
2
A Global Perspective on
Drug-Resistant Tuberculosis
Key Messages
- Despite considerable progress against drug-resistant TB in many countries, great challenges remain in the areas of infection control, diagnostics, treatment, and drug development.
- Unless these challenges are met, the numbers of cases and levels of drug resistance will continue to rise.
- The battle against drug-resistant TB can be viewed from a social medicine perspective, in which social and biomedical factors are intertwined.
Salmaan Keshavjee, Harvard Medical School, Partners In Health, and chair of WHO’s Green Light Committee (GLC), explained that MDR TB occurs in most countries of the world. In parts of Europe and Asia, rates of MDR TB among new TB cases from 1994 through 2009 were less than 6 percent. In parts of Eastern Europe and Russia, however, this figure was more than 18 percent. In many parts of the world, 12−30 percent of patients being retreated for TB have MDR TB. In some parts of Eastern Europe and Central Asia, MDR TB represents more than 50 percent of retreatment cases.
Keshavjee shared 2008 data from WHO indicating that among 27 high-burden countries, China, India, and Russia have the highest numbers
of MDR TB patients. It is estimated that 50 percent of MDR TB cases worldwide occur in China and India. Other countries with large numbers of MDR TB cases include Bangladesh, Indonesia, Myanmar, Nigeria, Pakistan, the Philippines, and South Africa.
This chapter begins by briefly reviewing the difficulties involved in estimating the burden of MDR TB. It then looks at MDR and XDR TB first in South Africa and then in China. The fourth section presents an historical perspective on MDR TB control efforts. The final section details remaining challenges in global efforts to combat MDR TB.
DIFFICULTIES IN ESTIMATING THE BURDEN OF MDR TB1
The official figures for MDR TB prevalence and incidence raise many questions. Farmer cited official numbers of 1.5 million cases of MDR TB, with 500,000 new cases annually. But he raised the question of how prevalence could remain at 1.5 million with 500,000 new cases annually given existing rates of mortality and transmission.
Farmer acknowledged that estimating the prevalence and incidence of diseases such as TB is extremely complicated. In Lesotho and Peru, for example, similar conditions exist. They include poor health care infrastructures, limited access to diagnostics, fragmented health care delivery systems, a lack of public support for TB care, varying levels of knowledge about TB among providers, inadequate infection control, and a shortage of appropriate drugs for circulating strains. However, the importance of these factors differs considerably between the two countries. In Lesotho, for example, transnational migration is a significant part of the problem, but it is much less important in Peru. These differences make modeling and quantification difficult. Farmer quoted the French poet Paul Valéry: “All that is simple is false, and all that is complex is useless.”
Farmer noted that modeling is a good way to estimate the size of a problem. It may be the case, as some have insisted, that half of TB cases are not diagnosed at all and that the number of drug-resistant TB cases is unknown. But important progress has been made in the past decade. XDR TB is recognized as a serious health issue. Molecular diagnostics have created a much deeper understanding of the resistance problem. According to Farmer, it will be especially useful to link a social medicine perspective on the disease with new molecular techniques to better appreciate the dimensions of the epidemic, as well as the directions in which it is headed (see Box 2-1).
![]()
1 This section is based on the presentation of Dr. Farmer.
BOX 2-1
A Social Medicine Perspectivea
Farmer suggested that a social medicine perspective is the best way to think about TB, whether considering new diagnostics, new therapeutics, or programs to prevent and respond to drug-resistant TB. This social medicine perspective is deeply rooted in Russia, where social vulnerability is a leading cofactor for TB. For example, rates of TB are much higher among the unemployed than the employed in Russia, in the United States, and throughout the world.
Drug resistance is also a social medicine problem. Just a few weeks after the introduction of streptomycin to combat TB in the 1940s, patients began to develop resistance to the drug. TB specialists sometimes forget a general rule of infectious disease—when pathogens are challenged with anti-infectives, they mutate and develop resistance. Farmer noted that this is a classic social medicine problem in infectious disease. The development of drug resistance is a natural cycle, although modern medicine can break this cycle by introducing new diagnostics or therapeutics.
An integral part of a social medicine perspective is the understanding that help-seeking behaviors also have a profound influence on a disease like TB. Regardless of whether formal programs or national policies to treat MDR TB are in place, the sick and their family members seek care. Farmer said this help-seeking behavior is a powerful driver of antibiotic use, which in turn shapes drug resistance.
