemic on the living arrangements of the African elderly in South Africa, a country that over the last decade has experienced an exceptionally rapid spread of HIV/AIDS. We have proceeded in two steps. First, we combined results from macrosimulation models of the epidemic with backward and forward projections of HIV incidence and related mortality to estimate expected current
availability of adult children for the elderly, prevalence of sickness among the children born to elderly people, and to project changes in availability and sickness over the next 10 to 15 years. We then used the macromodel as a heuristic tool and compared expected outcomes with observed changes in the living arrangements of the elderly over time and across provinces, using three consecutive South African censuses conducted before and after the onset of the HIV/AIDS epidemic, in 1991, 1996, and 2001.
Because the progression of HIV/AIDS is expected to increase the proportion of children who are orphaned and the proportion of women who are widowed, we calibrated our ability to detect gross effects of HIV/AIDS by examining the association between patterns of orphanhood and widowhood among African children and women and HIV/AIDS in each data source. The examination of orphanhood and widowhood indeed revealed the signature of HIV/AIDS as the epidemic progresses over time.
The results from the macromodel suggested that the fall in the number of healthy children and the growing loss of children to AIDS may leave the elderly with fewer or no surviving children to live with and may increase the propensities of grandparents to take in their grandchildren to ease the burden on their sick adult children or to care for their orphaned grandchildren. Our descriptive analysis of changes in the living arrangements of the elderly as they relate to the growth of HIV prevalence has revealed flickers of evidence suggesting the effect of HIV/AIDS. Some of the outcomes we analyzed have changed in the way expected by models of availability, whereas some others have done so in accordance with what one would expect given hypothesized changes in preferences.
Most notably, in support of the expected decline in demographic availability of adult children due to HIV/AIDS, we have observed an increase in the proportion of the elderly who live with an orphaned grandchild in provinces that have experienced the fastest rise of HIV/AIDS prevalence. Where the record is inconclusive, it may be because the epidemic has not worked its way through with sufficient force, because individuals and groups react in ways that conceal the trail left by HIV/AIDS, or because we may be unable to distinguish the effects associated with HIV/AIDS from those triggered by migration, which mimics the effects of HIV/AIDS on the availability of kin, or those induced by modernization, which changes preferences for coresidence. As shown by the data, the observed growth of skipped-generation households is more likely to reflect levels and changes of provincial migration flows than the growth of HIV/AIDS. Similarly, our inability to detect the effects of HIV/AIDS on solitary living is overwhelmed by the tug of modernization, which may increase the elderly’s propensity for solitary living.
Establishing benchmarks using model-based approaches as we have done here is useful but insufficient. Unless all the minimal identification
conditions are simultaneously met, conventional cross-sectional data sources, such as censuses, can sustain only weak inferences, because they reduce the analytical options to a handful of indicators, for example, household distributions and the living arrangements of the elderly, which do not reveal the processes that produced them.
More promising ways to address the problem of identification of causal pathways include obtaining richer and better data, such as those provided by longitudinal studies or demographic surveillance systems performed at lower levels of aggregation. These data collection efforts can elicit direct information on residential preferences, changes in availability, and changes in actual living arrangements in subgroups affected and not affected by HIV/AIDS.
Another promising approach to enhance knowledge of the effects of the HIV/AIDS epidemic on the elderly and to isolate the most important contributors to observed patterns in living arrangements is the implementation of microsimulations that combine the realistic modeling of the HIV/AIDS epidemic, of kin availability, and of coresidence. The realism of the simulations hinges on the availability of demographic information (such as marriage, fertility, and mortality), epidemiological information to estimate parameters governing the spread of the epidemic (such as transmission probabilities, rates of partner change, incubation times), and information that enables the estimation of explicit rules of coresidence, such as the timing of children’s leaving home and types of destination households. While censuses and cross-sectional surveys provide information on realized residential arrangements, longitudinal studies and demographic surveillance systems are the ideal sources of quantitative information on residential rules and preferences and would easily accommodate questions aimed at the explicit identification of residential rules and preferences under AIDS and non-AIDS regimes.
