
3
Demographic Impacts of the HIV Epidemic and Consequences of Population-Wide Treatment of HIV for the Elderly: Results from Microsimulation
Samuel J. Clark
INTRODUCTION
The high levels and continued increase in HIV prevalence in parts of sub-Saharan Africa are bringing with them substantial increases in adult mortality (Dorrington, Bourne, Bradshaw, Laubsher, and Timaeus, 2001; Timaeus, 1998; Joint United Nations Programme on HIV/AIDS, 2002) and decreases in fertility (Gregson, 1994; Gregson, Zaba, and Garnett, 1999; Zaba, 1998). Together these change the composition of infected populations significantly with important consequences for the elderly. Added to this is the potential for widespread prevention and treatment programs that will have substantial impacts of their own.
One of the most important and widely recognized consequences for the elderly is the creation of a large number of “AIDS orphans”—children who lose one or both of their parents as a result of HIV-related mortality. The report Children on the Brink: 2002 indicates that there were 38 million orphans in Africa in 2001, 11 million of whom were attributable to AIDS mortality (Joint United Nations Programme on HIV/AIDS, UNICEF, and U.S. Agency for International Development, 2002). The same report predicts it is likely that there will be 42 million orphans in Africa in 2010, 20 million of whom are the result of AIDS mortality; others make even larger estimates of the number of orphans by 2010 (Monk, 2002). Bicego, Rutstein, and Johnson (2003) observed a strong correlation between the percentage of children who are orphans and national HIV prevalence for several African countries during the 1990s, lending weight to the conclusion that HIV is related to the rise in the number of orphans.
The sheer number of orphans being created is unusual in human history, as is the fact that many are dual orphans, children who have lost both parents and must be cared for by someone else. Compounding the problem for the elderly is the fact that their own numbers and the proportion of the population they constitute are also being affected by the epidemic, and all of the changes wrought by an HIV epidemic evolve as the epidemic grows and stabilizes. Accordingly, to adequately understand the total impact of the epidemic on the number and proportion of children who are orphans and on the number of grandparents and other family members who will be alive to care for them, one must employ a “whole population” model. Such a model takes into account all of the major avenues through which HIV impacts a population and how these interact with one another. Gregson, Garnett, and Anderson (1994) constructed one such model in the mid-1990s and used it to predict the major increase in the number and proportion of children who are orphaned as a result of HIV. Many of their theoretical findings are being validated now, as the epidemic unfolds and large numbers of orphans begin to appear in the worst affected African countries (Joint United Nations Programme on HIV/AIDS, UNICEF, and U.S. Agency for International Development, 2002).
Gregson and colleagues (1994) also examined more general demographic impacts of an HIV epidemic and demonstrate significant changes in the age-specific sex ratio, population age structure, and overall growth rates—all of which affect the elderly as the underlying structure and size of the population changes. Results presented here largely corroborate their findings while adding some additional nuances.
The work presented here employs a different modeling strategy from that used by Gregson and colleagues (1994) to explore many of the same questions. The individual-level microsimulator used here is capable of modeling marriage, sex, and the biological and behavioral impacts of HIV. The individual-level nature of the model allows it to track the links between parents and children and grandparents and grandchildren. In comparison to the deterministic, compartmental model used by Gregson and colleagues, this model provides a direct means through which to measure the number of orphans and the number of grandparents who could be living with orphaned grandchildren. In addition, it is able to realistically model two different types of intervention: a preventive, largely behaviorally mediated intervention and an antiretroviral treatment program, which reduces viral load and increases the time between infection and death without having other specific preventive effects. Treatment programs of these two types are simulated in the late phase of an HIV epidemic to ascertain their overall effects and how these affect the situation of the elderly. It is important to keep in mind that the microsimulator used here is a heuristic tool that allows us to explore the intricate, interrelated processes operating to create
an HIV epidemic. A heuristic tool of this kind is not designed to faithfully reproduce a specific population, but rather to represent a generalized population of a given type, sub-Saharan African in this case, and to provide a virtual sandbox in which to manipulate that population in order to gain better understandings of the inner workings of a system of that type.
Below we discuss the specific questions to which the model is addressed and provide some context for each. Following that is a brief discussion of the simulator itself. A full description of the model and its calibration is outside the scope of this work but can be found in detail elsewhere (Clark, 2001a). Finally there is a detailed presentation of the results from 15 40-year simulations, three in each of five scenarios: (1) a stable population with no HIV, (2) a population with untreated HIV, (3) a population with HIV treated with a preventive program, (4) a population with HIV treated with antiretrovirals, and (5) a population with HIV treated with both preventive and antiretroviral treatment programs.
QUESTIONS
Orphans can be created either through the loss of one or both of a child’s parents or through abandonment by one or both parents. Orphans of the first type are genealogical or demographic orphans, while those of the second type are social orphans. HIV-related mortality in Africa is primarily creating orphans of the first, genealogical, type. The strong household and extended family structure in many African settings is absorbing the vast number of orphans created by HIV-related morbidity and is thereby preventing the creation of a large number of social orphans. In addition to other related adults, elderly people play a critical role in this extended family.
This work addresses the demographic and structural consequences of heterosexually spread HIV epidemics and the impacts of different treatment strategies on elderly people. Consequently, the following investigations address structural questions relating to genealogical or demographic orphanhood. This in and of itself is a surprisingly complicated set of issues, which must be well understood in order to begin studying the very urgent and important social problems wrought by the creation of so many genealogical orphans. Future work will add household and extended family structures to the existing modeling framework in order to begin addressing questions relating to the impact of orphanhood on a more broadly defined set of older kin.
As a heterosexually transmitted HIV epidemic grows and a substantial fraction of the general adult population is infected, the structure of the population gradually changes as a result of the influences of HIV—often mediated through behavioral mechanisms—on mortality, and perhaps more
important, on fertility. These structural changes have significant implications for older people, and it is specifically these impacts that are the focus of the questions posed here.
