
3
The Presumptive Disability Decision-Making Process
This chapter describes the current presumptive disability decision-making process for veterans and outlines the roles of various participants in the process. The description is based on presentations at the Committee’s open sessions, public documents, documents provided by the Department of Veterans Affairs (VA), the Institute of Medicine (IOM) reports, and other relevant materials.
SUMMARY OF THE PROCESS
The current presumptive disability decision-making process for veterans involves multiple parties and is not controlled by any single entity or organization. The process involves input from Congress, VA, the National Academies (IOM and National Research Council [NRC]) and the veteran community. Decisions made in the courts have also influenced the current presumptive process. Figure 3-1 depicts roles of participants in the current process. Although the number and extent of presumptions have varied over the last 80 years, it appears that the presumptive decisions established since the early 1990s have led to growing concerns and questions about the presumptive process itself.
When Congress enacted the Agent Orange Act of 1991 (Public Law 102-4. 102d Cong., 1st Sess.), it started a model for a decision-making process that is still in place today. Congress asked VA to contract with an independent organization—VA contracted with IOM—to review the scientific evidence related to Agent Orange and disease. The process begins with VA supplying a study charge to the IOM committee carrying out the review,
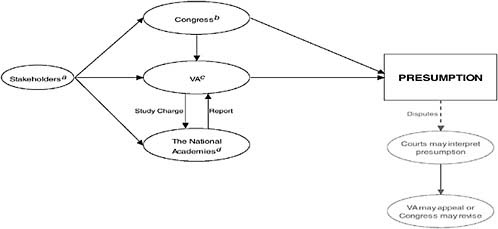
FIGURE 3-1 Roles of the participants involved in the presumptive disability decision-making process for veterans.
a Stakeholders include (but are not limited to) veterans service organizations (VSOs), veterans, advisory groups, federal agencies, and the general public; these stakeholders provide input into the presumptive process by communicating with Congress, VA, and independent organizations (e.g., the National Academies).
b Congress has created many presumptions itself; in 1921, Congress also empowered the VA Secretary to create regulatory presumptions; on several occasions in the past, Congress has directed VA to contract with an independent organization (e.g., the National Academies) to conduct studies and then use the organization’s report in its deliberations of granting or not granting regulatory presumptions.
c VA can establish regulatory presumptions; VA sometimes contracts with the National Academies to conduct studies and uses the organization’s report in its deliberations of granting or not granting regulatory presumptions.
d The National Academies (Institute of Medicine and National Research Council) submit reports to VA based on requests and study charges from VA.
and it ends with the IOM committee responding with a report, based on a comprehensive review, that addresses the charge. Since 1994, IOM has produced six biennial reports on Agent Orange (IOM, 1994, 1996, 1999, 2001, 2003b, 2005b) and five volumes on the Gulf War (IOM, 2000a, 2003a, 2005a, 2006b, 2007a) for VA to use in its deliberations when making presumptive decisions.
Through this process, health outcomes, such as prostate cancer and type 2 diabetes, have been presumptively service connected to Agent Orange exposure in Vietnam. The process for establishing presumptions continued to evolve in recent years to respond to veterans who were deployed to the Persian Gulf during or shortly following the Gulf War in 1990. Although the focus for presumptions among Vietnam veterans centered on their exposure and health outcomes relating to the dioxin-contaminated herbicide Agent Orange, the Gulf War has added new challenges caused by the multiple and various agents to which Service members were exposed. The IOM report process has responded to the multiplicity of agents of concern by developing reports on large groups of similar agents, such as combustion products (IOM, 2000a, 2003a, 2005a).This chapter reviews the roles of each major participant in the presumptive disability decision-making process for veterans.
DESCRIPTION OF ROLES FOR SPECIFIC PARTICIPANTS (IN ALPHABETICAL ORDER)
Role of Congress
The power to compensate veterans for their service-connected adverse health effects resides in Congress. Consequently, Congress has the power to create presumptions that make it easier for a veteran to establish service connection (see Chapter 2). Congress has sometimes exercised its power through legislation; at other times Congress has delegated its authority to the VA Secretary to prescribe “all rules and regulations … with respect to the nature and extent of proof and evidence and the method of taking and furnishing them in order to establish the right to benefits under such laws” (Rules and Regulations. 2003. 38 U.S.C. § 501(a); emphasis added). This general authority has been used sparingly by VA over the years to establish presumptions.