Uncontrollable natural forces also have a profound effect on population health and the ability to provide care. An obvious example comes from the devastation in Haiti that occurred early in 2010. When the Haitian earthquake leveled the entire capital city—with 20 percent of all federal employees in Haiti being killed—not just the physical but the human infrastructure was massively disrupted, said Farmer. For example, of the eight people from the United Nations on the leadership team in Haiti with which Farmer was working, seven were killed. Farmer said this has been a reminder, in a very crude way, of the fact that large-scale social forces that are completely beyond the control of physicians, epidemiologists, pharmaceutical manufacturers, and policy makers can shape, and reshape, the dimensions of a problem.
The collapse of the Soviet Union in the late 1980s similarly led to enormous disruptions in the provision of TB prevention and care. Interruptions in the supply chain of medications led to acquired resistance, and high rates of incarceration helped the disease spread. “In other words, large-scale social and political forces shaped the nature of the epidemic here, as elsewhere in the world,” said Farmer.
Biosocially complex phenomena require multiple and complementary methodologies. A useful metaphor is to think of several spigots or faucets turned on at the same time. In the 1980s, drug resistance was thought to arise from inadequate treatment programs and from patients who failed to adhere to treatment regimens. According to Farmer, “It turns out that there are many more spigots turned on than we understood.” Reinfection played a major role. Nosocomial transmission served to amplify the epidemic. Strain variation became a consideration. While the number of turned-on spigots is not infinite, Farmer said, there are at least four or five major factors that vary from place to place. The bottom line is that drug-resistant TB is an exceedingly complex disease that will require more than simple models.
The TB community has several immutable responsibilities, Farmer said:
- It must work on novel tools for prevention, diagnosis, and care. Most of these tools will come from basic science.
- It must avoid trade-offs between prevention and care, which in turn reflect trade-offs between public health and clinical medicine. “Those trade-offs have been very palpable and pernicious,” he said, especially in places where resources are scarce. On a positive note, new diagnostics are being linked more rapidly to implementation, and many more people now understand that proper diagnosis and treatment are central to prevention. This represents important progress. In Russia, in particular, prevention and care have been integrated for many decades.
- It must work from a biosocial framework, whether the subject is basic science or TB control. In particular, MDR and XDR TB can be properly understood only from this broad biosocial view.
- The flow from several spigots can be stopped at the same time. Infection control is linked to ventilation, to administrative controls, and to the quality of diagnosis and care. Diagnostic methods are linked to both care and prevention. For example, a molecular diagnostic for rifampin resistance would be invaluable, since one mutation describes about 80 percent of rifampin resistance, and
rifampin resistance stands as a marker for MDR TB. Yet such a diagnostic is not yet available,b although Farmer commended the Russian TB community for working hard to improve the quality of diagnostics. “We need new preventives, we need a vaccine, we need new diagnostics, we need new therapeutics, and we also need to focus on the implementation gap and get these out into the field,” Farmer said. New discoveries and technologies will be essential to counter increasingly resistant TB. New drugs now in development pipelines were not even imagined several years ago. Also, a paradigm shift in diagnostics is about to occur with the advent of molecular techniques. These advances could be a large part of the solution to the problem.
Clinical trials cannot be conducted ethically without a commitment to improving the scope, scale, and quality of clinical efforts, Farmer said. There needs to be a unified, aspirational standard of care, not the cheap comfort of alternative therapies for people from different backgrounds or different regions. The clinical imperative must always be transregional and transnational, even though most regulatory bodies and review boards are either institutional or national. That is why international workshops and other meetings are so important, according to Farmer, even though “transnational” is a term not used frequently in clinical medicine. This tension between the local and the translocal, or between the small-scale and the large-scale, is inevitable, Farmer said, especially when dealing with an airborne communicable disease. Farmer stated that he has a deep faith in the ability of science to help us develop the tools we need.
![]()
aThis box is based on the presentation of Dr. Farmer.
bSince the workshop was held, a new, fully automated DNA test (Xpert MTB/RIF) for TB has been validated and subsequently recommended by WHO for broad implementation as the initial diagnostic for individuals suspected of MDR TB or HIV−TB coinfection. The test simultaneously detects TB and rifampicin drug resistance (a reliable indicator for MDR TB) in sputum. WHO reports that the Foundation for Innovative New Diagnostics (FIND) has negotiated a reduced price for 116 low- and middle-income countries (including South Africa, Russia, India, and China) of US$16.86 per test cartridge. The test provides results in 100 minutes, allowing proper treatment to begin immediately (WHO, 2010d).
