
6
Papers on Research in
Preventing Violence Against
Women and Children
The science behind preventing violence against women and children has evolved greatly over the past several decades. Several speakers offered overviews of the research and described the growing awareness of the complexities of the causes, risk factors, and adverse effects of such violence. They also explored potential intervention points that were illuminated by this discussion.
The first paper is a reprint from the World Health Organization publication Preventing Intimate Partner and Sexual Violence Against Women (WHO and LSHTM, 2010b). The full report provides an overview of the magnitude of the issue; this workshop summary includes Chapter 3, which is an in-depth analysis of preventive interventions in low- and middle-income countries and was the basis for Claudia García-Moreno’s presentation at the workshop.
The second paper is adapted from the International Men and Gender Equality Survey (IMAGES), a multi-country study that explored men’s perspectives on gender norms and violence. The survey examined the evolving views of men on gender equality as well as whether these views affected men’s sense of well-being and their commitment to reducing violence.
The third paper, by Claire Crooks from the University of Western Ontario and the Centre for Addiction and Mental Health, provides an overview of the intergenerational transmission of violence. It also explores the ways in which violence against children can have long-term impacts as well as what considerations are valuable in designing interventions to prevent child maltreatment.
The final two papers, from Roger Fallot and Julian Ford, explore secondary and tertiary prevention of the long-term effects of violence and associated trauma by including the “trauma lens” in the provision of social services as well as through the empowerment of individuals who are exposed to violence. Trauma-informed care and psychosocial empowerment are two means by which survivors of violence can overcome potential adverse outcomes and prevent the recurrence of violence.
PREVENTING INTIMATE PARTNER AND SEXUAL VIOLENCE
AGAINST WOMEN: PRIMARY PREVENTION STRATEGIES1
Intimate partner and sexual violence are not inevitable—their levels vary over time and between places because of a variety of social, cultural, economic, and other factors. This can result in substantial differences between and within countries in the prevalence of intimate partner and sexual violence (WHO and LSHTM, 2010a). Most importantly, this variation shows that such violence can be reduced through well-designed and effective programs and policies. There are important factors related to both perpetration and victimization—such as exposure to child maltreatment, witnessing parental violence, attitudes that are accepting of violence, and the harmful use of alcohol—that can be addressed (WHO and LSHTM, 2010c).
At present, evidence on the effectiveness of primary prevention strategies for intimate partner and sexual violence is limited, with the overwhelming majority of data derived from high-income countries (HICs)—primarily the United States. Consequently, current high priorities in this field include adapting effective programs from high-income to lower-income settings; further evaluating and refining those for which evidence is emerging; and developing and testing strategies that appear to have potential, especially for use in low-resource settings, with rigorous evaluation of their effectiveness. At the same time, the dearth of evidence in all countries means that the generating of evidence and the incorporation of well-designed outcome evaluation procedures into primary prevention programs are top priorities everywhere. This will help to ensure that the efforts made in this area are founded upon a solid evidence base. Furthermore, program developers should be encouraged to explicitly base programs on existing theoretical frameworks and models of behavior change to allow underlying mechanisms to be identified and to make replication easier. Most of the evaluated strategies aimed at preventing intimate partner and sexual violence have
________________
1 Reprinted from World Health Organization and London School of Hygiene and Tropical Medicine. 2010. Preventing intimate partner and sexual violence against women: Taking action and generating evidence. Geneva, Switzerland: World Health Organization.
targeted proximal risk factors—primarily at the individual and relationship levels of the ecological model.
The Need for Upstream Action
In the public health framework, primary prevention means reducing the number of new instances of intimate partner and sexual violence by addressing the factors that make the first-time perpetration of such violence more likely to occur. Primary prevention therefore relies on identifying the “upstream” determinants and then taking action to address these. The impact of widespread, comprehensive programs can then be measured at the population level by comparing the rates at which such violence is either experienced or perpetrated. Given the lifetime prevalence of intimate partner and sexual violence, the hundreds of millions of women worldwide in need of services would outstrip the capacity of even the best-resourced countries (WHO and LSHTM, 2010a). A problem on this scale requires a major focus on primary prevention.
Upstream actions can target risk factors across all four levels of the ecological model. To decrease intimate partner and sexual violence at the population level, it is particularly important to address the societal or outer level of the model.
Such measures include national legislation and supportive policies aimed at social and economic factors—such as income levels, poverty and economic deprivation, patterns of male and female employment, and women’s access to health care, property, education, and political participation and representation. It is sometimes even argued that programs that aim to reduce intimate partner and sexual violence against women without increasing male–female equity will ultimately not succeed in reducing violence against women. However, while many strategies involving legal and educational reform and employment opportunities are being implemented to increase gender equality, few have been assessed for their impact on intimate partner and sexual violence, making the evaluation of such strategies a priority. Any comprehensive intimate partner and sexual violence prevention strategy must address these sociocultural and economic factors through legislative and policy changes and by implementing related programs.
Creating a Climate of Non-Tolerance
Addressing risk factors at the societal level may increase the likelihood of successful and sustainable reductions of intimate partner and sexual violence. For example, when the law allows husbands to physically discipline wives, implementing a program to prevent intimate partner violence may have little impact. National legislation and supportive policies should
therefore be put in place to ensure that women have equal rights to political participation, education, work, social security, and an adequate standard of living. They should also be able to enter freely into a marriage or to leave it, to obtain financial credit, and to own and administer property. Laws and policies that discriminate against women should be changed, and any new legislation and policies should be examined for their impact upon women and men. Legislation and policies that address wider socioeconomic inequalities are likely to reduce other forms of interpersonal violence, which will in turn help to reduce intimate partner and sexual violence.
Legislation and policies that address wider socioeconomic inequalities can make a vital contribution to empowering women and improving their status in society; to creating cultural shifts by changing the norms, attitudes, and beliefs that support intimate partner and sexual violence; and to creating a climate of non-tolerance for such violence.
The human rights of girls and women need to be respected, protected, and fulfilled as part of ensuring the well-being and rights of everyone in society. As a first step toward this, governments should honor their commitments in implementing the following international legislation and human rights instruments:
- Convention on the Elimination of All Forms of Discrimination Against Women (1979);
- The Convention on the Rights of the Child (1991);
- The Declaration on the Elimination of Violence Against Women (1993);
- The Beijing Declaration and Platform for Action (1995);
- The Millennium Declaration (2000); and
- The Inter-American Convention on the Prevention, Punishment and Eradication of Violence Against Women (Convention of Belem do Para, 1994).
Legislation and criminal justice systems must also be in place to deal with cases of intimate partner and sexual violence after the event. These systems should aim to help prevent further violence, facilitate recovery, and ensure access to justice—for example, through the provision of specialized police units, restraining orders, and multi-agency sexual assault response teams. Potentially, legal protection against intimate partner and sexual violence helps to reinforce non-violent social norms by sending the message that such acts will not be tolerated. Measures to criminalize abuse by intimate partners and to broaden the definition of rape have been instrumental in bringing these issues out into the open and dispelling the notion that such violence is a private family matter. In this regard, they have been very important in shifting social norms (Heise and García-Moreno, 2002; Jewkes et
al., 2002). However, the evidence surrounding the deterrent value of arrest in cases of intimate partner violence shows that it may be no more effective in reducing violence than other police responses, such as issuing warnings or citations, providing counseling, or separating couples (Fagan and Browne, 1994; Garner et al., 1995). Some studies have also shown increased abuse following arrest, particularly for unemployed men and those living in impoverished areas (Fagan and Browne, 1994; Garner et al., 1995). Protective orders can be useful, but enforcement is uneven, and there is evidence that they have little effect on men with serious criminal records (Heise and García-Moreno, 2002). In cases of rape, reforms related to the admissibility of evidence and removing the requirement for victims’ accounts to be corroborated have also been useful but are ignored in many courts throughout the world (Du Mont and Parnis, 2000; Jewkes et al., 2002).
Currently, on the whole, sufficient evidence of the deterrent effect of criminal justice system responses on intimate partner and sexual violence is still lacking (Dahlberg and Butchart, 2005). Dismantling hierarchical constructions of masculinity and femininity predicated on the control of women and eliminating the structural factors that support inequalities are likely to make a significant contribution to preventing intimate partner and sexual violence. However, these are long-term goals. Strategies aimed at achieving these long-term objectives should be complemented by measures with more immediate effects that are informed by the evidence base presented in this paper.
ASSESSING THE EVIDENCE FOR DIFFERENT
PREVENTION APPROACHES
From the perspective of public health, a fundamental question is, “Do intimate partner and sexual violence prevention programs work?” That is to say, are there certain programs or strategies that are effective in preventing or reducing intimate partner and sexual violence? Effectiveness can only be demonstrated using rigorous research designs, such as randomized controlled trials or quasi-experimental designs. These typically compare the outcomes of an experimental group (which receives the program) with a control or comparison group (which is as equivalent as possible to the experimental group but which does not receive the program). One major concern is to be able to rule out alternative explanations for any observed changes in outcome in order to be confident that the changes really were due to the program and not some other factor.
