
8
Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate1
RESEARCH RECOMMENDATIONS AND OTHER ISSUES
Presenter: Lawrence J. Appel
In this session, Lawrence J. Appel of Johns Hopkins University, who chaired the panel on Dietary Reference Intakes (DRIs) for electrolytes and water, presented a brief overview of the DRIs for sodium, potassium, water, and sulfate; covered research recommendations specific to those nutrients; and addressed some related issues concerning the DRI taxonomy, evidence-based medicine and nutrition policy, and general research. The DRI Electrolytes and Water Report (IOM, 2005) is the most recently published DRI report.
Overview
The DRI Electrolytes and Water Report provides no Estimated Average Requirements (EARs) or Recommended Dietary Allowances (RDAs). Instead, it gives Adequate Intakes (AIs) for water, sodium, and potassium, but no AI value for sulfate. A Tolerable Upper Intake Level (UL) was set for sodium but for none of the other nutrients. This background information is provided to help highlight major knowledge gaps.
Rationales for Adequate Intakes
The rationales for the AIs vary by nutrient and are summarized in Box 8-1.
Water For water, the focus primarily was on dehydration as an end point, and serum or plasma osmolality was the indicator used. Examining data on water intake and osmolality from the Third National Health and Nutrition Examination Survey, no evidence of dehydration was found in the general population, even at the first decile of water intake. Serum osmolality basically was identical across the reported intakes. Thus the median water intake was used to set the AI, which is consistent with the definition of AI.
Sodium For sodium, “nutrient adequacy” refers to the sodium intake level at which one could consume a diet that basically meets all the recommended dietary intakes for other nutrients. Of several hypothesized adverse effects of inadequate sodium intake, only nutrient inadequacy and volume depletion in the setting of acute thermal stress were considered to be sufficiently well documented to use in setting the AI.
Potassium A controlled feeding study (Morris et al., 1999) was one of several pieces of data that contributed to the basis for the AI of 1,500 mg (120 millimoles) of potassium per day. The investigators fed different
|
BOX 8-1 Rationale for Adequate Intake, by Nutrient
NHANES III = Third National Health and Nutrition Examination Survey |
amounts of potassium and then challenged the subjects with salt to see what percentage of individuals experienced a blood pressure increase that was greater than 3 mm Hg. Morris and colleagues reported a steady reduction in salt sensitivity with increasing intakes of potassium. A question that remains is whether it is potassium or some concomitant nutrient (specifically one or more anions) that might be contributing to the protective effect.
Rationale for Tolerable Upper Intake Level for Sodium
In terms of the adverse effects of excess sodium intake, several potential outcomes were considered, but increased blood pressure was the adverse effect used as the basis for setting the UL.
Current Status of Research Recommendations
Because the report was released in 2004, one cannot expect a large amount of progress in filling research gaps. For the nutrients covered in the DRI Electrolytes and Water Report, data were lacking that would be useful in setting EARs or AIs for infants, children, pregnant women, and the elderly—as was the case for most other nutrients. A summary of the current status of research recommendations on sodium and potassium, water, and sulfate follows.
Sodium and Potassium
-
With regard to the development of effective public health strategies to achieve and sustain reduced sodium intake and to increase potassium intakes in the general population, activities are underway at the National Heart, Lung, and Blood Institute of the National Institutes of Health, in the New York City Health Department, and in Great Britain.
-
Progress regarding the recommendation to develop alternative processing technologies to reduce sodium content of foods is uncertain because much of the relevant information is proprietary.
-
An investigator-initiated proposal has been developed for a large-scale trial to test the efficacy of increased potassium intake,
-
alone and in combination with reduced sodium intake, on prevention of stroke; however, funding for such work is difficult to obtain.
-
A few pilot studies are under way to test the main and interactive effects of sodium and potassium intake on bone mineral density and, if possible, bone fractures.
-
Only one trial of potassium intake on kidney stones has been conducted, and that study addresses recurrent stones rather than the risk of kidney stones.
-
A creative method is being used to assess—without a major new effort—the impact of sodium reduction on clinical cardiovascular events. (The research recommendation called for a formal assessment of the feasibility of a large-scale, long-term clinical trial designed for this purpose.) In particular, a publication is in process that has followed long-term (10 to 15 years) participants who were enrolled in two trials of hypertension prevention. Together, these two trials have documented about a 20 percent reduction in the risk of cardiovascular events.
One interesting line of research relates to the recommendation to conduct randomized trials to compare the effects of different potassium salts on blood pressure and other outcomes at different levels of sodium intake. The effects of anions had been specified as of low priority for the panel. Research by He (2005) indicates that potassium citrate and potassium chloride had similar effects on blood pressure. For bone, in contrast, the anion may have considerable effect.
Dr. Appel views the recommendation to conduct trials that assess the effects of high potassium intake on serum potassium levels and blood pressure in the setting of early stages of kidney disease to be very important from a public health perspective. Although potassium is beneficial in the majority of the population (those with normal kidney function), potassium starts to be harmful as soon as some evidence of kidney dysfunction develops. Given that several million people in the United States alone have chronic kidney disease, it appears very important to determine the point at which a change from benefit to harm occurs. The problem is further exacerbated because angiotensin-converting enzyme inhibitors (medications that commonly are used in the setting of renal disease) tend to increase serum potassium concentration. Such research, however, would involve some substantive methodological challenges.
