
8
Do Cross-Country Variations in Social Integration and Social Interactions Explain Differences in Life Expectancy in Industrialized Countries?
James Banks, Lisa Berkman, and James P. Smith with Mauricio Avendano and Maria Glymour
INTRODUCTION
Variations in life expectancy among industrialized countries have been attributed to differences in patterns of health behavior, health care, socioeconomic conditions, and variations in social and economic policies. In this chapter, we explore whether variations in morbidity, mortality, and life expectancy are related to variations in the extent to which countries have different levels of social integration or social support. Extensive research suggests that aspects of social networks and social integration may be associated with mortality in a number of countries (Berkman and Syme, 1979; Berkman et al., 2004; Blazer, 1982; Fuhrer and Stansfeld, 2002; Fuhrer et al., 1999; House, Robbins, and Metzner, 1982; Kaplan et al., 1988; Khang and Kim, 2005; Orth-Gomer and Johnson, 1987; Orth-Gomer, Rosengren, and Wilhelmsen, 1993; Orth-Gomer, Unden, and Edwards, 1988; Orth-Gomer et al., 1998; Penninx et al., 1998; Sugisawa, Liang, and Liu, 1994; Welin et al., 1985). But in no studies have we been able to compare either risks or distributions of comparably defined social networks across countries, nor have we been able to understand if variations in social networks and social participation might explain cross-country variations in population health.
We explore these issues from several perspectives. Ideally, we want to assess the variability in distributions of social networks and support in many countries. We would also like to identify whether risks associated with social isolation and various health outcomes are the same in each country. For social networks and support to “explain” cross-country differences in life expectancy, at least one of two conditions must be met. First, a differ-
ent fraction of the population needs to be exposed to risk factors across countries. Second, the health risk—“toxicity”—associated with risk factors might differ between countries. For common risk factors, even small differences in toxicity may have large population health effects. Differences in toxicity could occur if population differences in exacerbating or compensatory factors influence the risk of disease. For example, if countries had public policies protecting citizens against deleterious health effects of extreme poverty, we might not see health effects manifest themselves there, even though poverty was present. Third, we would hope to assess in a single model whether social integration and support can account for cross-country differences in life expectancy. In this chapter we examine the first two but do not have adequate data to test the third in a compelling way, except for a comparison of England and the United States.
The lack of truly harmonized individual-level data across countries on relevant exposures and health outcomes over time limits our ability to examine this question. To overcome this limitation, we start by comparing associations between social integration and social support in the United States and England, using data from the Health and Retirement Survey (HRS) and the English Longitudinal Study of Ageing (ELSA). Although not identical, these surveys have very comparable measurements of social networks and social support, as well as comparable data on health conditions and associated risks. We then consider ways in which related psychosocial conditions tapping dimensions of stress may explain observed health variations between the United States and England. We examine these questions for a variety of self-reported outcomes and measured biomarkers of disease. In addition, we use the mortality follow-up in HRS and ELSA to examine impacts of social networks and interactions on all-cause mortality.
Since differences in life expectancy between the United States and England are relatively small, we then examine how 28 industrialized countries vary on several dimensions of social networks and support. In these analyses, we draw on recent data from the Gallup World Poll for Japan and a number of European and North American countries. We present data on the distribution of dimensions of social integration explored in our HRS/ELSA comparisons. Although the items are not fully identical, they provide us with a general overview of variations in these dimensions in a wider set of countries. We conclude with suggestions for carrying this work forward by exploring whether variability in social networks is related to a country’s level of health and well-being.
The chapter is divided into four sections. First, we compare morbidity and health risks in England and the United States by social networks and support, using cross-sectional data from HRS and ELSA. Second, we briefly report on whether other psychosocial stressors often related to social networks may help explain cross-country differences. Third, we examine
mortality risks associated with these social networks in ELSA and HRS. In the last section, we use data from Gallup to examine the extent to which countries vary on domains related to social networks, social integration, and support.
We were unable to explore whether social networks actually explain diverging trends in life expectancy because we do not have data on long-term trends in these conditions across countries. However, this is a first attempt at addressing this question by exploring whether such conditions are able to explain variations in health outcomes contemporaneously and whether variations are large enough in and of themselves to be able to explain diverging trends. We conclude with a summary of our findings and a discussion of strengths and weaknesses of the work as well as ideas for how to extend work in this area.
SOCIAL NETWORKS, SUPPORT, AND HEALTH IN THE UNITED STATES AND ENGLAND
In this section we provide a descriptive portrait of social networks and social support of older residents in the United States and England and examine their association with health outcomes. We concentrate on the United States and England because the most comparable, comprehensive data on social networks and social support are available for them. A recent study (Banks et al., 2006) documented large health differences between England and the United States, and it is possible that social network and social support differences may explain the U.S. disadvantage in health.
Data
For the United States, our research is based on the Health and Retirement Survey, a nationally representative survey that now includes more than 20,000 people over age 50 in the United States (Juster and Suzman, 1995). HRS began in 1991, and new cohorts have been subsequently added to maintain population representation of this age segment. Respondents are reinterviewed biannually.
For England, we use the English Longitudinal Survey of Ageing, which contains around 12,000 respondents recruited from 3 separate years of the Health Survey for England (HSE) providing representative samples of the English population age 50 and over (Marmot et al., 2002). The health data were supplemented by social and economic data collected in the first ELSA wave, fielded in 2002. Like HRS, the initial baseline sample was of the noninstitutionized population, and follow-ups (including of those subsequently moving into institutions) are conducted every 2 years. However, since the ELSA study is still a younger study, in the sense that the baseline
is more recent, it will presumably be less representative of the entire population age 50 and over (including those in institutions).
For our analysis we selected key health and social network and support constructs in which strong a priori measurement comparability existed. The 2004 waves of ELSA and HRS were used for analysis, since this was the year in which HRS first contained social network and social support variables directly comparable to those collected in ELSA.
Measures of Chronic Conditions, Biomarkers of Disease Risk, and Health Behaviors
Both surveys collect data on individual self-reports of diseases in the form “Did a doctor ever tell you that you had ___?” In addition, both studies have biomarkers of diabetes risk (HbA1c) and have assessed blood pressure. These two biomarkers permit us to assess diabetes and hypertension status more reliably. The specific diseases analyzed include diabetes (assessed by either self-report of diabetes or HbA1c over 6.5 percent), hypertension (assessed by measured systolic blood pressure ≥ 140 or diastolic blood pressure ≥ 90 or self-report of hypertensive medication), self-reported heart disease, pulmonary function (using a clinical assessment of peak flow), and obesity (body mass index, BMI, ≥ 30).
Lung function in HRS was measured using peak flow (averaged over 3 measures), and in ELSA it was measured with forced expiatory volume (FEV). To account for this difference, we show parameter estimates for each social indicator as a percentage of the average for the reference group. These measures operate similarly with this transformation, as the effect estimated for smoking on lung function is similar in both HRS and ELSA. The two surveys also collect several health-related behaviors in common, including smoking (currently and ever smoked), alcohol consumption (heavy drinking defined as drinking on more than 4 days per week in HRS and twice a day or more/daily or almost daily in ELSA). While other risk factors may be important, we used only these comparably measured variables in our multivariate models.
Measures of Social Networks, Social Support, and Negative Interactions
Measures of the size of social networks and various forms of social participation and quality of social support available to individuals were measured in both surveys using almost identical questionnaires. One key advantage of using these two surveys is that their comparable questions cover many key domains of the social network. Questions were asked in several domains about relationships with children, partners, close family members, and friends. In addition, the surveys included questions about
voluntary activities. With regard to children, in addition to the number of children, respondents were asked about the frequency of their interactions with their children on a 4-point scale (a lot, some, a little, not at all). We coded these scores numerically from 0 to 3.
Three questions address elements of positive interaction: (1) do your children really understand the way you feel about things, (2) can you rely on them if you have a serious problem, and (3) can you open up to them if you need to talk about your worries. The other three address negative interactions: (1) how much do your children criticize you, (2) how much do they let you down when you are counting on them, and (3) how much do they get on your nerves. We separated these into two components—positive support and negative interactions—and summed the numerical scores. The total scores for both positive support and negative support vary between 0 and 9. So that high scores on positive and negative interactions mean the same thing, the top score of 9 for negative interactions implies no negative interactions.
HRS and ELSA respondents were asked (not counting those children living with you) about the frequency of contact with children on three dimensions: (1) meeting (arranged and chance meetings), (2) speaking on the phone, and (3) writing an email. The scale for each dimension consists of six possible categories: (1) three or more times a week, (2) once or twice a week, (3) once or twice a month, (4) every few months, (5) once or twice a year, and (6) less than once a year or never. Finally, respondents were asked with how many children they have a close relationship. Our measure does not distinguish between individuals without children and individuals with children who are not close or not in contact, since our measure is intended to capture contact, which would be zero in both cases. However, to assess whether differences between childless individuals and those with children are influencing our results, we also estimated our models for the sample of those with children only. The results were broadly unaffected, with one exception: the social estimated interaction effects were slightly weaker, suggesting that some of the identification of these effects was coming from differences between the childless and those with children. However, since all substantive conclusions of our analysis were unaffected (indeed, if the interaction effects are weaker, our conclusions are strengthened) we do not present this analysis in the tables of results.
Respondents were also asked the same set of questions about positive and negative interactions, frequency of contact, and the number of close relationships they have with other immediate family members, defined as siblings, parents, cousins, or grandchildren. Friends are also a potentially important component of any support network. HRS and ELSA ask the same set of questions (positive and negative interactions), frequency of contact, and number of friends. Scales for positive and negative interactions and
frequency of contact are scored in the same way as for children: scores were translated into a scale that ranges from 0 to 9. In the data in these analyses we have summed the total of either positive or negative social interactions across children, friends, and relatives. High scores represent high levels of positive interaction or low levels of negative interactions (in both cases, “high” is the more optimal interaction).
Questions about social participation in voluntary and civic organizations and religious attendance were also asked. In HRS, the item about voluntary activity was framed in terms of frequency of participation, whereas in ELSA it was asked as the number of organizations the participant belonged to. Ties with religious organizations were assessed by attendance. Finally, we developed a summary index of social integration that summed network domains related to children, partner, friends, and relatives and volunteer and religious activities into a single score. This index has six dimensions: (1) married/partnered, (2) frequency of visits with children, (3) frequency of visits with family, (4) frequency of visits with friends, (5) participation in voluntary organizations, and (6) religious attendance. The score could range from 0 to 16, with 0 reflecting no tie and 3 in each domain reflecting high levels of contact. Religious attendance, however, was scored 0 or 1 due to limitations in the availability of more nuanced measures in the ELSA questionnaire (in the HRS-only analysis of mortality, we were able to distinguish between those attending religious services regularly and those attending periodically, and this distinction did prove to be important).
