
Summary
INTRODUCTION
The United States has long recognized and honored military veterans’ service and sacrifices. Veterans injured by their service, becoming ill while in service, or having an illness after discharge as a long-term consequence of their service have been given healthcare coverage and disability compensation. As the complexity of exposures during combat has increased, the list of service-connected illnesses has grown. The Department of Veterans Affairs (VA) now provides disability compensation to approximately 2.6 million veterans for 7.7 million disabilities annually, expending approximately $24 billion for this purpose (VBA, 2006, pp. 19, 24, 27).
Disability compensation for military veterans requires that there be a service connection. A medical illness or injury that occurred while a member was in military service is considered service connected whether caused by or aggravated by an exposure or event during service or simply occurring coincidentally with military service. However, if a medical condition appears after the period of military service and it is presumed to be caused by or aggravated by an exposure or an event that occurred during military service, then veterans may receive compensation based on that presumption (Pamperin, 2006).
In making a decision to provide compensation, VA needs to determine whether the illness of concern can generally be caused by exposures received during service and whether the illness in a specific claimant was caused by the exposure. The answer to the general question of causality comes from a careful review of all available scientific information, while the answer
to the question of causation in a specific person hinges on knowledge of the exposure received by that individual and of other factors that may be relevant. If the scientific evidence is incomplete, there may be uncertainty on the question of causation generally; if there is limited or no information on exposure of individual claimants or if other factors also contribute to disease causation, there may be uncertainty on the question of individual causation.
To provide benefits to veterans in the face of these two broad types of uncertainty, Congress and VA make presumptive decisions that bridge gaps in the evidence related to causation and to exposure. Presumptions may relieve the veteran of persuading VA that the exposure produced the adverse health outcome and of proving that an exposure occurred during military service (Pamperin, 2006). Once a medical condition is service connected through presumptions, and the veteran can document military service consistent with having received the given exposure, the veteran only has to show the basic fact that he or she suffers from the condition in order to receive a disability payment and eligibility for medical care (Zeglin, 2006).
In 2004, Congress established the Veterans’ Disability Benefits Commission (the Commission), which was charged with “studying the benefits provided to compensate and assist veterans for disabilities attributable to military service” (VDBC, 2006, p. 1; as found in Appendix A). The Commission identified the presumptive disability decision-making process as a topic needing assessment and asked the Institute of Medicine (IOM) to establish a committee for this purpose that would be funded by VA. The resulting committee, the Committee on Evaluation of the Presumptive Disability Decision-Making Process for Veterans (the Committee), was given the following charge by VA:
-
Describe and evaluate the current model used to recognize diseases that are subject to service connection on a presumptive basis.
-
If appropriate, propose a scientific framework that would justify recognizing or not recognizing conditions as presumptive.
The Commission further elaborated the charge, asking the Committee to “help ensure that future veterans are granted service connection under a presumptive basis based on the best scientific evidence available” (VDBC, 2006, p. 4; as found in Appendix A). The Commission asked the Committee to “evaluate the current model used to determine diseases that qualify for service connection on a presumptive basis, and if appropriate, propose improvements in the model” (VDBC, 2006, p. 1; as found in Appendix A). The Commission emphasized that “having a method of granting service connection quickly and fairly based on a presumption is
of critical importance to our disabled veterans and their surviving spouses” and that “ensuring that future presumption processes reflect the then current medical knowledge about the causal relationship would benefit the entire veteran community” (VDBC, 2006, p. 4; as found in Appendix A). The Commission’s summary statement further commented that “[t]o the extent possible, suggestions that will avoid the necessity for many future presumptions by ensuring that exposure of service members is documented and scientific evidence is made available would be important” (VDBC, 2006, p. 4; as found in Appendix A).
IOM appointed a 14-member committee that covered the broad scientific and medical areas of general, occupational, and psychiatric medicine; biostatistics; epidemiology; toxicology; industrial hygiene; and exposure and risk assessment. The Committee’s members also brought expertise in law, philosophy, causal decision making, and policy as well as knowledge of the Department of Defense (DoD) and VA’s approach to disability compensation.
THE COMMITTEE’S APPROACH TO ITS CHARGE
In fulfilling its charge, the Committee first investigated and attempted to characterize Congress’ and VA’s recent approach to presumptive disability decision making, and then developed a conceptual framework for a new, more evidence-based process. It then constructed a way to move forward that builds on the framework and addresses deficiencies of the current process.
The Committee held three open meetings to gather information on the current presumptive disability decision-making process. The Committee heard from past and present congressional staff members, representatives of VA, DoD, IOM, various stakeholder groups (e.g., veteran service organizations [VSOs]) and the general public. Committee members also participated in conference calls with DoD experts on medical surveillance and exposure data collection and exposure assessment systems.