Water
Dr. Appel considers a major research recommendation to be investigating the effect of hydration status and fluid intake on chronic disease such as kidney stones and gallstones, as well as on the occurrence of specific cancers, including colon cancer and bladder cancer. From his perspective, a case can be made for conducting observational studies rather than trials to address this research recommendation.
Dr. Appel took the position that the recommendation to use large-scale surveys to validate estimates of total water intake (from food plus fluids) should be expanded to include the electrolytes and other nutrients. A comparison of potassium intakes that were reported in the Health Professionals Follow-up Study, the Nurses Health Study, and national survey data (IOM, 2005) reveals large differences. In view of this and of large absolute values reported at the upper quintiles of potassium intake, Dr. Appel suggests that the results of food frequency questionnaires be investigated for systematic bias.
Sulfate
No progress was reported related to the two research recommendations for sulfate, both of which call for studies of relationships between sulfate intake and specific disease conditions.
DRI Taxonomy and Process
The following comments relate to improving the DRI process.
Consideration of Chronic Disease
Dr. Appel concurred with Dr. Lupton that the process of applying the DRI model to chronic diseases needs further consideration. A related concern involves the definition of a healthy population, especially given the high probability of subsequently developing chronic disease. It could be that only 10 percent of people are healthy from the standpoint that they will never develop a problem with hypertension. In Dr. Appel’s
view, however, the public health problem is that 90 percent of people develop hypertension, and nutritional factors are related to its incidence.
Approaches to Setting Recommendations
Evidence-based medicine The most highly valued types of studies in evidence-based medicine—namely nutrition intervention trials with several doses and well-defined clinical outcomes—are rare for any nutrient. There are major impediments to conducting such studies.
Surrogate outcomes It often was necessary for DRI panels to use surrogate outcomes for setting nutrient recommendations. However, the criteria and process for selecting surrogate outcomes are ill defined and, in some cases, may have led to results that merit reconsideration.
Adequate Intake As illustrated for water, sodium, and potassium, different approaches were used to set the AI for each nutrient. It may be helpful to catalog the approaches used for setting the AI for different nutrients and consider revision to the definition.
Tolerable Upper Intake Level There is a need to consider ways to apply the DRI model for nutrients for which there is a direct progressive relationship between intake and the occurrence and/or severity of the adverse effect but for which there is no threshold. As illustrated by Figures 8-1 and 8-2, a threshold is not evident for either saturated fat or sodium intake.
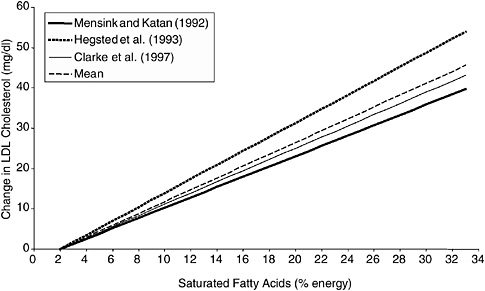
FIGURE 8-1 Calculated changes in serum low density lipoprotein cholesterol (LDL-C) concentration in response to percent change in dietary fatty acids.
SOURCE: IOM (2005).
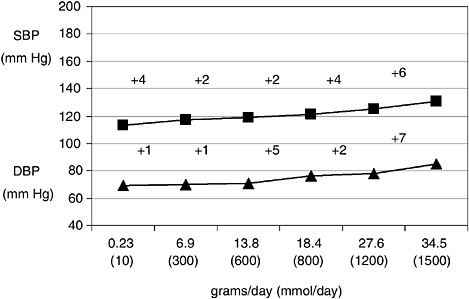
FIGURE 8-2 Increases in blood pressure observed in sodium dose– response trials.
NOTE: SBP = systolic blood pressure; DBP = diastolic blood pressure.
SOURCE: IOM (2005), with data from Luft et al. (1979).
Adjusting Nutrient Recommendations
Criteria are needed for determining whether adjustments need to be made in nutrient recommendations and for the kind of adjustment to make if one is needed. For example, should the specific type of DRI be based on calorie intake, weight, age, and/or sex? A major determinant of sodium intake is the number of calories consumed. A 4,000 kcal diet is likely to provide about twice as much sodium as a 2,000 kcal diet, but, as set, the AI does not take this into consideration.
Prioritizing Recommendations
A deliberate process is needed for writing and refining the research recommendations and then identifying the ones that are most likely to advance the field.
DISCUSSION
Tolerable Upper Intake Level for Potassium
In response to a request for a reason why a UL was not set for potassium, Dr. Appel clarified that no evidence of toxicity could be found for healthy people despite extensive searches, and that it would have been beyond the panel’s charge to set a UL for the large number of people with chronic renal disease.
Ongoing Research
Dr. Dwyer asked whether the Chronic Renal Insufficiency Cohort (CRIC) Study might be a source of answers to some of the research questions raised. Dr. Appel noted that CRIC is an observational study, but that the need really is for some experimental evidence.








