
10
Health and Exposure Data Infrastructure to Improve the Scientific Basis of Presumptions
INTRODUCTION
This chapter addresses the implementation of a system of data collection to support surveillance and research, as well as to track the exposures of individual military personnel. The long-term goal is a system that would improve or complete many of the evidence gaps that now lead to presumptions. Information on exposure is needed to conduct studies that will provide data for calculating attributable fractions and for determining exposure groups of particular individuals.
Once a causal relationship has been established or presumed between a specific disease and a type of exposure, it becomes crucial to establish whether the Service member was exposed during military service. When data are not sufficient to describe a specific Service member’s service-exposure history, presumptions are needed to give guidance about what to assume as exposure magnitude is considered. One clear path toward reducing the need for presumptions in decision making is to accurately document and provide Service member-specific exposure and health data to those making decisions regarding that Service member’s case. Thus individuals determined by an adequate exposure surveillance system not to be exposed to an agent of concern would not be at risk for the particular health outcome(s) caused by that specific exposure. The availability of exposure data would provide evidence to support a veteran’s claim that the exposure occurred while in military service. The availability of exposure data will allow more informative epidemiological studies to be performed and a more accurate determination of service-attributable fraction (SAF).
The need for having better exposure data has been recognized repeatedly in numerous external reviews of Department of Defense (DoD) and Department of Veterans Affairs (VA) activities regarding Service member health protection and veteran health care and disability determination (GAO, 1999, 2000a,b, 2005a,b, 2006; IOM, 1996a, 1999b, 2000c).
Detailed health status data collected throughout a Service member’s active duty and veteran experience, coupled with individual exposure data collected during that period, would provide the data needed to make better decisions about an individual’s likelihood of service-related disease causation and thus minimize the need for presumptions. As the Institute of Medicine (IOM) noted in 1996,
The DoD, the branches of the armed services, and the DVA should continue to work together to develop, fund, and staff medical information systems that include a single, uniform, continuous, and retrievable electronic medical record for each [S]ervice member. The uniform record should include each relevant health item (including baseline personal risk factors, every inpatient and outpatient medical contact, and all health-related interventions), allow linkage to exposure and other data sets, and have the capability to incorporate relevant medical data from beyond DoD and DVA institutions (e.g., U.S. Public Health Service facilities, civilian medical providers, and other health-care institutions)…. (IOM, 1996a, p. 10)
DoD and VA have been working together since 1998 to improve sharing of medical information for active-duty military personnel and veterans. The agencies have developed a short-term plan to improve their existing health information systems and a long-term plan to create a modern health information system based on computable data. However, as GAO points out, DoD and VA lack a detailed project management plan to guide their efforts (GAO, 2007).
In 1997, President Clinton issued a directive to DoD and VA “to create a new Force Health Protection Program. Every soldier, sailor, airman, and Marine will have a comprehensive, life-long medical record of all illnesses and injuries they suffer, the care and inoculations they receive, and their exposure to different hazards. These records will help us prevent illness and identify and cure those that occur” (DoD, 2006a, p. 2).
Also in 1997, coincident with the presidential directive described above, DoD issued an instruction describing the “Implementation and Application of Joint Medical Surveillance for Deployments.” This document defined initial expectations for more detailed medical surveillance and exposure assessment data collection systems for both deployment and in-garrison or nondeployment settings. This plan laid the groundwork for systems that would “eventually be capable of linking deployment and nondeployment
environmental and occupational exposure and data to health hazard and/or health risk assessments to individual medical records and medical outcome databases” (DoD, 1997, p. 5).
The vision for a more comprehensive and continuous surveillance system was articulated in DoD Directive 6490.2 issued in 2004. It proposed that
Health surveillance systems shall be continuously in effect throughout each [Service member]’s career, capturing data about individual health status; instances of disease and injury; medical interventions such as immunizations, treatments, and preventive medications; and exposures to potential and actual health hazards associated with occupation, deployment, and lifestyle. (DoD, 2004, p. 3)
It also dictated policy that “[s]urveillance data collected on individual [Service member]s during their careers shall be provided to VA upon their separation or retirement from the military” (DoD, 2004, p. 4).
Defining and developing the mechanisms and systems to implement these goals has been an iterative process that has taken years—largely due to the magnitude and complexity of the issues being addressed. Those efforts are now bringing action as a series of systems and expectations are being implemented. DoD Instruction 6490.03 of 2006, which replaced the 1997 DoD Instruction 6490.3, sets clear expectations that deployment exposure assessment and monitoring data be submitted to individual health records and to a DoD-wide database (DOEHRS—the Defense Occupational and Environmental Health Readiness System) (DoD, 2006c, p. 21).
The remainder of this chapter reviews the current state and future plans for DoD and VA collection and use of health and exposure data throughout a Service member’s span of service. The availability of such data would enable studies to better understand potential linkages between service-connected exposures and future health status and would reduce reliance on presumptions in decision making.
DOD HEALTH AND EXPOSURE ASSESSMENT DATA COLLECTION
DoD Health Assessment and Medical Surveillance
Overview
Opportunities for health assessments of Service members on active duty occur at obvious service milestones throughout the Service member’s span of service. These milestones include the initial medical evaluation at accession, or entry into the service, and subsequent periodic health assessments
that continue until separation or retirement from the service. These milestones are displayed in Figure 10-1. Additional surveillance may precede or follow specific deployments with assessments tailored to the particular hazards of a deployment.
Routine Health Assessments Throughout the Span of Service
Elements of the health data collected for each of the assessments performed over the span of a Service member’s service are found in Table 10-1. They may include responses to a health history questionnaire, physical examination findings, and laboratory test results. The degree of detail and areas of emphasis in each assessment vary based on the specific point in the span of service or on the purpose of each individual assessment. Generally, a self-completed questionnaire contains a core set of questions regarding physical and mental health, and history of environmental and occupational exposures and stressors. This is intended to follow the recommendations of the U.S. Preventive Health Services Task Force’s Guide to Clinical Preventive Services (AHRQ, 2006). Data are collected in a combination of written and electronic formats.
All new recruits and enlisted Service members undergo an initial evaluation at the time of accession. This is the most comprehensive of the assessments and provides the baseline set of data that is updated at the time of each future assessment. As in all assessments, the nature of the responses and test results partly determine what additional evaluation or screening is performed. At this time, data from this evaluation are generally saved only in a hard copy format. The Health Assessment Review Tool (HART) is an electronic and standardized implementation of the self-reporting questionnaire that is currently being pilot tested at Ft. Jackson (Army) and San Diego (United States Marine Corps); the HART-A (the accession version) is expected to be more generally available in the next few months (Personal communication, Col. K. Cox and C. Postlewaite, Department of Defense, November 1, 2006).
The periodic health assessments (PHAs) are episodic (generally annual) follow-up evaluations primarily employing self-completed questionnaires. Positive responses on this questionnaire, or additions to previously collected information, trigger a more detailed assessment. In following the U.S. Preventive Health Services Task Force recommendations, the PHAs are ideally targeted based on gender, age, disease risk factors, medical history, and exposure history (DoD, 2006d). The PHA is currently being instituted by the Army, but it has been established in the Navy and Air Force for several years.
The separation, retirement, or deactivation assessment is the final routine evaluation that all Service members undergo. Whereas previously a
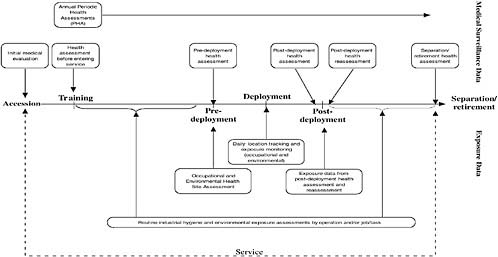
TABLE 10-1 Timeline for Medical Surveillance and Exposure Data Collection
|
|
Accession |
After Training Before Service |
In Service |
Post-Deployment Reassessment |
Separation/Retirement |
|||
|
Throughout Service |
Pre-Deployment |
Deployment |
Post-Deployment |
|||||
|
Routine Medical Surveillance Dataa |
||||||||
|
Self-Administered Questionnaire |
|
|
|
|
|
|
|
|
|
Family history of chronic diseases |
X |
|
X |
|
|
|
|
|
|
Personal habits |
X |
|
|
|
|
|
|
|
|
Past medical history |
X |
|
|
|
|
|
|
|
|
Medications |
X |
|
|
X |
|
X |
|
X |
|
Allergies |
X |
|
|
|
|
|
|
|
|
General health status |
|
|
X |
X |
|
X |
X |
|
|
Significant events since last periodic health assessment |
|
|
|
X |
|
|
|
X |
|
On a profile, light duty, or undergoing a medical board |
|
|
|
X |
|
|
|
|
|
Medical or dental problems |
|
|
|
X |
|
|
|
X |
|
Pregnancy |
|
|
|
X |
|
|
|
|
|
Counseling or care for mental health in past year |
|
|
|
X |
|
|
|
|
|
Questions or concerns about health |
|
|
|
X |
|
|
|
|
|
Health changes during deployment |
|
|
|
|
|
X |
X |
|
|
In sick call during deployment |
|
|
|
|
|
X |
X |
|
|
Nights spent as a patient in a hospital during deployment |
X |
X |
X |
|
Vaccinations |
X |
|
|
|
Symptoms now or developed anytime during this deploymentb |
X |
X |
|
|
See anyone wounded, killed, or dead during this deployment |
X |
|
|
|
Engaged in direct combat where discharged weapon |
X |
|
|
|
During deployment, feel like in great danger of being killed |
X |
|
|
|
Interested in receiving help for a stress, emotional, alcohol, or family problem |
X |
X |
X |
|
Little interest or pleasure in doing things |
X |
X |
|
|
Feeling down, depressed, or hopeless |
X |
X |
|
|
Thoughts that you would be better off dead or hurting yourself in some way |
X |
|
|
|
Nightmares due to an experience so frightening, horrible, or upsetting |
X |
X |
|
|
Constantly on guard, watchful, or easily startled |
X |
X |
|
|
Numb or detached from others, activities, or your surroundings |
X |
X |
|
|
|
Accession |
After Training Before Service |
In Service |
Post-Deployment Reassessment |
Separation/Retirement |
|||
|
Throughout Service |
Pre-Deployment |
Deployment |
Post-Deployment |
|||||
|
Concerns of serious conflicts with spouse, family members, or close friends |
|
|
|
|
|
X |
X |
|
|
Concerns of hurting or lose control with someone |
|
|
|
|
|
X |
|
|
|
Having problems if wounded, injured, or assaulted during deployment |
|
|
|
|
|
|
X |
|
|
Alcohol use |
|
|
|
|
|
|
X |
|
|
Difficulty working, taking care of things at home, or getting along with other people |
|
|
|
|
|
|
X |
X |
|
Illnesses or injuries that caused you to miss duty for longer than 3 days |
|
|
|
|
|
|
|
X |
|
Treated by a healthcare provider, admitted to a hospital, or had surgery |
|
|
|
|
|
|
|
X |
|
Injuries or illnesses while on active duty for which you did not seek medical care |
|
|
|
|
|
|
|
X |
|
Other questions or concerns about your health |
|
|
|
|
|
|
|
X |
|
Intend to seek Department of Veterans Affairs disability |
|
|
|
|
|
X |
|
Laboratory Tests |
|
|
|
|
|
|
|
Urinalysis (albumin, sugar, HCG) |
X |
X |
X |
|
|
|
|
H/H |
X |
X |
X |
|
|
|
|
Blood type |
X |
X |
X |
|
|
|
|
Drugs and alcohol |
X |
X |
X |
|
|
|
|
Serum sample |
X |
|
X |
X |
X |
|
|
HIV testing |
X |
|
X |
|
|
|
|
CBC |
X |
|
|
|
|
|
|
Hemoglobin |
X |
|
|
|
|
|
|
Hematocrit |
X |
|
|
|
|
|
|
Vaccination status |
X |
|
|
|
|
|
|
Clinical Screening and Measurements |
|
|
|
|
|
|
|
Height |
X |
X |
X |
|
|
|
|
Weight |
X |
X |
X |
|
|
|
|
Temperature |
X |
X |
X |
|
|
|
|
Pulse |
X |
X |
X |
|
|
|
|
Blood pressure |
X |
X |
X |
|
|
|
|
Distant vision, near vision |
X |
X |
X |
|
|
|
|
Refraction by autorefraction or manifest |
X |
X |
X |
|
|
|
|
Heterophoria |
X |
X |
X |
|
|
|
|
Color vision |
X |
X |
X |
|
|
|
|
Depth perception, field of vision, night vision |
X |
X |
X |
|
|
|
|
|
Accession |
After Training Before Service |
In Service |
Post-Deployment Reassessment |
Separation/Retirement |
|||
|
Throughout Service |
Pre-Deployment |
Deployment |
Post-Deployment |
|||||
|
Intraocular tension |
X |
X |
X |
|
|
|
|
|
|
Audiometer |
X |
X |
X |
|
|
|
|
|
|
Pap smear |
X |
X |
X |
|
|
|
|
|
|
Allergies |
|
|
X |
|
|
|
|
|
|
Tobacco use |
|
|
X |
|
|
|
|
|
|
