
Introduction 1
The United States faces the real possibility of a catastrophic public health event that involves tens of thousands or hundreds of thousands of victims. Public health emergencies—such as the 2009 H1N1 pandemic, an intentional anthrax release, infectious disease threats such as severe acute respiratory syndrome (SARS), fires, floods, earthquakes, and hurricanes—highlight the ever-changing threats posed by acts of terrorism and other public health emergencies, while also underscoring the pressing reality of these events. A tremendous effort has been made over the past decade to prepare for public health emergencies. Many states and healthcare organizations have developed preparedness plans that include enhancing surge capacity to increase and maximize available resources and to manage demand for healthcare services in response to a mass casualty event.
During a wide-reaching catastrophic public health emergency or disaster, however, these surge capacity plans may not be sufficient to enable healthcare providers to continue to adhere to normal treatment procedures and follow usual standards of care. This is a particular concern for emergencies that may severely strain resources across a large geographic area, such as a pandemic influenza or the detonation of a nuclear device. Healthcare organizations and providers may face overwhelming demand for services, severe scarcity of material resources, insufficient numbers of qualified providers, and too little patient care space. Under these circumstances, it may be impossible to provide care according to the standards of care used in non-disaster situations, and, under the most extreme
circumstances, it may not even be possible to provide basic life-sustaining interventions to all patients who need them.
In recent years, a number of federal, state, and local efforts have taken place to develop crisis standards of care protocols and policies for use in conditions of overwhelming resource scarcity. Those involved in these efforts have begun to carefully consider these difficult issues and to develop plans that are ethical, consistent with the community’s values, and implementable during a crisis. These planning efforts are essential because, absent careful planning, there is enormous potential for confusion, chaos, and flawed decision making in a catastrophic public health emergency or disaster.
However, although these efforts have accomplished a tremendous amount in just a few years, a great deal remains to be done in even the most advanced plan. Furthermore, the efforts have mainly been taking place independently, leading to a lack of consistency across neighboring jurisdictions and unnecessary duplication of effort. Lastly, many states have not yet substantially begun to develop policies and protocols for crisis standards of care during a mass casualty event.
These issues prompted the Institute of Medicine’s (IOM’s) Forum on Medical and Public Health Preparedness for Catastrophic Events (Preparedness Forum) to organize a series of regional workshops on this topic. These workshops were held in Irvine, CA; Orlando, FL; New York, NY; and Chicago, IL, between March and May of 2009.
FORUM AND WORKSHOP OBJECTIVES
The IOM’s Preparedness Forum was established to foster dialogue among a broad range of stakeholders—practitioners, policy makers, community members, academics, and others—and to provide ongoing opportunities to confront issues of mutual interest and concern. The Forum provides a neutral venue for broad-ranging policy discussions that can aid in coordination and cooperation between public and private stakeholders in developing and enhancing the nation’s medical and public health preparedness. Sponsoring members include federal agencies, state and local associations, health professional associations, and private-sector business associations.
The goals of the workshops on Crisis Standards of Care were to learn from the work already being done to develop state, regional, and local crisis standards of care policies and protocols; to identify areas that re-
quire further development, research, and consideration; and to facilitate communication and collaboration among neighboring jurisdictions.
Organized by an independent planning committee, the workshops brought together a wide range of key stakeholders, including policy makers from state and local public health departments; local and regional public health leaders; local and state government representatives; healthcare providers, including representatives of relevant medical disciplines, nursing, pediatrics, emergency medical services (EMS), palliative care, mental health, hospice, and home health; and healthcare and hospital administrators. See Appendix C for workshop agendas and Appendix E for biographical sketches of planning committee members, invited speakers, and panelists. This report is a summary of the presentations and discussions that took place during the workshop. Any opinions, conclusions, or recommendations discussed in this workshop summary are solely those of the individual participants at the workshop and are not necessarily adopted, endorsed, or verified by the Forum or the National Academies.
Workshop speakers and attendees discussed the roles and responsibilities of each stakeholder community in establishing state, regional, and local crisis standards of care protocols. In addition, they were asked to discuss what resources, guidance, and expertise had been established regarding crisis standards of care, including the legal and ethical guidance used to frame those discussions in different localities across the country. Finally, meeting participants were asked to help identify and discuss what resources they needed from federal, state, and regional authorities in order to advance and accelerate the establishment of coordinated and consistent crisis standards of care protocols.
This workshop summary aims to highlight the extensive work that has already been done on this topic across the nation and to raise awareness of current barriers and promising directions for future work. In particular, this document will draw attention to existing federal, state, and local policies and protocols for crisis standards of care; discuss current barriers to increased provider and community engagement; relay examples of existing interstate collaborations; and present workshop participants’ ideas, comments, concerns, and potential solutions to some of the most difficult challenges.
RELATED IOM WORK ON CRISIS STANDARDS OF CARE
This workshop series served as background for a subsequent Institute of Medicine letter report entitled Guidance for Establishing Crisis Standards of Care for Use in Disaster Situations (IOM, 2009). This letter report was requested by the Office of the Assistant Secretary for Preparedness and Response (ASPR), Department of Health and Human Services (HHS). The workshop series was organized prior to the onset of the letter report and was not technically part of those efforts. However, the committee that authored the letter report was aware of the information discussed at the regional workshops and this information was subsequently used as one of the key background sources for the committee’s work. Consequently, the letter report helped to inform and advance many of the issues that were identified by participants at the workshops.
Unlike this workshop summary, the letter report offers a series of consensus committee recommendations. The report concludes that “[i]n an important ethical sense, entering a crisis standards of care mode is not optional—it is a forced choice, based on the emerging situation. Under such circumstances, failing to make substantive adjustments to care operations—i.e., not to adopt crisis standards of care—is very likely to result in greater death, injury, or illness.” The committee also concluded that there is an urgent and clear need for a single national guidance for states with crisis standards of care that can be generalized to all crisis events and is not specific to a certain event. However, the committee recognized that within such a single general framework, individual disaster scenarios may require specific considerations, such as differences between no-notice events and slow-onset events, while the key elements and components remain the same.
The report articulates current concepts and guidance that can assist state and local public health officials, healthcare facilities, and professionals in the development of systematic and comprehensive policies and protocols for crisis standards of care in disasters in which resources are scarce. The committee also identified a series of five key elements and associated components that should be included in all crisis standards of care protocols. Finally, in an extensive “operations” section, the report provides guidance to clinicians, healthcare institutions, and state and local public health officials on how those crisis standards of care should be implemented in a disaster situation. A summary of the committee’s recommendations, findings, and practical guidance is included in Appendix B.
The complete letter report is available at http://www.iom.edu/disasterstandards.
Definition of “Crisis Standards of Care”
For purposes of developing recommendations for situations in which healthcare resources are overwhelmed, in the letter report the IOM committee defined the level of health and medical care capable of being delivered during a catastrophic event as “crisis standards of care”:
“Crisis standards of care” is defined as a substantial change in usual healthcare operations and the level of care it is possible to deliver, which is made necessary by a pervasive (e.g., pandemic influenza) or catastrophic (e.g., earthquake, hurricane) disaster. This change in the level of care delivered is justified by specific circumstances and is formally declared by a state government, in recognition that crisis operations will be in effect for a sustained period. The formal declaration that crisis standards of care are in operation enables specific legal/regulatory powers and protections for healthcare providers in the necessary tasks of allocating and using scarce medical resources and implementing alternate care facility operations.
This definition was developed by the committee that authored the letter report after the workshops took place, and no formal definition was used for the purposes of the workshop. In addition, for consistency this workshop summary uses the term “crisis standards of care” even though this term was only adopted by the IOM after the workshops took place. The remainder of this document outlines the discussions and presentations that took place during the workshops.
Other Related Work
The IOM letter report and these regional workshops built on a series of previous efforts, many of which were mentioned during the workshops. Workshop attendees praised the work of the Agency for Healthcare Research and Quality (AHRQ) and the Office of the Assistant Secretary for Preparedness and Response for driving the discussion for-
ward. The two agencies came together in 2004 to jumpstart the discussion by convening a panel with experts in the fields of bioethics, emergency medicine, emergency management, health administration, health law and policy, and public health. The result of that meeting was a critical document, Altered Standards of Care in a Mass Casualty Event, which served as a foundational document for communities approaching the issues of critical care (AHRQ, 2005).
Producing the document, however, was not easy. “When we first starting working on this subject in 2004, [hospital leaders] wouldn’t even agree to sit with us,” said Sally Phillips, director of public health emergency preparedness for AHRQ. “Their risk managers wouldn’t allow them to come.”
A subsequent report, published in 2007 and entitled Mass Medical Care with Scarce Resources: A Community Planning Guide, further advanced the field by providing an initial framework for developing policies and protocols for crisis standards of care (Phillips and Knebel, 2007).
Professional societies and academia also have made several recent efforts. Many workshop participants were involved with or highlighted the work undertaken through the American College of Chest Physicians, which resulted in a supplemental issue on the management of mass critical care in the journal Chest. This group brought together a multidisciplinary group of experts to provide an in-depth look at current U.S. and Canadian baseline critical care preparedness and response capabilities and limitations, and developed a framework for the development of mass critical care plans. Of particular interest to the workshop participants was the work on allocation of scarce critical care resources (Devereaux et al., 2008). The American Nurses Association (ANA) has also addressed this topic (ANA, 2008; Gebbie et al., 2009).
CRISIS STANDARDS OF CARE PROTOCOLS
In the past few years, several states have developed policies and protocols for allocation of scarce resources and crisis standards of care. However, these efforts have largely been taking place independently. In fact, many workshop participants expressed surprise at learning how much work had already been done on this topic in states across the nation.
Many panelists and other participants at the workshops were integrally involved in developing those policies and protocols and shared their documents and experiences at the workshops. Among the states that have publicly available protocols are California, Colorado, Massachusetts, Minnesota, New York, Utah, Virginia, and Washington (California Department of Public Health, 2008; Colorado Department of Public Health and Environment, 2009; Levin et al., 2009; Minnesota Department of Health, 2008; Powell et al., 2008; The Commonwealth of Massachusetts Department of Public Health, 2007; The Utah Hospitals and Health Systems Association, 2009; Virginia Department of Health, 2008; Washington State Department of Health’s Altered Standards of Care Workgroup, 2008). In Canada, the province of Ontario has also developed crisis standards of care protocols, including particular considerations for patients with cancer or chronic renal disease/acute renal injury, and for blood services and long-term care (Ontario Ministry of Health and Long-term Care, 2008). At the federal level, the Veterans Health Administration (VHA) has developed a protocol for allocation of scarce life-saving resources in VHA during an influenza pandemic (VHA, 2008a, 2009a).
Despite the ongoing work in pockets around the country, it was also clear that most state and local governments and healthcare facilities were in very early stages of developing such policies and protocols or had yet to begin. Among participants who completed the feedback survey after the workshops, just less than half responded that the organization they represented had developed or begun to develop crisis standards of care policies (see Appendix D for the complete set of responses).
At the meeting in Orlando, Kenn Beeman, a senior physician in the Office of Emergency Planning and Response for the Mississippi State Department of Health, discussed significant barriers in his state that have, to date, prohibited the development of crisis standards of care protocols and the engagement of providers in this issue. Among them, “The vast number of Medicare, no-care, no-pay patients [in Mississippi, Arkansas, and West Virginia] places a burden on us from the standpoint of reimbursement,” he said. “Philosophically, [many providers] believe that they are already practicing potentially in somewhat of an altered standard of care.”
Developing Crisis Standards of Care Protocols
Many participants at the workshops described efforts under way in their states to begin the discussion about crisis standards of care. In many cases this involved convening a committee or panel of experts to begin to lay the groundwork. For example, in Louisiana the Department of Health and Hospitals organized a Pandemic Influenza Clinical Forum, which was designed to engage a wide variety of healthcare participants to provide guidance to the state as it develops policy and procedural guidelines for crisis standards of care (Box 1). The goal of the group is to use the clinical expertise and knowledge of its members to help develop decision-making steps or matrixes for the ethical distribution of scarce medical resources.
Drawing on the experiences of states already significantly advanced in the process of developing crisis standards of care protocols, the 2009 IOM letter report laid out a five-step process that states could follow to develop such protocols (Appendix B; IOM, 2009). This process, together with the adoption of key elements and components that the committee identified, offers an opportunity to develop a consistent national framework for crisis standards of care.
