
4
The Role of Physical Activity
Over the past several decades, as Americans have gotten heavier, they have also adopted an increasingly sedentary lifestyle, becoming less physically active and less physically fit (Centers for Disease Control and Prevention, 2010). These two trends are certainly related. The role of obesity was examined in the previous chapter, so it is natural to ask what role, if any, this decline in physical activity and fitness has played in the nation’s slower-than-expected growth in life expectancy over the past several decades.
EFFECTS OF PHYSICAL ACTIVITY ON HEALTH
There is nothing new about the observation that physical activity and exercise lead to a greater sense of health and well-being. Nearly two millennia ago, the Roman poet Juvenal wrote of the importance of mens sana in corpore sano, or a healthy mind in a healthy body, and the ancient Greeks and Romans were well aware of the importance of exercise in maintaining a healthy body. Despite this ancient wisdom, accurate quantification of the effect of physical activity or physical fitness on various health outcomes, including the risk of mortality, has yet to be determined. Not surprising, then, the extent to which differences in physical activity might contribute to variations in observed life expectancy across countries is poorly understood (Steptoe and Wikman, 2010).
Measurement Issues
Accurate measurement of the level of physical activity in a normal day-to-day environment is obviously fundamental to the study of the relation
ship between physical activity and mortality. A variety of techniques are available for assessing levels of physical activity, including use of self-reported data from diaries or recall questionnaires and objective measurement using pedometers, accelerometers, or other similar devices. Each method has advantages and drawbacks (Vanhees et al., 2005; Westerterp, 2009). Self-reported data are easier to obtain but are vulnerable to recall error, reporting bias (if respondents systematically tend to exaggerate or downplay their level of physical activity), and cross-national differences in interpretation of questions. The net result of such measurement errors is generally to weaken any effect that is present in the data; thus to the extent that these issues are a problem, the effects of physical activity are likely to be greater than estimated, rather than less.
Cross-national studies also need to take account of cross-cultural differences in customary forms of physical activity (Steptoe and Wikman, 2010). For example, bicycling, ice-skating, playing softball, lawn bowling, and playing boules are all activities whose popularity varies enormously across countries. Differences among countries in the physical demands of occupations, urban design, or the built environment can also generate differences in moderate or light activity that occurs as part of everyday life, which can easily be missed in surveys of leisure activities or purposeful exercise. Objective measurement of physical activity is more expensive but usually preferable as it can eliminate some of the problems associated with obtaining information from self-reports.
A variety of methods for obtaining objective measures are available. The most useful for population studies is the use of accelerometers (Westerterp, 2009). One of the most comprehensive measures of the level of physical activity among Americans was performed by Troiano and colleagues on more than 6,000 participants in the 2002–2003 National Health and Nutritional Examination Survey (NHANES). These subjects, who ranged in age from 6 to older adults, agreed to wear an accelerometer for at least an entire day and, for nearly 5,000 of them, 4 or more days. The accelerometer-derived data indicated that very few Americans engage in the recommended level of physical activity—at least 30 minutes of moderate or vigorous activity at least 5 days per week—and the percentage that do so decreases with age. Teenagers (aged 16–19) performed poorly, with only 7.1 percent of boys and 4.1 percent of girls getting the recommended minimum amount of exercise. But adults fared even worse: among those aged 20–59, just 3.8 percent of men and 3.2 percent of women performed enough exercise, and only 2.5 percent of older men and 2.3 percent of older women (Troiano et al., 2008).1
Observational Studies Linking Physical Activity and Health in Older Adults
Observational studies in older adults have found that physical activity is correlated with a number of measures of health, including increased strength and flexibility, increased aerobic capacity, improved balance and fewer falls, a reduced decline in bone density, improved glucose metabolism and insulin sensitivity, enhanced emotional well-being, and a reduced decline in cognitive function (Steptoe and Wikman, 2010). It should be noted, however, that drawing conclusions about the link between physical activity in older adults and health based on observational studies is somewhat hazardous because individuals can self-select into various states of physical activity. This selection is likely to be affected by their health. For example, people with chronic obstructive lung disease may be less likely to engage in vigorous activities. Both their high relative mortality risk and their low levels of exercise would likely be attributable to preexisting disease rather than to any effect of physical activity on mortality. It is also true that people with certain characteristics and behaviors (e.g., being poor and smoking) may be both less likely to exercise and more likely to be unhealthy. This section reviews the results from the large number of observational studies that have attempted to quantify the benefits of physical activity for older adults. The following section describes the far fewer studies that have used a randomized design to assign people to levels of activity.