APPENDIX TO CHAPTER 4
Assume we focus on an elderly woman age x who is alive in the census year 1995. This will be the target or target person and the year the target year. The main objective is to derive expressions for the following probabilities applicable to the female children born alive when the target was age x − y at time t − y: (a) that these female children have survived healthy (no HIV) to time t; (b) that they survived to t but contracted HIV along the way; and (c) that they have died due to HIV and other causes. In all these cases, the index variable y varies from a minimum equal to x − 50 to a maximum equal to x − 15, thus bounding the childbearing period of the target between ages 15 and 50. We assume that none of the targets contracted HIV prior to age x or that the fraction that does is trivial and can be
dismissed. Because we use a minimum value for x of 60, this assumption is sensible but not entirely accurate, since some of these women could have been infected in the 10 years prior to 1995. However, since the HIV incidence rates between ages 49 (attained the year the epidemic started) and 60 (attained in the middle of the census year 1996) are very low, the assumption is highly realistic. Furthermore, to the extent the assumption departs from reality, our calculations will be in error only if the childbearing patterns to which targets not affected by HIV and the mortality and HIV incidence pattern of her children are different from those that apply to targets who were infected prior to the target year.
To derive expressions for these probabilities, we rely on the following simplified scheme: let µ(z, t*) be the force of mortality (in the absence of HIV) at age z at year t*, the year when the target’s child attained age z, let ι(z, t*) be the rate of HIV infection at age z and time t*, and finally let γ(d) be the joint rate of incubation and mortality due to HIV/AIDS and other causes for individuals who have been infected d years. The set of all the target’s children born x − y years ago who could be age y at time t is the union of several disjoint subsets: one containing individuals who will not reach age y due to mortality in the absence of HIV, Q(y,t); another subset containing those who will attain age y at time t but are infected with HIV, QI(y,t); a third subset containing those who will die of HIV/AIDS-related causes, QID(y,t); and, finally, a subset including those who will attain age y at time t as healthy individuals (not infected), SI(y,t). The expression for the corresponding probabilities, referred to a target age x at time t, are as follows:
If one knows the time distribution of children ever born reflected in the age pattern of fertility to which women age x at time t were exposed during childbearing, ![]() , it is possible to calculate the weighted probabilities of having a child in any of the four statuses defined above. This is achieved multiplying
, it is possible to calculate the weighted probabilities of having a child in any of the four statuses defined above. This is achieved multiplying ![]() by each of the quantities defined above for every permissible value of y. These weighted values represent the average probabilities for an elderly woman age x at time t. In particular,
by each of the quantities defined above for every permissible value of y. These weighted values represent the average probabilities for an elderly woman age x at time t. In particular, ![]() is the average fraction of all children born to the target elderly women who are infected with HIV at age y at time t;
is the average fraction of all children born to the target elderly women who are infected with HIV at age y at time t; ![]() is the average probability of having a child age y at time t who is healthy; and, finally,
is the average probability of having a child age y at time t who is healthy; and, finally, ![]() is the average prob-
is the average prob-
ability of having lost a child to either HIV/AIDS or to mortality due to other causes.
In addition to the assumptions discussed above, we rely on the simplification that one can follow the progression to mortality of infected individuals by combining the force of mortality due to other causes, the incubation function, and AIDS-related mortality in a single synthetic superfunction, γ(d), which depends only on duration since infection and not at all on age.
Estimation of the Model
Estimation of the model depends of five pieces of information. The first and most important are the yearly HIV incidence rates from the onset of the epidemic until time t. The second is the incubation function that determines the waiting time in the infected state. The third is the mortality of healthy individuals, of individuals who are HIV+, and of those with full-blown AIDS. The fourth piece of information is the time distribution of children ever born or, equivalently, the fertility function approximating the childbearing experience of the target population. Finally, we also need the distribution of targets by number of children ever born, w(j). Below we briefly define the nature of these inputs.
Estimation of HIV Incidence
A most difficult task is to derive estimates of HIV incidence for the period 1985-2010. We proceed in several stages. In a first stage, we obtain a time series of prevalence estimates for each province during the period 1990-1999. These estimates were obtained from calculations made at Statistics South Africa using the estimates prepared by the UNAIDS and independent estimates obtained from surveillance sites and gathered at the U.S. Census Bureau. The second stage consisted of fitting a curve to the estimated cumulative prevalence, Pre(t). We used a Gamma function of the form
where d(t) is the duration of the epidemic at year t and k, α, and λ are parameters to be estimated.20 Our motivation in using this expression is more a matter of adherence to convention than of logical reasoning or empirical judgment; there is no compelling reason to prefer this function over
a virtually infinite set of equally plausible ones. Indeed, the utilization of this function leads to serious problems that require ad hoc solutions. The most important of these problems is that, by its own nature, the associated incidence curve—the density function associated with the cumulative Gamma function—will tend to peak very early and taper off and drift to zero very rapidly. For starters, this type of behavior is inconsistent with the possibility that HIV/AIDS becomes endemic with a constant level of incidence, a possibility that is not only mathematically feasible but also quite likely. Second, systematic comparisons with a number of simulated results using one detailed macromodel of HIV/AIDS (Palloni and Lamas, 1991) demonstrate that almost always, and regardless of the nature of input parameters, the Gamma incidence drops too fast and does not reflect at all the post-peak course of the epidemic.