In addition to the structural changes resulting from the disease directly, prevention and treatment programs have significantly different structural effects that arise from their varied effects on the transmission and progression of HIV infections. Taking this into account, the two primary questions posed below are examined in five different treatment scenarios to ascertain the impacts of both the HIV epidemic itself and various treatment programs.
Number of Orphans
One of the most discussed impacts of heterosexually transmitted HIV epidemics is the excess number of orphans they can generate, and the potential for those orphans to place additional burdens on the elderly. Throughout the remainder of this work I use the word “orphan” to indicate genealogical or demographic orphans—children who have lost one or both of their biological parents. Establishing the relationship between the population prevalence of HIV and the number of additional orphans generated is complicated by the facts that (1) the HIV-related mortality of women and their children is strongly correlated, leading to significant excess HIV-related mortality of orphans who result from women’s HIV-related mortality and (2) the magnitude of non-HIV-related excess mortality suffered by orphans as a result of simply being orphans is poorly measured. This is mainly because orphans have historically been relatively rare, are often difficult to identify if they have been fostered, are less likely than nonorphans to be covered by many data collection systems, and finally because the excess mortality seems to persist for only a short period immediately after the death of the parent(s), making it less likely that dead children who have very recently been orphaned are properly categorized as orphans at the time of their deaths.
Given that accurate reliable empirical data describing orphans are unusual, one must turn to modeling to gain a better understanding of the relationship between overall indicators of an HIV epidemic and the number and sex and age distribution of orphans. To accurately model the creation of orphans, the link between individual parents and their individual children must be represented—something that is possible only in an individual-level modeling framework like the one employed here. In the context of an HIV epidemic, maternal, paternal, and dual orphans are of interest, which requires the model to represent and account for marriage so that children who lose their father can be identified. However, simply accounting for the links between parents and children is insufficient because the overall num-
ber of orphans of a given age is a function of fertility, adult mortality, child mortality rates, and the size of the base population of adults and orphans to which those rates are applied. Consequently, to realistically model orphan-hood, it is necessary to accurately model an entire two-sex population at the individual level with realistic pairing dynamics.
The model utilized for this work is of this type and is suitable to accurately model orphanhood dynamics in the context of a whole population. Because mother-to-child transmission of HIV is modeled and infection with the virus has realistic duration-since-infection impacts on the mortality of both adults and children, the correlation between the mortality of mothers and children resulting from HIV infection is correctly modeled. However, the model does not account for the additional non-HIV-related excess mortality associated with being an orphan; empirical work in progress by the author suggests that there is substantial excess mortality associated with becoming an orphan—during the first year after losing their mother for young children (Clark, 2004). Taking this into account, the mortality of orphans is underrepresented in the model and consequently the model produces a conservative (slight over-) estimate of the number of orphans.
A number of specific questions relate to the number and fraction of all children who are maternal, paternal, and dual orphans as an HIV epidemic grows and stabilizes:
-
How many and what percentage of children are maternal, paternal, and dual orphans in a rapidly growing population with relatively high mortality but no HIV?
-
How many and what percentage of children are maternal, paternal, and dual orphans in the same population infected with HIV, and how do these indicators change as the HIV epidemic grows and stabilizes?
-
What impact do preventive (behavioral) and antiretroviral treatment programs have on the number and percentage of children who are maternal, paternal, and dual orphans after an HIV epidemic has stabilized?
Numbers of Children and Grandchildren
The important intergenerational consequence (alluded to above) of a significant increase in the number of orphans is that after children lose both parents, other members of the extended family, including grandparents, often must take responsibility for them. If large numbers of maternal and dual orphans are produced, these orphaned children will become a significant challenge for the extended family, the social services that may be available to assist them, and, particularly in the case of dual orphans, for grandparents who must care for them. Recognizing that a variety of related adults
will contribute to the care of orphans, the specific aim of this work is to examine the impacts of HIV and its treatments on the elderly, and consequently the focus is on genealogically related grandparents who are likely to be the elderly people most closely related to the orphans.
To adequately describe and investigate this issue, all links between parents and children must be known so that links between grandparents and grandchildren can be reconstructed. Empirical studies of this issue must both record these links and have good data to describe orphans— something that very few empirical studies have. This strongly motivates a modeling approach to gain insight into these issues. The model employed here produces a realistic base population affected by HIV, including the number and age distribution of children, orphans, adults, and adults age 50 and over. Combined with the links between parents and children, it is possible to examine changes in the average number of orphaned grandchildren per grandparent age 50 and over, taking into account sex differentials brought about by the sex differentials in HIV-related mortality and consequent distortions in the age-specific sex ratio.
A number of specific questions relate to the number of orphaned grandchildren per grandparent age 50 and older as an HIV epidemic grows and stabilizes:
-
How many and what percentage of adults age 50 and older have surviving orphaned grandchildren but no surviving children in a rapidly growing population with relatively high mortality but no HIV?
-
How many and what percentage of adults age 50 and older have surviving orphaned grandchildren but no surviving children in the same population infected with HIV, and how do these indicators change as the HIV epidemic grows and stabilizes?
-
Are there different numbers and percentages of elderly women and men age 50 and older who have surviving grandchildren but no surviving children as an HIV epidemic grows? How much of a difference is there?
-
As an HIV epidemic grows and stabilizes, how are the different numbers and percentages of elderly women and men age 50 and older with surviving grandchildren but no surviving children related to the prevalence of HIV in the population as a whole and the prevalence of HIV among those age 50 and older?
-
What impact do preventive (behavioral) and antiretroviral treatment programs have on the number and percentage of adults age 50 and older who have surviving orphaned grandchildren but no surviving children after an HIV epidemic has stabilized?