The vast majority of presumptions have resulted from public laws that specifically identify a disability or disease and set forth the conditions under which a presumption of service connection attaches (see Appendix F). Subsequent legislative enactments often modify the conditions under which these specific presumptions apply. As a matter of law, most presumptions can be rebutted by competent evidence (see Chapter 2) although this rarely occurs in practice.
Beginning in the 1980s, Congress has also legislated procedures to be employed in responding to service-related claims initially concerning herbicide and radiation exposures and later with respect to various exposures encountered during the Gulf War (see Appendix F). The procedures that Congress has established essentially involve review by a committee from the National Academies (e.g., IOM and NRC) of medical and scientific evidence concerning the relationship of disabilities or diseases to certain exposure agents. On a periodic basis, IOM furnishes findings for Agent Orange and Gulf War to the VA Secretary who must then decide whether or not to grant a presumption within a specified number of days of receipt of a report (Agent Orange Act of 1991. Public Law 102-4. 102d Cong., 1st Sess.; Veterans Programs Enhancement Act of 1998. Public Law 105-368. 105th Cong., 2d Sess.).
The formal role of Congress in establishing these presumptions follows a comparatively transparent process. Issues are brought to the attention of Congress by individual constituents seeking assistance from members in securing veteran benefits for which they claim entitlement, and by veteran service organizations (VSOs) that represent their interests. Media attention concerning veteran issues can also engage the interest of Congress. Finally, legislation concerning presumptions can also be initiated at the request of the executive branch, although this has been a rare occurrence.
A bill to establish a presumption is introduced in one or both houses of Congress, and it is usually accompanied by the sponsors’ floor statements setting forth the reasons why it should be enacted. Public hearings are held by one or both of the veterans affairs committees and testimony is received from a variety of witnesses including VSOs and individual veterans who are often constituents of various committee members. VA’s position on the legislation along with cost estimates prepared by the Director of the Congressional Budget Office, where applicable, are also received and considered by Congress (Johnson, 2003).
The Veterans Affairs Committee considering the legislation next moves to consider the legislation and amendments thereto in executive session. At one time these meetings were closed to the public, but they have been conducted in open session for approximately the past 30 years. After consideration of any amendments, the measure, if approved by the committee, is ordered to the floor for consideration by the entire Senate or House. The bill as amended is accompanied by a report prepared by the committee’s majority staff that sets forth the rationale for the legislation. The report also includes a summary of testimony received and information considered together with the administration’s position and cost estimates (Johnson, 2003). The report may also include separate and minority views, although this has been infrequent with veterans legislation that is more often than not reported unanimously.
Floor debate on the pending bill is televised and transcribed in the Congressional Record. Procedures for considering legislation on the floor, however, differ substantially between the House and the Senate. The amount of debate and the ability to consider amendments to the measure on the floor of the House is for the most part limited, which enhances the authority of the House Committee on Veterans Affairs. In the Senate the ability to attach amendments and to have extensive debate is rarely constricted (Johnson, 2003). Because of the frequent need to keep the “trains moving on time,” an individual Senator need not be a member of the Veterans Affairs Committee to exercise considerable influence in shaping veterans legislation.
It should be observed parenthetically that historically the House Veterans Affairs Committee has been the initiator of most veterans legislation. This resulted from the fact that until 1971 only the House had a full standing committee on veterans affairs. The Committee enjoyed a stable, “tenured” leadership and staff for long periods of time that enabled it to develop considerable expertise in veterans’ matters. Given House floor procedures, committee views were rarely challenged and invariably prevailed (Carr, 2001). In the Senate, by contrast, veterans legislation—depending on its content—was handled either by the Committee on Finance or the Committee on Labor and Public Welfare (SOURCE: http://veterans.senate.gov/index.cfm?FuseAction=About.CommitteeHistory), both of which had numerous other issues that engaged the committee members’ time and interest. As a result, the Senate frequently deferred to the position of the House in veterans’ matters prior to 1971.
The creation of the Senate Committee on Veterans Affairs in 1971 amid concern generated about treatment of returning Vietnam veterans altered the status quo as the Senate developed a larger voice in veterans’ matters (SOURCE: http://veterans.senate.gov/index.cfm?FuseAction=About.CommitteeHistory). This contributed to changes in how presumptions were created as the issue of Agent Orange exposure grew in intensity.