Hamer and Chida (2008) performed a meta-analysis of 18 prospective studies that looked at the effects of walking on the risk of cardiovascular disease. The likelihood of developing cardiovascular disease was 31 percent lower among the group that walked the most compared with the group that walked the least. The benefits of walking were similar for men and women, and greater benefit came from walking briskly rather than from walking for longer periods of time. There was also some evidence of a dose–response relationship—that is, the more walking people did, the more it decreased their risk of developing cardiovascular disease.
In a subsequent review, the same authors examined the effects of physical activity on neurodegenerative diseases, such as dementia and Alzheimer’s disease (Hamer and Chida, 2009). Based on a meta-analysis of 16 prospective studies, they found that people in the highest physical activity category were 28 percent less likely to develop dementia and 45 percent less likely to develop Alzheimer’s disease than those in the lowest physical activity category. There is also good evidence that older adults who exercise are less likely to become depressed. Hamer and colleagues (2009) followed 4,300 older men and women (average age of 63) for 4 years. None reported symptoms of depression at the beginning of the study, while 8 percent did so 4 years later. The authors found that the people who reported engaging in regular, moderate physical activity were 29 percent less likely to develop
the symptoms of depression, while those who engaged in vigorous physical activity were 42 percent less likely.
A more recent study covered a longer period and focused on sedentary behavior. Among 7,800 men surveyed in 1982, time spent watching television and time spent riding in a car were significantly and positively related to mortality from cardiovascular disease over the next 21 years (Warren et al., 2010). The pattern of the association did not change materially after the introduction of covariates.
In short, there is considerable observational evidence that regular physical activity leads to improved health among older adults and, conversely, that a sedentary lifestyle with little physical activity is associated with an increased risk of developing a variety of physical, emotional, and mental problems.
Intervention Studies Linking Physical Activity and Health in Older Adults
Several investigators have conducted randomized intervention studies of the effect of physical activity on various measures of health among older adults. These studies are more difficult and expensive to perform than observational studies and thus typically have far fewer subjects, but the research design is clearly superior for assessing causal relationships. Not all validity problems will be solved with this approach, however, as persons who agree to participate in such trials are unlikely to be representative of the general population. Randomized controlled trials are inherently nonrepresentative, as those who are the best functioning, most motivated, and most capable of understanding and being enthusiastic about the trial are more likely to participate. However, by assigning subjects randomly to different groups, some of them exercising more and some less, these behavioral intervention studies avoid the issue of whether subjects who are more physically active might also have other characteristics—such as being in better health—that could explain the different outcomes seen.
In one randomized controlled trial, Martin and colleagues (2009) recruited 430 postmenopausal women and assigned each to one of four groups: no exercise and exercise at 50 percent, 100 percent, and 150 percent of the physical activity recommendation. After 6 months they measured the women’s physical and mental health, including physical functioning, body pain, social functioning, and sense of well-being or vitality. Consistently, in every category of physical and mental health, the women who were assigned to the exercise groups reported being healthier than those who were assigned to the no-exercise group, and the higher the level of exercise, the healthier they were.
A study in Australia looked at 170 adults aged 50 and older who were at risk of Alzheimer’s disease. Half were entered into a 24-week home-based
program of physical activity, while the other half were provided only with education and standard care. At the end of 6 months, the participants who had exercised showed improvements in cognitive functioning, while those in the other group had become worse. After the subjects in the physical activity group stopped exercising, most of the effect disappeared, implying that the benefits of physical activity lasted only as long as the activity was continued (Lautenschlager et al., 2008).
Another randomized controlled trial looked at the effect of exercise on depression, although this trial did not include older adults. Eighty adults aged 20–45 who had been diagnosed with major depressive disorder were assigned to perform different levels of aerobic exercise weekly. After 12 weeks, those in the higher-intensity group scored significantly lower on a depression scale than those in the lower-intensity group and those in the control group (Dunn et al., 2005).