METHODS
The questions posed above are generally not amenable to empirical investigation in their entirety because that would require observation of whole populations over the entire period during which HIV epidemics subjected to various forms of treatment grow and stabilize. In addition, the level of detailed information necessary to investigate the intergenerational questions is typically not available from empirical studies. And finally, ethical concerns relating to measuring the incidence and prevalence of HIV would make empirical studies of this type prohibitively expensive and in most cases impossible—through the influence of the investigation on the process.
In contrast, modeling is comparatively very cheap, flexible, fast, and ethically neutral. The primary disadvantage is that models are not the real thing, nor will they even reflect the real thing very well; so whatever insights are gained through modeling are transmitted through a comparatively blurry, low-resolution lens. In addition, the closer a model is to representing the complexity of reality, the more difficult it is to parameterize with empirically observed parameters. So, one lives with relatively simple models that average the internal complexity of reality and reflect the aggregate reality well, or more complex models that begin to adequately reflect the internal complexity of reality but do not reflect aggregate reality well because complete sets of empirically observed parameter values are not available. Vast quantities of accurate, detailed, individual-level data are required to adequately parameterize models of the second type, and this heavy data requirement often limits the application of such models. Models in the first group are useful to project or predict into the future with reasonable accuracy, while models in the second group are useful to probe the inner workings of a system and understand how the components of a system are related to each other in a dynamic sense over time and as the system is perturbed.
To understand how heterosexually transmitted HIV affects populations, one needs to understand how it affects various components of a population and how these effects in turn affect other components of the population and interact synergistically to produce the population-level impacts observed. Investigations of this type are best pursued by using the second type of model that offers an ability to manipulate and observe the inner workings of a process in detail.
The questions posed here are investigated using a two-sex, individual-level stochastic microsimulator (Clark, 2001d) parameterized with empirically observed mortality, fertility, and nuptiality parameters describing a rural population living in southern Zambia1 between 1950 and 1995
(Clark, 2001c). The populations it simulates closely resemble rapidly growing, high-fertility, high-mortality, polygynous populations similar to those now living in parts of Southern Africa. The simulator models polygynous marital and both polygynous and polyandrous nonmarital pairings2 of men and women, and, within all these types of union, individual sexual intercourse events. The sexual intercourse events lead to both conceptions and the transmission of the human immunodeficiency virus, thereby tightly and accurately coupling reproduction of the population and transmission of the virus. Once infected with the virus, an individual gradually develops AIDS and eventually dies. During this progression, the disease impacts both their behavior and biology, causing them to be, among many things, less likely to enter into unions of all types, less likely to have sex, more likely to be divorced, increasingly more likely to die and, if female, less likely to conceive and more likely to miscarry.
Simulator
In this section is a very brief description of the simulator, containing just enough detail to understand what it is, how it works, and what it produces. For a detailed description of the simulator, see Clark (2001d), and for a complete exposition of the large set of demographic parameters and how they were calculated, see Clark (2001c).3 Both these references can be downloaded from Clark (2001b).
The simulator contains entities corresponding to individual people, individual unions (both marital and extramarital) between men and women, fertility histories for women, and pregnancies for women. Together with the union-mediated links between spouses or partners and between parents and children, this is sufficient to model all the important dynamics of a whole population. Planned additions to the simulator include modeling households, but this requires a significant amount of so far unavailable quantitative data describing the detailed dynamics of households.
Simulated time is incremented in units of one month, and during each month every entity is exposed to the risk of the events for which it is eligible. Event hazards governing the monthly probability of occurrence of each event are compared with random numbers to decide which events occur during a given month. These occurrences and their repercussions are recorded—often changing the eligibility of the affected entities for future events—and the process is repeated until the desired number of months has been simulated.
The simulator utilizes a relational database to store the long event histories generated by this process. The Structured Query Language (SQL) is used to manipulate the database—both to conduct the simulation and to extract data for analysis. The additional logic necessary to run the simulator is written in Visual Basic for Applications® (a standard programming language) that makes changes to the database by executing SQL. A significant benefit of this architecture is that the entire history of every modeled entity is recorded permanently, a situation that allows unlimited ad hoc analysis of the resulting simulated population using the same tools one would employ to analyze similar data describing a real population. Another benefit is that any simulation can be stopped and restarted without having to employ any special logic or procedures. Additional benefits include the ability to easily utilize both time-invariant and time-varying parameters, and through the straightforward use of SQL, to employ dynamically scaled parameters that are functions of aggregate indicators that are calculated on the fly as the simulation progresses.
Simulator Components
The simulator is organized around modules that manage events relating to (1) mortality, (2) fertility, (3) nuptiality, (4) extramarital unions, or affairs, and (5) sexual intercourse—which occurs with differing frequency in the context of the two types of unions. An additional module manages the effects of infection with HIV on the event probabilities that are managed by the other five modules. See Clark (2001d) for a detailed description of these components and how they interact.
The set of parameters used to parameterize the simulator is too large to describe here; see Clark (2001d) for details. The parameter values are derived from 40 years of observation of a population living in southern Zam-bia. Those data are unique for Africa and make it possible to calculate a complete, internally consistent set of parameters describing the dynamics of an African population. With very few exceptions, such data are unavailable for other parts of Africa, and it is primarily for this reason that they were chosen to parameterize the simulator. Stable populations unaffected by HIV that result from running the simulator for many years with the parameter
set used for this work have (1) mortality levels associated with expectations of life at birth of about 50 years for men and about 52 years for women, (2) fertility levels associated with a total fertility rate of about 6.2, and (3) annual proportionate growth rates of about 4 percent. These and more specific indicator values closely match the empirical values describing the population of Gwembe Tonga (in southern Zambia), from which the parameter values are taken (see Clark, 2001d).