In situations where the two houses have not adopted identical measures, the differences need to be resolved often through a formal House-Senate conference committee. The veterans affairs committees, however, rarely resort to the formal conference committee process. Instead they negotiate their differences in informal, nonpublic meetings that frequently involve committee staff acting as surrogates for the members. Once agreement is reached, an amended version is reported to the floor of either the House or the Senate where it is passed and sent to the other body, which accepts the measure as amended causing it to be transmitted to the President for action. Both committees insert an identical joint explanatory statement in the Congressional Record that sets forth the changes made and the parties’ understanding and rationale of the compromise measure (Johnson, 2003).
As this description of the congressional process indicates, an extensive public record is developed with respect to the consideration and adoption of presumptions. Whether this record is a complete and accurate description of why a presumption was or was not adopted or why processes or standards were crafted in the manner they were is another matter. The politics of an issue often are not openly acknowledged in the public record. The personal views of key individual members can often have enormous weight. “Horse trading” on other matters often affects the shape and outcome of a particular bill. Moreover, substantive differences are sometimes papered over with ambiguous language to gain approval of the legislation, which presents a variety of problems to those who are charged with implementing their provisions. All of this suggests that the science justifying a presumption is but one factor considered by Congress in the enactment of the legislation. For additional information and analysis of the role of Congress in the development of presumptions, the reader is directed to the case studies, in particular the discussion of Agent Orange and Gulf War presumptions, found in Appendix I.
Congressional Perspective
The Committee received views from a panel of former congressional staff members, most of whom had served on either the Senate or the House Veterans Affairs committees in the 1980s and 1990s at a time when there were intense concern and questions about the effect of service exposures on the subsequent health of veterans (presentations made to the Committee on October 5, 2006). Among the factors arguably affecting the enactment of presumption legislation were (1) increasing concern about federal budget problems, (2) the perceived strength of key members of Congress considering the legislation, and (3) the continuing reminder of American Service members who had been recently killed or wounded and the debt our society owed them (Petrou, 2006; Ryan, 2006; Scott, 2006; Yoder, 2006).
It was observed that “scientific integrity is critical” in the presumptive disability compensation process and that if it was “lacking, the quality of the decisions [would] suffer, and veterans and the American people [would] lose faith in the decision-making process” (Petrou, 2006, p. 8). At the same time, faced with the claims of veterans with many real disabilities and diseases, it was acknowledged that presumptive decisions were shaped by the perceived “need to make ‘yes or no’ decisions in the face of pervasive uncertainty” with regards to the level, if any, of exposure and the likely health effects resulting therefrom (Yoder, 2006, p. 1). Panel members were critical of insufficient efforts to monitor the health of Service members. They noted the absence of predeployment health assessments and inadequate surveillance of environmental exposures that troops may have encountered
during the Gulf War notwithstanding lessons that should have been learned from Agent Orange and Vietnam (Petrou, 2006; Ryan, 2006; Scott, 2006; Yoder, 2006). Although there was disagreement as to its wisdom, there was uniform agreement that if a connection between exposure and disease were established, Congress has a strong bias in favor of compensating all veterans even if the attributable risk was small and large numbers of false positives would result (Petrou, 2006; Ryan, 2006; Scott, 2006; Yoder, 2006).
Role of Department of Veterans Affairs (VA)
The Committee’s description of the VA process is based on presentations to the Committee as well as a general description provided by VA (see Appendix G). The Committee requested internal documents related to specific presumptions, but these were not provided (see Chapter 1). Based on the information available, the Committee found that VA has developed an ad hoc process for establishing presumptions that relies upon National Academies (e.g., IOM and NRC) reports, recommendations of advisory committees, and VA research findings (Barrans, 2006; Pamperin, 2006a). Currently, VA follows the process that began with the Agent Orange Act of 1991 (Public Law 102-4. 102d Cong., 1st Sess.). Upon receipt of an IOM Veterans and Agent Orange (VAO) or Gulf War (GW) report, the VA Secretary is required to determine whether a presumption of service connection is warranted for any diseases discussed in the report.
VA has not adopted formal procedures governing its internal review and utilization of findings of IOM reports. However, a general practice has developed that VA usually follows in conducting its internal review. The general practice involves a three-tiered review with a working group (tier 1), a task force group (tier 2), and the VA Secretary (tier 3). Working group members include internal VA staff and outside experts as needed, with the option of seeking input from VSOs, Congress, and veterans (Deyton, 2006). Representatives at each tier are shown in Box 3-1.