Although “testimonials” are not a sound basis for evaluating the effectiveness of a program, they can provide insights into its running and on whether participants find it worthwhile. However, approaches that are based upon testimonials might expend significant resources and capacity on
programs that may be ineffective or may even make things worse (Dahlberg and Butchart, 2005). Various criteria have now been proposed to more systematically evaluate the effectiveness of different programs. The most stringent criteria involve program evaluation using experimental or quasi-experimental designs; evidence of significant preventive effects; evidence of sustained effects; and the independent replication of outcomes.
In spite of the emphasis on and visibility of efforts to promote gender equality and prevent intimate partner and sexual violence, very few of the programs reviewed in this paper meet all of these criteria, while others have not been subjected to any kind of scientific evaluation. Rigorous scientific evaluation of programs for preventing intimate partner and sexual violence are even rarer in low- and middle-income countries (LMICs). The field of intimate partner and sexual violence prevention must therefore be considered to be at its earliest stages in terms of having an established evidence base for primary prevention strategies, programs, and policies. The limited evidence base for intimate partner and sexual violence prevention has three important implications for this paper.
First, the paper extrapolates, when relevant, from the stronger evidence base for child maltreatment and youth violence prevention but clearly signals that these extrapolations remain speculative. Much, however, can be learned from the literature on youth violence and child maltreatment prevention.
Second, the paper describes those primary prevention programs that have the potential to be effective either on the grounds of theory or knowledge of risk factors—even if there is currently little or no evidence to support them or where, in certain cases, they have not yet been widely implemented. In the process, an attempt is made to draw attention to the underlying theories, principles, and mechanisms on which the programs are based. However, it is noted that a firm theoretical base and consistency with identified risk factors do not guarantee the success of a program.
Third, the paper includes programs developed in LMIC settings on condition that they have some supporting evidence (even if it is weak) or are currently in the process of being evaluated, that they appear to have potential on theoretical grounds, or that they address known risk factors. The inclusion criteria are designed on the one hand to avoid setting the bar of methodological standards too high—which would lead to the exclusion of many of the programs developed in low-resource settings on the grounds that they have no or low-quality evidence supporting them. On the other hand, setting the bar too low would run the risk of appearing to endorse programs unsupported by evidence. However, the limitations of the evidence presented are clearly spelt out and the need for rigorous outcome evaluation studies emphasized.
Although still in its early stages, there are sound reasons to believe that this field is poised to expand rapidly in coming years. Some programs have been demonstrated to be effective following rigorous outcome evaluations, evidence is beginning to emerge to support the effectiveness of many more, and suggestions for potential strategies have proliferated. Furthermore, tried and tested methods for developing effective evidence-based primary prevention programs and policies for other forms of interpersonal violence have been reported. The field of evidence-based intimate partner and sexual violence prevention now requires an open mind to promising approaches and to innovative new ideas at all stages of the life cycle.
SUMMARY TABLES OF PRIMARY PREVENTION
STRATEGIES AND PROGRAMS
Table 6-1 summarizes the strength of evidence for the effectiveness of those strategies to prevent intimate partner violence and sexual violence for which some evidence is available. Strategies are grouped according to life stage. An important distinction must be drawn between a strategy and a specific program. Although specific programs may have been demonstrated to be effective, this in no way implies that all other programs categorized under the same strategy are also effective. For example, the Nurse Family Partnership, developed in the United States, is a home-visitation program that has been demonstrated to be effective in preventing child maltreatment. Nevertheless, it is the only program within the broader strategy of home visitation (which includes a multitude of different programs) that is supported by solid evidence of its effectiveness (MacMillan et al., 2009). The outcome measures of effectiveness are described in Box 6-1.
Strategies are ranked for their effectiveness in preventing intimate partner violence and sexual violence as follows:
- Effective: strategies that include one or more programs demonstrated to be effective. Effective refers to being supported by multiple well-designed studies showing prevention of perpetration and/or experience of intimate partner and/or sexual violence.
- Emerging evidence: strategies that include one or more programs for which evidence of effectiveness is emerging. Emerging evidence refers to being supported by one well-designed study showing prevention of perpetration and/or experience of intimate partner and/or sexual violence or studies showing positive changes in knowledge, attitudes, and beliefs related to intimate partner violence and/or sexual violence.
- Effectiveness unclear: strategies that include one or more programs of unclear effectiveness due to insufficient or mixed evidence.
- Emerging evidence of ineffectiveness: strategies that include one or more programs for which evidence of ineffectiveness is emerging. Emerging evidence refers to being supported by one well-designed study showing lack of prevention of perpetration and/or experience of intimate partner and/or sexual violence or studies showing an absence of changes in knowledge, attitudes, and beliefs related to intimate partner violence and/or sexual violence.
- Ineffective: strategies that include one or more programs shown to be ineffective. Ineffective refers to being supported by multiple well-designed studies showing lack of prevention of perpetration and/or experience of intimate partner and/or sexual violence.
- Probably harmful: strategies that include at least one well-designed study showing an increase in perpetration and/or experience of intimate partner and/or sexual violence or negative changes in knowledge, attitudes, and beliefs related to intimate partner and/or sexual violence.
As shown in Table 6-1, there is currently only one strategy for the prevention of intimate partner violence that can be classified “effective” at preventing actual violence. This is the use of school-based programs to prevent violence within dating relationships. However, only three such programs—described below—have been demonstrated to be effective, and these findings cannot be extrapolated to other school-based programs using a different approach, content, or intensity. At present, there are no correspondingly evaluated effective programs against sexual violence.
TABLE 6-1 Primary Prevention Strategies for Intimate Partner Violence and Sexual Violence for Which Some Evidence Is Available
| Strategy | Intimate Partner Violence | Sexual Violence |
| During Infancy, Childhood, and Early Adolescence | ||
|
Interventions for children and adolescents subjected to child maltreatment and/or exposed to intimate partner violence |
2 | 3 |
|
School-based training to help children recognize and avoid potentially sexually abusive situations |
3 | 2 |
| During Adolescence and Early Adulthood | ||
|
School-based programs to prevent dating violence |
1 | N/A |
|
Sexual violence prevention programs for school and college populations |
N/A | 3 |
| Strategy | Intimate Partner Violence | Sexual Violence |
|
Rape-awareness and knowledge programs for school and college populations |
N/A | 4 |
|
Education (as opposed to skills training) on self-defense strategies for school and college populations |
N/A | 5 |
|
Confrontational rape prevention programs |
N/A | 6 |
| During Adulthood | ||
|
Empowerment and participatory approaches for addressing gender inequality: Microfinance and gender-equality training |
2 | 3 |
|
Empowerment and participatory approaches for addressing gender inequality: Communication and relationship skills training (e.g., Stepping Stones) |
2 | 3 |
|
Home-visitation programs with an intimate partner violence component |
3 | 3 |
| All Life Stages | ||
|
Reduce access to and harmful use of alcohol |
2 | 3 |
|
Change social and cultural gender norms through the use of social norms theory |
3 | 2 |
|
Change social and cultural gender norms through media awareness campaigns |
2 | 3 |
|
Change social and cultural gender norms through working with men and boys |
2 | 3 |
1—Effective: strategies that include one or more programs demonstrated to be effective; effective refers to being supported by multiple well-designed studies showing prevention of perpetration and/or experiencing of intimate partner and/or sexual violence;
2—Emerging evidence of effectiveness: strategies that include one or more programs for which evidence of effectiveness is emerging; emerging evidence refers to being supported by one well-designed study showing prevention of perpetration and/or experiencing of intimate partner and/or sexual violence or studies showing positive changes in knowledge, attitudes, and beliefs related to intimate partner violence and/or sexual violence;
3—Effectiveness unclear: strategies that include one or more programs of unclear effectiveness due to insufficient or mixed evidence;
4—Emerging evidence of ineffectiveness: strategies that include one or more programs for which evidence of ineffectiveness is emerging; emerging evidence refers to being supported by one well-designed study showing lack of prevention of perpetration and/or experience of intimate partner and/or sexual violence or studies showing an absence of changes in knowledge, attitudes, and beliefs related to intimate partner violence and/or sexual violence;
5—Ineffective: strategies that include one or more programs shown to be ineffective; ineffective refers to being supported by multiple well-designed studies showing lack of prevention of perpetration and/or experiencing of intimate partner and/or sexual violence;
6—Probably harmful: strategies that include at least one well-designed study showing an increase in perpetration and/or experience of intimate partner and/or sexual violence or negative changes in knowledge, attitudes, and beliefs related to intimate partner and/or sexual violence; N/A—Not applicable.
BOX 6-1
Outcome Measures of Effectiveness
The effectiveness of a program can be evaluated in terms of three different types of outcome—each of which can be measured at different intervals after the program:
- Changes in knowledge, attitudes, and beliefs regarding intimate partner and sexual violence. This is the weakest of the three outcomes because changes in knowledge, attitudes, and beliefs do not necessarily lead to changes in violent behavior. In this respect, even successful programs in this area cannot be assumed to be effective at preventing actual intimate partner or sexual violence without further research demonstrating corresponding reductions in violent behavior.
- Reductions in the perpetration of intimate partner or sexual violence.
- Reductions in the experience of intimate partner or sexual violence.
