
3
Lessons from Other Systems
Workshop chair Arthur Kellermann introduced the next session, entitled “Lessons from Other Systems.” He said the previous sessions had explored the concept of regionalization primarily on the basis of conditions or diseases. This session shifts the frame and looks at regionalization from the perspective of systems of care, whether they are large geographic systems or integrated delivery systems.
Session chair Gregory Timberlake, director of the Department of Defense (DOD)/Department of Veterans Affairs (VA) Interagency Program Office and assistant deputy surgeon general for Total Force Integration, introduced the three speakers: Kenneth W. Kizer, former under secretary for health in the VA and former director of the California Department of Health Services; John Holcomb, director of the Division of Acute Care Surgery at the University of Texas Health Science Center at Houston and former trauma consultant for the U.S. Army surgeon general; and David Magid, director of research for the Colorado Permanente Medical Group.
REGIONALIZATION IN THE DEPARTMENT OF VETERANS AFFAIRS
Kenneth W. Kizer said that informal regionalization has been the norm in the United States for the simple reason that there is no health care system. He said if you’re going to have formal regionalization, you have to have a system of care. A system can be either vertically or virtually integrated, but it requires that the different types of care facilities and other resources
be connected in a predictable and consistent manner, according to specified expectations. To date, this is something that the United States overall has not had.
However, he said, there have been a number of efforts to institute formal regionalization in the United States that date back many decades. For example, the VA decided to regionalize vision impairment and rehabilitation of the blind in 1948 and spinal cord injury in the 1950s. Other examples include the trauma care system regulations that he wrote for the state of California more than 25 years ago, and the development of Emergency Medical Services (EMS) systems that occurred throughout the 1970s.
Kizer noted that a major milestone for regionalization for non-emergency conditions was a paper by Hal Luft, Alain Entoven, and others that appeared in the New England Journal of Medicine in 1979 regarding the relationship between volume and outcomes in cardiac surgery. This, he said, has been a highly controversial subject ever since and is the basis for an ongoing debate about regionalization of cardiac surgery and surgery for a number of other infrequent conditions.
Kizer focused the rest of his talk on the efforts that have been made by the VA to regionalize a number of its services. He noted that the veterans health care system was established circa World War I and is the largest health care system in the country—albeit an anomaly in that it is a national, centrally administered, government-run, and government-funded care delivery system based on a moral or philosophical view that those who have served in the nation’s armed forces should not be denied health care regardless of financial status.
He emphasized that the VA is not part of the military health care system—a common misunderstanding—but to be a VA patient you must have served in and been honorably discharged from the armed forces. He characterized the VA as very much of an academic system: 85 percent of VA hospitals are teaching hospitals and 70 percent of the physicians are university faculty members. The VA also has a $2 billion research program.
Kizer said that that many of the reforms that occurred in the VA in the latter part of the 1990s were predicated on the concept of regionalization. During that time, the VA’s approximately 1,300 facilities of various types were organized into 22 networks, or regional veterans integrated service networks (VISNs), based on criteria about how to best use its resources to serve geographically defined populations of veterans. However, as mentioned above, regionalization of specific service lines within the VA dates back as far as the 1940s.
Kizer noted that most regionalized conditions in the VA employ a hub-and-spoke wheel model. For example, there are currently 24 very specialized spinal cord injury centers and 134 primary care spinal cord centers within
the VA. Overall the VA serves about 26,000 spinal cord-injured patients each year and it is the largest single network of spinal cord injury care in the nation.
Transplants are also regionalized. In 1995 the VA established a central registry for all transplant patients. To date, more than 15,000 patients have been entered into the transplant registry, producing a significant store of information. Kizer echoed comments earlier in the day regarding the importance of registries for quality assurance and other purposes.
More recently, cardiac care has been regionalized in the VA, and quite recently the system has adopted a regionalized approach to treating multiple sclerosis and Parkinson’s disease. The VA has also regionalized traumatic brain injury in concert with both the DOD and the private sector. According to Kizer, stroke has been under consideration for regionalization for over 10 years, but for a variety of reasons it has not yet been formally regionalized. He said he expects it will happen.