Using a quasi-experimental design, MacDonald and colleagues (2010) studied the effect of introducing a light rail system in Charlotte, North Carolina, on a variety of health outcomes. After the system was introduced, those who used it significantly increased their physical activity levels relative to those who did not, with baseline characteristics being controlled for. The odds of obesity were significantly reduced among users of the system.
Mechanisms
Given the wide range of benefits of exercise for physical and mental health, it would appear likely that these benefits would be mediated through numerous physiological mechanisms. Indeed, the evidence does indicate that physical activity affects a number of bodily functions, from the cellular level on up. Steptoe and Wikman (2010) provide a list of such effects that have been identified in various studies. Regular physical activity has been linked to reduced blood pressure, improved lipid profiles, improved glucose metabolism, reduced levels of inflammatory markers, the induction of growth factors, and increased strength and flexibility. Ekelund and colleagues (2007) found that increases in energy expenditure as a result of greater physical activity are associated with reduced metabolic risk factors, independent of any change in fatness or fitness.
A good deal of research has been conducted on how exercise and training affect brain function, particularly in older adults (see National Research Council, 2000a). One recent study found that the medial temporal lobe tended to shrink with age among older adults who did little or no exercise but not among adults of the same age who engaged in high levels of exercise (Bugg and Head, 2009). Generally speaking, the best evidence of the benefits of exercise for brain function is the links between physical activity and the alleviation of depression, positive effects on learning and memory,
and protection from neurodegeneration. A basic mechanism underlying these effects is the exercise-induced production of growth factors, molecules that direct the brain to make various structural and functional changes (Cotman et al., 2007). Such findings suggest numerous possibilities for effective intervention to improve cognitive function in older people.
EFFECTS OF PHYSICAL ACTIVITY ON MORTALITY
Over the past several decades, numerous large cohort studies have attempted to quantify the protective effect of physical activity on cardiovascular and all-cause mortality. Nocon and colleagues (2008) reviewed 33 cohort studies with 883,372 participants that assessed the primary prevention impact of physical activity on all-cause and cardiovascular mortality. Follow-up ranged from 4 years to more than 20 years. The majority of studies reviewed reported significant risk reductions for physically active participants. Being in the most physically active subgroup was associated with a 35 percent increase in cardiovascular mortality and a 33 percent increase in all-cause mortality relative to the most active group. Studies that used patient questionnaires to assess physical activity generally reported lower risk reductions than studies that used objective measures.
While many studies have reported the positive effects of regular exercise, the dose–response relationship remains unclear. Consequently, several researchers have attempted to quantify the relationship between various levels of physical activity and mortality risk. Löllgen and colleagues (2009) report the results of a meta-analysis of 38 prospective cohort studies conducted between 1990 and 2006 to investigate the effect of various levels of intensity of physical activity on all-cause mortality. All-cause mortality was significantly lower for active compared with sedentary individuals. For studies with three levels of activity, highly active men had a 22 percent lower risk of all-cause mortality compared with mildly active men; highly active women had a 31 percent lower risk. Similar results were observed for moderately active compared with mildly active individuals.
A critical question with respect to the effect of physical activity on mortality is whether the incremental benefits of additional physical activity vary with the level of activity. Woodcock and colleagues (2011) conducted a systematic review and meta-analysis of the dose–response relationship between nonvigorous physical activity and all-cause mortality. They found that moderate activity reduced mortality risk by 24 percent compared with no activity.
Quantifying the effects of physical activity on mortality is complicated by the difficulty of determining physical activity over long periods of time. Is the current level of physical activity important, or is it the levels at early ages? Byberg and colleagues (2009) examined how changes in the level
of physical activity after middle age influence mortality. They followed a group of 2,200 men who were age 50 in 1970–1973, keeping track of their levels of physical activity over the years. The men who maintained a high level of physical activity over that time had a 32 percent lower chance of dying compared with the men who maintained a low level of physical activity. Furthermore, as shown in Figure 4-1, the study found that men who previously had a low level of physical activity and then increased their activity level had relatively lower mortality risks over time. They continued to have a high mortality rate for 5 years or so after increasing their physical activity, but after 10 years of this increased activity, their risk of dying was reduced to that of the men who had maintained a high level of physical activity all along (Byberg et al., 2009). It should be noted that while these results may reflect the effect of exercise patterns on mortality, reverse causation is also possible—that the results reflect instead the effect of health on physical activity.