Intimate partner violence is not a unitary construct and can take different forms, including physical, sexual, and psychological violence. Despite this, outcome evaluations generally do not examine effectiveness in relation to these different types of violence—nor are programs generally designed to address specific types of intimate partner violence in particular. It is possible that programs considered to be effective or promising may only be so for certain forms of intimate partner violence (Whitaker et al., 2007a).
Table 6-2 lists those strategies for which there is currently no evidence or very weak evidence but that appear to have potential on the grounds of theory, known risk factors, or outcome evaluations that are methodologically of lower quality; it also includes some promising strategies that are currently undergoing evaluation.
All the strategies reviewed have been organized according to the main life stages. When strategies are relevant to more than one life stage, they have been categorized under the stage at which they are most often delivered. Strategies relevant to all life stages are described last. Because of the way programs are organized, intimate partner violence is considered here to include instances of sexual violence that occur within an intimate partnership, while sexual violence is used here to refer to sexual violence occurring outside intimate partnerships (i.e., perpetrated by friends, acquaintances, or strangers). Dating violence can be considered to incorporate both possibilities because dating partners can range from being little more than acquaintances to more intimate partners. However, in Table 6-1 and Table 6-2 dating violence is classified for the sake of convenience under intimate partner violence.
TABLE 6-2 Primary Prevention Strategies for Intimate Partner Violence and Sexual Violence with Potential
| STRATEGY |
| During Infancy, Childhood, and Early Adolescence |
|
Home-visitation programs to prevent child maltreatment |
|
Parent education to prevent child maltreatment |
|
Parent education to prevent child maltreatment |
|
Improve maternal mental health |
|
Identify and treat conduct and emotional disorders |
|
School-based social and emotional skills development |
|
Bullying prevention programs |
| During Adolescence and Early Adulthood |
|
School-based multi-component violence prevention programs |
| During Adulthood |
|
U.S. Air Force multi-component program to prevent suicide |
During Infancy, Childhood, and Early Adolescence
Home-Visitation and Parent-Education Programs to Prevent Child Maltreatment
As noted in earlier sections of this document, a history of child maltreatment substantially increases the risk of an individual becoming either a perpetrator or victim of intimate partner violence and of sexual violence. It is therefore reasonable to assume that preventing child maltreatment has the potential to reduce subsequent intimate partner and sexual violence (Foshee et al., 2009). However, direct evidence of the effect of such programs on the levels of intimate partner violence is currently still lacking.
In general, however, reducing the risk of the different forms of child maltreatment reviewed in Preventing Child Maltreatment: A Guide to Taking Action and Generating Evidence (WHO and International Society for Prevention of Child Abuse and Neglect, 2006) can contribute to reducing the intergenerational transmission of violence and abuse. The most promising strategies for preventing child maltreatment in this area include home-visitation and parent-education programs (Mikton and Butchart, 2009). However, neither type of program has been evaluated for its long-term effects on the prevention of intimate partner and sexual violence among the grown-up children of parents who were involved in such programs.
Improve Maternal Mental Health
Maternal depression (which affects at least 1 in 10 new mothers) can interfere with good bonding and attachment processes. This in turn
increases the risk of persistent conduct disorders in children (a key risk factor for the later perpetration of violence) by as much as five-fold (Meltzer et al., 2003). Effective approaches for addressing maternal depression include early recognition (antenatally and postnatally) followed by peer and social support, psychological therapies, and antidepressant medication (National Collaborating Centre for Mental Health, 2007). The long-term effects on the children of mothers treated for maternal depression in terms of their later involvement in intimate partner and sexual violence have not been assessed, but the approach appears to have potential.
Identify and Treat Conduct and Emotional Disorders in Children
Conduct disorders in childhood and adolescence—a precursor of antisocial personality disorder—are associated with an increased risk of experiencing and/or perpetrating intimate partner and sexual violence. Additionally, emotional disorders are associated with later depression and anxiety in adult years and can increase the risk of postnatal depression and persistent maternal depression. As outlined above, these in turn contribute to as much as a five-fold increased risk of emotional or conduct disorders in the children of mothers with poor mental health (Meltzer et al., 2003). The early identification and effective treatment of conduct and emotional disorders in childhood and adolescence could therefore be expected to reduce the occurrence of subsequent intimate partner and sexual violence.
Good evidence exists of the links between early conduct disorder and later involvement in violence as both victim and perpetrator and of the effectiveness of interventions to reduce conduct disorder and youth offending. However, despite their potential, there is at present no evidence showing that the strategy of identifying and treating conduct and emotional disorders in childhood or early adolescence leads to reductions in intimate partner and sexual violence during later adolescence and adulthood.
Interventions for Children and Adolescents Subjected to Child Maltreatment and/or Exposed to Intimate Partner Violence
Because children or adolescents who have been subjected to child maltreatment or exposed to parental violence are at increased risk of becoming the perpetrators and victims of intimate partner and sexual violence, interventions in this area are particularly important.
One meta-analysis examined 21 programs involving psychological interventions targeted at children and adolescents who had experienced child maltreatment (Skowron and Reinemann, 2005). Results suggested that psychological treatments for child maltreatment yielded improvements among participants: Some 71 percent of treated children appeared to be functioning
better than their non-treated counterparts. All of the interventions were designed to improve cognitive, emotional, and behavioral outcomes, with 11 of the studies considered to be experimental. A randomized trial of one of these programs used adolescent dating violence as an outcome and found a reduction in the experiencing and perpetration of physical and emotional abuse (Wolfe et al., 2003).
Psychological interventions for children and adolescents subjected to child maltreatment and/or exposed to intimate partner violence therefore appear to represent a strategy for the prevention of intimate partner violence supported by emerging evidence. Their effect on sexual violence remains unclear at present.
School-Based Social and Emotional Skills Development
Factors such as impulsiveness, lack of empathy, and poor social competence—which may be indicative of conduct disorder, a precursor of antisocial personality disorder—are important individual risk factors for perpetrating various forms of violence, including intimate partner and sexual violence. Cognitive-behavioral skills training programs and social development programs that address these factors in children and young adolescents are therefore promising strategies for preventing subsequent violence. These programs seek to promote pro-social behavior and to provide social and emotional skills such as problem solving, anger management, increased capacity for empathy, perspective taking, and non-violent conflict resolution. They can either be population-based or targeted at those at high risk and are typically delivered in schools. Although there is strong evidence that such programs can be effective in reducing youth violence and improving social skills, there is currently no evidence that they can reduce sexual and dating violence among adolescents and young adults or intimate partner and sexual violence later in life (Lösel and Beelmann, 2003). Nonetheless, they appear to have potential in preventing subsequent intimate partner violence and sexual violence.
School-Based Training to Help Children to Recognize and Avoid Potentially Sexually Abusive Situations
School-based programs to prevent child sexual abuse by teaching children to recognize and avoid potentially sexually abusive situations are run in many parts of the world, but evaluated examples come mainly from the United States. A recent systematic review of reviews found that although school-based programs to prevent child sexual abuse are effective at strengthening knowledge and protective behaviors against this type of abuse, evidence showing whether such programs reduce its actual
occurrence is lacking (Mikton and Butchart, 2009). Two studies that measured future experience of sexual abuse as an outcome reported mixed results (Finkelhor et al., 1995; Gibson and Leitemberg, 2000). Nonetheless, emerging evidence of their effectiveness in preventing subsequent sexual abuse victimization appears to support the use of such programs. Further research on the long-term impact on actual sexual abuse victimization is, however, required (Finkelhor, 2009).
Bullying Prevention Programs
Bullying has both immediate and long-term consequences on perpetrators and victims, including social isolation and the exacerbation of antisocial behavior that can lead to juvenile and adult crime (for perpetrators) and depression, suicidal ideation, social isolation, and low self-esteem (for victims). Some of these consequences may increase the risk of later involvement in intimate partner and/or sexual violence either as perpetrator or victim. A number of reviews have concluded that bullying prevention programs are effective in reducing bullying (Smith et al., 2004; Baldry and Farrington, 2007). A systematic review and meta-analysis of school-based programs to reduce bullying and victimization showed that, overall, school-based bullying prevention programs are effective in reducing both bullying and being bullied (Farrington and Ttofi, 2009). On average, bullying perpetration decreased by 20 to 23 percent and the experiencing of being bullied decreased by 17 to 20 percent.
Although such programs are likely to have broader potential benefits, evidence of their effect on the experiencing or perpetrating of intimate partner and/or sexual violence later in life is limited. A number of studies, however, have demonstrated an association between bullying and sexual harassment. Some sexual violence prevention programs in the United States include bullying prevention components for elementary- and middle-school-age children (Basile et al., 2009).
During Adolescence and Early Adulthood
School-Based Programs to Prevent Dating Violence
Dating violence is an early form of partner violence, occurring primarily in adolescence and early adulthood, and experienced within a “dating relationship.” Dating violence prevention programs have been the most evaluated of all intimate partner violence prevention programs, with 12 evaluations of adolescent dating violence prevention programs, including 5 randomized trials (Foshee et al., 2008). Targeted at early sexual relationships, in contexts where marriage is usually entered into from about 20
years of age, these programs have been shown to prevent dating violence and sexual violence. Furthermore, dating violence appears to be a risk factor for intimate partner violence later in life and is also associated with injuries and health-compromising behaviors, such as unsafe sex, substance abuse, and suicide attempts (Smith et al., 2003; Wolfe et al., 2009). Accordingly, the prevention of dating violence can be assumed to be preventive of intimate partner and sexual violence in later life (Foshee et al., 2009).
