
5
Measuring Health System Responses to Health Literacy
AMERICA’S HEALTH INSURANCE PLANS‘ RESPONSE TO HEALTH LITERACY
Julie Gazmararian, Ph.D., M.P.H.
Emory University Rollins School of Public Health
Why should health plans care about health literacy? In addition to the general complexity of the current health care system, the Institute of Medicine report on health literacy (IOM, 2004) identified several emerging themes or issues that are important aspects of the health system context with respect to health literacy. These include chronic disease care and self-management, patient-provider communication, patient safety and health care quality, access to health care and preventive services, provider time limitations, consumer-directed health care, and health care expenditures. The bottom line for all these issues is that health plan members who do not understand and cannot act on the medical information and instructions they are given are more likely to have poor health status that results in unnecessary costs.
Several years ago America’s Health Insurance Plans (AHIP) created a Task Force on Health Literacy that included individuals from a variety of backgrounds, including health communication experts, physicians, health educators, marketers, and AHIP staff who are also involved with work in health disparities and cultural competency.
The Task Force recently began discussions with the American College
of Physicians Foundation on areas of possible collaboration. Furthermore, as part of their monthly conference calls, the Task Force is scheduling case study presentations from member organizations to share information on major issues related to health literacy, thereby providing an opportunity to learn what is working and to make available different resources and tools in health literacy improvement.
In April 2008, the Task Force, along with AHIP’s personal health records task force, evolved a checklist of reader- and user-friendly web design for health plans (http://www.ahip.org/content/default.aspx?docid=22865) and held a web seminar on the topic. More than 200 individuals participated. These participants included individuals responsible for health literacy efforts in health plans as well as web designers, information technology specialists, and those responsible for personal health records.
The Task Force also sponsored an all-day training session in June 2008 that attracted 100 individuals from health plans across the country who are starting or building health literacy programs in their organizations. The 6-hour program included case studies providing background information about issues in health literacy reported by various member plans.
AHIP also recently transformed that training session into a series of three webinars to extend its reach. The faculty for this series includes a nationally renowned health literacy expert and professionals from a variety of disciplines and health insurance plans who have helped build capacity for clear health communication organizations. The three-part virtual seminar on health literacy can be found on the AHIP website (http://www.ahip.org/virtual/healthliteracy). It includes a session that provides a health literacy overview and steps for implementing a program, a session on starting up and advancing a company health literacy program, and a session on health literacy campaigns that provides case studies from national health insurance plans.
The AHIP board proposed four key steps toward creating a culture of clear health communication. AHIP recently surveyed its member companies to determine the current level of adoption of these four key steps. Results of that survey should be available in late spring of 2009. The four steps include the following:
-
Create responsibility for health literacy at an appropriate level in the organization;
-
Adopt a consistent approach to clear health communication;
-
Provide training in clear health communication for staff who prepare written communications for members and interact with members directly; and
-
Adopt a target reading level for written consumer communications
-
and review the content of documents to ensure that they meet the target.
Finally, AHIP is collaborating with Emory University on developing, piloting, and evaluating a health literacy friendliness assessment. This project was funded by the Agency for Healthcare Research and Quality (AHRQ) and The Robert Wood Johnson Foundation. The contributions of the project officer, Cindy Brach from AHRQ, have been of particular importance.
The Pharmacy Intervention for Limited Literacy Study
The study, the Pharmacy Intervention for Limited Literacy (the PILL study), tested a three-pronged approach: a phone reminder call for prescription refills, clear health communication training for pharmacists who counsel patients on their medications, and pill cards given to patients when they pick up their medication. The pill cards include pictures of pills, information about what the medication is for, when to take the medication, and possible side effects.
The primary question of interest is the effect of the intervention on program medication refill adherence and cost. Secondary outcomes of interest include self-reported adherence, understanding of medication instructions, patient satisfaction, and pharmacist satisfaction. The study also assessed the effect of health literacy on the intervention.
The study was conducted in two different pharmacy settings affiliated with Grady Hospital in Atlanta that fill 5,000 prescriptions per day. Patients in these settings have a high burden of comorbidities.
The first phase of the study was the pharmacy health literacy assessment. Why conduct such an assessment? Because a pharmacy or other organization can improve the quality of services offered to patients or clients of limited literacy by raising awareness of health literacy issues among the organization staff; by identifying barriers that may prevent individuals with limited literacy from accessing, comprehending, and taking advantage of health information; and by identifying areas where improvements can be made and focusing on these areas first.