The Committee reviewed extensive background information including: documents provided by the Commission, public laws and supporting House and Senate reports, Federal Register notices, VA documents (e.g., cost estimates, a white paper on VA’s decision-making processes [found in Appendix G], and responses by VA to written questions from the Committee), DoD documents, and past IOM reports commissioned by DoD and VA. The Committee conducted 10 case study reviews—Mental Disorders’ Presumptions, Multiple Sclerosis Presumption, Prisoners of War Presumptions, Amputees and Cardiovascular Disease Presumption, Radiation Presumptions, Mustard Gas and Lewisite Presumptions, Gulf War Presumptions, Agent Orange and Prostate Cancer Presumption, Agent Orange and Type 2
Diabetes Presumption, and Spina Bifida Program (not a presumption but a VA program area)—that cover a wide variety of circumstances for which presumptions have been established by Congress and VA since 1921. The case studies were a foundation for the Committee’s efforts in understanding past practices of all participants in the presumptive disability decision-making process (see Appendix I).
The Committee also researched and considered capabilities and limitations of the exposure data and health outcome information available to DoD and VA for exposure assessment, surveillance, and research purposes. The Committee examined whether DoD and VA have a strategic research plan and vision for the necessary interface between the agencies, as well as with other, relevant research organizations.
The Committee considered the use of scientific evidence in guiding the process for making presumptive decisions that affect the compensation of veterans. Drawing upon the Committee members’ expertise in epidemiology, medicine, toxicology, biostatistics, and causal decision making, the Committee covered the evaluation of evidence for inferring association and causation as well as methods for quantifying the contribution of an agent to disease causation in populations and extending this quantification to individuals. Using this framework, the Committee developed an evidence-based approach for making future decisions with regard to presumptions.
THE PRESUMPTIVE DISABILITY DECISION-MAKING PROCESS FOR VETERANS
In 1921 Congress empowered the VA Administrator (now Secretary) to establish presumptions of service connection for veterans. Only Congress and the VA Secretary have the authority to establish presumptions. Over time, presumptions have been made to relieve veterans of the burden to prove that disability or illness was caused by a specific exposure that occurred during military service (e.g., Prisoners of War). Since 1921, nearly 150 health outcomes have been service connected on a presumptive basis (see Appendix F). In February 2006, Congress codified all regulatory presumptions that VA had put in place to that time.
The current presumptive disability decision-making process for veterans involves several steps and several organizations. The process involves input from many parties—Congress, VA, the National Academies, and stakeholders (e.g., VSOs, advisory committees, and individual veterans) (Figure S-1). Congress has made presumptions itself. In the current model, Congress or stakeholders acting through Congress may call on VA to assess whether a presumption is needed. The VA turns to IOM for completion of a review of the scientific evidence. The findings of that evaluation are consid-
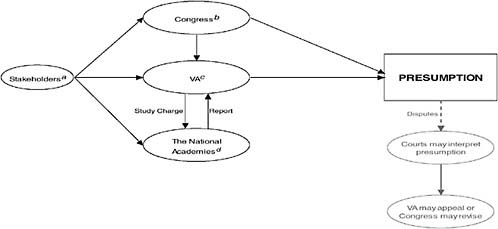
FIGURE S-1 Roles of the participants involved in the presumptive disability decision-making process for veterans.
a Stakeholders include (but are not limited to) veterans service organizations (VSOs), veterans, advisory groups, federal agencies, and the general public; these stakeholders provide input into the presumptive process by communicating with Congress, VA, and independent organizations (e.g., the National Academies).
b Congress has created many presumptions itself; in 1921, Congress also empowered the VA Secretary to create regulatory presumptions; on several occasions in the past, Congress has directed VA to contract with an independent organization (e.g., the National Academies) to conduct studies and then use the organization’s report in its deliberations of granting or not granting regulatory presumptions.
c VA can establish regulatory presumptions; VA sometimes contracts with the National Academies to conduct studies and uses the organization’s report in its deliberations of granting or not granting regulatory presumptions.
d The National Academies (Institute of Medicine and National Research Council) submit reports to VA based on requests and study charges from VA.
ered by VA in its presumptive disability decision-making process. Decisions made in the courts have also influenced the current presumptive process.
