
12
The Way Forward
INTRODUCTION
In previous chapters of this report, the Committee examined and described Congress’ and the Department of Veterans Affairs’ (VA’s) past and present approaches to establishing presumptions. The case studies illustrate the application of the current approach, as well as approaches taken previously, and point to multiple points in the process of establishing presumptions that, in the Committee’s view, should be modified by its participants (Chapter 5). The Committee set out principles related to evidence evaluation and causal inference as a foundation for setting in place an approach that is as firmly grounded as possible in the relevant base of scientific evidence for particular exposures and health outcomes (Chapters 6-9). The Committee also addressed the task of more comprehensively tracking the exposures of those serving in the military and prospectively monitoring military personnel and veterans for disease occurrence so that the risks of exposures can be assessed more systematically (Chapter 10) and so that exposures subject to secrecy can be considered (Chapter 11).
Based on the case studies and other information that was gathered, the Committee has concluded that there is a basis for making changes to the present approach. Building on the conceptual foundation developed in these earlier chapters, the Committee addresses the second part of its charge in this chapter and recommends a framework for establishing presumptions in the future.
The Committee suggests that its recommended framework be considered as a model to guide the evolution from the current approach toward
that proposed by the Committee. The Committee recognizes that specific elements of its proposal (e.g., the call for carrying out exposure assessments and making exposure estimates) are not fully practicable for all relevant exposures at present and would take time to develop and implement. However, feasibility of specific elements of its proposal should be enhanced with future methodologic developments. The Committee believes that its approach can be applied to the full range of factors (e.g., chemical, biological, infectious, physical, and psychological) that may adversely affect the health of military personnel and veterans. The Committee does not intend that its approach be applied retrospectively to existing presumptions. The Committee is aware that policy or other concerns could lead Congress or VA to modify or even reject some of the Committee’s recommendations. Congress and VA may find alternative processes to achieve the overall objective of the Committee’s recommendations: an evidence-based approach to making presumptive disability decisions. However, the Committee suggests that its proposal will prove feasible and practical over time, that many of the elements in its proposal can and should be implemented without delay, and that the Committee’s proposal would significantly improve the presumptive disability decision-making process for veterans.
Out of necessity, the Committee also makes some recommendations related to the implementation of its proposed approach. The Committee makes specific recommendations with regard to proposed advisory and review committees that will likely require congressional authorization, and the Committee recommends that VA would need to make adjustments in its overall approach to the presumptive disability decision-making process in order to follow the Committee’s recommendations.
The Committee’s recommended approach (Figure 12-1) has multiple new elements: a process for proposing exposures and illnesses for review; a systematic evidence review process incorporating a new evidence classification scheme and quantification of the extent of disease attributable to an exposure; a transparent decision-making process by VA; and an organizational structure to support the process. In using the term “exposure,” the Committee defines exposure in a broad manner to include chemical, biological, infectious, physical and psychological stressors. We also call for a comprehensive approach to tracking exposures of military personnel and monitoring their health while in service and subsequent to service. The tracking should cover the full spectrum of exposures relevant to future risk for disease, including chemical, biological, infectious, physical and psychological stressors. The Committee’s recommendations are based in a framework that sets out this evidence-based process (Figure 12-1).
The proposed process includes the engagement of two panels: An Advisory Committee and a Science Review Board. The Advisory Committee would be advisory to VA and would consider proposals for the review
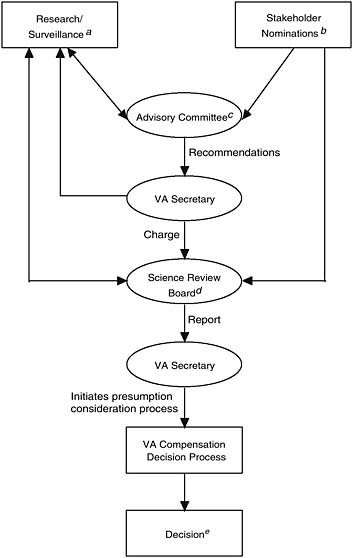
FIGURE 12-1 Proposed framework for future presumptive disability decision-making process for veterans.
a Includes research for classified or secret activities, exposures, etc.
b Includes veterans, veterans service organizations, federal agencies, scientists, general public, etc.
c This committee screens stakeholders’ proposals and research in support of evaluating evidence for presumptions and makes recommendations to the VA Secretary when full evidence review or additional research is appropriate.
d The board conducts a two-step evidence review process (see report text for further detail).
e Final presumptive disability compensation decisions are made by the Secretary, Department of Veterans Affairs, unless legislated by Congress.
of exposures and illnesses that might be the basis for presumptions and recommend to the VA Secretary exposures and illnesses needing further consideration. The Science Review Board, which would be independent from VA, would conduct a comprehensive evaluation of the evidence for causation and, if warranted by the level of evidence in support of causation, estimate the service-attributable fraction of disease.