The Working Group convenes after receiving the briefing from the IOM VAO or GW committee. “Prior to the meeting, VHA personnel usually will seek to identify, based on the IOM report and the committee briefing, the diseases that may warrant special consideration because IOM’s findings with respect to those diseases appear to be potentially significant. The … VHA generally provides the working group members with additional information concerning those diseases, including copies of any significant scientific studies identified in the IOM report and other information…” (VA, 2006, p. 3; as found in Appendix G).
“At the initial working group meeting, the OGC [Office of the General Counsel] representative briefs the working group on the legal standard governing the VA Secretary’s decision…. The working group will try to
|
BOX 3-1 Representatives at Each Tier of VA’s Internal Review of NAS Reports Tier 1: Working Group Representatives*
Tier 2: Task Force Representatives**
Tier 3: The VA Secretary SOURCE: Deyton, 2006; VA, 2006; as found in Appendix G. |
reach consensus as to whether the scientific evidence appears to warrant a presumption of service connection for any diseases under the applicable legal standard” (VA, 2006, p. 3; as found in Appendix G).
“If the Working Group concludes that the scientific evidence and legal standard do not provide a clear basis for recommending for or against establishing a presumption … the Working Group generally will agree to set forth a range of options for a decision by VA policy-making officials. In those circumstances, the Working Group will discuss the factors that preclude a clear recommendation, which may include ambiguity in the governing statutory standard as applied to certain IOM findings…. The Working Group will discuss the options available to the VA Secretary and may also
discuss the factors that may be relevant to the VA Secretary’s decision among those options” (VA, 2006, pp. 3-4; as found in Appendix G). The Working Group prepares a written report that typically includes the following:
-
A summary of the issues to be decided under applicable law and the IOM report
-
A summary of the findings contained in the IOM report
-
A summary of the legal standard governing VA’s decision
-
A summary of the Working Group’s analysis of the medical evidence in relation to the legal standard, particularly with respect to any potentially significant findings in the IOM report
-
A statement of the Working Group’s recommendations or of the options identified by the Working Group
In arriving at such recommendations, the Working Group generally does not prepare or obtain a cost estimate for the options. However, it may provide general information, for example, the prevalence rates of certain diseases under consideration. If the Working Group report lists a range of options available to the VA Secretary, it ordinarily would identify the scientific and legal considerations relevant to the VA Secretary’s choice among those options, and may also identify policy implications associated with various options” (VA, 2006, p. 4; as found in Appendix G).
The VA task force receives this report and reviews its recommendations. “The Task Force often, though not always, provides a separate report to the VA Secretary that is … usually similar to the Working Group’s report in format and content…. [O]nce the report is drafted, it is circulated to the Task Force members for signature and is then transmitted to the VA Secretary” (VA, 2006, p. 4; as found in Appendix G).
“Based on the Task Force’s report, the VA Secretary determines whether to establish presumptions for any diseases discussed in the IOM report and directs appropriate action to implement the decision…. [I]f the VA Secretary determines that a presumption of service connection is warranted for any disease, VBA (through the C&P Service staff) will prepare proposed rules to establish such presumptions” and “an estimate of the costs associated with the rule…. VA will transmit the proposed rule and cost estimate to OMB [Office of Management and Budget] for review. If OMB approves the proposed rule, it will be transmitted to the VA Secretary for signature. VA will then transmit the rule to the Federal Register for publication. Once the period for providing public comments on the rule has ended, VBA will prepare a final rule. VA will submit the final rule to the Federal Register for publication” (VA, 2006, p. 5; as found in Appendix G).
“If the VA Secretary determines that a presumption of service connection is not warranted for certain diseases, VBA will prepare a notice
explaining the scientific basis for that decision with respect to each such disease prior to publication” (VA, 2006, p. 5; as found in Appendix G). VA then publishes this notice in the Federal Register.
Presentations made at Committee open session meetings brought out several issues of importance to VA. The scientific, independent review process, as well as the breadth and thoroughness of IOM reports, provide credibility to the presumptive disability decision-making process. However, interpretation of the IOM reports can be problematic for VA. The difficulty lies not only in determining the effects of exposure but in separating the effects of a specific exposure of concern from the effects of other potential exposures. Past IOM committees have not been charged to provide guidance on this issue. VA is also hindered by not having exposure data for individuals. VA noted that some exposures known to contribute to conditions of concern are common in nonmilitary settings, complicating interpretation of studies of risks of military exposures for these outcomes.