Three major legislative actions by Congress have influenced the recent presumptive decisions—the Radiation Exposed Veterans Compensation Act of 1988 (Public Law 100-321. 100th Cong., 2d Sess.), the Agent Orange Act of 1991 (Public Law 102-4. 102d Cong., 1st Sess.), and the Persian Gulf War Acts of 1995 (Veterans’ Benefits Improvement Act of 1994. Public Law 103-446. 103rd Cong., 2d Sess.) and 1998 (Making Omnibus Consolidated and Emergency Appropriations for the Fiscal Year Ending September 30, 1999, and for Other Purposes. Public Law 105-277. 105th Cong., 2d Sess.). The concept of “at least as likely as not” with regard to exposure potential was introduced for radiation exposures and its use has since been continued. The Agent Orange Act (Public Law 102-4. 102d Cong., 1st Sess.) grew out of events following the Vietnam War, and its language expresses substantial and significant elements of the presumptive story. The presumptions put in place by Congress for Gulf War illnesses represent the first time that Congress produced a list of health outcomes that it defined as “undiagnosed illnesses” (Veterans Education and Benefits Expansion Act of 2001. Public Law 107-103. 107th Cong., 1st Sess.).
When Congress enacted the Agent Orange Act of 1991 (Public Law 102-4. 102d Cong., 1st Sess.), it started a model for a decision-making process that is still in place. Congress asked VA to contract with an independent organization—VA contracted with IOM—to review the scientific evidence for Agent Orange. Since 1994, IOM has produced biennial reports on Agent Orange for VA to use as it considers making presumptive decisions (IOM, 1994, 1996, 1999, 2001, 2003b, 2005b). IOM has also delivered five volumes on the Gulf War (IOM, 2000a, 2003a, 2005a, 2006, 2007). Congress requires VA to respond after receiving an IOM report with a determination as to whether VA will make a service connection for particular health outcomes on a presumptive basis. VA has described its internal decision-making processes to the Committee in a general fashion, and the Committee has reviewed VA’s Federal Register notices and documents (see Chapter 3). However, it remains unclear to the Committee how VA makes particular determinations with regard to weighing strength of evidence for causation and exposure potential in making its presumptive decisions.
Analysis of the Agent Orange and Gulf War case studies (see Appendix I) shows important similarities and differences relevant to the overall presumptive process. One difference is that Agent Orange is a single product (actually a mixture of compounds that contains the contaminant dioxin), extensively researched for associated health outcomes, whereas the health consequences of the Gulf War are unlikely to be the result of any single agent. Military service men and women may have received a number of health-relevant exposures during service in the Persian Gulf, complicating the development of evidence reviews. For Agent Orange, there is one
exposure of concern and a more constrained set of health indicators. There have been some differences in approaches of Agent Orange and Gulf War committees. The IOM Agent Orange reports (IOM, 1994, 1996, 1999, 2001, 2003b, 2005b) did not explicitly include a causal category in their evaluations whereas recent Gulf War reports (IOM, 2000a, 2003a, 2005a, 2006, 2007) did include a category for evidence sufficient to infer causation when characterizing the strength of evidence for agents evaluated. For neither set of reports does VA describe in its Federal Register notices how it accounted for exposure potential or magnitude in making its presumptive decisions.
FINDINGS OF CASE STUDIES
The case studies offered a diverse set of lessons learned and indicated elements of the current process that need to be addressed. In carrying out the case studies, this Committee had the opportunity to retrospectively examine the work of IOM committees as they grappled with the challenge of using uncertain evidence and of VA staff as they used the findings of IOM committees to make decisions about presumptions. The case studies demonstrate that the process has acted to serve the interests of veterans in many instances. Congress and VA have repeatedly acted to maximize the sensitivity of presumptive decisions so as to assure that no veteran who might have been affected is denied compensation. On the other hand, in maximizing sensitivity of presumptive disability decision making, substantial numbers of veterans whose illnesses may or may not have been actually service related are nonetheless compensated. There are both financial and nonfinancial costs to such decisions.
The case studies illustrate the use of presumptions to cover gaps in evidence, gaps that exist in part because of lack of information on exposures received by military personnel and inadequate surveillance of veterans for service-related illnesses. Secrecy is a particularly troubling source of incomplete information, as illustrated by the veterans who participated in studies of mustard gas and lewisite. Research carried out directly on the health of veterans has proved useful in some instances, leading to a decision, for example, on granting disability compensation for cardiovascular disease in amputees. But the research has not been systematic, and in the example of cardiovascular disease in amputees no further evidence relevant to a presumption made in 1979 has been collected. Research on radiation risks in veterans has been severely constrained by a lack of dose information, and the studies on radiation-exposed veterans have not been highly informative.