Effects of HIV
An HIV disease progression (DP) indicator is used to govern the progress of an infected individual’s HIV infection. The DP indicator consists of a time series of values that correspond loosely to an infected individual’s viral load as the disease progresses. The shape of this indicator with time is different for children and adults, reflecting the different pace of the disease in children and adults. The shape of the DP indicator with time is that of a lop-sided U with the initial value being small but rapidly decreasing to a very small value that persists for some time and very slowly increases. For children the rapid increase begins at about 18 months after infection, and for adults the DP begins to increase steadily from about 80 months, reaching substantial levels at about 120 months.
HIV treatment programs that utilize antiretroviral pharmaceuticals to suppress viral load and extend the life of infected individuals are modeled by changing the shape and time scale of the DP indicator. For adults, the whole curve is stretched by about 10 years and the intermediate values are diminished to approximately zero—mimicking the effects of properly administered antiretroviral drugs. For children, the curve is stretched by about three years.
The DP indictors translate into average times between death and infection of about 10 years for adults and 2 years for children with no antiretroviral treatment, and 20 years for adults and 5 years for children with antiretroviral treatment.
Transmission of HIV between adults occurs only through heterosexual sexual intercourse from an infected individual to their partner, with an average per intercourse probability of transmission of roughly 10−3 over the course of an HIV infected individual’s disease. Individuals can be infected more than once, but their DP indicator starts at the date of their first infection. The actual transmission probability applied to each intercourse event is scaled by the DP indicator of the infected individual, allowing the transmission probability to change as the disease progresses and roughly reflect the infected individual’s viral load and hence their potential to transmit.
Infected mothers transmit the virus to their newborns at birth, with an average transmission probability of about .3 over the course of an infected
woman’s disease. Again, the specific transmission probability applied to a given birth is scaled by the mother’s DP indicator, allowing her transmission probability to track the progress of her disease and accurately reflect her viral load and hence her potential to transmit at each time following her own infection.
The transmission probability utilized in both the horizontal and vertical modes of transmission is governed by the infected individual’s DP indicator, allowing changes in the DP indicator—such as those that implement the virtual antiretroviral treatment program—to be reflected in the transmission probabilities.
Infection with HIV has a number of other effects whose details are not discussed here beyond mentioning that they are implemented; see Clark (2001d) for details on these effects. Being HIV positive affects
-
the probability that a conception will lead to a miscarriage,
-
the fecundity of an infected woman,
-
the daily hazard of intercourse between a man and a woman if one or both are infected,
-
the probability of transmitting the virus from an infected to an uninfected individual through sexual intercourse,
-
the probability of transmitting the virus from an infected woman to her newborn child through the birth process,
-
the probability that a possible couple with one or both possible partners infected will form a marital union,
-
the probability that a marital union will dissolve if one or both of the partners are infected, and
-
the probability that an infected individual will die.
Indicators
Indicators presented to explore the questions posed above include measures of the composition of the population through time and the prevalence of HIV in various sex and age groups. The majority of these are familiar, are calculated in the standard way, and should be self-explanatory in terms of definitions and calculation methods (see Preston, Heuveline, and Guillot, 2001).
The orphanhood indicators relate to maternal (mother dead), paternal (father dead), and dual (both parents dead) orphans age 15 and younger. The percentage of children who are orphans of each type are presented as a function of time. The percentage of children who are orphans is calculated as the ratio of the number of children who are orphaned (by type) to the total number of children, including the orphans.
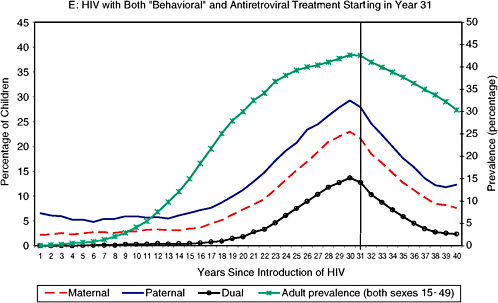
The grandchildren indicators relate the total number of adults age 50
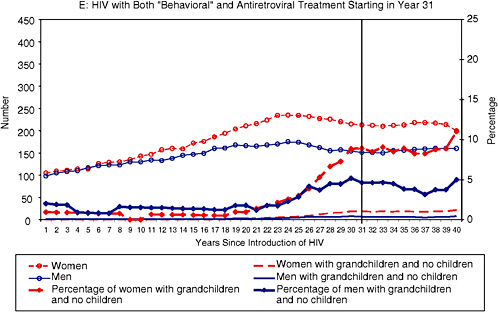
and over (by sex) to the number of their surviving children and grandchildren over time. The indicators presented here are the sex-specific: (1) total number of adults age 50 and older, (2) the total number of adults age 50 and older who have no surviving children but at least one surviving grandchild under the age of 15, and (3) the percentage of total adults age 50 and older who have no surviving children but at least one surviving grandchild under the age of 15.
HIV Prevalence
Sex- and age-specific HIV prevalence is calculated as the ratio of the number of person-years lived infected with HIV to the total number of person-years lived. Age-specific HIV prevalence values are weighted by the age structure of wider age groups to aggregate HIV prevalence across those wider age groups (i.e., 15-64).
Running the Simulator: Five Scenarios
To start the analysis presented here, a stable population consisting of 1,271 women and 1,230 men was created by letting the simulator run for 150 years from an initial population consisting of 15 women and 15 men of young reproductive age. This stable population served as the starting point for all of the simulations presented here and is referred to as P0 below.
The choice was made to begin “treatment” in the treated simulations in year 31 of the 40 years that are simulated for each of the scenarios described below. This is to roughly mimic the sequence of events in the HIV epidemics in Southern Africa. HIV has been affecting Central Africa for 30 to 40 years and Southern Africa for 15 to 30 years. Widespread treatment programs are in the near future for South Africa and perhaps for other nations in the region, so it seems appropriate to let the HIV epidemics grow for three decades before instituting treatment programs in order to roughly mirror the time scale of the real epidemics and their potential treatment in Southern Africa. Future work will address the impact of treatment programs earlier and later in the life of the epidemic.