The three components of the pharmacy assessment tool are complementary and designed to be completed together. The first component of the assessment tool is a pharmacy assessment tour that is designed to be completed by trained assessors who evaluate the pharmacy environment from an objective perspective. These assessors do not work for or receive services from the pharmacy.
The second component is a survey of pharmacy staff that is completed
by pharmacy members, including pharmacists, pharmacy technicians, administrative personnel, and supervisors. The third component of the assessment is patient focus group discussions with members of the pharmacy population. The assessment guide is available on the AHRQ website (http://www.ahrq.gov/qual/pharmlit/).
The Pharmacy Assessment
During the first phase of the pharmacy assessment, the pharmacy assessment tour, assessors observe both the physical environment of the pharmacy as well as staff interaction with the patients. The assessors identify existing barriers that inhibit clear communication of health information to patients with limited literacy skills, including promotion of services, print materials, and verbal communication. Because it is important that assessors observe the pharmacy in different situations, one assessor may conduct the assessment on a busy day and another on a slower day. Additionally, to avoid bias, the pharmacy staff should not be aware that the assessments are being conducted so that they do not act differently because they know they are being observed. Each assessment takes 20 to 30 minutes.
To minimize bias in the results, the pharmacy assessment tour should be conducted by at least two people who are trained together to promote consistent assessment techniques. The assessors should be familiar with principles of clear health communication, should not be pharmacy staff or patients, and should be able to blend in with patients who use the pharmacy.
All pharmacy staff are surveyed in the second phase of the pharmacy assessment because pharmacy staff members help create the environment within the pharmacy. Their choices and interactions with patients determine the health literacy friendliness of the pharmacy environment. Pharmacy staff have a unique perspective on the strengths and weaknesses of the pharmacy in serving patients with limited health literacy that may or may not be consistent with the viewpoints of outside assessors and patients. The pharmacy staff survey evaluates staff opinions of pharmacy sensitivity to the needs of limited-literacy patients in three areas: print materials, clear verbal communication, and sensitivity to health literacy. This survey takes about 20 to 30 minutes.
The third component of the pharmacy assessment is the focus group discussions with pharmacy patients. This is an effective way to collect detailed feedback directly from patients about their personal experiences with and impressions of pharmacy services. Four areas are discussed: the physical environment, care process and workforce, paperwork and written communication, and culture. The perceptions of focus group patients
help to identify physical and institutional barriers in the pharmacy that might prevent those with limited literacy from fully understanding pharmacy instructions and assessing pharmacy services.
Results
Results of the pharmacy assessments showed that although the pharmacies had a number of strengths, they needed to improve in several areas, including
-
Literacy-sensitive counseling;
-
Pharmacy flow, signage, and wait times;
-
Take-home materials available;
-
Services for limited English proficiency; and
-
Printed information not easy to understand.
Health Plan Assessment
The pharmacy assessment project has led to a new project that is broadening the application of the pharmacy assessment tool kit. The goal of the new project is to modify the PILL assessment tool and its applicability to the needs of health insurance plans throughout the country. The PILL assessment tool will be adapted and tested in a variety of health plan organizations and disseminated for widespread use in assessing health literacy friendliness of health insurance plans. There is incredible enthusiasm from AHIP member plans; plans are volunteering to be part of the pilot project. Pilot testing of the adapted tool is scheduled for spring 2009 with a report ready in late summer or early fall.
The project is currently in the early stages of adapting the assessment tool for use with health plans. Several areas have been identified in which questions will be developed to examine the health literacy friendliness of the health plans, including member information, member services/communication personnel, web navigation, forms, nurse call line, and nurse case/disease management.
Parallel to adapting the assessment tool, the project conducted an assessment of health literacy activities in health plans. Forty-one plans were invited to complete by e-mail a 10-minute web-based survey in January and February 2009. As of the time of the workshop, 27 of the 41 plans had completed the survey. Of those who responded, 100 percent said they had heard of health literacy. Sixty-nine percent of the plans indicated they have a policy or program in place to assess health literacy.