COMPARISONS BETWEEN ENGLAND AND THE UNITED STATES
There are several ways of characterizing social networks, including the existence, number, and type of key people in the network and the nature of interactions taking place, both positive and negative. Although we examined each social network domain individually, in this section we provide tables or figures on summary measures related only to the social network index, the summary measure, and positive and negative social interactions. We describe social networks in England and the United States for spouses, children, other immediate family members, and friends.
Distribution of Social Networks
We begin with a description of an aggregate index of social networks in the two countries. While there are some differences in how older men and women maintain contact with friends, family, and larger civic, religious, and voluntary organizations, the overall distribution of social networks is virtually identical in the two countries.
Figures 8-1A and 8-1B show the distribution of scores for our overall
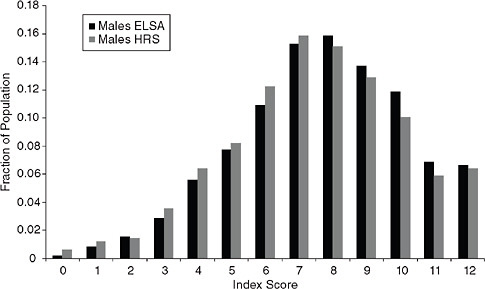
FIGURE 8-1A Distribution of scores of the index of social networks in England and the United States among men.
SOURCES: Authors’ calculations from the Health and Retirement Survey (2004) and the English Longitudinal Study of Ageing (2004) microdata.
index of social networks for men and women in HRS and ELSA. For both men and women, the largest numbers of people scored in the mid-range, between 6 and 9, and this concentration of scores is almost identical in England and the United States. Women tended to be slightly more isolated than men, but even among U.S. women (the most isolated), only around 5 percent of older women scored 2 or lower on the summary index.
Some differences in the frequency of contact of specific ties are of some note, but these differences are unlikely to be sufficiently large to explain cross-country variations in health or life expectancy. The prevalence of those with partners, children, other family members, and friends are listed in Table 8-1. Overall, the percentages of those with children are almost identical in the two countries, but there are some cohort differences. Among men and women age 75 and over (those born before 1930), U.S. men and women were more likely to have children than their English counterparts, reflecting greater fertility in the United States among those cohorts. In addition, U.S. men, particularly those ages 65+, were more likely to be living with a partner. Among more recent cohorts (those born in 1940 or later), English men and women were more likely to have children than their U.S. counterparts.
There are conflicting data on closeness of contact and relationship with children in the two countries. For all birth cohorts ages 50+, English
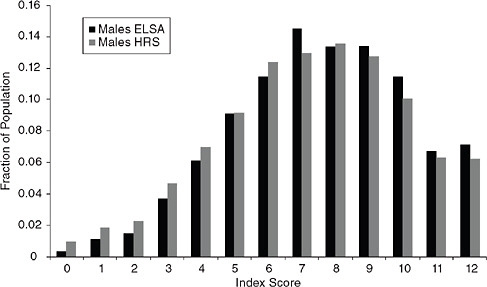
FIGURE 8-1B Distribution of scores of index of social networks in England and the United States among women.
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata.
TABLE 8-1 Distributions of Social Networks in England and the United States
|
Age Group |
England |
USA |
England |
USA |
||
|
Male |
Female |
Male |
Female |
|||
|
Percentage with Spouse/Partner |
||||||
|
50-64 |
81.3 |
76.0 |
85.0 |
78.7 |
83.0 |
71.2 |
|
65-74 |
70.0 |
75.7 |
79.9 |
60.8 |
85.8 |
67.8 |
|
75 plus |
47.6 |
55.1 |
65.8 |
32.1 |
77.1 |
39.0 |
|
Total |
71.9 |
72.2 |
79.6 |
63.4 |
83.0 |
64.4 |
|
Percentage with Children |
||||||
|
50-64 |
87.2 |
85.5 |
84.5 |
89.4 |
83.3 |
87.0 |
|
65-74 |
86.9 |
90.1 |
86.5 |
87.3 |
88.9 |
91.0 |
|
75 plus |
81.0 |
83.2 |
82.3 |
80.1 |
85.2 |
81.8 |
|
Total |
85.9 |
86.7 |
84.7 |
86.9 |
85.8 |
87.5 |
|
Percentage with Friends |
||||||
|
50-64 |
94.0 |
89.4 |
93.0 |
94.8 |
88.9 |
89.8 |
|
65-74 |
90.0 |
90.3 |
87.7 |
91.9 |
88.9 |
91.3 |
|
75 plus |
85.1 |
88.3 |
81.7 |
87.5 |
85.6 |
90.3 |
|
Total |
91.2 |
85.9 |
89.5 |
92.6 |
88.3 |
90.4 |
|
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata. |
||||||
men and women with children were more likely to see them at least once a month: 67 percent of English women said that they met with their children at least once a month compared with 62 percent of U.S. women. Comparable numbers for English men and U.S. men are 62 and 56 percent, respectively. These differences may not be surprising, given the relative size of the two countries and much lower mobility among the English compared with Americans. However, one-third of Americans in this age range stated that they are close to three or more of their children compared with a quarter of the English.
Distributions and means of positive interactions with children, friends, and relatives are shown in Figure 8-2A for women and men, and the distribution of negative interactions in Figure 8-2B. There are some differences between the two countries. U.S. men and women reported somewhat lower levels of both positive and negative interactions with children, but there is a clear preretirement and postretirement distinction to this pattern. Preretirement positive interactions with children were worse for Americans, presumably representing a conflict with work. But in postretirement (i.e., after age 65), the pattern switches, and Americans had greater levels of positive interactions with their children. Americans tended to lag behind the English, in that they experienced more negative interactions with children at all these ages. With other family members, however, Americans tended to experience both greater positive interactions and greater absence of negative interactions than their English counterparts. Interestingly, there were no cross-country differences in distributions of positive and negative interactions with friends.
Relationship Between Social Networks, Positive and Negative Interactions, and Five Health Outcomes
Previous evidence suggests that U.S. men and women have higher prevalence of many chronic diseases than their English counterparts (Banks et al., 2006). Table 8-2 shows means of selected health measures in ELSA and HRS, which confirm that Americans had worse health than the English, both using self-reports and biomarkers of disease. Our aim here is twofold: to assess whether associations between social networks and support and morbidity and health risks are similar between countries and to examine whether differences in prevalence of these risk factors can account for observed cross-country variations in health between the United States and England.
Since in most cases distributions of social relations were very similar, our goal was to see if risks or benefits of social relations varied more or less in one country or the other. The weakness of cross-sectional analyses is that it is impossible to determine which condition is shaping the other. In the case
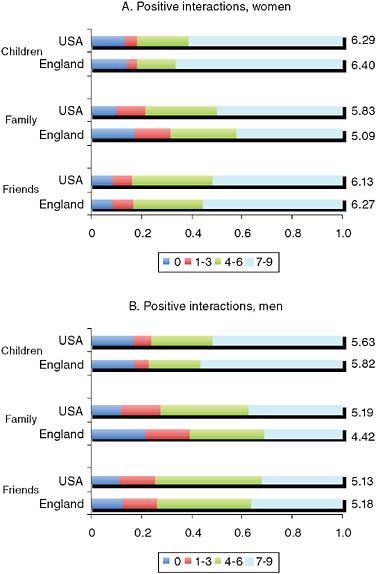
FIGURE 8-2A The distribution of positive interactions with children, family, and friends.
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata.
of social relations and chronic morbidity, it is very likely that the relations are bidirectional, with strong social ties and support influencing health in a positive way and poor health itself placing stresses on social ties and making interactions difficult. Still, acute illnesses tend to elicit greater expressions of social support, and the provision of care for an ill or disabled family member often requires frequent contact. These processes may create a spurious as-
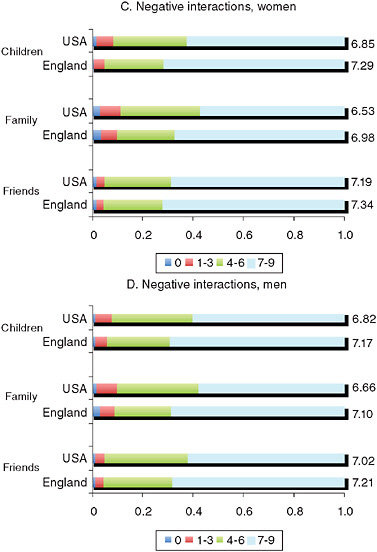
FIGURE 8-2B The distribution of negative interactions with children, family, and friends.
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata.
sociation between support and poor health in cross-sectional analyses. We conducted cross-sectional analyses on each subdomain of social ties (with children, family, friends, and partners and social and religious activities) as well as associations with interactions with children, friends, and relatives. In this section, we present cross-sectional associations between summary measures of social ties, negative interactions, and partnership in relation
TABLE 8-2 Means of Selected Health Outcomes Among Men and Women in HRS (United States) and ELSA (England)
to five health outcomes: hypertension, diabetes, heart disease, obesity, and pulmonary function assessed from a measure of peak flow.
Figures 8-3A and 8-3B show the odds ratios for men and women, respectively, between the social network index and the prevalence of obesity, hypertension, diabetes, and self-reported heart disease. Figure 8-3C shows the association with pulmonary function and the network index for women and men. In these figures, we indicate a statistically significant estimate by an asterisk.
The social network index is not associated with any health outcomes for men with one exception: men with high levels of ties reported somewhat higher levels of heart disease in the United States. Among women in England and the United States, high levels of ties were related to lower health risks, with the exception of obesity. U.S. women with more ties had higher obesity. The social network index is significantly and positively associated with lung function among women in the United States but in not in other groups.
Figures 8-4A, 8-4B, and 8-4C show the relationship between partnership status and the same five health conditions. For both U.S. and English men, having a partner was associated with better lung function. Among English men, having a partner was also associated with lower odds of having hypertension. No other conditions were associated with partnership status among men. Among U.S. women, partnership was associated with lower prevalence of obesity, hypertension, and diabetes. Among English women, partnership was associated only with a lower prevalence of hypertension.