Population Without HIV
Three simulations were run from P0 for 40 years without any HIV infection, resulting in final population sizes of roughly 12,000 individuals. These three simulations serve as the healthy “control” to which the HIV-affected simulations can be compared. They also provide some feel for the level of stochastic variability that one may expect to see in the various indi-
cators unaffected by HIV. Averages of these three simulations are presented as the “No HIV” results below.
Population with Untreated HIV
Three simulations were run from P0 for 40 years with HIV. Throughout these simulations there was a very low hazard of “external” infection (equal to 15 per 100,000 per month) for adults ages 15 to 49. Because the simulated population is a closed one, the epidemic has to be seeded in some reasonably realistic way, and without modeling special high-risk groups and their subdynamics within the population, this seems like the most reasonable approach. Over the course of a typical 40-year HIV simulation, about 2 to 3 percent of all adult infections ages 15 to 49 resulted from “random external” transmission—a value that does not seem unreasonable. Averages of these three are presented as the “HIV” results below.
Population with HIV Treated with Behavioral Preventative Programs
A behaviorally mediated HIV prevention program was simulated using the three HIV simulations. Starting in year 31 and running for 10 years through year 40, each of the three HIV populations was subjected to a complete cessation of the formation of extramarital relationships. This had the immediate effect of reducing women’s exposure to intercourse and completely curtailed the high levels of sexual mixing across age groups that results from formation and dissolution of extramarital relationships. The immediate consequences are a sharp reduction in fertility and a concurrent sharp reduction in the transmission (incidence) of HIV. Although this is a drastic and ultimately “unreal” treatment strategy, in keeping with the heuristic nature of this work the results clearly demonstrate what the total overall effect of such a program could be and clearly illuminate the important dynamic and structural characteristics of such a treatment strategy. Realistic implementations could attain at best substantially less impact than that demonstrated here, and it is important to keep in mind that the results of this simulated treatment are exaggerated. Averages of these three simulations are presented as the “HIV with ‘Behavioral’ Treatment Starting in Year 31” results below.
Population with HIV Treated with Pharmacological Antiretroviral Programs
A pharmacologically mediated HIV treatment program was simulated using the three HIV simulations. Starting in year 31 and running for 10 years through year 40, in each of the three HIV populations the untreated
DP indicator was removed and replaced with the lengthened and reduced DP indicator described above in “Effects of HIV” that reflects the impact of antiretroviral drugs on the progression of HIV disease and a treated infected individual’s viral load. This had the effect of substantially reducing the transmission of HIV from mothers to children and between adults and of dramatically reducing the other impacts of HIV, including its fertility-reducing and mortality-elevating effects. This virtual treatment was applied to all HIV-infected individuals and so, like its behavioral corollary, does not reflect a real-world treatment program that would undoubtedly reach only a limited fraction of HIV-infected individuals. That understood, it reveals the maximum effect that such a treatment program could have and a typical time course over which that effect might be observed. Averages of these three simulations are presented as the “HIV with Antiretroviral Treatment Starting in Year 31” results below.
Population with HIV Treated with Both Preventative and Antiretroviral Programs
The last set of three simulations applies both types of treatment using the three HIV simulations starting in year 31. Averages of these three simulations are presented as the “HIV with Both ‘Behavioral’ and Antiretroviral Treatment Starting in Year 31” results below.
FINDINGS
In the course of conducting this work, a number of other questions were investigated to fully understand the results relating to orphans. To keep the page count reasonable, in-depth discussion of these investigations is not possible, and consequently they are summarized briefly. After 40 years of an untreated HIV epidemic, the annual proportionate growth rate of the population is reduced to zero or below; the age structure converges on a younger, two-tiered shape with fewer young children and adults; the age-specific sex ratio attains a high of roughly 1.5 men per woman in the 45-49 age range and a low of 0.5 men per woman at ages older than 70; and the dependency ratio falls substantially. While discussing the results related to orphans, it is useful to keep these general findings in mind.
Number of Orphans
Panel A of Figure 3-1 demonstrates that the percentage of children under the age of 15 who are maternal, paternal, and dual orphans remains constant in the population unaffected by HIV and, importantly, that the percentage of children who are dual orphans is literally negligible in the
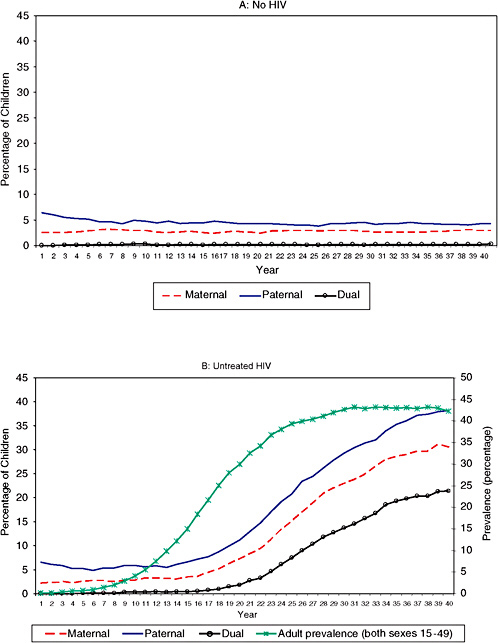
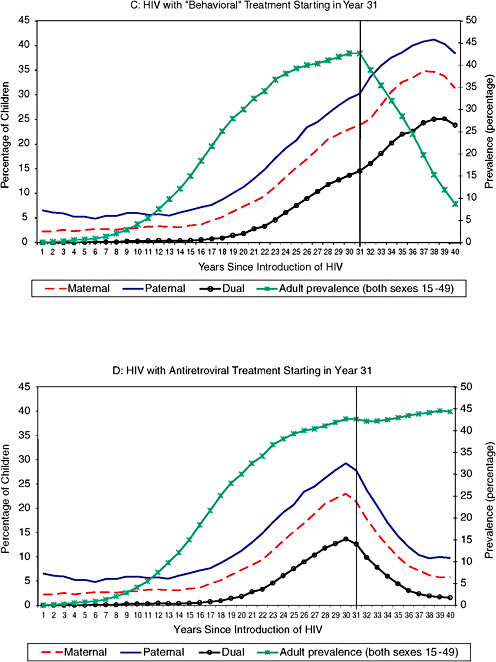
HIV-free population. There are always a few more paternal orphans resulting from the slightly higher adult mortality of men.