To resolve this problem, other researchers have adopted arbitrary solutions. They cannot be otherwise, since there are no observations beyond the peak of the epidemic. Estimates exceeding that point are anybody’s guess. In this paper we adopt a rather sui generis solution: we take a large set of simulated results using parameters that are deemed to represent well the situation in South Africa (with respect to mortality, fertility, number of partners per person per year, etc.) and then retrieve the estimated incidence curves after the onset of the simulated epidemics. We then fit a Gamma function to the simulated cumulated prevalence, derive estimates of incidence, and calculate the difference between the simulated and estimated incidence rates. These differences are tantamount to “Gamma-adjustment factors.” To modify the post-peak estimated incidence for South Africa, we search for the set of Gamma parameters estimated in the simulated model that most closely resemble those observed in South Africa and adopt the corresponding Gamma-adjustment factors. We do not adjust the pre-peak estimates, which are heavily determined by the observed prevalence, but only the post-peak profile of incidence rates. In all provinces and in South Africa nationwide, the adjustments apply to the years after 2003, not before. In this sense, the uncertainty surrounding the estimates of HIV incidence is larger in the post-2003 period than before, when the estimates are at least more closely anchored to the trajectory of observed prevalence.21 This fact makes the calculations of the key quantities via forward projections less sensitive to errors associated with the use of incorrect Gamma-adjustment factors because post-peak epidemic incidence rates will affect
only the cohorts who reach age 15 some time after 2005. All our calculations refer to periods before 2010.22
Estimation of the Incubation Function
We assumed that γ(d) follows a Weibull hazard function with parameters α = .08 and β = 3.2, dictating a survival distribution with a median survival time of approximately 10 years. Given the fact that mortality among HIV-infected individuals in Africa is likely to be much higher than normal even in the absence of full-blown AIDS, this assumption does not seem unrealistic. It is also consistent with reports suggesting that the median survival time of HIV-infected individuals in Africa is of the order of 7.5 years (Boerma et al., 1998).23
Estimation of Healthy Mortality Levels
We use mortality levels estimated for South Africa by the United Nations (UN) for the period 1950-2000 and then the projected life expectancies through the year 2010 corresponding to the UN medium projections. For the years before 1950 we estimate life expectancy linearly, extrapolating backward from 1960. In all cases, we use the North female pattern of mortality from the Coale-Demeny model life tables.24
Estimation of Fertility and of  and w
and w
Estimates of ![]() were obtained from the age pattern of fertility implicit in the Coale-Demeny stable models. We made no extra efforts to approximate
were obtained from the age pattern of fertility implicit in the Coale-Demeny stable models. We made no extra efforts to approximate
closely a fertility scheduled for South Africa since what mattered in our calculation was the experience of women who are now 60 and above, that is, the childbearing experience pertaining to years as late as 1980 and as early as 1945. The fertility pattern between 1945 and 1975 at least is a matter of guesswork, and instead of deriving original estimates we chose to adhere to accepted age patterns that have been widely applied.
Estimates of w(j) were obtained directly from the observed distribution of children ever born to mothers age 50 at the time of the 1996 census. Although this distribution may differ from the one that applies to mothers age 60 and above in 1995, it is unlikely that the difference will be major, since substantial fertility changes are unlikely to have been experienced by women younger than 30 or 35 in 1996.
REFERENCES
Ainsworth, M., and Dayton, J. (2001). The impact of the AIDS epidemic on the health of the elderly in Northwestern Tanzania. Presented at the 2001 meeting of the Population Association of America, Washington, DC.
Ainsworth, M., and Over, M. (1999). Confronting AIDS: Public priorities in a global epidemic. New York: Oxford University Press.
Ainsworth, M., and Semali, I. (1998). The impact of adult deaths on the nutritional status of children. Presented at the Workshop on the Consequences of Maternal Morbidity and Mortality, October 19-20, Committee on Population, National Research Council, Washington, DC.