“The challenge is not to wait for every community in the country to have a disaster befall [its] own citizens, but to figure out how can we proactively move this conversation forward,” said Edward Gabriel, the director of global crisis management and business continuity at The Walt Disney Corporation.
|
BOX 1 Louisiana Pandemic Influenza Clinical Forum Priorities
|
Several workshop participants emphasized that careful advance planning to avoid or mitigate the effects of scarce resources, along with other aspects of effective surge capacity planning, would in fact decrease or delay the need to implement crisis standards of care.
Who Makes the Plan?
One of the topics discussed in detail at each regional meeting was who should be brought to the table to ensure that the protocols developed are fair and equitable. One of the first steps toward building consensus on fair and ethical crisis standards of care is to bring in all of the parties who have a stake in the discussion. It is not enough, clearly, for a single hospital to have an established plan for how it will handle resource shortages. Those plans must be shared and coordinated across regional lines to prevent the kind of “hospital shopping” that could cause chaos and further overwhelm the system. Participants discussed the importance of bringing political and community leaders and members of the media into the fold and encouraging them to reach out to their communities to educate, inform, and, if necessary, guide appropriate behavior. Many participants also stressed that the community must be engaged, emergency medical experts consulted, and external providers such as pharmacists and insurance providers enlisted in the cause.
However, one lesson that emerged from the workshops is that the list of groups that should be involved and engaged in the planning process is much bigger even than this (Box 2). Deborah Levy, chief of health preparedness for the Centers for Disease Control and Prevention (CDC), described a program in which the CDC works with a community to develop a model for healthcare delivery during a public health crisis. Communities are selected based on a set of criteria, one of which is the level of collaboration between public health and the various components of the healthcare sector. “We want 911 and other call centers, emergency medical services, emergency departments, hospital administrators, public health, primary care providers, urgent care and other outpatient clinics, long-term care and skilled nursing facilities, hospice and palliative care, home health organizations, pharmacists, emergency management, local government such as mayors, and VA [Veterans Administration] and DoD [Department of Defense] facilities if they happen to be in your community,” said Levy. “We usually require at least three representatives from
each of those sectors to be at the table and over a 2½-day time period … to think through how they’d deliver care.”
Others added further to that list, including groups traditionally considered completely outside the healthcare field, such as funeral directors and morticians.
The reason for including all these different participants in planning goes deeper than the simple practicality of integrating care.
“If you’re doing this kind of emergency planning … every institution needs to be represented,” said Gabriel of The Walt Disney Corporation. “Otherwise they will sit back after you are done and say that they had no involvement.” Gabriel noted that the lack of participation paves the way for outsiders to criticize the difficult decisions when the time comes. That makes it particularly critical to capture the buy-in of both hospital leadership and politicians.
|
BOX 2 Who Should Participate in Planning for Crisis Standards of Care? A Partial List
|
In order to facilitate this broad involvement in Utah, the Governor’s Public Health Emergency Preparedness Advisory Council convenes partners from government, health care, and the private sector in the governor’s executive boardroom. Members of the council are appointed by the governor. “People have a hard time saying they won’t come when they know they’re in his own executive boardroom, and that makes it very effective for us,” said Paul Patrick, director of the Bureau of EMS and Preparedness in the Utah Department of Health.
Even while stressing the importance of engaging a wide range of stakeholders, several workshop participants also emphasized the importance of leadership and the use of effective procedures to ensure that the planning process does not become unwieldy. The 2009 IOM letter report outlines a five-step process that state public health authorities can use to develop crisis standards of care protocols (IOM, 2009). The process uses a series of working groups and committees to outline ethical considerations, review legal authority, and draft guidance. This is followed by a broad public stakeholder engagement process, after which the ethical elements and crisis standards of care can be finalized, incorporating changes raised during the engagement process, as appropriate. The final step of the process is the establishment of a Medical Disaster Advisory Committee that will provide ongoing advice to the state authority regarding changes to the situation and potential corresponding changes in the implementation of crisis standards of care. In this way, the process incorporates both broad stakeholder and public engagement as well as smaller groups that can function effectively to draft, refine, and provide real-time advice about implementation.
CONTINUUM OF SURGE CAPACITY AND STANDARDS OF CARE
Many workshop participants stressed that making changes to usual standards of care is not an all-or-none situation. The changes required depend on the nature and extent of the disaster, the existing capabilities of the community, and the particular resources that become scarce, among many other variables. Several participants emphasized that the response to the disaster should be proportional, and changes to standards of care should be the minimum necessary given the circumstances.
Efforts to define a common taxonomy and framework for discussion are a first step to ensuring a proportional response, to developing proto-
cols that are sufficiently detailed so as to be implementable, and to begin the discussion of exactly when healthcare providers and facilities should implement crisis standards of care.
Conventional, Contingency, and Crisis Standards of Care
John Hick, associate medical director for EMS and medical director of emergency preparedness at Hennepin County Medical Center, MN, presented a framework from an article published in the June 2009 issue of the Journal of Disaster Medicine and Public Health Preparedness (Hick et al., 2009). Hick and his coauthors described three categories of surge capacity: conventional capacity, contingency capacity, and crisis capacity (Box 3). The description resonated strongly with workshop participants and came to define the discussions of care at each of the workshops. The recent IOM committee on crisis standards of care also adopted this terminology and framework (IOM, 2009).
“Conventional capacity is really about providing patient care without any change in daily practice,” said Hick. Most hospitals and other healthcare resources can face small surges in demand, but still operate within the conventional framework. They may cancel elective surgeries, or accelerate the discharge of healthy patients, but they will still perform invasive procedures in standard operating rooms, follow standard protocols, and generally operate in a business-as-usual mindset. Staff may be asked to pitch in and support different areas of the hospital—a trauma surgeon may be pulled into the emergency room—but staff will not be operating outside of their bounds of expertise.
“As you move into contingency modes of reaction, you’re starting to … change practice a little, but it still really doesn’t have any significant impact on the care delivered or on the outcomes achieved,” said Hick.
Contingency care might mean using rooms of the hospital for different kinds of clinical care than usual, such as using post-anesthesia care rooms or procedure areas for care that would usually be delivered in an intensive care unit (ICU). Practitioners may start conserving supplies by, for example, not providing precautionary oxygen to patients who under normal circumstances would receive it, but who can survive and recover without it.
“As we move into the crisis level, we’re really starting to make some pretty substantial changes to the way we provide care, and there are some
implications for patient outcomes,” said Hick. “We’re trying to do the best we can with the resources available.”
In crisis situations, staff may be asked to practice outside of the scope of their usual expertise. Supplies may have to be reused and recycled. In some circumstances, resources may become completely exhausted. Family members may be asked to provide basic patient hygiene and other aspects of care that do not require medical expertise.
“Crisis capacity is really defined as adapting spaces, staff, and resources so that … you’re doing the best you can with what you have,” said Dan Hanfling, special advisor to the Inova Health System in Falls Church, VA, on matters related to emergency preparedness and disaster response. “You’re providing the best possible care under the circumstances.”
As Hick noted, the goal is always to avoid entering contingency or crisis care. However, if that becomes unavoidable and a facility is operating under contingency or crisis care, the goal is “to get back to a conventional footing.” Hick discussed strategies of preparation, substitution, adaptation, conservation, reuse, and finally, reallocation. Strategies that have a lesser impact on clinical care, such as substitution, should be used first, and strategies such as reallocation should be used only when other strategies have not been sufficient to address the resource shortage. He
|
BOX 3 Continuum of Conventional, Contingency, and Crisis Capacity Conventional capacity: The spaces, staff, and supplies used are consistent with daily practices within the institution. These spaces and practices are used during a major mass casualty incident that triggers activation of the facility emergency operations plan. Contingency capacity: The spaces, staff, and supplies used are not consistent with daily practices, but maintain or have minimal impact on usual patient care practices. These spaces or practices may be used temporarily during a major mass casualty incident or on a more sustained basis during a disaster (when the demands of the incident exceed community resources). Crisis capacity: Adaptive spaces, staff, and supplies are not consistent with usual standards of care, but provide sufficiency of care in the setting of a catastrophic disaster (i.e., provide the best possible care to patients given the circumstances and resources available) (Hick et al., 2009). |
highlighted a set of informational cards for healthcare providers and institutions that he and others developed in Minnesota that lays out patient care strategies for scarce resource situations (Minnesota Department of Health, 2008). The card set lists appropriate substitution, adaptation, conservation, reuse, and reallocation strategies for oxygen, medication administration, hemodynamic support and IV fluids, mechanical ventilation, nutrition, and staffing.
Stages of Care in the North Dakota Plan
Officials in the state of North Dakota have also outlined incremental changes to standards of care. During the Chicago workshop, Tim Wiedrich, chief of emergency preparedness and response for the North Dakota Department of Health, presented their work on outlining levels of care (Box 4).
Stage 1 involves a small shift in patient care that may inconvenience some patients, but will not have a measurable impact on patient care. It is akin to the “conventional” care category outlined by Hick.
As an event escalates, North Dakota moves into Stage II, taking steps that limit the quality of care and may impact patient outcomes. Doctors and nurses are asked to operate slightly outside their normal bounds of expertise, retired caregivers are called back onto the job, and changes are made in standard operating procedures such as charting and checking vital signs.
Stage III is akin to the crisis care scenario outlined by Hick and others. In a Stage III emergency, the North Dakota system operates under a “best efforts” basis that attempts to stretch the medical response to serve as many patients as possible. At Stage III, the impact on care is severe. A decision such as “no CPR” has real consequences, but in this scenario is deemed necessary to ensure the best possible care is delivered to the maximum number of people.
|
BOX 4 Stages of Care in North Dakota’s Plan STAGE 1: SMALL OUTCOME IMPACT
STAGE II: MODERATE OUTCOME IMPACT
STAGE III: SEVERE OUTCOME IMPACT
|
CLINICAL OPERATIONS
The decision to implement crisis standards of care is a significant event—it changes how hospitals and caregivers operate, it changes the legal environment, and it changes citizen expectations. A significant portion of the workshops was devoted to how and when that decision would be made, and how hospitals should implement crisis standards of care.
Indicators
Implementation of crisis standards of care first requires recognition of an actual or impending resource shortfall. Workshop participants noted that many different resources may become scarce at different times, depending on the nature of the disaster and the characteristics of the community and the healthcare facility. The 2009 IOM report listed the following resources as likely to be scarce in a crisis care environment and possibly justifying specific planning and tracking:
-
Ventilators and components
-
Oxygen and oxygen delivery devices
-
Vascular access devices
-
Intensive care unit beds
-
Healthcare providers, particularly critical care, burn, and surgical/anesthesia staff (nurses and physicians) and respiratory therapists
-
Hospitals (due to infrastructure damage or compromise)
-
Specialty medications or IV fluids (sedatives/analgesics, specific antibiotics, antivirals, etc.)
-
Vasopressors/inotropes
-
Medical transportation
Workshop participants emphasized that it was important that healthcare facilities be aware of impending shortages so they could take steps to avoid having to implement crisis standards of care. Participants also noted the importance of having situational awareness of the system because the entire network of indicators will provide the most accurate sense of the level of stress on the system. For example, a shortage of ventilators will be compensated by the use of other ventilator processes, in turn making those supplies scarce for their originally specified use. In this way, a small number of significantly scarce resources can cause strain throughout the entire system.
Triggers
To achieve integrated, consistent, and fair care, every participant in the system must be operating with the same understanding of where
things stand on the conventional/contingency/crisis scale. In fact, many workshop members indicated the need for multiple triggers operating at different levels and with different time frames.
Speaking of his own experience in New York, David Hoffman from Wyckoff Heights Medical Center said his group identified the need for multiple triggers. “There needs to be a trigger based on the declaration of disaster from government officials if there is a statewide or regional event,” Hoffman suggested. “There needs to be a trigger at an institutional level so that there is the means of communicating to the staff that … a new set of rules applied.… And what we’ve learned from the situation in Katrina … is that there needs to be a factual trigger that can be applied retroactively” to provide legal protection for caregivers.
