
3
Opportunities and Challenges for Individuals Under the ACA
The ACA will directly impact individuals and their interactions with the health care system in many ways. In the context of the commissioned paper (described in Chapter 2 and available in Appendix C), panelists discussed the health literacy-related challenges and opportunities facing vulnerable populations in general, and children and the elderly in particular.
Cheryl Bettigole, M.D., M.P.H. Health Center #10, Philadelphia Department of Public Health
Vulnerable populations, as defined by Final Report of the President’s Advisory Commission on Consumer Protection and Quality in the Health Care Industry are groups of people “made vulnerable by their financial circumstances or place of residence; health, age, or functional or developmental status; or ability to communicate effectively . . . [and] personal characteristics, such as race, ethnicity and sex” (Advisory Commission on Consumer Protection and Quality in the Health Care Industry, 1998). The ACA presents both challenges and opportunities for vulnerable populations. Bettigole provided examples in each of the six health and health care domains outlined by Somers and Mahadevan.
Coverage Expansion
Bettigole gave three examples of patients from her practice, people who were eligible for insurance before the ACA was passed, but who encountered barriers as they tried to obtain that insurance: A Portuguese-speaking man applied for Medicaid after a devastating assault requiring surgery. He was given application materials in Spanish. He obtained coverage only because of the social worker who accompanied him to the office. A young mother failed to obtain coverage for her children because she could not read the Medicaid application; they went without care. An African-American woman in her 50s refused to apply for Medicaid because she was so humiliated by her treatment at the local Department of Public Welfare office. She too goes without care.
These scenarios illustrate just a few of the challenges that will need to be addressed as coverage expansion is implemented, Bettigole said. In many cases, the literacy level in materials is too high for many patients. While some states have set a literacy level of sixth grade or lower for materials, she noted that many of her patients do not read at that level, or do not read at all. There is inadequate access to translated materials and interpreters. Many patients do not have access to computers or do not have basic computer skills. The new requirements for proof of citizenship using original documents is also a barrier to enrollment for many people. Families of mixed immigration status often fear applying for Medicaid coverage. And lastly, attitudinal barriers and health literacy among frontline medical staff are also issues.
The ACA does present many opportunities to address some of these issues. For example, the literacy level of materials that are used in the exchanges can be regulated, and interpretation and translation requirements can be integrated as these materials are created. TV and radio can be used to reach low literacy populations and those without computer access. It is also important to engage groups already in the community that are trusted by vulnerable populations, to help bridge the divide.
With regard to Medicaid coverage expansion, Bettigole said that states should be allowed to relax the requirements for documented proof of citizenship. This would help facilitate other application methods like Internet and phone applications. Financial incentives for increasing enrollment of vulnerable populations are also needed. There is funding for community assistance programs and ombudsman programs in the exchange funding, and the availability of this assistance needs to be advertised on TV and radio, in multiple languages, so people know where to go for help when literacy and language requirements are not met.
Equity
Bettigole described a Haitian patient in her practice who has diabetes and high blood pressure. He misses his appointments at the clinic frequently, and often runs out of his medicines for months at a time. Earlier this year, he had a stroke. Because he was uninsured, he was not referred to rehabilitation (either inpatient or outpatient). Although he now has a walker, he has fallen repeatedly and his family is struggling to care for him at home. He and his family did not have the medical knowledge to ask about rehabilitation services and how to access them. They also did not have the knowledge or negotiating skills to realize that he should not have been sent home until he had learned to walk safely with his walker. Rehabilitation after a stroke is critical for regaining function. Ultimately, the clinic advocated for him and was able to have him readmitted for inpatient, and then outpatient rehabilitation.
This case demonstrates some of the challenges of obtaining equitable care. Patients from minority groups are often not offered the same treatment options as whites. Disparities in insurance status may explain part, but not all of the disparities in care and outcomes. In many cases, patients and families may not be comfortable challenging providers, even when they disagree or do not understand. Linguistic, cultural, and health literacy barriers compound the situation.
The non-discrimination provisions in the ACA provide protections for patients excluded from public or private coverage based on personal status. Bettigole also noted that the requirements for data collection on race, ethnicity, sex, primary language, and disability status will help facilitate assessments of progress in enrolling vulnerable populations. There is also a requirement for workforce training in culturally and linguistically appropriate care.
Workforce
Workforce development presents a variety of challenges. There is new money in the ACA for expansion of community health centers, which are expected to serve the majority of new Medicaid enrollees. But recruitment and retention of staff are major ongoing challenges for community health centers. In addition, there has been little attention to training in communication with low health literate patients, and in culturally and linguistically appropriate methods. Such training is not just for doctors, nurses, nurse practitioners, and other care providers; it is also necessary for the clerks who greet the patient and everyone else who interacts with patients along the care pathway.