The Committee calls for the implementation of a health and exposure surveillance system such that veterans’ health would be seamlessly tracked from entry into the service through retirement or separation and on to death. The resulting evidence on service-caused risks to health would be one critical component of the foundation of evidence for decision making, along with other sources of evidence, including studies of other populations, toxicologic studies, and other research. The accumulating evidence would undergo periodic review in a transparent and uniform fashion to gauge the strength of evidence in support of general causation and for determination of individual causation, drawing on the exposure data and perhaps other information. This review, carried out by the Science Review Board, would classify the strength of evidence for general causation in a standardized classification scheme as input into a compensation process by VA. VA, also deliberating in a transparent fashion based on established principles, would render a decision by the VA Secretary with regard to a presumption. The process includes a mechanism for stakeholders to propose exposures and illnesses for potential presumptions. These would be considered by the Advisory Committee.
GENERAL FRAMEWORK: THE ADVISORY COMMITTEE AND THE SCIENCE REVIEW BOARD
In the Committee’s view, a change in the processes for the entities involved in the presumptive disability decision-making process is needed. In its recommendations for Congress, the Committee proposes the creation of an Advisory Committee and a Science Review Board.
The Advisory Committee would serve as an advisory committee to VA and consider the wide range of exposures and illnesses that might be a basis for presumptions. It would also consider research needs and assist VA in strategic research planning. The Science Review Board (independent from VA) would evaluate the evidence for causation and, if warranted, estimate the attributable fraction of disease in veterans due to exposure.
The role of the Advisory Committee would be to gather suggestions from all stakeholders (i.e., veterans service organizations, veterans, scientists, policy makers, and others) regarding specific exposures and illnesses that might be considered for comprehensive evaluation as potential presumptions, and to recommend to the VA Secretary those exposures and
illnesses worthy of further consideration. This committee would also advise on research to be carried out by various entities.
The role of the Science Review Board would be to weigh the evidence on general causation of disease (including data from a wide range of sources) and to provide recommendations to the VA Secretary regarding presumptions. One critical element in the deliberations of the Science Review Board would be evidence from monitoring the veterans themselves. The health of military personnel should be seamlessly tracked from entry into the service through retirement or separation and on to death. This accumulating evidence would undergo periodic review by the Science Review Board in a transparent and consistent manner. The Science Review Board would also consider evidence from studies of nonveteran populations, toxicological studies, and basic science research. The Science Review Board would provide VA with input for its presumptive decisions, including a summary report of the available scientific evidence in a standardized classification scheme. VA would then render its decision with regard to a presumption through a transparent process of deliberation for potential compensation.
PRINCIPLES FOR THE PRESUMPTIVE DISABILITY DECISION-MAKING PROCESS FOR VETERANS
This section describes the principles that should be incorporated into this process at every level. VA’s decision to make a presumption may involve weighing difficult and incomplete scientific evidence, in the context of veterans’ concerns and society’s obligations to the affected veterans as well as potential costs. Although the potential complexity of the presumptive disability decision-making process may make a complete codification difficult, the underlying principles can be clearly expressed.
Our country has long recognized that veterans make great sacrifices through their service, including being willing to risk their lives in combat. Historically, presumptions established by Congress and VA have acknowledged the special responsibilities of the government to injured veterans. Recent military conflicts have brought new concerns that extend beyond combat injury and that reflect the potential for delayed adverse consequences of complex combat exposures from chemical, biological, infectious, physical, and psychological stressors. The principles underlying presumptive disability decision making are critical for its success, and consequently the Committee calls for Congress and VA to affirm certain principles that underlie decision making around presumptions. The Committee recommends the following six principles as such a foundation:
-
Stakeholder inclusiveness
-
Evidence-based decisions
-
Transparency
-
Flexibility
-
Consistency
-
Causation, not just association, as the target for decision making
Each of these principles is discussed in detail below.
Stakeholder Inclusiveness
The Committee was impressed with the number of groups who expressed intense interest in the Committee’s deliberations and in this report. The Committee’s meetings were attended by representatives of veterans service organizations and by individual veterans. Optimal decision making has to include input from such stakeholders who will be affected by the process. Veterans and their families already have some input to VA through the political process. However, the Committee sees a need for more active solicitation of stakeholder input, not just into decisions on specific presumptions but more generally with regard to VA’s overall process for making presumptions. It is with this principle in mind that the Committee recommends the creation of the Advisory Committee, separate from but advisory to VA, to consider exposures and diseases for which comprehensive scientific evaluation and possible presumptions may be warranted. Among others, this entity should consult with: representatives of veterans service organizations; veterans; veterans’ families; medical personnel at VA who are engaged in the research, diagnosis, and treatment of conditions at issue; and personnel at the Department of Defense (DoD) who are knowledgeable about pertinent exposures and exposure data.