Alcohol abuse and stress management |
|
|
X |
|
|
|
|
|
|
Chronic illnesses |
|
|
X |
|
|
|
|
|
|
Medications |
|
|
X |
|
|
|
|
|
|
Cholesterol |
|
|
X |
|
|
|
|
|
|
Breast exam, mammogram |
|
|
X |
|
|
|
|
|
|
Fecal occult blood |
|
|
X |
|
|
|
|
|
|
Sigmoid |
|
|
X |
|
|
|
|
|
|
Colonscopy |
|
|
X |
|
|
|
|
|
|
Immunizations |
|
|
X |
|
|
|
|
|
|
Clinical Evaluations |
|
|
|
|
|
|
|
|
|
Head, face, neck, and scalp |
X |
X |
X |
|
|
|
|
|
|
Nose, sinuses |
X |
X |
X |
|
|
|
|
|
|
Mouth and throat |
X |
X |
X |
|
|
|
|
|
|
Heart |
X |
X |
X |
|
|
|
|
|
|
Lungs and chest, vascular system |
X |
X |
X |
|
Anus and rectum |
X |
X |
X |
|
Abdomen and viscera |
X |
X |
X |
|
External genitalia |
X |
X |
X |
|
Upper and lower extremities |
X |
X |
X |
|
Spine, musculoskeletal system |
X |
X |
X |
|
Body marks, scars, tattoos |
X |
X |
X |
|
Skin |
X |
X |
X |
|
Neurologic and psychiatric disorders |
X |
X |
X |
|
Pelvis |
X |
X |
X |
|
Endocrine system |
X |
X |
X |
|
Routine Exposure Dataa |
|||
|
Industrial Hygiene Exposure Assessment of Operations, Jobs/Tasks |
|
|
X |
|
Qualitative Exposure Judgments |
|
|
X |
|
Occupational Exposure Monitoring |
|
|
X |
|
Routine Environmental Health Programs |
|
|
X |
|
|
Accession |
After Training Before Service |
In Service |
Post-Deployment Reassessment |
Separation/Retirement |
|||
|
Throughout Service |
Pre-Deployment |
Deployment |
Post-Deployment |
|||||
|
Environmental Health Site Assessment (EHSA)c |
|
|
|
|
|
|
|
|
|
Current use of site, adjoining properties, and surrounding area |
|
|
|
X |
|
|
|
|
|
Past use of site, adjoining properties, and surrounding area |
|
|
|
X |
|
|
|
|
|
Geologic, hydrogeologic, hydrologic, meteorologic, and topographic conditions |
|
|
|
X |
|
|
|
|
|
General description of structures |
|
|
|
X |
|
|
|
|
|
Roads |
|
|
|
X |
|
|
|
|
|
Potable water supply |
|
|
|
X |
|
|
|
|
|
Sewage disposal system |
|
|
|
X |
|
|
|
|
|
Hazardous materials in connection with identified use |
|
|
|
X |
|
|
|
|
|
Storage tanks |
|
|
|
X |
|
|
|
|
|
Odors |
|
|
|
X |
|
|
|
|
|
Pools of liquid |
|
|
|
X |
|
|
|
|
|
Drums |
|
|
|
X |
|
|
|
|
|
Hazardous materials and petroleum products containers |
X |
|
|
|
|
Unidentified substance containers |
X |
|
|
|
|
Heating and cooling |
X |
|
|
|
|
Stains or corrosion |
X |
|
|
|
|
Drains and sumps |
X |
|
|
|
|
Pits, ponds, and lagoons |
X |
|
|
|
|
Stained soil or pavement |
X |
|
|
|
|
Stressed vegetation |
X |
|
|
|
|
Solid waste |
X |
|
|
|
|
Waste water |
X |
|
|
|
|
Well |
X |
|
|
|
|
Septic systems |
X |
|
|
|
|
Daily Location Tracking |
|
X |
|
|
|
OEHS Site Assessments |
|
X |
|
|
|
Environmental Monitoring |
|
X |
|
|
|
Exposure Incident Response |
|
X |
|
|
|
Self-Administered Questionnaire |
|
|
|
|
|
DEET insect repellant applied to skin |
|
|
X |
X |
|
Pesticide-treated uniforms |
|
|
X |
X |
|
|
Accession |
After Training Before Service |
In Service |
Post-Deployment Reassessment |
Separation/Retirement |
|||
|
|
Throughout Service |
Pre-Deployment |
Deployment |
Post-Deployment |
||||
|
Environmental pesticides (like area fogging) |
|
|
|
|
|
X |
X |
|
|
Flea or tick collars |
|
|
|
|
|
X |
X |
|
|
Pesticide strips |
|
|
|
|
|
X |
X |
|
|
Smoke from oil fire or burning trash or feces |
|
|
|
|
|
X |
X |
|
|
Vehicle or truck exhaust fumes |
|
|
|
|
|
X |
X |
|
|
Tent heater smoke |
|
|
|
|
|
X |
X |
|
|
JP8 or other fuels |
|
|
|
|
|
X |
X |
|
|
Fog oils (smoke screen) |
|
|
|
|
|
X |
X |
|
|
Solvents |
|
|
|
|
|
X |
X |
|
|
Paints |
|
|
|
|
|
X |
X |
|
|
Ionizing radiation |
|
|
|
|
|
X |
X |
|
|
Radar/microwaves |
|
|
|
|
|
X |
X |
|
|
Lasers |
|
|
|
|
|
X |
X |
|
|
Loud noises |
|
|
|
|
|
X |
X |
|
|
Excessive vibration |
|
|
|
|
|
X |
X |
|
|
Industrial pollution |
|
|
|
|
|
X |
X |
|
|
Sand/dust |
|
|
|
|
|
X |
X |
|
|
Depleted uranium |
|
|
|
|
|
X |
X |
|
|
Days wear MOPPS over garments |
|
|
|
|
|
X |
|
|
retirement evaluation of a career Service member was optional, this has become mandatory since 2005 (Personal communication, Col. K. Cox and C. Postlewaite, Department of Defense, November 1, 2006). The final assessment is performed to document any history of a “limiting” condition. This is determined by a medical evaluation board and may describe the need for “alternative duty” in subsequent employment because of a disability suffered while in the service. The determination of this board addresses the service connectedness of a condition that a Service member may have and thus that Service member’s eligibility for VA services.
Nonroutine Health Assessments
Event-driven assessments Health evaluations are also performed in the event of acute health problems or worsening of preexisting conditions. These are focused evaluations that address the specific concern at hand.
Deployment-specific health assessments The predeployment assessment occurs within 60 days of deployment and builds on the PHA. This brief evaluation focuses on interval changes since the most recent PHA, highlighting medications used and any limited duty or short-term disability given. A serum sample is archived and any theater-specific or occupation-specific testing is performed. An HIV test is required if none has been done in the previous 12 months. For deployments lasting less than 30 days, the predeployment assessment is optional as determined by the deployment health authority. Combatant command determines whether additional specific tests will be required, such as cholinesterase levels if deployed into pest management activities or zones, or G6PD enzyme levels. Although not all Service members undergo this assessment, at least 90 percent do (Personal communication, Col. K. Cox and C. Postlewaite, Department of Defense, November 1, 2006).
During deployment there are no generic health assessments. Evaluations are triggered by specific exposures or events, and there may be theater-specific assessments. Also, follow-up may be indicated when environmental sampling suggests a hazard, such as poor water quality. Patient-encounter data are often in electronic format and are captured by the Armed Forces Health Longitudinal Technology Application (AHLTA); sites that are currently not using an electronic data record are planned to have their data entered in the future. Depending on the circumstance, exposures to documented excursions of ambient air, water, or soil concentrations, are also theoretically entered into individual records. Under a new requirement, environmental summaries for all permanent and semi-permanent base camps will be generated according to time and location (Personal
communication, Col. K. Cox and C. Postlewaite, Department of Defense, November 1, 2006).
Postdeployment evaluations must occur within 30 days of reployment, although most take place before actually leaving the deployment arena, or while in transit from theater. This evaluation uses a self-reported questionnaire, but also includes a personal interview with a care provider who determines the need for further follow-up. A serum sample is typically obtained when a Service member is at “home.” There is documentation of environmental and occupational exposures. Rosters of specific exposure- or event-defined cohorts are assembled based on professional judgment; these are used for purposes of health follow-up or risk communication. Examples include lung function testing following sulfur dioxide exposures or follow-up of those exposed to depleted uranium (Personal communication, Col. K. Cox and C. Postlewaite, Department of Defense, November 1, 2006). Though the impact of combat related stressors on mental health may be significant, structured assessments on symptoms related to emotional stressors, depression, anxiety, posttraumatic stress disorder, and interpersonal difficulties, including hurting someone or losing control, are brief and only assessed at postdeployment period.
HEALTH DATABASES
The above-described assessments generate data that are stored in several databases or formats, thus requiring record linkage, and data entry, for analysis. One primary database is the Defense Medical Surveillance System (DMSS). The DMSS is a relational database that currently contains up-to-date Service member data for all in- and out-patient in-garrison health encounters including acute health events and exposures. It currently has some in-theater encounters provided by AHLTA, but not all. As noted above, HART-A is only now being implemented, so much of the accession evaluation is only present in hard copy form. Also, while standardization is the goal, data collection is not completely standardized across the service branches. AHLTA is the new DoD automated medical records system and clinical data repository; this includes all laboratory data and electronic PHAs. Integration of medical records is clearly a goal in DoD. This is manifested in the current process of establishing an Armed Forces Health Surveillance Center to integrate DMSS, AHLTA, and personnel data (from the Defense Manpower Data Center). Although much of the surveillance health data present in the DMSS are relevant to AHLTA (for example, reportable medical conditions), there is no need for complete overlap (Personal communication, Col. K. Cox and C. Postlewaite, Department of Defense, November 1, 2006).
Troop Tracking and Linking of Individual Exposure and Health Data
Improvements in tracking of troop location are underway, reflecting in part an awareness of the need to perform troop tracking to allow reconstruction of exposure scenarios. A new tracking software, the Defense Theater Accountability Software, which is in limited use, currently requires data entry by hand at the unit level. The Defense Manpower Data Center can currently query records in the DMSS. There is no capability to resolve location within a 24-hour period, as only one 24-hour entry is currently used (Personal communication, Col. K. Cox and C. Postlewaite, Department of Defense, November 1, 2006).
The need to link exposure data with health outcomes is appreciated, but this capability is currently not fully developed. The current situation is driving efforts to construct environmental monitoring summaries for various theaters and locales, and to assign surveillance exposure data to individual health records.
DOD EXPOSURE ASSESSMENT
Overview
Occupational and environmental exposures occur throughout the span of a Service member’s service career. In summarizing the exposure assessments needed to cover that experience, we can use the same milestones as were used to describe health assessments. They begin with exposure opportunities in the first months of service immediately following service entry and also proceed in a longitudinal manner through routine garrison experiences through multiple deployments and on through separation or retirement (see Figure 10-1).
Exposure Assessments Throughout the Span of Service
Exposure assessment elements collected for each milestone of the Service member’s span of service are summarized in Table 10-1 and may include qualitative exposure judgments, occupational exposure monitoring, and environmental monitoring results. As in the case of health assessments, the degree of detail and areas of emphasis vary based on the specific point in the span of service or a specialized reason for the assessment. Data are collected in a combination of written and electronic formats, but there is significant activity moving DoD toward fully integrated electronic records.
Exposure assessments are made so that appropriate exposure controls can be planned and implemented. In the case of routine operations or low-risk combat scenarios the implementation of these controls is straight-
forward. Under high-risk combat scenarios, however, it may be difficult or impossible to consistently implement controls for environmental agents as the risks posed by implementing those controls under severe combat conditions may be higher than those posed by the exposures. In each case, however, there is a need to characterize and document exposures to agents from occupational and environmental sources.
Nondeployment Military Bases
The individual services within DoD have had traditional industrial hygiene and environmental health programs in place for many years in military base or installation settings. These programs conduct occupational and environmental exposure risk assessments for routine and nonroutine operations and document results in a variety of service-specific paper and electronic data repositories.
Predeployment
In support of deployment occupational environmental health and safety (OEHS) measures for information/intelligence preparation of the environment, a phase I deployment OEHS assessment is produced for military location(s) of interest that assesses known and/or potential deployment OEH hazards and threats ranging from industrial chemicals, historical contamination, radiation, infectious disease, entomological risks, weapons of mass destruction, and specified intelligence based threats. These assessments are quantitative and also identify any preventive medicine measures and counter-measures and deployment OEH surveillance activities to ensure force health protection measures for deployments. For deployments less than 30 days, some of these activities are performed at the discretion of the operational commander as it is recognized that for special operations and very short deployments they may not all be feasible (DoD, 2006c).
Deployment
OEHS site assessments, exposure assessments, environmental monitoring, exposure incident response (and reports), and daily individual troop locations as determined by global positioning system (GPS) or other means are performed during deployment (see Figure 10-2) (DoD, 2006c). The content and detail included in these assessments vary depending on the length of deployment, the location of deployment, the intensity of combat operations, the number of deployed personnel, and the training of deployed personnel (DoDI 6490.03 2006 [DoD, 2006c]).