Some clinical services are also regionalized, Kizer said, pharmacy being perhaps the best example. There are seven consolidated mail order pharmacies that serve the several million VA patients each year, and this is perhaps the only health care service anywhere that has been documented to consistently operate at a six-sigma level of excellence. Radiology and teleradiology support are also regionalized.
In general, he said, systems of care look to regionalize services for cases that are complex, have a high risk of death or serious disability, and require particularly high-intensity care, usually involving a multidisciplinary approach. Typically, the resources that are needed for these patients—personnel, technology, and other—are in limited supply. Regionalization is a means to optimize the use of those limited resources.
Regionalization can improve quality of care, and it can also be a means to control system costs. What is often found, Kizer said, is that control of cost and control of quality go hand in hand. For example, demonstrated economies of scale have come out of promoting mail-order pharmacies.
Kizer identified a number of issues and challenges that come with regionalization (see Box 3-1). He noted that information flow is often a challenge. This includes information needed to take care of an individual patient or deal with more systematic issues, such as the availability of beds and services and quality assurance. These problems can be difficult to manage, even with sophisticated electronic information systems in place.
Patient and family satisfaction is also a challenge. Regionalization means that not all services will be available in a local area, which means patients are more likely to receive care farther from home and families may have to travel longer distances to visit them. Patients requiring prolonged periods of care may have to stay outside of their usual social support systems for extended periods of time, which is a source of dissatisfaction.
|
BOX 3-1 Challenges Related to Regionalization
SOURCE: Kizer (2009). |
Another significant challenge is managing quality at the system level. System-level quality management, Kizer said, is very different from managing quality at a single facility or a single service within a facility. Data collection requires that data elements be standardized and that many different sources of information come together in a seamless manner, to be shared bi-directionally. Protecting the privacy of this sensitive information requires a more sophisticated and rigorous approach to information security than is generally found.
Kizer emphasized that the financial consequences of regionalization are real. He agreed with earlier comments about the need for a sustainable business model to support regionalization, pointing to the Los Angeles County trauma care system in its early days as perhaps a good example of failing to operationalize this understanding. Another good example of what can happen in this regard is the California Poison Control System that he initiated in the 1980s. This model statewide system is now being dismantled because of the budget situation in California and a lack of non-government support.
Also, he observed that the community perception of a facility that does not receive top-tier designation in a regional system (e.g., Level I trauma center status) can be damaged, and this is often a major concern of hospital directors or boards of trustees. This has implications for these facilities and for the delivery system.
Finally, there are political and community impacts of regionalization that are often not considered. Kizer said that hospitals are always among
|
BOX 3-2 Lessons from Previous Regionalization Experience
SOURCE: Kizer (2009). |
the top three employers in a community. If care is regionalized, it will have labor and other implications that go far beyond medical care—and these implications are usually what gets politicians upset.
In summary, Kizer noted that regionalization of care is conceptually pretty straightforward. There are good evidence-based arguments for why it should be established for many conditions. However, in reality, regionalization is anything but straightforward. Regionalization of health care services is much more difficult and complicated than for most other types of services and certainly more complicated than most people understand (see Box 3-2). He added that many of the people in the audience probably have scars from doing this with trauma care, and these would help to prove this point.
Kizer concluded that strong and effective medical leadership is absolutely crucial for regionalization to occur. Regionalization is not going to happen unless there are physicians and other health care professionals leading the effort. The financial impacts are generally not well understood, but often they are what undermine a system. Also, in the public debate about regionalization of care, the potential improvements in service quality typically become overshadowed by the loss of local service.
THE U.S. ARMED FORCES JOINT THEATER TRAUMA SYSTEM
John Holcomb, former commander of the U.S. Army Institute of Surgical Research and trauma consultant for the Army surgeon general, discussed the Joint Theater Trauma System. He said that after visiting Iraq in 2003 to assess the military’s trauma system, he briefed the Army surgeon, and told him: “Sir, we do not have a trauma system. Your helicopters are disconnected from your ground units. Your ground units can’t talk to any
of the hospitals. Your big hospital can’t talk to the little hospital. Nobody can talk to anybody. And when a patient flows through that, quote, system, nobody knows what happens to them when they leave and nobody knows they’re coming when they get there.” The guidance he said he received from the general was clear: “Go fix it.”
