
in type 1 diabetes. She addressed key issues and strategies for overcoming challenges in recruiting and retaining clinical trial subjects, designing trial protocols for Institutional Review Board (IRB) approval, and navigating requirements of the informed consent process.
Patient Recruitment and Retention
Greenbaum described the process of identifying, screening, and recruiting patients to participate in a type 1 diabetes natural history/prevention trial. To achieve enrollment of the 300–400 patients necessary for a prevention trial, 200,000 relatives of people with type 1 diabetes will need to be screened, a number representing approximately 2–3 percent of the total potential pool of such individuals. About 4 percent, or 8,000, of these 200,000 individuals will be antibody positive—the necessary trait for participating in the trial. After 5 years of patient recruitment efforts, approximately 70,000 relatives have been screened; progress has been steady but remains a challenge. Greenbaum noted that the magnitude of the screening effort necessary to find the relatives at risk for type 1 diabetes and eligible for the prevention study is sustainable only with the broad support of a clinical research network, in this case TrialNet.
Limited information is available regarding how people approach the decision of whether or not to participate in a diabetes clinical trial. Greenbaum speculated whether people with diabetes know that their families are at 15 times greater risk for the disease than the general population, and whether they know that they can be tested or know but prefer not to be tested. In the absence of any systematic, rigorous study in this area, Greenbaum offered a few anecdotal thoughts about why people participate in diabetes trials. In her experience in the northwestern United States, rural participation in diabetes clinical trials is much greater than urban or suburban participation. Greenbaum hypothesized that in urban and suburban areas, families may already be so overwhelmed by such demands as having to take children to various school events and team practices that joining a clinical trial would be an additional, and unwanted, burden.
Greenbaum also described the age distribution of the relatives screened for the type 1 diabetes prevention study. Young adults (ages 19–32) are participating in research at a much lower rate than other age groups. In Greenbaum’s experience, the young adult population is difficult to recruit for clinical research because it is generally characterized by a level of self-absorption that does not lend itself to voluntary participation in a clinical trial that may or may not lead to any personal benefit.
In contrast to prevention studies, clinical trials on the new onset of type 1 diabetes have had greater success in identifying and recruiting participants. Figure 7-2 shows the recruitment rates for four such trials. Greenbaum
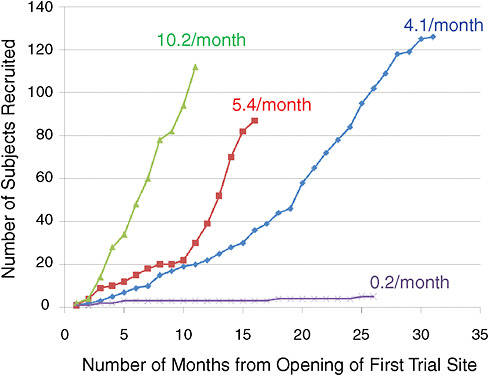
FIGURE 7-2 Patient recruitment rates for four type 1 diabetes trials.
SOURCE: Greenbaum, 2009. Reprinted with permission from Carla Greenbaum 2009.
discussed some of the factors associated with each study that she believes affected their ability to attract patients in an efficient manner.
For each trial depicted in Figure 7-2, the sites were large diabetes centers that are highly committed to recruiting patients. Thus, differences in recruitment rates should not be attributable to variation in the commitment level of trial sites. The trial that recruited 4.1 subjects per month required daily, chronic medication therapy. In the trial that recruited 5.4 patients per month, the drug treatment was two doses (not a chronic therapy), and some follow-up visits were required. The study with the most successful patient recruitment rate is surprising because it involved younger subjects, who, as noted, are typically difficult to recruit, for an intravenous (IV) infusion over 24 visits, one visit per month. In contrast, the study with the lowest recruitment rate has yet to recruit the 10 subjects it requires. Greenbaum explained that this is a phase I study, started at only one site and including only individuals aged 18 and older. In addition, subjects have to have been diagnosed with type 1 diabetes at least 4 years previously, but still have significant insulin secretion to qualify for enrollment in the study.
In light of these differences in recruitment rates, Greenbaum discussed factors that, in her view, can impact patient enrollment and retention:
-
Enthusiastic health care providers—Greenbaum and Kahn both referred to the importance of having research teams that are supported by full-time equivalent (FTE) employees. With time dedicated to clinical research, staffs have a greater sense of responsibility for enrolling and retaining patients in a trial. Greenbaum indicated that within her home institution, the successful recruitment and retention of study participants is due to the connections research staffs have with patients and families. The relationship between staff and patients engenders a strong sense of loyalty to the study, as well as to each other.
-
Patient vulnerability—There is a level of vulnerability associated with patients who are newly diagnosed with a disease. In Greenbaum’s experience, individuals entering clinical trials are looking to cure their diabetes, regardless of the information presented to them on consent forms. Perhaps people who are further from diagnosis are not enrolling in clinical trials at the same high rate as those who are newly diagnosed because they have adapted to the lifestyle of their condition and are more attuned to the risks and benefits of a particular study. Greenbaum also noted the high level of clinical trial participation among children and speculated that it may be associated with parents’ sense of guilt and fear and their desire to do anything they can to help their children, including enrolling them in clinical trials.
-
Socioeconomic status—Greenbaum noted, as did Musa Mayer (Chapter 6), that variations in socioeconomic status (income, education, occupation) affect an individual’s level of engagement with the health care system and exposure to clinical trials. An individual with higher socioeconomic status may be more likely to be aware of the clinical research opportunities available and better equipped to weigh the risks and benefits of participating as a research subject.
-
Physician support—The critical importance of physician support in recruiting and retaining patients in clinical trials was noted by Greenbaum, as well as a number of workshop participants. Most clinical trial subjects cite their physician’s encouragement as the reason why they decided to participate in a clinical trial.
Reflecting on her work with TrialNet, Greenbaum also highlighted a number of effective tools this network brings to the clinical trial process and to the recruitment and retention of patients. TrialNet uses FTE-supported