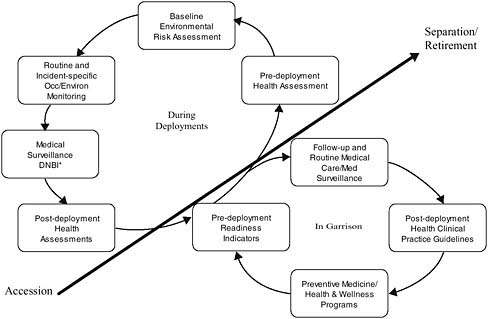
FIGURE 10-2 DoD’s deployment health surveillance elements.
*DNBI (disease and nonbattle injury).
SOURCE: Adapted from Postlewaite, 2006.
Postdeployment
Postdeployment assessment activities primarily involve data and report cleanup and submission for central documentation—including documentation of health and exposure data and incidents in individual health records.
EXPOSURE DATABASES
Service Specific
The Army and Navy maintain collected exposure data at their respective occupational health and preventive medicine headquarters, the U.S. Army Center for Health Promotion and Preventive Medicine and the Navy Environmental Health Center respectively. The Air Force retains its data at each individual Air Force base (Table 10-2). Although the Army and Navy have a central headquarters database maintenance system, they also have individual activity databases for exposure data. These individual activity databases are rolled into the headquarters system but are also maintained at
TABLE 10-2 Service-Specific Databases for Exposure
|
Service |
Database |
Data Maintenance |
Health Hazard Inventory Database |
Quantitative Exposure Data |
Deployment Exposure Data |
In-Garrison Data |
|
Army |
HHIM |
CHPPM |
HHIM |
Yes |
No |
Yes |
|
Army |
DESS |
USACHPPM |
DESS |
Yes |
Yes |
No |
|
Navy |
IHIMS |
NEHC |
NOED |
Yes |
Yes |
Yes |
|
Air Force |
CCS |
AF Bases |
AF-EMIS/HMMS |
Yes |
No* |
Yes |
|
NOTE: Table conveys the service-specific databases available and where the data are stored. ABBREVIATIONS: AF-EMIS = Air Force Environmental Management Information System; CCS = Command Core System; CHPPM = U.S. Army Center for Health Promotion and Preventive Medicine; DESS = Deployment Environmental Surveillance System; HHIM = Health Hazard Information Module; HMMS = Hazardous Material Management System; IHIMS = Industrial Hygiene Information Management System; NEHC = Navy Environmental Health Center; NOED = Navy Occupational Exposure Database. *Some deployment exposure data are currently stored in the Air Force’s Global Expeditionary Medical System (GEMS). SOURCE: Adapted from DoD, 2006a. |
||||||
the respective individual activities. All data will eventually be consolidated into the DOEHRS program, but individual activity data are also retained at the respective individual sites. Services have indicated that they will retain some of their legacy systems after inclusion of data into DOEHRS. Industrial hygiene exposure data consolidation into DOEHRS is expected to be completed by 2010 with all exposure data entry completed by 2013.
DOEHRS—DEFENSE OCCUPATIONAL AND ENVIRONMENTAL HEALTH READINESS SYSTEM
Overview
DOEHRS is an automated information system designed to replace existing service-specific database collection and storage systems. It supports reduction in redundant data entry between worksites and occupational health clinics. DOEHRS also eliminates redundant exposure data collection through interfaces with clinical, environmental, safety, and personnel automated information systems. The DOEHRS structure is outlined in Figure 10-3.
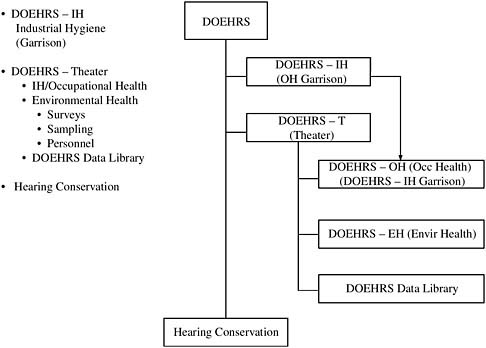
FIGURE 10-3 National Defense Occupational and Environmental Health Readiness System (DOEHRS).
SOURCE: Adapted from Heller, 2006.
According to the DOEHRS student guide,
The Industrial Hygiene module of DOEHRS, DOEHRS [sic] is a key enabling technology within the presidentially mandated FHP and is further supported by Public Law 105-85. DOEHRS is a comprehensive, automated information system for assembling, comparing, using, evaluating, and storing occupational personnel exposure information, workplace environmental monitoring data, personal protective equipment usage data, observation of work practices data, and employee health hazard educational data. DOEHRS provides information needed by occupational health staff and command surgeons for reporting options to commanders regarding the reduction of health threats. (DoD, 2006b, ch. 1, p. 2)
DOEHRS supports the prevention of illness and injury in DoD military members and civilian employees from exposure to chemical, biological, or physical hazards. Exposures can occur throughout the continuum of military operations, such as industrial maintenance facilities, administrative offices, hospitals, aboard ship, while operating weapon systems in training
exercises, and while deployed in war fighting or other military operations. DOEHRS prevents illness by identifying potential health hazards; providing and documenting exposures and provides recommendations to commanders, supervisors, and personnel to minimize adverse health effects; and monitoring effectiveness of procedures followed. Interface with other DOEHRS occupational health programs provides medical surveillance for early identification of exposure, treatment, rehabilitation, and follow-up to ensure that no repeated illnesses occur. (DoD, 2006b, ch. 1, p. 3)
DOEHRS maintains longitudinal exposure records for individual workers in DoD. Longitudinal exposure records contain a history of predeployment, deployment, and postdeployment exposure. These records provide a baseline to facilitate postdeployment follow-up. (DoD, 2006b, ch. 1, p. 2) DOEHRS is scheduled to interface with each service’s hazardous material tracking system and laboratory information management systems.
DOEHRS is the occupational medicine answer for DoD’s medical records system (AHLTA)…. DOEHRS will be deployed on a Defense Information Systems Agency (DISA) platform in the DISA Defense Enterprise Computing Center Detachment in San Antonio, Texas to support the Army, Navy, Coast Guard, and other agencies. (DoD, 2006b, ch. 1, p. 3)
Initial implementation of this system includes the DOEHRS industrial hygiene module, which supports the DoD industrial hygiene exposure assessment model based on the American Industrial Hygiene Association’s “Strategy for Assessing and Managing Occupational Exposures,” a state-of-the-art approach developed through consensus of government, industry, and academic industrial hygienists (DoD, 2006b). The approach is applicable to assessing and managing occupational and environmental exposures associated with routine and nonroutine operations that may be encountered in-garrison and during deployment. Core to the approach is the appropriate grouping of individuals into similar exposure groups and the characterization, assessment, and control of exposures common to individuals in those groups (DoD, 2006b).
DOEHRS Implementation and Continuous Improvement
DODI 6490.3 (DoD, 1997, p. 9) set the original intent to integrate exposure records with medical records. DODI 6490.03 (DoD, 2006c, p. 28) directed that exposure data records will be integrated into individual medical records and commits DoD to accomplish the integration. DoD personnel acknowledge that this integration will be a continuous improvement effort as functionalities of DOEHRS are developed (Personal communication, C. Postlewaite et al., Department of Defense, November 21, 2006).
The current version of DOEHRS, version 1.0.5.0, includes the first iterations of the industrial hygiene and theater-focused environmental health sample management capabilities. Many additional requirements were addressed in the DoD planning and programming budget for fiscal year (FY) 2013 (POM 2008-2013).
Because DOEHRS is a platform information system for all services, DODI 6490.03 specified how integration would occur and provided standardized definitions and exclusions for compliance. Recording exposures occurring during deployment is a crucial part of the database with deployment defined here as “[t]he relocation of forces and materiel to desired operational areas. Deployment encompasses all activities from origin or home station through destination, specifically including intracontinental United States, intertheater, and intratheater movement legs, staging, and holding areas” (DoD, 2006c, p. 2). This definition allows for home station (in-garrison) delineation of exposure data distinct from deployment data. The use of the term deployment for the Navy has different connotations and consequently this instruction addresses that issue: “[s]hipboard operations that are not anticipated to involve operations ashore are exempt from the requirements of this instruction except for recording individual daily deployment locations or when potential health threats indicate actions necessary beyond the scope of shipboard occupational health programs or per the decision of the commander exercising operational control” (DoD, 2006c, p. 2).
DOEHRS Current Functionality
DOEHRS is being implemented step-by-step, phasing in each of its functional elements. The hearing conservation portion of DOEHRS has been functional since 1997, as directed by the DoD Instruction 6490.3. (DoD, 1997). Some industrial hygiene exposure data have been collected and entered into the system through the DoD Industrial Hygiene Exposure Assessment Model released in January 2000 (DoD Industrial Hygiene Working Group, 2000). The Navy and Air Force plan to fully implement the industrial hygiene (in-garrison) function by the end of FY 2008. This implementation includes the downloading of currently stored exposure data as applicable. The use of the DOEHRS industrial hygiene functionality for currently collected exposure data will be deployed to all Army installations by March 2007. While deployment data are currently being collected and archived, the deployment exposure data function has not been fully developed or implemented. The Army serves as the DoD lead for deployment occupational and environmental health surveillance data archives (DODI 6490.03, 2006; CJCS Memorandum MCM-0006-02, 2002, under revision). This deployment data with DOEHRS is expected to be fully completed and online in FY 2010 (POM 2008-2013).
As set out in the DoD POM 2008-2013 for DOEHRS, all anticipated requirements and functionalities for the project have been addressed. Funding support is anticipated on a fiscal year basis with new functionalities being developed and implemented on the same fiscal year basis. If fully funded as anticipated, all DOEHRS functionalities will be completed and online by the end of FY 2013. As presented by DoD representatives (Postlewaite, 2006; Personal communication, C. Postlewaite et al., Department of Defense, and reiterated during the teleconference on November 21, 2006), DOEHRS has full funding support by DoD, and DoD is fully committed to DOEHRS full implementation and triservice functioning by the end of FY 2013.
DOEHRS Effectiveness
As proposed and defined, DOEHRS will be a highly effective system for coordinating collected exposure data from both home station (in-garrison) and deployment locales. Combining the Service member’s medical records with the consolidated environmental monitoring and personal exposure data in DOEHRS is key to enabling VA to provide necessary health care to these future veterans. A major problem encountered in the current VA health-care provision system is a lack of exposure data. The DOEHRS program has the potential to alleviate this lack of data. However, the data must be provided to VA to be of any use. Currently, there is no avenue to transfer these data from DoD to VA. This avenue of data transference must be developed and supported by both DoD and VA for DOEHRS to fully benefit the veteran. An agency-to-agency coordinating board between DoD and VA would be a starting point. VA is at a distinct disadvantage if it must consistently request the data from DoD.
One barrier to implementation of this system of shared exposure data is the concern that sharing some of these data may compromise the secrecy of troop locations or other combat-specific or national security issues. Although DoD classification for security purposes must be considered, there remains a need to work through this challenge for the benefit of the veteran. Although secrecy is a necessary requirement for the protection of Service members during conflict, a rapid declassification of the collected exposure data is also necessary to provide health care to Service members when needed. Furthermore, if exposure studies are conducted involving secrecy classification, VA must make their health-care providers aware of the possible adverse health effects so that presenting veterans can be properly treated.
DOEHRS, as envisioned, is a project that can greatly benefit DoD and VA when used effectively and competently by both agencies. Full funding to complete development and implementation of DOEHRS is necessary to
provide and deliver to VA the exposure data needed for the provision of health care for our nation’s veterans.
USE OF HEALTH AND EXPOSURE DATA BY VA
Veteran Care and Disability Support
Overview
The Veterans Health Administration (VHA) is the largest of the three operational administrations of VA and comprises more than 200,000 employees who provide medical, surgical, and rehabilitative care via a system of over 150 hospitals and 1,000 outpatient clinics nationwide. Close to 8 million veterans were enrolled in the VA hospital system in 2005; of those, more than 5.3 million sought and received care (VA, 2006a, pp. 2, 3, 6).
The vast majority of care provided by VHA is through its network of outpatient clinics, which registered more than 57 million visits in 2005. Close to 600,000 inpatients were also treated in hospitals (VA, 2006a, p. 2).
Eligibility
Eligibility for VHA care has been codified into an elaborate hierarchy of eight levels with the first level being the highest priority for care. In this level are veterans with service-connected disabilities rated 50 percent or more or veterans determined by VA to be unemployable due to service-connected conditions (VA, 2007a, p. 2). Lower priority levels of eligibility for VHA care are a function of degree of service-connected disability and income. Importantly, by FY 2005, it was estimated that close to 80 percent of all disabled and low-income veterans had enrolled with VHA for care, and 65 percent sought care and were treated (VA, 2006a, pp. 2-3).
It is also important to note that while incurring a disability during military service is one pathway to eligibility for VA care, the care provided is not limited to that required for the qualifying disability, but rather, that needed for the total care the veteran requires. Following entry into the VA health-care system, a veteran may request an appointment with a primary care physician who can conduct a comprehensive assessment of the veteran’s health-care needs.. For veterans in the first level of eligibility, the wait time for this initial appointment is supposed to be less than 30 days (VA, 2007d).