Across the case studies, the Committee found variable approaches to synthesizing evidence on the health consequences of military service. The inferential target of scientific evidence reviews has not been consistent
and varied between causation (e.g., mustard gas and lewisite, Gulf War) and association alone (e.g., Agent Orange). The more recent IOM Agent Orange reports have emphasized findings of observational studies on association and interpretation that might have been enhanced by placing the findings within a biological framework strengthened by greater attention to other lines of evidence. In the Agent Orange case studies, the category “limited/suggestive” for classifying evidence for association has been used for a broad range of evidence from indicating the mere possibility of an association to showing that an association is possibly causal. The “limited/ suggestive” evidence of association—on which the VA’s presumptive decisions to compensate type 2 diabetes and prostate cancer were made—may be below the level of certainty needed to support causation absent strong mechanistic understanding or to meet the congressional language of “if the credible evidence for the association is equal to or outweighs the credible evidence against the association,” which the Committee refers to “at least as likely as not.”
Both prostate cancer and type 2 diabetes illustrate situations in which the contribution of military exposures should be assessed against a background of disease risk that has other strong determinants: age in the case of prostate cancer and family history and obesity in the case of type 2 diabetes, as indicated by the IOM committee in its report (IOM, 2000b). For both type 2 diabetes and prostate cancer, the magnitude of the relative risks observed for pesticide exposure implies that the contribution of military exposures is likely to be small in comparison to those of the other contributing factors. In such circumstances, an estimation of the proportion of cases attributable to military exposures could be helpful to the VA in considering whether or not to presumptively service-connect disabilities. The Committee recognizes that development of such estimations is a complicated process dependent on acquiring better exposure data, which may not be available for some period of time.
In the case studies, the Committee’s analyses were based on the very general information provided by VA about its internal decision-making processes. The case studies and VA’s decision to withhold documents related to specific decisions from the Committee did make clear, however, that these processes are not fully transparent. VA believes that access to predecisional documents by outside sources could stifle candid staff discussions on issues. Once IOM carries out its reviews and provides VA with reports documenting the extent of evidence available on associations, the internal processes of VA that follow are not fully open to scrutiny. This closed process could reduce trust of veterans in the presumptive disability decision-making process and may hinder efforts to optimize the use of scientific evidence. The Committee also found inconsistency in the decision-making process.
SCIENTIFIC FOUNDATION FOR PRESUMPTIVE DISABILITY DECISION MAKING
In developing a future approach for presumptive disability decision making, the Committee first gave extensive consideration to causal inference and the processes used to make causal judgments. In other words, the Committee considered how scientific evidence is used to determine if exposure causes some disease. These determinations are generally made by expert committees that examine all relevant evidence for strengths and weaknesses and then synthesize the evidence to make a summary judgment. The Committee defines “exposure” in a broad manner to include chemical, biological, infectious, physical, and psychological stressors. The Committee recognizes that psychological stressors may be particularly difficult to describe, let alone measure and quantify.
The Committee then considered the quantification of the contribution of a particular exposure to disease causation. This second issue addresses the question of how much of the observed disease in a group, in both absolute and relative terms, is caused by the exposure.
Provision of compensation to veterans on a presumptive basis, or to any other group that has been injured, requires a general decision as to whether the agent or exposure of concern has the potential to cause the condition or disease for which compensation is to be provided in at least some individuals, and a specific decision as to whether the agent or exposure has caused the condition or disease in a particular individual. The determination of causation in general is based in a review and evaluation of all relevant evidence including (1) data on exposures of military personnel during service; (2) evidence on risks for disease coming from observational (epidemiologic) studies of military personnel; (3) other relevant epidemiologic evidence, including findings from studies of nonmilitary populations exposed to the agent of interest or similar agents; and (4) findings relevant to plausibility from experimental and laboratory research. The determination of causation in a particular case is based first on the general determination as to whether the exposure can cause disease, then on information about the exposures of the individual being evaluated for compensation, and on any other relevant information about the individual.
The Committee considered the properties of a decision-making process, recognizing the possibility of two types of systematic errors: making a decision to compensate when the exposure has not caused the illness (false positive) and to not compensate when the exposure has actually caused the illness (false negative). The Committee recommends that any decision process consider the trade-off between these two errors and attempt to optimize both the sensitivity (i.e., minimize the false negatives) and the specificity (i.e., minimize the false positives). Generally, higher sensitivity
cannot be achieved without lower specificity. These errors have costs. False positive errors result in the expenditure of funds for cases of disease not caused by military service while false negative errors leave deserving veterans uncompensated. The appropriate balancing of these costs also needs consideration.