Negative interactions were more strongly related to prevalent health conditions than positive interactions, suggesting the importance of incorporating these measures into further research. Among both English and U.S.
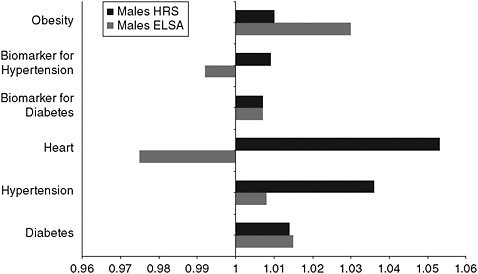
FIGURE 8-3A Odds ratios of disease prevalence for a one-point increase in the social network index for men.
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata.
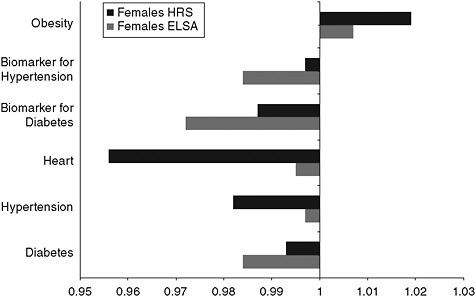
FIGURE 8-3B Odds ratios of disease prevalence for a one-point increase in the social network index for women.
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata.
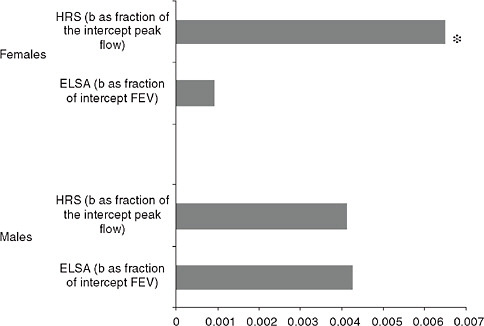
FIGURE 8-3C Association between pulmonary function and the network index for men and women.
NOTES: Statistical significance is indicated by an asterisk, FEV = forced expiatory volume.
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata.
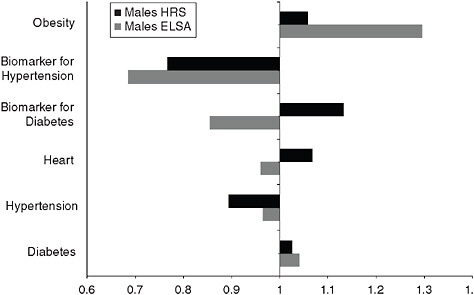
FIGURE 8-4A Odds ratios of disease prevalence by partnership status for men.
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata.
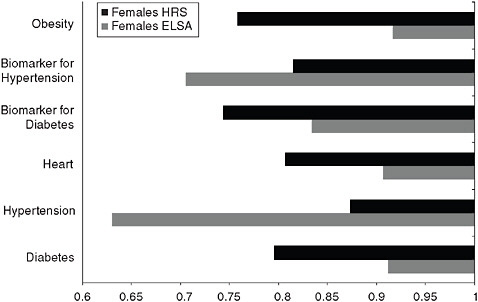
FIGURE 8-4B Odds ratios of disease prevalence by partnership status for women.
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata.
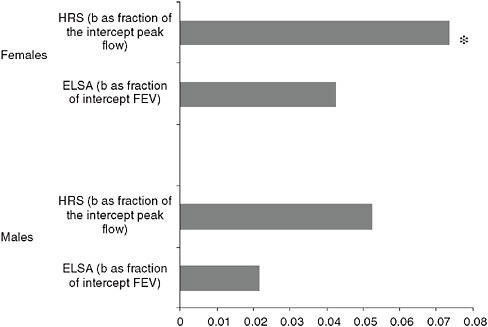
FIGURE 8-4C Association between partnership status and lung function for men and women.
NOTES: Statistical significance is indicated by an asterisk, FEV = forced expiatory volume.
SOURCES: Authors’ calculations from the Health and Retirement Study (2004) and the English Longitudinal Study of Ageing (2004) microdata.
men, low levels of negative interactions were associated with lower levels of obesity and diabetes and better lung function. Among U.S. women, negative interactions were associated with obesity, diabetes, heart disease, and lung function. English women with fewer negative interactions had significantly less hypertension and tended to have fewer chronic conditions, although these later associations were not statistically significant.
In each case, the 95 percent confidence intervals for the estimated coefficients of social network variables for the United States overlap with the confidence intervals in England. The current results do not therefore support the hypothesis that differences in the toxicity of current levels of social networks and integration explain current health differences between the two countries.
Other Psychosocial Factors and Health
We have been considering variables related to social contacts and interactions and their relationship with health outcomes. In the literature on inequalities in health, however, considerable attention has been given to a broader set of psychosocial factors that are argued to be relevant to health through neuroendocrine as well as behavioral pathways. The hypothesis is that stress, a lack of control over one’s life, and even subjective social status itself lead to neuroendocrine dysregulation and/or high-risk behaviors, which are then risk factors for subsequent health (in particular heart disease) and mortality. Is it possible that differences in such factors across countries need to be factored into our comparative analysis?
In recent work, Banks et al. (n.d.) examined the impacts of a set of commonly used psychosocial factors to assess what role they might play in the much higher rates of morbidity in the United States compared with England. The study exploited ELSA and HRS data from 2004, which contain identical measures of both psychosocial risk factors and health for a sample of individuals ages 52+. The psychosocial factors included control at home and control at work (using items that were developed and are collected on an ongoing basis in the Whitehall study), subjective social status summarized in one’s position on the ladder, and loneliness. In addition, the CASP-19 scale, a general quality-of-life instrument covering four broad dimensions (control, autonomy, self-realization, and pleasure) was included (Netuveli et al., 2005).
The analysis shows that differences in these psychosocial risk factors or their health consequences failed to explain higher prevalence of major health conditions in America relative to England. Measures of control and self-realization were strongly and consistently associated with health in both countries. But, much like the social network and contact indicators described previously, the mean levels of these factors and their distribution across age and sex groups differed only slightly between the two countries.
In addition, the direction and strength of their relationships with health were nearly identical in the United States and England. Simulations of disease prevalence, holding levels of psychosocial risk factors constant in the two countries, demonstrated that neither levels of psychosocial risk nor estimated differences in marginal effects of psychosocial risk factors on health were sufficiently different to explain any meaningful fraction of the differences in prevalence of disease between the two countries.
SOCIAL NETWORKS AND MORTALITY
In this section, we present our analysis of mortality in England and the United States using ELSA and HRS. Our models focus on effects of some basic social network and interaction variables in the two countries. The principal constructs of interest are measures of marital/partnership status, the amount and nature of support from family and friends, membership in clubs, and religious organizations. These are the same variables defined and discussed earlier and are derived from a self-completion leave-behind booklet administered to ELSA respondents in 2002 (N = 10,541) and to HRS respondents in 2004 (N = 3,084).
Tables 8-3 and 8-4 present our analysis of time to death of ELSA respondents between Wave 1 (interviews took place between April 2002 and March 2003) and February 2008. Notification of deaths comes from the national death register and does not depend on subsequent participation in the follow-ups of ELSA. Table 8-3 contains models for both genders combined, with separate estimates depending on whether or not deaths within the first 12 months of the interview were included or not. The purpose of this distinction is to control at least partially for any social network reactions to impending deaths of a loved one that reflect reverse causality. Table 8-4 (which excludes those who died 12 months following the interview) contains separate models for men and women. For all models, we present a model that aggregates all social interaction variables into a single index and a model in which each unique dimension of the social interaction index is entered separately.
For completeness we briefly discuss nonsocial variables, all dated at baseline. Not surprisingly, men are at higher risk of death than women. A set of age group controls is included in all models, with the reference group being individuals ages 65-69. Individuals under age 50 at baseline (the younger partners of ELSA sample members) were omitted from the estimation sample. Not surprisingly, all models show a sharply increasing mortality risk with age. In the gender-specific models, age gradients are somewhat steeper for women than for men.
These empirical models also replicate the well-established strong association of smoking with mortality. In English mortality models, we distinguish four types of smoking behavior: (1) never smoked (the reference group),
TABLE 8-3 English Mortality Hazard Models: Time (months) to Death from ELSA Wave 1 Interview Month (by treatment of deaths within 12 months of interview)
|
|
Early Deaths Excluded |
Early Deaths Included |
||
|
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
|
|
Male |
1.460** |
1.562** |
1.517** |
1.618** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ages 50-59 |
0.332** |
0.340** |
0.334** |
0.340** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ages 60-64 |
0.650** |
0.659** |
0.625** |
0.633** |
|
|
0.005 |
0.007 |
0.001 |
0.001 |
|
Ages 70-74 |
1.784** |
1.741** |
1.742** |
1.704** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ages 75-79 |
2.919** |
2.786** |
2.893** |
2.775** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ages 80-84 |
4.508** |
4.181** |
4.503** |
4.208** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ages 85+ |
9.434** |
8.514** |
8.825** |
8.054** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ex-smoker current |
1.793** |
1.711** |
1.796** |
1.714** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ex-smoker regular |
1.294** |
1.297** |
1.288** |
1.289** |
|
|
0.002 |
0.001 |
0.001 |
0.001 |
|
Ex-smoker occasional |
1.029 |
1.027 |
1.013 |
1.013 |
|
|
0.836 |
0.846 |
0.922 |
0.917 |
|
Medium-waist risk |
1.353** |
1.356** |
1.260* |
1.266* |
|
|
0.004 |
0.004 |
0.013 |
0.012 |
|
High-waist risk |
1.544** |
1.522** |
1.381** |
1.365** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Wealth 1 |
1.421** |
1.366** |
1.621** |
1.553** |
|
|
0.001 |
0.005 |
0.000 |
0.000 |
|
Wealth 2 |
1.580** |
1.520** |
1.659** |
1.592** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Wealth 3 |
1.417** |
1.382** |
1.433** |
1.395** |
|
|
0.002 |
0.004 |
0.001 |
0.002 |
|
Wealth 4 |
0.990 |
0.986 |
1.014 |
1.008 |
|
|
0.931 |
0.905 |
0.902 |
0.944 |
|
Positive support |
0.988* |
0.983** |
0.985** |
0.980** |
|
|
0.045 |
0.006 |
0.006 |
0.000 |
|
Negative interactions |
1.008 |
1.009 |
1.008 |
1.008 |
|
|
0.274 |
0.255 |
0.268 |
0.256 |
|
Index |
0.956* |
|
0.955** |
|
|
|
0.014 |
|
0.004 |
|
|
Frequency of meeting: |
|
|
|
|
|
Children |
|
1.017 |
|
1.004 |
|
|
|
0.655 |
|
0.914 |
|
Friends |
|
1.022 |
|
1.021 |
|
|
|
0.590 |
|
0.574 |
|
|
Early Deaths Excluded |
Early Deaths Included |
||
|
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
|
|
Other family |
|
0.983 |
|
0.991 |
|
|
|
0.679 |
|
0.804 |
|
Membership: |
|
|
|
|
|
Club other than below |
|
0.918* |
|
0.912* |
|
|
|
0.028 |
|
0.010 |
|
Sports club |
|
0.696** |
|
0.713** |
|
|
|
0.006 |
|
0.005 |
|
Religious organization |
|
1.023 |
|
0.997 |
|
|
|
0.798 |
|
0.968 |
|
Partner |
|
0.765** |
|
0.773** |
|
|
|
0.000 |
|
0.000 |
|
N |
10,541 |
10,541 |
10,745 |
10,745 |
|
Number of deaths |
|
|
|
|
|
NOTES: Medium-waist risk: 94-102 cm (men), 80-88 cm (women). High-waist risk: > 102 cm (men), > 88 cm (women). Wealth quintiles are single/couple-specific quintiles of gross housing wealth. *p < 0.05, **p < 0.01. SOURCE: Authors’ calculations from English Longitudinal Study of Ageing microdata. |
||||
(2) currently smoke, (3) a current nonsmoker who regularly smoked in the past, and (4) a current nonsmoker who only occasionally smoked in the past. The relative risks of these patterns of smoking behaviors were as expected—compared with those who never smoked, the highest relative mortality risks were for current smokers (59 percent higher risk for men and almost double for women), followed by ex-smokers who smoked regularly in the past (25-30 percent higher risk). There apparently is no statistically significant extra risk from having been an occasional smoker in the past. These estimated effects were similar by gender.