Military Service and Special Eligibility for VA Health Care
On the application form for health benefits required for entry into the VA health-care system, veterans record their service branch, dates of service, and type of discharge. Veterans are also queried about history of injury (Purple Heart awarded), presence of a service-connected disability, percentage of impairment, and a host of questions on specialized exposure opportunities including Agent Orange, radiation, and presence of illness from Gulf War service or spinal cord injury (VA, 2005b).
Seamless Transition
There has been an increased effort on the part of VA to publicize to Service members who are preparing for discharge their eligibility for VA benefits and health care (VA, 2007b). This is true for both those who have not incurred a service-related disability and those who have. A network of field-based VA employees has been sent to the larger military transfer facilities to act as onsite liaisons and offer counseling on benefit eligibility to Service members. Currently, under the seamless transition effort, VA has employees staffed at Landstuhl, Germany, and major military transfer facilities, such as Walter Reed and Eisenhower medical centers. These VA employees assist with disability claims and Service members’ transfer to enrollment in the VA system. The VA Secretary also notifies every new veteran by mail of his or her potential eligibility. There is also an attempt, again in the field, when large groups of Service members are separating, to have onsite VA counselors on hand to help with the transition. However, the “seamless transition” appears to be more about communicating eligibility for care and benefits than about the transfer of medical and exposure records. With the exception of Service members who are being discharged from a military transfer facility to a local VA facility with significant residuals of traumatic injuries, the likelihood that a Service member’s medical record, much less an exposure record (if one existed), seamlessly passes from DoD to the VA health-care system is remote at best.
Seamless Transfer of DoD Data to VA
The medical records system of the DoD (AHLTA) does not interface easily with VA’s (VISTA) systems. Some transfer to VA of both physical and electronic records takes place, but this is generally on a case-by-case basis.
The reports from medical evaluation boards dealing with a Service member’s health conditions that render him or her unfit for regular duty or requiring restricted duty (e.g., asthma, insulin-dependent diabetes) are
currently relatively crude, impairing their usefulness for decision making regarding service connectedness for VA care. This directly affects the ability of VA to determine care and benefit eligibility assessments and disability evaluations. A postdeployment electronic form—the Health Assessment Form—is under development and uses the Federal Health Information Exchange to transfer information in one direction, between DoD and VA. The plan is to use the Federal Health Information Exchange (FHIE) to allow two-way data transfer (Do, 2006), though currently it provides only for unidirectional flow of information from DoD to VA. The plan is for the FHIE to evolve into the Clinical Health Data Repository (CHDR).
EPIDEMIOLOGIC STUDIES OF VETERANS
Introduction
Epidemiologic studies on the adverse health effects of military service in veterans have covered exposures that have occurred in essentially every war in which U.S. Service members have been deployed, beginning with World War I. Although the largest group of these studies has been carried out in some fashion through VA, some have been supported through the National Institutes of Health (NIH), the Centers for Disease Control and Prevention (CDC), and other funding organizations. In this section, we review the breadth of these studies with a view to understanding the sources of data and the sources of funding. In this way, it is hoped that insights can be gained that might recommend preferred, or even alternative, approaches to carrying out epidemiologic studies on the health of veterans to inform the compensation and disability decision-making process. It is not the primary purpose of this chapter to review these studies with a view to assessing the validity of their findings.
VA has carried out and been involved in many epidemiologic studies addressing the health of veterans. Here we provide an overview of studies that specifically deal with veterans’ health in relation to actual or suspected exposures that occurred while they were serving in the U.S. military.
Department of Veterans Affairs Epidemiologic Studies
Veterans Health Administration (VHA) Studies
The VHA funds research studies through its Office of Research and Development. A broad range of health-related studies is supported, including clinical, basic science, and epidemiologic studies. Epidemiologic studies include those on the effects of wartime exposures on veterans’ health, including studies on recently returning Service members. For example, in
2005 the Office of Research and Development announced an invitation for research proposals on combat casualty neurotrauma (VA, 2005a), and in 2006 it announced an invitation for research proposals on health studies of veterans returning from Afghanistan and Iraq (VA, 2006b). Other research surveillance activities sponsored by VA include the establishment of several registries. In 2003, the Office of Research and Development created a national registry of veterans with amyotrophic lateral sclerosis to track the health status of veterans with the disease and help recruit research participants (VA, 2003). Strategic planning for VHA-funded research is carried out by the Field Research Advisory Committee.
Two centers for the study of war-related illnesses were established in VA medical centers in 2001, one in Washington, D.C., and one in East Orange, New Jersey. Initially known as the Centers for the Study of War-Related Illnesses, these were subsequently renamed the War-Related Illness and Injury Study Centers (WRIISC). Both have clinical and research responsibilities (VA, 2006c).
The largest and undoubtedly the most substantial body of research on health effects of returned veterans has been carried out by Dr. Han K. Kang and his colleagues at the Environmental Epidemiology Service at the VHA in Washington, D.C., which is now part of the Washington, D.C., WRIISC. Dr. Kang has carried out studies of veterans in the following broad areas: mustard gas exposure, prisoners of war, radiation exposure, Vietnam veterans, Gulf War veterans, and women veterans. A bibliography of Dr. Kang’s epidemiologic studies is included in Appendix K-1, organized by these subject areas.
Twin Registry Studies
In 1958, the Medical Follow-Up Agency, with funding by NIH and VA, began a project to identify white male twin pairs who had been in military service during World War II (The National Academy of Sciences [NAS]/ National Research Council [NRC] Twin Registry of WWII Military Veteran Twins [SOURCE: http://www.iom.edu/CMS/3795/4907.aspx]). Using state birth records, searches were made by hand against VA files to determine veteran status. Eventually, nearly 16,000 twin pairs were identified. Baseline data were abstracted from VA and military records and a baseline questionnaire was mailed to the twin pairs. Anthropometric and fingerprint data were used to determine zygosity (IOM, 2004b).
A bibliography of research studies based on this NAS/NRC twin registry can be found at http://www.iom.edu/CMS/3795/4907/17038.aspx. A total of 308 published research studies and 7 research reports are based on this registry.
The Vietnam Era Twin (VET) Registry The VET registry was created by VA in the mid-1980s in response to concerns regarding the health effects specifically of exposure to Agent Orange (Goldberg et al., 2002). The registry was built using DoD computerized records and consists of 7,369 male-male twin pairs born between 1939 and 1957, who served from 1965 to 1975 (VA, 2007e). It is now housed in the Seattle Epidemiological Research and Information Center, a joint venture of the Department of Epidemiology at the University of Washington’s School of Public Health and Community Medicine and VA (VA, 2007c). Approximately half of the twins are monozygotic, and half are dizygotic (Henderson et al., 1990). Table 10-3 details the research studies that have been completed using the VET registry, or are currently underway.
National Academies’ Monographs on Veterans’ Health by Theater or Exposure
The National Academies has produced a large number of monographs on veterans’ health dealing with exposures during military service dating back to WWI (Table 10-4). These provide useful summaries, assessments, and updates of scientific findings based on studies completed before the publication of each monograph. It is evident that the more recent the exposure, the larger the number of monographs devoted to it.
Non-VA Epidemiologic Studies of Veterans’ Health
The Millennium Cohort Study
The Millennium Cohort Study is the largest prospective study of military personnel ever conducted. Sponsored by DoD, and recommended by the IOM Committee on Measuring the Health of Gulf War Veterans (IOM, 1999a, p. 6), the study was initiated in 2001 to evaluate the long-term health effects of military service, particularly operational deployment. More than 110,000 people are enrolled currently, and a total of 140,000 are expected to be enrolled by the end of study recruitment in 2007. Study participants will complete a paper or Web-based questionnaire assessing demographics, medical conditions and symptoms, and health-related behaviors once every 3 years until 2022. Survey data will be linked with data from other military databases on deployment, occupation, vaccinations, health-care utilization, and disability. It is hoped that the cohort data will serve as a foundation upon which additional epidemiologic studies of military personnel might develop, in addition to revealing trends in veterans’ health over time (Gray et al., 2002; The Millennium Cohort Study, 2007).
TABLE 10-3 Summary of VET Registry Projects
|
Study Name |
Method of Recruitment |
Recruitment Period |
Number of Participants |
Twin Pairs |
|
Registry construction |
|
|
|
|
|
Military Records |
Record abstracts |
1983-1986 |
14,750 |
7,375 |
|
Studies of the full registry |
|
|
|
|
|
Survey of Health |
Mail/telephone follow-up |
1987 |
10,979 |
4,774 |
|
NHLBI VET Study of Cardiovascular Disease |
Mail/telephone follow-up |
1990 |
8,169 |
3,698 |
|
Harvard Twin Study of Drug Abuse and Dependence |
Telephone |
1991-1993 |
10,979 |
3,698 |
|
Male Health Survey |
|
1999 |
5,349 |
1,615 |
|
Studies of selected twins |
|
|
|
|
|
Impulsivity and aggression |
Mail/telephone follow-up |
1992 |
796 |
314 |
|
Consequences of drug abuse |
In-person |
1995-1996 |
254 |
127 |
|
Alcohol and health services use |
Telephone |
1995 |
2,936 |
|
|
Biologic markers for posttraumatic stress disorder (PTSD) |
In-person |
1995-1998 |
322 |
161 |
|
Telephone |
1995-1996 |
2,003 |
322 |
|
|
Alcohol vulnerability |
In-person |
1997-1999 |
760 |
380 |
|
PTSD Sleep study |
In-person |
Ongoing |
11/22 |
9 |
|
Telephone |
|
207/248 |
248 |
|
|
Twin-family study of health behaviors |
Telephone and mail |
Ongoing |
533 |
214 |
|
PTSD MRI study 1 |
In-person |
Ongoing |
48 |
45 |
|
PTSD MRI study 2 |
In-person |
Ongoing |
52 |
|
|
New studies of selected twins pathological gambling |
||||
|
Spirituality and PTSD |
|
Newly funded 2006 |
510 |
255 |
|
Cardiovascular disease and depression |
|
Newly funded 2006 |
320 |
160 |
|
Twins as parents |
Telephone and mail |
Newly funded 2006 |
1,060 |
530 |
|
SOURCE: Adapted from VA, 2007c. |
||||
TABLE 10-4 National Academies’ and VA Medical Monographs on Veterans’ Health by Theater or Exposure
|
Mustard gas exposure |
IOM. 1993. Veterans at risk: The health effects of mustard gas and lewisite. |
|
Prisoners of war |
VA Medical Monographs. 1954. A follow-up study of World War II prisoners of war (Cohen and Cooper, 1954). IOM. 1992. The health of former prisoners of war: Results from the Medical Examination Survey of Former POWs of World War II and the Korean Conflict. |
|
Other WWII |
VA Medical Monographs. 1955. Tuberculosis in the Army of the United States in World War II. (Long and Jablon, 1955). VA Medical Monographs. 1961. A follow-up study of head wounds in World War II (Walker and Jablon, 1961). |
|
Radiation exposure |
NRC. 1985. Studies of participants in nuclear tests (Robinette et al., 1985). IOM. 1995a. Adverse reproductive outcomes in families of atomic veterans: The feasibility of epidemiologic studies. IOM. 1996b. Mortality of veteran participants in the CROSSROADS nuclear test. |
|
Vietnam veterans |
IOM. 1994. Veterans and Agent Orange: Health effects of herbicides used in Vietnam. IOM. 1996b. Mortality of veteran participants in the CROSSROADS nuclear test. IOM. 1997. Characterizing exposure of veterans to Agent Orange and other herbicides used in Vietnam: Scientific considerations regarding a request for proposals for research. IOM. 1999c. Veterans and Agent Orange: Update 1998. IOM. 2000d. Veterans and Agent Orange: Herbicide/dioxin exposure and type 2 diabetes. IOM. 2001b. Veterans and Agent Orange: Update 2000. IOM. 2002. Veterans and Agent Orange: Herbicide/dioxin exposure and acute myelogenous leukemia in the children of Vietnam veterans. IOM. 2003a. Characterizing exposure of veterans to Agent Orange and other herbicides used in Vietnam: Interim findings and recommendations. IOM. 2003b. Characterizing exposure of veterans to Agent Orange and other herbicides used in Vietnam: Final report. IOM. 2003d. Veterans and Agent Orange: Update 2002. IOM. 2004c. Veterans and Agent Orange: Length of presumptive period for association between exposure and respiratory cancer. IOM. 2005b. Veterans and Agent Orange: Update 2004. |
|
Gulf War veterans |
IOM. 1995b. Health consequences of service during the Persian Gulf War: Initial findings and recommendations for immediate action. IOM. 1996a. Health consequences of service during the Persian Gulf War: Recommendations for research and information systems. IOM. 1998a. Adequacy of the VA Persian Gulf Registry and Uniform Case Assessment Protocol. IOM. 1998b. Measuring the health of Persian Gulf veterans: Workshop summary. IOM. 1999a. Gulf War veterans: Measuring health. IOM. 2000a. The five series study: Mortality of military participants in U.S. nuclear weapons tests. IOM. 2000b. Gulf War and health, volume 1: Depleted uranium, pyridostigmine bromide, sarin, vaccines. IOM. 2001a. Gulf War veterans: Treating symptoms and syndromes. IOM. 2003c. Gulf War and health, volume 2: Insecticide and solvents. IOM. 2004a. Gulf War and health: Updated literature review of sarin. IOM. 2005a. Gulf War and health, volume 3: Fuels, combustion products, and propellants. IOM. 2006. Gulf War and health, volume 4: Health effects of serving in the Gulf War. IOM. 2007. Gulf War and health, volume 5: Infectious diseases. |
CDC-Funded Studies
The CDC and its National Center for Environmental Health has supported studies on veterans of Vietnam (SOURCE: http://www.cdc.gov/nceh/veterans/default1.htm) and the Gulf War (SOURCE: http://www.cdc.gov/nceh/veterans/default2.htm). Relating to Vietnam, CDC supported the following studies:
-
Vietnam Experience Study
-
Postservice Mortality Among Vietnam Veterans Study
-
Agent Orange Validation Study
-
Selected Cancers Study
On the Gulf War, CDC funded the following studies:
-
Health Effects of Exposure to Smoke from Oil Well Fires
-
Birth Defects
-
Air Force Study
-
Health Assessment of Gulf War Veterans from Iowa
-
Iowa Asthma Follow-Up Study
-
Cognitive Function and Symptom Patterns in Gulf War Veterans
-
Defining Gulf War Illness
-
Epidemiologic Study of the Occurrence of Amyotrophic Lateral Sclerosis (ALS) among Gulf War Veterans
-
Deployment to the Gulf War and Subsequent Development of Cancer
Of these CDC-funded studies, the Vietnam Experience Study was arguably the most influential. A random sample of 7,924 men who enlisted in the period from 1965 to 1971 and who served in Vietnam, and 7,364 non-Vietnam veterans, were interviewed by telephone. Vietnam veterans reported more health problems than non-Vietnam veterans, including less fertility and more health problems in their children. An in-person, comprehensive health evaluation was done on a random subsample of 2,490 Vietnam veterans and 1,972 non-Vietnam veterans. Although the vast majority of comparisons showed no differences, results of this examination showed more hearing loss, lower sperm concentrations, and more depression, anxiety, and PTSD in Vietnam veterans. Offspring of Vietnam veterans did not show increased birth defects (see Appendix K-3) (CDC VES, 1989).