He first went and listened to members of the civilian trauma system and asked specifically where they had failed so that the military could try to avoid those mistakes. At that time, the DOD did not have a trauma registry, and that became the initial focus. From the interviews they had learned not to try to capture too many data elements. “If you try to catch too much, then you won’t catch anything,” Holcomb said. So the system they implemented now tracks about 50 data elements. By 2005, Holcomb said, they had built a fairly functional system, and it has continued to evolve and mature.
Holcomb agreed with Kizer about the importance of information systems and data transfer. At the beginning of the war, he said, the military was relying on written notes on scraps of paper. Those notes were getting lost. People were writing instructions on the dressings of the wounded in order to communicate to the personnel at the next level of care.
Holcomb reported that that has been fixed. Before the registry was complete, medical staff was hanging thumb drives around soldiers’ necks to pass information along to the next care facility. Now, the registry database has been instituted across all areas and has more than 25,000 combat injuries collected. “That allows us to do many, many things with a lot of fidelity,” he said.
The military has been able to disseminate best practices as it learns what works best in the field. It does not provide prospective randomized data, but it works effectively in combination with experience and opinion. The military has also disseminated clinical practice guidelines and, more importantly, conducted weekly telephone conferences to review cases. These involve providers across the many levels of care, from Iraq and Afghanistan to Germany to facilities in the United States, including Walter Reed, Bethesda, the Air Force hospitals, “or wherever the patient happens to go.” Holcomb said they are obviously not doing this with every patient, but “you have to be able to track [patients] and give feedback to people.” Telephone conferences also allow the military to communicate best practices to individual providers.
At the beginning of the Iraq war, Holcomb said, the general officers were getting most of their data about care from The Washington Post and CNN. The colonels in the military did not have a way to deliver systems data to the admirals and the general officers to help them make good decisions. Holcomb said that within the past year they have added outcomes data to the system and now “We know exactly what happens to these guys.” There
is a performance improvement system in place that has become “the feedback mechanism for everybody. That really is what makes this thing go.”
Holcomb also described the other components of the military’s system, ranging from prevention (better body armor and armor on vehicles) to research. Leadership and communication are extremely important, as is integration with prehospital care. Being able to modify training so that it addresses the issues being seen on the battlefield is also essential. The military is now modifying its training of surgery residents to address the system issues they are finding. “Whatever the issue is,” he said, “our system data can inform training very nicely.”
Holcomb also discussed the delivery system that transports the wounded from the theater back to the states (see Figure 3-1). An injured soldier goes by ground or helicopter to surgery teams that have been moved “pretty far forward,” both in Afghanistan or Iraq. Whereas they used to have two big hospitals in theater, now there is just one.
One of the lessons learned has been to keep the conveyor belt moving and get patients out of the hospitals very quickly. So fairly quickly the wounded are put onto critical care air transport cargo planes and flown to Germany. “It’s pretty amazing,” Holcomb said, “we’ve transferred about 10,000 patients that way, with amazingly little loss of life in transport, much like you would expect in any ICU [intensive care unit]. We’re able to do all
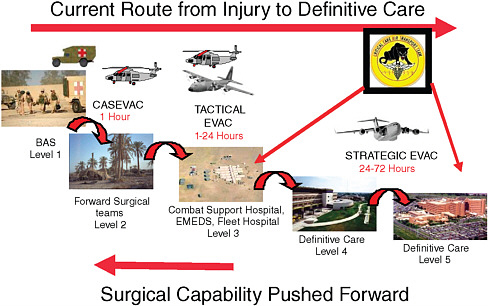
FIGURE 3-1 Care delivery in the military’s joint theater trauma system.