Bettigole said that the expansion of the National Health Service Corp will help with recruitment of a larger workforce to community health
centers. There is funding for scholar programs and loan repayment, and for the first time people will be allowed to do loan repayment service part time (i.e., they can work in a community health center, and also do academic medicine or private practice at the same time). Another opportunity is that training grants in primary care will give preference to programs that provide training in communication, cultural competency, and health literacy. It would also be helpful to develop model health professions curricula that focus on patient-centered collaborative care that is culturally and linguistically appropriate and addresses health literacy issues.
Patient Information
A woman in her 50s was sent to Bettigole’s clinic for the first time after being in a local hospital for 4 weeks with what she said was “a bad cold.” She arrived at the clinic with a single sheet of “discharge instructions” that had only a scribbled list of medications. There was no diagnosis, and no information about her care over the month. A full review of her hospital records revealed she had been admitted for pneumonia complicated by congestive heart failure and diabetes. Her physicians in the hospital were certain they had communicated these diagnoses to the patient, as well as follow-up care instructions. But she did not have any recollection of this.
Such patient information challenges are a daily occurrence at a public clinic. The system has huge gaps that allowed this woman to fall through the cracks. Handoffs from one institution to another pose a particular problem for patients with low health literacy. Currently there are no standards for discharge procedures in place at many hospitals. For many of the patients that do receive some sort of information, the literacy level of the material is often too high for them to understand.
Accountable care organizations (ACOs) offer a significant opportunity to improve handoffs because they have financial incentives to decrease costs and improve quality. Electronic health records are an important piece of this process, but they are useful only if the system allows for sharing of the information between facilities. Financial incentives can also be used to increase the use of community health workers and liaisons who can take the time to sit with patients who are unable to understand written materials and explain what needs to be done.
Other opportunities include using standardized tools to assess a patient’s health literacy; teaching simple techniques such as “teach back” to healthcare workers to improve communication; and creating a clearing house for low health literacy materials screened to a very low (e.g., second or third grade) reading level, and even pictogram materials.
Public Health and Wellness
The ACA does expand coverage for preventive services, and funds expansions of community health interventions such as tobacco cessation and obesity prevention. This needs to be communicated clearly, in culturally and linguistically appropriate media, including not just print, but TV, radio, Internet, and social media as well. It will be especially important to collect data and assess the impact of these programs on the health of vulnerable populations.
Quality Improvement
Quality is particularly an issue for low health literacy populations with chronic conditions because they are at especially high risk for poorer outcomes. The accountable care organizations provide some incentives to improve quality of care for these populations, and Medicaid managed care plans offer opportunities to pilot interventions strategies for defined populations. Overall, improving communication has the greatest potential to improve quality of care for low literacy groups.
Summary
In conclusion, Bettigole said that systems for enrollment need to include multiple options for populations with low health literacy; there is no “one size fits all” solution. Funded community assistance and ombudsman programs should include the use of trusted community brokers who can help vulnerable populations understand insurance options and serve as advocates for those experiencing problems. Data collection and oversight will be critical to ensure that vulnerable populations enroll at rates equal to those of other communities. Financial incentives may be needed to ensure compliance with recommendations for culturally and linguistically appropriate care. Accountable care organizations need to be used as tools to improve patient-centered care, and teach back, or other standardized tools, should be required prior to discharge. There is an urgent need for widespread use of standardized discharge summaries to improve the quality of handoffs between inpatient and outpatient care. Success of these measures will depend on adequate training and commitment by the entire health care team, Bettigole said.
Lee Sanders, M.D., M.P.H. University of Miami Miller School of Medicine
Health literacy is strongly associated with health outcomes. Low health literacy is associated, for example, with worse general health status, increased hospitalization, depression, and worse control of chronic illness (Berkman et al., 2004). The association for children is complex as it relates to the health literacy not just of the child, but of the parents and adult caregivers.
Health patterns and behaviors that last throughout a lifetime begin to develop early on as mother and child establish their bond. The life course perspective on child health and health literacy acknowledges that there are many factors that influence a child’s health outcomes, including biology, environment, and the health system, as well as the family environment that is informed by the health literacy of the parents and other adult caregivers.