VA, under statutes outlining the presumptive process for Agent Orange and Gulf War (Agent Orange Act of 1991. Public Law 102-4. 102d Cong., 1st Sess.; Veterans Programs Enhancement Act of 1998. Public Law 105-368. 105th Cong., 2d Sess.), is not required to consider any evidence on exposure magnitude that would be necessary for a direct service connection. It can offer little or no guidance for making decisions based on exposure magnitude or duration. VA is left to treat all exposures as equally likely to lead to an associated long-term health effect (Brown, 2006; Deyton, 2006).
The Impact of Presumptions
VA does not track the number of presumptive service-connected disability claims granted and/or denied for each condition, nor are health outcomes within the VBA data systems coded in a manner that would permit VA to easily determine how many veterans are presumptively service connected (as stated in Pamperin, 2006b). For various categories of health conditions, some information regarding the number of presumptions may be determined. That is, if it is clear that the only or most readily anticipated method for connection is via presumption (and not direct service connection), then one may conclude that the number of cases for various categories of health conditions are presumptively service connected (Pamperin, 2006b). The Committee was unable to obtain additional data on the number of presumptive cases or their impact to the overall VA system. Table 3-1 provides data that were provided to the Committee during its first open session meeting (Pamperin, 2006b).
Because disability cases adjudicated on the bases of presumptive decisions are not routinely counted, the costs are not known with certainty.
TABLE 3-1 Presumptions in VA’s Disability Program
|
Condition |
Number of Veterans |
Disability Severity Rating |
|
Chronic Diseases |
|
|
|
Arteriosclerosis |
Unknown |
Not differentiated |
|
Arthritis |
Unknown |
Same |
|
Leukemia |
Unknown |
Same |
|
Raynaud’s disease |
Unknown |
Same |
|
Tropical Diseases |
|
|
|
Malaria |
30,000 |
0% |
|
Leishmaniasis |
283 |
0% |
|
Dysentery |
872 |
0% |
|
Plague |
10 |
0% |
|
Prisoners of War |
|
|
|
Any anxiety |
Unknown |
Most rated 100% |
|
Stroke and its complications |
Unknown |
100% |
|
Cirrhosis of the liver |
Unknown |
100% |
|
Peripheral neuropathy |
Unknown |
100% |
|
Radiation |
|
|
|
Lung cancer |
Unknown |
Not differentiated |
|
Colon cancer |
Unknown |
Same |
|
Lymphomas |
Unknown |
Same |
|
Stomach cancer |
Unknown |
Same |
|
Herbicide Agents |
|
|
|
Type II diabetes |
197,000 |
Most are 10% and 20% |
|
Prostate cancer |
30,000 |
1/3 at 100%, average 40% |
|
Respiratory cancer |
5,000 |
Half at 100% |
|
Non-Hodgkin’s and Hodgkin’s |
5,000 |
Half at 100%, balance 50% |
|
Gulf War |
|
|
|
Undiagnosed illness |
3,259 |
Typically a 10% evaluation |
|
SOURCE: Pamperin, 2006b. |
||
However, estimates are made. VA estimated administrative costs for presumptive radiation decisions (bone, brain, colon, lung, and ovarian cancers) as $33,934,297 over 10 years with benefit costs of $768,601,698 over that same time period (McLenachen, 2005, slide 8). Estimated administrative costs for type 2 diabetes from 2001 through 2005 were $62 million with estimated benefit costs of $3.3 billion during that same time period. VA estimated that there would be 20,399 new type 2 diabetes awards in the first year and 179,000 over the next 5 years. The estimates did not include retroactive payments (McLenachen, 2005, slide 12). Today, the most frequent disability for which Vietnam veterans are receiving service-connected compensation is type 2 diabetes (VBA, 2006, p. 34). “At end of fiscal year
2006, nearly 248,000 veterans were service-connected for diabetes. More than 215,000 of these awards were based upon herbicide exposure in Vietnam” (VA, 2007, pp. 6B-13).
Role of Institute of Medicine (IOM)
The National Academies is a private, nonprofit, and independent entity that advises the nation on science, engineering, and health matters (NAS, 2007a). The IOM is one of four entities within the National Academies. The other entities are the National Academy of Sciences, which was created by Congress during Abraham Lincoln’s presidency, the National Academy of Engineering, and the National Research Council.