The Committee considered ways to classify evidence, reaching the conclusion that a broader and more inclusive evidence review process is needed. It found that IOM reviews could be enhanced if a broader array of epidemiologic and other evidence (e.g., animal and mechanistic data) was considered. The Committee also found that the target of inference had varied from causation (e.g., mustard gas and lewisite, Gulf War) to association (e.g., Agent Orange). Consequently, the Committee recommends that categories of evidence for reviews be established to make clear those relationships that are at least as likely as not to be causal. The Committee has concluded that a categorization of evidence is needed that gives a scientifically coherent rendering of the language employed by Congress in calling for review of available scientific evidence. The Committee proposes a four-level hierarchy that classifies the strength of evidence for causation, not just association, and that incorporates the concept of equipoise: that is, whether the weight of scientific evidence makes causation at least as likely as not in the judgment of the reviewing group.
The Committee also gave consideration to the quantification of the burden of disease attributable to an exposure. This quantification would be made to provide an evaluation of the numbers of veterans to be compensated, but it would not be a component of the evidence evaluation for causation. For the purpose of quantification, the attributable risk, termed the service-attributable fraction, can be calculated if the needed information is available on the relative risk of disease among exposed individuals. For those exposures meeting the necessary level of evidence for compensation, the Committee recommends that the service-attributable fraction should be estimated overall and for subgroups of veterans, perhaps grouped by level of exposure, if the requisite data are available. Until more complete exposure information becomes available in the future, such calculations may not be possible for all conditions for which presumptions are made.
COMMITTEE’S RECOMMENDED APPROACH FOR THE FUTURE
Overview
The Committee’s recommended approach for the future (Figure S-2) has multiple new elements: a process for proposing exposures and illnesses for review; a systematic evidence review process incorporating a new evidence classification scheme and quantification of the extent of disease
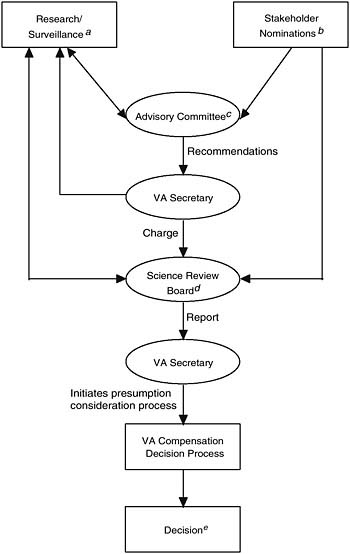
FIGURE S-2 Proposed framework for future presumptive disability decision-making process for veterans.
a Includes research for classified or secret activities, exposures, etc.
b Includes veterans, Veterans Service Organizations, federal agencies, scientists, general public, etc.
c This committee screens stakeholders’ proposals and research in support of evaluating evidence for presumptions and makes recommendations to the VA Secretary when full evidence review or additional research is appropriate.
dThe board conducts a two-step evidence review process (see report text for further detail).
e Final presumptive disability compensation decisions are made by the Secretary, Department of Veterans Affairs, unless legislated by Congress.
attributable to an exposure; a transparent decision-making process by VA; and an organizational structure to support the process. The Committee also calls for comprehensive tracking of exposures of military personnel and monitoring of their health while in service and subsequently.
Organizational Structure
The Committee recommends the creation by Congress of two new permanent boards: the Advisory Committee, serving in an advisory capacity to VA, and the Science Review Board (independent from VA). The Advisory Committee would consider the exposures and illnesses that might be a basis for presumptions and recommend to the VA Secretary exposures and illnesses needing further consideration. It would also consider research needs and assist VA with strategic research planning. The Science Review Board would evaluate the evidence for causation and, if warranted, estimate the service-attributable fraction of disease in veterans. One critical element in the deliberations of the Science Review Board would be evidence from monitoring the exposures and health of the veterans. The Science Review Board would provide VA with input for its presumptive decisions, including a summary report of the available scientific evidence in a standardized classification scheme.
Congress and VA may find alternative processes to achieve the overall objective of the Committee’s recommendations: an evidence-based approach to making presumptive disability decisions. The Committee recognizes that specific elements of its proposal (e.g., the call for carrying out exposure assessments and making exposure estimates) are not yet fully practicable and would take time to develop and implement. However, future methodologic developments should enhance the feasibility of some of the challenging elements of this proposal. The Committee believes that this proposal can significantly improve the presumptive disability decision-making process for veterans and, therefore, the process for implementing it should begin without delay.
Underlying Principles
VA’s decision to make a presumption may involve weighing difficult and incomplete scientific evidence, in the context of veterans’ concerns and society’s obligations to the affected veterans, and potential costs. Although the potential complexity of the decision-making process may make a complete codification difficult, the underlying principles can be clearly expressed. The Committee suggests the following six principles as a foundation for its proposed framework: (1) stakeholder inclusiveness; (2) evidence-based decisions; (3) transparent process; (4) flexibility; (5) consistency; and (6) using
causation, not just association, as the basis for decision making. Flexibility and consistency are not contradictory constructs here. Flexibility refers to the ability to be adaptable through time in evaluating scientific evidence, and consistency refers to being consistent in the process of evaluating evidence and making consistent decisions based on a comparable level of certainty based on the scientific evidence.