Evidence-Based Decisions
Over the last several decades, there has been a strong movement to ground clinical medicine and public health in an evidence-based framework for decision making. The systematic and consistent capture and analysis of all relevant evidence is central in this approach. Many previous IOM committees addressing scientific issues that would later be used by Congress or VA in establishing presumptions have followed structured approaches, typically evaluating all relevant observational studies on particular hazards faced by veterans and interpreting the findings in a broad biomedically grounded framework. However, while some of these reviews evaluated additional available toxicological or mechanistic evidence, they did not incorporate this evidence when reaching conclusions about the available scientific evidence for the relationship. The Committee recommends giving more consideration to toxicological investigation in general and to mecha-
nisms of action in particular. The overall presumptive disability decision-making process needs to be grounded in the full extent of the scientific evidence available.
Although previous IOM committees have appropriately considered all available epidemiologic evidence on veterans, both domestic and foreign, as well as relevant studies from civilian populations, the available studies may be limited for many agents. In spite of efforts over the years by VA, the Medical Follow-Up Agency at IOM, and other federal and non-federal organizations to address critical health matters for veterans, the array of studies and findings is lacking as a basis for establishing well-grounded scientific presumptive disability decisions for many health outcomes. With the principle of evidence-based decisions in mind, this Committee also recommends that veterans be more effectively monitored, both in their military exposures and in relevant health outcomes throughout their lifetimes.
Transparency
Transparency in decision making is critical to the perception of fairness. The Committee strongly recommends that more emphasis be put on assuring transparency at every stage of the presumptive disability decision-making process. There are multiple stakeholders concerned with every specific presumption, including veterans who are already ill, those potentially at risk of illness, veterans service organizations, and the general public. Transparency means that each step of decision making should have a clear and known basis; stakeholders should be able to fully understand how decisions about presumptions are made, and the basis for those decisions, with reference to documented details of the presumptive disability decision-making process. VA has expressed concern that transparency could compromise internal discussion and affect decision-making deliberations; any unanticipated, adverse consequences of transparency should be noted and implications considered.
Flexibility
Scientific evidence is not static, and it often is less than certain. Given that the scientific basis for presumptive decisions will change over time, the Committee recommends that VA should be able to adjust future decisions when such change is scientifically justified. This does not mean that the Committee recommends that benefits previously granted should be terminated. The Committee is aware that disabled veterans and their families are often dependent on such payments and that it could create a hardship to remove them, a matter that VA disability policy recognizes in other situations. There should be a process of ongoing data collection so that
relevant new findings are recognized and taken into account as quickly as possible. Differing approaches to assisting affected veterans might be used as evidence is accumulating. For example, when causation is very uncertain, a decision might be made by VA to award medical care to the veterans possibly harmed, leaving open the possibility of future financial compensation if the evidence strengthens over time.
Another aspect of flexibility is ongoing improvement of the decision-making process. At present, the Committee found little indication that VA assesses the performance of its own presumptive disability decision-making process or seeks to improve it. Even if VA were to adopt the decision-making structure recommended by the Committee (see Figure 12-1), it would also be necessary to set up mechanisms for evaluating VA’s internal process over time. The Committee recommends that VA establish ongoing monitoring and evaluation to allow the decision-making process to be refined and improved. An information-gathering process would be needed for this purpose; consideration might also be given to appointment of an external committee to provide independent guidance on quality improvement, or the Advisory Committee could provide this function.
For the short term, as a new approach is implemented, careful review and evaluation may be particularly critical. Consequently, Congress may choose to be involved in the assessment and change the process as well, particularly as there is a transition from the current approach to a new process.
Consistency
One lesson from the case studies is that there is no firm consistency in the basis for presumptive decisions, possibly contributing to a perception by some of arbitrariness in the presumptive disability decision-making process. VA has offered a description of its internal processes as they have evolved over the last 15 years with regard to the receipt and consideration of IOM’s Agent Orange and Gulf War reports. The materials from VA do not describe a standard protocol by which various internal groups respond to an IOM report. Although the Committee lacks full information on VA’s processes, the Committee was left with the impression that better structure and documentation of its approach are needed. The Committee recommends that VA take steps to ensure that the bases for its internal decision making are explicit and applied consistently from case to case. To achieve consistency, consideration should be given to procedures for each element of the process within VA: evidence review, decision making, and implementation. For some elements of the process, models are already available, as in the instance of previous IOM Agent Orange and Gulf War committees.