One dating violence prevention program that has been well evaluated using a randomized controlled design is Safe Dates. Positive effects were noted in all four published evaluations (Foshee et al., 1998, 2000, 2004, 2005). Foshee et al. (2005) examined the effects of Safe Dates in preventing or reducing perpetration and victimization over time using four waves of follow-up data. The program significantly reduced psychological, moderate physical, and sexual dating violence perpetration at all four follow-up periods. The program also significantly reduced severe physical dating abuse perpetration over time, but only for adolescents who reported no or average prior involvement in severe physical perpetration at baseline. Program effects on the experiencing of sexual dating violence over time were marginal. Safe Dates did not prevent or reduce the experiencing of psychological dating abuse. Program effects were primarily due to changes in dating violence norms, gender role norms, and awareness of community services. The program did not affect conflict-management skills. The program was found to have had a greater impact upon primary prevention as opposed to preventing re-abuse among those with a history of previous abuse (Foshee et al., 1996, 1998, 2000, 2004, 2008).
Two school-based programs for preventing dating violence in Ontario, Canada, have also been evaluated (Wolfe et al., 2003, 2009). An outcome evaluation of The Fourth R: Skills for Youth Relationships used a cluster-randomized design and found that, based on self-reported perpetration at 2.5-year follow-up, rates of physical dating violence were 7.4 percent in the program group and 9.8 percent in the control group—a difference of 2.4 percent. However, for reasons not fully understood, this decrease of self-reported perpetration was found in boys (7.1 percent in controls versus 2.7 percent in intervention students) but not in girls (12.1 percent versus 11.9 percent). The program—evaluated by sampling more than 1,700 hundred students aged 14 to 15 years from 20 public schools—was integrated into the existing health and physical education curriculum and taught in sex-segregated classes. An underlying theme of healthy, nonviolent relationship skills was woven throughout the 21 lessons, which included extensive skills development using graduated practice with peers to develop positive strategies for dealing with pressures and the resolution of conflict without abuse or violence. The cost of training and materials averaged 16 Canadian dollars per student (Wolfe et al., 2009).
The other Canadian school-based program that has been evaluated is the Youth Relationship Project (Wolfe et al., 2003). This community-based program aimed to help 14- to 16-year-olds who had been maltreated as children to develop healthy non-abusive relationships with dating partners. The program educated participants on both healthy and abusive relationships and helped them to acquire conflict resolution and communication skills. A randomized controlled trial showed that the program had been effective in reducing incidents of physical and emotional abuse and the symptoms of emotional distress over a 16-month period after the program (Wolfe et al., 2003). These three school-based programs therefore appear to be effective for the prevention of physical, sexual, and emotional violence in dating relationships in adolescents and may also help to prevent intimate partner and sexual violence among adults. However, there are a number of necessary caveats concerning dating violence prevention programs. Although high-quality evaluations of the three programs described above found reduced violence at moderately long follow-up periods, the evaluations of most other programs have been of poor quality, used short follow-up periods, and only included knowledge and attitude changes as outcomes (for which some positive effects were found). Whether changes in knowledge and attitudes lead to corresponding changes in behavior is uncertain (Whitaker et al., 2006). Moreover, further research is needed to evaluate the effectiveness of dating violence prevention programs in the longer term, when integrated with programs for the prevention of other forms of violence, and when delivered outside North America and in resource-poor settings. A particular concern that has been raised about programs such as Safe Dates is the extent to which they are culture-bound to North America and hence may be of limited value in LMICs.
School-Based Multi-Component Violence Prevention Programs
Universal multi-component programs are the most effective school-based violence prevention programs (Dusenbury et al., 1997; Adi et al., 2007; Hahn et al., 2007). Such programs are delivered to all pupils and go beyond the normal components of curriculum-based teaching to include teacher training in the management of behavior, parenting education, and peer mediation. There can also be after-school activities and/or community involvement. One systematic review estimated that, on average, universal multi-component programs reduced violence by 15 percent in schools that delivered the programs compared to those that did not (Hahn et al., 2007).
School-based multi-component violence prevention programs have mostly focused upon bullying and youth violence as outcomes. Given that the risk factors for youth violence and intimate partner and sexual violence are to some extent shared, such programs would appear to have some
potential for preventing these latter forms of violence. However, there is currently no evidence of their effectiveness in these areas.
Sexual Violence Prevention Programs for School and College Populations
In the United States, the majority of programs for the primary prevention of sexual violence by strangers, acquaintances, and non-intimate dating partners have focused on college students—though they have also increasingly been delivered to high school and middle school pupils. In settings where few go into higher education this approach has obvious limitations. Developmentally, it makes sense to educate young people in appropriate and inappropriate sexual behavior at a time when their sexual identities are forming and their attitudes to romantic partners are beginning to take shape. However, once again there is a severe paucity of evidence to confirm the effectiveness or otherwise of such programs (Schewe, 2007).
Two recent systematic reviews in the United States have evaluated the effectiveness of specific primary prevention programs in this area. The first of these included college, high-school, and middle-school populations and found that programs usually included several components (most often the challenging of rape myths, information on acquaintance and date rape, statistics on rape, and risk reduction and protective prevention skills) (Morrison et al., 2004). Of the 50 studies reviewed, 7 (14 percent) showed exclusively positive effects on knowledge and attitudes, but none used the actual experiencing or perpetration of violence as outcomes; 40 (80 percent) reported mixed effects; and 3 (6 percent) indicated no effect. The studies also had a number of serious methodological limitations that led the reviewers to conclude that the effectiveness of such programs remains unclear. These limitations included the use of knowledge and attitude as the only outcome measures, studies of higher-quality design showing poorer results, and the positive effects of the programs being found to diminish over time.
The second systematic review examined 69 education programs for college students on sexual assault and found little evidence of the effectiveness of such programs in preventing such assaults or in increasing levels of rape empathy (the cognitive–emotional recognition of a rape victim’s trauma) or awareness (Anderson and Whiston, 2005). However, the programs evaluated were found to increase factual knowledge about rape and to beneficially change attitudes toward it. The acute shortage of studies that use behavior as outcomes led the authors to conclude that more research using such outcomes was needed before definitive conclusions could be reached. The effectiveness of such programs, on the basis of these two reviews, is currently unclear. It has been found that the provision of “factual” information as part of addressing rape myths appears to have no effect on attitudes to rape or on the levels of empathy for its victims (Schewe, 2007).
Evaluation studies indicate that rape awareness and knowledge programs based on imparting such information rarely work. Similarly, educating women on effective self-defense strategies without teaching them actual self-defense skills has been found to be of questionable value and may even be potentially harmful in some contexts (Schewe, 2007). Two evaluations of programs that focused on a discussion of self-defense strategies without teaching the corresponding skills found no reduction in sexual assault risk at follow-up (Breitenbecher and Gidycz, 1998; Breitenbecher and Scarce, 2001). Rape prevention programs that use a style of personal confrontation with participants actually appear to be harmful. One study evaluating such a program found that it resulted in greater tolerance among men of the justifiability of rape (Fisher, 1986).
A number of other approaches have been tried for which there is presently very limited evidence of effectiveness. Encouraging victim empathy has been associated with both improvements and worsening of attitudes toward sexual violence and the acceptance of rape myths (Schewe, 2007). Educating women on how to avoid high-risk situations (such as hitchhiking, abusing alcohol, or becoming involved with older men) has also led to mixed results, and it too has been associated with greater acceptance of rape myths. To avoid the encouragement of victim-blaming, it is crucial that such education is delivered to female-only audiences. There have also been mixed indications of the effectiveness of programs that emphasize the negative consequences of sexual violence to men and that try to persuade them to see such sex as less rewarding than consensual sex.
Finally, several programs for preventing sexual violence have been proposed that have as yet been neither widely implemented nor evaluated. These include providing universal rape prevention education and parent education in sexual violence prevention throughout schools and workplaces, educating teachers and coaches about sexual violence and its prevention, and changing organizational practices to include activities such as mandatory training in the prevention of violence against women.
During Adulthood
Empowerment and Participatory Approaches to Reduce Gender Inequality
Empowerment is an approach that helps individuals and communities to identify their own problems and to develop, through participatory methods, the resources, skills, and confidence needed to address them. This approach emphasizes the role of individuals and communities as agents of change and prioritizes community ownership and leadership of the entire process. Comprehensive programs deal with the community as a whole or
with multiple subgroups of the population, have several components, and are designed to effect social change by creating a supportive environment for changing individual and community attitudes and behavior. Such approaches often utilize a combination of participatory rapid needs assessment, education or training, public awareness campaigns, and community action (Lankester, 1992).
Two examples of empowerment approaches for preventing intimate partner violence are the use of microfinance with gender-equality training and the Stepping Stones training package.