MDR AND XDR TB IN SOUTH AFRICA2
Coetzee reported that the incidence of TB in South Africa is 600 cases per 100,000 population and in two of the country’s provinces, the incidence is well over 1,000 per 100,000 population. At the same time, the prevalence of HIV coinfection in TB patients is about 60 percent.
In 2007, South Africa had the fourth-highest reported total number of MDR TB cases among nations. In 2009 the total exceeded 9,000 patients, which is a large number for a country with 48 million people. At the same time, the percentage of MDR TB cases among new TB patients remains below 5 percent. South Africa also has a significant XDR TB burden, accounting for 7–8 percent of MDR TB cases. These numbers are not exact, said Coetzee, because some provinces are grossly underserviced, making it impossible to draw firm conclusions about numbers of cases.
MDR AND XDR TB IN CHINA3
China is a very large country with a population of more than 1.3 billion. It consists of 31 provinces and the Xinjiang construction corps, along with two special administrative regions—Hong Kong and Macao. Chen described the country’s strategies for MDR TB control and prevention. According to a national TB prevalence survey conducted in 2000, China had about 4.5 million TB patients; about 1.5 million new cases occurred that year and 130,000 deaths from TB. According to Chen, more recent data indicate that China has more than 1.3 million new cases of TB each year, representing the world’s second-largest TB burden.
The estimated incidence of MDR TB is about 120,000 annually, and the estimated incidence of smear sputum−positive MDR TB is about 80,000—again the second-largest burden among the 27 MDR TB high-burden countries. Box 2-2 presents the results of a national drug resistance surveillance conducted in China in 2007–2008.
As noted in Chapter 1, patients with MDR TB need longer and more complex treatments than those with drug-susceptible TB. Since at least four second-line drugs are required, MDR TB patients experience more serious adverse drug reactions, and expenditures for these patients can be 100 times greater or more than those for drug-susceptible cases. In the 16 provinces of China where the Global Fund to Fight AIDS, TB, and Malaria is supporting the treatment and management of drug-resistant TB patients, the total budget is about $78 million.
![]()
2 This section is based on the presentation of Gerrit Coetzee, National Health Laboratory Service of South Africa.
3 This section is based on the presentation of Mingting Chen, National Centre of Tuberculosis Control and Prevention of China.
China has encountered success in controlling and preventing TB, said Chen. The Directly Observed Therapy, Short course (DOTS) coverage rate is 100 percent, the detection rate of new cases is about 80 percent, and the cure rate for new cases is more than 90 percent. China achieved the targets set by the country’s National Tuberculosis Plain and cured 3.1 million patients from 2001 to 2007.
To combat MDR and XDR TB, China is enhancing the quality of DOTS through several steps:
- making a strong government commitment;
- improving the laboratory network;
- identifying TB patients in vulnerable groups and giving them more care;
- improving the recording and reporting system for TB;
- improving the quality of drugs, including first-line and second-line drugs;
- implementing improved practices in drug supply and management systems; and
- emphasizing cooperation between public health institutes and hospitals.
China also is formulating a national policy and launching pilot projects for the programmatic management of drug-resistant TB. It is increasing the number of pilot sites for implementing drug resistance surveillance and is improving laboratories from the national to the county level to meet the standards for MDR TB diagnostic tests (see Box 2-2 for a discussion of China’s drug-resistant TB surveillance results).
For the treatment and management of MDR and XDR TB patients, China is taking steps in the areas of technical support, research, drug resistance surveillance, diagnosis, and cooperation. In the area of technical support, it is developing:
- guidelines for the programmatic management of MDR TB;
- a manual for second-line drug management;
- guidelines for TB infection control;
- guidelines for responding to adverse drug reactions; and
- a manual for drug susceptibility testing for laboratories.
In the area of research, China is:
- conducting a survey of policies against MDR and XDR TB;
BOX 2-2
Drug-Resistant TB in China: Surveillance Resultsa
Renzhong Li of the Center for Disease Control and Prevention, China, reported that China has been engaged in an effort to establish a surveillance system for resistance to anti-TB drugs according to guidelines from WHO and the International Union Against Tuberculosis and Lung Disease. The goals have been to collect data on initial and acquired drug resistance in 11 provinces initially and then for the whole country, to determine the prevalence of drug-resistant TB at the provincial and national levels, and to evaluate the efficacy of ongoing TB control strategies.