We found elevated mortality risks for those with greater waist circumference, especially for women—men with high waist risk had a 45 percent higher mortality hazard, and for women a close to 70 percent one. Finally, these models include controls for five wealth quintiles, with the top (richest) quintile serving as the reference group.1 For men, the relative risks increased with wealth quintiles, but at a highly nonlinear rate—that is, there is little
TABLE 8-4 English Mortality Hazard Models: Time (months) to Death from ELSA Wave 1 Interview Month (deaths within 12 months of interview excluded)
|
|
Men1 |
Men2 |
Women1 |
Women2 |
|
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
|
|
Ages 50-59 |
0.298** |
0.303** |
0.393** |
0.404** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ages 60-64 |
0.599** |
0.608* |
0.733 |
0.745 |
|
|
0.008 |
0.010 |
0.217 |
0.243 |
|
Ages 70-74 |
1.670** |
1.652** |
1.985** |
1.886** |
|
|
0.001 |
0.001 |
0.001 |
0.002 |
|
Ages 75-79 |
2.426** |
2.362** |
3.743** |
3.485** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ages 80-84 |
4.097** |
3.977** |
5.260** |
4.672** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ages 85+ |
7.803** |
7.099** |
12.448** |
10.925** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Smoker current |
1.683** |
1.589** |
1.936** |
1.856** |
|
|
0.000 |
0.001 |
0.000 |
0.000 |
|
Ex-smoker regular |
1.295* |
1.279 |
1.252* |
1.257* |
|
|
0.042 |
0.054 |
0.039 |
0.036 |
|
Ex-smoker occasional |
0.870 |
0.861 |
1.191 |
1.197 |
|
|
0.518 |
0.487 |
0.325 |
0.313 |
|
Medium-waist risk |
1.257 |
1.277 |
1.491* |
1.480* |
|
|
0.092 |
0.072 |
0.018 |
0.020 |
|
High-waist risk |
1.451** |
1.442** |
1.690** |
1.669** |
|
|
0.004 |
0.005 |
0.001 |
0.001 |
|
Wealth 1 |
1.572** |
1.533** |
1.282 |
1.226 |
|
|
0.003 |
0.006 |
0.116 |
0.207 |
|
Wealth 2 |
1.741** |
1.681** |
1.378* |
1.328 |
|
|
0.000 |
0.001 |
0.043 |
0.080 |
|
Wealth 3 |
1.429* |
1.406* |
1.411* |
1.378* |
|
|
0.021 |
0.030 |
0.032 |
0.049 |
|
Wealth 4 |
0.985 |
0.998 |
0.988 |
0.975 |
|
|
0.927 |
0.989 |
0.945 |
0.881 |
|
Positive support |
0.987 |
0.981* |
0.992 |
0.988 |
|
|
0.099 |
0.025 |
0.365 |
0.193 |
|
Negative interactions |
1.008 |
1.008 |
1.008 |
1.008 |
|
|
0.438 |
0.434 |
0.508 |
0.480 |
|
Index |
0.977 |
|
0.936* |
|
|
|
0.317 |
|
0.011 |
|
|
Frequency of meeting: |
|
|
|
|
|
Children |
|
1.062 |
|
0.966 |
|
|
|
0.248 |
|
0.535 |
|
Friends |
|
1.072 |
|
0.952 |
|
|
|
0.201 |
|
0.408 |
|
Other family |
|
0.965 |
|
1.008 |
|
|
|
0.518 |
|
0.900 |
|
|
Men1 |
Men2 |
Women1 |
Women2 |
|
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
|
|
Membership: |
|
|
|
|
|
Club other than below |
|
0.933 |
|
0.901 |
|
|
|
0.169 |
|
0.086 |
|
Sports club |
|
0.724 |
|
0.657* |
|
|
|
0.057 |
|
0.046 |
|
Religious organization |
|
1.053 |
|
1.015 |
|
|
|
0.692 |
|
0.904 |
|
Partner |
|
0.775* |
|
0.741** |
|
|
|
0.012 |
|
0.010 |
|
N |
4760 |
4760 |
5781 |
5781 |
|
Number of deaths |
|
|
|
|
|
NOTES: Medium-waist risk: 94-102 cm (men), 80-88 cm (women). High-waist risk: > 102 cm (men), > 88 cm (women). Wealth quintiles are single/couple-specific quintiles of gross housing wealth. *p < 0.05, **p < 0.01. SOURCE: Authors’ calculations from English Longitudinal Study of Ageing microdata. |
||||
evidence of any association above the third quintile. This association of mortality with baseline wealth was smaller among women.
Our main focus concerns the estimated mortality impacts of variables that measure aspects of the extent of social interactions reported by respondents. Our key variables can be conceptually divided into four groups: the extent of positive support and/or negative interactions, the presence of a spouse, the frequency of meeting with family and friends, and membership in clubs or organizations. In an alternative specification, the last three variables are also aggregated into a single measure of social interactions that we label the “index,” which is equivalent to the index of social networks used in previous sections.
Consider first estimates that include measures of positive and negative social support and the index. For our English sample, negative interactions were never statistically significant in either the combined gender or the gender-specific models. The amount of positive interaction was statistically significant in several of the models, pointing to a potentially relevant role of the quality of interactions in relation to mortality risk. The coefficient per unit change in positive support is quite small, although the range of this variable, which is 0-27, needs to be borne in mind when interpreting the magnitude of the coefficient. Examination of the distribution of this variable in the two samples (which is similar in both countries) shows that the majority of individuals were located toward the upper ends of the scale—a movement from the 25th percentile to the 75th percentile, for example,
would be an increase of around 7 points, from 15 to 22—suggesting a relatively small overall effect.
For our English sample, we found that the single aggregate social network index had a statistically significant protective effect on mortality. However, the estimated impacts of subcomponents are highly different and reject aggregation into a single index. Estimated impacts on subsequent mortality vary considerably across social network subcomponents. For men and women, presence of a spouse/partner was found to be highly protective of reduced future mortality. This replicates a widely found result in the literature. With this exception, we did not find any significant associations between any of the other social network measures and subsequent mortality. In this analysis, other than the spouse, we found no evidence that the frequency of meeting with children, friends, or other relatives has any impact on subsequent mortality.
Combining all different types of clubs (religious organizations, sports clubs, and all other types of clubs) into a single aggregate variable on club membership, we found a significant protective effect of clubs on subsequent mortality. However, the reason is apparent from disaggregation of club membership into its different forms. The only type of club that had a statistically significant negative impact on mortality is membership in sports clubs. A straightforward and plausible explanation for that association is not a social network effect, but that only healthier people are able or willing to join and remain members of sports clubs where exercise may be required. Membership of religious organizations or clubs (other than sports clubs or religious organizations) was not statistically significantly associated with mortality. This analysis demonstrates that it is essential to disaggregate club membership social network variables before drawing any conclusions about their potential health impacts.
Tables 8-5 and 8-6 contain parallel analysis for our U.S. HRS sample. We attempt to make our U.S. mortality analysis as close as possible to the English one, but some data differences remain. The key social network variables in HRS are in a 2004 psychosocial leave-behind module, so our analysis of U.S. mortality begins in 2004 and covers all deaths to the end of 2007, the most recent year of mortality follow-up. After excluding the first 12 months of follow-up, this provides approximately 2 or 3 years of mortality data for each respondent. Since our U.S. analysis is by necessity restricted to a random subsample of the full HRS sample that received the psychosocial leave-behind questionnaire, sample sizes are smaller than for the English ELSA, and the raw number of deaths in the analysis sample is also lower due to the shorter mortality follow-up period. Our empirical findings are somewhat less precise as a result.