Many of the studies that have looked at the relationship between physical activity and mortality have been forced to rely on self-reports of physical activity. Manini and colleagues (2006) measured energy expenditure directly using a technique known as doubly labeled water. The researchers measured the daily energy expenditure of 300 older adults (aged 70–82) and followed them for just over 6 years. They found that nearly a
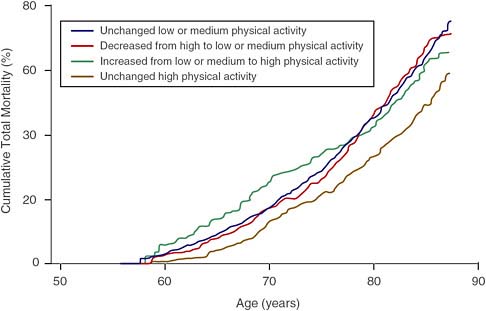
FIGURE 4-1 Association between physical activity level and mortality.
SOURCE: Byberg et al. (2009). Reprinted with permission.
quarter of the subjects with the lowest daily energy expenditure died during that period, compared with only an eighth of the subjects with the highest energy expenditure.
Another way to study the effects of physical activity is to focus on cardiorespiratory fitness instead, assuming that fitness is achieved through physical activity. Fitness should result from routine physical activity over a period of time. The Aerobics Center Longitudinal Study followed more than 80,000 patients between 1970 and 2005 to study the effects of fitness and other factors on health and mortality. More than 3,000 women and 10,000 men were given baseline treadmill tests between 1970 and 1981 to determine their cardiorespiratory fitness. Blair and colleagues (1989) compared mortality risks over a follow-up period averaging 8 years among groups of patients categorized as having low, moderate, or high fitness at baseline. Men with high levels of fitness at baseline were less than a third as likely to die during the study period than men with low levels of fitness, while women with high levels of fitness at baseline were less than a quarter as likely to die than women with low levels of fitness. Similar findings are reported in a subsequent study focused on older adults: across the age range, those with high levels of cardiorespiratory fitness were significantly less likely to die than those with moderate or low levels of fitness (see Figure 4-2) (Sui et al., 2007). As noted earlier, however, the observation that fitter people live longer is not indicative of a causal relationship between physical activity and mortality, since many causal pathways could produce such a correlation. One striking result from the Sui et al. (2007) study is that obesity did not affect mortality risk once fitness was taken into consideration. This result has led some researchers (Sui et al., 2007) to emphasize the role of fitness over fatness, but not all (Stevens et al., 2002). We return to this discussion in Chapter 10.
INTERNATIONAL COMPARISONS
Given the large body of evidence linking physical activity and fitness to better health and lower mortality risk, it is natural to ask whether the perceived low levels of fitness and physical activity in the United States relative to other countries have contributed in some way to the recent underperformance of U.S. life expectancy. Unfortunately, a significant gap exists in international physical activity surveillance, and cross-national comparisons of physical activity using comparable objective measures currently do not exist (Steptoe and Wikman, 2010). Nevertheless, survey instruments have been developed and validated for use in collecting internationally comparable self-reported data on physical activity (see, for example, Craig et al., 2003). These instruments make it possible to explore whether the popular perception that levels of physical activity in the United States are signifi-
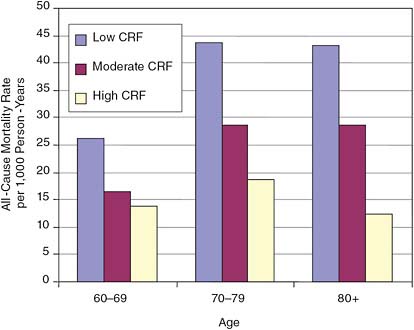
FIGURE 4-2 Cardiorespiratory fitness (CRF) and mortality from all causes for different age groups.
SOURCE: Adapted from Sui et al. (2007).
cantly lower than in other countries is accurate, particularly in relation to those countries where life expectancy has been increasing at a faster rate than in the United States.