Some participants believed those triggers should be driven on the scene by frontline staff. “I think those kinds of triggers need to be defined by the people who are on the front lines and will be forced to make those decisions,” said HHS’s Rear Admiral Ann Knebel. “We need to support them and make sure that there is, as much as possible, consistency in terms of the principles that drive what those triggers are.” Knebel said that the trigger point comes when available resources are no longer adequate to support patient demand.
Different states have taken different approaches to determining who should make the decision, some empowering governors and others looking to public health officials to help define the triggers and determine the mechanism for transitioning from normal to crisis standards of care. However, as the 2009 IOM report concluded, working through a framework that begins at the institutional and local levels, the authority to institute crisis standards of care lies with the state. In most states, the state department of health holds this responsibility. Some states have well-defined processes for establishing their protocols, but many others are still in development.
Triage
Once a determination has been made that conventional care standards no longer apply, workshop participants commented, the rapid implementation of an effective triage program should be one of the first goals of any healthcare program. A triage program aims to rapidly screen, evaluate, and sort patients based on their medical status and likely outcome.
Ken Berkowitz from the Veterans Administration National Center for Ethics explained a working model of the VHA Hospitals’ operating protocol during pandemic influenza: “Our tertiary triage protocol is the process of sorting acute care hospital patients into three treatment groups. Initial decisions are based on survivability, and that’s justified by the goal of making optimum use of resources and meeting the goal of overall population health. Second-order decisions for equally prioritized patients are based on a first-come, first-served basis, or if that’s not possible, on a lottery basis. That is justified by the principle of fairness.”
As many participants noted, the triage process outlined in the American College of Chest Physicians work on mass critical care has formed the basis for the protocols developed by the VHA and many of the states (Colorado Department of Public Health and Environment, 2009; Devereaux et al., 2008; IOM, 2009; Minnesota Department of Health, 2008; The Utah Hospitals and Health Systems Association, 2009; VHA, 2008a, 2009a). This triage process includes the use of the Sequential Organ Failure Assessment (SOFA) score for determining triage priorities. The system uses a variety of measures linked to six major organ systems— (1) cardiovascular, (2) coagulation, (3) hepatic, (4) neurological, (5) renal, and (6) respiratory—and is already in use in multiple hospitals. The SOFA scores help triage teams rapidly determine how sick people are, and are relatively easy for hospitals to execute and record. The IOM report’s basic triage process is outlined in Figure 1 and exclusion criteria are described in Box 5.
Under this triage process, both patients who score too high and too low on the SOFA assessment are not given critical care resources during an emergency: patients who score too high because they will not likely benefit from medical care, and patients who score too low because they will likely survive without substantial care.
Many workshop participants also emphasized that the use of SOFA scores is far from the perfect solution. “From a pragmatic standpoint, on an individual–patient level, to say that this person is getting resources and this person is not based on a one-point difference on a SOFA score … that’s a huge issue and something we think about very carefully,” said Hennepin County Medical Center’s Hick.
Moreover, SOFA scores may not apply to some of the most vulnerable patient groups. Stephen Cantrill, an emergency physician in Colorado, noted that SOFA hasn’t been studied in pediatrics, and is not designed as a predictive tool. Many workshop participants noted that the lack of research on SOFA scores and other potential decision tools in
pediatric populations is a significant gap and emphasized that much more research should be done in this area so that it can better inform important policy decisions.
Hick said his hospital had an appeals process whereby a patient’s physician could appeal back to the triage team for a rescoring if a patient’s condition changed.
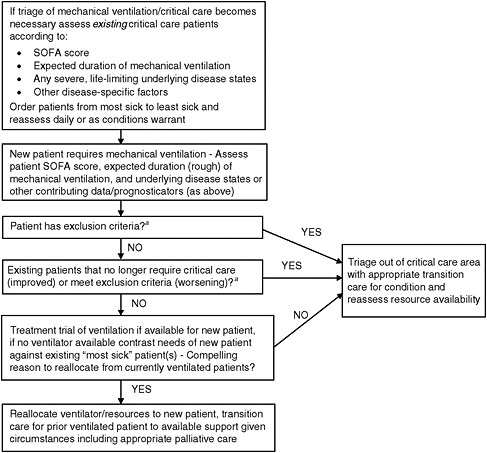
FIGURE 1 Triage algorithm process.
aExample exclusion criteria include severe, irreversible organ failure (congestive heart failure, liver failure, etc.), severe neurologic compromise, extremely high or not improving sequential organ failure assessment (SOFA) scores, etc.
SOURCE: IOM (2009) (adapted from Devereaux et al., 2008).
Triage Across the Health System
Hospital-level triage, however, is really only one piece of the puzzle. “I would encourage us to be very inclusive in our language,” advised Cheryl Peterson, director of nursing practice and policy at the ANA, speaking at the Orlando workshop. “It is not only physicians who do triage. It is your mental health provider. It is your registered nurse. It could be your respiratory therapist. There are a whole host of providers out there who are responsible for making some very difficult decisions, and
as we think about our planning, every one of these providers has to be engaged in that decision.”
Others discussed the need for a focus on triage at all stages of care. In the Colorado protocol, “We tried to address things from the beginning to the end, starting with telephone triage,” said Cantrill. “That’s trying to get some standard approach to telephone triage because we know that’s going to be a hot area of heightened importance during any type of pandemic.”
EMS triage is another area that needs to be aggressively studied, but hasn’t. “From the EMS level, we have to decide the basic issues of triage,” said North Carolina EMS’s Roy Alson. “Who’s going to get an ambulance? Who gets transported to the non-hospital care facility?”
Training was another important factor emphasized by workshop participants, who cited the practice in some emergency departments to have “Triage Tuesdays,” where all patients are run through the triage system to keep the process fresh in the minds of all practitioners involved.
Alternate Care Facilities
Most surge capacity plans contain some means of providing non-critical care outside of the hospital setting to free up as many hospital beds as possible for more seriously ill patients. This can take the form of either formal, dedicated facilities that are idle most of the time, or of convertible public spaces such as schools, restaurants, houses of worship, or meeting halls. These facilities are important components of a surge plan, but they raise additional questions regarding crisis standards of care because the facilities may have different staffing levels, make greater use of volunteers or providers practicing outside of their duties, and have more limited care capabilities. Although this was not discussed in great detail at the workshops, participants also mentioned a number of additional challenges related to establishing alternate care facilities, including facility licensing and reimbursement.
“We have bought, thanks to a grant, a 250-bed surge-capacity facility.… The beds and everything are in trailers and we can move them to a church hall or to a school gym,” said John Robinson, discussing Baptist Memorial Hospital in northern Mississippi’s approach to prestaged surge capacity.
Others cautioned that, even if adequate additional resources are available, these facilities must be adequately staffed or they will not
function. “We’ve got eight very nice tractor-trailer-mounted disaster hospitals,” said North Carolina’s Alson. But “nobody is going to be able to staff them [in a true pandemic]. This is not a hurricane where it’s going to go for 4 or 5 weeks maybe. This is months and it’s going to be in multiple events and you’re going to do it with half your staff eventually.”
Workshop participants considered staffing these facilities with a combination of full-time health care physicians, retired physicians, nurse practitioners, and other providers. Many noted that providing palliative care in a surge facility was one area where retired healthcare workers could provide excellent support during a crisis.
In North Dakota, alternate care facilities will provide such care and be staffed by volunteer providers, according to a presentation by North Dakota’s Wiedrich. He detailed the basic capabilities that alternate care facilities in North Dakota would provide (Box 6).
Rick Hong, medical director for public health preparedness in the Delaware Division of Public Health, discussed the model for alternate care facilities being used in Delaware (Box 7). He detailed how each component of the system would be staffed, and what kinds of treatments would be available in each.
|
BOX 6 North Dakota Alternate Care Facility Capabilities
|
|
BOX 7 Modular Medical Expansion: An Example from Delaware The surge program in Delaware is based on a concept called “modular medical expansion.” When developing the program, all the parties involved agreed that simply sending all the patients to the hospital was untenable, so they set up a triad of facilities to provide approach care. The first piece of that triad is Neighborhood Emergency Health Centers, or NEHCs. The NEHCs are located in communities and are designed to handle triage and to function as the gateway for patients into the healthcare system. |
|
“We’re relying on historical data stating that most of the patients affected in a disaster do not need medical care or do not need critical care, about 50–80 percent,” said Rick Hong, medical director for public health preparedness in the Delaware Division of Public Health. “So our concept is if we can identify those patients first and remove them from the healthcare system, then we'll be able to manage the situation.” The NEHC will be able to provide simple care such as distributing vaccines or antiviral medication. It will be staffed by public health nurses, pharmacists, and other healthcare providers who may not usually see patients. These providers currently undergo annual training to prepare to staff these areas. Patients identified as needing more significant medical care at the NEHCs will be sent to either an Acute Care Center or a hospital. The Acute Care Centers are out-of-hospital care settings that are capable of providing a limited array of supportive care to patients in need: IV antibiotics, IV pain medication, IV fluids, and nebulizer treatments. The list of available treatments is intentionally kept small so that these Acute Care Centers can be staffed by non-specialists. Hospitals are required to staff these centers by donating care providers. “The hospitals said, ‘There’s no way we’re going to be able to give you staff,’” said Hong. “Our response was, ‘OK, we’ll just send the patients to you. How do you like that?’ And they [all agreed] to give staff members.” With NEHCs and the Acute Care Centers siphoning off a large portion of the potential patient population, Delaware’s hospitals can be reserved to providing crisis care to the truly ill. To make the system function, Delaware has put in place laws that limit the liability of providers operating in this situation, and that allow healthcare professionals to expand outside their traditional scope of practice, such as allowing pharmacists to administer vaccines to patients or emergency medical technicians to provide pills. |
Broadening the Scope: Emergency Medical Services, Community Health, and Other Components of the Health System
One reality driven home by the workshops is that the forces involved in disaster preparedness are almost, by definition, top-heavy. While the regional workshops brought together a wide array of professions—public health officers, physicians, hospital administrators, researchers, nurses, and emergency medical technicians (EMTs), to name but a few—most planning and policy work on crisis standards of care is focused on the hospital or hospital-network level.
The reason is simple: These larger and more sophisticated healthcare networks are often the only ones with the resources to spend on disaster
preparedness. Unfortunately, this top-heavy approach runs counter to the actual nature of responses to medical emergencies.
“Most emergency responses are an upside-down pyramid,” noted Kathryn Brinsfield, associate chief medical officer at the Department of Homeland Security (DHS). “Critical care patients are a very small piece of that, and the outpatient care, visiting nurses, all the other places” are crucial.
Emergency Medical Services
One recurring theme throughout the workshops was the critical role that the emergency medical services play in directing emergency response, and the limited extent to which they have been incorporated into planning for crisis standards of care.
During day-to-day operations, EMS systems have a mandate to transport individual patients to the closest available hospital, while providing stabilizing care along the way. But as Leslee Stein-Spencer, a Registered Nurse and manager at the Chicago Fire Department, told the Chicago workshop, that approach won’t work during a mass casualty situation.
In a mass casualty situation, EMTs may be called on to transfer multiple patients at a single time, to provide medicine to limit infection, to triage patients onsite, or to transport only those who meet certain qualifications. EMTs may be asked to operate outside their standard scope of practice, or transport patients to alternate care facilities. But so far, at least in her region, training and preparation have overlooked this critical link (Box 8).
|
BOX 8 Status of Emergency Medical Services Preparedness in Chicago
|
Stein-Spencer identified a series of issues that must be addressed in developing the emergency response, including the following:
-
Defining credentialing/licensing activities, both local and state
-
Determining the trigger for crisis standards and identifying who makes the call: local, regional, state
-
Finalizing mutual aid agreements
-
Handling the differences between private and public responders
-
Ensuring the consistency of care in adjacent communities
Some participants also noted the special challenges that arise in many communities, particularly rural areas, in which EMS units are largely or entirely volunteer.
Community Health Centers and Other Resources
Like EMS, community health centers and other “boots on the ground” facilities are also often overlooked in the planning process. But the need to coordinate their care with hospital settings to ensure a single, unified approach to standards is critical.
Kevin McCulley, emergency preparedness coordinator at the Association for Utah Community Health, emphasized that these community health centers represent a largely untapped resource for planners, and could be called on in a pinch to provide critical care space on a short-term basis.