While most variables are the same in English and U.S. samples, there are some differences. Variables that are identical include age groups, wealth
TABLE 8-5 U.S. Mortality Hazard Models: Time (months) to Death from HRS 2004 Wave Interview Month (by treatment of deaths within 12 months of interview)
|
|
Early Deaths Excluded |
Early Deaths Included |
||
|
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
|
|
Male |
1.225 |
1.219 |
1.387 |
1.378 |
|
|
0.276 |
0.288 |
0.037 |
0.042 |
|
Ages 50-59 |
0.315** |
0.322** |
0.330** |
0.334** |
|
|
0.004 |
0.005 |
0.002 |
0.002 |
|
Ages 60-64 |
0.632 |
0.638 |
0.820 |
0.821 |
|
|
0.223 |
0.232 |
0.522 |
0.524 |
|
Ages 70-74 |
2.029** |
2.056** |
2.343** |
2.375** |
|
|
0.018 |
0.016 |
0.001 |
0.001 |
|
Ages 75-79 |
2.879** |
2.889** |
3.334** |
3.351** |
|
|
0.002 |
0.002 |
0.000 |
0.000 |
|
Ages 80-84 |
4.483** |
4.550** |
4.245** |
4.290** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Ages 85+ |
8.485** |
8.802** |
7.521** |
7.692** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Smoker current |
1.402 |
1.415 |
1.216 |
1.221 |
|
|
0.186 |
0.175 |
0.374 |
0.365 |
|
Ever smoked |
1.615** |
1.614** |
1.566** |
1.566** |
|
|
0.015 |
0.016 |
0.008 |
0.008 |
|
Vigorous exercise |
0.582** |
0.574** |
0.455** |
0.451** |
|
|
0.029 |
0.025 |
0.001 |
0.000 |
|
Vigorous exercise 1 to 3 |
0.471 |
0.480 |
0.567 |
0.573 |
|
|
0.144 |
0.154 |
0.148 |
0.155 |
|
Wealth 1 |
3.161** |
3.269** |
2.786** |
2.875** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Wealth 2 |
2.179** |
2.249** |
2.047** |
2.105** |
|
|
0.014 |
0.011 |
0.007 |
0.005 |
|
Wealth 3 |
2.030** |
2.100** |
1.756** |
1.808** |
|
|
0.028 |
0.022 |
0.039 |
0.030 |
|
Wealth 4 |
1.522 |
1.545 |
1.404 |
1.412 |
|
|
0.209 |
0.194 |
0.227 |
0.220 |
|
Positive support |
1.031 |
1.032 |
1.020 |
1.020 |
|
|
0.044 |
0.043 |
0.120 |
0.120 |
|
Negative interactions |
1.025 |
1.024 |
1.014 |
1.012 |
|
|
0.156 |
0.189 |
0.356 |
0.398 |
|
Index |
0.959 |
|
0.984 |
|
|
|
0.318 |
|
0.662 |
|
|
Frequency of meeting: |
|
|
|
|
|
Children |
|
1.060 |
|
1.033 |
|
|
|
0.500 |
|
0.668 |
|
Family |
|
0.840 |
|
0.901 |
|
|
|
0.081 |
|
0.217 |
|
|
Early Deaths Excluded |
Early Deaths Included |
||
|
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
|
|
Friends |
|
0.983 |
|
1.033 |
|
|
|
0.853 |
|
0.675 |
|
Number of meetings |
0.996 |
0.996 |
0.996 |
0.995 |
|
|
0.149 |
0.133 |
0.085 |
0.070 |
|
Religion regularly |
0.649** |
0.658** |
0.620** |
0.621** |
|
|
0.034 |
0.041 |
0.006 |
0.007 |
|
Religion periodically |
0.927 |
0.929 |
0.965 |
0.965 |
|
|
0.738 |
0.744 |
0.852 |
0.849 |
|
Partner |
1.012 |
0.966 |
0.892 |
0.880 |
|
|
0.952 |
0.863 |
0.506 |
0.452 |
|
N |
3007 |
3007 |
3062 |
3062 |
|
Number of deaths |
|
|
|
|
|
*p < 0.05, **p < 0.01. SOURCE: Authors’ calculations from English Longitudinal Study of Ageing microdata. |
||||
quintiles, positive support and negative interactions, having a partner, and frequency of meeting with children, family, or friends. The main difference in social network domain concerns the membership variables. In ELSA, membership means whether you are a member of each of various types of organizations. Although there is a single question asking, for all organization types, in total, how many meetings are attended in a year, this variable was not used, primarily because of the inability to split out religious attendance from attendance at other organizations. In HRS, the closest comparable question is “Not including attendance at religious services, how often do you attend meetings or programs of groups, clubs, or organizations that you belong to?” We converted the possible answers into numbers of days per year.2
Since religious services are excluded in this question phrasing but are included in ELSA organizational membership questions, we added two variables that measure whether or not one attends religious services regularly or attends periodically. The omitted group is those who did not attend at all. For participation in clubs or organizations, our English analysis indicated that it was crucial to separate out participation in sports clubs or organizations. Since we had no direct HRS measure of sports club participation, we
TABLE 8-6 U.S. Mortality Hazard Models: Time (months) to Death from HRS 2004 Wave Interview Month (deaths within 12 months of interview excluded)
|
|
Men1 |
Men2 |
Women1 |
Women2 |
|
|
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
|
Ages 50-59 |
0.380 |
0.386 |
0.216** |
0.217** |
|
|
0.066 |
0.072 |
0.020 |
0.021 |
|
Ages 60-64 |
0.713 |
0.718 |
0.541 |
0.538 |
|
|
0.515 |
0.525 |
0.264 |
0.261 |
|
Ages 70-74 |
1.999 |
1.982 |
2.147 |
2.164 |
|
|
0.104 |
0.110 |
0.073 |
0.070 |
|
Ages 75-79 |
1.602 |
1.604 |
4.469** |
4.447** |
|
|
0.370 |
0.369 |
0.001 |
0.001 |
|
Ages 80-84 |
2.967** |
2.913** |
6.289** |
6.465** |
|
|
0.026 |
0.030 |
0.000 |
0.000 |
|
Ages 85+ |
8.184** |
8.219** |
10.365** |
10.997** |
|
|
0.000 |
0.000 |
0.000 |
0.000 |
|
Smoker current |
1.580 |
1.589 |
1.297 |
1.323 |
|
|
0.193 |
0.186 |
0.500 |
0.469 |
|
Smoker ever |
1.747 |
1.747 |
1.547 |
1.548 |
|
|
0.123 |
0.123 |
0.076 |
0.075 |
|
Vigorous exercise |
0.546 |
0.542 |
0.583 |
0.561 |
|
|
0.062 |
0.060 |
0.162 |
0.134 |
|
Vigorous exercise 1 to 3 |
0.393 |
0.396 |
0.642 |
0.638 |
|
|
0.201 |
0.205 |
0.541 |
0.536 |
|
Wealth 1 |
7.323** |
7.274** |
1.871 |
1.970 |
|
|
0.001 |
0.001 |
0.105 |
0.082 |
|
Wealth 2 |
3.428** |
3.408** |
1.745 |
1.842 |
|
|
0.033 |
0.035 |
0.152 |
0.118 |
|
Wealth 3 |
5.006** |
4.979** |
0.989 |
1.055 |
|
|
0.004 |
0.004 |
0.980 |
0.900 |
|
Wealth 4 |
2.978 |
3.001 |
1.057 |
1.072 |
|
|
0.064 |
0.062 |
0.895 |
0.870 |
|
Positive support |
1.019 |
1.021 |
1.045** |
1.044 |
|
|
0.393 |
0.361 |
0.049 |
0.055 |
|
Negative interactions |
1.039 |
1.037 |
1.011 |
1.007 |
|
|
0.134 |
0.148 |
0.677 |
0.775 |
|
Index |
0.972 |
|
0.954 |
|
|
|
0.669 |
|
0.398 |
|
|
Frequency of meeting: |
|
|
|
|
|
Children |
|
1.033 |
|
1.078 |
|
|
|
0.812 |
|
0.517 |
|
Family |
|
0.930 |
|
0.790 |
|
|
|
0.646 |
|
0.076 |
|
Friends |
|
0.936 |
|
1.024 |
|
|
|
0.642 |
|
0.849 |
|
Number of meetings |
0.995 |
0.995 |
0.996 |
0.995 |
|
|
Men1 |
Men2 |
Women1 |
Women2 |
|
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
Hazard ratio p-value |
|
|
|
0.252 |
0.263 |
0.262 |
0.212 |
|
Religion regularly |
1.106 |
1.124 |
0.456** |
0.455** |
|
|
0.740 |
0.703 |
0.004 |
0.004 |
|
Religion periodically |
0.843 |
0.856 |
0.976 |
0.958 |
|
|
0.643 |
0.675 |
0.934 |
0.883 |
|
Partner |
0.797 |
0.762 |
1.208 |
1.158 |
|
|
0.444 |
0.351 |
0.484 |
0.582 |
|
N |
1262 |
1262 |
1745 |
1745 |
|
Number of deaths |
|
|
|
|
|
*p < 0.05, **p < 0.01. SOURCE: Authors’ calculations from English Longitudinal Study of Ageing microdata. |
||||
added two variables measuring the extent of vigorous exercise.3 Finally, with regard to the other controls, we were unable to measure waist circumference in the U.S. sample, since in-person interviews to collect biomarker data did not start in HRS until 2006. Our categorization of smoking is also slightly different from the English specification presented earlier. More specifically, we included a dummy variable to capture whether an individual has ever smoked (regardless of their current smoking status), and then an additional variable to capture whether they are currently smoking. In addition, there is no measure of past smoking frequency, so there is no distinction between the two types of “ever-smoker” (i.e., regular and occasional).
The U.S. mortality analysis is presented in Table 8-5 and Table 8-6 using the same structure as the English mortality results. Consider briefly the nonsocial interaction and social support variables. Similar to our English results, mortality increased sharply with age, and there was a significant wealth gradient in mortality. In aggregate, smokers did have significantly elevated mortality rates, although the additional mortality risk for current smokers over and above past smokers was not statistically significant in this sample (presumably reflecting either inadequate statistical power or the relatively short follow-up period). With regard to physical activity, vigorous or intermediate exercise was associated with lower mortality risk.
Turning to social support variables for the U.S. sample, the evidence indicates that negative interactions had no statistically significant effect on subsequent mortality. Surprisingly, people who reported more positive
support were at elevated mortality risk during the follow-up. In gender-stratified models, this association was found for women but not for men. Similar to our English results, we found no statistically significant results for frequency of meeting with children, friends, or other relatives. Finally, the number of meetings of organizations or friends also appears to have no effect on subsequent mortality in America.
Attending religious services regularly but not periodically was associated with much lower subsequent mortality risk among women but not men. The concentration of a health promotion association of strong religious attendance among women is a common finding in U.S. samples (see, for example, Hummer et al., 2004; Deaton, 2009; Idler, 2009). There is as yet little consensus about what mechanisms may underlie that association, although some of the more obvious candidates, such as smoking, have been controlled in the analysis. Finally, having a partner was protective for mortality, but only for men. This contrasts with ELSA, in which we found a protective effect of partnership for both men and women.