One question asked who is responsible for the health literacy program and activities within the respondent’s company. The responses were
-
Media, Public Affairs, Communications, Marketing, Editing – 7;
-
Health Education, Promotion, Cultural, Health Equity – 6;
-
Management – 6;
-
Project, Program Coordinator, Manager (vague) – 3;
-
Quality/Health Care Improvement – 2; and
-
None, N/A – 3.
When asked how they would rate company-wide support for health literacy policies and programs, 10 percent of respondents indicated excellent and 59 percent indicated good, while 28 percent indicated support was fair and 3 percent indicated it was poor. In terms of funding for health literacy programs and policies, a large percentage (43 percent) indicated funding came from sources other than the categories specified (categories were “health literacy department,” “each department,” “not sure,” and “other”).
When asked how responsibility for carrying out health literacy programs and policies was distributed, 4 percent of respondents indicated responsibility rested with the health literacy department, 32 percent said it was the responsibility of each department, 11 percent were not sure, and 54 percent responded by checking the “other” category. In terms of the focus of health literacy efforts, 50 percent of respondents said the focus was on universal health precautions, 14 percent indicated health literacy efforts were targeted at plan members with low health literacy skills, 14 percent indicated they were not sure of the focus, and 21 percent indicated the “other” category.
Examples of programs for plan members with low literacy skills included specific reading levels for all materials, staff training, simplified consent forms, simplified health education materials, a plain language tool kit, a revised enrollment form, and interpreter translation of materials.
In response to a question that asked if the plan had conducted any activities that assess whether plan members understand materials distributed by the health plan, 11 respondents said yes (surveys, focus groups, informally at member benefit education classes), 4 respondents indicated “sort of” through a health plan satisfaction survey or advertising understanding, and 9 said no or that they did not know.
For the future, Gazmararian said, efforts at measuring and improving health literacy must infuse clear health communication into all prevention and chronic disease management programs, integrate disciplines and approaches within organizations, collaborate with other health care partners and communities, and document success.
AN ACCREDITOR’S EFFORT TO PUSH THE PUBLIC POLICY AGENDA FORWARD
John P. DuMoulin, M.S.
URAC
URAC is a nonprofit, independent organization whose mission is to promote continuous improvement in the quality and efficiency of managed health care through processes of accreditation and education. URAC was established in 1990 to accredit utilization review services. Currently, URAC offers more than 25 distinct accreditation and certification programs across the continuum of care and accredits more than 400 organizations operating in all 50 states. URAC programs are now recognized by 39 state governments, the District of Columbia, and 4 federal agencies (Center for Medicare & Medicaid Services, Office of Personnel Management, Department of Defense, and Department of Veterans Affairs).
The accreditation programs include programs in health care management; workers compensation, property, and casualty management; pharmacy quality management; core organizational quality; vendor certification; health care operations; and health information technology. URAC accreditation is recognized as a “seal of approval” because the accreditation standards are
-
Set and enforced by an independent group of experts representing all stakeholders;
-
Current with market conditions;
-
The intersection of health policy goals and health service delivery reality; and
-
Built with performance measures to ensure there are data to support a continuous quality improvement cycle.
In terms of health literacy, URAC began working in this area with consumer-directed health care plans in the early 2000s. Following publication of the National Standards for Culturally and Linguistically Appropriate Services (CLAS) in Health Care: Final Report (HHS, 2001), URAC focused on making sure its efforts addressed areas highlighted in that report. Currently, URAC is engaged in promulgating health literacy requirements for managed health care organizations. An early effort in this area was the URAC Consumer Education and Support (CES) Accreditation Standards of 2005. The focus of this effort was twofold: to make sure that health plans communicate with consumers in such a way that the consumers understand the information, and to make sure sufficient information is made available to consumers so that they can make good decisions about their health care.
Standard CES 2, a nonmandatory standard, addresses pre-enrollment consumer information requirements and requires descriptions of the processes the organization uses to provide information and support to consumers for whom English is not the primary language, who are from different cultural backgrounds, or who have special needs, such as cognitive or physical impairments.
The nonmandatory standard addressing health literacy communication (Standard CES 13) requires that the organization provide information that meets the following goals:
-
Lowers, to the extent practicable, the cognitive effort required to use the information;
-
Helps consumers understand what effect a health care decision may have for their daily lives; and
-
Displays the information in a way that highlights information important to the consumer.