During the national drug resistance surveillance in 2007–2008, 70 counties in all 31 provinces of China were randomly selected for surveillance by cluster sampling. Sputum smears and cultures were examined at the county level, while drug susceptibility tests were performed at the national level. Bacterial typing and susceptibility testing were done for all positive samples. The patient’s history was carefully obtained, and available medical records were reviewed to determine whether the patient had previously received anti-TB drugs. All laboratory processes were quality assured in cooperation with the Hong Kong Supranational Reference Laboratory.
In the national drug resistance survey, MDR TB cases were found to be 8.3 percent of all cases. Among new cases, 5.7 percent were MDR TB, and the MDR TB rate among retreatment cases was 25.6 percent. The proportion of XDR TB cases was 0.7 percent among all cases, 0.5 percent among new cases, and 2.1 percent among retreatment cases.
Of the 11 provinces where surveillance has been conducted to date, Inner Mongolia has shown the highest percentage of MDR TB cases, at 16.1 percent (see the figure below). Among new cases of TB, the resistance rate is 7.0 percent, while resistance is found in 36.8 percent of retreatment cases.
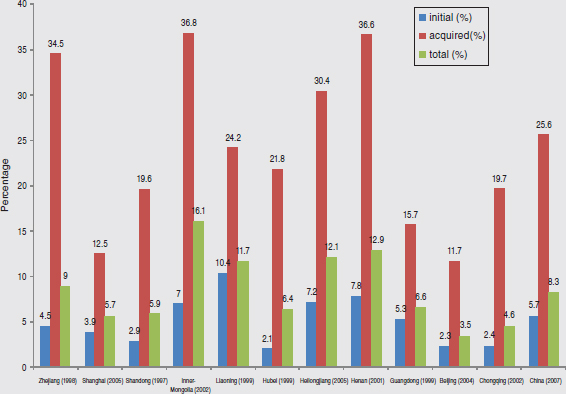
Percentages of MDR TB among initial (new) and retreatment (acquired) cases differ among 11 surveyed provinces and in comparison with China as a nation (last bar graph on right).
SOURCE: Li, 2010.
The proportion of resistance to isoniazid (19 percent) or streptomycin (28.9 percent) among all cases is higher than for other drugs. The proportions of resistance to streptomycin, ethambutol, ofloxacin, and kanamycin among MDR TB cases are 73 percent, 55 percent, 27 percent, and 12.5 percent, respectively. MDR and XDR TB prevalence is higher in rural and developing areas than in developed areas.
![]()
a The information presented this box is based on the work of Renzhong Li, Lixia Wang, Mingting Chen, Yanlin Zhao, Caihong Xu, and Cheng Chen of the National Center for Tuberculosis Control and Prevention, Center for Disease Control and Prevention, China.
- using a mathematical model to analyze the cost-effectiveness of programmatic management of drug-resistant TB over the next decade; and
- providing other forms of evidence on programmatic management of drug-resistant TB for policy makers.
In the areas of drug resistance surveillance and diagnosis, China is:
- updating the epidemiology of drug-resistant TB;
- conducting drug resistance surveillance in 13 provinces with support from WHO, in 6 provinces with support from the Global Fund, and in 1 province with support from local government;
- accelerating the implementation of rapid diagnostic methods; and
- assessing rapid diagnostic methods for MDR TB.
Finally, in the area of cooperation, China is determining effective models of cooperation between hospitals and TB dispensaries. The responsibilities of hospitals, according to Chen, include diagnosis, treatment, and response to side effects, whereas the responsibilities of public health institutes include management, supervision, follow-up, detection, and drug management.
The next step is to carry out the National Action Plan on Programmatic Management of Drug-Resistant TB in China. The pilot phase of 2007−2009 is currently undergoing preliminary scale-up, with rapid scale-up scheduled for 2013−2019 and full coverage for 2020 and beyond. During the rapid scale-up, all smear-positive TB cases will be tested using the Hain test. This plan will require regulation and legislation, an MDR TB expert committee at the central level, a high-quality and continuous supply of second-line anti-TB drugs, cooperation, and fund-raising mechanisms.
Already a single stream of funding from the Global Fund has been received, and 87 prefecture levels in 29 provinces will be covered. Actions expected in the future include expert review and demonstration, issuance of an action plan by the State Council of China, and integration of the action plan for MDR TB control with the National TB Control Plan for the next 10 years (Chen, 2010).