The National Academies convenes committees of its own members and “other experts to address the scientific and technical aspects of society’s most pressing problems” (NAS, 2007b, p. 2). All committee members serve without pay. Committee members are screened to ensure that they do not have conflicts of interest. The committees include “experts with the specific expertise and experience needed to address the study’s statement of task” (NAS, 2007b, p. 3).
The National Academies use a systematic study process. Study committees typically gather information through “(1) meetings that are open to the public and that are announced in advance through the National Academies’ Web site; (2) the submission of information by outside parties; (3) reviews of scientific literature; and (4) the investigations of the committee members and staff” (NAS, 2007b, pp. 5-6).
Committee deliberations are closed to the public and sponsors in order to “develop draft findings and recommendations free from outside influence…. All analyses and drafts of the report remain confidential” (NAS, 2007b, p. 6). A rigorous external peer review by a separate group of volunteer experts is undertaken prior to completion of the study. The National Academies are responsible for the final products and their public release. For additional information on the National Academies and the committee process, see http://nationalacademies.org/.
IOM Perspective
The Committee heard from IOM staff about how studies requested by VA were conducted over several decades (Martinez, 2006). On each occasion that VA has asked IOM to conduct a new study for Agent Orange or the Gulf War in support of a possible presumption, a new committee was selected and convened. Each committee had access to the publically available information regarding the work of previous IOM committees but interpreted their statement of task independent of prior committees.
As a result, each committee’s operating assumptions and study plans were similar but not fully identical to those of prior committees. They were free to construct their own evidence criteria and ways to weigh the individual research studies that they considered (see Appendixes H-1 and H-2 for IOM Agent Orange and Gulf War committee study charges).
IOM has completed six full, biennial Veterans and Agent Orange (VAO) reviews (IOM, 1994, 1996, 1999, 2001, 2003b, 2005b) and three focused (IOM, 2000b, 2004b, 2006a) Agent Orange reviews (see Appendix H-1). A new VAO update report was recently published (IOM, 2007b); this VAO report was being drafted simultaneously and independently of this report. Each of the VAO committees was composed of experts with diverse backgrounds to address their charge. Because of the unique nature of the Agent Orange biennial reviews, some consistency of membership for subsequent reviews across committees has been sustained. As a result, approximately one-third of each VAO committee’s members had served on a previous committee and were familiar with the past literature on Agent Orange. This overlap of membership helped to provide historical perspective and some consistency throughout the review process.
The IOM committees have been faced with significant challenges, including
-
few directly applicable epidemiologic studies;
-
no contemporaneous exposure measurements;
-
uncertainty about which veterans were exposed to which agents;
-
multiple, possibly synergistic exposures;
-
possible long latency for health effects from some agents; and
-
significant confounders. (Martinez, 2006, slides 7-8)
Source reference material includes epidemiologic studies (e.g., occupational, environmental, veterans) and toxicologic studies (e.g., animal health effects, cellular-level mechanistic).
The first IOM VAO committee categorized the strength of the evidence available into the following four categories: “(1) sufficient evidence of an association, (2) limited/suggestive evidence of an association, (3) inadequate/ insufficient evidence to determine whether an association exists, and (4) limited/suggestive evidence of no association” (IOM, 1994, pp. 6-7). Although there have been minor changes to the characterization of these categories over the past 15 years, each of the committees has continued to categorize evidence in this manner (IOM, 1996, 1999, 2001, 2003b, 2005b; see also Appendix H-3).
The committees carrying out the Gulf War (GW) studies requested by VA have approached their task somewhat differently. Similar to the process outlined for Agent Orange, VA requested IOM to “conduct a study
to evaluate the published scientific literature concerning the association between the agents to which the Gulf War veterans may have been exposed and adverse health effects” (IOM, 2000a, p. 2). The first IOM Gulf War committee began its work in January 1999 and identified an initial list of compounds of greatest concern to veterans. Two public laws (Veterans Programs Enhancement Act of 1998. Public Law 105-368. 105th Cong., 2d Sess.; Making Omnibus Consolidated and Emergency Appropriations for the Fiscal Year Ending September 30, 1999, and for other Purposes. 1998. Public Law 105-277. 105th Cong., 2d Sess.) mandated further studies.