There is also a nonmandatory standard (CES 14) that addresses cultural sensitivity communication. The requirement is that information be presented and delivered in ways that are sensitive to the diversity of the organization’s enrollment, including literacy levels, language differences, cultural differences, and cognitive and/or physical impairment.
URAC has continued to be active in the area of health literacy. In 2007 the Health Standards Committee (HSC) agreed to address “Health Literacy/Diversity” as a topic for all its accreditation program standards (with the exception of the health information technology standards). Additionally, URAC worked with the Center for Information Therapy (Ix Center) to draft health information therapy standards for its disease management accreditation program. These new standards were developed and approved by the URAC board in 2008. Health literacy is now addressed in all URAC health care accreditation programs.
The core health literacy standards state the organization will implement written policies and/or document problems addressing health literacy that
-
Require consumer materials to be in plain language;
-
Assess the use of plain language in consumer documents; and
-
Provide relevant information and guidance to staff who interface directly with, or write content for, consumers.
Additionally, in 2008 URAC launched a five-part educational web seminar series on health literacy topics for its accredited companies, in partnership with the Northern Virginia Area Health Education Center.
However, health care organizations can still achieve accreditation without meeting this core health literacy standard.
URAC is committed to continuing its work in the area of health literacy, DuMoulin stated. The standards are becoming more granular and specific, and are being applied more broadly to the majority of managed care accreditation programs. The key thing has been to embed these standards (performance measures) in the accreditation programs so there is a scoring system to capture where organizations stand at any point in time. With such a system, URAC can provide feedback to the industry about the status of health literacy in the organizations with the goal of continuing to improve over time as an industry.
DEVELOPING AND TESTING A CAHPS®HEALTH LITERACY ITEM SET
Beverly Weidmer Ocampo, M.A.
The RAND Corporation
The Consumer Assessment of Healthcare Providers and Systems (CAHPS), which is funded by the AHRQ, is a set of standardized, evidence-based surveys for assessing patient experiences with their health care encounters. The CAHPS project not only develops survey instruments, but also provides reports that consumers can use to make decisions about their choices in health care. The project has also started to develop provider reports that can be used by providers to identify areas for quality improvement.
CAHPS has a number of surveys. There is the CAHPS Hospital Survey (the H-CAHPS), the CAHPS Health Plan Survey, the CAHPS In-Center Hemo-Dialysis Survey for dialysis facilities, the Experience of Care and Health Outcomes (ECHO) Survey of behavioral health services, a dental plan survey, and an ambulatory survey instrument for health plans (the CAHPS Clinician & Group Survey). A survey instrument for assessing nursing home care is in the final stages of development.
Each CAHPS survey includes a core set of items that can be supplemented with additional items. Each survey has its own set of supplemental items. For example, there is a supplemental item set for children with chronic diseases and people with mobility impairment that can be added to the CAHPS Health Plan Survey. Two new supplemental item sets are in development—one that assesses health literacy issues and one that is for health information technology issues.
In developing CAHPS instruments, strict design principles must be followed. The items emphasize collection of information from the per-
spective of the consumer and patient. The focus is on things for which the patients are the best source of information. For example, if information is best collected from records or physicians, then that item is not included in the survey.
Furthermore, the survey instrument must report on actual experiences, not just patient satisfaction. The surveys include ratings from 0 to 10. The survey instruments are standardized across the board, input is sought from stakeholders, there is extensive testing and validation of the surveys, and the surveys are publicly available.
For health literacy, two different supplemental item sets are being developed: one for H-CAHPS and one for the CAHPS Clinician & Group Survey. They both cover the same broad range of concerns, but because two types of settings are involved, the items are slightly different. These surveys are designed as supplements to the core surveys and are not intended to be stand-alone surveys. The intent is to develop a set of items that can be used to measure patients’ perspectives on how well health care professionals communicate health information. The goal of these supplements is to gather data to help health providers improve communication skills and patients’ health literacy. The supplements are being developed by all CAHPS grantees under RAND leadership.
The instrument development process for the health literacy supplements adheres to the same instrument development protocol used for the other CAHPS instruments. Preliminary survey development work on the health literacy supplemental item set for the Clinician & Group Survey involved identifying domains and subdomains of health literacy through review of an environmental scan of the literature and a call for input through the Federal Register, through discussions with key information sources in the area of health literacy, and through a stakeholders’ meeting. Stakeholders included health plan representatives, government agencies, health literacy advocates, researchers, and clinicians.