Causation, Not Just Association
One of the most critical matters, in the Committee’s view, is clarifying the basis for making a decision to compensate veterans for service-related disability. The Committee recommends that causation, not just association, should be the basis of presumptive compensation. The justification for this recommendation is provided below.
Presumptive disability decisions are based on two judgments: (1) that a group of veterans was exposed to a potentially harmful agent or condition during service, and (2) that the agent or condition is able to cause disease leading to disability. The second proposition states a causal association, and not merely an association for which causation has not been established. An association between an exposure and outcome can be good evidence for a causal claim, but it is not the same as a causal claim.
The history of presumptions for Agent Orange illustrates the need to be clear on this point. The Veterans’ Dioxin and Radiation Exposure Compensation Standards Act of 1984 (Public Law 98-542. 98th Cong., 2d Sess.) used language of both association and causation in describing the evidence required for presumptions. Initially, VA interpreted the law as requiring a certain threshold of evidence for causation, and as a result denied presumptions between Agent Orange and all diseases except chloracne. Veterans interpreted the intent of the law differently, and a district court sided with the veterans finding the Act ambiguous and interpreting congressional intent as establishing a threshold of evidence for an association (Nehmer v. United States Veterans’ Administration, 1989. Henderson, T. E. United States District Court for the Northern District of California Case Number C86-6160 TEH).
The Agent Orange Act of 1991 (Public Law 102-4. 102d Cong., 1st Sess.) led the VA to provide the following charge to IOM in making scientific determinations:
-
whether a statistical association with herbicide exposure exists, taking into account the strength of the scientific evidence and the appropriateness of the statistical and epidemiologic methods used to detect the association;
-
the increased risk of the disease among those exposed to herbicides during service in the Republic of Vietnam during the Vietnam era; and
-
whether there exists a plausible biological mechanism or other evidence of a causal relationship between herbicide exposure and the disease.
VA contracted with IOM to provide a biennial review of the scientific evidence, and VA provided each of the IOM Agent Orange committees (IOM, 1994, 1996, 1999, 2001, 2003b, 2005b) the 3-point charge con-
tained in the Agent Orange Act. IOM reports on Agent Orange (IOM, 1994, 1996, 1999, 2001, 2003b, 2005b) generally stated that the committees were unable to address the second point of their charge and did not use evidence from the third point of their charge to incorporate into the overall strength of evidence decision on association. The first IOM Agent Orange committee (IOM, 1994) established categories for the strength of evidence based on an association (sufficient, limited/suggestive, inadequate/insufficient, and no association) that have been used by subsequent IOM Agent Orange committees (IOM, 1996, 1999, 2000b, 2001, 2003b, 2005b).
Based in part upon IOM’s categorization of limited/suggested evidence of an association between exposure to Agent Orange and a specific health outcome—without scientific research on increased risk in exposed veterans (second point of charge), or robust evidence for a plausible biological mechanism (third point of charge), VA has presumptively service-connected several health outcomes to Agent Orange since 1994. In the example of type 2 diabetes, the scientific basis for the presumption was not evidence of a causal connection, but far more limited evidence of an association. Of course, the Committee recognizes that Congress and VA may choose to presumptively service-connect health outcomes for which the evidence for causation is weak; however, the basis for making such a decision should be made explicit.
In recommending a shift from association to causation as the underlying basis for compensation decisions, the Committee notes that such a shift would not necessarily raise the bar for establishing a presumption. It should be noted here that previous IOM committees reviewing mustard gas and lewisite (IOM, 1993) and the Gulf War (IOM, 2000a, 2003a, 2005a, 2006, 2007) each used a causal categorization in their reports. A more thorough consideration of mechanistic evidence of causation could actually reduce the need for evidence of an association. For example, in Gulf War and Health (IOM, 2003a, p. 330) IOM found that “there is inadequate/ insufficient evidence to determine whether an association exists between chronic exposure to benzene and myelodysplastic syndromes” in veterans even though many toxicologists and hematologists view the overall evidence as strongly supportive of a causal relationship in rodents.
The Committee recommends a scheme for the classification of evidence for causation in the following section.
STRUCTURE AND ACTIVITIES OF THE PRESUMPTIVE DISABILITY DECISION-MAKING PROCESS
The Committee proposes a transparent, public process through which diseases or health conditions potentially caused or aggravated by military service and the putative causal agents (e.g., chemical, biological, infectious,
physical, and psychological stressors) would be nominated for review and, given sufficient information and numbers of veterans affected, formally evaluated to determine if the evidence for causality supports consideration of presumptive service connection by VA. The process would be fully transparent and the outcomes of the evaluation made available in a timely manner.