The Bill and Melinda Gates Foundation is supporting a project to develop new models, tools, and techniques for preventing and controlling MDR and XDR TB in China. Launched on April 1, 2009, the project covers four prefectures in four provinces in Phase I and will expand to 20 prefectures in six provinces in Phase II. Project activities include:
- determining a model and mechanism for cooperation between hospitals and public health institutes;
- developing policies, guidelines, and operational procedures for this cooperative program;
- determining the financing and incentives needed to implement the program;
- providing an uninterrupted supply of quality second-line TB drugs;
- implementing collaborative models;
- evaluating the model program; and
- developing human resources needed to implement and scale up the cooperative model.
The program is designed to provide a good model for the control and prevention of MDR TB, a standardized regimen for treatment, management of second-line drugs, laboratory methods for detection, the development of human resources, and a strong government commitment to the program goals. MDR TB treatment and management sites have been set up by prefecture, with plans for gradual and capacity-based expansion. Also, the TB dispensaries and other health services have been directed to cooperate closely.
Chen pointed out several lessons learned from both successful and unsuccessful experiences in the effort to fight drug-resistant TB in China. First, it is necessary to establish policies to regulate the management of MDR TB and the use of second-line drugs. Second, MDR TB control needs to be combined with broader changes in the medical system so the effort can draw on the resources of township health insurance plans, the new rural cooperative plans, the central government, and international cooperation. Third, depending on resources, an appropriate strategy for case finding is to give high-risk populations the highest priority and to screen all smear-positive patients for MDR TB. Fourth, the diagnosis of MDR TB cases can be accomplished more rapidly by using molecular biology methods. Finally, it is important to increase the number of TB staff at all levels and to enhance human resources through training.
HISTORICAL PERSPECTIVE ON MDR TB CONTROL EFFORTS4
Keshavjee explained that when New York City experienced an outbreak of drug-resistant TB in the late 1980s and early 1990s (see Box 2-3), it quickly became clear that these patients needed appropriate diagnostics, particular drug regimens, and a system of treatment follow-up in order to be cured. As a result, by the time the first global drug resistance surveys began in the mid-1990s, treatment regimens were well defined and relied on drugs that had been tested in the 1950s and 1960s. In Russia, too, the
![]()
4 This section is based on the presentation of Dr. Keshavjee.
BOX 2-3a
The New York City TB Epidemic
In 1991, Hamburg became health commissioner of New York City just as the city was experiencing an epidemic of resurgent TB. Nearly 4,000 cases were reported that year, representing a 152 percent increase over 1980. “This was sadly ironic,” said Hamburg, “because when I was in medical school I had learned about TB as a disease of historical interest only, not an ongoing scourge. I certainly never imagined that I would be spending so much of my time in New York City dealing with the problem of tuberculosis.”
Having had limited previous experience with TB, Hamburg was “stunned” to learn that this was not a new problem. TB rates had been increasing for years, particularly in inner-city areas and underserved communities. The problem was fueled by poverty, homelessness, AIDS and other diseases, and the erosion of the public health infrastructure. In addition, at that time New York City was experiencing an economic crisis, although not on the scale seen today. “Every year the TB program had been noting increases, raising signals of concern, but we had failed to act,” said Hamburg.
New York City quickly mobilized to mount a comprehensive response. Officials invested significant energy and resources in ensuring appropriate treatment. The implementation of DOTS increased the number of patients receiving directly observed therapy from 100 in 1988 to 1,300 in 1993. The city also increased screening, monitoring, and isolation capacity in hospitals, shelters, and other congregate facilities. Thanks to a well-designed program, adequate resources, and what Hamburg described as “real political will and program commitment from the mayor and others,” New York City was able to turn the epidemic around. Between 1992 and 1997, the number of TB cases in the city dropped by almost 46 percent, and for the most drug-resistant cases, by 86 percent. “Frankly, we were surprised by how quickly we were able to make that kind of difference,” said Hamburg. “It was a real accomplishment. I’m very proud of what we did and how the city responded overall to the epidemic. We were fortunate. We had resources. We had leadership. I think we showed what could be done.”
![]()
aThe information presented in this box is based on the presentation of Margaret Hamburg, commissioner, U.S. Food and Drug Administration.
treatment of drug-resistant TB during this period relied largely on previously developed approaches.
However, there was some reluctance on the part of WHO to apply the same approaches in less developed countries, said Keshavjee. In its publication Groups at Risk (WHO, 1996), WHO suggested that “MDR TB is too expensive to treat in poor countries; it detracts attention and resources from treating drug-susceptible disease.” As a result, poorer countries were urged to ignore the treatment of MDR TB with second-line anti-TB drugs and to focus on the DOTS strategy (using first-line short-course chemotherapy) as a means of enrolling large numbers of patients in TB treatment. According to Keshavjee, WHO’s position exemplifies a policy decision based on a discourse that did not fully reflect the available scientific data. In response to WHO’s stance, some groups took up the challenge of proving that MDR TB could be treated successfully in resource-limited settings.