NIH-Funded, Individual Investigator Studies
The NIH has funded a large number of health studies involving veterans through its several research funding mechanisms, and has also collaborated with VHA and CDC in providing funding for research on veterans. Relatively few NIH studies focus on investigating the role of military exposures in disease. Many use a population sample of veterans to gain mechanistic insight into diseases affecting the general population. Others evaluate effectiveness of disease treatment. NIH-funded studies that are relevant to the assessment of military exposure effects are listed in Appendix K-4 by title and year funding was begun.
Observations and Recommendations on Epidemiologic Studies of Veterans
Clearly a large number of epidemiologic studies on health effects of military exposure in veterans have been completed over the years. Many continue to be performed, reflecting the ongoing military engagements in Iraq and Afghanistan. There has been a near-exponential increase in the number of completed health studies and IOM reports in relation to the proximity in time of the specific engagement.
Although the scientific information on military exposures and subsequent health status is extensive, some exposures of concern remain inadequately studied or the relevant studies on these exposures have yielded findings that are inconclusive. It is acknowledged that there may be obsta-
cles to performing rigorous observational studies on the veteran population. Nevertheless, there are at least three other potential reasons for some of the inadequacy in the scientific information: (1) there has been no effective organized approach to setting research priorities; (2) exposure information and exposure metrics are relatively crude for most exposure-disease combinations of interest; and (3) there is no standardized, comprehensive, universal, and accessible source of information on veteran’s health outcomes.
Two complementary options for improving the utility of this health research in strengthening the scientific foundations for veterans’ compensation are (1) establishing a body that is responsible for strategically managing the research agenda on veterans and military exposures, and (2) developing and maintaining a repository of research on veterans’ health to allow an overview of research supported by various funding agencies. Suggestions to facilitate carrying out these studies and to allow more rigorous study of exposure health effects center on exploiting the exposure and health information systems described above. This would require more centralized data storage and improved data access.
VA REGISTRIES
Another public health surveillance tool that can be used to collect and organize health status data of a specific population is a registry. “A registry is an organized system for the collection, storage, retrieval, analysis, and dissemination of information on individual persons who have either a particular disease, a condition (e.g., a risk factor) that predisposes to the occurrence of a health-related event, or prior exposure to substances (or circumstances) known or suspected to cause adverse health effects” (SOURCE: From FAQ on Public Health Registries: www.ncvhs.hhs.gov/9701138b.htm).
Registry data offer a number of valuable uses in public health and medicine, “including estimating the magnitude of a problem,” “determining the incidence of disease,” “examining trends of disease over time,” “identifying groups at high-risk,” estimating health service needs, and “conducting research” (SOURCE: www.ncvhs.hhs.gov/9701138b.htm). For some groups of veterans, surveillance could be extended to intermediate markers, such as indicators of physiological functioning, so that adverse effects of exposures could be detected before the level of impairment became sufficient to produce a diagnosed disease. For example, in personnel exposed to respiratory hazards, lung function could be tracked over time to detect a rate of loss beyond that expected on the basis of aging alone.
Registries collect data on individuals who share certain characteristics, typically a specific disease or condition. This information includes demographic and medical information. Registries often seek validation of the
data by collecting detailed test results (such as a pathology report from a biopsy or a specific blood test result).
More recently, the registry concept has been applied to follow groups of people who do not share a common disease, but rather, a common exposure history. Examples here would include the National Exposure Registry operated by the Agency for Toxic Substances and Disease Registry (ATSDR), part of CDC. This registry identifies and enrolls persons likely to have been exposed to hazardous environmental toxicants, usually due to the location of the person’s residence near a contaminated Superfund site. The registry establishes a pool of persons, potentially at increased risk of health harm, and allows tracking of this group. This tracking enables subsequent contact of the registered persons by health authorities, who may offer health information, opportunities for study participation, or care recommendations. The course of the registrant’s health may also be followed over time through periodic surveys performed by the registry (ATSDR, 2003).
VA has used the public health registry concept to identify and track several different groups of veterans. It operates registries that are both disease based, such as the multiple sclerosis (MS) and amyotrophic lateral sclerosis (ALS) registries, and those that are exposure based, such as the Agent Orange and Gulf War registries (see Table 10-5).
Summary of Important Findings and Recommendations
DoD and VA are clearly intent on improving the breadth, depth, and availability of health and exposure data. In addition, there are numerous examples of those data being used to better understand Service member and veteran health and its relationship to exposures. Suggestions follow for ensuring that the data improvements are fully realized and the data fully utilized in Service member–veteran disease prevention and treatment in well-conceived and coordinated surveillance and research efforts and in compensation adjudication and presumptive decision-making. Many of these recommendations are also found in the Committee’s overall recommendations in Chapter 13. The Committee presents these suggestions here to tie back into the specific lessons learned from an assessment of the military personnel’s and veterans’ health and exposure data infrastructure.
-
Ensure that DOEHRS is implemented as planned.
DOEHRS is a major undertaking that has potential for dramatically increasing the availability of exposure data. However, DoD has many important priorities and short-term funding pressures have the potential to delay implementation activities. Due to the importance of these efforts for both DoD and VA, we recommend that additional steps be taken to ensure that DOEHRS is fully implemented as planned. In addition, due to the
importance of adequately trained individuals to the success of DOEHRS, we further recommend that these steps specifically include detail on the training of individuals needed to make the accurate professional judgments and generate appropriate exposure data critical to DOEHRS. These additional steps are as follows:
-
Include a specific DoD budget line item for DOEHRS that includes funding for system development and enhancement, system implementation, and training of personnel.
-
Develop clear metrics for tracking the effective deployment and utilization of DOEHRS throughout DoD.
-
Require an annual status report to Congress on DOEHRS development and implementation progress and related training activities.
-
Improve the interface between the electronic health record data systems used by DoD and VA—including capabilities for handling individual exposure information that is included as part of a Service member’s health record.
While there are efforts underway to electronically transfer Service member health records from DoD to VA, these efforts are moving slowly and the timeline for completion of a seamless interface is unclear. DoD and VA should increase attention to this effort with a clear integration plan, time-table for implementation, metrics for tracking implementation progress, and annual reporting of metric results.
To date, there has been little discussion regarding the electronic transfer of Service member exposure information to VA. As the inclusion of exposure data in employee health records is a key DoD strategy for ensuring that exposure information is available for individual Service members, this seems a major disconnect. DoD and VA should explicitly include the integration of these individual exposure data into the health record transfer integration plan, implementation timetable, metrics, and annual reporting. Reports on progress of these plans should be included in the annual report to Congress on DOEHRS progress.
-
Develop an interface that allows the VA to access the electronic exposure data systems used by DoD.
DoD is investing heavily in DOEHRS and other improved exposure data systems that are standardized across the various armed services. In our interviews with people responsible for development and deployment of these systems we did not encounter anyone with knowledge of activities by DoD or VA to develop a VA interface with these systems that will allow use of the Service member-specific and longitudinal exposure data by VA.
TABLE 10-5 VA Health Registries
|
Registry Management Purpose |
Number of Veterans |
Basis for Enrollment |
Source of Data |
Type of Data |
|
Agent Orange Registrya (Started in 1978) |
408,811 400,849 men 7,962 women |
Service in Vietnam, Korea, or otherwise exposed |
Dates, areas of service, possible Agent Orange exposure, birth defect data |
Purely voluntary; data from Agent Orange Registry exams; veterans are well informed of the existence of registry exams |
|
Managed by the Environmental Agents Service |
|
|||
|
To identify medical problems associated with Agent Orange exposure |
|
|
|
|
Data Collected |
Selected Publications from Registry |
|
Demographics: Race/ethnicity; martial status; gender; current military status; branch of service; service in either/or Vietnam or Korea; dates of last two periods of service if other than Vietnam or Korea; full medical history, including information about the family, occupation, social history noting tobacco, alcohol, and drug use; civilian exposure to possible toxic agents; psychosocial history |
Bullman TA, Kang HK. 1994. Posttraumatic stress disorder and the risk of traumatic deaths among Vietnam veterans. Journal of Nervous and Mental Disorder 182:604-610. |
|
Bullman TA, Watanabe KK, Kang HK. 1994. Risk of testicular cancer associated with surrogate measures of Agent Orange exposure among Vietnam veterans on the Agent Orange Registry. Annals of Epidemiology 4:11-16. |
|
|
Medical history: Assessment of own health; date of registry examination; complaints/symptoms (coders are asked to enter ICD-9 codes on form); chest X ray (if determined to be medically necessary); complete blood count; comprehensive metabolic panel or blood chemistries and enzyme studies; urinalysis; hepatitis C screening |
Bullman TA, Kang HK, Thomas TL. 1991. Posttraumatic stress disorder among Vietnam veterans on the Agent Orange Registry: A case control analysis. Annals of Epidemiology 1:505-512. |
|
Exposure: Exposure to Agent Orange (definitely yes, not sure, definitely no); handling or spraying Agent Orange; not directly sprayed but in a recently sprayed area; exposed to herbicides other than Agent Orange; directly sprayed with Agent Orange; ate food/drink that could have been sprayed with Agent Orange |
|
|
Registry Management Purpose |
Number of Veterans |
Basis for Enrollment |
Source of Data |
Type of Data |
|
Gulf War Registryb (Started in 1992) |
97,002 87,074 men 9,928 women |
Service in SW Asia (1990 to present) Operation Enduring Freedom (OEF) veterans not included because they are in Afghanistan |
Exposures of concern, combat experiences, birth defect data |
Purely voluntary; data from Gulf War Registry exams |
|
Managed by the Environmental Agents Service |
||||
|
To identify medical problems associated with exposures in the Persian Gulf |
|
|
|
|
Data Collected |
Selected Publications from Registry |
|
Demographics: Race/ethnicity; marital status; gender; occupation; current military status; branch of service; military service in Persian Gulf area; dates and MOS of last two periods of service |
Miller R, Costigan, Young H, Kang H, Salager N, Crawford H, Page W, Thaul S. 2006. Patterns of health care seeking of Persian Gulf War Registry members prior to deployment. Military Medicine 171:370-375. |
|
Medical history: Family history; occupational history; social history including tobacco, alcohol, drug use; civilian exposure(s) history to possible toxic agent; psychosocial history; military service in Persian Gulf area; dates and military occupational specialty (MOS) of last two periods of service |
Gray GC, Gackstetter GD, Kang HK, Graham JT, Scott KC. 2004. After more than 10 years of Gulf War veteran medical evaluation, what have we learned? American Journal of Preventive Medicine 26:443-452. |
|
Hallman WK, Kipen HM, Diefenbach M, Boyd K, Kang H, Leventhal H, Wartenber D. 2003. American Journal of Public Health 93:624-629. |
|
|
Medical history: Psychosocial conditions; review of systems; complaints and symptoms (coders asked to include ICD-9 codes on form); time of onset of the symptoms or conditions; intensity; degree of physical incapacitation; details of any treatment received; complete blood count; blood and serum screening tests; urinalysis; pulmonary function, sperm counts, or other diagnostic studies if medically indicated |
Smith TC, Smith B, Ryan MA, Gray GC, Hooper TI, Heller JM, Dalager NA, Kang HK, Gackstetter GD. 2002. Ten years and 100,000 participants later: Occupational and other factors influencing participation in US Gulf War health registries. Journal of Occupational and Environmental Medicine 44:758-768. |
|
Murphy FM, Kang HK, Dalager NA. 1999. The health status of Gulf War veterans: Lessons learned from the Department of Veterans Affairs health registry. Military Medicine 164:327-331. |
|
|
Kipen HM, Hallman W, Kang HK, et al. 1999. Prevalence of chronic fatigue and chemical sensitivities in Gulf Registry veterans. Archives of Environmental Health 54:313-318. |
|
Registry Management Purpose |