The Committee recommends that Congress create an Advisory Committee to VA. This Advisory Committee would be composed of scientific experts and veterans’ representatives who would identify and recommend to the VA Secretary health conditions and agents (i.e., chemical, biological, infectious, physical, and psychological stressors) for referral to and comprehensive evaluation by the independent Science Review Board. In turn, the Science Review Board’s findings and report would be provided to the VA Secretary for consideration in establishing presumptive compensation decisions.
The Advisory Committee
An Advisory Committee, chartered by Congress, is needed to identify potential exposures during military service, and related disabilities caused by these exposures, and to refer these topics for comprehensive review to the Science Review Board. This permanent committee would receive proposals for review, screen the available scientific information and research, and give priority to proposals based on the nature and extent of evidence supporting the relationship. The Advisory Committee would be composed of veterans’ representatives and recognized and credible experts in relevant fields, for example epidemiology, industrial hygiene, toxicology, occupational medicine, public health, military surveillance and databases, and exposure assessment. The Advisory Committee would be supported by VA and other federal staff with appropriate backgrounds and expertise to assist the committee. The Advisory Committee would review the initial assessment, give priorities, and make recommendations for proceeding with the full, comprehensive scientific review to the VA Secretary. The VA Secretary would have the authority to select conditions and agents for comprehensive scientific review by the Science Review Board.
Open Proposal Process
Health conditions and causative agents or circumstances would be proposed for review based on evidence of a connection between the condition and military service, and evidence that a sizable or well-defined group of veterans is likely to be affected. Concerns as to the need for a presumption might arise from the health surveillance of veterans or active military
personnel, laboratory research discoveries, or findings from occupational studies of exposures and health effects (e.g., by the International Agency for Research on Cancer [see Chapter 8]). Proposals from any source on behalf of affected veterans (e.g., veterans, veterans’ families, veterans service organizations, VA, DoD, other governmental bodies, researchers, or the general public) would be accepted. Proposals along with supporting information would be tracked and evaluated on a scheduled basis.
Screening of Proposals
An initial review of the evidence would be performed by professional VA staff in support of the Advisory Committee. The purpose of the screen would be to determine whether there is a minimum amount of evidence suggesting that the condition could have been caused or aggravated by military service, or of military exposure to the putative causal agent, and also to gauge the extent and nature of the evidence supporting the proposal. The process of proposal review would be structured to be responsive to stakeholders of varying expertise and capabilities, and include the gathering of additional evidence beyond that submitted with the proposal.
Prioritization
Those exposures found to, at a minimum, have some positive evidence of a relationship to health conditions and adequate data to initiate review would be candidates for full evaluation. Higher priority would be given to the conditions and causative agents or circumstances with the strongest evidence, affecting the largest numbers of veterans, and leading to the most severe health consequences.
Advisory Committee Review
The Advisory Committee would review materials assembled by the VA staff and other input from stakeholders and the general public to make recommendations to the VA Secretary for full, comprehensive scientific review by the Science Review Board. The process used by the Advisory Committee, which would be subject to the Federal Advisory Committee Act, and the rationale for recommendations would be documented and transparent. The process would also provide opportunities for input by stakeholders during the Advisory Committee’s review of proposals. To assist the Advisory Committee in developing recommendations, it is important that VA improve its data collection processes to track claims filed by veterans for benefits so that environmental exposure issues connected with new claims can be identified quickly.
The VA Secretary
Ultimately, the decision regarding which topics deserve full, comprehensive scientific evaluation resides with VA. VA would take the Advisory Committee recommendations under advisement, and consider the nature and extent of evidence, number of veterans potentially affected, severity of the conditions, public comment, and potentially other factors to decide the topics that would proceed to the Science Review Board for full, comprehensive scientific evaluation. Transparency at this stage by VA is critical. The VA Secretary would be required to respond to the Advisory Committee’s recommendations, providing an explanation for his or her decisions, a copy of which would be filed with Congress on an annual basis.
In the Committee’s proposed presumptive disability decision-making process, VA would receive the full, comprehensive scientific evaluation, as described below, from the Science Review Board. We recommend that VA establish a uniform and transparent process for making decisions with regard to presumptions following receipt of such evidence reviews. The process should incorporate the principles embodied in this Committee’s proposed approach. VA procedures should be established with input from the many concerned stakeholders. Its protocols should acknowledge who would be accountable for considering the reports of the Science Review Board and a description of how the reports would be used. A clear and comprehensive evidence-based rationale should be offered for all decisions and made public.