The first IOM Gulf War and Health Study committee decided to categorize strength of evidence into the following five categories: (1) sufficient evidence of a causal relationship, (2) sufficient evidence of an association, (3) limited/suggestive evidence of an association, (4) inadequate/insufficient evidence to determine whether an association does or does not exist, and (5) limited/suggestive evidence of no association (IOM, 2000a, pp. 4-5). Although there have been minor language changes to these categories or description of these categories, the individual, stand-alone committees have continued to categorize evidence in this manner (IOM, 2003a, 2004a, 2005a, 2006b, 2007a; see also Appendix H-4). As in the case of the Agent Orange committees, there has been some overlap of committee membership in the Gulf War series. However, the nature of the individual Gulf War reports and specific statements of task have required less overlap of membership and increased the need for more specific scientific expertise and background in the various areas of biological, chemical, and infectious agents depending upon the specific charge to the committee.
These Agent Orange and Gulf War examples show important similarities and differences relevant to the overall presumptive process. Of note, Agent Orange reports by IOM did not explicitly include a causal category in the evaluation, whereas Gulf War reports did include a category of evidence sufficient to infer causation when characterizing the strength of evidence available for all agents evaluated. Consideration of the actual exposure potential for veterans was beyond the charges to the committees.
The statements of task and conclusions from each of the Agent Orange and Gulf War reports may be found in Appendix H.
Role of Veterans Service Organizations (VSOs)
There are numerous VSOs that voice their members’ concerns. VSOs and their advisory committees have played an important role in the evaluations and actions of Congress, VA, and the National Academies (e.g., IOM and NRC). There are also special veteran advisory groups, such as the Advisory Committee on Former POWs, with direct access to the VA Secretary. The impact and voices of the veteran community can be very
powerful. A review of the “Agent Orange Update,” which describes some of the actions and influence VSOs and other organizations had in moving the Agent Orange Act forward (Cranston, 1990), provides insight into the role VSOs played in that specific congressional action.
The Committee received extremely helpful and diverse input from representatives of VSOs and individual veterans who attended open session committee meetings or who prepared written material to provide to the Committee for its consideration.
Veterans Perspective
The Committee heard that VSOs struggle with how scientific evidence that is uncertain and sometimes limited is used in evaluating cause and effect relationships. The VSO representatives wanted to make certain not only that the Committee considered past conflicts and practices but also that the Committee took into account what is occurring in today’s environment and what future veterans may be facing, including emerging problems such as traumatic brain injuries, a signature wound of the current Gulf conflict (Sullivan, 2006).
Other issues raised included better data collection on exposures and health status during military service, the use of International Classification of Diseases codes for illness and injuries, and seamless transition to VA after discharge. The importance of collecting data for reservists and National Guard members identical to those serving active duty was emphasized (Sullivan, 2006).
The Committee repeatedly heard from representatives of VSOs and individual veterans that they expect a fair, equitable, and scientifically based system for establishing presumptions (Kinderman, 2006; Overstreet, 2006; Selfon, 2006). However, the Committee was also cautioned that more rigorous application of tests for cause and effect may not serve the process well (Violante, 2006).
Each of the VSOs reaffirmed the responsibility and commitment to care for all men and women who have served in our stead—past, present, and future. Each stakeholder brings an important perspective to the presumptive disability decision-making process for veterans. There are clearly factors other than science that are considered in these decisions especially when the science base is weak or absent. The future framework will seek to identify ways to improve information and the methods needed to make the best possible presumptive decisions.
REFERENCES
Barrans, D. 2006. History of presumptions of service connection. Paper presented at the first meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
Brown, M. 2006. The role of science in Department of Veterans Affairs disability compensation policies for environmental and occupational illness and injuries. Paper presented at the first meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
Carr, T. P. 2001. CRS report for Congress. Parliamentary reference sources: House of Representatives. CRS report RL30787. Washington, DC: Congressional Research Service. http://lugar.senate.gov/CRS%20reports/Parliamentary_Reference_Sources_House.pdf (accessed April 30, 2007).
Cranston, A. 1990. Agent Orange update. Senate Congressional Record 101st Cong., 2nd Sess. November 2. Presented by Scott, E. P., at the third meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, San Antonio, TX.
Deyton, L. 2006. Introduction to VA health care system and assessing environmental/ occupational exposures. Paper presented at the second meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
IOM (Institute of Medicine). 1994. Veterans and Agent Orange: Health effects of herbicides used in Vietnam. Washington, DC: National Academy Press.
