
2
Trends in Maternal and Gestational Weight
Mary Cogswell and Patricia Dietz described several important trends that have occurred in the weight distribution of different populations of women in their childbearing years. Figure 2-1 and Figure 2-2 summarize obesity and overweight prevalence trends among women of childbearing age (ages 20–39) and adolescents (ages 12–19) from 1960 to 2004, respectively. While several major sources provide data that help describe these trends, a national surveillance system for assessing maternal weight (prior to, during, and after pregnancy) does not exist. Available data sets have well-known shortcomings, but together they provide a general picture of the current situation with respect to maternal and gestational weight.
Among U.S. women ages 20 to 39 years who are not pregnant, the prevalence of obesity has increased from about 9 percent in 1970 to about 28 percent in 2000 (Flegal et al., 2002; Ogden et al., 2006). The obesity rate varies, however, among different ethnic populations: 24 percent for non-Hispanic white women, 36 percent for Mexican American women, and 50 percent for non-Hispanic black women (Ogden et al., 2006). Figure 2-3 summarizes these obesity prevalence rates in women of childbearing ages (ages 20–39). Adolescent girls (ages 12–19) have a prevalence of overweight (defined as greater than or equal to the 95th percentile of body mass index, BMI, based on gender and age) that statistically increased from 5 percent in 1970 to 15 percent in 2000. This rate increased slightly to 16 percent in 2004 (Flegal et al., 2002; Ogden et al., 2002, 2006). This prevalence was 15 percent for non-Hispanic white girls, 14 percent for Mexican
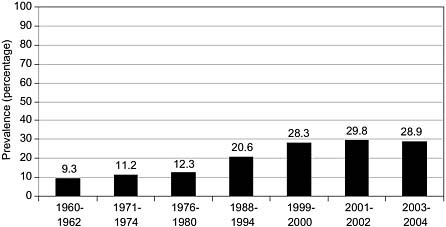
FIGURE 2-1 Prevalence (%) of obesity among nonpregnant U.S. women, ages 20– 39. Obesity is defined as a body mass index of greater than 30.0.
SOURCE: Flegal et al. (2002) and Ogden et al. (2006).
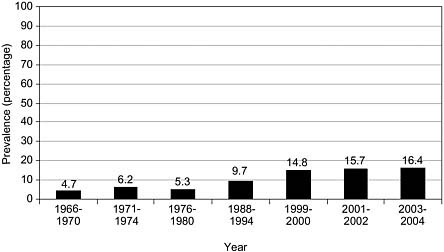
FIGURE 2-2 Prevalence (%) of overweight among nonpregnant U.S. adolescents, ages 12–19. Overweight is defined as greater than or equal to the 95th percentile of body mass index based on gender and age.
SOURCE: Ogden et al. (2002, 2006).
American girls, and 25 percent for non-Hispanic black girls (Ogden et al., 2006). Figure 2-4 summarizes these prevalence rates for overweight in adolescent women (ages 12–19). No nationally representative data exist for other minority populations, such as non-Mexican Hispanic, American Indian, Alaskan Native, and Asian women.
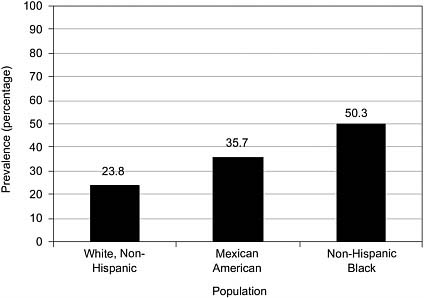
FIGURE 2-3 Prevalence (%) of obesity among U.S. nonpregnant women, ages 20– 39, by race/ethnicity, 2003–2004. Obesity is defined as a body mass index of greater than 30.0.
SOURCE: Ogden et al. (2006).