Private Sector
Large corporations and other private entities must also be brought into the discussion as well, participants said, as they can have outsized influence over disseminating information regarding emergency response and standards of care in an emergency setting. One of the four workshops, in fact, was hosted by a private company—the Orlando meeting was hosted at a Disney resort—reflecting an increased recognition by the private sector that managing these kinds of situations is critical to business continuity.
“Many large corporations are willing to engage in preparedness planning,” noted Knebel. “It makes good business sense, and they are part of the community.”
Resource Availability and Distribution
Workshop participants said that identifying available resources is an essential part of laying the foundation for a sound approach to standards of care. Does a hospital know how many emergency beds or emergency ventilators are available? If not, that kind of resource survey should be among the first orders of business when creating a surge program.
William Fales, associate professor of emergency medicine at Michigan State University’s Kalamazoo Center for Medical Studies, discussed the work of the Great Lakes Healthcare Partnership to identify the resources available for surge care during an emergency situation. They identified and categorized 123 types of resources available in the region, consolidating those resources into a centralized database that could be used in emergencies.
“It’s incumbent on every state and community and planning group to know what your resources are so you can figure out how you’re going to fill and meet that gap,” said Knebel of HHS.
Davis Tornabene of Sarasota Memorial Hospital, FL, described what she learned in the planning process. “When we did our tabletop regarding pan flu some issues came to light … we had really no idea of the state supply of available ventilators, antivirals, things like that,” she said.
Others wondered how hospitals could learn more about available resources in the Strategic National Stockpile, such as the numbers and types of ventilators available during a crisis. Although that information may be classified, there were calls to have at least some basic information shared so hospitals could do facility planning.
A broader point made about resources was the need to ensure a fair and adequate distribution of resources, based on processes that can be upheld even as situations become turbulent. “You need those triggers to determine when you’re going to say [to hospital distributors] that you can’t distribute all your N95 respirators to the hospitals that are paying you the most money,” said HHS’s Knebel. “You have to make sure you distribute them to those people who don’t go to those hospitals, the people who live in the inner cities.”
It is all too easy to imagine hospitals hoarding supplies, or suppliers demanding ever higher prices for the remaining few doses of a particular drug. In Colorado, one workshop participant offered, draft orders were under consideration that would allow the governor to seize supplies from any location and redistribute them to other locations.
When supplies do run out, a number of participants suggested developing guidelines for how to reuse and recycle spent resources. Studies are needed, they suggested, on how long supplies such as surgical masks can be used before being discarded in suboptimal environments. In an environment focused on doing the greatest good for the greatest number, extracting the maximum value from limited supplies is crucial.
Pediatrics and Other At-Risk Populations
If crisis standards of care are to be fair, particular attention must be paid to planning for at-risk populations such as children and older adults, workshop participants noted. The challenges of basic triage multiply in these populations for a variety of reasons. There is less available research on which to base decisions, and the care required may be more specialized so even during non-disaster times there are fewer trained healthcare providers and appropriate resources. There is also the potential that a communications problem or a lack of understanding of the special needs of people with disabilities such as sight or hearing impairments could impact the triage process. In some cases, the decisions are simply more emotional.
“Large-scale pediatric casualties could be more than we could bear,” warned George Foltin, speaking of his work on emergency planning with the New York City Department of Health, at the meeting in the Bronx. When triaging pediatric patients, “we need to think of this sometimes as if we were wartime England. We need to be brave. We need to make correct choices. We need to protect our way of life and we need to focus on our children.” Most hospital settings do not have the specialty equipment or specially trained doctors to provide surge coverage of pediatric patients, Foltin noted. As a result, “The major pediatric center must surge,” he said. “We think that critically ill and injured children are better off at a major center that has [the equipment and expertise] to take care of them, even under less than optimal circumstances, rather than going to a hospital that doesn’t know how to take care of them.”
Children represent 25 percent of the U.S. population, so our failure to plan explicitly for their care represents an acute failure of overall planning.
Children, of course, are not the only ones. In fact, there may be situations where the rest of the population is carrying on as normal even as a special-population care facility is completely overwhelmed. “A perfect example was the [New York City] blackout in 2003,” added Judith Ahronheim, a New York geriatrician. “We were thinking about terrorism, but the largest number of admissions to the hospital was vulnerable elderly people whose electrical appliances had failed.”
Mental health patients are another vulnerable population that deserves special attention and care. Anticipating and responding to those needs is a critical part of maintaining a fair standard of care. The importance of upholding fairness during the development and implementation of crisis standards of care is discussed in greater detail below in the section on Ethical Considerations.
Finally, Phillips, of AHRQ, highlighted pregnant women as another group of vulnerable patients. “We don’t really want pregnant healthy women going into some of the hospitals during pandemic influenza,” said Phillips. But how do we encourage woman to deliver at home in contrast to the broader push for hospital births over the past few decades?
Palliative Care
Ultimately, despite surge capacity, despite stretching resources, and despite best efforts, the implementation of crisis standards of care in a mass casualty event may mean that some patients will not have access to critical care resources.
Workshop participants widely believed that no patient, regardless of the circumstance, should simply be “left to die.” Participants stressed that care is never withdrawn. Patients who are not offered access to critical life-sustaining resources should receive the best available palliative care. Participants also discussed regular reevaluation of patients to see if improving conditions have increased their likelihood of responding to more aggressive treatment using available resources.
These situations “contemplate a context where there will be many, many deaths among people who receive critical care resources, and among those who don’t, so it puts an enormous emphasis on palliative
care,” said Tia Powell, director of the Montefiore-Einstein Center for Bioethics in The Bronx, New York.
Despite the obvious need, participants worried that too little had been done to establish protocols and standards for palliative care for those who do not receive life sustaining resources. So much energy is spent worrying about resource allocation for those patients who do receive critical care resources that almost none is left over for those who don’t. “It’s distressing after this many years that there’s still a reluctance to talk about palliative care,” said Knebel from the HHS. Even in healthcare circles, there’s a reluctance to admit that sometimes the best the healthcare system can do is to make a patient more comfortable.
“It’s a perfectly acceptable standard of care in the appropriate situation,” said Jan Rhyne of the North Carolina Medical Board, who thought it should not even qualify as a crisis standard of care. “It is a very noble type of care, and I think the hospitals are having a tough time getting that message out right now.”
Workshop participants highlighted the need for extensive work on how patients should be treated if life-sustaining treatment such as ventilator support is not offered or is discontinued. Similarly, caregivers should be taught how to deal with the stress of these situations, and to handle the very real potential mental health challenges of those involved.
“I find that personally, in the circles I travel in [palliative care] is now the new third rail of disaster medicine,” said Inova’s Hanfling. “We can talk somewhat comfortably about this shift in standards of care … but when we talk about palliative care … withdrawing ongoing life support—you know it is really frowned upon and I get a lot of push back.”
The decision to reallocate life-sustaining treatment from one patient in favor of another is a very real, on-the-ground issue in a mass casualty situation. “How do you manage that transition?” asks Minnesota’s Hick. “You’re in the ICU, [the patient is] on the ventilator, and now you extubate the person.… Do you keep the patient there? … Do you have a palliative care area you move them to? What kind of support do they have? Those are exactly the kinds of issues we need to think through.”
The scenario is even more basic than that. “There’s virtually no standard protocols for external extubation in the literature now. I mean, there was something in Chest Soundings a few years ago, but there’s very little for non-pandemic standards of how to do it. So that’s just an existing gap, period,” noted Berkowitz from the VHA.
These are not easy issues. In the context of a mass casualty event, palliative care may be given to patients who, in normal situations, would
receive aggressive interventions and potentially life-sustaining therapies. Exactly how, where, and when to provide this care—and the preparations that must be made to ensure that care is as good as possible—was an area identified as needing significant research.
Mental Health Care
One area that to date has received little attention is the mental health consequences surrounding some of the hardest decisions contemplated—such as removing ventilator assistance from a patient or ceasing pediatric resuscitations in the field. “One of the things we don’t do very well is understand how [practitioners] are likely to respond,” said Jack Herrmann, senior advisor for public health preparedness at the National Association of County and City Health Officials. “We plan for how we want them to respond, and less for how they do respond.”
The long-term fallout on practitioners and patients will also be great, and multiple participants voiced the need to prepare ahead of time to assist patients and caregivers coping with post-event stress. “When people are going to live in this environment for any period of time, the providers are going to need a lot of support,” said Phillips. “They’re going to have to live with these decisions. And I think that’s something we haven’t paid much attention to.”
“Grief management’s going to be a huge, huge component … not just for the individuals who are falling victim to this, but also to the providers who are not able to provide the kind of care and treatment that they feel is important,” said David Fleming, professor of Clinical Medicine and the Director of the Center for Health Ethics at the University of Missouri School of Medicine. To meet this need, Missouri is developing just-in-time pandemic grief training for managers and supervisors.
Robert Hood, an ethicist at the Florida Department of Health, noted that Johns Hopkins University has a CDC funding allotment to work on ethical issues and mental health preparedness.
The broader population will also face significant mental health issues. “The community is going to have to deal with families having family members die in their homes [when] normally they would have had a hospice provider maybe coming in and helping them. They may not have that kind of support,” noted Phillips. “I think there are a whole lot of implications for the mental health field and mental health providers.”
Training
One challenge that workshop participants consistently noted was the difficulty in effectively training and building relationships across organizational boundaries. Efforts like Levy’s community-based CDC workshops help, but the need was identified to develop opportunities that would build ongoing, hands-on, face-to-face relationships among stakeholders before disaster strikes. That means holding joint training exercises and developing personal relationships so that, when disaster does strike, lines of communication will be open.
Inova’s Hanfling noted that “planned disasters” can often provide a framework for exactly this kind of discussion. Hanfling noted that the 2009 presidential inauguration provided an opportunity for representatives from Maryland, Virginia, and the District of Columbia to sit together in an emergency operations center ready to manage an emergency response. This enabled them to provide information in real time from their respective jurisdictions, and in turn to communicate information back from the emergency operations center.
Ultimately, no major events occurred during the Inauguration that required a community-wide response. But bringing people together to sit at the same actual table and build relationships was seen as a major and significant step forward. “One of the things that, even for communities that are fairly advanced [in their preparedness planning] … is that it is quite interesting when you bring these groups together,” said the CDC’s Levy. “For one, they usually end up realizing that they don’t really know the details of each other’s plans, or they’re making assumptions that turn out to be incorrect, or someone will have a plan and another group didn’t even know they had that plan. Also hospital leaderships, we’ve found, usually haven’t grasped the complexity of the issues that are involved in these types of mass events.”
As these diverse groups are brought together, however, there is a need to mediate the situation and foster a fair discussion. These are difficult issues, and tensions can be high.
“I would encourage everybody to look at having a neutral, outside moderator when you bring your core group together,” said Roy Alson, medical director of disaster services for the North Carolina Office of EMS. “You often have disparate groups who have individual issues, and having somebody who’s neutral to guide the process can get you over some rocks and shoals.”
PROVIDER INVOLVEMENT AND ENGAGEMENT
At all of the regional workshops, as well as in the 2009 IOM report, one of greatest priorities identified was the need for extensive engagement with community and provider stakeholders. Provider stakeholders include not just doctors, nurses, EMTs, and other healthcare providers, but also participants in other parts of the healthcare system, including payers, regulators, the media, and the public. In a true public health emergency, each of these participants will have a critical role to play in achieving optimal care, and participants found uneven levels of understanding and commitment among these groups.
“About 3 years ago our quality management team put together a questionnaire just asking what one would do in the event of a pandemic flu outbreak,” said Michael Spence of Kalispell Regional Medical Center, Montana. “From this, the ethics committee decided to develop a mass casualty group from the responses we got because we got various responses all over the map depending upon the type of person who was answering the questions.”
Spence’s group includes hospital leaders, epidemiologists, pharmacists, nurses, respiratory care technicians, emergency doctors, public health executives, hospital trustees, morticians, emergency services, and others. The group meets once a month and has worked with the local legislature to get laws passed facilitating the response to crisis standards of care.
Engaging Frontline Providers
Spence wasn’t the only one who found uneven preparations in the healthcare community. Despite all of the money and time spent on disaster preparedness, workshop participants observed that the penetration of that knowledge into the broader caregiver community is limited.