Steptoe and Wikman (2010) review the available evidence on international differences in the prevalence of physical activity across countries from self-reported data. Four recent attempts have been made to compare levels of physical activity across countries (see Table 4-1). Each of these four studies used a slightly different survey instrument, adopted a slightly different criterion for assessing moderate or vigorous activity, and surveyed a slightly different target population. Consequently, the level of reported physical activity varies from one survey to another, and it is not possible to compare the levels of physical activity for a particular country across surveys for purposes of validation. Nevertheless, it is possible to compare the rank ordering of countries within the various surveys. Three points stand out almost immediately. First, the United States, which appears only in the International Prevalence Study on Physical Activity (IPS), does not appear to be atypical when it comes to the proportion of the population aged 40–65 that engages in moderate or intense physical activity (Bauman et al., 2009). Second, each of the surveys produces a slightly different rank
TABLE 4-1 Ranking of Levels of Moderate or Intense Physical Activity Across Countries
|
|
IPSa |
Eurobarometerb |
EPICc |
EU Studyd |
|
|
Moderate/Intense |
Sufficient Activity (IPAQ, %) |
Total Recreational Activity (hr/week) |
MET/hr/wk (median %) Activity % |
|
Country Ranking (High to Low) |
|
|
|
|
|
1 |
Czech R (88.0) |
Netherlands (44.2) |
Netherlands (19.38) |
Sweden (24.0) |
|
2 |
New Zealand (86.5) |
Germany (40.2) |
United Kingdom (14.34) |
Netherlands (21.0) |
|
3 |
Canada (83.0) |
Greece (37.0) |
Germany (13.17) |
Denmark (19.5) |
|
4 |
United States (82.5) |
Denmark (34.1) |
Spain (11.82) |
United Kingdom (16.0) |
|
5 |
Australia (81.5) |
Finland (32.5) |
Greece (11.08) |
Germany (12.7) |
|
6 |
Sweden (73.0) |
United Kingdom (38.7) |
Denmark (10.29) |
France (10.0) |
|
7 |
Norway (71) |
Ireland (29.0) |
Italy (8.35) |
Italy (8.0) |
|
8 |
Spain (70.5) |
Italy (25.8) |
Sweden (5.86) |
Spain (8.0) |
|
9 |
Belgium (51.5) |
Spain (25.2) |
Greece (8.0) |
|
|
10 |
|
Belgium (25.0) |
|
|
|
11 |
|
France (24.1) |
|
|
|
12 |
|
Sweden (22.9) |
|
|
|
NOTE: IPAQ = International Physical Activity Questionnaire; MET = metabolic equivalents. aInternational Prevalence Study on Physical Activity (Bauman et al., 2009), conducted 2002–2004; ages: 40–65; sample size = 2,746. bEurobarometer Study (Sjöström et al., 2006), conducted 2002; ages ≥15; sample size = approximately 15,000. cEuropean Prospective Investigation into Cancer and Nutrition (Haftenberger et al., 2002), conducted 1992–2000; ages: 50–64; sample size = 236,386. Data from the largest center in each country are included. dEuropean Union Study (Martínez-González et al., 2001), conducted 1997; ages: ≥15; sample size = 15,239. SOURCE: Adapted from Steptoe and Wikman (2010). |
||||
ordering of countries with respect to levels of moderate or intense physical activity, although there are some similarities across surveys. Denmark, one of the three countries identified in Chapter 1, along with the Netherlands and the United States, as having slightly lower growth in life expectancy relative to other high-income countries, appears to be particularly difficult to classify. The Eurobarometer Study, which used the International Physical Activity Questionnaire (IPAQ), found that Denmark had slightly lower levels of activity than Germany and Greece but significantly higher levels than Spain (Sjöström et al., 2006). The European Prospective Investigation into Cancer and Nutrition (EPIC) study found that older adults in Denmark reported lower levels of recreational activity than those in Germany, Spain, or Greece, while another European Union study found that adults in Denmark expended more metabolic equivalents (MET) than those in Germany, Spain, or Greece (Haftenberger et al., 2002; Martínez-González et al., 2001). Finally, the Netherlands consistently ranks high in international comparative studies of physical activity, a finding that reflects in part the relatively frequent use of bicycles in that country (Steptoe and Wikman, 2010).