In sum, we found relatively small or inconsistent effects of social interaction and network-type measures on subsequent mortality in either country with the length of follow-up period in cohorts to date. In some cases, we found associations that are inconsistent with well-established prior results (e.g., increased mortality among recipients of positive support). However, coupled with the lack of substantial differences in the distribution of social ties across the two countries, these results suggest that differences in social interactions across countries are quite unlikely to be a cause of longevity or life-expectancy differences between the United States and England.
VARIATIONS IN OTHER EUROPEAN COUNTRIES
Differences in life expectancy between England and the United States are less marked than between the United States and other industrialized countries. For example, in 2006, male life expectancy was 75 in the United States and 77 in the United Kingdom, while among women it was 80 for the United States and 81 for the United Kingdom (World Health Organization, 2009). Diverging trends between the United States and other countries are considerably more marked for populations in Sweden (79 for men and 83 for women), Switzerland (79 for men and 84 for women), Japan (79 for men and 86 for women), and Italy (78 for men and 84 for women) (World Health Organization, 2009). Similarly, as our analysis shows, the differences between England and the United States in the extent of social networks and kinds of interactions are small and in some cases quite subtle.
To explore the hypothesis that variations in social networks and interactions might explain cross-country variations in life expectancy in industrialized countries, we examined variations in social ties and life expectancy
in 28 countries, including Japan, the United States, and several European countries. In this exploratory analysis, we used data from the Gallup World Survey to examine variations in distributions of social connections and social participations across countries. Although the Gallup survey includes data for a much larger array of developing and developed countries, we focused on 28 member states of the Organisation for Economic Co-operation and Development and the European Union as a first step. We chose these countries because our purpose here is to understand diverging trends in life expectancy primarily among industrialized nations.
We used data from the Gallup World Survey to examine variations in distributions of social connections and social participations across countries. We discuss both first-order correlations and a simple descriptive model of aggregate levels of social connections and social participation and World Health Organization (WHO) data on life expectancy at birth. These analyses are not meant to be conclusive and aim only to broaden the research agenda by illustrating the potential to use cross-country variations in social networks to understand their role in explaining health variations among populations. We regard this analysis as descriptive, with the aim of opening the discussion about these associations and not at establishing any inferences of causality.
Measures
Social integration measures were obtained from the Gallup Survey (2006 and 2007) based on the following survey questions: (1) Have you attended a place of worship or religious service within the last 7 days? (2) What is your current marital status? (Marital status was measured as a dichotomous variable: married or living in a domestic partnership or not.) (3) Approximately how many hours did you spend, socially, with friends or family yesterday? (4) Have you done any of the following in the past month? … How about volunteered your time to an organization?
Life-expectancy measures for both men and women at birth and at ages 15, 50, and 65 were obtained for 2006 from the WHO Statistical Information System (see http://apps.who.int/whosis/data/Search.jsp?countries=[Location]. Members [accessed June 2010]). Results did not vary when Gallup measures for social integration (questions listed above) were assessed against life expectancy at these different ages, so, in the final analyses, only life expectancy at birth was used.
Distribution of Social Integration Across Countries
Tables 8-7 and 8-8 list mean levels of social integration and life expectancy for each of the 28 countries in the Gallup data. To highlight com-
TABLE 8-7 Distribution of Social Network Measures in 28 Countries Participating in the Gallup Survey, Women
|
|
Married or Living with Partner |
Attended Religious Services Past Week |
Social Time with Friends/ Family Yesterday (hours) |
Volunteered Time to an Organization in Past Month |
Life Expectancy |
|
Austria (2006) |
0.63 |
0.37 |
7.31 |
0.25 |
82.7 |
|
Belgium (2007) |
0.62 |
0.28 |
7.55 |
0.29 |
82.2 |
|
Canada (2005) |
0.63 |
0.33 |
— |
0.42 |
82.9 |
|
Cyprus (2006) |
0.64 |
0.60 |
5.54 |
0.17 |
81.9 |
|
Czech Republic (2007) |
0.55 |
0.15 |
4.50 |
0.19 |
79.9 |
|
Denmark (2007) |
0.64 |
0.21 |
7.26 |
0.25 |
81.0 |
|
Estonia (2006) |
0.47 |
0.12 |
5.10 |
0.17 |
78.5 |
|
Finland (2006) |
0.67 |
0.15 |
5.84 |
0.27 |
82.8 |
|
France (2006) |
0.55 |
0.19 |
6.50 |
0.28 |
84.2 |
|
Germany (2007) |
0.49 |
0.42 |
8.21 |
0.23 |
82.3 |
|
Greece (2007) |
0.56 |
0.38 |
3.52 |
0.07 |
82.5 |
|
Ireland (2006) |
0.59 |
0.63 |
5.27 |
0.41 |
81.9 |
|
Italy (2007) |
0.62 |
0.59 |
8.66 |
0.21 |
84.0 |
|
Japan (2007) |
0.67 |
0.23 |
10.75 |
0.24 |
85.9 |
|
Latvia (2006) |
0.46 |
0.19 |
5.11 |
0.18 |
76.3 |
|
Lithuania (2006) |
0.46 |
0.29 |
4.10 |
0.15 |
77.1 |
|
Netherlands (2007) |
0.59 |
0.26 |
8.33 |
0.38 |
82.0 |
|
Norway (2006) |
0.64 |
0.15 |
7.69 |
0.36 |
82.7 |
|
Poland (2007) |
0.61 |
0.71 |
7.56 |
0.09 |
79.5 |
|
Portugal (2006) |
0.61 |
0.50 |
5.41 |
0.11 |
82.3 |
|
Romania (2007) |
0.62 |
0.43 |
7.51 |
0.05 |
76.1 |
|
Slovakia (2006) |
0.51 |
0.53 |
5.28 |
0.13 |
78.3 |
|
Slovenia (2006) |
0.58 |
0.37 |
5.34 |
0.28 |
81.7 |
|
Spain (2007) |
0.59 |
0.33 |
7.83 |
0.16 |
84.1 |
|
Sweden (2007) |
0.67 |
0.14 |
8.44 |
0.12 |
83.0 |
|
Switzerland (2006) |
0.56 |
0.33 |
6.80 |
0.29 |
84.2 |
|
United Kingdom (2007) |
0.45 |
0.29 |
7.53 |
0.25 |
81.3 |
|
United States (2007) |
0.51 |
0.46 |
— |
0.43 |
80.4 |
|
SOURCE: Authors’ calculations from Gallup World Survey (2006-2007). |
|||||
parisons with our previous analysis, means for the United Kingdom and the United States appear in the last two rows. These tables show considerable variation among the industrialized countries in these social outcome measures. For example, the highest percentage of married/partnered women and men was found in Finland, Japan, and Sweden, where about 65 percent or more of people were married. The lowest percentages are in the United Kingdom and several countries in Eastern Europe or the former Soviet Union, where about 50 percent were married/partnered.
TABLE 8-8 Distribution of Social Network Measures in 28 Countries Participating in the Gallup Survey, Men
|
|
Married or Living with Partner |
Attended Religious Services Past Week |
Social Time with Friends/ Family Yesterday (hours) |
Volunteered Time to an Organization in Past Month |
Life Expectancy |
|
Austria (2006) |
0.61 |
0.28 |
7.13 |
0.35 |
77.2 |
|
Belgium (2007) |
0.67 |
0.22 |
7.97 |
0.30 |
76.6 |
|
Canada (2005) |
0.60 |
0.29 |
— |
0.33 |
78.3 |
|
Cyprus (2006) |
0.69 |
0.36 |
5.29 |
0.15 |
78.8 |
|
Czech Republic (2007) |
0.54 |
0.07 |
4.59 |
0.18 |
73.5 |
|
Denmark (2007) |
0.59 |
0.14 |
7.08 |
0.23 |
76.2 |
|
Estonia (2006) |
0.53 |
0.06 |
5.46 |
0.16 |
67.4 |
|
Finland (2006) |
0.65 |
0.12 |
5.23 |
0.32 |
75.8 |
|
France (2006) |
0.61 |
0.14 |
6.86 |
0.29 |
77.2 |
|
Germany (2007) |
0.52 |
0.37 |
8.41 |
0.23 |
77.0 |
|
Greece (2007) |
0.58 |
0.24 |
3.59 |
0.07 |
77.4 |
|
Ireland (2006) |
0.46 |
0.51 |
4.96 |
0.40 |
77.3 |
|
Italy (2007) |
0.60 |
0.51 |
8.41 |
0.22 |
78.4 |
|
Japan (2007) |
0.66 |
0.21 |
7.55 |
0.26 |
79.2 |
|
Latvia (2006) |
0.58 |
0.09 |
5.43 |
0.19 |
65.3 |
|
Lithuania (2006) |
0.61 |
0.15 |
4.87 |
0.11 |
65.3 |
|
Netherlands (2007) |
0.57 |
0.21 |
6.60 |
0.36 |
77.7 |
|
Norway (2006) |
0.63 |
0.19 |
7.76 |
0.42 |
78.1 |
|
Poland (2007) |
0.55 |
0.62 |
7.23 |
0.12 |
70.9 |
|
Portugal (2006) |
0.65 |
0.31 |
5.71 |
0.13 |
75.5 |
|
Romania (2007) |
0.61 |
0.30 |
7.28 |
0.06 |
69.2 |
|
Slovakia (2006) |
0.58 |
0.34 |
5.00 |
0.13 |
70.4 |
|
Slovenia (2006) |
0.64 |
0.27 |
5.11 |
0.36 |
74.4 |
|
Spain (2007) |
0.57 |
0.23 |
7.46 |
0.13 |
77.5 |
|
Sweden (2007) |
0.64 |
0.10 |
8.14 |
0.13 |
78.7 |
|
Switzerland (2006) |
0.57 |
0.27 |
5.58 |
0.39 |
79.1 |
|
United Kingdom (2007) |
0.54 |
0.20 |
7.16 |
0.21 |
77.0 |
|
United States (2007) |
0.58 |
0.46 |
— |
0.43 |
75.5 |
|
SOURCE: Authors’ calculations from Gallup World Survey (2006-2007). |
|||||
There is even wider variation in attendance at religious ceremonies. In Ireland, Italy, and Poland, between 50 and 60 percent of people attended a religious ceremony in the past week. In the United States, 46 percent of men and women reported similar attendance, but only 29 percent of the English did so. At the other extreme, attendance was 15 percent or below for France, Sweden, and several Eastern European or former Soviet countries. Turning to social time with family and friends, there was much variation
across countries. Japan, Switzerland, and the Netherlands reported among the highest levels of social time, while Greece and the Czech Republic reported relatively low levels. This question was not asked in U.S. and Canadian samples. Time volunteered to an organization in the past month also varied widely among countries, with the United States ranking highest for both men and women (43 percent), followed by Ireland, the Netherlands, and Norway. In several countries, less than 15 percent of the population reported volunteering, among them Greece and Romania.