Panel B in Figure 3-1 displays the same numbers for the untreated population with HIV. Added to this plot is the trend in the adult (both sexes ages 15 to 49) prevalence of HIV. About 20 years after HIV is introduced, the number of orphans begins to rise significantly. Interestingly the number of orphans begins to increase about 10 to 15 years after the adult prevalence begins its rise, and the number of orphans does not reach significant levels until HIV has been affecting the population for at least 20 years—a significant lag associated with the average time between infection and death of roughly 10 years for adults. Given that most HIV epidemics in sub-Saharan Africa are less than 20 years old, big increases in the numbers of orphans may yet be coming. Looking at panel B of Figure 3-1 reveals the stunning fact that 37 percent of all children under age 15 are maternal orphans by year 40, 30 percent are paternal orphans, and 22 percent are dual orphans. Compare this number to the figure just above 0 percent in panel A of Figure 3-1. The 15-year (or so) lag is very apparent in this plot when comparing the trends in the percentage of children who are orphans and adult prevalence. The dramatic increase in the percentage of children who are orphans is driven both by the falling number of children (denominator) and by the
rising number of those who are orphans (numerator); working together, these two movements create a large fraction of children who are orphaned.
Examining the impacts of the behavioral preventive treatment program in panel C of Figure 3-1 reveals the familiar sharp drop in adult prevalence induced by the treatment, accompanied by a strong reduction in the total number of children ages 0 to 15 but no big drop in the number of orphans until the latest years of the simulation, 38 through 40. This results from the fact that adult HIV-related mortality is unaffected by this treatment, and hence the parents of existing children keep dying as they did until near the end of the 10-year period of the treatment, when the reservoir of HIV-infected adults begins to thin and the number of HIV-related deaths among adults begins to abate. Panel C makes clear that there is a sharp downturn in the percentage of children who are orphans toward the end of the treatment period. Keep in mind that the behavioral treatment implemented here is extreme, in that all extramarital sexual activity is eliminated; this clearly shows the type and direction of the effects of such a treatment but overestimates the magnitudes of both positive and negative consequences.
The antiretroviral treatment program has the opposite effect on orphanhood. Immediately after the treatment begins, the total number of children begins to climb again as the HIV-mediated reduction in fertility is ameliorated, and concurrently the number of orphans begins to decline because the treatment defers HIV-related adult mortality to older adult ages that are attained after the children have lived to age 15, and existing orphans age out of the 0 to 15 age range. These changes translate into a very sharp decline in the percentage of children who are orphans, panel D of Figure 3-1, that softens and flattens out toward the end of the treatment period as the system begins to stabilize.
Combining the two treatment programs produces a result similar to the antiretroviral treatment program, except accompanied by a clear decrease in the total number of children and in adult HIV prevalence (panel E).
Clearly, HIV-induced changes in the numbers and percentage of children who are orphaned are very significant and will produce substantial intergenerational tensions in the population, as well as the necessity to reallocate resources to the caregivers of these orphans. Now we examine this same question from the point of view of those caregivers—in this case, adults age 50 and over.
Numbers of Children and Grandchildren
Figure 3-2 describes the number and percentage of adults age 50 and older who have surviving grandchildren less than 15 years of age but no surviving children. Panel A indicates that in a population unaffected by HIV, the number of adults age 50 and older rises at a constant proportion-
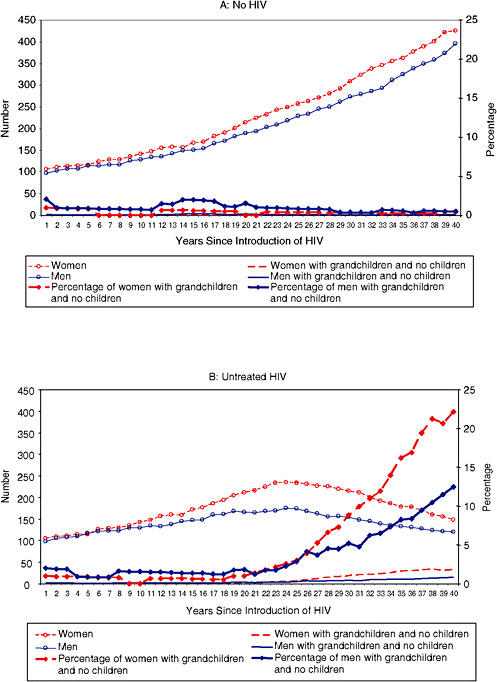
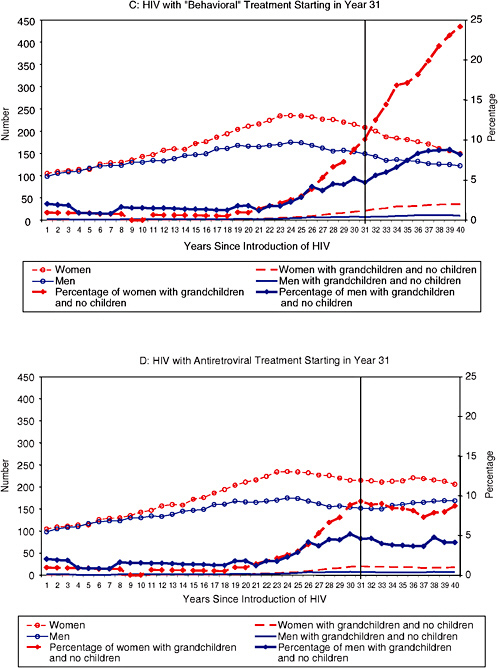
ate rate with slightly fewer men than women—a natural result of the mortality of adult men exceeding that of adult women. The number and percentage of older people of either sex who have surviving grandchildren without surviving children are negligible and constant.