In four of the six broad themes outlined by Somers and Mahadevan there are child-specific charges that can be used to foster health literacy. Based on these, Sanders2 offered specific recommendations to help make the ACA work for children in low literacy families, developed out of his participation with workgroups of the American Academy of Pediatrics and the Academic Pediatric Association (summarized in Box 3-1).
Child Health Insurance
There are at least 9 million children in the United States who are uninsured. Of those, at least 5 million and perhaps as many as 6 million, are eligible for public services such as Medicaid or the State Children’s Health Insurance Program (CHIP) (Holahan et al., 2007). It is still not fully clear why many of them are not enrolled. Children of low literacy parents are at particularly high risk for being uninsured. They are also at risk for having decreased access to care, unmet health care needs, increased and more expensive usage as a result of increased ER visits, and decreased use of other preventive services. Many parents, not just low literacy parents, cannot complete insurance forms for child health insurance. Although Children’s Health Insurance Program (CHIP) forms are required to be written at the sixth grade reading level, a 2007 analysis
________________
1This presentation is based on a more extensive discussion of the topic which is presented in a paper in Appendix D.
2Further information and associated references are available in Appendix C
by Sanders showed that at least half of those forms were written above the tenth grade level (Figure 3-1).
There are a number of sections of the ACA (Sections 1413, 2715, and 3306) and the CHIP Reauthorization Act (CHIPRA) of 2009 that offer financial incentives to states for “eligibility simplification efforts.” Sanders recommended that efforts include enforcing grade-level standards for enrollment forms; outreach campaigns tailored to low literacy and limited English proficiency parents; bundling of eligibility assessments at the time of enrollment in other maternal and child health care programs; and eligibility assessment of all children at school entry and at school health clinics.
Quality Improvement
Up to 15 percent of all U.S. children have a chronic condition or a special health care need (e.g., asthma, obesity, diabetes); however they comprise more than 70 percent of national child health expenditures (Perrin, 2002). Children of low-literacy parents are at the greatest risk for low health care quality. The family-centered “medical home” presents an opportunity to moderate these disparities by providing coordinated, culturally effective, and comprehensive care. All of the principles of the medical home are rooted in principles of health literacy, Sanders said, making information more user-friendly and easier to understand. A recent study by Sanders suggests that family language and literacy (limited English proficiency, lower education, and lower literacy skills) are the
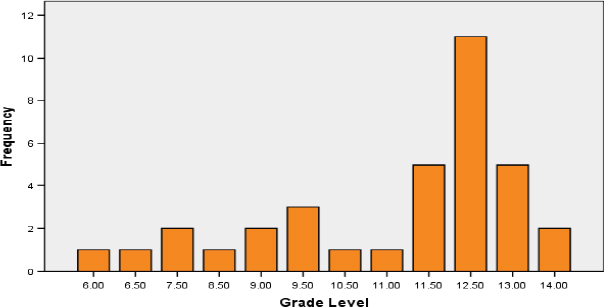
FIGURE 3-1 Readability of CHIP forms in all 50 states.
SOURCE: Sanders et al., 2007.
most modifiable social determinants of the quality of care coordination for a child.
The ACA supports quality improvement initiatives for child health, specifically: Sections 3501 and 3506 (Quality Improvement for Chronic Care), Section 4306 (Childhood Obesity Demonstration Projects), and Section 2951 (Early Childhood Home Visiting Programs).
Opportunities to improve family-centered care as outlined by Sanders include building literacy centers through the medical home; developing low literacy decision aids for children with special health care needs (including easy to use personal health records); and facilitating literacy and numeracy components of demonstration projections for preventing and managing childhood obesity (e.g., understanding food labels and portion sizes).
Child Medication Safety
There is a propensity for errors in dosing pediatric liquid medication by all parents and caregivers, but particularly among individuals with limited literacy and numeracy skills (Yin et al., 2007, 2008). Many over the counter medications do not include a dosing device, and for those that do, many have nonstandard markings on the device (Yin et al., 2010).
Section 3507 of the ACA calls for HHS to implement drug label standards, in consultation with evidence and expertise from the field of health literacy. Sanders said this provision provides the opportunity to standardize dosing instructions in both nonprescription and prescription medication, as well as to develop easy to understand dosing aids that can be used in pediatric care settings, as well as pharmacies.
The Pediatric Provider Workforce
Although the Accreditation Council for Graduate Medical Education (ACGME) competencies allude to health literacy, there are no specific requirements for it. A representative survey of all pediatricians in the United States showed that few pediatric providers use good health communication techniques, and pediatricians are asking for help in communicating across literacy barriers, not just language barriers (Turner et al., 2009). As a result, the American Academy of Pediatrics has developed an online set of training modules to teach providers about health literacy and health communication skills, including video vignettes (www.pedialink.org/cme/healthliteracy).