Associations with Life Expectancy
To illustrate a simple first-order relationship between life expectancy and measures of social integration, Figures 8-5, 8-6, 8-7, and 8-8 show plots of life expectancy at birth for men and women against country-level means or percentages for four types of social connections or social participation: religious attendance, partnership status, social time with friends and relatives, and volunteered time. Table 8-9 presents a simple multivariate model predicting country-level life expectancy that includes all social network variables.
Countries with higher percentages of ties with regard to marriage had higher life expectancy (Figures 8-5A and 8-5B). However, in our model that controls for all measures of social ties and participation, this association was statistically significant for women (p = .05) but not for men (p = .35). Countries with high levels of social time also had higher life expectancy (Figures 8-7A and 8-7B), but these associations were not significant in multivariate models (the effect is positive but the p-values are around 0.2). A higher percentage who volunteered their time was associated with higher life expectancy (Figures 8-8A and 8-8B), and this association was significant for men (p = .02) and of borderline significance for women (p = .06). Finally, there is no correlation between life expectancy and religious attendance (Figures 8-6A and 8-6B) or in the results shown in Table 8-9.4
This analysis indicates large variability across these countries both in life expectancy and aggregate levels and distribution of social integration and social ties and participation. While our results indicate that some measures of social integration might be correlated with life expectancy, aggregated Gallup data for these industrialized countries by themselves were not able to distinguish sufficiently among alternative measures of social integration, even without placing into these models other relevant health behaviors on which countries differ. Even if we take these results at face value, their
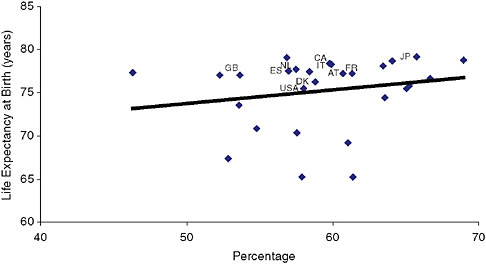
FIGURE 8-5A Life expectancy and marriage/living with partner for men in 28 countries.
NOTE: AT = Austria, CA = Canada, DK = Denmark, ES = Estonia, FR = France, GB = Great Britain, IT = Italy, JP = Japan, NL = the Netherlands, USA = United States.
SOURCE: Authors’ calculations from the Gallup World Survey (2006-2007).
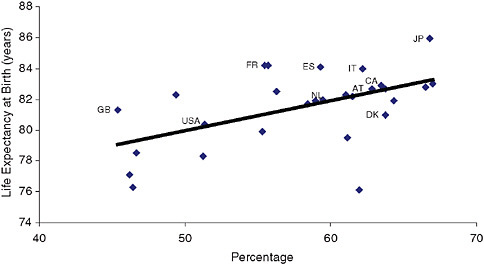
FIGURE 8-5B Life expectancy and marriage/living with partner for women in 28 countries.
NOTE: AT = Austria, CA = Canada, DK = Denmark, ES = Estonia, FR = France, GB = Great Britain, IT = Italy, JP = Japan, NL = the Netherlands, USA = United States.
SOURCE: Authors’ calculations from the Gallup World Survey (2006-2007).
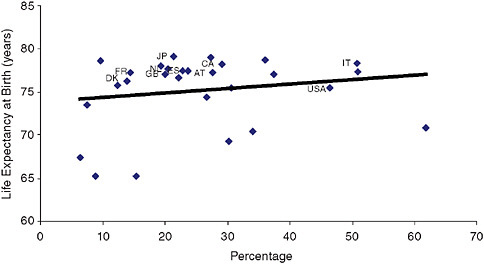
FIGURE 8-6A Life expectancy and religious attendance in past week for men in 28 countries.
NOTE: AT = Austria, CA = Canada, DK = Denmark, ES = Estonia, FR = France, GB = Great Britain, IT = Italy, JP = Japan, NL = the Netherlands, USA = United States.
SOURCE: Authors’ calculations from the Gallup World Survey (2006-2007).
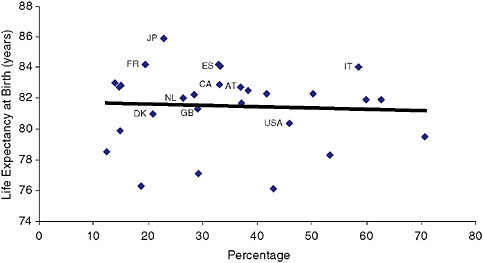
FIGURE 8-6B Life expectancy and religious attendance in past week for women in 28 countries.
NOTE: AT = Austria, CA = Canada, DK = Denmark, ES = Estonia, FR = France, GB = Great Britain, IT = Italy, JP = Japan, NL = the Netherlands, USA = United States.
SOURCE: Authors’ calculations from the Gallup World Survey (2006-2007).
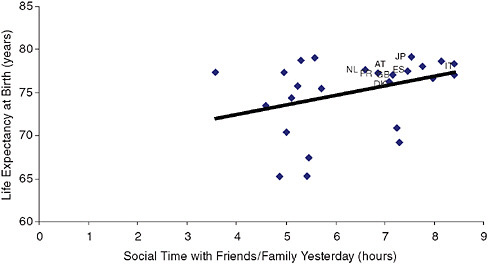
FIGURE 8-7A Life expectancy and social time for men in 28 countries.
NOTE: AT = Austria, CA = Canada, DK = Denmark, ES = Estonia, FR = France, GB = Great Britain, IT = Italy, JP = Japan, NL = the Netherlands, USA = United States.
SOURCE: Authors’ calculations from the Gallup World Survey (2006-2007).
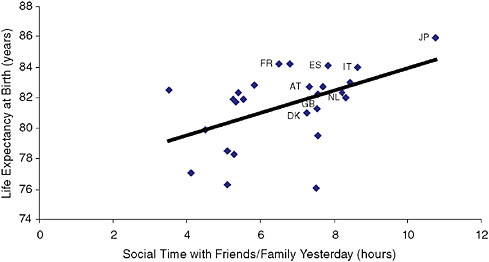
FIGURE 8-7B Life expectancy and social time for women in 28 countries.
NOTE: AT = Austria, CA = Canada, DK = Denmark, ES = Estonia, FR = France, GB = Great Britain, IT = Italy, JP = Japan, NL = the Netherlands, USA = United States.
SOURCE: Authors’ calculations from the Gallup World Survey (2006-2007).
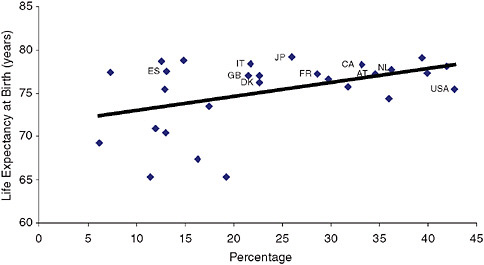
FIGURE 8-8A Life expectancy and volunteered time to organization in past month for men in 28 countries.
NOTE: AT = Austria, CA = Canada, DK = Denmark, ES = Estonia, FR = France, GB = Great Britain, IT = Italy, JP = Japan, NL = the Netherlands, USA = United States.
SOURCE: Authors’ calculations from the Gallup World Survey (2006-2007).
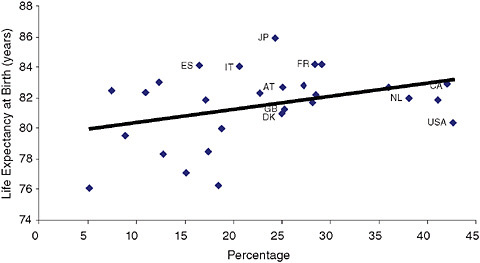
FIGURE 8-8B Life expectancy and volunteered time to organization in past month for women in 28 countries.
NOTE: AT = Austria, CA = Canada, DK = Denmark, ES = Estonia, FR = France, GB = Great Britain, IT = Italy, JP = Japan, NL = the Netherlands, USA = United States.
SOURCE: Authors’ calculations from the Gallup World Survey (2006-2007).
TABLE 8-9 Linear Regression Model of Country Life Expectancy on Social Participation and Ties: Gallup and World Health Organization Data
implications for explaining the U.S. health disadvantage are far from clear. While America might rank relatively low on some measures of social integration, such as marriage and social ties, it ranks relatively high on other measures, such as religious attendance and especially volunteering. Finally, the extent to which these associations are causal, produced by reverse causation, or are the result of underlying variations in third factors, such as gross domestic product, needs to be adequately examined in future research. Our purpose is to illustrate the window of opportunity to examine these issues by capitalizing on variations across countries in social integration and life expectancy.
IMPLICATIONS
In this chapter we attempt to assess whether aspects of social relationships and social participation might account for country differences in morbidity and life expectancy. The findings from our cross-sectional analyses and 3- to 5-year follow-ups suggest that current differences in these social conditions between the United States and England do not explain current differences in mortality or morbidity. First, observed differences in social networks and support between these two countries are small. Second, we found weak and inconsistent effects of the social network and support variables on the health outcomes we considered, with few associations reaching conventional levels of statistical significance.
Our analyses highlight the difficulty in undertaking comparative analyses in these domains. Even with tightly harmonized studies, such as HRS and ELSA, some differences in measurement remain, and mortality follow-up periods for studies with relevant social network constructs remain relatively short—5 years for ELSA and 3 years for HRS. Only time will tell whether these factors affect our results, as future data waves become available. The potential contribution of future data and analysis derived from long-term follow-ups of these and other, even more tightly harmonized cohorts is clear.