Barnett, T., and Blaikie, P. (1992). AIDS in Africa: Its present and future impact. New York: Guilford Press.
Bignami-Van Assche, S., Salomon, J.A., and Murray, C.J.L. (2005). Evidence from national population-based surveys on bias in antenatal clinic-based estimates of HIV prevalence. Presented at the 2005 meeting of the Population Association of America, March 31-April 2, Philadelphia, PA.
Boerma, T., Nunn, A.J., and Whitworth, A.G. (1998). Mortality impact of the AIDS epidemic: Evidence from community studies in less-developed countries. AIDS, 12(Suppl. 1), S3-S14.
Boerma, T., Urassa, M., Senkoro, K., Klokke, A., and Ng’weshemi, J.Z.L. (1999). Spread of HIV infection in a rural area in Tanzania. AIDS, 13, 1233-1240.
Bray, R. (2003). Predicting the social consequences of orphanhood in South Africa. African Journal of AIDS Research, 3, 39-55.
Bureau of Market Research. (2000). The South African provinces: Population and economic welfare levels. (Report 276). Pretoria: BMR, University of South Africa. Available: http://www.unisa.ac.za/Default.asp?Cmd=ViewContent&ContentID=2456 [accessed May 5, 2004].
Burman, S. (1996). Intergenerational family care: Legacy of the past, implications for the future. Journal of Southern African Studies, 22, 585-598.
Case, A., and Deaton, A. (1998). Large cash transfers to the elderly in South Africa. Economic Journal, 108, 1330-1361.
Collinson, M., Tollman, S., Kahn, K., and Clark, S. (2003). Highly prevalent circular migration: Households, mobility, and economic status in rural South Africa. Presented at the Conference on African Migration in Comparative Perspective, June 4-7, Johannesburg, South Africa.
Cronje, M., and Budlender, D. (2004). Comparing census 1996 and census 2001: An operational perspective. South African Journal of Demography, 9(1), 67-89.
Department of Health. (2003). National HIV and syphilis antenatal seroprevalence survey in South Africa, 2002. (Summary report). Pretoria, South Africa: Department of Health.
Dorrington, R., Bourne, D., Bradshaw, D., Laubscher, R., and Timaeus, I.M. (2001). The impact of HIV/AIDS on adult mortality in South Africa. (Technical report). Cape Town, South Africa: Burden of Disease Research Unit, South Africa Medical Research Council.
Foster, G., Makufa, C., Drew, R., and Kralovec, E. (1997). Factors leading to the establishment of child-headed households: The case of Zimbabwe. Health Transition Review, 7(Suppl. 2), 155-168.
Foster, G., Shakespeare, R., Chinemana, F., Jackson, H., Gregson, S., Marange, C., and Mashumba, S. (1995). Orphan prevalence and extended family care in a peri-urban community in Zimbabwe. AIDS Care, 7(1), 3-17.
Groenewald, P., Nannan, N., Bourne, D., Laubscher, R., and Bradshaw, D. (2005). Identifying deaths from AIDS in South Africa. AIDS, 19, 193-201.
Hosegood, V., Vanneste, A.M., and Timaeus, I.M. (2004). Levels and causes of adult mortality in rural South Africa: The impact of AIDS. AIDS, 18, 663-671.
Hunt, C.W. (1989). Migrant labor and sexually transmitted disease: AIDS in Africa. Journal of Health and Social Behavior, 30, 353-373.
Kinsella, K., and Ferreira, M. (1997). Aging trends: South Africa. (International brief no. 97-2). Washington, DC: Bureau of the Census, U.S. Department of Commerce.
Knodel, J., VanLandingham, M., Saengtienchai, C., and Im-em, W. (2001). Older people and AIDS: Quantitative evidence of the impact in Thailand. Social Science and Medicine, 52(9), 1313-1327.
Kok, P., O’Donovan, M., Bouare, O., and van Zyl, J. (2003). Post-apartheid patterns of internal migration in South Africa. Cape Town, South Africa: Human Sciences Research Council Publishers.
Livi-Bacci, M. (1978). La société italienne devant les crises de la mortalité. Firenze, Italy: Dipartimento Statistico.
Lurie, M., Harrison, A., Wilkinson, D., and Karim, S.A. (1997). Circular migration and sexual networking in rural KwaZulu-Natal: Implications for the spread of HIV and other sexually transmitted diseases. Health Transition Review, 7(Suppl. 3), 17-25.