In August 1996, Partners In Health and Harvard Medical School, with the Peruvian National TB Program, initiated a large-scale, community-based program to combat drug-resistant TB in the Northern Cone of Lima—the first program of its kind in any poor country. The challenge was substantial, Keshavjee noted, as their efforts were counter to the global discourse regarding the appropriate approach to treating drug-resistant TB in disadvantaged populations. Employing a treatment and transmission control strategy similar to that which had been used in New York City, the efforts in Peru were successful and achieved an 83 percent cure rate (PIH, 2010).
Based in part on the success in Peru, Partners In Health and other groups developed their own guidelines for the medical management of drug-resistant TB. Several philanthropists funded care for patients with MDR TB. In addition, a series of meetings starting in 1998 focused on the treatment of drug-resistant TB, leading to the development of DOTS-Plus, a supplemental approach to DOTS designed to cure MDR TB using second-line drugs. This was followed later by the formation of a coalition of partners that included the U.S. Centers for Disease Control and Prevention (CDC), the Task Force for Child Survival and Development, and WHO. In 2000, a coalition of nongovernmental, governmental, and multilateral partners created the GLC, with the objectives of ensuring access to quality-assured second-line drugs at affordable prices, monitoring and evaluating second-line drug use in approved projects, and promoting technical assistance for MDR TB projects to ensure that they would adhere to WHO guidelines.
Once the GLC was formed, several DOTS-Plus pilot projects—including those in Lima (Peru), Tomsk (Russia), Manila (Philippines), Latvia, and Estonia—joined and became models of care. Over the next few years, data from these projects informed what became guidelines for the programmatic
management of drug-resistant TB (WHO, 2006). Keshavjee noted that although there had been previous WHO guidelines, these new guidelines better reflected international standards of care.
A number of other treatment and funding initiatives also advanced the treatment of MDR TB. In 2002 the Global Fund Board decided that all MDR TB drugs funded by the Global Fund should go through the GLC mechanism to ensure the efficacy of the drugs. UNITAID was created in 2006 by France, Brazil, Norway, Britain, and other countries with the aim of lowering the market price and increasing the availability of drugs. Money became available from the U.S. Agency for International Development (USAID), the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), and the Lilly MDR TB Partnership to provide assistance to countries through the WHO and GLC systems. Combined with assistance from other partners, the result was a rapid increase in GLC projects in countries throughout the world. By 2009, roughly 60,000 patients were covered. Cure rates have averaged 62.8 percent, with a slight drop-off over time as the number of projects has increased.
REMAINING CHALLENGES5
Keshavjee stressed that, despite recent successes in mobilizing a number of international resources to fight MDR TB, significant challenges remain. As the urgency of treating the increasing number of MDR TB patients (diagnosed and undiagnosed) grows, the organizational and technical challenges involved in implementing the necessarily complex health interventions also grow. Challenges remain in the areas of infection control, diagnostics and laboratory infrastructure, second-line drug supplies, treatment delivery and health care infrastructure, and drug development. Failing to act on these challenges will have dire consequences, Keshavjee said.
Infection Control
Halting the person-to-person transmission of MDR TB is integral to any effective TB control program. Infection control measures are most commonly located in treatment facilities, which can be a nexus for the transmission of TB bacilli. A study from Tomsk, Siberia, showed that patients hospitalized for drug-susceptible TB had a sixfold greater risk of contracting MDR TB than those not hospitalized (Gelmanova et al., 2007). Part of the reason for this increased risk of infection is delays in diagnosis. Patients wait together for weeks in hospitals, many of which lack proper infection control, to learn whether they have MDR TB.
![]()
5 This section is based on the presentation of Dr. Keshavjee.
A number of interventions are possible even in resource-limited settings. In Lesotho, for example, infection control measures include respirators worn by staff and TB wards with negative pressure ventilation. The design of infection control measures can vary according to the unique needs and capabilities of the community. For instance, the climate in some parts of Africa lends itself to doors and corridors that open to the outside, whereas in Tomsk, the cold climate necessitates internal ventilation systems.