Science Review Board
For the process of comprehensive scientific review of the evidence to be successful, it must be regarded as credible by veterans, the general public, and the scientific community. It is essential that the process be objective, transparent, and of the highest scientific quality, reflecting scientific consensus among acknowledged experts at the time of the review. The Science Review Board is envisioned as following a transparently operated, adequately funded and staffed process in which outside experts, with various disciplinary backgrounds serving as needed, would conduct the full, comprehensive scientific evaluation. Rereview of cases would be conducted as new evidence would emerge, and further research would be encouraged when important hypotheses are unresolved by the available scientific evidence.
An independent Science Review Board would be authorized by Congress and funded by VA. The group would have expertise in the key disciplines needed to weigh the causal evidence and determine the service-attributable fraction. Ad hoc members could be added when specialized expertise was needed or issues of secrecy would need to be addressed. Members of the
Science Review Board would serve as independent experts, and without conflicts of interest. The Science Review Board would be housed in an organization or institution that would ensure its credibility, its sustained growth, and consistent efforts and products.
A staff of professionals with expertise in relevant disciplines would be needed to support the Science Review Board. Staff would seek out and compile relevant information, solicit input from outside organizations, and assist in report writing and in developing and finalizing recommendations from the Science Review Board.
Public and Other Requests for Relevant Data
VA would publicly announce in the Federal Register the health conditions and putative causal agents that would undergo full, comprehensive scientific review by the Science Review Board. In the initial preparations for the evidence review, a request for information on the evidence for and against causal relationship for the particular condition and agent or circumstance would be announced, for example in the Federal Register and on VA’s website. Relevant data may also be requested from DoD, organizations within VA, or other knowledgeable organizations, by project staff or the Science Review Board.
Two-Step Process of Evidence Utilization
The Committee recommends a two-step process for evaluation of scientific evidence by the Science Review Board. Step one would involve a systematic review of relevant data to determine the strength of evidence for causation, using one of four categories as presented in Chapter 8:
-
Sufficient: The evidence is sufficient to conclude that a causal relationship exists.
-
Equipoise and Above: The evidence is sufficient to conclude that a causal relationship is at least as likely as not, but not sufficient to conclude that a causal relationship exists.
-
Below Equipoise: The evidence is not sufficient to conclude that a causal relationship is at least as likely as not, or is not sufficient to make a scientifically informed judgment.
-
Against: The evidence suggests the lack of a causal relationship.
The scientific review would include all relevant evidence using existing systematic review models. The Science Review Board would develop standard operating procedures, which would be reviewed and updated on a regular basis, and outline the protocol by which evidence would be
reviewed and categorized. The evidence gathered and reviewed would be similar in nature to that supporting cancer or reproductive toxicity evaluations by the National Toxicology Program’s Center for the Evaluation of Risks to Human Reproduction, the National Toxicology Program’s Report on Carcinogens, the International Agency for Research on Cancer, and the U.S. Environmental Protection Agency. The public and stakeholders would be encouraged to provide input into the scientific review process.
If the evidence for causation were categorized as Sufficient or at Equipoise and Above, then we anticipate that VA would consider a presumptive service connection based upon causal evidence categorization and the service-attributable fraction if available (to be estimated in the second step of the process, described below). As is current VA policy, if the evidence is at Equipoise, the benefit of the doubt would be given to the veteran, and a presumptive service connection would be considered. If the evidence were categorized as Against, then we anticipate that VA would not consider a presumptive service connection. If, however, the evidence were categorized as Below Equipoise, then we anticipate that VA would, after carefully considering the prospects and recommendations for future research, decide on an appropriate time frame for the subsequent scientific review of the evidence, with the expectation that the evidence would then be sufficient to resolve matters either for or against the causal claim at that time. Such information would be considered by the Advisory Committee serving in its capacity as overseer of the overall process and advisor to the VA Secretary.
If the VA Secretary were to decide that a presumption would not be established for evidence categorized as Below Equipoise or, for other reasons, for evidence categorized as Equipoise and Above, then during the period of further evidence development and gathering and prior to the subsequent scientific review of the evidence, VA should consider providing some support to potentially affected veterans, such as providing provisional access to medical care.
As evidence accumulates, the balance might move to strengthen or to weaken the case for causality. Importantly, the Science Review Board should be free to upgrade the level of evidence, to downgrade the level of evidence, or to leave it as the same categorization. For evidence that has reached the classification of Sufficient, we would not anticipate a potential lowering of the classification, if the original determination was correctly made and based on sound scientific evidence.
If the strength of the evidence reaches Sufficient or Equipoise and Above, then the evaluation would move to step two, the calculation of the service-attributable fraction of disease when required information and data are available. This calculation is independent of the classification of the strength of evidence for causation, and the magnitude of the service-attributable fraction is not considered in the application of the four-level
schema for categorizing evidence. Rather, the service-attributable fraction would be of value for decision making, giving an understanding of the scope of the population to be covered by a presumption.