“The people who are hardest to get in the room and participate and speak are … the physicians,” said Brian Currie, vice president and medical director for research at Montefiore Medical Center. “Most of the time they have to be chased to a meeting or have their arms bent to sit on a committee.”
Several participants also expressed concern over the lack of involvement of emergency medical services (EMS) providers in the planning process. Frank Pratt, medical director of the Los Angeles County Fire
Department emphasized the importance of engaging EMS providers. “We are trapped [among] healthcare policy makers, elected officials, and citizens who are completely disconnected from the process” of planning for a disaster, said Pratt. “But we are the people who will be in someone’s bedroom at 2:00 in the morning, making a decision.”
One workshop participant cited a recent PricewaterhouseCoopers (PWC) report titled Closing the Seams. The report found that although $8 billion was spent on disaster preparedness since September 11, 2001, only 20 percent of the primary care providers surveyed believed they knew how to respond in a mass casualty situation (PricewaterhouseCoopers, 2007). That is compared to 100 percent of hospital executives, disaster coordinators, and public health departments. The PWC report highlights the fact that hospitals tend to operate in silos where personnel and information are not routinely shared. There is also no standard core of knowledge or credentialing regarding disaster preparedness.
The obvious answer to the problem is to regularly engage in training exercises. But given how stretched most doctors are already, getting them to take part in training exercises or think about disaster preparedness is nearly impossible, participants said. This was a rare corner of the topic in which there seemed to be few “best practices” from which to draw.
Asha Devereaux, a pulmonary and critical care physician in Coronado, CA, laid out some of the issues involved in engaging doctors in the issue of crisis standards of care (Box 9).
For most caregivers, however, a primary concern is time. Doctors and nurses are simply busy, working to save lives today, and do not have much time to plan for hypothetical disasters in the future.
|
BOX 9 Engaging Doctors Barriers to Understanding
|
|
Potential Solution Educate physicians in language and venues in which they commonly receive information (avoid silos):
|
Because of this, Peterson of the ANA noted that events such as the 2009 H1N1 virus must be seized as opportunities for on-the-job, real-world training. “The realities are in our day-to-day lives: Most nurses and other providers are busy … [and] the ability for them to take time off to really be able to engage in education … is very limited. How do we use teachable moments … as a way of engaging people in the conversation?”
A second issue is simply culture. Many workshop participants worried that physicians and nurses will resist the very concept of crisis standards of care, and will tend to push off the idea and assume that the resources will eventually be there. In a training scenario, you can remove those resources one by one until you arrive at a critical decision point. But convincing providers to actually face the reality of the situation could prove to be a major issue.
Then there are those who simply don’t want to address the issues. “I hear providers … say ‘Well, you know, if that’s what I am going to be expected to do, I am sure as heck not showing up for work,’” noted Phillips. “Yes, someone has to do it, and I understand it is important, but it’s not going to be me. That’s not what I came into health care to do.”
There were further concerns on how to engage doctors and caregivers outside the hospital setting. “Ambulatory physicians, infectious disease physicians [and others] have not really been at the table,” said Currie. “How do you reach out and embrace people still practicing … anecdotal medicine … one patient, one problem, one process?”
One idea did rise to the top of the discussions: Pay providers to train. “I think we do what we’re paid to do, and there are few financial incentives to exercise,” said Shawn Rogers, director of EMS from the Oklahoma State Department of Health. Rogers went on to propose an innovative solution: “I think that if regular exercise participation was a condition of Medicare participation, we’d see a whole lot more of it.” Cantrill of the Department of Emergency Medicine at Denver Health
Medical Center added that in order for that to be possible, the Centers for Medicare and Medicaid Services (CMS) would have to allow reimbursement for preparedness. He noted that this would be a critical step forward for hospital preparedness.
Even when training isn’t possible, however, keeping providers in mind when designing the systems and methodologies will ensure more consistent implementation of crisis standards of care. When imagining a scenario that would require removing patients from life-sustaining care, Devereaux noted some of the following requirements: “We will need security to protect us from the demands of unrealistic family members. We will need transparency to assure us that other facilities are operating in the exact same manner. And we’ll need constant communication and updates.”
Others worried that, even with the best protocols, ensuring that doctors will follow through with the crisis standards remains a significant challenge. “When the rubber meets the road, when you have to make a decision to pull a patient off a vent, are we going to have individuals who are going to be willing to do that?” asked Cantrill. “I think it’s a real challenge.”
Hospital Officials
For hospital officials, the reasons for not being engaged are similar—a lack of time, a lack of funding, and a concern about committing to rationed care—but the methodology for encouraging their commitment is different.
“All this discussion fits into the broader question of whether your business model will survive the next catastrophe,” said Hanfling, putting himself in the administrator’s shoes. “At the CEO [chief executive officer] level, they want to know that there is a revenue stream coming in after the fact. The reason we’re looking at this is because we’re talking about protecting our facilities, protecting our staff, providing an ongoing capability to our community-based mission.”
Again, the opportunity for on-the-job training does present itself. Shawn Rogers, director of EMS for the Oklahoma State Department of Health and the President-Elect of the National Association of State EMS Officials, spoke of the experience of the Oklahoma City hospital groups, and how it took not one—but two—disasters to force executives to confront the need for a coordinated response:
[After the Oklahoma City bombing, there] was no system to share patients and appropriately distribute them. We, the medical community, in our after-action critique said, “[W]ell, we really need to do something about that” and then we didn’t.
Four years later we had a big tornado and there were again centers where the tornado hit and there were lots of casualties and those hospitals nearby were again swarmed and the hospitals further out were not appropriately used. So we again had after-action reports and we got together and we said we really need to do something about that and we did.
We put together a metropolitan emergency resource center whose role was to coordinate where patients would go in disasters. The way we got the hospitals to buy into that was to ask for each hospital to send a representative to be trained and [be able to be activated] during a disaster. This representative would come down and man the resource center, one rep. from each hospital, to serve as the speaker to that facility in that disaster. The next time we had a tornado, in 2001, that hit down in the metro area and our response system worked rather well. Engaging facilities in that kind of a forum was effective for us.
PUBLIC ENGAGEMENT AND EDUCATION
Many participants noted the importance of public engagement and education on this very difficult issue. If the public is not engaged in developing crisis standards of care, if it is not involved in evaluating the harsh choices that must be made, if it does not understand and agree with the ethics and logic surrounding those choices, even the best laid plans will fail.
“If you are going to alter how you deliver care, your public has to be on board,” said the CDC’s Levy. The public “will only follow [plans] if they (a) know about it and (b) have bought into it.”
Melba Moore, commissioner of health from the City of St. Louis Department of Health, emphasized the importance of engaging the public. “You must be in the community. You must get out there because there is a history of distrust in the community of providers.” Without that relationship no decision will get buy-in from the public.
Yet most workshop participants agreed this had not yet occurred.
“The public is … uneducated on this topic,” said Brinsfield of DHS. “That’s our fault because we’re not sharing the information with them in a way that they can process and understand.”
The question, though, is how to bring them into the discussion in an efficient, effective, and constructive way. Unfortunately, the easiest and most obvious approaches do not seem to work.
The Montefiore-Einstein Center’s Powell noted that that bringing big community groups together to discuss these sorts of issues can be ineffective. “This is a really frightening issue, and if you’re going to have 200 people together who have not spent their work lives contemplating this issue, it really slaps you in the face,” she said. “You’re going to have a couple of people who are really distressed in a not particularly productive way, and it can really derail that kind of meeting.”
Powell recommended holding smaller focus group meetings, perhaps relying on community groups or faith-based organizations as a centralizing mechanism. Given how critical the public role could be in directing an emergency response, however, workshop participants explored two approaches, discussed in more detail below.
Changing the Culture of Preparedness
The most comprehensive idea—and one which arose in multiple regional meetings and from multiple providers—was to use the heightened awareness after recent tragic events like Hurricane Katrina and September 11 to institute a new “culture of preparedness” in the community.
“I think one of the goals we as a group should have is to introduce preparedness into the national educational curriculum,” suggested James Prudent, an emergency physician from New Jersey. “Just like patients come to us with something they’ve read online and compel us to go and learn about [new diseases] … if the public is energized to learn these things, then we too would be energized to learn these things.”
Indeed, Shawn Fultz, senior medical advisor at the VHA, suggested creating a whole new culture around civil defense for the 21st century, an idea that was first broached during the Forum’s March 2008 Workshop on Dispensing Medical Countermeasures (IOM, 2008). Just as children in the 1950s learned to “duck and cover,” citizens today would learn how to respond to a bioterror attack, a pandemic flu, or a natural disaster.
It only takes a minute to realize how much a prepared population benefits the public health response. Models have suggested that a very
large portion of the patients coming to the hospital during emergencies do not need urgent care. Preventing even half of these patients from clogging the system would free up tremendous resources. Similarly, having an informed public that understands that crisis standards of care are uniform across regional boundaries would discourage the inefficiencies and potential chaos that go along with “hospital shopping.” Most importantly, an informed public should be better able to accept the sacrifices required in a mass casualty event, including understanding that resources may not exist to provide uninhibited care during the heart of the emergency.
“People are hungry for information,” said Inova’s Hanfling. “They’re hungry for credible information that comes from trusted leaders.”
If we can build a shared commitment and even a sense of civic responsibility, we will show the difference between panic and order, chaos and efficiency, and a population that works with the healthcare system during an emergency versus a population that revolts against the implementation of crisis standards of care.
“People are going to vote with their feet,” noted Phillips. “How do we engage the public in this decision? [Some believe] we aren’t really ready to engage the public yet because we haven’t gotten our act together yet. But you could take it on the other side and say, well, if the public was part of getting our act together, then we wouldn’t have to wait and then convey something to them.”
The task of working with the public is a large one, and it’s one for which users did not have a firm solution. Some even called for federal help. “I think it would be very useful from the federal level [to have a] tool kit that could be deployed regionally with health literacy, language barriers, and cultural competency … that could be modified per region … to address the specific cultural, spiritual, and community issues unique to our locals, but that would provide standardization in terms of the kind of information we are providing throughout the country,” said Fleming.
Elected Officials and the Media
The entity of the mass media is both a tremendous tool in a crisis and a significant challenge. The media will control the messages that most of a population receives in a crisis, and many workshop participants suggested that they should be assiduously courted as key stakeholders.
“It is critical to bring the media in early, because if they’re in early and are a part of the planning process and see what goes into it, they’re going to be much better prepared to support you during the time of disaster,” said Nancy Auer, special medical advisor to the CEO at Swedish Medical Center in the state of Washington.
Workshop participants emphasized the importance of having a public information officer with the task of developing relationships with the media before a disaster strikes, so that those relationships can be leveraged after a disaster occurs. Others noted the importance of delivering a consistent message: Something simple, such as a universal agreement that the public should “shelter in place” and avoid the hospital unless they are truly critically ill, could prevent a wave of non-critically ill patients from besieging a facility.
“We had an approach in New York City … that we affectionately called ‘One Voice,’” explained Walt Disney’s Gabriel, who served previously as deputy commissioner for planning and preparedness for the New York City Office of Emergency Management.
The “One Voice” concept assumes that the public and the media will want to hear from a recognized leader—generally an elected official—during a disaster; think of then-Mayor Rudy Giuliani’s role during the September 11 tragedy. That recognized leader may or may not be an expert on medical events, but if that leader is surrounded by the right people—legal counsel, hospital administrators, influential physicians, public health officials—and provided with consistent and reliable messaging, that “One Voice” will be able to drive forward the single message and inform the community of evolving standards.
This is the reason that efforts must be made to engage directly with elected officials and the media before events take place.
As with doctors, hospital administrators, and others, participants worried that elected leaders will blanch at the concept of implementing crisis standards of care.
DEVELOPING INTRASTATE AND INTERSTATE COOPERATION AND CONSISTENCY
Without consistency across communities, regions, and states on crisis standards of care, there is much greater potential for chaos and unfairness. Participants at all of the workshops discussed the difficult balance between developing standards and procedures based on a community’s
particular values, characteristics, and needs, and ensuring a consistent approach across neighboring jurisdictions.
Different states have taken different approaches to developing crisis standards of care. Two that were highlighted at the meeting in New York were the approaches used by Massachusetts and Virginia. “Slightly different approach(s), though in reality our goals are similar,” stated Lisa Kaplowitz, health director from the Alexandria Health Department in Virginia (Box 10).