Diagnostics and Laboratory Infrastructure
In the area of diagnosis, rapid culture and drug sensitivity testing for MDR TB is desperately needed. In parts of many countries, people cannot access clinics easily. Once they reach a clinic, solid culture tests can take 4 to 8 weeks, liquid culture tests 2 to 4 weeks, and rapid molecular tests 2 hours to 2 days; many of these tests require proper laboratory infrastructure (see Chapter 5 for more information on current diagnostic methods). Returning for the test results and the initiation of treatment can be difficult for patients. If testing were available at the point of care, treatment could start right away, which in turn would reduce transmission to other patients.
Important steps have been taken in this area in the past 10 years. Laboratory facilities have been built in a number of resource-poor settings. In 2006, for example, Partners In Health worked with FIND to establish a state-of-the-art laboratory facility in Lesotho for approximately $500,000. In the span of about 6 months, Lesotho went from not having proper laboratory facilities to having solid media culture, then liquid media culture, and most recently DNA-based technologies. Today, Lesotho’s laboratory can diagnose a patient’s drug resistance profile in 2 days or less. This capability is especially important since the country has high levels of HIV, which increases the risk of contracting TB, the risk of having a drug-resistant form of TB, and the risk of experiencing excess morbidity and mortality (see Chapter 6). Thus, diagnosing patients quickly and initiating the appropriate regimen of TB drugs and HIV antiretrovirals is critical to optimal patient care.
The Global Laboratory Initiative (GLI), created by WHO and the STOP TB Partnership in 2007, draws extensively on the Lesotho model. It has received funding from UNITAID to implement this type of laboratory strategy in other countries, along with a supranational laboratory network to monitor new technologies. The goal is to be able to diagnose 130,000 people with these laboratories by 2013. This is an important step, said Keshavjee, but it will remain important to expand efforts to develop and rapidly deploy point-of-care testing for drug-susceptible and drug-resistant TB.
Responding to a question about the ideal diagnostic laboratory, Keshavjee said that the ideal test would use a sample from a patient’s
mouth, produce results very quickly, determine whether the patient has TB, and identify the drug resistance pattern of the strain. If such a test could take place within 1−2 hours, people could wait for their results and be started on the appropriate treatment immediately. Today, when results can take up to 2 months to be available (depending on the technology at hand in a given setting), many patients cannot even be found once their results are available. Peter Cegielski of CDC agreed that a rapid molecular screen for resistance would permit individualized treatment. In the meantime, he suggested, suspected MDR TB cases should be treated aggressively with empiric regimens until their drug susceptibility test results become known, after which treatment can be individualized.
Second-Line Drug Supplies
The situation with respect to second-line drugs for treating MDR TB is characterized by an inadequate number of manufacturers of these drugs, a limited supply of quality-assured drugs, and insufficient forecasting of need that contributes to opaque markets for drug manufacturing. Second-line drugs also have seen serious delivery delays for various reasons. Under the current global system, countries are required to use a central procurement mechanism housed at the STOP TB Partnership; while this mechanism has helped many countries, it does not work for all. For example, some countries use a tender process whereby they must take bids to purchase drugs, while others may want to use local manufacturers, which makes buying quality-assured drugs from outside the country difficult.
WHO has a prequalification program to identify quality anti-TB drugs. The number of prequalified suppliers increased from two in 2007 to eight in 2009. Also, the Global Drug Facility (GDF) established a Strategic Rotating Stockpile of second-line drugs for 5,800 patients, developed a forecasting tool, and formed a price negotiation task force. But Keshavjee noted that these efforts will not fully meet the needs of even a significant fraction of the estimated 500,000 new MDR TB patients each year. He suggested that new ways of thinking about the provision of drugs are needed, as are new drugs beyond those already in clinical development for TB treatment.
Treatment Delivery and Health Care Infrastructure
The STOP TB Partnership developed a plan to treat 1.6 million people between 2006 and 2015. But with 500,000 new patients a year, this strategy leaves many people to seek alternative types of care that are not effective and can worsen the drug resistance problem, according to Keshavjee. Even the goal of reaching 1.6 million people has not been achieved. Treating MDR TB requires not only that people take the necessary drugs but also
that they do so for 2 years. Meanwhile, side effects must be monitored; laboratory services must be provided; and systems must be in place to transfer samples, provide results, analyze and manage data, and use information effectively to improve patient care. Many countries lack the funds, the health system capability, and in some cases the political will to carry out such a complex health intervention.