Sanders said that Section 5301 of the ACA can be used by HHS to make health literacy training a required component of post-graduate training, including a focus on child health and improving existing training modules.
BOX 3-1
Making the ACA Work for Children in Low-Literacy Families
To Extend Coverage to All Children:
Simplify the CHIP and Medicaid enrollment processes
- Enforce grade-level standards for paper- and web-based insurance enrollment forms
- Tailor CHIP outreach campaigns for low-literacy and limited English-proficiency parents
- Bundle eligibility assessment for all maternal and child health programs (e.g., WIC, SNAP, CHIP, Medicaid, school lunch programs)
- Assess eligibility for all maternal and child health programs at school entry and at school health clinics
To Improve the Quality of Child Health Care:
Tailor medical services for low-literacy parents of children, especially those with complex chronic illnesses
- Build health literacy through the medical home
- Literacy-sensitive models of family-centered care, particularly for children with chronic conditions (AHRQ’s Center for Quality Improvement, Section 3501; State-based Early Childhood Home Visiting Programs, Section 2951)
- Low-literacy measures of child-health quality (Center for Medicare and Medicaid Innovation)
- Develop low-literacy decision aids for children with special needs
- The CDC and NIH (Section 3506) should develop low-literacy decision aids for both children with special needs and their parents
- This should include easy-to-use personal health records
- Demonstration Projects for Childhood Obesity (Section 4306)
- Develop tools to simplify literacy- and numeracy-sensitive tasks (food labels, portion sizes)
To Improve Child Patient Safety:
Promote national standards for safe-use labeling of liquid pediatric medication
- Standardize dosing instructions on prescription and nonprescription liquid medication
- Develop easy-to-understand dosing aids for all pediatric liquid medication
To Improve the Skills of the Pediatric Workforce:
Require health literacy training
- Make health literacy training a required component of post-graduate training in child health (e.g., pediatrics, family medicine, pediatric nurse practitioners) (Section 5301)
- Improve and disseminate interactive health literacy training modules for pediatric providers
________________
SOURCE: Sanders, 2010.
SENIOR CITIZENS WITH HEALTH PROBLEMS
Harold Fallon, M.D. University of Alabama at Birmingham, School of Medicine
There are currently 40 million senior citizens in the United States and by 2020 the number is expected to reach 60 million. Fallon defined senior citizen as anyone who is on Medicare, and emphasized that there must be outreach to this sizable and growing population if we are to have a viable and healthy health care system.
Most seniors, regardless of level of education or literacy, do not understand the ACA, Fallon said. False information about what the provisions of the Act mean for seniors exacerbates fear, insecurity, and hostility, and impacts their use of the system. This is a significant and serious concern that must be addressed for all elderly, and especially those with limited health literacy.
There are generational issues to be aware of. For senior citizens, obedience to physicians’ instructions is quite commonplace. Many seniors have poor science and technical knowledge, and they can be gullible, not questioning what they read in the newspaper. Privacy is very important to seniors, and their dignity often inhibits their seeking help. There is also a disinclination to entitlements. Many of today’s seniors are children of the Depression, familiar with austerity and not inclined to waste money. Senior citizens also generally have an aversion to discussing disease, especially cancer, dementia, and mental illness. Poverty is an issue at any age, and compounds the many other issues seniors face.
A host of medical restrictions are more common in seniors than in younger adults, including dementias of all kinds; chronic pain, which can lead to a disinterest in life and a disinterest in seeking medical care; vision and hearing defects; and physical barriers to obtaining care.
There are the same cultural, racial, and ethnic subsets of seniors as there are for other generations. Hispanic and African American seniors have much greater difficulty entering into the healthcare system. Many of these older Americans lived through times when minorities did not have the benefits of an equal opportunity in education. Some are still not altogether adjusted to the freedoms that came during the Civil Rights era. This is something that people need to be sensitive to, Fallon noted.
What is needed, Fallon said, is a national campaign to address seniors. Every year, seniors receive a roughly 100-page document from Medicare that is an extreme challenge to navigate or understand, and Fallon suggested that many seniors simply discard it. Instead, the information needs to be brief. A succinct, one-page summary of the ACA and of Medicare is sufficient for most literate seniors, he said.
For seniors with low literacy levels, it is important to make use of all
of the available community resources. The ACA affords the opportunity to expand community resources to reach senior citizens and there are a large number of senior citizen centers, retirement facilities, nursing homes, and religious facilities that provide free medical care. Many senior citizens do not use the Internet for information, and evidence suggests that television is the best vehicle for delivering health care information to seniors. Fallon recommended simple, brief, one- to two-minute TV ads.