SOURCE: Holcomb (2009).
the ICU care … that you can do in any civilian hospital anyplace.” Patients are also transported by cargo plane back to the United States, “so it’s across three continents that ICU care happens,” he said.
Summarizing, Holcomb said, “The DOD has evolved an effective system of communication and regionalization of trauma care, which has become the standard of care on the battlefield.”
ACCOUNTABLE CARE ORGANIZATIONS
David Magid, director of research for the Colorado Permanente Medical Group, discussed the need for improved systems of care. He referenced the 2001 Institute of Medicine’s report, Crossing the Quality Chasm, which talked about how patients encounter multiple professionals across multiple different settings. Typically the quality of care provided is limited because of the lack of access to medical records and the poor communication and coordination among providers. As a result, patients often experience poor transitions, and these can increase rehospitalizations for patients with conditions like heart failure.
Magid cited Elliott Fisher, who has developed the concept of accountable care organizations. These are intended to foster shared accountability among providers, rather than dividing accountability among specific settings of care, such as inpatient or outpatient care. The idea, Magid said, is that shared accountability will also support the development of systems such as EHRs [electronic health records] and thereby improve quality and afford-ability overall.
Many examples of accountable care organizations currently exist, such as academic centers, county hospital systems with clinics, the VA, and integrated delivery systems such as Geisinger, Intermountain Health, and Kaiser Permanente.
Regionalization is something that has been supported for cases such as trauma, stroke, and critical pediatric patients. The data to support regionalization is not always good, but it is thought to improve outcomes and efficiency and reduce waste, Magid said. He proposed implementing regionalization through accountable care organizations.
In preparing for this talk, Magid said he spoke with representatives from 15 integrated care delivery systems across the country and compiled several illustrative patient scenarios based on their experience. He provided three case examples to illustrate the benefits of directing care to accountable care organizations.
He began with a hypothetical patient who was brought by EMS to Elsewhere General Hospital, which is not part of an accountable health care organization. He described the patient as an 80-year-old male with vomiting and confusion. The patient’s medical records are unavailable. The workup
reveals the patient has a urinary tract infection and he is treated with IV fluids and provided Cipro. He returns to his baseline minimal status and is discharged. However, the patient returns one week later with an upper GI bleed resulting from an interaction between the Cipro and the Coumadin that he was also taking.
Magid said that if the patient had been brought to Accountable General Hospital, his medical records would have been available. The treating physician would have been alerted that the patient was on Coumadin for a valve replacement and instead of Cipro he could have prescribed a different antibiotic.
A second example is a 50-year-old female brought in with chest pressure. Again, the patient’s records are not available. The patient is anxious. The physical exam for the patient is normal and the electrocardiogram shows nonspecific changes and initial troponin is normal. The patient is admitted overnight. She experiences chest pain and is treated in the cardiac catheterization lab. The results of the catheterization are normal.
Magid said had this patient been brought by EMS to Accountable General Hospital, medical records would have revealed that the patient has had multiple visits for chest pain. A stress test was conducted six months ago and the readings were found to be normal, and a catheterization had been performed three months ago and was also shown to be normal. Rather than admitting the patient, she is reassured and discharged with instructions to follow-up with her primary care physician.
The third case is that of a 45-year-old male with cough and shortness of breath. The patient is brought by EMS to Elsewhere General Hospital and a chest x-ray shows a left lower lobe infiltrate. A complete blood count (CBC) test reveals a hematocrit of 30 percent. The physician prescribes antibiotics appropriate for the community in which they practice and advises the patient to follow up with his primary care physician for evaluation of anemia.
The patient does not understand the explanation and never follows up. A year later the patient presents with weight loss and fatigue and is diagnosed with stage III colon cancer. He has surgery to remove the tumor and affected nodes and then is treated with chemotherapy and radiation.
Had the patient been brought to Accountable General Hospital, the physician might have noted the anemia and sent a priority message through the health record to the primary care physician. The patient might have then been scheduled to receive a colonoscopy within a month, where stage I colon cancer could have been revealed. That would have been removed and no other treatment would have been required.