Martin, W.G., and Beitel, M. (1987). The hidden abode of reproduction: Conceptualizing households in Southern Africa. Development and Change, 18, 215-234.
Marwick, M. (1978). Household composition and marriage in a Witwatersrand African township. In W.J. Argyle and E. Preston-Whyte (Eds.), Social system and tradition in Southern Africa (pp. 36-53). New York: Oxford University Press.
Møller, V., and Devey, R. (1995). Black South African families with older members: Opportunities and constraints. Southern African Journal of Gerontology, 4(2), 3-10.
Møller, V., and Sotshongaye, A. (1996). My family eats this money too: Pension sharing and self-respect among Zulu grandmothers. Southern African Journal of Gerontology, 5(2), 9-19.
Mukiza-Gapere, J., and Ntozi, J.P.M. (1995). Impact of AIDS on marriage patterns, customs, and practices in Uganda. Health Transition Review, 5(Suppl.), 201-208.
Murray, C. (1980). Migrant labour and changing family structure in the rural periphery of Southern Africa. Journal of Southern African Studies, 6(2), 139-156.
Murray, C. (1987). Class, gender, and the household: The development cycle in Southern Africa. Development and Change, 18, 235-259.
Ntozi, J.P.M. (1997). AIDS morbidity and the role of the family in patient care in Uganda. Health Transition Review, 7(Suppl.), 1-22.
Ntozi, J.P.M., and Zirimenya, S. (1999). Changes in household composition and family structure during the AIDS epidemic in Uganda. In I.O. Orubuloye, J.C. Caldwell, and J.P.M. Ntozi (Eds.), The continuing African HIV/AIDS epidemic in Africa: Response and coping strategies (pp. 193-209). Canberra: Australian National University, National Centre for Epidemiology and Population Health, Health Transition Centre.
Ntozi, J.P.M., Ahimbisibwe, F.E., Ayiga, N., Odwee, J.O., and Okurut, F.N. (1999a). The effect of the AIDS epidemic on widowhood in northern Uganda. In I.O. Orubuloye, J.C. Caldwell, and J.P.M. Ntozi (Eds.), The continuing African HIV/AIDS epidemic (pp. 211-224). Canberra: Australian National University, National Centre for Epidemiology and Population Health, Health Transition Centre.
Ntozi, J.P.M., Ahimbisibwe, F.E., Odwee, J.O., Ayiga, N., and Okurut, F.N. (1999b). Orphan care: The role of the extended family in northern Uganda. In I.O. Orubuloye, J.C. Caldwell, and J.P.M. Ntozi (Eds.), The continuing African HIV/AIDS epidemic (pp. 225-236). Canberra: Australian National University, National Centre for Epidemiology and Population Health, Health Transition Centre.
Nunn, A.J., Wagner, H.U., Kamali, A., Kengeya-Kayondo, J.F., and Mulder, D.W. (1995). Migration and HIV-1 seroprevalence in a rural Ugandan population. AIDS, 9, 503-506.
Orkin, F.M. (2000). From apartheid to democracy: Global lessons from a national experience. Paper presented at the International Association for Official Statistics Conference 2000 on Statistics, Development, and Human Rights, September 4-8, Montreux, Switzerland.
Palloni, A. (1990). Assessing the levels and impact of mortality in crisis situations. In J. Vallin, S. D’Souza, and A. Palloni (Eds.), Measurement and analysis of mortality: New approaches (pp. 215-249). New York: Oxford University Press. Also in (1988) J. Vallin, S. D’Souza, and A. Palloni (Eds.), Mesure et Analyse de la Mortalité: Nouvelles Approches. Paris, France: Institut National Etudes Démographiques.
Palloni, A. (2000). Living arrangements of older persons. (CDE Working Paper No. 2000-02). Madison: Center for Demography and Ecology, University of Wisconsin.
Palloni, A., and Lamas, L. (1991). The Palloni approach: A duration-dependent model of the spread of HIV/AIDS in Africa. In The AIDS epidemic and its demographic consequences (pp. 109-118). New York: United Nations and World Health Organization.
Palloni, A., and Lee, Y.J. (1992). Some aspects of the social context of HIV and its effects on women, children, and families. Population Bulletin of the United Nations, 33, 64-87.