When HIV is introduced to the population in panel B the situation changes; about 20 to 25 years into the epidemic—10 years or so after prevalence begins rising—the number of adults age 50 and older plateaus and immediately starts declining. At the same time, the number and percentage of adults age 50 and older with surviving grandchildren but no surviving children begins to rise. Because the total number of adults age 50 and older is declining while the number with surviving grandchildren but no surviving children is rising, the percentage with surviving grandchildren but no surviving children rises very quickly. Roughly 22 percent of women age 50 and older and roughly 12 percent of men are in this category by year 40. The discrepancy between the female and male percentages probably results from the fact that women can have children only during the years when they are fertile, whereas men can have children over a wider (and older) range of ages. This results in an oldest age at which women as a population reproduce, and as a consequence they cannot replenish their pool of children as they age and therefore more quickly lose all of their children, compared with men, who always have the potential to have another child. In this way, men are able to maintain their pool of children longer than women.
Introducing the behavioral preventive treatment program in panel C of Figure 3-2 has little impact because most of the transmission is happening at much younger ages, which do not impact the total number of adults age 50 and older during the comparatively short period of 10 years over which the treatment is applied. The existing HIV-positive population at the time the treatment started continues to die as it did over the 10 years of the treatment, thereby continuing to create the orphans that contribute to the percentage of adults age 50 and over who have surviving grandchildren but no surviving children.
In contrast, the antiretroviral treatment program has an immediate and very positive impact on this indicator, panel D of Figure 3-2. The number of adults age 50 and older stabilizes because HIV-related adult mortality is deferred, and the number of adults age 50 and older with surviving grandchildren but no surviving children also stabilizes for the same reason. The net result is a stabilization of the percentage of adults age 50 and older with surviving grandchildren but no surviving children at a level of about 9 percent for women and 4 percent for men.
The combined treatment program (panel E) produces a result almost identical to the antiretroviral program—as expected given the fact that the behavioral preventive program had little effect.
HIV-mediated changes in the number and percentage of adults age 50 and older who are in a position to be required to care for young children are very significant and display a strong sex differential. By the time a vigorous HIV epidemic stabilizes, up to one-quarter of women age 50 and older may have surviving orphaned grandchildren for whom they must care, while up to 15 percent of older men may be in the same position. The 40 years simulated here are not sufficient to see these indices stabilize; they are still rising steadily in year 40. Given the 20- to 25-year lag between the time HIV is introduced to the population and the beginning of the rise in this indicator, the future is ominous for those who will be age 50 and older in sub-Saharan Africa over the next 10 to 15 years.
CONCLUSION
Taken as a whole, the findings presented here paint a nuanced picture of the impact of HIV on a population, and in particular of the consequences for older people. Results obtained in the course of this work but not presented here indicate that through subtle changes in the age structure, driven by changes in both fertility and mortality, the dependency ratio is likely to fall and that furthermore the decline is largely driven by changes in the male age structure. Additional big changes are wrought on the age structure, resulting in a stable age structure with a “stepped” shape after the epidemic has stabilized that is likely to be younger than the pre-HIV age structure.
Because of the sex differentials in age-specific incidence and prevalence, women die of HIV-related causes at younger ages than men, leading to severe distortions in the age-specific sex ratio that result in a substantial predominance of women living at older ages in HIV-infected populations. And overall the population growth rate is likely to fall substantially, to the vicinity of 0 percent per annum. The average time from infection to death of roughly 10 years appears in many guises—mainly the typical duration of the lag between the initial rise in prevalence and the appearance of some other effect, such as the creation of excess numbers of orphans.
Perhaps the most salient results with respect to the older segment of an HIV-infected population have to do with the creation of a large number of orphans of all three types—maternal, paternal, and dual. The situation grows even grimmer when viewed from the point of view of the elderly themselves, with the result that nearly 25 percent of women older than age 50 potentially live with surviving grandchildren but no surviving children after 40 years of an HIV epidemic. Taken together with the impact of HIV on the age-specific sex ratio, which after 40 years of an epidemic results in two-thirds of the population age 50 and older being female, the final result is that fully one-fifth of the total population over 50 years of age will potentially be in a position of some obligation to care for grandchildren. Acknowledging that each grandchild has two grandmothers, two grandfathers, a number of aunts and uncles on both sides of the family, and in some cases social services designed to help them, the entire burden will be diluted. Despite this, the fact remains that a substantial fraction of older people, who will be largely women under any circumstances, will be caring for young children.
The impacts of the behavioral preventive and antiretroviral treatment programs are varied and often work in opposite directions. The most important impacts of the prevention program have to do with its effect on fertility, the fact that it can, depending on the scope and success of the intervention, substantially reduce fertility. This feeds back through the age structure to affect other processes in the population and the indicators used to measure the impact of HIV, such as the dependency ratio. The fertility impacts of the preventive programs are felt immediately, whereas the drop in incidence does not work through to have an impact on HIV-related mortality for about 10 years, which produces a lag in the mortality impact; because the treatment programs were simulated for only 10 years, these mortality impacts were largely not yet evident.