Proposals to Review for Potential Presumption
In this process, conditions and causative agents or circumstances would be proposed for review based on evidence of a connection between the condition and military service and evidence that a sizable or well-defined group of veterans is likely to be affected. The possibility of a need for a presumption might arise from surveillance of veterans or active military personnel, laboratory research discoveries, or findings from studies of exposed workers. The process would be open, with proposals accepted from any source (e.g., veterans, veterans’ families, VSOs, VA, DoD, other governmental bodies, researchers, the general public). Proposals accepted by the VA Secretary would be sent to the Science Review Board for full, comprehensive scientific evaluation.
Science Review Board
The Committee recommends a two-step process for scientific evaluation by the Science Review Board. The first step would involve a systematic review of all relevant data to decide the strength of evidence for causation, using one of four categories:
-
Sufficient: The evidence is sufficient to conclude that a causal relationship exists.
-
Equipoise and Above: The evidence is sufficient to conclude that a causal relationship is at least as likely as not, but not sufficient to conclude that a causal relationship exists.
-
Below Equipoise: The evidence is not sufficient to conclude that a causal relationship is at least as likely as not, or is not sufficient to make a scientifically informed judgment.
-
Against: The evidence suggests the lack of a causal relationship.
If the evidence for causation were categorized as Sufficient or at Equipoise and Above, then we anticipate that VA would consider a presumptive service connection based upon causal evidence categorization and its consideration of the service-attributable fraction if available (to be estimated in the second step of the process, described below). As is current VA policy,
if the evidence is at Equipoise, the benefit of the doubt would be given to the veteran. If the evidence were categorized as Against, then we anticipate that VA would not consider a presumptive service-connection. If, however, the evidence were categorized as Below Equipoise, then we anticipate that VA would, after carefully considering the prospects and recommendations for future research, decide on an appropriate time frame for the subsequent scientific review of the evidence, with the expectation that the evidence would then be sufficient to resolve matters either for or against the causal claim at that time. Such information would be considered by the Advisory Committee serving in its capacity as overseer of the overall process and advisor to the VA Secretary.
If the VA Secretary were to decide that a presumption would not be established for evidence categorized as Below Equipoise or, for other reasons, for evidence categorized as Equipoise and Above, then during the period of further evidence development and gathering and prior to the subsequent scientific review of the evidence, VA should consider providing some support to potentially affected veterans, such as providing provisional access to medical care.
As evidence accumulates, the balance might move to strengthen or to weaken the case for causality. Importantly, the Science Review Board should be free to upgrade the level of evidence, to downgrade the level of evidence, or to leave it as the same categorization. For evidence that has reached the classification of Sufficient, we would not anticipate a potential lowering of the classification, if the original determination was correctly made and based on sound scientific evidence.
If the strength of the evidence reaches Sufficient or Equipoise and Above, then the evaluation would move to step two, the calculation of the service-attributable fraction of disease when required data and information are available. This calculation is independent of the classification of the strength of evidence for causation, and the magnitude of the service-attributable fraction is not considered in the application of the four-level schema for categorizing evidence. Rather, the service-attributable fraction would be of value for decision making, giving an understanding of the scope of the population to be covered by a presumption.
In step two, the Science Review Board would consider the extent of exposure among veterans and subgroups of veterans, as well as dose-response relationships. When such information is available, the board would estimate the service-attributable fraction and its related uncertainty. The purpose of step two is to convey the impact of the exposure on veterans as a whole for the purpose of decision making and planning, but not to serve inappropriately as an estimate of probability of causation for individuals. Some exposures may contribute greatly to the disease burden of veterans, while other exposure (even with a known causal effect) may have
a small impact overall. This additional information would be useful to VA in its decision making as to whether a presumption should be made for the veteran population in general, for subgroups, or not at all. In the absence of service-attributable fraction data, as will likely occur for many exposures over the short term, we assume the VA would consider presumptions on the information contained in step one.
Expanding the Evidence Base
In the Committee’s view, the best scientific decisions about presumptions can be made only with comprehensive exposure and health surveillance of military personnel. Data collection should begin on entry into the military and continue through discharge, and when harmful exposures are suspected surveillance should be extended indefinitely. Surveillance refers to the ongoing collection, analysis, and use of data relevant to the health of a population. Elements of a surveillance system are already in place, but fall short of what is required. A fully functioning surveillance system would track military exposures and health outcomes, during military service and after discharge, and maintain a repository of data and biological specimens so that emerging and unanticipated questions could be retrospectively addressed. The system needs to be seamless in following military personnel, including National Guard and reservists, from active duty as they transition and become civilians.