We found remarkable similarities in the cross-sectional distributions of social contacts and participation between the United States and England. We focused on these two countries because comparable data on social contacts and health were available for these populations, and recent research has demonstrated that health differences in morbidity are large. However, given the similarity in the two distributions, this focus also limited our ability to detect the potential role that these factors might have in a context of wider variation in social contacts and support. Our descriptive analysis based on the Gallup survey illustrates this limitation by pointing out the much larger variability in social contacts in other industrialized nations. Our analysis of England and the United States might not reveal the full potential contribution of social networks and social support to health differences across a broader set of countries. In exploring whether social networks might account for cross-country differences, priority should therefore be given to harmonizing data across countries that allow us to test this hypothesis in a broader international context.
A second issue refers to what the appropriate measures of social networks and participation might be. We have focused here on self-reports of frequency of contacts and levels of positive and negative support in England and America. Beyond these measures, there may be other key aspects, including how close relationships truly are and whether individuals feel they can rely on a social network. These less tangible aspects of social networks might have health effects not captured by the measures in our surveys. For example, some studies suggest that it might be the perception of social connectedness rather than the actual level of social support that influences health outcomes (Ashida and Heaney, 2008). Others have argued that one special friend or relative is the key concept, implying that the nature of the relations with others may not be relevant. Compared with many areas of determinants of health, the development of conceptual measures of social networks and support is relatively recent. It is fair to say that the field has not yet reached a consensus on the most appropriate set of conceptual measures, especially harmonized measures in an international comparative context.
Besides social networks and integration, other aspects of social behavior
not incorporated into our study could be important in explaining health differences among countries. In addition, social contacts may influence health via several distinct mechanisms, including social regulation and behavioral norms; direct contagion of disease; transfer of material resources or information; positive emotional experiences, such as feeling loved, valued, or “belonging” to a group; or negative emotional experiences, such as shame or loneliness (Berkman and Glass, 2000). The importance of each pathway may depend on the specific health outcome—for example, smoking behavior may be very responsive to norms and social regulation, whereas they may be less relevant for breast cancer survival rates. Our study focuses primarily on whether networks and support have an overall association with health outcomes, but future studies should examine whether other social mechanisms might contribute to health differences across countries.
A fourth issue refers to differences in reporting styles among countries. While we found no differences in levels of social support and networks between English and U.S. respondents, many measures rely on subjective scales that have been shown in other contexts to exhibit considerable international variation (Kapteyn, Smith, and VanSoest, 2007). Individuals in each country might report their level of contact using different reporting thresholds, which may in turn influence their answers to these subjective questions. Additional investigations, perhaps including the use of vignettes, are needed in order to evaluate heterogeneity in reporting styles and, if such heterogeneity exists, to identify true differences in the distribution of social networks and support among countries.
A final set of issues relates to the fact that our analysis has been predominantly cross-sectional in nature, out of necessity given the availability of comparable data. As such, we can neither investigate nor control for intertemporal or, for that matter, intergenerational issues. This has a number of consequences. First, we can say nothing about how current differences across countries (to the extent they exist) in social integration and interactions might affect future life expectancy, nor how past trends in social integration are related to past trends in life expectancy. Second and closely related, to the extent that there are differences among countries in the level and trajectories of past social interactions and this history matters for current health and mortality outcomes, these differences are uncontrolled for in our study. Once again, when one extends the set of countries being analyzed beyond the United States and England, this may be an even more important issue than when considering these two countries alone. For example, to the extent that historical trajectories in Europe and the former Soviet Union countries differ for marriage, age of childbearing, and single parenthood, there may well be knock-on effects onto past trajectories of social support and integration, which could plausibly affect life-course health and mortality outcomes, and hence life expectancy, in these countries. Given the data
available, investigation of such a hypothesis is beyond the scope or capacity of our analysis. Similarly, it is also impossible to investigate the hypothesis that one possible role of social integration and support is alleviating or mitigating the consequences of adverse shocks when they happen, given the lack of internationally comparable historical data. The intuitive plausibility of such intertemporal hypotheses suggests that data collection activities should be prioritized in order to facilitate analyses of these issues in the future.
Taken together, the analyses of this chapter and the caveats in the discussion above suggest that future research should focus on identifying multiple measures that can capture the most relevant aspects of the life-course trajectories of social networks, integration, and support that might be important to health, as well as developing strategies to make these measures comparable across countries. Until that happens, claims about the power of social network constructs to explain international health differences are still premature. Such an approach might also yield a new line of research that will allow the testing of the role of social networks and support in explaining diverging trends in life expectancy in a wider set of industrialized nations.
REFERENCES
Ashida, S., and Heaney, C.A. (2008). Differential associations of social support and social connectedness with structural features of social networks and the health status of older adults. Journal of Aging Health, 20(7), 872-893.
Banks, J., Marmot, M., McMunn, A., and Smith, J.P. (n.d.). The English Are Healthier Than Americans: Do Social Risk-Factors Contribute? Manuscript in preparation.
Banks, J., Marmot, M., Oldfield, Z., and Smith, J.P. (2006). Disease and disadvantage in the United States and in England. Journal of the American Medical Association, 295(17), 2037-2045.
Berkman, L.F., and Glass, T. (2000). Social integration, social networks, social support, and health. In L.F. Berkman and I. Kawachi (Eds.), Social Epidemiology (pp. 137-173). New York: Oxford University Press.
Berkman, L.F., and Syme, S.L. (1979). Social networks, host resistance, and mortality: A nineyear follow-up study of Alameda County residents. American Journal of Epidemiology, 109(2), 186-204.
Berkman, L.F., Melchior, M., Chastang, J.F., Niedhammer, I., Leclerc, A., and Goldberg, M. (2004). Social integration and mortality: A prospective study of French employees of Electricity of France-Gas of France: The GAZEL Cohort. American Journal of Epidemiology, 159(2), 167-174.
Blazer, D.G. (1982). Social support and mortality in an elderly community population. American Journal of Epidemiology, 115(5), 684-694.
Deaton, A. (2009). Aging, Religion, and Health. NBER Working Paper w15271. Cambridge, MA: National Bureau of Economic Research.
Fuhrer, R., and Stansfeld, S.A. (2002). How gender affects patterns of social relations and their impact on health: A comparison of one or multiple sources of support from “close persons.” Social Science & Medicine, 54(5), 811-825.
Fuhrer, R., Stansfeld, S.A., Chemali, J., and Shipley, M.J. (1999). Gender, social relations and mental health: Prospective findings from an occupational cohort (Whitehall II study). Social Science & Medicine, 48(1), 77-87.
House, J.S., Robbins, C., and Metzner, H.L. (1982). The association of social relationships and activities with mortality: Prospective evidence from the Tecumseh Community Health Study. American Journal of Epidemiology, 116(1), 123-140.
Hummer, R.A., Ellison, C.G., Rogers, R.G., Moulton, B.E., and Romero, R.R. (2004). Religious involvement and adult mortality in the United States: Review and perspective. Southern Medical Journal, 97(12), 1223-1230.
Idler, E., Contrada, R.J., Boulifard, D.A., Labouvie, E.W., Chen, Y., and Krause, T.J. (2009). Looking in the black box of “attendance at services”: Exploring an old dimension for religion and health research. International Journal for the Psychology of Religion, 9, 1-20.
Juster, F.T., and Suzman, R. (1995). An overview of the Health and Retirement Study. Journal of Human Resources, 30, S7-S56.
Kaplan, G.A., Salonen, J.T., Cohen, R.D., Brand, R.J., Syme, S.L., and Puska, P. (1988). Social connections and mortality from all causes and from cardiovascular disease: Prospective evidence from eastern Finland. American Journal of Epidemiology, 128(2), 370-380.
Kapteyn, A., Smith, J.P., and VanSoest, A. (2007). Vignettes and self-reported work disability in the US and the Netherlands. American Economic Review, 97(1), 461-473.
Khang, Y.H., and Kim, H.R. (2005). Explaining socioeconomic inequality in mortality among South Koreans: An examination of multiple pathways in a nationally representative longitudinal study. International Journal of Epidemiology, 34(3), 630-637.
Marmot, M., Banks, J., Blundell, R., Lessof, C., and Nazroo, J. (Eds.). (2002). Health, Wealth, and Lifestyles of the Older Population in England: The 2002 English Longitudinal Study of Ageing. London, England: Institute for Fiscal Studies.
Netuveli, G., Wiggins, R.D., Hildon, Z., Montgomery, S.M., and Blane, D. (2005). Functional limitation in long standing illness and quality of life: Evidence from a national survey. British Medical Journal, 331(7529), 1382-1383.
Orth-Gomer, K., and Johnson, J.V. (1987). Social network interaction and mortality: A six-year follow-up study of a random sample of the Swedish population. Journal of Chronic Diseases, 40(10), 949-957.
Orth-Gomer, K., Unden, A.L., and Edwards, M.E. (1988). Social isolation and mortality in ischemic heart disease: A 10-year follow-up study of 150 middle-aged men. Acta Medica Scandinavica, 224(3), 205-215.
Orth-Gomer, K., Rosengren, A., and Wilhelmsen, L. (1993). Lack of social support and incidence of coronary heart disease in middle-aged Swedish men. Psychosomatic Medicine, 55(1), 37-43.
Orth-Gomer, K., Horsten, M., Wamala, S.P., Mittleman, M.A., Kirkeeide, R., Svane, B., Ryden, L., and Shenck-Gustafsson, K. (1998). Social relations and extent and severity of coronary artery disease: The Stockholm Female Coronary Risk Study. European Heart Journal, 19(11), 1648-1656.
Penninx, B.W., Guralnik, J.M., Ferrucci, L., Simonsick, E.M., Deeg, D.J., and Wallace, R.B. (1998). Depressive symptoms and physical decline in community-dwelling older persons. Journal of the American Medical Association, 279(21), 1720-1726.
Sugisawa, H., Liang, J., and Liu, X. (1994). Social networks, social support, and mortality among older people in Japan. Journal of Gerontology, 49(1), S3-S13.
Welin, L., Tibblin, G., Svardsudd, K., Tibblin, B., Ander-Peciva, S., Larsson, B., and Wilhelmsen, L. (1985). Prospective study of social influences on mortality: The study of men born in 1913 and 1923. Lancet, 1(8434), 915-918.
World Health Organization. (2009). WHO Statistical Information System. Available: http://apps.who.int/whosis/data/ [accessed August 2009].








