The GLC has approved treatments for approximately 60,000 patients over the past decade, and GLC-approved projects have actually treated about 23,000. However, the latter number represents less than 0.5 percent of the 5,000,000 new MDR TB patients over that 10-year period. In a given year, the GLC treats less than 3 percent of the estimated 500,000 new patients; countries have reported to WHO that they are treating around 8 percent of cases themselves. Thus, more than 85 percent of MDR TB patients either are not receiving any treatment or are obtaining some treatment of unknown duration or quality.
Many people with drug-resistant TB live in isolated communities, and expecting them to come to clinics for care every day or twice a day for 2 years is unrealistic. An alternative is to train local health care workers to administer injections. Community-based approaches also provide a way to treat large numbers of patients rapidly and safely, said Keshavjee. For example, MDR TB cases in Tomsk were increasing between 1998 and 2004 but then declined as efforts were made to provide universal access to treatment. Curing the reservoir of transmitting patients is important to lowering the incidence of both drug-resistant and drug-susceptible TB, Keshavjee observed. Ambulatory care also can be much less expensive than hospitalization, although most physicians are trained to think in terms of the latter.
In May 2009, the World Health Assembly adopted a resolution urging all member states to achieve universal access to diagnosis and treatment of MDR and XDR TB as part of the transition to universal health care coverage. The resolution calls for directly observed treatment and community-based and patient-centered care. Effecting these changes will require long-term technical assistance and, where necessary, on-site implementation teams.
The global community has not yet begun to treat drug-resistant TB as an emergency, Keshavjee stated. For example, the number of people receiving treatment through PEPFAR programs increased from 155,000 in 2004 to 1.64 million in 2008; however, there has been much less growth in the treatment of MDR TB. Moreover, individual countries need to move beyond relying on international sources of funding and take the initiative in expanding treatment. Peru, for example, shifted from a heavy reliance on Partners In Health and the Global Fund for MDR TB treatment in 2001 to a major reliance on government resources by 2006.
If the ideal MDR TB treatment delivery plan could be instituted and
were not limited by resources or political will, Keshavjee suggested, such a program would diagnose people rapidly, start them on the appropriate treatment immediately, and ensure that they remained on treatment. “Even in settings where we can diagnose people and we do bring them the drugs, it’s very hard to keep them on [the treatment] for 2 years,” he said. Also, new second-line drugs are needed to improve cure rates (see the next section and Chapter 8).
Cegielski suggested that the greater limitation in TB control is the human capacity to identify, manage, treat, and follow patients. The people who perform those roles must be adequately trained and motivated, which means they must be able to earn a reasonable living at what they do. “With unlimited funding, I would dramatically expand both training and compensation for the health care workforce,” he said.
Finally, a participant stated that a key step in stopping the spread of MDR TB would be legislation forbidding free access to antibiotics without a prescription. In the former Soviet Union and China, essentially any drugs are available in drugstores. Cegielski observed that achieving the proper balance in antibiotic availability is difficult. Making antibiotics easily available has great benefits for people who suffer from infections other than TB. For example, he said he could not imagine restricting the fluoroquinolones to the treatment of TB because they are so widely useful for other infections. “There is not an easy solution,” he said. “It’s easy to say we need to control the second-line drugs, but we also have to look at the benefits that broad availability of antibiotics has had for populations.”
Drug Development
The development of a new “cocktail” of three to four drugs to treat MDR TB is a scientific, organizational, and technical challenge that is key to advancing the treatment of drug-resistant TB, said Keshavjee. Antibiotics that are more effective, less expensive, and able to shorten the course of MDR TB treatment are greatly needed. Cassell noted that it takes 10−14 years and $1 billion to create a new drug from discovery to regulatory approval. Unfortunately, she said, the total global investment in the development of new TB drugs—$179 million in 2009—is lacking by current standards.
Consequences of Inaction
The consequences of inaction on the above challenges are dire, said Keshavjee. Over the next 10 years, 5 million new cases of MDR TB will occur if current incidence rates persist. If current mortality rates continue, more than a million people will die. The large pool of living, untreated
patients will continue to infect others. People will continue to buy drugs from pharmacies or receive drugs from relatives and take them for short periods, which will increase drug resistance. Current plans to treat these patients have major gaps. Already, many countries are reporting increasing levels of XDR TB, and the number of TDR TB cases is completely unknown. Despite notable successes in recent decades, the global community has thus far been unable to significantly reduce the burden of MDR TB throughout the world. Keshavjee suggested that a major transformation is necessary to have a meaningful impact on this growing epidemic.
This page intentionally left blank.




