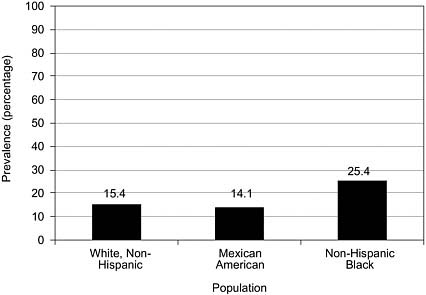
FIGURE 2-4 Prevalence (%) of overweight among U.S. nonpregnant women, ages 12–19, by race/ethnicity, 2003–2004. Overweight is defined as greater than or equal to the 95th percentile of body mass index based on gender and age.
SOURCE: Ogden et al. (2006).
PREPREGNANCY WEIGHT
Cogswell and Dietz observed that two sets of criteria exist for categorizing pregnancy weight status: the criteria of the 1990 Institute of Medicine (IOM) report and the 1998 criteria of the National Heart, Lung, and Blood Institute (NHLBI) (see Table 2-1). Studies that examined the association between prepregnancy BMI and maternal morbidity and mortality frequently classify prepregnant weight status by the IOM or NHLBI criteria.
These variations in the classification criteria have several ramifications, which can be seen in studies that draw on data from the Pregnancy and Nutrition Surveillance System (PNSS), a national database based on information about low-income women from 25 states and 6 tribal agencies. Estimates of the prevalence of underweight according to the IOM criteria using these data are more than twice the prevalence rates based on the NHLBI criteria. The prevalence of overweight is 40 percent lower and the prevalence of obesity is just slightly higher using IOM criteria. The prevalence of prepregnancy underweight using IOM criteria has declined from 22 percent in 1983 to about 12 percent in 2004, whereas the prevalence of overweight has increased from 24 percent in 1983 to 43 percent in 2004 (Centers for Disease Control and Prevention, 2006; see Figure 2-5).
GESTATIONAL WEIGHT GAIN
The recommendations of the 1990 IOM report specify weight gain ranges during pregnancy for singleton term births based on prepregnancy BMI (Table 2-2). National birth certificate data include maternal weight. However, data allow for a comparison between very low gestational weight gain groups (less than 15 lbs.) and very high gestational weight gain groups
TABLE 2-1 Criteria for Classifications of Prepregnancy Weight Status
|
|
IOM (1990) Body Mass Index |
NHLBI (1998) Body Mass Index |
|
Underweight |
<19.8 |
<18.5 |
|
Normal |
19.8–26.0 |
18.5–24.9 |
|
Overweight |
>26.0–29.0 |
25.0–29.9 |
|
Obese |
>29.0 |
30.0+ |
|
SOURCE: Institute of Medicine (1990); National Heart, Lung, and Blood Institute (1998). |
||
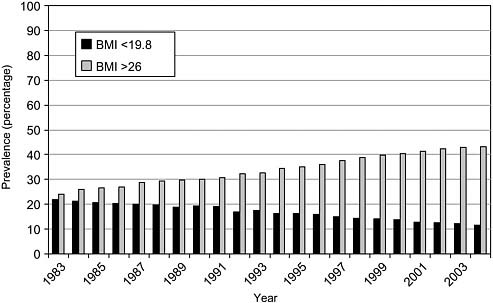
FIGURE 2-5 Prevalence of prepregnancy underweight (BMI <19.8) and overweight (BMI >26), Pregnancy and Nutrition Surveillance System. BMI refers to body mass index.
SOURCE: Centers for Disease Control and Prevention (2006).
TABLE 2-2 Summary of IOM Recommended Total Weight Gain Ranges for Pregnant Women,a by Prepregnancy Body Mass Index (BMI)b
|
Weight-for-Height Category |
Recommended Total Gain |
|
|
kg |
lb |
|
|
Low (BMI <19.8) |
12.5–18 |
28–40 |
|
Normal (BMI of 19.8 to 26. 0) |
11.5–16 |
25–35 |
|
Highc (BMI >26.0 to 29.0) |
7–11.5 |
15–25 |
|
aYoung adolescents and black women should strive for gains at the upper end of the recommended range. Short women (<157 cm, or 62 in) should strive for gains at the lower end of the range. bBMI is calculated using metric units. cThe recommended target weight gain for obese women (BMI >29.0) is at least 6.8 kg (15 lbs). SOURCE: Institute of Medicine (1990). |
||
(greater than 40 lbs.). Data are not available to support analyses of national birth certificate data in relation to the 1990 IOM recommendations based on prepregnancy BMI; such analyses can examine only total gestational weight gain at this time.