This surveillance system should also track job and deployment history for each Service member through the period of service, with exposure assessment and monitoring for a range of job categories. Information on disease risk factors more generally could also be tracked. Use of personal biological samples for individual monitoring also holds promise.
Assessing exposures relevant to the neuropsychiatric disorders that are frequent among veterans of recent and current combats is particularly problematic. Documentation of stress is requisite to the diagnosis of posttraumatic stress disorder (PTSD), but approaches for capturing exposures to such stressors and to the circumstances of combat have not yet been developed and put into place. Research is needed for this purpose that builds on existing approaches so that data become available over the long-term.
In addition to surveillance, the Committee recommends an effort to coordinate and focus research on the health effects of military exposures. Associations identified in the surveillance data might need follow-up through more focused epidemiologic studies or exposure assessments. Toxicological research might be indicated to explore the mechanistic basis for an association between an exposure and a health condition.
VA Procedures
Ultimately, the decision regarding which proposed topics for potential presumptions deserve full evaluation resides with VA. In the Committee’s proposed process, VA also receives scientific input from the Science Review Board. We recommend that VA establish a uniform and transparent process for making decisions regarding presumptions following receipt of evidence reviews. VA should establish procedures with input from the many stakeholders, and a clear, evidence-based rationale should be offered for all decisions. The Committee’s recommendations are aimed at providing a sound scientific framework for the presumptive disability decision-making process. The Committee clearly recognizes that there are social, economic, political, and legal factors beyond the scope of scientific evidence that may influence the presumptive disability decision-making process for veterans and the presumptive decisions that are established by Congress and VA.
Scientific evidence is not static, and it often is less than certain. Given that the scientific basis for presumptive decisions will change over time, the Committee recommends that VA should be able to adjust future decisions when such change is scientifically justified. This does not mean that the Committee recommends that benefits previously granted should be terminated. The Committee is aware that disabled veterans and their families are often dependent on such payments and that it could create a hardship to remove them, a matter that VA disability policy recognizes in other situations.
SPECIFIC RECOMMENDATIONS
Based on its evaluation of the current process for establishing presumptive disability decisions and its consideration of alternatives, the Committee has specific recommendations for an approach that would build stronger scientific evidence into the decision-making process and, at the same time, be even more responsive and open to veterans. We propose a transformation of the current presumptive disability decision-making process. We recognize that considerable time would be needed to implement some of these recommendations as would additional investment to create systems needed to track exposures and health status of currently serving military service personnel and veterans. Progress depends on greater research capacity and improvements in the evaluation and utilization of scientific evidence in making compensation decisions. We find that there are elements of the current process that could be changed quickly and we recommend that VA consider prompt action as it moves toward implementation of a new approach. The recommendations that follow are based around the Committee’s proposed framework for making presumptive decisions. We list the recommendations in relation to the appropriate body.
Congress
Recommendation 1. Congress should create a formal advisory committee (Advisory Committee) to VA to consider and advise the VA Secretary on disability-related questions requiring scientific research and review to assist in the consideration of possible presumptions.
Recommendation 2. Congress should authorize a permanent independent review body (Science Review Board) operating with a well-defined process that will use evaluation criteria as outlined in this Committee’s recommendations to evaluate scientific evidence for VA’s use in considering future service-connected presumptions.
Department of Veterans Affairs
Recommendation 3. VA should develop and publish a formal process for consideration of disability presumptions that is uniform and transparent and clearly sets forth all evidence considered and the reasons for the decisions reached.
Science Review Board
The recommendations that follow are directed towards the proposed, future Science Review Board, the entity to be established in the Committee’s proposed approach.
Recommendation 4. The Committee recommends that the goal of the presumptive disability decision-making process be to ensure compensation for veterans whose diseases are caused by military service and that this goal must serve as the foundation for the work of the Science Review Board. The Committee recommends that the Science Review Board implement its proposed two-step process.
Recommendation 5. The Committee recommends that the Science Review Board use the proposed four-level classification scheme, as follows, in the first step of its evaluation. The Committee recommends that a standard be adopted for “causal effect” such that if there is at least as much evidence in favor of the exposure having a causal effect on the frequency or severity of disease as there is evidence against, then a service-connected presumption will be considered.
-
Sufficient: The evidence is sufficient to conclude that a causal relationship exists.
-
Equipoise and Above: The evidence is sufficient to conclude that a causal relationship is at least as likely as not, but not sufficient to conclude that a causal relationship exists.
-
Below Equipoise: The evidence is not sufficient to conclude that a causal relationship is at least as likely as not, or is not sufficient to make a scientifically informed judgment.