In addition to the studies cited above, the Survey of Health, Ageing, and Retirement in Europe (SHARE), the Health and Retirement Study (HRS) in the United States, and the English Longitudinal Study of Ageing (ELSA) all employed a similar measure of physical activity in a large population sample of men and women aged 50 and above (Steptoe and Wikman, 2010). Participants were asked about the frequency with which they had participated in a variety of forms of vigorous, moderate, or light physical activity over the course of the past week. Figure 4-3 displays the proportion of respondents in each country who reported that they had engaged in vigorous or moderate activity at least once during the past week. Reassuringly, the SHARE/HRS/ELSA samples reported levels of vigorous or moderate activity quite similar in many cases to those in the first column of Table 4-1, which were derived using the IPAQ. One notable exception, however, is the United States. The level of physical activity reported in the HRS is significantly lower than that in the IPS sample, probably because the former was restricted to adults aged 50 and above, while the IPS survey was based on a sample aged 40–65.
Potentially as important as the percentage of the population that is engaged in vigorous or moderate physical activity is the percentage that is sedentary. As can be seen in Figure 4-4, about 22 percent of U.S. adults aged 50 and over reported engaging in no vigorous or moderate activity, which is higher than the percentage in all European countries in the figure except Poland. In both Denmark and the Netherlands—the two European countries that, along with the United States, had lower-than-expected increases in life expectancy—a relatively small percentage of the population, around 7 percent, was sedentary. Thus at this level of abstraction, there ap
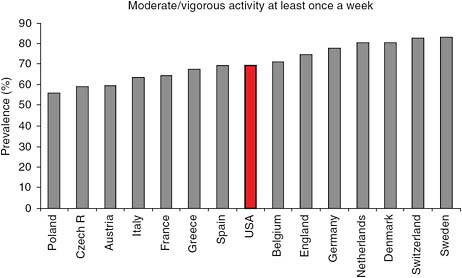
FIGURE 4-3 Physical inactivity in adults aged 50 and over in Europe and the United States.
NOTE: Data from the Survey of Health, Ageing, and Retirement in Europe (SHARE) (2006–2007), the English Longitudinal Study of Ageing (ELSA) (2004–2005), and HRS (2004).
SOURCE: Steptoe and Wikman (2010, Figure 7-3). Reprinted with permission.
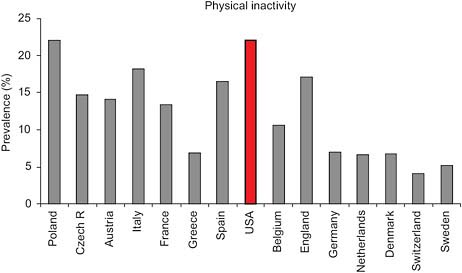
FIGURE 4-4 Proportion of adults aged 50 or older who report being moderately or vigorously physically active at least once per week.
NOTE: Data from the Survey of Health, Ageing, and Retirement in Europe (SHARE) (2006–2007), the English Longitudinal Study of Ageing (ELSA) (2004–2005), and the Health and Retirement Study (HRS) (2004).
SOURCE: Steptoe and Wikman (2010), Figure 7-2. Reproduced with permission.
pears to be little correlation between international levels of physical activity or inactivity and changes in life expectancy at older ages.
Steptoe and Wikman (2010) found that these measures of physical activity were significantly correlated with self-reported health for both men and women, while levels of inactivity were positively correlated with the prevalence of diabetes across countries. On the other hand, a regression analysis of the relationship between levels of physical activity and life expectancy at age 50 for men in various countries failed to find a significant relationship after controlling for one outlier. Furthermore, no statistically significant association was seen for women.
DISCUSSION
The bottom line is that at such a high level of aggregation and in the absence of suitable controls, it is not possible to demonstrate convincingly that international differences in levels of fitness or increased levels of physical activity are associated with international patterns of longevity. Given that the available data relate to levels of fitness and physical activity at only one point in time, it is impossible to assess the role played by fitness and physical activity in the divergent trends in life expectancy from 1980 to 2005. In contrast to the discussion of obesity in Chapter 3, the research base is not sufficient to identify a reasonable range of uncertainty in estimates of the contribution of physical activity to international differences in mortality. Physical activity may be an important determinant of mortality, significant in explaining cross-national differences and trends, but its role cannot be adequately evaluated with current data.