IOM. 1996. Veterans and Agent Orange: Update 1996. Washington, DC: National Academy Press.
IOM. 1999. Veterans and Agent Orange: Update 1998. Washington, DC: National Academy Press.
IOM. 2000a. Gulf War and health, volume 1: Depleted uranium, pyridostigmine bromide, sarin, and vaccines. Washington, DC: National Academy Press.
IOM. 2000b. Veterans and Agent Orange: Herbicide/dioxin exposure and type 2 diabetes. Washington, DC: National Academy Press.
IOM. 2001. Veterans and Agent Orange: Update 2000. Washington, DC: National Academy Press.
IOM. 2003a. Gulf War and health, volume 2: Insecticides and solvents. Washington, DC: The National Academies Press.
IOM. 2003b. Veterans and Agent Orange: Update 2002. Washington, DC: The National Academies Press.
IOM. 2004a. Gulf War and health: Updated literature review of sarin. Washington, DC: The National Academies Press.
IOM. 2004b. Veterans and Agent Orange: Length of presumptive period for association between exposure and respiratory cancer. Washington, DC: The National Academies Press.
IOM. 2005a. Gulf War and health, volume 3: Fuels, combustion products, and propellants. Washington, DC: The National Academies Press.
IOM. 2005b. Veterans and Agent Orange: Update 2004. Washington, DC: The National Academies Press.
IOM. 2006a. Disposition of the Air Force Health Study. Washington, DC: The National Academies Press.
IOM. 2006b. Gulf War and health, volume 4: Health effects of serving in the Gulf War. Washington, DC: The National Academies Press.
IOM. 2007a. Gulf War and health, volume 5: Infectious diseases. Washington, DC: The National Academies Press.
IOM. 2007b. Veterans and Agent Orange: Update 2006. Washington, DC: The National Academies Press
Johnson, C. W. 2003. How our laws are made, revised and updated. Washington, DC: Government Printing Office. http://www.senate.gov/reference/resources/ pdf/howourlawsaremade.pdf (accessed May 7, 2007).
Kinderman, Q. 2006. Statement presented at the second meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans. Washington, DC.
Martinez, R. 2006. Institute of Medicine: Agent Orange and Gulf War studies. Presented at the second meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
McLenachen, D. 2005. Presumptive service connection in VBA. Presented to Veterans’ Disability Benefits Commission, Washington, DC.
NAS (The National Academies). 2007a. The National Academies: Advisors to the nation on science, engineering, and medicine. http://www.nationalacademies.org/ (accessed May 9, 2007).
NAS. 2007b. The National Academies study process: Ensuring independent, objective advice. http://www.nationalacademies.org/studycommitteprocess.pdf (accessed May 9, 2007).
Overstreet, H. G. 2006. Statement presented at the third meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans. San Antonio, TX.
Pamperin, T. J. 2006a. An overview of the disability benefits program and presumptions affecting veterans’ benefits. Paper presented at the first meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
Pamperin, T. J. 2006b. Presumptions in VA’s disability program—The effect. Paper presented at the first meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
Petrou, L. 2006. Statement presented at the third meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans. San Antonio, TX.
Ryan, P. 2006. Perspectives on veterans’ legislative disability presumptions. Paper presented at the third meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, San Antonio, TX.
Scott, E. P. 2006. Statement presented at the third meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, San Antonio, TX.
Selfon, L. J. 2006. Statement from the United Spinal Association presented at the second meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
Sullivan, P. 2006. Testimony presented at the third meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, San Antonio, TX.
VA (Department of Veterans Affairs). 2006. Internal VA process for reviewing reports of the IOM under the Agent Orange Act of 1991 and the Persian Gulf War Veterans Acts of 1998. Presented to the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
VA. 2007. Fiscal year 2008 budget submission. National cemetery administration, benefits program, and departmental administration. Vol. 2. Washington, DC: Department of Veterans Affairs. http://www.va.gov/budget/summary/ (accessed May 9, 2007).
VBA (Veterans Benefits Administration). 2006. Annual benefits report fiscal year 2005. Washington, DC: Department of Veterans Affairs.
Violante, J. A. 2006. Public comments for the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans. San Antonio, TX.
Yoder, C. 2006. Thoughts on presumptions of service-connection for veterans presumed to have been exposed to environmental hazards. Paper presented at the third meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, San Antonio, TX.


