Number of Veterans |
Basis for Enrollment |
Source of Data |
Type of Data |
|
Ionizing Radiation Registryc (Started in 1986) |
23,624 23,472 men 152 women |
Set up for WWII and Cold War veterans |
Receipt of nasopharyngeal treatment, birth defect data, diagnoses if possible radiogenic-related diseases, disability claims |
Purely voluntary; data from Ionizing Radiation Registry exams |
|
Managed by the Environmental Agents Service |
|
Service in Hiroshima and Nagasaki, gaseous diffusion plants, and area K25 in United States; nuclear weapons testing |
||
|
To identify medical problems associated with ionizing radiation exposure |
|
|||
|
ALS Registry |
1,602 |
Diagnoses of ALS within VA health-care system and self-referrals |
Health-care utilization, ALS Functional Rating Scale every 6 months |
Data from existing VA files and self-referrals; a consecutive registry |
|
Managed by the Epidemiologic Research and Information Center in Durham, NC |
|
|||
|
To identify and characterize veterans with ALS |
|
|
|
|
Data Collected |
Selected Publications from Registry |
|
Exposure: Exposure to environmental factors (smoking cigarettes, years of smoking cigarettes, number of packs smoked per day, years smoked); while in the Gulf exposure to smoke from oil fires, fumes from tent heaters, cigarette smoke (passive from others), diesel and/or other petrochemical fumes, and burning trash/ feces; skin exposure to diesel; chemical agent-resistant compounds; other paint or solvent and/or petrochemical substances; depleted uranium; microwaves; personal pesticide use; nerve gas or other nerve agent |
Gray GC, Hawksworth AW, Smith TC, Kang HK, et al. 1998. Gulf War veterans’ health registries. Who is most likely to seek evaluation? American Journal of Epidemiology 148:343-349. |
|
Blanck RR, Hiatt J, Hyams KC, Kang HK, et al. 1995. Unexplained illnesses among Desert Storm Veterans: A search for causes, treatment, and cooperation. Archives of Internal Medicine 155:262-268. |
|
|
Demographics: Family; occupation; tobacco, alcohol, and drug use |
|
|
Medical History: Psychosocial conditions; time of the onset of the veteran’s symptoms or conditions; intensity of symptoms or conditions; degree of physical incapacitation; details of any treatment received; chest X ray (if medically necessary), complete blood count; basic metabolic panel and comprehensive metabolic panel or equivalent blood chemistries and enzyme studies; urinalysis |
|
|
|
Kasarkis EJ, Dominic K, Oddone EZ. 2004. The National Registry of Veterans with Amyotrophic Lateral Sclerosis: Department of Veterans Affairs Cooperative Studies Program (CSP). Amyotrophic Lateral Sclerosis & Other Motor Neuron Disorders 5(Supplement 1):129-132. |
|
Registry Management Purpose |
Number of Veterans |
Basis for Enrollment |
Source of Data |
Type of Data |
|
MS Registry (Started in 1998) |
31,946 |
Diagnoses of MS within the VA health-care system |
Health-care utilization, health economic data |
Data from existing VA files; a consecutive registry |
|
Managed by the MS Center of Excellence East in Baltimore, MD, and the MS Center of Excellence West in Portland, OR, and Seattle, WA, to identify and characterize veterans with MS |
|
|||
|
Cancer Registry (Started in 1995) |
356,174 |
Diagnoses of cancer within the VA healthcare system |
Possible cancer risk factors, cancer identification, prognosis factors, treatment data, follow-up, and recurrence |
Compilation of cancer registries at each VA facility; a consecutive registry |
|
Managed by the Program Office for Oncology in Washington, DC |
|
|||
|
To identify and characterize veterans with cancer, analysis of specific therapies and outcomes, and resource allocation |
|
|
|
Data Collected |
Selected Publications from Registry |
|
|
Culpepper WJ, Mhrmantraut M, Wallin MT, Flannery K, Bradham DD. 2006. Veteran Health Administration multiple sclerosis surveillance registry: The problem of case-finding from administrative databases. Journal of Rehabilitation Research and Development 43(1):17-24. |
|
Registry Management Purpose |
Number of Veterans |
Basis for Enrollment |
Source of Data |
Type of Data |
|
HIV Registry (Started in 1983) |
54,000 |
Diagnoses of HIV within the VA healthcare system |
Possible risk factors, lab results, pharmacy use |
Data from existing VA files; a consecutive registry |
|
Managed by the Center for Quality Management in Public Health in Palo Alto, CA |
|
|||
|
To track overall trends in HIV-related outcomes, health-care utilization planning, quality improvement of care |
|
|
|
|
|
Hepatitis C Registry (Started in 1996) |
253,160 |
Diagnoses of hepatitis C within the VA health-care system |
Liver biopsy data, lab results, pharmacy use |
Data from existing VA files; a consecutive registry |
|
Managed by the Center for Quality Management in Public Health in Palo Alto, CA |
|
|||
|
To track overall trends in hepatitis C-related outcomes, healthcare utilization planning, quality improvement of care |
|
|
|
|
|
Registry Management Purpose |
Number of Veterans |
Basis for Enrollment |
Source of Data |
Type of Data |
|
Depression Registry (Started in 2001)d |
690,867 (in FY 2005) |
Diagnoses of depression within the VA health-care system |
Health-care utilization, Global Assessment Functioning Scores, medication use, health-care costs |
Data from existing VA files; an annual registry |
|
Managed by the Serious Mental Illness Treatment, Research, and Evaluation Center in Ann Arbor, MI |
|
|||
|
To identify and characterize veterans with depression; monitor and evaluate care |
|
|
|
|
|
Psychoses Registrye (Started in 1988) |
239,304 (in FY 2005) |
Diagnoses of psychoses within the VA health-care system |
Healthcare utilization, Global Assessment Functioning Scores, medication use, health-care costs |
Data from existing VA files; a consecutive registry |
|
Managed by the Serious Mental Illness Treatment, Research, and Evaluation Center in Ann Arbor, MI |
|
|||
|
To identify and characterize veterans with psychoses; monitor and evaluate care |
|
|
|
|
|
a More information can be found at http://www1.va.gov/vhapublications/ViewPublication.asp?pub_ID=77. b More information can be found at http://www.vethealth.cio.med.va.gov/Pubs/1303.2GWHB-05.pdf. c More information can be found at http://www1.va.gov/irad/docs/IRADHANDBOOK012006.PDF. |
||||
|
Data Collected |
Selected Publications from Registry |
|
Demographics: Age, gender; race/ethnicity; marital status; VISN analyses; service connection; VERA patient class, homelessness, access to medical care |
|
|
Medical History: Inpatient and outpatient services uses; medication and services use; health-care costs; primary care treatment; mortality; psychiatric comorbidities (depression alone or depression with an anxiety disorder other than PTSD); depression and substance abuse; depression and PTSD; other complicated depression; medical comorbidities (peripheral vascular disease, chronic obstructive pulmonary disease, diseases of the digestive system, liver disease, genitourinary symptoms, arthritis, injury and poisoning); Global Assessment of Functioning (GAF) |
|
|
Demographics: Age, gender, race; martial status |
|
|
Medical History: Pharmacy and medical services use; cost; diagnoses (total, schizophrenia, bipolar, other); GAF scores; mortality; VERA patient class; homelessness; service connection; access to health care; inpatient psychiatric care; inpatient rehabilitation; inpatient domiciliary care; inpatient nursing home care; outpatient care |
|
|
d More information can be found at http://www.hsrd.ann-arbor.med.va.gov/documents/2002NARDEP.pdf. e More information can be found at http://www.hsrd.ann-arbor.med.va.gov/documents/3rdAnnual_psychosisVHA.pdf. SOURCE: Derived from a DoD/VHA, 2000; b DoD/VHA, 2005; c DoD/VHA, 2006; Kang, 2006; d SMITREC, 2002; e SMITREC, 2001. |
|
VA should move quickly to develop plans for interfaces to these new DoD exposure data systems. This should not require massive new data systems within VA but instead consist of appropriate interfaces and views to the data within DoD systems that are accessible by the VA. The first step would be a VA team embedded with DoD implementation team at the Army’s CHPPM where they can examine the system capabilities and data structures so that appropriate interfaces can be defined and developed to meet the needs of VA.
Recommendation: Conduct a critical evaluation of Gulf War troop tracking and environmental exposure monitoring data so that improvements can be made in this key DoD strategy for characterizing exposures during deployment.
Characterizing exposures during intense combat deployment scenarios is the most challenging aspect of DoD’s efforts to characterize Service member exposures throughout their military service. An important part of the current strategy is a combination of troop tracking and environmental monitoring such that overlaying of troop location with the location of environmental monitoring results will enable the characterization of troop exposures. The success of this approach depends directly on the detail of both the troop tracking and the environmental monitoring. More frequent measurement and recording of troop location coupled with more frequent (e.g., time and location) environmental exposure monitoring will allow more accurate characterization of individual exposures. The current goal is to record troop location at least once every 24 hours. Minimal environmental monitoring requirements are less clear. In particular, monitoring during shorter deployments (less than 30 days) may be sporadic as requirements vary depending on the predeployment risk assessment, the availability of appropriate medical personnel, and the commander’s discretion (DOD Instruction 6490.03 [DoD, 2006c]).
DoD should undertake a detailed review of this strategy using data from the Gulf War and subsequent deployments in Afghanistan and Iraq to determine limitations to the current approach and identify opportunities for improvement. The review should consist of the formation of exposure matrices for a group of randomly selected Service members who served in that theater using data available on troop location, environmental measurements, and exposure data in individual health records. Gaps in those exposure matrices should then be examined to identify data limitations so that strategies can be developed for future approaches that minimize those limitations.
-
Develop DoD policy to ensure that classification/declassification (secrecy) issues are managed appropriately for both DoD and the veteran.
There are clearly times when national security or mission success depends on maintaining secrecy regarding certain aspects of a Service member’s military experience. However, every effort should be made to find mechanisms for characterizing Service member exposure and health histories in manners that do not interfere with the broader issues of national security or mission success. DoD should develop procedures that ensure full or partial declassification of sensitive information for the timely provision of that Service member’s or veteran’s health care. When such declassification is not possible, DoD should establish procedures whereby blinded data relevant to the Service member’s health and exposure history are provided.
In some instances where national security and secrecy issues cannot be resolved, DoD and VA may need to establish mechanisms involving experts with appropriate security clearances to monitor affected registry cohorts for potential health outcomes and define surveillance or research activities that may need to be conducted within appropriate secrecy clearances. An interagency agreement could be developed between DoD and VA addressing the secrecy issue. Since both agencies have used the classification system in the past this agreement would address the policy development process and the exchange of classified information between the two agencies. The process would include establishment of a joint DoD-VA board comprised of individuals who have sufficient security clearance to discuss classified data. The access to classified information process would be contained in a written document outlining a mechanism to identify, monitor, track, and medically treat individuals who were part of research activities involving human subjects and whose research design and results have been classified.
Recommendation: Establish registries of Service members and veterans based on exposure, deployment, and disease histories.
Recommendation: DoD and VA should establish and implement mechanisms to identify, monitor, track, and medically treat individuals involved in research and other activities that have been classified and are secret.
-
Strengthen the assessment of psychological stressors and symptoms.
Psychological and combat-related stressors may detrimentally impact the long-term mental and emotional well-being of military personnel and should be thoroughly assessed at key points during the military career of men and women. Currently, basic clinical evaluations for neurological and psychiatric disorders are made at accession, after training, and throughout
the service career. Very brief structured assessments for some psychiatric symptoms occur during the post-deployment periods only.
Assessment of exposure to combat and of psychological stress during deployment is a particularly challenging element of the Committee’s proposed approach to tracking factors influencing the health of veterans. Scales have been developed to assess exposures during combat and the validity and reliability of these instruments has been assessed (Friedman et al., 1986; Janes et al., 1991; Keane et al., 1989; Laufer et al., 1984; Lund et al., 1984; Wessely et al., 2003). These instruments have been used in investigations of Vietnam veterans (Buydens-Branch et al., 1990; Frueh et al., 2005; Green et al., 1989; Yehuda et al., 1992) and more recently for personnel deployed in Iraq and Afghanistan (Hoge et al., 2004). A 2004 study carried out by military investigators addressed mental health problems and combat duty in personnel deployed to Iraq and Afghanistan (Hoge et al., 2004). This study demonstrates the feasibility of investigations directed at troops in relation to combat deployment. A follow-up study of Vietnam veterans, the National Vietnam Veterans Readjustment Study, incorporated an exposure measure based on military records (Dohrenwend et al., 2006). Onset of posttraumatic stress disorder (PTSD) was associated with combat exposure, with evidence for a positive close-response relationship.