Point of service is also an opportunity to connect with seniors. Written material alone is not sufficient, and seniors generally need more direct intervention from physicians, pharmacists, and nurses, than younger adults do. During interactions, it is important to avoid lingo and talking too fast. Politeness and respect are also at the core of successful interactions with seniors.
The electronic health record programs in the ACA also offer opportunities to improve efficiency and coordination of care, as seniors often see many different providers (e.g., dermatologist, cardiologist, internist, orthopedist).
Community Engagement
Participants discussed further the need for more community engagement. Bettigole suggested holding meetings on a local level, and potentially asking HHS to attend those meetings and coordinate stakeholders. There are multiple community groups that would like to be heard on these issues, and to be seen as partners, and the potential for funding through the outreach and assistance programs will attract organizations as well. As an example of local, community-level involvement, Sanders mentioned the Human Services Coalition in Miami, which is involved in expanding child enrollment and would be an ideal recipient agency for funds to improve outreach efforts. There is also a CHIPRA demonstration project in Florida to improve the child medical home, involving 14 primary care sites. Community programs can play a role in educating at the state level, Fallon added. There are, for example, state governors that want to do away with Medicaid and CHIP. State legislatures need to hear articulate, well-thought-out, business-like presentations on the importance of these programs for their citizens.
Enrollment
A question was asked about evidence supporting a link between the readability of forms and actual enrollment rates of children in state CHIP.
Sanders responded that there are few specific data available. The Urban Institute released a report several years back that suggested a number of reasons for the gap between the eligible and enrolled children. The readability of forms may be as much a symptom as a cause; it represents the disconnection between the overall enrollment process and the people it serves. Sanders said that there should be a state-level position that is responsible for overseeing the improvement and simplification of the enrollment process. In the CHIPRA legislation there are renewed standards that need to be enforced.
The Business Case for Health Literacy
A question was asked about what would motivate accountable care organizations to address heath literacy. Bettigole responded that a significant driver of health care costs is hospital admissions. It is in the financial interest of an ACO to keep their patients out of hospitals, and if they do need hospitalization, to see to it that they do not need to be readmitted shortly after discharge. This is a key motivator for working on health literacy, but it will take some action on the part of literacy advocates to ensure that ACOs realize this, she said.
Bettigole also pointed out that undocumented immigrants are another vulnerable population who, by and large, will remain uninsured for the foreseeable future. This fact also supports the business case for health literacy as this is a sizable population, and a hospital should have every interest in helping them avoid being admitted and readmitted due to the potential for unreimbursed costs.
Re-engineering Discharge
A participant remarked that the examples shared by Bettigole illustrate how badly hospital discharge done this country. She mentioned a study that showed that activities such as patient education and support in the hospital, scheduling follow up appointments with primary care providers before the patient leaves the hospital, and follow-up phone calls after discharge, could reduce readmissions and emergency room visits by 30 percent. The discharge process needs to be re-engineered in association with health literacy efforts. Health literacy should not be viewed as an add-on or extra expense, but a way to change how care is organized and delivered.
Sanders agreed, and noted that from the pediatric health perspective there are some good business cases from Rochester and Wisconsin that show that implementing the medical home process as part of discharge for children with special health care needs produced significant savings.
This was not exclusively related to literacy dimensions of the discharge paperwork but to the whole discharge process.
Fallon drew attention to a recent Annals of Internal Medicine article on hospital recidivism in the Veterans Administration health system. The study found that patients with diabetes who were discharged from the hospital and had intensive nursing follow-up, did just as well as those who were part of a “buddy group,” a group of veterans who live in the same area and watch out for each other (somewhat similar to the Alcoholics Anonymous type of model). Fallon suggested that this is one low-cost way to help reduce hospital readmissions.
Roundtable Activities
A roundtable member asked Fallon for his advice on how to foster health literacy. Fallon responded that, in his opinion, what is needed is to integrate health literacy and improved communication into everything that a physician in the health care system does. The ACA, accountable care organizations, public health services, and others are all important individual pieces of the puzzle. The roundtable brings together various entities and provides the opportunity to explore ways in which integration can be achieved. Physicians need to be speaking the same language, aiming in the same direction, integrating health literacy concepts into everything they do. Sanders added that the Residency Review Committees should make literacy more prominent in graduate and continuing medical education.
This page intentionally left blank.