Magid said that these types of scenarios happen every day in institutions across the country. He said he is hoping that part of what comes out of this conference will be an endorsement of the idea of patient transports to accountable health care organizations.
AUDIENCE DISCUSSION
Joseph Waeckerle, former senior advisor to the U.S. surgeon general, said that the three panelists each work within a unique, self-created system. The VA by its very design has been a closed regionalized system since its inception. The DOD has theaters of conflict which have created a need for regionalization. The Kaiser network is a proprietary system that starts with the insurance policy but has extended all the way through the continuum of care to wellness.
Waeckerle said that the panelists had been visionary and innovative, but “you still have closed systems [and] you had a head start on the rest of us.” He said that taking those types of systems nationwide to 305 million people, who have a multitude of needs in different disease areas and extremely differential abilities to pay and insurance coverage, is challenging at best. The general health care system, he said, includes a public system and a private system, and there are rivalries among the proprietary systems within communities.
He asked how the panelists see their closed systems integrating into America’s system and what lessons learned they could bring, given the advantages of the systems they have had to work with.
Kizer replied that the term “American health care system” is a misnomer. There is no system, and that is the crux of the problem. He said “the ability to do some of this within, quote/unquote, closed systems is really due to the fact that they were systems.” It is not impossible to replicate, he added. He cited a neonatal intensive care system that he helped to establish in the private sector in California. He said this is a specialized area, but the system has been in place now for 25-30 years.
Kizer called the early days of the trauma care system in Los Angeles County a good case study of what not to do. When initially setting up its trauma system in the early 1980s, the Los Angeles County Board of Supervisors chose not to abide by expert advice. They allocated trauma center designations to essentially every hospital that wanted it and could meet key criteria. The hospitals appeared to believe that designation would result in a lot of new paying business. “Very predictably,” he said, “things did not work out this way.” Over the next decade, many of these hospitals found that they could not afford to continue to be trauma centers, and one by one they went out of the trauma business. There are now 12 trauma centers, down from 21. At the time we had said that about 11 would be needed. Kizer concluded that when you have a collage of facilities that are financially driven and are not part of a system, “it is a prescription for what we have today.”
Holcomb noted that the DOD system was designed based upon what worked well and what did not work well in the civilian system. There are great lessons to learn, he said. Fundamentally, he observed that “data does rule, and quality is absolutely the bottom line.”
He said that the system measures quality and presents the information through dashboards. He said those who run the hospitals and have the money really pay attention to those outcomes. “Politically,” he said, “they cannot afford not to.”
Alternatives to Centralization
John McKurson, an emergency physician at the University of Maryland, said he was struck by Colonel Holcomb’s slide showing all the patients flowing to a central point outside of the theater that was able to take them all in. McKurson said that his institution is now overwhelmed with patients, to the point that staff have had to board patients in hallways. He argued, “if [patients are] always coming to a central location, you are really creating a system that may be overrun at that location, unless there is some design within that that allows you to push people back,” for example through transfers back to the smaller hospitals once the acute condition has been treated. Also, McKurson said, “If you have it all flowing to the center … there may be some degradation of the outside resources if they are not supported.” He asked, “How do you see the regionalization being able to support the areas that are referring to it and how are you going to flow the patients and provide for those other resources?”
Holcomb replied that “I could not agree with you more.” He said, “you must maintain capacity across the system … if you take all the patients out of those hospitals, they may become non-functional and they can no longer help you take care of patients because they lose the capability—whether it’s the nurses, equipment, or the docs. The administrators certainly lose the desire to admit those patients.”
In the military, Holcomb continued, we actually did something similar where all the patients were coming out of Germany and landing on the east coast. We quickly decided that wasn’t very smart, because it overwhelmed the receiving hospital. A lot of patients got redirected to some capable hospitals more in the center part of the United States.
Holcomb reiterated, “I could not agree with you more. You must maintain [other facilities] not just to offload from the central [location], but to make sure all the other sites remain capable not only on a day-to-day basis but in a surge capacity.”