In step two, the Science Review Board would consider the extent of exposure among veterans and subgroups of veterans, as well as dose-response relationships. When such information is available, the board would estimate the service-attributable fraction and its related uncertainty. The purpose of step two is to convey the impact of the exposure on veterans as a whole for the purpose of decision making and planning, but not to serve inappropriately as an estimate of probability of causation for individuals. Some exposures may contribute greatly to the disease burden of veterans, while other exposures (even with a known causal effect) may have a small impact overall. This additional information would be useful to VA in its decision making as to whether a presumption should be made for the veteran population in general, for subgroups, or not at all. When service-attributable fraction data are not available, the VA may consider presumptions on the information contained in step one.
Periodic Reevaluation of Evidence
All but the most conclusive evaluations would be subject to rereview and updating. Rereviews could follow a fixed cycle, for example every 5, 7, or 10 years. Rereview and updating could also be triggered by new compelling scientific information, in which case outside parties could make nominations to the Advisory Committee for reconsideration by the Science Review Board.
EXAMPLE OF APPLICATION IN CURRENT CONFLICTS
The Committee’s framework is intended for prospective application during peace- and wartime and for in-garrison exposures as well as those experienced in wartime theatres. The potential utility of the recommended approach might be considered by applying it retrospectively to the case studies or prospectively to the current conflicts in Iraq and Afghanistan. For the purposes of this hypothetical illustration we use the current conflicts, although in establishing the framework we drew on lessons learned from the case studies regarding such matters as secrecy (e.g., mustard gas and lewisite), lack of ongoing epidemiological surveillance (e.g., cardiovascular disease in amputees), and insufficient exposure information (e.g., Agent Orange and Gulf War in 1990).
With regard to the current military actions in Iraq and Afghanistan, the conflicts have been marked by the hostility of the environments with ubiquitous threats to military personnel and widespread use of improvised
explosive devices (IEDs) bringing risk of maiming and death. The level of psychological stress has increased risk for posttraumatic stress disorder (PTSD) and the IEDs have led to high rates of limb loss and traumatic brain injury (TBI). Additionally, many of the deployed personnel are in the National Guard and Reserves and have faced unexpected disruption of their civilian lives from one or several deployments during the course of the current conflicts.
How might a full implementation of the Committee’s proposed framework prove useful for the purpose of presumptive disability decision making for veterans of the current conflicts in Iraq and Afghanistan? We call for systematic and ongoing exposure assessment that would extend beyond chemical, biological, and physical stressors to psychological stress; with suitable instruments, exposures to stress would be estimated among samples of various at-risk groups of individuals, as the basis for future observation for onset of PTSD or other disorders in relation to exposure. For chemical exposures, industrial hygiene approaches could also be used for exposed groups of individuals, again as the basis for assigning exposures to various groups. Stored blood samples from pre- and post-deployment examinations could also be used to indicate and assess exposures to chemical agents, to assess immune responses to infectious agents, or to measure other biomarkers of exposure or of injury. For all deployed personnel, geographic location and duties could serve as the basis for assigning potential exposures to groups of individuals.
Information on future disease risks in relation to exposure could be obtained through follow-up via health status and exposure data records linkage to VA, DoD, and other data systems, including the National Health Index for mortality. Special cohorts (e.g., registries) could be constructed to identify and track particular exposed groups with greater intensity and focused outcome assessment. Service members with TBI should be identified and tracked, for example, for level of functioning and quality of life. Risk for PTSD might be monitored in groups with greater and lesser levels of stress.
A general consequence of the Committee’s approach would be continuous monitoring of health outcomes among those who had been deployed to the zones of current conflict in Iraq and Afghanistan. Comparison of disease risks in those deployed to those not deployed in these areas could signal any potential increased risk and lead to more focused assessment and review of exposure and health outcomes concerns, including review by the Advisory Committee.
In the event that the Advisory Committee determined that an evidence evaluation was needed, the Science Review Board would be able to use the findings of the exposure and health tracking system. Evidence would be available directly from the tracking of veterans that would be
included in the review along with other relevant information. If indicated by the classification of strength of evidence, the service-attributable fraction should be estimable. The size of the exposed, and hence eligible, pool of veterans would be known with some degree of certainty. The evidence review conducted by the Science Review Board would be reported back to VA, so that the VA Secretary could make a determination as to whether a service-connection presumption would be established. These activities would follow the transparent process laid out by the Committee, possibly increasing confidence in the decisions made.