A number of initiatives involving microfinance have now been established to increase the economic and social power of women. These initiatives provide small loans to mobilize income-generating projects that can alleviate poverty. Stand-alone credit and rural development programs such as Grameen Bank and the Bangladesh Rural Advancement Committee target women and appear to show some promise in reducing intimate partner violence. However, the evaluation of such programs needs to take into account reports of lenders exploiting disadvantaged borrowers with very high rates of interest, which can trap people in debt and contribute to further poverty, as well as reports of increases in intimate partner violence (Kabeer, 2001; Rhyne, 2001). Disagreements over the control of newly acquired assets and earnings combined with women’s changing attitudes toward traditional gender roles, improved social support, and greater confidence in defending themselves against male authority has sometimes led to marital conflicts and violence against women perpetrated by their partners (Schuler et al., 1996). Increases in violence following participation in credit programs have also been reported elsewhere, at least in the initial stages of membership (Rahman, 1999; Ahmed, 2005). Pre-existing gender roles appear to affect the violence-related outcomes of credit programs—in communities with rigid gender roles, women’s involvement can result in increased levels of intimate partner violence not seen in communities with more flexible gender roles (Koenig et al., 2003). The outcome evaluations conducted to date of such stand-alone microfinance programs have not been as rigorous as that of the Intervention with Microfinance for AIDS and Gender Equity (IMAGE) program described in Box 6-2.
Although microfinance programs can operate as discrete entities, IMAGE is an example of such a program that also incorporates education sessions and skills-building workshops to help change gender norms, improve communication in relationships, and empower women in other ways and has been shown to be effective at reducing intimate partner violence (Kim et al., 2009). Through education and skills building for women and engagement with boys and men and the broader community, IMAGE was effective in reducing intimate partner violence and supporting women. This was achieved without producing the type of negative effects seen in other
BOX 6-2
Intervention with Microfinance for AIDS
and Gender Equity (IMAGE)
One of the most rigorously evaluated and successful microfinance and women’s empowerment programs to date has been the Intervention with Microfinance for AIDS and Gender Equity (IMAGE) in South Africa. This program targets women living in the poorest households in rural areas, and combines a microfinance program with training and skills-building sessions on preventing HIV infection, and on gender norms, cultural beliefs, communication, and intimate partner violence.
The program also encourages wider community participation to engage men and boys. It aims to improve women’s employment opportunities, increase their influence in household decisions and their ability to resolve marital conflicts, strengthen their social networks, and reduce HIV transmission.
A randomized controlled trial found that two years after completing the program, participants reported experiencing 55 percent fewer acts of violence by their intimate partners in the previous 12 months than did members of a control group. In addition, participants were more likely to disagree with statements that condone physical and sexual violence toward an intimate partner (52 percent of participants versus 36 percent of the control group).
settings where cultural shifts and other changes have taken place in the absence of efforts to engage men.
The Stepping Stones training package is another participatory approach that promotes communication and relationship skills within communities. Training sessions are run in parallel for single-sex groups of women and men. Originally designed for the prevention of HIV infection, several communities have now incorporated elements of violence prevention. The approach has been used in 40 LMICs in Africa, Asia, Europe, and Latin America. Versions of the program have now been evaluated in a number of countries (Welbourn, 2009). The most thorough evaluation to date has been a randomized controlled trial in the Eastern Cape province of South Africa, with participants aged 15 to 26 years. This study indicated that a lower proportion of men who had participated in the program committed physical or sexual intimate partner violence in the two years following the program compared with men in a control group (Jewkes et al., 2008).
Furthermore, an evaluation in Gambia compared two villages where the program was carried out with two control villages and followed participating couples over one year. It found that, compared to couples not receiving the program, communication was improved and quarrelling reduced in participating couples. In addition, participating men were found
to be more accepting of a wife’s refusal to have sex and less likely to beat her (Paine et al., 2002).
SASA! is an “activist kit” for mobilizing communities to prevent violence against women, focusing in particular on the connection between HIV/AIDS and violence against women. “Sasa” is a Kiswahili word meaning “now,” and the kit includes practical resources; activities-monitoring and assessment tools to support local activism, media, and advocacy activities; and communication and training materials. It targets community norms and traditional gender roles and aims to change knowledge, attitudes, skills, and behavior to redress the power imbalance between men and women. It was created by Raising Voices, a Uganda-based nongovernmental organization that works in the Horn of Africa and Southern Africa. The London School of Hygiene and Tropical Medicine, Raising Voices, the Kampala-based Center for Domestic Violence Prevention, and Makerere University are currently conducting a joint randomized controlled trial to evaluate the effectiveness of the approach.
Thus evidence is emerging of the effectiveness in LMICs of empowerment and participatory approaches in preventing intimate partner violence through microfinance combined with gender-equality training and through the Stepping Stones training package.
The results of the SASA! evaluation are expected to provide further evidence on the effectiveness of this type of program, which seems to have potential for reducing intimate partner violence. There is a need to replicate and scale up this type of approach. Several other participatory and community-empowerment strategies to prevent intimate partner violence may be of value, although these have seldom been implemented as primary prevention strategies or rigorously evaluated. Couples counseling focuses on violence and/or substance abuse and may be effective for couples who have not resorted to intimate partner violence but who may be at risk. Family programs to promote positive communication and healthy relationships and prevent family violence might also be effective in preventing both intimate partner and sexual violence, given the importance of family factors in their development. In Ecuador one intimate partner violence prevention program that was implemented (but not evaluated) consisted of close friends or relatives being assigned to “monitor” newlyweds and to intervene should serious conflict arise. There is also some initial evidence that social cohesion among residents increases a community’s capacity to manage crime and violence (by increasing “collective efficacy”), leading to decreases in both lethal and non-lethal intimate partner violence. Such community-level interventions can beneficially change community-level characteristics and warrant further evaluation.
Home Visitation Programs to Prevent Intimate Partner Violence
A systematic review of home visitation programs (Bilukha et al., 2005) identified only one evaluation study (Eckenrode et al., 2000) that examined the effect of home visitation on levels of intimate partner violence. No significant difference in the incidence of such violence among the program and control groups was found.
A five-year project (2007-2012) funded by U.S. Centers for Disease Control and Prevention is currently under way, which will develop, test, and evaluate a program to reduce intimate partner violence among low-income women enrolled in the Nurse Family Partnership during pregnancy and in the first two years postpartum. The Nurse Family Partnership is a nurse home visitation program of demonstrated effectiveness in reducing child maltreatment. The primary aims are to develop a model for an in-home intimate partner violence prevention program for enrolled mothers at risk of such violence, to test the feasibility and acceptability of the program, and in a randomized controlled study to compare the effectiveness of the approach to that of the Nurse Family Partnership alone.
An evaluation of the Hawaii Healthy Start Program—an early childhood home visitation program—found that when compared with a control group, the participation of mothers was associated with reduced perpetration and experiencing of intimate partner violence. The effect persisted for the first three years of a child’s life, with small decreases in both the perpetration and experiencing of maternal intimate partner violence at follow-up when the child was seven and nine years old (Bair-Merritt et al., 2010). Evidence for the effectiveness of such programs can currently thus be considered to be unclear.
U.S. Air Force Multi-Component Program to Prevent Suicide
This program was primarily aimed at reducing the rate of suicide among U.S. Air Force (USAF) personnel but was also shown to reduce “family violence,” which included both intimate partner violence and child maltreatment. The program was based upon:
- the full involvement of the USAF leadership to ensure the program had the support of the entire service;
- incorporation of suicide prevention into professional military education;
- community education and training of military personnel to identify risk factors, provide appropriate intervention, and refer individuals who were potentially at risk of suicide; and
- the creation of a multidisciplinary team consisting of mental health providers, medical providers, and chaplains who could respond to traumatic events at the community level, including suicides.
The program reduced the rate of suicide by 33 percent and the rates of severe and moderate family violence by 54 percent and 30 percent, respectively. Because of the combination of intimate partner violence and child maltreatment in the same outcome measure, it is not possible to determine the effect of the program on intimate partner violence specifically (Knox et al., 2003); hence this program is considered to have potential, rather than being supported by emerging evidence.
All Life Stages
Reduce Access to and Harmful Use of Alcohol
Harmful use of alcohol is associated with the perpetration of intimate partner and sexual violence (WHO and LSHTM, 2010c). It can therefore be hypothesized that reducing both access to alcohol and its harmful use will lead to reductions in intimate partner and sexual violence. However, the relationship between harmful use of alcohol and violence is complex—not everyone who drinks is at equally increased risk of committing violence, and intimate partner and sexual violence can occur at high rates in cultures where alcohol use is taboo. Furthermore, there is disagreement among experts on whether or not alcohol can be considered to be a “cause” of intimate partner and sexual violence or whether it is better viewed as a moderating or contributory factor. It seems clear, however, that individual and societal beliefs that alcohol causes aggression can lead to violent behavior being expected when individuals are under the influence of alcohol and to alcohol being used to prepare for and excuse such violence. To date, research focusing on the prevention of alcohol-related intimate partner and sexual violence is scarce. There is, however, some emerging evidence suggesting that the following strategies aimed at reducing alcohol consumption may be effective in preventing intimate partner violence:
- Reducing alcohol availability: In Australia, a community intervention that included restricting the hours of sale of alcohol in one town reduced the number of domestic violence victims presenting to hospital (Douglas, 1998). In Greenland, a coupon-based alcohol rationing system implemented in the 1980s that entitled adults to alcohol equivalent to 72 beers per month saw a subsequent 58 percent reduction in the number of police call outs for domestic
quarrels (Finnish Foundation for Alcohol Studies and World Health Organization, 2003).