-
Against: The evidence suggests the lack of a causal relationship.
Recommendation 6. The Committee recommends that a broad spectrum of evidence, including epidemiologic, animal, and mechanistic data, be considered when evaluating causation.
Recommendation 7. When the causal evidence is at Equipoise and Above or Sufficient, the Committee recommends that an estimate also be made of the size of the causal effect among those exposed.
Recommendation 8. The Committee recommends that, as the second part of the two-step evaluation, the relative risk and exposure prevalence be used to estimate an attributable fraction for the disease in the military setting (i.e., service-attributable fraction).
Department of Defense and Department of Veterans Affairs
The following recommendations are intended to improve the evidence on exposures and health status of veterans:
Recommendation 9. Inventory research related to the health of veterans, including research funded by DoD and VA, and research funded by the National Institutes of Health and other organizations.
Recommendation 10. Develop a strategic plan for research on the health of veterans, particularly those returning from conflicts in the Gulf and Afghanistan.
Recommendation 11. Develop a plan for augmenting research capability within DoD and VA to more systematically generate evidence on the health of veterans.
Recommendation 12. Assess the potential for enhancing research through record linkage using DoD and VA administrative and health record databases.
Recommendation 13. Conduct a critical evaluation of Gulf War troop tracking and environmental exposure monitoring data so that improvements can be made in this key DoD strategy for characterizing exposures during deployment.
Recommendation 14. Establish registries of Service members and veterans based on exposure, deployment, and disease histories.
Recommendation 15. Develop a plan for an overall integrated surveillance strategy for the health of Service members and veterans.
Recommendation 16. Improve the data linkage between the electronic health record data systems used by DoD and VA—including capabilities for handling individual Service member exposure information that is included as part of the individual’s health record.
Recommendation 17. Ensure implementation of the DoD strategy for improved exposure assessment and exposure data collection.
Recommendation 18. Develop a data interface that allows VA to access the electronic exposure data systems used by DoD.
Recommendation 19. DoD and VA should establish and implement mechanisms to identify, monitor, track, and medically treat individuals involved in research and other activities that have been classified and are secret.
REFERENCES
IOM (Institute of Medicine). 1994. Veterans and Agent Orange: Health effects of herbicides used in Vietnam. Washington, DC: National Academy Press.
IOM. 1996. Veterans and Agent Orange: Update 1996. Washington, DC: National Academy Press.
IOM. 1999. Veterans and Agent Orange: Update 1998. Washington, DC: National Academy Press.
IOM. 2000a. Gulf War and health, volume 1: Depleted uranium, pyridostigmine bromide, sarin, vaccines. Washington, DC: National Academy Press.
IOM. 2000b. Veterans and Agent Orange: Herbicide/dioxin exposure and type 2 diabetes. Washington, DC: National Academy Press.
IOM. 2001. Veterans and Agent Orange: Update 2000. Washington, DC: National Academy Press.
IOM. 2003a. Gulf War and health, volume 2: Insecticides and solvents. Washington, DC: The National Academies Press.
IOM. 2003b. Veterans and Agent Orange: Update 2002. Washington, DC: The National Academies Press.
IOM. 2005a. Gulf War and health, volume 3: Fuels, combustion products, and propellants. Washington, DC: The National Academies Press.
IOM. 2005b. Veterans and Agent Orange: Update 2004. Washington, DC: The National Academies Press.
IOM. 2006. Gulf War and health, volume 4: Health effects of serving in the Gulf War. Washington, DC: The National Academies Press.
IOM. 2007. Gulf War and health, volume 5: Infectious diseases. Washington, DC: The National Academies Press.
Pamperin, T. J. 2006. An overview of the Disability Benefits Program and presumptions affecting veterans’ benefits. Paper presented at the first meeting of the IOM’s Committee on the Evaluation of the Presumptive Disability Decision-Making Process for Veterans, Washington, DC.
VBA (Veterans Benefits Administration). 2006. Annual benefits report fiscal year 2005. http://www.vba.va.gov/bln/dmo/reports/fy2005/2005_abr.pdf (accessed February 26, 2007).
VDBC (Veterans Disability Benefits Commission). 2006. Statement of the Veterans’ Disability Benefits Commission to the IOM’s Committee on Presumptive Disability Decision-Making Process. Washington, DC: VDBC.
Zeglin, D. E. 2006. Presumptions of service connection. Paper prepared for the Veterans’ Disability Benefits Commission. https://www.1888932-2946.ws/vetscommission/e-documentmanager/gallery/Documents/Reference_Materials/Presumption-Paper_3-7-06.pdf (accessed March 8, 2007).




