On the basis of these data, between 1990 and 2003, the percentage of women who gained less than 15 lbs. during pregnancy increased slightly from about 4 to 6 percent, and the percentage of women who gained more than 40 lbs. also increased, from 20 to about 25 percent (see Figure 2-6).
Weight Gain Across BMI Categories
Cogswell and Dietz described several data sets that make it possible to examine gestational weight gain across BMI categories (albeit not in nationally representative populations), including the National Vital Statistics System: Birth Data (NVSS), the Pregnancy Risk Assessment Monitoring System (PRAMS), the Pregnancy Nutrition Surveillance System (PNSS), and the California Maternal and Infant Health Assessment (CA-MIHA) (Table 2-3). These data sets support analyses of the distribution of gestational weight among different age groups as well as selected racial and ethnic populations (see Table 2-4).
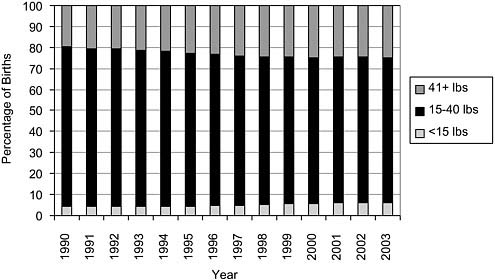
FIGURE 2-6 U.S. trends in weight gain during pregnancy, singleton, term, primiparous births, 1990–2003.
SOURCE: 1990–2000: Rhodes et al. (2003), reproduced with permission from Pediatrics, 111:1181–1185; 2001–2003: National Vital Statistics System, birth data, unpublished analysis.
TABLE 2-3 U.S. Data Sources for Gestational Weight Distribution
|
Sources |
Description |
|
National Vital Statistics System: Birth Data |
Contains data on all births in the United States as reported on state birth certificates |
|
Pregnancy Risk Assessment Monitoring System |
State-specific population-based surveys of mother’s attitudes and experiences before, during, and after pregnancy
|
|
Pregnancy Nutrition Surveillance Systems |
Program-based public health surveillance system among low-income pregnant women who participated in federally funded public health programs
|
|
California Maternal and Infant Health Assessment |
Ongoing population-based survey of mothers delivering live infants in California from February through May of each year
|
|
SOURCE: Cogswell, Dietz, and Branum (2006). |
|
Cogswell and Dietz presented preliminary analyses of these data sets. Their analyses indicate that similar gestational weight gain patterns can be found across the different data sets, with several exceptions. The PNSS data set (which includes more minority populations) shows higher estimates (of about 5 percent) for women who gained less than 15 lbs. during their pregnancies. PNSS also shows a higher percentage of women who have gained more than 40 lbs. during their pregnancies than other data sources.
These data sets also contain data for BMI. In the PRAMS data from 1993 to 2003, the gestational weight gains of a little over one-third of women were consistent with the 1990 IOM recommendations, with no real change evident over time. In the CA-MIHA data from 1999 to 2004, about 40 percent of women met the IOM recommendations for weight gain during pregnancy, with little change over time. And in the PNSS data from 1992 to 2004, the weight gains during pregnancy of about one-third of women were within the IOM guidelines. In addition, the PNSS data suggest
TABLE 2-4 Distributions of Age and Race/Ethnicity by Data Source, Current Year
a general increase in the percentage of women gaining weight during pregnancy above the IOM recommendations, from about 37 percent in 1993 to about 46 percent in 2004, and a decrease in the percentage of women gaining weight during pregnancy below the IOM guidelines, from about 30 to 23 percent also in 1993–2004.