- Regulating alcohol prices: Increasing the price of alcohol is an effective means of reducing alcohol-related violence in general (Chaloupka et al., 2002). Although research evaluating the effectiveness of this approach in reducing intimate partner violence specifically is scarce, one study using economic modeling estimated that in the United States a 1 percent increase in the price of alcohol may decrease the probability of intimate partner violence toward women by about 5 percent (Markowitz, 2000).
- Treatment for alcohol-use disorders: In the United States, treatment for alcohol dependence among males significantly decreased husband-to-wife and wife-to-husband intimate partner violence 6 and 12 months later, suggesting that such treatment may also be an effective primary prevention measure (Stuart et al., 2003).
Intimate partner and sexual violence may also be reduced through primary prevention programs to reduce the more general harms caused by alcohol (Anderson et al., 2009). Approaches for which effectiveness is well supported by evidence include:
- Making alcohol less available: This can be achieved by introducing minimum purchase-age policies and reducing the density of alcohol retail outlets and the hours or days alcohol can be sold. Such an approach has been shown to lead to fewer alcohol-related problems, including homicide and assaults (Duailibi et al., 2007).
- Banning of alcohol advertising: Alcohol is marketed through increasingly sophisticated advertising in mainstream media; through the linking of alcohol brands to sports and cultural activities; through sponsorships and product placements; and through direct marketing via the Internet, podcasting, and mobile telephones. The strongest evidence for the link between alcohol advertising and consumption comes from longitudinal studies on the effects of various forms of alcohol marketing—including exposure to alcohol advertising in traditional media and promotion in the form of movie content and alcohol-branded merchandise—on the initiation of youth drinking and on riskier patterns of youth drinking (Anderson et al., 2009). However, evidence showing that such measures reduce intimate partner and sexual violence is currently lacking.
- Individually directed interventions to drinkers already at risk: These include screening and brief interventions. Alcohol screening and brief interventions in primary health care settings have
proven effective in reducing levels and intensity of consumption in LMICs and HICs (Finnish Foundation for Alcohol Studies and World Health Organization, 2003). However, their direct effect on alcohol-related intimate partner violence has not been measured. Evidence indicates that drinkers may reduce their consumption by as much as 20 percent following a brief intervention and that heavy drinkers who receive such an intervention are twice as likely to reduce their alcohol consumption as heavy drinkers who receive no intervention. Brief interventions include the opportune provision of advice and information in health or criminal justice settings (typically during a 5- to 10-minute period) but can also extend to several sessions of motivational interviewing or counseling (FPH, 2008; Sheehan, 2008).
School-based education on alcohol does not appear to reduce harm, but public-information and education programs (while again apparently ineffective at reducing alcohol-related harm) can increase the attention given to alcohol on public and political agendas (Anderson et al., 2009).
As with most primary prevention programs to prevent intimate partner and sexual violence, programs to reduce access to and harmful use of alcohol have mainly been conducted and evaluated in HICs, and little is known of their suitability or effectiveness outside such countries. For many LMICs, programs such as efforts to strengthen and expand the licensing of outlets could be of great value in reducing alcohol-related intimate partner and sexual violence. In many developing societies, a large proportion of alcohol production and sales currently takes place in unregulated informal markets. One study in São Paolo, Brazil, found that just 35 percent of alcohol outlets surveyed had a license of some form, and that alcohol vendors (whether licensed or not) faced few apparent restrictions on trading (Laranjeira and Hinkly, 2002). Furthermore, in many LMICs there are far fewer specialist health facilities, reducing the opportunities for alcohol treatment or screening. In such settings it may instead be beneficial to develop the role of primary health care workers or general practitioners in identifying and alleviating the harmful use of alcohol.
Although evidence for the effectiveness of measures to reduce access to and harmful use of alcohol is only beginning to emerge and high-quality studies showing their impact on intimate partner and sexual violence are still largely lacking, alcohol-related programs for the prevention of intimate partner violence and sexual violence appear promising. The strong association between alcohol and intimate partner and sexual violence suggests that primary prevention interventions to reduce the harm caused by alcohol could potentially be effective. Approaches to preventing alcohol-related intimate partner and sexual violence should also address the social acceptability of
excessive drinking as a mitigating factor in violence, while altering normative beliefs about masculinity and heavy drinking. There remains a pressing need for additional research to evaluate the effectiveness of such approaches in reducing intimate partner and sexual violence, especially in LMICs.
Change Social and Cultural Norms Related to Gender That Support Intimate Partner and Sexual Violence
Cultural and social gender norms are the rules or “expectations of behavior” that regulate the roles and relationships of men and women within a specific cultural or social group. Often unspoken, these norms define what is considered appropriate behavior, govern what is and is not acceptable, and shape the interactions between men and women. Individuals are discouraged from violating these norms through the threat of social disapproval or punishment or because of feelings of guilt and shame in contravening internalized norms of conduct. Often traditional social and cultural gender norms make women vulnerable to violence from intimate partners, place women and girls at increased risk of sexual violence, and condone or support the acceptability of violence (Box 6-3).
Efforts to change social norms that support intimate partner and sexual violence are therefore a key element in the primary prevention of these
BOX 6-3
Examples of Social and Cultural Norms That
Support Violence Against Women
- A man has a right to assert power over a woman and is considered socially superior. Examples: India (Mitra and Singh, 2007), Nigeria (Ilika, 2005), and Ghana (Amoakohene, 2004).
- A man has a right to physically discipline a woman for “incorrect” behavior. Examples: India (Go et al., 2003), Nigeria (Adegoke and Oladeji, 2008), and China (Liu and Chan, 1999).
- Physical violence is an acceptable way to resolve conflict in a relationship. Example: United States (Champion and Durant, 2001).
- Intimate partner violence is a “taboo” subject. Example: South Africa (Fox et al., 2007).
- Divorce is shameful. Example: Pakistan (Hussain and Khan, 2008).
- Sex is a man’s right in marriage. Example: Pakistan (Hussain and Khan, 2008).
- Sexual activity (including rape) is a marker of masculinity. Example: South Africa (Petersen et al., 2005).
- Girls are responsible for controlling a man’s sexual urges. Example: South Africa (Ilika, 2005; Petersen et al., 2005).
forms of violence. Approaches have been adopted, although rarely evaluated, throughout the world to break the silence that often surrounds intimate partner and sexual violence, to try to inform and influence social attitudes and social norms on the acceptability of violence, and to build political will to address the problem. The use of research findings for advocacy has been shown to be promising in bringing attention to, and raising awareness of, the problem and in contributing to the shaping of reforms and policies (Ellsberg et al., 1997). Currently the three main approaches for changing social and cultural norms that support intimate partner and sexual violence are social norms theory (i.e., correcting misperceptions that the use of such violence is a highly prevalent normative behavior among peers), media awareness campaigns, and working with men and boys. Often several approaches are used in one program.
Social norms theory assumes that people have mistaken perceptions of other people’s attitudes and behaviors. The prevalence of risk behaviors (such as heavy alcohol use or tolerance of violent behavior) is usually overestimated, while protective behaviors are normally underestimated. This affects individual behavior in two ways: (1) by increasing and justifying risk behaviors, and (2) by increasing the likelihood of an individual remaining silent about any discomfort caused by risky behaviors (thereby reinforcing social tolerance). The social norms approach seeks to rectify these misperceptions by generating a more realistic understanding of actual behavioral norms, thereby reducing risky behavior.
In the United States, the social norms approach has been applied to the problem of sexual violence among college students. Among such students, men appeared to underestimate both the importance most men and women place on sexual consent and the willingness of most men to intervene against sexual assault (Fabiano et al., 2003). Although the evidence is limited, some positive results have been reported. In one university in the United States, the A Man Respects a Woman project aimed to reduce the sexual assault of women, increase accurate perceptions of non-coercive sexual behavior norms, and reduce self-reported coercive behaviors by men. The project used a social norms marketing campaign targeting men, a theater presentation addressing socialization issues, and male peer-to-peer education. Evaluation of the campaign two years after its implementation found that men had more accurate perceptions of other men’s behavior and improved attitudes and beliefs regarding sexual abuse. For example, a decreased percentage of men believed that the average male student has sex when his partner is intoxicated; will not stop sexual activity when asked to if he is already sexually aroused; and, when wanting to touch someone sexually, tries and sees how they react. However, the percentage of men indicating that they have sex when their partner is intoxicated increased (Bruce, 2002).