“[Standards] should not be imposed from above,” cautioned Powell of the Montefiore-Einstein Center. “But there does need to be a kind of crosschecking and a network of cooperation across the country so that plans are reasonably interchangeable, and there is an agreed-upon system or what people think are consistent and fair allocations of scarce resources.”
Without consistent standards, patients will shop for hospitals with the most advantageous treatment protocols. Without consistency, individual physicians may be exposed to increased legal liability from patients who believe they could have received better care at a different hospital down the road. Without consistent standards and interneighbor cooperation, there cannot be a fair allocation of resources among neighboring facilities or by tapping into emergency reserves of supplies.
However, at each level of organization, from the departments of individual hospitals to communities, states, and regions, the issue becomes progressively more complicated. “If you think you have a problem trying to get adjacent hospitals to work together or communities to work together, imagine trying to do this across multiple states,” said Terry Schenk, a consultant for the Florida Department of Health.
Several participants described existing mechanisms for interstate collaboration and cooperation that could serve as a basis for broad geographic coordination of crisis standards of care. In addition, consistency was a major theme of the IOM’s letter report.
|
BOX 10 Two States: Two Approaches Massachusetts In 2006 The Commonwealth of Massachusetts convened a statewide committee to look at alternate care facilities. Initial and ongoing concerns were liability in a below-optimal resource environment and creating guidance that would help engender trust with the public. To that end:
SOURCES: Levin et al. (2009); The Commonwealth of Massachusetts Department of Public Health (2007). Virginia By contrast, the Commonwealth of Virginia’s approach to crisis standards of care (or “care in situations of critical resource shortage,” as Virginia calls it) is driven outside the umbrella of state government, instead delegating the planning authority to the medical community. To that end:
SOURCE: Virginia Department of Health (2008). |
FEMA Regions
A number of workshop participants highlighted the Federal Emergency Management Agency (FEMA) Emergency Response Regions as one way to subdivide the nation and create partnerships across state lines. FEMA divides the nation into 10 emergency response regions, each of which is tasked with protecting institutions from all types of hazards by
developing a program to mitigate and respond to disaster scenarios. The regions have dedicated staff as well as on-call “reservists,” who can be brought in to support regional response efforts.
The Region IV ESF-8 Unified Planning Coalition, bringing together representatives from Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina, and Tennessee, received particular attention at the Orlando conference. “They have as their mission a collaborative effort to really look at … all hazards planning,” added Terry Schenk, speaking of the same issue. “One of the things they are really trying to do is establish some consistency state to state.”
James Blumenstock, chief program officer for public health practice at the Association of State and Territorial Health Officials said, “There are six or seven other regional coalitions around the country that exist primarily for the same purpose.… They have different levels of investments of leadership and they are really literally and figuratively all over the map with regards to the way they handle particular regional issues. I think that’s a diamond in the rough for the purposes of building stronger regional coalition and coordination.”
An obvious extension of this thinking, of course, is to create consistency from region to region. Disaster and diseases do not honor state lines or arbitrary regional designations. Blumenstock and others noted that, in an ideal scenario, regional and state-level planning committees would approach the problem of regional preparedness within a shared framework. This idea of regional and local coalitions operating under federal or other guidance was a theme that appeared again and again throughout the presentations.
The All Hazards Consortium
In the National Capital Region (see http://www.ncrhomelandsecurity.org/), eight states have banded together to create an “All Hazards Consortium” that seeks to build collaboration to address the management of catastrophic events in and around the region. The states are Delaware, Maryland, New Jersey, New York, North Carolina, Pennsylvania, Virginia, and West Virginia. Their successes provide yet another model for approaching the problem.
As workshop participants noted, the states involved in the All Hazards Consortium secured a regional catastrophic planning grant from HHS. But rather than applying that grant to traditional planning exer-
cises, it applied much of the money to developing a software system that will allow all of the emergency management organizations in those states to share information in real time. This software, updated and functioning, has been used for planning and training exercises, and stands ready to support event management and recovery the next time disaster strikes, explained Floyd Russell, Homeland Security liaison at the Office of the Vice President for Research and Economic Development at West Virginia University.
The Interstate Disaster Medical Cooperative
The Interstate Disaster Medical Cooperative was created in 2007. The mission of the cooperative, as Timothy Conley, preparedness planning director at Western Springs Fire Department and Emergency Medical Services, IL, explained at the Chicago workshop, is to provide a forum to allow states to network with one another and share best practices. “The purpose of the interstate disaster medical cooperative is to establish for state medical teams a common framework and a way to work together,” Conley said, “a way not to reinvent the wheel.”
In addition to monthly teleconference calls and face-to-face meetings, the group is working together to create a standardized model of state operating procedures to promote interoperability and smooth the process whereby one group can surge to help another. The group also aims to identify both the special skills and the special resources housed in each state, to ensure a more robust regional response to specific emergencies. “Every state has a little bit of a different strength,” said Conley, who noted that 20 states had signed up to participate in the cooperative.
The organization has created working groups to tackle specific issues, such as establishing and credentialing a Medical Reserve Corps or standardizing best practices for alternative care facilities. The group is also sponsoring a study on pediatric care during emergencies. In short, it is a grassroots organization tackling issue after issue in an effort to link people in an enhanced model of disaster preparedness.
Village-to-Village Communication
Despite all the planning—and there is clearly a tremendous amount of solid groundwork being done—many participants worry that the
boots-on-the-ground training has yet to start. There is a concern that, even where a regional system may be well fleshed out, local healthcare officials may be in the dark.
Conley brought up the example of his own town, the Village of Western Springs. When the H1N1 virus emerged, Western Springs developed an emergency response plan and laid out new protocols that took actions such as limiting provider interaction with the public to reduce illness; the neighboring town did nothing. Meanwhile, a third village in the area began requiring responders to wear masks on each EMS call. That level of confusion only served to foment panic in the public.
Conley also expressed serious concern that the local responders are not integrated into the planning taking place at the upper levels. “For the fun of it, I went out to one of the medics and asked them, ‘Hey, what’s our alternate care site for this region?’ And guess what their answer was: They have no idea. They don’t know that they won’t be transporting cardiac arrest. They don’t know that they will be making triage decisions whether somebody goes to a hospital or an alternate care site,” Conley said.
Some level of just-in-time training on issues like this is surely inevitable: plans change, employees come and go, and training can never be totally universal. But the point is clear: planning cannot simply take place in the upper reaches of hospital departments, but must reach down to providers, emergency medical service providers, homecare nurses, and other critical points on the healthcare chain.
Communications and Consistency
Communications among stakeholders during an emergency was a critical issue that was mentioned throughout the meetings, with different groups taking different approaches. Sometimes, the solution is as simple as having the right phone system in place.
Chris Dent, an infection prevention nurse at Saint Alphonsus Regional Medical Center in Idaho, told the Irvine workshop about the work that the Idaho Hospital Coalition had done to set up a “bridge call service.” The service allows emergency management systems to contact area hospitals, who are then required to dial into a shared conference-call number. That shared conference call serves as a confidential and reliable source on the exact nature of an emergency and the plans regarding interfacility cooperation, supply sharing, and standards of care.
“The bridge calls [let us] tell the hospitals what the real story is, not what gossip is coming in over the radio,” noted Dent. “We have not only practiced this, but have used it … including during a vaccine shortage. We used the bridge call to come up with [a plan] so that every hospital was using vaccines in the same way.”
Although no system will foresee every eventuality or forecast every concern, establishing lines of communication in advance can improve the application of consistent crisis standards of care during an emergency. At the workshop in Florida, Lori Upton, assistant director of emergency management at Texas Children’s Hospital, described the circumstances that led to increased coordination and communication among stakeholders in her region (Box 11).
|
BOX 11 A Lesson Learned “Back in 2001,” said Lori Upton, assistant director of emergency management for Texas Children’s Hospital, “before the collapse of the World Trade Center, we had a little storm that came over Houston called Allison. It dropped 34 inches of rain on us and it completely wiped out the Texas Medical Center in downtown Houston … which includes 13 large facilities with medical schools attached to it. So we wiped out over 5,000 hospital beds in one evening, and it was Labor Day weekend. We learned about evacuations of health care. We learned about alternate standards of care for patients that were leaving an acute care facility and going to an alternate care site or going to a nursing home because they were stable and the nursing homes had beds. What we didn't have at the time is we didn't have a coordinating entity: one person or one voice that was able to get all of the information out to the hospitals to let them know what's happening, what the standards are right now, and who's going where, and who's going to be moving when. As a result, we formed a regional hospital-preparedness council … and now it includes every hospital in the region. It includes our EMS providers, our ME's offices, our VA and EMS liaisons, our offices of emergency management, our public health, medical societies, our nursing schools, our medical schools … all of our partners that we may touch. They come together once a month. … We [now] have a catastrophic medical operations center that falls underneath our public health authority. We have one coordinating entity that our hospitals look for, EMS look for regarding transportation, for asset utilization, etc.” |
THE ROLE OF THE FEDERAL GOVERNMENT AND NATIONAL LEADERSHIP
The role of the federal government in helping to guide and facilitate the development of crisis standards of care was highly debated at the workshops. Some participants worried that a heavy-handed approach from Washington could derail more in-the-trenches attempts to develop plans at the state and local levels and lead to policies that are inconsistent with state and local values and needs. Many participants, however, believed some level of guidance at the federal or national level would be helpful. They saw a range of ways that federal or national leadership could facilitate the development of fair and consistent crisis standards of care policies and protocols, and could help reduce unnecessary duplication of effort.
On the practical end, there was a widespread call for the federal government to perform a role as “chief information coordinator” on the topic of crisis standards of care. “There are people all across the country and states, at county and other facility levels, who really are kind of reinventing the wheel,” said Montefiore’s Powell. They are “starting all over again, trying to do the literature search and figure out what’s going on. It’s an enormous investment of time and manpower across the country when in fact there are scholars who at least have some of that information as ready knowledge.”
Indeed, that insight was demonstrated tangibly at the workshops, where dozens of state and local plans were presented, each of which required huge investments of time and energy to produce, and each of which in many cases ended up with similar conclusions. If a way to index that information in a single location as a resource was established, Powell and others suggested, it would massively improve the efficiency of developing these guidelines throughout the nation.
Federal or national involvement would also provide a level of legal, societal, and practical protection that cannot be achieved at the lower levels of leadership. Many people at the workshops noted that there may be some issues for which federal or national involvement is the only practical choice.
“These are politically explosive issues,” noted Powell. “At every single facility and even at the state level you’ll have people who either don’t want to talk about it or just come up with vague guidelines … because it’s a liability risk.” What’s needed, she suggested, is an acknowledgment at the highest level that the issue is worth talking about, and that the
uncomfortable must be confronted. “I think the higher you come from in saying that, the more security there is in believing that will be an acceptable plan.”
Looking at the bigger picture, participants noted that having broad federal guidance could help establish consistency from state to state and region to region. The unfortunate reality is that anything other than national guidance risks running into “border issues” in areas where one region, state, or community butts up against another. A coordinating policy that bridges those gaps and establishes a framework of consistency would be immensely valuable.
Many workshop participants praised the aforementioned work of AHRQ and ASPR to establish the outlines of a framework in their 2005 report, Altered Standards of Care in Mass Casualty Events and 2007 report, Mass Medical Care with Scarce Resources: A Community Planning Guide (AHRQ, 2005; Phillips and Knebel, 2007). These documents, however, only go as far as making broad recommendations about the scope and challenges that should be considered and laying out preliminary implementation considerations. Many workshop participants wanted more.
“We’ve got to start identifying players and start trying to get to some specificity of what that national guidance could look like,” said the ANA’s Peterson. She added that establishing evidence-based research for making decisions about crisis standards of care represents a massive and immediate opportunity for a nationally convening organization. Much of the work on crisis standards of care and emergency response is driven by principles and best guesses; there is little existing evidence about what works and what doesn’t in various situations.
These knowledge gaps extend from treatment protocols to triage to equipment usage. For example, there is little evidence about the use of SOFA scores for predicting outcomes in pediatric or geriatric populations, or about which simple treatments achieve the best outcome at acute care facilities during a pandemic influenza.