Age, Race/Ethnicity, and Stature
The 1990 IOM report provided specific gestational weight gain recommendations for particular subgroups, including adolescents, members of racial and ethnic groups, women of short stature, and women carrying twins. Data collected since 1990 allow for an examination of the degree to which these recommendations are consistent with gestational weight patterns among different age groups and racial and ethnic populations. Analyses of the PNSS data reveal gestational weight gain distributions for younger adolescents that are similar to the distribution of women of other ages. Similar analyses of the PRAMS data show that similar proportions of black and white women gain at the upper half of the IOM recommendations, about 20 percent, a finding consistent with the PNSS data, although at a lower percentage (about 12 to 13 percent).
The 1990 IOM report recommended that women of short stature (less than 62 inches tall) should strive for gestational weight gains in the lower end of the recommended gestational weight gain for their BMI. Analyses of the PNSS data, however, indicate that such women were no more likely to
be in the lower half of the IOM recommendations than taller women, a finding consistent with analyses of the PRAMS data.
In summary, analyses of the national data sets suggest that approximately one-third of pregnant women gain within the IOM gestational weight gain guidelines and that weight gain pregnancy patterns have been fairly stable over time, except in the PNSS, which contains more low-income women. There is no evidence that the IOM recommendations for specific populations of women have been followed.
POSTPARTUM WEIGHT RETENTION
As the speakers’ overview of the distribution of maternal weight indicated, national data on postpartum BMI or weight retention after pregnancy are limited. Analyses of data from the 1988 National Child and Infant Health Survey suggest that, on average at 12 months postpartum, about 40 percent of women in the sample retained 14 lbs. above their prepregnancy weight status. Obese women (BMI >29) were excluded from these analyses since the IOM gestational weight gain recommendations do not set an upper weight gain limit, and gestational weight gain was categorized using the IOM classification criteria. In this study, black women retained more weight postpartum than white women in all BMI categories. In addition, black women who had higher rates of weight gain during pregnancy were also likely to retain more weight postpartum. This pattern was similar to white women who gained in excess of the IOM recommendations (Figure 2-7). A discussion panelist, Anna Marie Siega-Riz, indicated that her unpublished study of a shorter period (3 months postpartum) found that the average amount of weight retained postpartum was about 9 lbs. with 45 percent of white women and 57 percent of black women retaining more than 10 lbs.
National data on postpartum weight retention collected since the 1990 IOM recommendations have not been analyzed. There are, however, some national and state data sources that may provide useful information about postpartum weight retention status since the IOM recommendations. For example, the 1988 National Maternal and Infant Health Survey data indicate that gestational weight gain is associated with excess postpartum weight retention (Keppel and Taffel, 1993), and preliminary analyses of the Early Childhood Longitudinal Study Birth Cohort suggest that little association exists between gestational weight gain and postpartum obesity except for women who weighed 130 to 149 lbs. before pregnancy. Other data sources include the Infant Feeding Practices Survey-2 (for which data are not yet available) and limited data from the PNSS (Table 2-5).
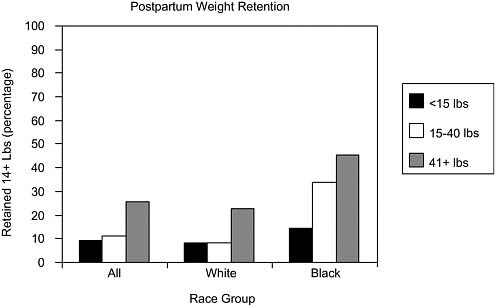
FIGURE 2-7 Retained weight after delivery (14+ lbs), by gestational weight gain in reference to IOM recommendations, United States, 1988 (excludes women with BMI >29).
SOURCE: Adapted with permission from Keppel and Taffel (1993).