Media awareness campaigns are a common approach to the primary prevention of intimate partner and sexual violence. Campaign goals might include raising public awareness (for example, about the extent of the problem, about intimate partner violence, and sexual violence as violations of women’s human rights and about men’s role in ending violence against women); providing accurate information; dispelling myths and stereotypes about intimate partner violence and sexual violence; and changing public opinion. Such campaigns have the potential to reach large numbers of people. An example of a media-awareness campaign is Soul City in South Africa. This multimedia health promotion and change project examines a variety of health and development issues, imparts information and aims to change social norms, attitudes, and practice. It is directed at individuals, communities, and the socio-political environment. One of its components aims to change the attitudes and norms that support intimate partner and sexual violence. This multi-level intervention was launched over six months and consisted of a series of television and radio broadcasts, print materials, and a helpline. In partnership with a national coalition on preventing intimate partner violence, an advocacy campaign was also directed at the national government with the aim of achieving implementation of the Domestic Violence Act of 1998. The strategy aimed for impact at multiple levels from individual knowledge, attitudes, self-efficacy, and behavior to community dialogue, shifting social norms, and the creating of an enabling legal and social environment for change. An independent evaluation of the program included national surveys before and after the intervention, focus groups, and in-depth interviews with target audience members and stakeholders at various levels. It found that the program had facilitated implementation of the Domestic Violence Act of 1998, had positively impacted on problematic social norms and beliefs (such as that intimate partner violence is a private matter), and had improved levels of knowledge of where to seek help. Attempts were also made to measure its impact on violent behavior, but there were insufficient data to determine this accurately (Usdin et al., 2005).
As the Soul City project indicates, evidence is emerging that media campaigns combined with other educational opportunities can change knowledge, attitudes, and beliefs related to intimate partner and sexual violence. Although good campaigns can increase knowledge and awareness, influence perceptions and attitudes, and foster political will for action, evidence of their effectiveness in changing behavior remains insufficient (Whitaker et al., 2007a).
Working with men and boys—There has been an increasing tendency to focus efforts to change social and cultural norms on adolescent males or younger boys using universal or targeted programs that are delivered
through a variety of mechanisms, including school-based initiatives, community mobilization, and public awareness campaigns.
Objectives typically include increasing an individual’s knowledge, changing attitudes toward gender norms and violence, and changing social norms around masculinity, power, gender, and violence. Some programs also aim to develop the capacity and confidence of boys and young men to speak up and intervene against violence, with the goal of changing the social climate in which it occurs (Katz, 2006). Failure to engage men and boys in prevention may result in the type of negative effects seen in some settings where cultural shifts and other changes have taken place in the absence of efforts to engage them (Box 6-4).
BOX 6-4
Nicaraguan Backlash Shows the Need to Engage Men as Well
Since 2000, Nicaragua has pioneered a number of initiatives to protect women against domestic violence. These have included:
- a network of police stations for women (Comisaria de la Mujer) where women who have been abused can receive psychological, social, and legal support;
- a ministry for family affairs (Mi Familia), which among other responsibilities ensures that shelter is available to women and children who suffer domestic violence; and
- reform of the national reproductive health program to address gender and sexual abuse.
During the same period, civil society groups have campaigned to promote the rights of women and to empower them to oppose domestic abuse. Because of these efforts, the reported frequency of intimate partner violence and sexual violence against women has increased dramatically. The more advocacy and awareness, the more likely women will report violence against them. For example, the number of reported cases of sexual violence received by the Comisaria de la Mujer rose from 4,174 (January to June 2003) to 8,376 (January to June 2004).
Researchers at the Universidad Centro Americana and the Institute for Gender Studies say a number of factors explain this increase—growing awareness among women that the cultural traditions that foster violence are no longer acceptable under international law and the Nicaraguan Domestic Violence Law, and better reporting of cases as women are encouraged to speak out. However, as Nicaraguan women have more actively opposed male hegemony, domestic conflicts have also increased and more men have resorted to intimate partner violence. These findings suggest that responses to intimate partner violence must not focus exclusively on women, but must also target men to prevent this type of backlash (Schopper et al., 2006).
A review of programs that work with men and boys to prevent violence against women (Barker et al., 2007) included 13 primary prevention programs, 5 of which were implemented in LMICs. Four of these programs were judged by the reviewers to be “effective,” six “promising,” and three “unclear.” For example, one community outreach and mobilization campaign in Nicaragua judged to be effective was called Violence Against Women: A Disaster We Can Prevent as Men (Solórzano et al., 2000). This was aimed at men aged 20-39 years who were affected by Hurricane Mitch. The campaign’s main messages addressed men’s ability and responsibility to help prevent or reduce violence against their partners. Constructing masculinity without intimate partner violence was a group-education program aimed at men in periurban districts of Managua, Nicaragua (Welsh, 1997). The effect of the program was, however, unclear because of the weakness of the outcome evaluation.
Indeed, the methodological quality of most of the outcome evaluations was very low, and outcome measures consisted mainly of attitude changes and self-reported rates of gender-based violence, often using only small sample sizes. One campaign in New South Wales in Australia—Violence Against Women: It’s Against All the Rules—targeted 21- to 29-year-old men and aimed to influence their attitudes. Sports celebrities delivered the message that violence toward women is unacceptable and that a masculine man is not a violent man. It also sought to enhance the community’s capacity to challenge and address violence against women. A post-campaign survey indicated that the campaign achieved some positive results: 83 percent of the respondents reported that the message of the campaign was that violence against women is “not on,” and 59 percent of respondents could recall the campaign slogan. However, 91 percent of the target group reported that the issue was not one they would talk about with their peers, irrespective of the campaign.
Similarly, in the United States Men Can Stop Rape runs a public education campaign for men and boys with the message: “My strength is not for hurting.” This campaign runs in conjunction with Men of Strength (MOST) clubs—a primary prevention program that provides high-school-age young men with a structured and supportive space to learn about healthy masculinity and the redefining of male strength.
Although programs to alter cultural and social norms are among the most visible and ubiquitous of all strategies for preventing intimate partner and sexual violence, they remain one of the least evaluated. Even where evaluations have been undertaken, these have typically measured changes in attitudes and beliefs rather than in the occurrence of the violent behaviors themselves, making it difficult to draw firm conclusions on their effectiveness in actually preventing intimate partner and sexual violence. Nonetheless, some evidence is emerging to support the use of the three types of programs reviewed above in changing the social and cultural gender norms
that support intimate partner and sexual violence. However, these must now be taken to scale and more rigorously evaluated.
KEY MESSAGES
- To achieve change at the population level it is important to target societal-level factors in the primary prevention of intimate partner and sexual violence. Approaches include the enactment of legislation and the development of supporting policies that protect women, addressing discrimination against women, and helping to move the culture away from violence—thereby acting as a foundation for further prevention work.
- Currently, there are no strategies of demonstrated effectiveness for preventing sexual violence outside intimate partner or dating relationships. Only one strategy has been demonstrated to be effective in preventing intimate partner violence, namely school-based programs for adolescents to prevent violence within dating relationships—and this still needs to be assessed for use in resource-poor settings.
- Although it is too early to consider them proven, evidence is emerging of the effectiveness of several other strategies for the prevention of intimate partner and sexual violence, particularly the use of microfinance with gender equality training and of programs that promote communication and relationship skills within communities.
- Developing the evidence base for programs for the primary prevention of intimate partner and sexual violence is still very much in the early stages. But there is every reason to believe that rigorous outcome evaluations of existing programs and the development of new programs based on sound theory and known risk factors will lead to a rapid expansion in coming years.
INTERNATIONAL MEN AND GENDER EQUALITY SURVEY2
Gary Barker, Juan Manuel Contreras, Brian Heilman,
Ajay Singh, Ravi Verma, and Marcos Nascimento
The International Men and Gender Equality Survey (IMAGES) is a comprehensive household questionnaire on men’s attitudes and practices—as well as women’s opinions and reports of men’s practices—on a wide
________________
2 Adapted from: Barker, G., J. M. Contreras, B. Heilman, A. K. Singh, R. K. Verma, and M. Nascimento. 2011. Evolving men: Initial results from the International Men and Gender Equality Survey (IMAGES). Washington, DC: International Center for Research on Women.
variety of topics related to gender equality. From 2009 to 2010, household surveys were administered to more than 8,000 men and 3,500 women ages 18 to 59 in Brazil, Chile, Croatia, India, Mexico, and Rwanda. Topics in the questionnaire included gender-based violence, health and health-related practices, household division of labor, men’s participation in care-giving and as fathers, men’s and women’s attitudes about gender and gender-related policies, transactional sex, men’s reports of criminal behavior, and quality of life. This report focuses on the initial, comparative analysis of results from the men’s questionnaires across the six countries, with women’s reports on key variables.
Methodology
IMAGES followed standard procedures for carrying out representative household surveys in each participating city, with the exception of Rwanda, where the survey is a nationally representative household sample. The survey was carried out in one or more urban settings in each country (and rural and urban areas in Rwanda) with men and women ages 18 to 59, guided by the following parameters:
- The men’s questionnaire has approximately 250 items and took from 45 minutes to an hour to administer; the questionnaire for women is slightly shorter and took from 35 minutes to an hour to administer. The survey instruments were pretested in the participating countries, and the study protocol was approved by the institutional review board (IRB) of the International Center for Research on Women and by in-country IRBs, when such existed.
- The survey instrument was designed to be relevant for adult men and women in stable, co-habitating relationships as well as those not in a stable relationship; women and men who define themselves as heterosexual as well as men and women of different sexual orientations and practices; and women and men who have children in the household (biological or otherwise) and those who do not.