In conducting the environmental scan, existing measures in the public domain were reviewed to identify items that could be included in the supplemental item set. In addition, existing CAHPS instruments were reviewed to identify domains that could be expanded to include a health literacy measure. New survey items were written for each of the proposed health literacy domains that are not currently addressed by CAHPS or other existing instruments. Twenty-nine health literacy items were developed to cover four health literacy domains. English and Spanish versions of the items were developed in parallel. The health literacy domains targeted in this item set included
-
Oral communication regarding health problems and concerns, medications, tests, health promotion, and forms;
-
Written communication regarding medications and tests;
-
Techniques utilized by health providers to ensure patient comprehension of health information (commonly referred to as “teach back methods”); and
-
Patient-provider relationship.
The instrument development team included several researchers who are completely bilingual and bicultural and are experienced in developing, translating, and testing CAHPS surveys. Although English served as the official “carrier” language in the development process, making sure that survey items in both Spanish and English were both conceptually and linguistically equivalent was a top priority. When necessary, English items were modified to better convey the concept in Spanish. In addition, English-language wording was modified as necessary for easier translation into Spanish. In some cases, the item was rewritten in Spanish first, then translated into English to ensure comparability of the two items. The item set for the Clinician & Group Survey includes 29 items that fall within 6 item clusters as follows:
-
Patient-provider communication (10 items);
-
Communication about health problems or concerns (2 items);
-
Disease self-management (5 items);
-
Communication about medications (6 items);
-
Communication about tests (2 items); and
-
Communication about forms (4 items).
Two rounds of cognitive testing in both English and Spanish were conducted, followed by a field test to evaluate the reliability and validity of the item set. Affinity Health Plan and the University of Mississippi Medical Center participated in the field test. Six hundred patients were randomly selected from each site to participate. The field test was conducted by mail, with telephone follow-up. Approximately 54 percent of English speakers and 57 percent of Spanish speakers completed a survey.
Analysis of the field test data is nearing completion. Results will be used to make final decisions about survey items. The final set will include approximately 25 items, with a recommendation to have both a short version of the item set and a longer version. The goal is to have the item set publicly available during the summer of 2009. (Please see Appendix C for the CAHPS® Clinician & Group Survey Health Literacy Item Set.)
The developmental work for the health literacy supplement for the H-CAHPS is just beginning. It will go through the same overall process as was followed in the development of the health literacy supplemental item
set for the CAHPS Clinician & Group Survey. The domains will include patient-provider communication, shared decision making, communication about care or treatment, communication with nurses, communication about medications, discharge planning and coordination, communication about test results, and communication about forms. The plan is to field test the item set in the fall or winter of 2009 with an expected release date of spring 2010.
PROMOTING EFFECTIVE COMMUNICATION: THE JOINT COMMISSION’S EFFORTS TO ADDRESS CULTURE, LANGUAGE, AND HEALTH LITERACY
Amy Wilson-Stronks, M.P.P.
The Joint Commission
The Joint Commission accredits about 88 percent of the nation’s hospitals. It also accredits other facilities such as ambulatory care and long-term care organizations. The emphasis of this discussion is primarily on what is occurring in the hospital setting. The key question for The Joint Commission regarding health literacy is the following: What accreditation standards will move hospitals in a manner that better meets the needs of patients who present with health literacy issues, but also patients who present with other issues and concerns that affect communication?
The Joint Commission has had standards that stress that every patient has the right to effective communication, thereby addressing the concept of effective communication and, less directly but also importantly, health literacy. There are also standards that address patient education and the need for that information to be provided to patients in a manner they understand. Historically, the standards reflected communication as a patient rights issue, but that thinking has evolved: Effective communication is not just a patient rights issue but is critical to patient safety.
The focus on health literacy has come primarily through a focus on issues related to culture and language and their impact on racial and ethnic health disparities. In 2003 The California Endowment funded The Joint Commission to conduct a cross-sectional qualitative study examining three questions:
-
What are the challenges hospitals face in providing care to diverse patient populations?
-
What are hospitals doing to address these challenges?
-
Are there any promising practices that can be replicated to improve care?