TABLE 2-5 U.S. Data Sources to Determine Postpartum Weight Distribution
|
Sources |
Description |
|
Early Childhood Longitudinal Study Birth Cohort |
A nationally representative longitudinal study of U.S. children born in 2001 that looks at children’s health, development, care, and education from birth through first grade |
|
Infant Feeding Practices Survey-2 |
A national mail panel survey on infant feeding practices that enrolled pregnant women in 2005 |
|
Pregnancy Nutrition Surveillance System |
Program-based public health surveillance system that monitors risk factors associated with infant mortality and poor birth outcomes among low-income pregnant women who participate in federally funded public health programs, 1983+ (1988+ for pregnancy weight gain) |
|
SOURCE: Cogswell, Dietz, and Branum (2006). |
|
SUMMARY
The workshop presentations indicated that almost 30 percent of women of childbearing age (20–39 years) are obese, and the prevalence of obesity is even higher among Mexican American and non-Hispanic black women. Over 15 percent of adolescent girls (ages 12–19) are overweight, with higher prevalence rates among non-Hispanic black adolescents. No national surveillance system exists to adequately monitor maternal weight prior to, during, and after pregnancy. The limited data that are available from 1983 through 2004, prepregnancy underweight declined, while the prevalence of prepregnancy overweight increased. The numbers of women gaining less than 15 and more than 40 lbs. during pregnancy (between 1990 and 2003) have slightly increased between 1990 and 2003. Postpartum weight retention data are limited, although data from 1998 indicate that black women retained more weight than white women in all BMI categories.
During the presentations and discussion sessions, several challenges were addressed for the prevention of obesity among adolescent girls and women of childbearing age and for the promotion of healthy weight gain during pregnancy. They include the striking absence of evidence of increased adherence to the IOM gestational weight gain recommendations during the course of a pregnancy among general or selected populations of women and the variations in prevalence estimates that persist from the use of different classification criteria (IOM or NHLBI). As noted by the participants, there continues to be uncertainty as to which criteria are best for categorizing prepregnant overweight and obesity. Finally, there is uncertainty concerning the application of the adult criteria (prepregnancy BMI and gestational weight gain recommendations), which are based on an assumption of relatively static adult weight (exclusive of pregnancy), to categorize adolescents in studies of weight-related pregnancy outcomes.
REFERENCES
Centers for Disease Control and Prevention 2006 Pediatric and Pregnancy Nutrition Surveillance System. Pregnancy Data Tables. Available: http://www.cdc.gov/pednss/pnss_tables/tables_numeric.htm. [accessed August 3, 2006].
Cogswell, M.E., Dietz, P.M., and Branum, A.M. 2006 Maternal Weight, Before, During, and After Pregnancy in the United States. Presentation at the Workshop on the Impact of Pregnancy Weight on Maternal and Child Health, May 30, Washington, DC.
Flegal, K.M., Carroll, M.D., Ogden, C.L., and Johnson, C.L. 2002 Prevalence and trends in obesity among U.S. adults, 1999–2000. Journal of the American Medical Association 288(14):1723–1727.
Institute of Medicine 1990 Nutrition During Pregnancy. Washington, DC: National Academy Press.
Keppel, K.G., and Taffel, S.M. 1993 Pregnancy-related weight gain and retention: Implications of the 1990 Institute of Medicine guidelines. American Journal of Public Health 83(8):1100–1103.
Ogden, C.L., Carroll, M.D., Curtin, L.R., McDowell, M.A., Tabak, C.J., and Flegal, K.M. 2006 Prevalence of overweight and obesity in the United States, 1999–2004. Journal of the American Medical Association 295(13):1549–1555.
Ogden, C.L., Flegal, K.M., Carroll, M.D., and Johnson, C.L. 2002 Prevalence and trends in overweight among U.S. children and adolescents, 1999– 2000. Journal of the American Medical Association 288(14):1728–1732.
National Heart, Lung, and Blood Institute 1998 Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. (National Institutes of Health Publication 98-4083). Washington, DC: National Institutes of Health.
Rhodes, J.C., Schoendorf, K.C., and Parker, J.D. 2003 Contributions of excess weight gain during pregnancy and macrosomia to the cesarean delivery rate, 1990–2000. Pediatrics 111(5 Part 2):1181–1185.