These studies show that combat exposure and related stress can be measured. They also show the feasibility of informative research on neuropsychiatric disorders among veterans. Further development will be needed to achieve the type of surveillance proposed by the Committee.
Psychiatric disorders, particularly PTSD, depression, and alcohol abuse and dependence are common. More data systematically collected using validated and structured instruments pre- and post-deployment will aid DoD and the VA to better identify stressors that may predispose individuals to develop these disorders, identify Service members to whom early intervention should be provided, and track individuals exposed to emotional trauma and with psychiatric symptoms in specialized registries.
A number of brief validated instruments are available for PTSD, major depression, and alcohol abuse and dependence—three common psychiatric disorders experienced by veterans. A dedicated, face-to-face interview by an experienced clinician, recognized to be the most valid method of assessing PTSD, is likely not feasible in the post-deployment or separation/retirement medical evaluations. While a host of instruments are available for assessing PTSD, realistically the only feasible instruments that might be useful in this context would be one of several available screening questionnaires. These include (1) the 4-question Primary Care PTSD Screen (Prins et al., 2003), (2) a 7-question scale keyed to the DSM-IV criteria for PTSD (Breslau et al., 1999), (3) the 17-question PTSD Symptom Scale Self-Report (Coffey et al., 1998), (4) the Screen for Posttraumatic Stress Symptoms (Carlson, 2001),
and (5) the PTSD subscale of the large Psychiatric Diagnostic Screening Questionnaire (Zimmerman and Mattia, 2001). Only the first of these, the Primary Care PTSD Screen, has been validated on combat veterans. Also, while these screening instruments may be useful in identifying veterans who may have PTSD, they are not adequate for diagnosing PTSD.
There are also a host of screening instruments for major depression including the 2 item Prime-MD, the 9 item Patient Health Questionnaire, and the 20 item Centers for Epidemiological Studies Depression (CES-D) scale, among others. Alcohol abuse and dependence can be screened with a number of instruments including the RAPS-QF, the AUDIT, and the CAGE, among others. These instruments vary in length and sensitivity and specificity in different populations.
Studies that employ these screening instruments for prospective research will need to account for some degree of misclassification of the health outcome. In spite of these shortcomings, data from a screening instrument on an unselected population of veterans obtained in a systematic manner would be very valuable for the type of prospective studies envisioned in this report to better understand service-related morbidity.
-
Establish registries of Service members and veterans based on exposure, deployment, and disease histories.
The Committee recommends that VA and Congress consider the initiation and prospective follow-up of specific veteran populations who may share a common exposure history as a viable surveillance tool. Creating a registry that may include initial demographic, exposure, and health information is a reasonable interim response to veterans with unexplained or underexplained health complaints that are temporally but not scientifically related to military service.
A registry would allow the formation of a pool of veterans who are linked by some shared attribute of military service, such as combat campaign, theater location, or catastrophic event (e.g., Khamisiyah, Iraq), to be identified and actively followed forward through regular follow-up contacts from the registry staff. Trends in health of the registrants could be followed forward, and communication with registrants about new health information or treatment recommendations could be facilitated. As well, the registrants could be invited to participate in scientific studies to elucidate the cause or proposed mechanism of health harm they may have experienced. Such a model is being used to follow the World Trade Center responders, workers, and neighborhood population. This model differs somewhat from existing VA registries (e.g., Gulf War or Agent Orange) in that these tend to be cross-sectional assessments, with little regular follow-up or interaction with staff.
Although registry costs can be high, so are the costs of presumptions. Enrollment in a registry may offer the veteran access to some of the medi-
cal services a presumption provides, but under a different mechanism that could allow time for the clinical and epidemiologic evidence to accumulate so as to make a more evidence-based decision about a presumption.
Recommendation: Develop a plan for an overall integrated surveillance strategy for the health of Service members and veterans.
It is critical that DoD and VA work together to define a common strategy for integrated health surveillance of Service members and veterans. Fully leveraging the Service member-veteran exposure and health data is critical to the full understanding of disease etiology and causation, the establishment of relative risk, the adjudication of disability claims, and the treatment of disease. It is also critical to appropriate deliberations regarding presumptions in disability decision making.
The need for surveillance can be identified at any point in a Service member’s or veteran’s experience history. Surveillance studies begun during a Service member’s service career may need to extend into his or her post-service experience. Data needs for the specific surveillance activity may have been generated during either the Service member experience or the veteran experience or both. Therefore this activity must be jointly well managed by DoD and VA. A strong central organization, staffed jointly by DoD and VA with external expert advisors, should be given responsibility for the ongoing evaluation of health and exposure data quality, the regular review of registry and surveillance activities, the definition of surveillance and research strategies, and the coordination of surveillance and research projects. This joint DoD-VA Service member and veteran exposure and health surveillance organization would have broad responsibility for oversight of all DoD and VA surveillance and research activities whether they are conducted internally or externally by those organizations.
Recommendation: Improve the data linkage between the electronic health record data systems used by DoD and VA—including capabilities for handling individual Service member exposure information that is included as part of the individual’s health record.
Although there are efforts underway to electronically transfer Service member health records from DoD to VA, these efforts are moving slowly and the timeline for completion of a seamless interface is unclear. DoD and VA should increase attention to this effort with a clear integration plan, timetable for implementation, metrics for tracking implementation progress, and annual reporting of metric results.
To date there has been little discussion regarding electronic transfer of Service members’ exposure information in their health records to VA. As the
inclusion of exposure data in employee health records is a key DoD strategy for ensuring that exposure information is available for individual Service members, this appears to be a major weakness in the system. DoD and VA should explicitly include the integration of these individual exposure data into the health record transfer integration plan, implementation timetable, metrics, and annual reporting. Reports on progress of these plans should be included in the annual report to Congress on DOEHRS progress.
Recommendation: Ensure implementation of the DoD strategy for improved exposure assessment and exposure data collection.
The DOEHRS program is a major undertaking that has potential for dramatically increasing the availability of exposure data. However, DoD has many important priorities, and short-term funding pressures have the potential to delay implementation activities. Because of the importance of these efforts, not only to DoD but to VA as well, we recommend that additional steps be taken to ensure that DOEHRS is fully implemented as planned. In addition, because of the importance of adequately trained individuals to the success of DOEHRS, we further recommend that these steps specifically include detail on the training of individuals needed to make the accurate professional judgments and generate appropriate exposure data critical to DOEHRS. These additional steps are as follows:
-
Include a specific DoD budget line item for DOEHRS that includes funding for system development and enhancement, system implementation, and training of personnel.
-
Develop clear metrics for tracking the effective deployment and utilization of DOEHRS throughout DoD.
-
Require an annual status report to Congress on DOEHRS development and implementation progress and related training activities.
Recommendation: Develop a data interface that allows VA to access the electronic exposure data systems used by DoD.
DoD is investing heavily in DOEHRS and other improved exposure data systems that are standardized across the various armed services. In the Committee’s interviews with people responsible for development and deployment of these systems, we did not encounter anyone with knowledge of activities by DoD or VA to develop a VA interface with these systems that will allow use of the Service member-specific and longitudinal exposure data by VA.
VA should move quickly to develop plans for interfaces to these new DoD exposure data systems. This should not require massive new data
systems within VA but instead consist of appropriate interfaces and views to the data within DoD systems that are accessible by VA. The first step would be a VA team embedded within the DoD implementation team at the Army’s Center for Health Promotion and Preventive Medicine where the VA team can examine the system capabilities and data structures so that appropriate interfaces can be defined and developed to meet the needs of VA.
Recommendation: Consider interim interventions for affected veterans while data are collected or more thoroughly analyzed to resolve scientific uncertainty.
It can take significant time to collect and analyze data needed to adequately resolve scientific uncertainty in establishing causal relationships between exposure and disease. VA should consider interim interventions in instances where veterans are severely affected during the time it takes to conduct the needed research. These measures might consist of provisional health care for affected veterans during the interim period.
REFERENCES
AHRQ (Agency for Healthcare Research and Quality). 2006. Guide to clinical preventive services. Recommendations of the U.S. Preventive Services Task Force. AHRQ Publication No. 06-0588. Rockville, MD: AHRQ.
ASTM (American Society for Testing and Materials). 2003. Standard guide for environmental health site assessment process for military deployments. Designation E 2318-03. West Conshohocken, PA: ASTM International.
ATSDR (Agency for Toxic Substances and Disease Registry). 2003. What Is the National Exposure Registry (NER)? http://www.atsdr.cdc.gov/NER/index.html (accessed April 6, 2007).
Breslau, N., E. L. Peterson, R. C. Kessler, L. R. Schultz. 1999. Short screening scale for DSM-IV posttraumatic stress disorder. American Journal of Psychiatry 156(6):908-911.
Buydens-Branch, N. D., and M. Branchey. 1990. Duration and intensity of combat exposure and posttraumatic stress disorder in Vietnam veterans. Journal of Nervous and Mental Disease 178:582-587.
Carlson, E. B. 2001. Psychometric study of a brief screen for PTSD: Assessing the impact of multiple traumatic events. Assessment 8(4):431-441.
CDC VES (Centers for Disease Control and Prevention Vietnam Experience Study). 1989. Health status of Vietnam veterans. Synopsis. Vol. 1. Atlanta, GA: Centers for Disease Control. http://www.cdc.gov/nceh/veterans/default1c.htm (accessed April 9, 2007).
Coffey, S. F., B. S. Dansky, S. A. Falsetti, M. E. Saladin, K. T. Brady. 1998. Screening for PTSD in a substance abuse sample: Psychometric properties of a modified version of the PTSD Symptom Scale Self-Report. Posttraumatic stress disorder. Journal of Traumatic Stress 11(2):393-399.
Cohen, B. M., and M. Z. Cooper. 1954. A follow-up study of World War II prisoners of war. VA Medical Monograph. Washington, DC: U.S. Government Printing Office.
Do, N. 2006. DoD and Veterans Affairs: Health information sharing. Paper presented at the third meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, San Antonio, TX.
DoD (Department of Defense). 1997. Instruction 6490.3: Implementation and application of joint medical surveillance for deployments. Fort Sam Houston, TX: Army Medical Department Center and School.
DoD. 2004. Directive 6490.2: Comprehensive health surveillance.
DoD. 2006a. Defense Occupational and Environmental Health Readiness System (DOEHRS): Implementation and training (I&T) plan. PLN-002. Washington, DC: DOEHRS Project Management Office.
DoD. 2006b. Defense Occupational and Environmental Health Readiness System (DOEHRS). Student Guide Version 1.0.2.0. Washington, DC: DOEHRS Project Management Office.
DoD. 2006c. Instruction 6490.03: Deployment health.
DoD. 2006d. Periodic health assessment policy for active duty and selected reserve members. Memorandum for Assistant Secretary of the Army, Assistant Secretary of the Navy, Assistant Secretary of the Air Force. HA Policy 06-006. Washington, DC: Department of Defense.
DoD Industrial Hygiene Working Group. 2000. DoD industrial hygiene exposure assessment model. Report 2000-1. https://www.denix.osd.mil/denix/Public/News/Army/DOHP/Occhealth/Documents/IHEAM/ihassessmodelv8.html (accessed July 28, 2007).
DoD/VHA (Veterans Health Administration). 2000. VHA Directive 1302: Agent Orange Registry (AOR) Program. Washington, DC: Department of Veterans Affairs/Veterans Health Administration. http://www1.va.gov/vhapublications/ViewPublication.asp?pub_ID=77 (accessed April 6, 2007).
DoD/VHA. 2005. VHA Handbook 1303.2: Gulf War (Including Operation Iraqi Freedom) Registry (GWR) Program—(formerly Persian Gulf Registry [GWR] Program). Washington, DC: Department of Veterans Affairs/Veterans Health Administration. http://www.vethealth.cio.med.va.gov/Pubs/1303.2GWHB-05.pdf (accessed April 6, 2007).
DoD/VHA. 2006. Ionizing Radiation Registry (IRR) Program procedures. Washington, DC: Department of Veterans Affairs/Veterans Health Administration. http://www1.va.gov/irad/docs/IRADHANDBOOK012006.PDF (accessed April 9, 2007).
Dohrenwend, B. P., J. B. Turner, N. A. Turse, B. G. Adams, K. C. Koenen, and R. Marshall. 2006. The psychological risks of Vietnam for U.S. veterans: A revisit with new data and methods. Science 313:979-982.
Friedman, M. J., C. K. Schneiderman, A. N. West, and J. A. Corson. 1986. Measurement of combat exposure, posttraumatic stress disorder, and life stress among Vietnam combat veterans. American Journal of Psychiatry 143:537-539.
Frueh, B. C., J. D. Elhai, A. L. Grubaugh, J. Monnier, T. B. Kashdan, J. A. Sauvageot, M. B. Hamner, B. G. Burkett, and G. W. Arana. 2005. Documented combat exposure of U.S. veterans seeking treatment for combat-related post-traumatic stress disorder. British Journal of Psychiatry 186:467-472.
GAO (Government Accountability Office). 1999. Veterans’ benefits claims: Further improvements needed in claims-processing accuracy. Report to the ranking minority member, Committee on Veterans’ Affairs, House of Representatives. GAO/HEHS-99-35. Washington, DC: Government Accountability Office. http://www.gao.gov/archive/1999/he99035.pdf (accessed February 14, 2007).