The first report of this project identified many challenges. One major challenge is related to time—not having enough time to address some of the things that need to be done. Another major challenge is availability of resources, such as sufficient workforce, bilingual staff, language services, and money. Another major challenge is lack of training and awareness. It was also found that in some instances the resources were available but not being used by the hospitals.
Sixty hospitals were included in the study (Wilson-Stronks and Galvez, 2007). Forty-seven percent of those hospitals indicated that executives have direct responsibility for cultural and linguistic competence, 8 percent have direct responsibility for linguistic competence only, 43 percent do not have executives with direct responsibility for either area, and 2 percent did not answer the question. Sixty percent of the hospitals indicated they had developed plans to meet the cultural needs of patients, and 77 percent had developed plans to meet patients’ linguistic needs. Figure 5-1 shows how funds are allocated for cultural and linguistic services.
The study resulted in 32 recommendations for hospitals, researchers, and policy makers. The recommendations addressed the areas of leadership, quality improvement and data use, workforce, language services,
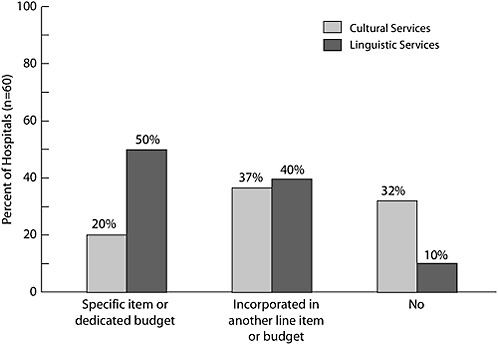
FIGURE 5-1 Operating funds allocated to cultural and linguistic services.
SOURCE: Wilson-Stronks and Galvez, 2007. Reprinted by permission from The Joint Commission.
provision of care/patient safety, and community engagement. One of the recommendations was to examine The Joint Commission standards more closely.
While this study was under way, The Joint Commission convened a public policy roundtable to address the issue of health literacy. Recommendations include
-
Recommendation 1: Make effective communications an organizational priority to protect the safety of patients.
-
Recommendation 2: Incorporate strategies to address patients’ communication needs across the continuum of care.
-
Recommendation 3: Pursue policy changes that promote improved practitioner-patient communications.
The common theme for addressing health literacy, cultural competence, and language issues is the need to address communication between the patient and the provider within the context of the health system. Support for this position can be found in examining The Joint Commission sentinel event data. These data have been voluntarily reported by accredited hospitals for more than 10 years. Since July 2005 hospitals have reported 1,400 sentinel events. For 843 of these events, detailed information on the root causes of the events was collected. Communication was identified as the primary root cause for 533 of these sentinel events.
Given the results of these investigations, The Joint Commission is considering how best to move toward creating standards for communication with vulnerable populations. Many patients are vulnerable, and access to direct communication can be inhibited by hearing impairment, visual impairment, speech impairment, cognitive limitation, intubation, disease, language, culture, health literacy, and health care proxy. Accurate information is needed for providers, practitioners, and patients. For example, practitioners need to be able to communicate and obtain accurate information to assess patient needs in order to determine a diagnosis, make a prognosis, provide treatment, obtain consent, and provide education and information.
Unfortunately, sometimes the health system hinders effective communication. For example, there is no standardized system in place to identify when a patient may have a communication need. Frequently there is a lack of supporting resources. Sometimes the resources are available, but the training needed for using the resources has not been conducted. Furthermore, there is a lack of evidence about which things work best to address which communication difficulties.
Given the findings, The Joint Commission has developed and is in the process of reviewing a Call to Action for communication (Patak et al., in review). The goals of the Call to Action are as follows:
-
Improve clinical practice to incorporate a systematic and methodological approach to patient-provider communication;
-
Optimize institutional availability and use of auxiliary services and increase frequency of referrals to specialists for “communication” purposes;
-
Educate health care providers; and
-
Revise health care policy and standards to set performance expectations for heath care providers on patient-provider communication.
The Joint Commission has a national patient safety goal concerning patient engagement. With a grant from The Commonwealth Fund, it is now in the process of developing culturally competent patient-centered care standards. The project will explore how diversity, culture, language, and health literacy issues can be better incorporated into current Joint Commission standards or drafted into new requirements. The standards will build on previous studies and projects, including the research framework from the Hospital, Language, and Culture Study and evidence from the current literature. Finally, a multidisciplinary Expert Advisory Panel, representing a broad range of stakeholders, will provide guidance regarding the principles, measures, structures, and processes. The standards are expected to address three main areas: effective communication, data collection and use to improve care, and meeting the special needs of different populations.