All of those things can be known to some extent using historical data on past tragedies or studies in non-disaster scenarios. But the unfortunate reality is that there has been neither the funding nor the initiative to do much direct, evidence-based disaster medical research.
One thing was clear from the workshops: Most participants did not want the federal government dictating the specifics of how to implement policies.
“One can’t get too prescriptive on the actual protocols, for a couple of reasons,” said Kristi Koenig, director of public health preparedness at University of California–Irvine. “One, the solutions are going to vary from community to community. And two, a lot of these are evolving situations, where resources are coming in and getting more scarce throughout.”
But still, the opportunity for the federal government to establish broad principles, roles, and objectives, as it did in a strong first step in the AHRQ documents—and then to take that one step forward by serving as a convening mechanism and research coordinator for multiple parties—is evident. Workshop participants suggested the time is now.
“In the context of the broader picture of healthcare reform, and with a shift in the administration … I’d like to see leadership from the top really help to bring this forward now … on a national level,” said Inova’s Hanfling.
Workshop participants’ call for federal and national leadership to provide practical, more detailed information to advance the development of crisis standards of care protocols, and to facilitate intrastate and interstate consistency, formed the basis for the subsequent Institute of Medicine committee report entitled Guidance for Establishing Crisis Standards of Care for Use in Disaster Situations (IOM, 2009). This letter report, summarized in Appendix B, provides guidance on ethical considerations; community and provider engagement, education, and communication; legal authority and environment; indicators and triggers; and clinical process and operations. The committee calls on states to work to ensure consistency in the implementation of crisis standards of care throughout the state and among neighboring states.
The Veterans Health Administration
The VHA was mentioned by a number of participants as both an untapped resource for support during emergencies and an underused resource for planning national, regional, and neighborhood collaboration.
The VHA runs more than 150 hospitals and some 800 outpatient medical clinics around the country, as well as 200-plus “Veterans Centers.” At each regional meeting, VHA representatives made a point of stating that they would be available—in most scenarios—as a resource for the community during disasters.
“We have a requirement to support both internal and external missions,” said Richard Callis, deputy chief consultant for planning and operations at the VHA. “We also have a responsibility under the emergency management support function … that requires working throughout the VHA system to bring clinicians to support field operations” during a disaster.
Several participants reiterated that the VHA actually has staff with full-time responsibilities for disaster preparedness, fulfilling a statutory mission for emergency management not just for the VHA system, but throughout the whole community. “There is one person assigned as the regional emergency manager for each FEMA region,” noted Fultz of the VHA. He added that these employees oversee additional staff.
The VHA representatives at the workshops suggested that communities looking to develop standardized supply and response tactics should tap into this VHA network aggressively. While it operates in multiple regions and hundreds of communities, it is also a single, national, integrated system. Therefore, several workshop participants suggested, it represents a unique opportunity to facilitate the development of consistent crisis standards of care across the nation. The IOM letter report also reached this conclusion (IOM, 2009).
The Department of Defense
One other way that the federal government can lead, many said, is by leveraging its position as a large provider and purchaser of healthcare services. That leadership can come through direct purchasing power; as noted earlier, some believe that provider participation in the Medicare program should be predicated on adequate disaster preparedness and emergency management training. Or it can come from serving as a model for other regions or localities in how to develop crisis standards of care. Wayne Hachey, director of preventive medicine for the Office of the Assistant Secretary of Defense, presented at the Irvine and Orlando workshops.
The Department of Defense is “the largest federal agency with a healthcare system,” Hachey said. “Throughout our DoD guidance, we’ve recognized that we will have to establish alternate standards of care [during an emergency] … and those standards of care will not be consistent with today’s standard.”
“We don’t have a DoD-wide standard,” Hachey explained. “What we’ve told folks is that their standards are going to mirror, at least as a baseline, the standards of the civilian community.”
In other words, the DoD program recognizes that each DoD facility has different staffing, different physical plans, a different population to serve, and different equipment and resources. So rather than forcing a top-down standard, it gives hospital administrators the opportunity to adapt their existing standards to the situation at hand. The only caveat, mentioned above, is that those standards be at or above the level of the surrounding community (Box 12). “Rather than being prescriptive, we gave them essentially rules of engagement in establishing altered standards of care,” said Hachey.
To help create and monitor those standards, each installation within the DoD has a Public Health Emergency Officer with responsibility for advising the station commander during a significant public health emergency. This officer also coordinates with the local community to ensure the military and civilian response plans are integrated. Again, the IOM letter report called on state and local officials to coordinate with DoD facilities in the development and implementation of their standards of care protocols (IOM, 2009).
“When we developed guidelines for prioritizing care … the request from our providers [was] asking for both prescriptive guidance but probably more importantly [was asking] for permission to make those kinds of decisions,” Hachey said. “So we gave them broad guidance, gave them sanction, made sure that they made their decisions transparent … [and] mandated that their standards of care at least as baseline be the same as their local standards of care.”
|
BOX 12 Department of Defense Resource Prioritization Policy
|
ETHICAL CONSIDERATIONS
The ethical issues in situations with scarce resources and crisis standards are both challenging and fundamental. They are challenging, as one workshop participant put it, because they contradict many of the values we hold dearest, such as providing each patient with the best available care.
But the ethical issues raised by these questions are fundamental for other reasons. They are fundamental because if we don’t act in accordance with our ethical principles, the repercussions both for individuals and the society after the fact will be enormous. They are fundamental because our ethical principles serve as the foundation of our laws. They are fundamental because people will only act and sacrifice if they believe they are operating in an ethical system, and that individuals are being treated with fairness and transparency in the full view of the law. In addition, they are fundamental, quite frankly, because many of the decisions contemplated will be made with imperfect information—they will be best guesses. Those guesses, in the absence of firm evidence, will need to be made based on a shared ethical construct.
As the workshops revealed, the work done on crisis standards of care focuses a great deal on achieving consistency, in part because consistency and fairness are integral to any ethical system. The 2009 IOM letter report outlines seven ethical considerations that are central to the development of ethical crisis standards of care protocols: fairness, duty to care, duty to steward resources, transparency, proportionality, and accountability (IOM, 2009). However, applying the ethical framework is difficult because these are challenging questions that rarely have obvious, singular “right” answers.
Powell of the Montefiore-Einstein Center presented the work her committee did when establishing an ethical framework for ventilator allocation during public health emergencies in New York (Powell et al., 2008). One question that came up immediately in the discussions, she said, was whether healthcare workers would receive priority access to ventilators during an emergency.
The points in favor of such a policy are obvious: Healthcare workers take extra risks during public health emergencies, especially in infectious situations such as a pandemic flu. If they are not given priority access to care, some may not show up to work. If healthcare workers don’t show up to work, fewer people will get care. It is a logical, reasoned argument for granting those workers priority access.
On the flipside, Powell noted, plenty of people take risks. Those include non-physicians inside and outside the hospital, such as custodians, nurses, respiratory techs, EMTs, and more. “You include all those people, and if your crisis is bad enough, I think you just ran out of ventilators and nobody in your community has them, only the healthcare workers.” Moreover, said Powell, if a ventilator triage program is structured based on employment, children are excluded.
A continuing question is that of priority, Powell added. Too often, she suggested, the people who write the rules for priority access put themselves at the top of the list. She cited one case where the rules were drawn up by a legislating body, and somehow, elected officials ended up at the top of the list.
The problem, of course, is that arguments can be made for many different constituencies. As a general rule, if the people making the prioritization list end up at the top, the community is unlikely to buy in to the program.
For the New York standard, Powell’s group decided that access to ventilators would be based solely on medical evaluations. Rather than granting healthcare workers priority access, New York decided to do more to protect them from getting sick in the first place.
It’s important to note that Powell wasn’t necessarily positioning New York’s decision as “the right one.” But it was “a right one” because it reflected the considered values of the community.
Many workshop participants stressed the importance of community values and the need to involve communities in the ethical planning process before a crisis hits.
Fortunately, as the workshops revealed, there is a tremendous trove of research that can be tapped into regarding the ethical issues surrounding crisis standards of care, including the work by Powell and many others (DeBruin et al., 2009; IOM, 2009; Powell et al., 2008; VHA, 2009a). Tools, guidebooks, and online planning systems can help communities walk through the process of developing ethically sound crisis standards of care (New Jersey Hospital Association, 2008; VHA, 2008b). One tool that multiple users pointed to was the IntegratedEthics tool offered on the website of the VHA’s National Center for Ethics in Health Care (VHA, 2009b). Developed by leading experts in the field and tested in a number of scenarios, it was highly recommended as a good starting point for communities.
But this work needs to be done before disasters strike. In the heat of the battle, there won’t be time to raise community awareness or think
through the ethical implications of each answer. That can put caregivers into impossible situations with extraordinary potential repercussions.
“You need to be able to give your workers at least one right answer,” said Powell. “It’s true that there’s not only one right answer, but [you don’t want to] make them do the wrong thing.” More work is needed on allocation of scarce resources, workforce issues, community involvement, and consistency.
Either way, ethical requirements come first, and must be integrated from the beginning.
LEGAL ISSUES FOR CRISIS STANDARDS OF CARE
Legal concerns hover over every issue in disaster planning and crisis standards of care. “Laws absolutely pervade emergency responses at every level of the government,” explained James Hodge, then executive director at Johns Hopkins’ Center for Law and the Public’s Health, one of several legal experts who presented at the four regional workshops. “Laws determine what constitutes a public health or other type of emergency; they help create the infrastructure through which we respond, prevent, and detect these emergencies; they authorize the performance or non-performance of various different actions by a host of different actors; and they flat-out determine the extent of responsibility for potential or actual harms that arise during emergencies.”
Planning ahead to ensure that the legal environment will support an effective, fair, and consistent response is a crucial step in preparing for crisis standards of care during an emergency event. Workshop participants found that this area still needs a significant amount of work.
Legal Liability
Most states have provisions that limit legal liability during emergencies. Ball from South Carolina outlined a number of laws that help limit medical malpractice liability during emergency situations in South Carolina, including the following:
-
Emergency Health Powers Act (44-5-570, (C)(1)): “Any health care provider appointed by [the South Carolina Department of Health & Environmental Control] … must not be held liable for
-
civil damages as a result of medical care … unless the damages result from … circumstances demonstrating a reckless disregard for the consequences.”
-
Medical Malpractice Act (38-79-30): “Volunteer (non-compensated) health care provider … not liable for any civil damage for any act or omission resulting from the rendering of the (medical) services unless … act or omission was the result of … gross negligence or willful misconduct.”
Similar laws exist in most other states. But although these laws represent a good start, they come with one major drawback during crisis standards situations. Raymond Pepe of the Uniform Law Commission (ULC) noted that the laws “by and large immunize ordinary acts of negligence while not immunizing gross negligence or willful disregard of standards of care.” Despite the drawbacks of this limitation, several participants added, it is also necessary to discourage harmful behavior and protect patients from those who do not act in good faith during disaster responses.
Crisis standards contemplated include not offering or discontinuing life-sustaining treatments such as ventilators as part of a broader triage program. “When we willfully and knowingly withdraw or withhold life support, knowing there may be a bad outcome, we tread that line of willful misconduct,” said Cheryl Starling of the California Department of Public Health. Starling and others noted that this is one of the key barriers to getting healthcare providers and facilities to come to the table to discuss crisis standards of care and disaster preparedness.
These issues, she said, make “lawyers run for the hills and refuse to let people even talk about this … because [many people believe] you’re setting yourself up for negligence and willful misconduct.” This fear is especially strong with regard to the most extreme situations that involve the need to discontinue life-sustaining treatment in some patients.
These issues can also make healthcare providers unwilling to act during these emergencies, even with the clearest directions in place by top-level public health administrators. If you can’t solve the legal liability issue, many noted, you can’t get anywhere.
Fortunately, a great deal of work has been done on this issue at both the federal and state levels, creating a reference body of potential options for various localities to explore.
Addressing the Liability Problem
The first question that must be asked when approaching the problem of legal liability, Pepe said, is what legal liability is based on. “An accepted community standard of care grows out of either custom or practice, or it grows out of outcomes-based research which has led to consensus with respect to how to treat certain conditions,” said Pepe. “When you’re dealing with an alternative standard of care, you’re dealing with something fundamentally different. There’s a need to have clear legal recognition that these alternative standards exist and that practitioners are authorized to follow them.”