SECRECY AND THE PRESUMPTIVE DISABILITY DECISION-MAKING PROCESS
Research involving individuals exposed to chemical, biological, or radiological agents is often classified for security reasons, and information related to clandestine missions is also classified. This classification can be detrimental to the long-term health status of our veterans, who maintain the oath of secrecy. So long as information remains classified—which can be for a long period of time—these veterans cannot openly investigate or inquire about the relationships between their disease or health condition and the exposures they received. Although secrecy must be applied and maintained for obvious homeland security and national defense reasons, this designation must not be used to deny or forestall necessary medical treatment for afflicted individuals. As made clear by the case study of mustard gas and lewisite (see Appendix I), veterans may be harmed by exposures from classified activities. It is absolutely necessary for DoD and VA to develop, implement, and maintain a policy program that addresses the issues of health maintenance and national security for our veterans. The case study of mustard gas and lewisite illustrates the opportunity for harm to occur in research volunteers because of secrecy (see Appendix I).
Regarding the processes for science review proposed here, review would be particularly challenging when classified or secret information is involved. Nonetheless, the Committee recommends that DoD and VA develop a process for ensuring that exposures sustained in the course of classified or secret activities are not excluded from the presumptive disability decision-making process. Our Committee can make only general comments on this matter. For some issues involving classified and secret information, consultants with appropriate expertise and security clearance might be added to the Advisory Committee and Science Review Board. They could review the classified or secret information and provide information or recommendations for the decision process in a format that would not violate the government’s need for secrecy. This variation in process would be clearly and openly described.
Perhaps in some circumstances, no element of the relationship between military exposure and the condition could be divulged. This circumstance would call for a separate special process to protect government secrecy as well as provide fair treatment for affected veterans.
ADDITIONAL DATA FOR DECISION MAKING
To make the best possible decisions regarding compensation for veterans, it is necessary to go beyond the published literature. In this section we will consider several sources of data that would greatly enhance the presumptive disability decision-making process for veterans.
At present, research on the health of veterans is conducted in a variety of venues. Examples include the following:
-
Intramural research of the War-Related Illness and Injury Study Center assesses the health consequences of deployment to a combat theater.
-
The Medical Follow-Up Agency of IOM’s Board on Military and Veterans Health carries out targeted epidemiologic research on health of military personnel.
-
Extramural research related to the health of veterans may be funded by VA through its extramural research program or by the National Institutes of Health.
Although investigators at the War-Related Illness and Injury Study Center have a track record of productivity, the Committee anticipates that substantial additional capacity for multidisciplinary research will be needed as better surveillance methods are put into place and new hypotheses are generated.
The approach to research should be driven by a sustained and iterative planning process that strategically identifies and addresses emerging questions. Issues needing investigation might be identified through surveillance findings, stakeholder input, or findings emerging in research conducted beyond VA. VA needs a process that strategically addresses research needs to ensure that presumptions are evidence-based to the best extent possible. In the Committee’s recommendations, we call for an Advisory Committee that would provide guidance to VA in developing and maintaining a targeted and strategic research planning process. The reviews carried out by the Science Review Board would also highlight gaps that need to be addressed through research.
REFERENCES
IOM (Institution of Medicine). 1993. Veterans at risk: The health effects of mustard gas and lewisite. Washington, DC: National Academy Press.
IOM. 1994. Veterans and Agent Orange: Health effects of herbicides used in Vietnam. Washington, DC: National Academy Press.
IOM. 1996. Veterans and Agent Orange: Update 1996. Washington, DC: National Academy Press.
IOM. 1999. Veterans and Agent Orange: Update 1998. Washington, DC: National Academy Press.
IOM. 2000a. Gulf War and health, volume 1: Depleted uranium, pyridostigmine bromide, sarin, vaccines. Washington, DC: National Academy Press.
IOM. 2000b. Veterans and Agent Orange: Herbicide/dioxin exposure and type 2 diabetes. Washington, DC: National Academy Press.
IOM. 2001. Veterans and Agent Orange: Update 2000. Washington, DC: National Academy Press.
IOM. 2003a. Gulf War and health, volume 2: Insecticides and solvents. Washington, DC: The National Academies Press.
IOM. 2003b. Veterans and Agent Orange: Update 2002. Washington, DC: The National Academies Press.
IOM. 2005a. Gulf War and health, volume 3: Fuels, combustion products, and propellants. Washington, DC: The National Academies Press.
IOM. 2005b. Veterans and Agent Orange: Update 2004. Washington, DC: The National Academies Press.
IOM. 2006. Gulf War and health, volume 4: Health effects of serving in the Gulf War. Washington, DC: The National Academies Press.
IOM. 2007. Gulf War and health, volume 5: Infectious diseases. Washington, DC: The National Academies Press.




