GAO. 2000a. Veterans Benefits Administration: Problems and challenges facing disability claims processing: Testimony before the Subcommittee on Oversight and Investigations, Committee on Veterans’ Affairs, House of Representatives, Statement of Cynthia A. Bascetta, Association Director, Veterans’ Affairs and Military Health Care Issues, Health, Education, and Human Services Division. GAO/T-HEHS/AIMD-00-146. Washington, DC: Government Accountability Office. http://www.gao.gov/new.items/h100146t.pdf (accessed February 14, 2007).
GAO. 2000b. Veterans’ benefits: Promising claims-processing practices need to be evaluated. Report to ranking minority member, Committee on Veterans’ Affairs, House of Representatives. GAO/HEHS-00-65. Washington, DC: Government Accountability Office. http://www.gao.gov/archive/2000/he00065.pdf (accessed February 14, 2007).
GAO. 2005a. DoD and VA systematic data sharing would help expedite servicemembers’ transition to VA services: Testimony before the Subcommittee on Oversight and Investigations, Committee on Veterans’ Affairs, House of Representatives. Statement of Cynthia A. Bascetta. Director, Health Care—Veterans’ Health and Benefits Issues. GAO-05-722T. Washington, DC: Government Accountability Office. http://www.gao.gov/new.items/d05722t.pdf (accessed February 14, 2007).
GAO. 2005b. Veterans’ Benefits: Further changes in VBA’s field office structure could help improve disability claims processing: Report to congressional requesters. GAO-06-149. Washington, DC: Government Accountability Office. http://www.gao.gov/new.items/d06149.pdf (accessed February 14, 2007).
GAO. 2006. VA and DoD health care: Opportunities to maximize resource sharing remain. Report to congressional committees. GAO-06-315. Washington, DC: Government Accountability Office. http://www.gao.gov/new.items/d06315.pdf (accessed February 14, 2007).
GAO. 2007. VA and DoD are making progress in sharing medical information, but remain far from having comprehensive electronic medical records. GAO-07-1108T. Washington, DC: Government Accountability Office. http://www.gao.gov/new.items/d071108t.pdf (accessed July 27, 2007).
Goldberg, J., B. Curran, M. E. Vitek, W. G. Henderson, and E. J. Boyko. 2002. The Vietnam Era Twin Registry. Twin Research 5(5):476-481.
Gray, G. C., K. B. Chesbrough, M. A. Ryan, P. Amoroso, E. J. Boyko, G. D. Gackstetter, T. I. Hooper, J. R. Riddle, Millennium Cohort Study Group. 2002. The millennium cohort study: A 21-year prospective cohort study of 140,000 military personnel. Military Medicine 167(6):483-488.
Green, B. L., J. D. Lindy, M. C. Grace, and G. C. Gleser. 1989. Multiple diagnosis in posttraumatic stress disorder. The role of war stressors. Journal of Nervous and Mental Disease 177:329-335.
Heller, J. M. 2006. Deployment health surveillance: Past, current, and future operations. Paper presented at the second meeting of the IOM’s Committee on the Evaluation of Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
Henderson, W. G., S. Eisen, J. Goldberg, W. R. True, J. E. Barnes, and M. E. Vitek. 1990. The Vietnam Era Twin Registry: A resource for medical research. Public Health Reports 105(4):368-373.
Hoge, C. W., C. A. Castro, S. C. Messer, D. McGurk, D. I. Cotting, and R. L. Koffman. 2004. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. New England Journal of Medicine 351:13-22.
IOM (Institute of Medicine). 1992. The health of former prisoners of war. Washington, DC: National Academy Press.
IOM. 1993. Veterans at risk: The health effects of mustard gas and lewisite. Washington, DC: National Academy Press.
IOM. 1994. Veterans and Agent Orange: Health effects of herbicides used in Vietnam. Washington, DC: National Academy Press.
IOM. 1995a. Adverse reproductive outcomes in families of atomic veterans: The feasibility of epidemiologic studies. Washington, DC: National Academy Press.
IOM. 1995b. Health consequences of service during the Persian Gulf War: Initial findings and recommendations for immediate action. Washington, DC: National Academy Press.
IOM. 1996a. Health consequences of service during the Persian Gulf War: Recommendations for research and information systems. Washington, DC: National Academy Press.
IOM. 1996b. Mortality of veteran participants in the CROSSROADS nuclear test. Washington, DC: National Academy Press.
IOM. 1997. Characterizing exposure of veterans to agent orange and other herbicides used in Vietnam: Scientific considerations regarding a request for proposals for research. Washington, DC: National Academy Press.
IOM. 1998a. Adequacy of the VA Persian Gulf registry and uniform case assessment protocol. Washington, DC: National Academy Press.
IOM. 1998b. Measuring the health of Persian Gulf veterans: Workshop summary. Washington, DC: National Academy Press.
IOM. 1999a. Gulf War veterans: Measuring health. Washington, DC: National Academy Press.
IOM. 1999b. Strategies to protect the health of deployed forces: Medical surveillance, record keeping, and risk reduction. Washington, DC: National Academy Press.
IOM. 1999c. Veterans and Agent Orange: Update 1998. Washington, DC: National Academy Press.
IOM. 2000a. The five series study: Mortality of military participants in U.S. nuclear weapons tests. Washington, DC: National Academy Press.
IOM. 2000b. Gulf War and health, volume 1: Depleted uranium, pyridostigmine bromide, sarin, vaccines. Washington, DC: National Academy Press.
IOM. 2000c. Protecting Those Who Serve: Strategies to Protect the Health of the Deployed U.S. Forces. Washington, DC: National Academy Press.
IOM. 2000d. Veterans and Agent Orange: Herbicide/dioxin exposure and type 2 diabetes. Washington, DC: National Academy Press.
IOM. 2001a. Gulf War veterans: Treating symptoms and syndromes. Washington, DC: National Academy Press.
IOM. 2001b. Veterans and Agent Orange: Update 2000. Washington, DC: National Academy Press.
IOM. 2002. Veterans and Agent Orange herbicide/dioxin exposure and acute myelogenous leukemia in the children of Vietnam veterans. Washington, DC: National Academy Press.
IOM. 2003a. Characterizing exposure of veterans to Agent Orange and other herbicides used in Vietnam: Interim findings and recommendations. Washington, DC: The National Academies Press.
IOM. 2003b. Characterizing exposure of veterans to Agent Orange and other herbicides used in Vietnam: Final Report. Washington, DC: The National Academies Press.
IOM. 2003c. Gulf War and health, volume 2: Insecticides and solvents. Washington, DC: The National Academies Press.
IOM. 2003d. Veterans and Agent Orange: Update 2002. Washington, DC: The National Academies Press
IOM. 2004a. Gulf War and health: Updated literature review of sarin. Washington, DC: The National Academies Press.
IOM. 2004b. Studies of U.S. veterans twins. http://www.iom.edu/CMS/3795/4907.aspx (accessed February 14, 2007).
IOM. 2004c. Veterans and Agent Orange: Length of presumptive period for association between exposure and respiratory cancer. Washington, DC: The National Academies Press.
IOM. 2005a. Gulf War and health, volume 3: Fuels, combustion products, and propellants. Washington, DC: The National Academies Press.
IOM. 2005b. Veterans and Agent Orange: Update 2004. Washington, DC: The National Academies Press.
IOM. 2006. Gulf War and health, volume 4: Health effects of serving in the Gulf War. Washington, DC: The National Academies Press.
IOM. 2007. Gulf War and health, volume 5: Infectious diseases. Washington, DC: The National Academies Press.
Janes, G. R., J. Goldberg, S. A. Eisen, and W. R. True. 1991. Reliability and validity of a combat exposure index for Vietnam era veterans. Journal of Clinical Psychology 47:80-86.
Kang, H. 2006 (July 27). VA health registries. Paper presented at the second meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
Keane, T. M., J. A. Fairbank, J. M. Caddell, R. T. Zimering, K. L. Taylor, and C. A. Mora. 1989. Clinical evaluation of a measure to assess combat exposure. Psychological Assessment 1:53-55.
Laufer, R. S., M. S. Gallops, and E. Frey-Wouters. 1984. War stress and trauma: The Vietnam veteran experience. Journal of Health and Social Behavior 25:65-85.
Long, E. R., and S. A. Jablon. 1955. Tuberculosis in the army of the United States in World War II. VA Medical Monograph. Washington, DC: U.S. Government Printing Office.
Lund, M., D. Foy, C. Sipprelle, and A. Strachan. 1984. The Combat Exposure Scale: A systematic assessment of trauma in the Vietnam War. Journal of Clinical Psychology 40:1323-1328.
The Millennium Cohort Study. 2007. http://www.millenniumcohort.org/about.php (accessed July 24, 2007).
Postlewaite, C. 2006. Overview: DoD deployment and installation-based occupational/ environmental health programs. Paper presented at the second meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC
Prins, A., P. Ouimette, R. Kimerling, R. P. Cameron, D. S. Hugelshofer, J. Shaw-Hegwer, A. Thrailkill, F. D. Gusman, and J. I. Sheikh. 2004. The primary care PTSD screen (PC–PTSD): Development and operating characteristics. Primary Care Psychiatry 9(1):9-14.
Robinette, C. D., S. Jablon, and T. L. Preston. 1985. Studies of participants in nuclear tests. Washington, DC: National Academy Press.
SMITREC (Serious Mental Illness Treatment Research and Evaluation Center). 2001. Care for veterans with psychosis in the VHA FY01: 3rd Annual National Psychosis Registry Report. Ann Arbor, MI: Serious Mental Illness Treatment Research and Evaluation Center, Health Services Research and Development Center of Excellence. http://www.hsrd.ann-arbor.med.va.gov/documents/3rdAn0nual_psychosisVHA.pdf (accessed April 6, 2007).
SMITREC. 2002. Specialty care for veterans with depression in the VHA: 2002 National Registry for Depression (NARDEP) Report. Ann Arbor, MI: Serious Mental Illness Treatment Research and Evaluation Center, Health Services Research and Development Center of Excellence. http://www.hsrd.ann-arbor.med.va.gov/documents/2002NARDEP.pdf (accessed April 6, 2007).
VA (Department of Veterans Affairs). 2003. Press release. VA begins registry for Lou Gehrig’s Disease. http://www.research.va.gov/news/press_releases/lou-gehrig-021803.cfm (accessed April 5, 2007).
VA. 2005a. Office of Research and Development Program announcement. Request for applications in combat casualty neurotrauma. http://www.research.va.gov/funding/solicitations/docs/neurotrauma.pdf (accessed April 5, 2007).
VA. 2005b. VA Form 10-10EZ. Application for health benefits. https://www.1010ez.med.va.gov/sec/vha/1010ez/Form/vha-10-10ez.pdf (accessed April 5, 2007).
VA. 2006a. Fact sheet: Facts about the Department of Veterans Affairs. Washington, DC: Department of Veterans Affairs. http://www1.va.gov/OPA/fact/docs/vafacts.pdf (accessed April 9, 2007).
VA. 2006b. Office of Research and Development Program announcement. Deployment health: OEF/OIF veteran research issues. http://www.research.va.gov/funding/solicitations/docs/Deployment_Health_2006.pdf (accessed April 5, 2007).
VA. 2006c. VA WRIISC-DC-Veterans Affairs War-Related Illness and Injury Study Center in Washington, DC. http://www.va.gov/WRIISC-DC/ (accessed April 5, 2007).
VA. 2007a. Federal benefits for veterans and dependents. Washington, DC: Department of Veterans Affairs. http://www1.va.gov/opa/vadocs/fedben.pdf (accessed April 5, 2007).
VA. 2007b. Seamless transition home. http://www.seamlesstransition.va.gov/ (accessed April 5, 2007).
VA. 2007c. Seattle Epidemiologic Research and Information Center. http://www.eric.seattle.med.va.gov/index.html (accessed April 6, 2007).
VA. 2007d. VA health care eligibility and enrollment: Getting care. http://www.va.gov/healtheligibility/gettingcare/ (accessed April 5, 2007).
VA. 2007e. Vietnam Era Twin Registry: Identification of Vietnam era veteran twins. http://www.eric.seattle.med.va.gov/VETR/identification_of_twins.html (accessed April 6, 2007).
Walker, A. E., and S. Jablon. 1961. A follow-up study of head wounds in World War II. VA Medical Monograph. Washington, DC: U.S. Government Printing Office.
Wessely, S., C. Unwin, M. Hotopf, L. Hull, K. Ismail, V. Nicolaou, and A. David. 2003. Stability of recall of military hazards over time. Evidence from the Persian Gulf War of 1991. British Journal of Psychiatry 183:314-322.
Yehuda, R., S. M. Southwick, and E. L. Giller, Jr. 1992. Exposure to atrocities and severity of chronic posttraumatic stress disorder in Vietnam combat veterans. American Journal of Psychiatry 149:333-336.
Zimmerman, M., and J. I. Mattia. 2001. The Psychiatric Diagnostic Screening Questionnaire: Development, reliability, and validity. Comprehensive Psychiatry 42(3):175-189.





























