It is important to note that there is a critical distinction between legal and medical standards of care (Box 13). Starling noted that the term “standard of care” actually comes from a legal setting, not a medical setting, defining the duty to provide a minimum acceptable standard of care. “The medical standard of care may be higher than that, but defining the legal bare-minimum of that standard of care … and analyzing how that will change during emergencies … is a critical issue that requires more work,” Starling said.
Participants discussed a variety of ways in which the actual legal protections could be achieved.
|
BOX 13 Medical and Legal Standards of Care Medical Standards of Care: The type and level of medical care required in specific circumstances by professional norms, accreditation or other requirements. Legal Standards of Care: The amount of skill that a medical practitioner should exercise in particular circumstances based on reasonable and common practice in medical care. |
Deputize Physicians
James Geiling, chief of medical services at the White River Junction VA Medical Center, VT, noted that some states have simply “deputized” physicians during states of emergency, or the federal government can make them federal agents. These actions can be enacted rapidly, and those deputized as state agents receive the state’s “sovereign immunity-type protections” that exist in many jurisdictions.
The complication of this action is that these deputized workers become the legal agents of the state or the federal government, and they must therefore be prepared to perform as the state or federal government mandates, not necessarily what their own healthcare institution or other usual employer might require. That concept can make many healthcare institutions and employers very uncertain, and they may be unwilling to cede that control.
Enact Comprehensive Liability Protection
Other states have taken more nuanced approaches. Virginia has enacted a comprehensive liability protection program that goes into effect if there is a declaration of emergency on behalf of the state government and it has resulted in resource shortages. Critically, the Virginia law does not require a separate act by the legislature to go into effect, but can be put into effect by the governor’s credo.
Montana passed a bill earlier in 2009 “that very much touches altered standards of care in an emergent situation if declared by the governor and protects us and gives us some immunity—and it’s different from the code of practice that we have,” noted Orlando meeting participant Michael Spence of Kalispell Regional Medical Center, MT.
A theme throughout the workshops was the concept of moving up the political chain of command when empowering this kind of legal liability protection, and putting the declaration of the emergency in the hands of a single powerful individual, such as a governor. Colorado, for instance, has draft executive orders that the governor can enact and that provide blanket protections for everything from license issues to who can dispense medicine.
Finding ways to make the standards as consistent and evenly applied as possible will be critical to mitigating liability for providers who are trying to do the right thing. That means, for example, having liability
protections that extend not just to doctors and nurses, but to triage officers, resource teams, and all other parties involved in the healthcare process. Persons involved in triage were of particular concern because triage is where many of the most difficult decisions must be made. Participants mentioned the challenge and importance of developing consistency across state lines, and this was also a theme in the 2009 IOM letter report (IOM, 2009).
Credentialing and Scope of Practice
In contemplating the legal ramifications of enacting crisis standards of care, one issue that was raised repeatedly at the workshops was the credentialing of out-of-state healthcare providers. Other means of augmenting the core caregiver community were seen as critical, including expanding the types of care that certain healthcare providers can provide and supporting retired healthcare workers who are interested in volunteering during times of crisis.
Participants discussed the critical importance of having sufficient, qualified personnel during an emergency. Finding ways to expand the size and scope of the caregiver community, while maintaining and supporting a community-based vision for crisis standards of care, was seen as a critical task.
One group that has taken the lead on this work is the Uniform Law Commission, an interstate organization that has done extensive work on the credentialing issue and has developed a draft law—the Uniform Emergency Volunteer Health Practitioners Act—that states can adopt (Box 14). It includes a robust system for the interstate recognition of healthcare licenses.
“It takes the fundamental approach that there is no reason that if your state is affected by a disaster you need to review on a case-by-case basis the credentials of people who are coming in from other states,” said the ULC’s Pepe.
The law limits the scope of medicine that these outside practitioners can practice, but it takes a common-sense approach of smoothing their entry into the disaster response. The idea is that multiple states can adopt the law in its written format.
|
BOX 14 Uniform Emergency Volunteer Health Practitioners Act
|
At the same time, statutes across the country envision expanding scopes of practice temporarily for existing healthcare providers to let them work beyond the boundaries of their traditional expertise. Pharmacists may be asked to administer vaccinations, nurses may be asked to function in the role of nurse practitioners, and emergency medical technicians may be asked to dispense medicine.
Similarly, many states have statutes that allow retired healthcare providers to provide a limited set of services, such as palliative care. These healthcare providers can be a tremendous aid during an emergency, many noted, as long as they are given tasks appropriate to their training and education.
“We polled about 10,000 different perspective volunteers back in 2006,” said Johns Hopkins’ Hodge. “Seventy percent of them, or nearly 70 percent, said that their potential exposure to liability is an important or essential fact in whether or not they’ll actually participate in an emergency.”
The math is simple: Better, clearer legal protections mean more personnel to confront a mass casualty event.
EMTALA and HIPAA
Multiple workshop participants expressed concerns about the impact of federal regulations—specifically, the Emergency Medical Treatment
and Labor Act (EMTALA) and the Health Insurance Portability and Accountability Act (HIPAA)—on the ability to respond to a medical disaster (Box 15). EMTALA requires certain hospitals to provide emergency care to all patients, regardless of their ability to pay; patients may not simply be denied care and turned away from the hospital’s doors. HIPAA governs privacy regulations and restricts the sharing of medical information. Compliance with these regulations is a significant concern for hospitals because failure to comply can result in exclusion from the Medicare program.
“How are you going to triage people to … alternate sites when you have EMTALA regulations in your face?” asked one participant, capturing the concerns of many. “How are you going to transfer people to other facilities when you have HIPAA that’s not going to let you get information back?”
To some extent, these specific concerns are already accounted for in the existing legal system. An apparently less well-known fact about the HIPAA and EMTALA regulations is that, when the HHS Secretary declares a public health emergency and the President declares an emergency or a disaster pursuant to the National Emergencies Act or the Stafford Act, HHS can issue an “1135 waiver” that temporarily suspends sanctions for noncompliance with certain provisions under both HIPAA and EMTALA.2 These waivers have been enacted in the past, and can be put in place quickly (and retroactively) during a disaster setting.
|
BOX 15 EMTALA and HIPAA EMTALA: The Emergency Medical Treatment and Labor Act was enacted by Congress in 1986 to “ensure public access to emergency services regardless of ability to pay.” The law requires hospitals participating in the Medicare system to provide medical screening examinations to patients requesting treatment for emergency medical conditions. Hospitals must also provide stabilizing treatment for these conditions, or, if such treatment is outside the hospital’s capability, provide an appropriate transfer (http://www.cms.hhs.gov/emtala/). HIPAA: Enacted by Congress in 1996, the Health Insurance Portability and Accountability Act protects the privacy of a patient’s personal health information. Medical providers are allowed to disclose that information “for patient care and other important purposes” (http://www.hhs.gov/ocr/privacy/hipaa/understanding/index.html). |
Florida’s Hood, however, cautioned about taking this comfort too far, noting that “many states have laws about medical confidentiality which are stricter than HIPAA.”
Hood and others noted that the 1135 waivers do not impact these more restrictive state-level laws. The recommendation was that states should individually evaluate their laws and put in place emergency orders to remove barriers to emergency response.
Legal Triage
Regardless of what legal rules are in place, or what standards have been agreed to, the legal landscape will be constantly shifting during an emergency, and participants will likely have to adjust their response accordingly.
Johns Hopkins’ Hodge introduced his own concept of “legal triage” to define how healthcare administrators must constantly adjust their operating procedures throughout an emergency to remain consistent with the evolving situation (Hodge and Anderson, 2008; Hodge et al., 2009). “It’s about prioritizing … legal issues in real time to construct a favorable legal environment … that facilitates legitimate public health responses during emergencies,” said Hodge. “Once an emergency has been declared, by design the legal landscape changes.… [I]t changes instantly and it can change drastically, and depending on how it changes, based on the type of emergency that we’re involved with, the legal responsibilities and liability protections and altered standards of care issues come into play.”
Hodge noted that since September 11, 2001, many new laws have been put into place governing emergency response and disaster preparedness. Forty-two states now officially allow for a declaration of disaster, and 26 states specifically define a public health emergency. The peculiarities of how those disasters are declared and what the term “disaster” actually means, legally, varies in nearly every case. Quite often there are different levels of declaration. “Your deployment, your abilities, your authorities, your liabilities, immunities are all dependent upon that level of an emergency,” explained Hodge.
In the midst of a disaster, having a legal team in place that is ready to respond to and interpret those evolving legal standards can be just as important as having the right medical triage and response teams. The message throughout the meetings was that if communities did not take care
of the legal issues, much of the other planning would be significantly less effective.
Education and Training
As well-designed and thoughtful as any legal liability protections or other crisis standards laws may be, their effectiveness rests on whether hospital administrators and their legal counsel know they exist.
A theme that emerged from the legal discussions was that the natural reaction at many hospitals is to protect against liability and limit activity, barring clear guidance otherwise. That will likely be the prevailing wisdom in the confusion sure to accompany a true healthcare disaster.
Workshop participants repeatedly observed that significant work was needed to disseminate information about legal liability protections to healthcare providers, even in those states that have tackled the problem head-on.
CONCLUSION
How can healthcare providers and facilities, with the support of state and local public health officials, the federal government, and their communities, provide the best care possible during a crisis? What steps can the health system take to avoid resource scarcity, manage demand, and minimize impact on clinical care? If these steps become insufficient, how should resources be allocated fairly and consistently? How can these steps be taken in an ethical, legal, and effective manner?
These were the questions that knitted together the four regional workshops in California, Florida, New York, and Illinois. While the individual approaches varied, participants were unified in recognizing that these were important questions, and that they were questions that had to be answered before it was too late.
A great deal of progress has been made over the past decade, motivated in part by events such as September 11, 2001, the anthrax attacks, and Hurricane Katrina. Ten years ago, hospital administrators and healthcare officials wouldn’t touch the third rail of crisis standards of care; now working groups are approaching this problem in regions, states, and communities around the nation. The workshops presented dozens of approaches, many of which shared common basic principles,
even if they differed on the specifics. National efforts from the CDC, AHRQ, and others were widely praised for laying the groundwork, even as participants identified more work that needs to be done.
These are not easy issues. The scenarios addressed at these meetings are uncomfortable. Fearsome words like “rationing” and dire concepts like discontinuing life-sustaining treatment in critically ill patients must be considered and confronted head-on, at every level—from federal oversight to local administrations—and by every party—from politicians to lawyers to primary caregivers.
Ultimately, the discussions are held with the aim of providing the best and most fair treatment to as many patients as possible during a crisis.
Healthcare providers will not have time during an emergency to develop programs from a standpoint of fairness and equity. There will not be time to develop laws to facilitate information sharing, dramatically increase staff, or provide legal liability. Any on-the-spot efforts to develop triage protocols, conduct evidence-based studies, or build relationships of trust among hospitals in different regions and communities will be impossible.
As a result, participants said, officials have a duty to plan for these scenarios. They have a duty to develop crisis standards of care protocols based on reasoned and ethical approaches that reflect the views and beliefs of the broader community. While much has been done, that work needs to be gathered into a central resource where other jurisdictions can reference and use it, and more evidence-based research is needed. Importantly, more work needs to be done to build relationships and ensure consistency in the approach of different regions and settings.
But there is more work to do, especially in some areas that will be critical during crises:
-
Palliative care planning: Caregivers and administrators need everything from simple definitions to detailed guidance on when and where it is given and who can provide it.
-
Mental/behavioral health implications for the public as well as care providers.
-
Preparedness planning for vulnerable populations, such as pediatric, geriatric, and mental health patients.
-
Public and provider engagement in the planning process.
-
Consistency across borders and regions.
“How far do we need to get in standards?” asked Phillips, summarizing the Irvine meeting. “Are they general principles that we should all be adhering to? Do we need to be setting some national standards? Should we be just aiming toward principles that ensure consistency, but allowing individual flexibility?”
Overall, participants said that the workshops had been helpful in highlighting how much work is going on around the nation on this issue, but also emphasized that much work remains to be done in order to ensure that the best care possible is provided under catastrophic circumstances.
































