Percival, V., and Homer-Dixon, T. (1995). Environmental scarcity and violent conflict: The case of South Africa. (Occasional paper for Project on Environment, Population, and Security). Washington, DC: American Association for the Advancement of Science and the University of Toronto.
Pison, G., Le Guenno, B., Lagarde, E., Enel, C., and Seck, C. (1993). Seasonal migration: A risk factor for HIV infection in rural Senegal. Journal of Acquired Immune Deficiency Syndromes, 6(2), 196-200.
Posel, D., and Casale, D. (2002, September). What has been happening to internal labour migration in South Africa, 1993-1999? (DPRU Working Paper No. 03/74). Cape Town, South Africa: Development Policy Research Unit.
Potash, B. (Ed.). (1986). Widows in African societies. Stanford, CA: Stanford University Press.
Quinn, T.C. (1994). Population migration and the spread of types 1 and 2 human immunodeficiency viruses. Proceedings of the National Academy of Sciences, 91, 2407-2414.
Quinn T.C., Mann, J.M., Curran, J.W., and Piot, P. (1986). AIDS in Africa: An epidemiologic paradigm. Science, 234(4779), 955-963.
Republic of South Africa Central Statistical Service. (1991). Census 91: 1991 population census. Pretoria, South Africa: Central Statistical Service.
Ruggles, S. (1987). Prolonged connections: The rise of the extended family in nineteenth-century England and America. Madison: University of Wisconsin Press.
Russell, M. (1998). Black urban households in South Africa. African Sociological Review, 2(1), 174-180.
Sher, R. (1986, October). Acquired immune deficiency syndrome (AIDS) in the RSA. Supplement to South African Medical Journal, 23-26.
Smit, R. (2001). The impact of labor migration on African families in South Africa: Yesterday and today. Journal of Comparative Family Studies, 32(4), 533-548.
Spiegel, A., Watson, V., and Wilkinson, P. (1996). Domestic diversity and fluidity among some African households in greater Cape Town. Social Dynamics, 22(1), 7-30.
Statistics South Africa. (1998a). The people of South Africa: Population census 1996, 10% sample of unit records. (Report No. 03-01013, 1996). Pretoria: Author.
Statistics South Africa. (1998b). Statistics for the calculation of the management echelon post provision for provincial administrations. Pretoria: Author.
Statistics South Africa. (1998c). October Household Survey (OHS), 1998. Pretoria: Author.
Statistics South Africa. (2001). Census 2001 10% sample. Pretoria: Author.
Statistics South Africa. (2004). Census 2001: Concepts and definitions (Report No. 03-02-26, 2001). Pretoria: Author.
Ubomba-Jaswa, P. (2000). The dying game: HIV/AIDS in South Africa. Unpublished manuscript, School of Development Studies, University of Natal-Durban, Durban, South Africa.
Urassa, M., Boerma, J.T., Ng’weshemi, J.Z.L., Isingo, R., Schapink, D., and Kumugola, Y. (1997). Orphanhood, child fostering, and the AIDS epidemic in rural Tanzania. Health Transition Review, 7(Suppl. 2), 141-153.
Urassa, M., Boerma, J.T., Isingo, R., Ngalula, J., Ng’weshemi, J.Z.L., Mwaluko, G., and Zaba, B. (2001). The impact of HIV/AIDS on mortality and household mobility in rural Tanzania. AIDS, 15, 1-7.
Wachter, K.W., Hammel, E.A., and Laslett, P. (1978). Statistical studies of historical social structure. New York: Academic Press.
Wachter, K.W., Knodel, J.E., and VanLandingham, M. (2002). AIDS and the elderly of Thailand: Projecting familial impacts. Demography, 39, 25-41.
Wolf, D.A. (1994). The elderly and their kin: Patterns of availability and access. In National Research Council, Demography of aging (pp. 146-194). L.G. Martin and S.H. Preston, Eds. Committee on Population, Commission on Behavioral and Social Sciences and Education. Washington, DC: National Academy Press.
Zaba, B., and Gregson, S. (1998). Impacts of HIV on fertility and family structure. Prepared for the World Bank/UNAIDS Seminar on Demographic Impacts of HIV.
Zuberi, T., and Khalfani, A.K. (1999). Racial classification and the census in South Africa, 1911-1996. (ACAP Working Paper No. 7). Philadelphia: University of Pennsylvania.

















