Post-Acute Trauma Care
Ellen MacKenzie, a panelist from session one, said we’ve shown we can save lives by regionalizing trauma care and we spent a lot of time this morning talking about that. But it’s also important for us to remember that one major study showed that among 2,500 people who were working up
until the time of their injury, only a little over 50 percent got back to work within a year of their injury. We have not yet developed a regionalized system of trauma care that truly addresses the issues of continuity of care and post-acute care, or that addresses getting people back to work and having a good quality of life. So while we have developed great models of trauma care in the civilian world and even more so in military, we still haven’t fixed the problem of what happens after patients leave the trauma center or the trauma system, she said.
Kizer noted that the VA system has nurtured vocational rehabilitation, job training, and other dimensions of care as a key part of their regionalized approach. MacKenzie acknowledged their work in those areas.
Reducing Overtransfers and Diversion Rates
Sabina Braithwaite, an emergency physician at the University of Virginia and a member of the Emergency Care Coordination Center (ECCC) staff, said that she is a clinician who has been on the receiving end of overtransfers from outside hospitals. She asked the panel how they would recommend decreasing some of the variability in the entrance points of the medical system. She said she can predict, based on who is working at the outside hospital, whether she can expect to receive every single one of their patients—even when the level of training is the same—or whether the person will be able to manage their own affairs.
Braithwaite asked whether we need a transfer center staffed by a physician to help facilitate these issues and a system to monitor outcomes to ensure that the patient gets married up with the right level of expertise.
Holcomb replied that in Houston what they’ve done is to go back to the individual hospitals and talk to the chief of staff and others. The problem, he said, is that many people moonlight in emergency rooms. It’s hard to get at that added variable, but he said they are able to show the outcome of what is happening. If the referring hospitals send a bunch of patients and the receiving hospital says yes to everything, its diversion rate will increase significantly. Holcomb said they are able to demonstrate that. “We tell them, here’s the outcome of what happens from a systems point of view. If there are 20 feeder hospitals, we show them that all they had to do was admit one more patient a day and the diversion rate changes from very high to very low. They understand that this means when they get a really sick patient, we will be able to take him.”
Holcomb said that this approach has been effective. His facility’s diversion rate has gone from very high to just 1 percent by using feedback, performance improvement measures, and a system approach. He added that the personnel in these other facilities are smart and they work hard. They face legitimate issues where they are, and these are different from the ones the receiving hos-
pital faces. But, he said, when you provide feedback and show the implications of their decisions, it is possible to modify their behavior.
Recommendations for Federal Dollars
Kellermann asked the panel if they had any specific recommendations for the federal officials in the ECCC who will be drafting the request for proposals (RFP) in support of regional programs across the country that hopefully will be supporting progress toward the IOM’s vision of regionalized, coordinated, accountable emergency care systems. Specifically, he asked, how would you recommend that they make strategic investments to enhance and improve regionalization?
Kizer responded that the choice of terms is the right one: it’s a fiscal issue and it’s an investment. The government controls the purse and it is possible to radically change hospital and individual physician behavior based on how funds are allocated, even very small amounts of funds.
Holcomb agreed but said he would add the dashboard of quality concept. Those dashboards are extremely helpful when they contain specific, well thought-out, clinically driven, and vetted quality indicators, he said.
Magid noted that the issues he had raised are not really financial. He noted that Seattle has an extraordinarily well-coordinated EMS system across all of King County. Patients get to where they are supposed to go, because the system is not fragmented and ambulance transports are not tied to a specific hospital. He argued that if we could establish more well-coordinated EMS systems that are organized and implemented across entire metropolitan areas, the problems that we see in other areas would go away. We need better organization of the EMS system as a whole, he said, rather than a collection of fiefdoms.
REFERENCES
Holcomb, J. 2009. PowerPoint slide presented at the Regionalizing Emergency Care Workshop, Washington, DC.
IOM (Institute of Medicine). 2001. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press.
Kizer, K.W. 2009. PowerPoint slides presented at the Regionalizing Emergency Care Workshop, Washington, DC.