The Joint Commission developed a publication titled “What Did the Doctor Say?” Improving Health Literacy to Protect Patient Safety (The Joint Commission, 2007). In addition, The Joint Commission developed the Speak Up™ Initiatives, which are
-
Speak up if you have questions or concerns. If you still don’t understand, ask again. It’s your body and you have a right to know.
-
Pay attention to the care you get. Always make sure you’re getting the right treatments and medicines by the right health care professionals. Don’t assume anything.
-
Educate yourself about your illness. Learn about the medical tests you get and your treatment plan.
-
Ask a trusted family member or friend to be your advocate (adviser or supporter).
-
Know what medicines you take and why you take them. Medicine errors are the most common health care mistakes.
-
Use a hospital, clinic, surgery center, or other type of health care organization that has been carefully checked out. For example, The
-
Joint Commission visits hospitals to see if they are meeting The Joint Commission’s quality standards.
-
Participate in all decisions about your treatment. You are the center of the health care team.
In conclusion, Wilson-Stronks said, The Joint Commission is committed to developing standards and programs that will help health care organizations improve communication and, thereby, health literacy.
DISCUSSION
Moderator: Carolyn Cocotas, R.T., M.P.A.
F.E.G.S. Health and Human Services System
One participant raised a caution and a question. The caution is not to confuse health communication with health literacy because, he said, they are different. The question for DuMoulin is, how does one convince organizations to adhere to standards if there are no consequences for not doing so?
DuMoulin responded that URAC seeks to set the minimum necessary and attempts to raise that minimum. Susan Pisano, vice president of communications for AHIP said AHIP is attempting to work with member health plans to make sure training programs and policies are in place for communication with patients either orally, in written form, or through the Internet. The approach taken is an operational approach.
Another participant said it was laudable that many groups have stepped forward to engage in the issue of health literacy. The accreditation organizations are wrestling with describing the problem, producing reports, and developing standards. But at this point the uptake is not large because there is a great deal to learn about how to incorporate health literacy into health care organizations. What needs to happen next to involve all the organizations engaged in health literacy in a more substantive manner, the participant asked?
Wilson-Stronks said it is early in the process of incorporating health literacy. One of the struggles is how to separate communication from health literacy. What kinds of programs can an organization put in place to address things we do not fully understand? How can systems be set up to support the patients who are the ultimate recipients of care? As a first step, this lack of understanding needs to be addressed.
Gazmararian said that in working with AHIP over the past 6 months, she has seen a great deal of enthusiasm from the plans to become involved in health literacy issues and programs. However, a careful assessment of the barriers to plan engagement needs to be conducted. Pisano said one
of the reasons AHIP has measured what its member plans have done is so that it can develop a plan to engage its members that is based on where the plans currently are.
Another participant said it is terrific that organizations are acknowledging that there is an issue with health literacy and want to do something about it, particularly when there is not a large science base to support interventions. There is, however, a knowledge base regarding levels of health literacy and interventions to improve health literacy that can be used to move forward. We have many disparate pieces, but is it possible to pull together what we have to develop a core health literacy set of indicators?
Gazmararian said she has become less certain over time about the possibility of developing one composite measure for health literacy. Perhaps the question is whether the one composite measure is the way to go or whether one should develop measures for the separate pieces that fit together.
Isham responded that he thinks there are tremendous opportunities at various levels. At the federal level, for example, there is a marvelous opportunity and challenge to develop measures that more effectively characterize health literacy, health, and quality in ways that fit together—much the way Lurie presented the mapping of health literacy with other indicators. At the organizational level, different measures may well be called for to use with health plans, hospitals, and ambulatory care organizations, and it is encouraging to see the development of the different CAHPS measures. There is also a need for patient-level data and data that can be used in research.
The challenge, Isham said, is to develop a framework for measures of health literacy that includes information necessary for research, for quality improvement, and for accountability. Perhaps what is needed is not a single metric, but rather a family of information at different levels—national, organizational, and individual.


