In comparison, the antiretroviral programs have little effect on fertility, and what little they do increases rather than decreases fertility. In contrast, they have an immediate impact on mortality by deferring it for an average of 10 years or so in adults. These mortality reduction/deferment impacts were evident immediately and often led to positive changes in the trend of
the epidemic. It is critical to note that these changes are temporary and result only from the immediate deferment of mortality. Again, because the simulated treatment lasted only 10 years, there was not sufficient time to see the rebound of HIV-related mortality as the deferment expired and HIV-related mortality began to reassert itself at a new level slightly lower than what it had been before the treatment began—because of the reduction in incidence brought about by the suppression of viral load and lowered transmission probability.
In general it appears that some mixture of the two types of treatment program is best; the combined approach often leads to a smoother result with less dramatic short-term changes, and often the two complement each other. It is clear that treatment alone does not solve all, or even most, of the problems associated with an HIV epidemic.
An important next step in this investigation is to restart all of the 15 simulations whose results are presented here and simulate another 40 years. This will provide ample time for the perturbations wrought by the treatment programs to stabilize and for the epidemics to reach new equilibria. In general there appear to be two important time scales in the temporal evolution of all of these epidemics. The first has to do with the latency between infection and death—about 10 years for adults. The second has to do with fertility, the latency between a change in fertility and the time when the children who were born at the time of that change reach reproductive ages themselves, or about one generation. This is the period over which the perturbations in fertility reverberate through the age structure. After about one generation, the fluctuations in the age structure are significantly reduced in magnitude, but at least one to two more generations are required for the echoes of a fertility perturbation to completely disappear.
Extending the investigation still further, work needs to be done to incorporate the household and larger extended social structures into the model so that their interactions with HIV-positive adults, the children of those adults, and eventually orphans can be properly studied. In a similar vein, the investigation also needs to widen to take into account the effects of HIV-related adult morbidity and the burden that this places on children and other adults in the social networks that support the HIV-positive adults. Challenging these expansions of the model is the need for reasonably accurate empirical data describing these structures and their dynamics; data that are so far very difficult to find.
The most important impression provided by the findings presented here is that the impacts of HIV on a population are subtle and multifaceted and must be understood together in the context of their joint impact on a whole population. Ignoring one or more of the major impacts results in a distorted view of the other impacts. It is also clear that the time scales over which an epidemic grows and treatments have their impacts are on the order of de-
cades or quarter-centuries, and that many will echo through the age structure for on the order of 50 to 100 years. These long time scales are important in motivating urgency in treatment but also cautioning patience after a program is instituted, because it may take some time for the effects to be strongly felt and even longer for a new equilibrium to be reached.
REFERENCES
Bicego, G., Rutstein, S., and Johnson, K. (2003). Dimensions of the emerging orphan crisis in sub-Saharan Africa. Social Science and Medicine, 56(6), 1235-1247.
Clark, S.J. (2001a). An investigation into the impact of HIV on population dynamics in Africa. (Ph.D. dissertation in demography). Philadelphia: University of Pennsylvania.
Clark, S.J. (2001b). An investigation into the impact of HIV on population dynamics in Africa. Available: http://www.samclark.net/ [accessed Oct. 2, 2006].
Clark, S.J. (2001c). Part 2: The demography of the Gwembe Tonga. In An investigation into the impact of HIV on population dynamics in Africa (pp. 55-195). (Ph.D. dissertation in demography). Philadelphia: University of Pennsylvania.
Clark, S.J. (2001d). Part 3: A two-sex stochastic microsimulation of a population with HIV. In An investigation into the impact of HIV on population dynamics in Africa (pp. 196-355). (Ph.D. dissertation in demography). Philadelphia: University of Pennsylvania.
Clark, S.J. (2004, April). Survival of orphans: Examples from southern Zambia and South Africa. Presentation at the annual meeting of the Population Association of America, Boston, MA.
Dorrington, R., Bourne, D., Bradshaw, D., Laubsher, R., and Timaeus, I.M. (2001). The impact of HIV/AIDS on adult mortality in South Africa. (Report). Cape Town: South African Medical Research Council.
Gregson, S. (1994). Will HIV become a major determinant of fertility in sub-Saharan Africa? Journal of Development Studies, 30(3), 650-679.
Gregson, S., Garnett, G.P., and Anderson, R.M. (1994). Assessing the potential impact of the HIV-1 epidemic on orphanhood and the demographic structure of populations in subSaharan Africa. Population Studies, 48(3), 435-458.
Gregson, S., Zaba, B., and Garnett, G.P. (1999). Low fertility in women with HIV and the impact of the epidemic on orphanhood and early childhood mortality in sub-Saharan Africa. Aids, 13(Suppl. A), S249-257.
Joint United Nations Programme on HIV/AIDS. (2002, July). Report on the global HIV/AIDS pandemic. Geneva, Switzerland: Author.
Joint United Nations Programme on HIV/AIDS, UNICEF, and U.S. Agency for International Development. (2002). Children on the brink 2002: A joint report on orphan estimates and program strategies. Washington, DC: Author.
Monk, N.O. (2002). Enumerating children orphaned by HIV/AIDS: Counting a human cost. Available: http://www.albinasactionfororphans.org/learn/OVCstats.pdf [accessed September 24, 2003].
Preston, S.H., Heuveline, P., and Guillot, M. (2001). Demography: Measuring and modeling population processes. Oxford, England: Blackwell.
Timaeus, I.M. (1998). Impact of the HIV epidemic on mortality in sub-Saharan Africa: Evidence from national surveys and censuses. Aids, 12(Suppl. 1), S15-S27.
Zaba, B. (1998). Evidence of the impact of HIV on fertility in Africa. (International conference). AIDS, 12(abstract no. 24196), 479.

