- Double-back translation of the questionnaire was carried out to ensure comparability and consistency of questions across settings. Some country-specific questions were included; some countries excluded items because of local political or cultural considerations.
- In Brazil, Chile, Mexico, and Rwanda the questionnaire was an interviewer-administered paper questionnaire. In India the questionnaire was carried out using hand-held computers, with a mixture of self-administered questions and interviewer-asked questions. In Croatia the questionnaire was self-administered (using a paper
questionnaire). Standard procedures were followed for ensuring anonymity and confidentiality.
- All research sites followed standard World Health Organization (WHO) practices for carrying out research on intimate partner violence in terms of offering referrals and information for services and special training of interviewers. Following these guidelines, men and women were not interviewed from the same household in any of the research sites.
- More sensitive questions were asked later in the questionnaire, and some key variables were included in multiple questions (to compare and thus be more informed in affirming validity). The questionnaire was pretested in all the settings prior to application.
- In all settings, male interviewers interviewed male respondents, and female interviewers interviewed female respondents, with the exception of Mexico, where some interviews with men were carried out by female interviewers (but only women interviewed women).
- Survey locations were chosen to represent different contexts in each country to achieve a mixture of major urban areas and a secondary city or cities. Within a survey location, neighborhoods or blocks were chosen based on population distributions from the most recent census data. Rural areas were included only in Rwanda and Croatia. Stratified random sampling and probability proportion to size sampling methods were used within each neighborhood or community to ensure the inclusion of adequate sample sizes by age and residence (and also socioeconomic status in the case of Chile).
- Although every participating country’s questionnaire included questions on all the themes that make up IMAGES, the questionnaire is not identical in all countries; thus data are not available from every country for every question. The questionnaire in Rwanda was the most abbreviated of the six study countries because of the much larger sample size—and thus the sheer number of interviews—required to make the study nationally representative. In those cases where Rwandan data does not appear in a table or figure in this document, that particular question was not included in the Rwandan questionnaire.
Topics
The questionnaire covers key topics in gender equality, including intimate relationships, family dynamics, and key health and social vulnerabilities for men. Based on previous research that found associations between early childhood exposure to violence and different gendered practices related to childrearing, items on childhood antecedents to particular men’s practices were included. Specific topics in the questionnaire include:
- Employment. Employment experience; unemployment and underemployment; stress and reactions associated with unemployment; reaction by spouse/partner when unemployed; income differentials between men and women; perceived gender dynamics in the workplace; work–life balance; and job satisfaction.
- Education. Educational attainment; perceived gender norms and patterns in school.
- Childhood experiences. Victimization by violence as children; witnessing of gender-based violence; gender-related attitudes perceived in family of origin; changes perceived from previous generation to the present; gender balance in work/child care in family of origin; gender patterns of childhood friendships.
- Relations at home (in current household). Marital/cohabitation status; division/participation in household chores; perceived satisfaction in family life; household decision making; time use in specific domestic chores and family care, including child care.
- Parenting and men’s relationships with their children (and with non-related children who may live in the household). Number of children; living situation of each child; time/money spent in care of each child; use of paternity/maternity leave; perceptions/attitudes toward existing parental leave in country; and child-care arrangements.
- Attitudes toward women and masculinity. Attitudes toward gender equality (using the Gender-Equitable Men [GEM] Scale and other measures); attitudes toward various gender-equality policies that may have been implemented in each country.
- Health and quality of life. Lifestyle questions (substance use, exercise, etc.); use of health services; sexual and reproductive behavior (contraceptive use, condom use); sexually transmitted infections, including HIV (past history, HIV testing); satisfaction with sexual relations; mental health issues (depression, suicide ideation); social support; use of/victimization by violence in other contexts; morbidity.
- Partner relations and spousal relations. Current relationship status/satisfaction; use of services/help-seeking in times of violence or relationship stress; relationship history.
- Relationship, gender-based violence, and transactional sex. Use of violence (physical, sexual, psychological) against partner (using WHO protocol); victimization of violence by partner (using WHO protocol); men’s use of sexual violence against non-partners; men’s self-reported purchasing of sex or paying for sex, including with underage individuals.
- Sexual behavior. Sexual experience; sexual orientation; behaviors related to sexual and reproductive health, HIV/AIDS; use of health services related to sexual and reproductive health.
Analytical Strategy
The report focuses on men’s attitudes and practices related to relationship dynamics, parenting and caregiving, health-related practices and vulnerabilities, violence (intimate partner violence and other forms), transactional sex, and attitudes toward existing gender equality policies. Women’s reports of men’s practices are included for some key variables.
The selection of questions in this initial data analysis was informed by previous research confirming the associations or impact of early childhood experiences, individually held gender-related attitudes, educational attainment, age (as a proxy of generational differences as well as developmental stage), social class (or income), and employment status and economic stress on women’s and men’s attitudes and practices in terms of their intimate relationships, their sexual practices, their use of violence, their domestic practices, and their health-seeking behaviors. Men’s knowledge of and attitudes toward key policy issues related to gender equality are also included. The report focuses on descriptive statistics and bi-variate analyses of the associations between these practices and educational levels, economic or work-related stress, gender-related attitudes, and age. In all cases where statistically significant differences are reported, these are at the p < .05 level as assessed using the Pearson’s chi-square test. As noted earlier, we also have an interest in understanding generational changes, or changes over time, in terms of men’s practices. IMAGES is not a longitudinal study; nonetheless, by comparing responses stratified by age groups we can make some inferences about generational change.
Key Findings
Work-Related Stress
Work-related stress is commonplace in all survey sites. Between 34 percent and 88 percent of men in the survey sites reported feeling stress or depression because of not having enough income or enough work. Men who experienced work-related stress were more likely to report depression, suicide ideation, previous arrests, and use of violence against intimate partners.
Gender Attitudes
Men showed tremendous variation in their gender-related attitudes, with India and Rwanda showing the most inequitable attitudes. As a measure of men’s and women’s gender-related attitudes, IMAGES applied the GEM Scale. Rwandan and Indian men consistently supported the least
equitable norms among the settings studied. For example, for the statement “Changing diapers, giving kids a bath and feeding kids are the mother’s responsibility,” only 10 percent of men in Brazil agreed, whereas 61 percent in Rwanda and more than 80 percent in India agreed with the statement. Men with higher educational attainment and married men had more equitable attitudes; unmarried men had the least equitable attitudes. Homophobic attitudes were common, although they varied tremendously by context. Men who said they would be ashamed to have a gay son ranged from 43 percent of men in Brazil to a high of 92 percent in India. A slightly lower, but still high proportion of men said that being around homosexual men makes them uncomfortable, ranging from a low of 21 percent of men in Brazil to a high of 89 percent in India. Younger men and men with higher levels of education were generally less homophobic.
Relationship Dynamics and Domestic Duties
Younger men, men with more education, and men who saw their fathers do domestic work are more likely to carry out domestic duties. Nearly half of men in all the sites said they play an equal or greater role in one or more household duties—with the exception of India, where only 16 percent of men reported that they played an equal or greater role in household duties. These household or domestic duties included washing clothes, repairing the house, buying food, cleaning the house, cleaning the bathroom or toilet, preparing food, and paying the bills. The tasks that men said they play an equal or greater role in are those traditionally associated with men—namely repairing the house, paying bills, and buying groceries. Men reported higher levels of sexual and relationship satisfaction than women. Women who said their partners do more domestic work are more sexually satisfied. Men reported relatively high rates of sexual satisfaction with their current stable partners, ranging from 77 percent in Croatia to 98 percent in India. In all the countries except India, men who reported more gender-equitable attitudes were more likely to report being sexually satisfied with their current female partner. In India, Brazil, and Croatia, women who reported that their male partner plays an equal or greater role in one or more domestic duties also reported higher levels of overall relationship and sexual satisfaction.
Parenting and Involvement in Childbirth
The majority of men were neither in the delivery room nor in the hospital for the birth of their last child. In Chile, however, a dramatic generational shift is under way in men’s presence at childbirth. Younger Chilean men reported much greater rates of presence in the delivery room
for the birth of their last child than older men. This shift is largely due to a national policy, aimed at “humanizing” the birth process, which encourages women to have a male partner or other person of their choice present during birth at public maternity wards. Men are taking few days of paid or unpaid paternity leave. Among men who took leave, the average duration ranged from 3.36 to 11.49 days of paid leave and from 3.8 to 10 days of unpaid leave. Younger men and men with more education were more likely to take leave. Close to half of men with children said they are involved in some daily care-giving. Unemployed men are dramatically more likely to participate in the care of children than employed men. For men with children under age four, play is the most common daily activity in which they participate (as affirmed by women and men).
Health Practices and Vulnerabilities
Men’s rates of regular abuse of alcohol—defined as having five or more drinks in one night on a once monthly or greater basis—vary from 23 percent in India to 69 percent in Brazil and are significantly higher than women’s reported alcohol abuse in all survey sites. In most sites, younger men and men with more inequitable gender attitudes are more likely to regularly abuse alcohol. High proportions of women who reported having sought an abortion affirmed that a male partner was involved in the decision to seek an abortion (ranging from 39 percent to 92 percent). Men reported high self-esteem, with the exceptions of Croatia and India; at the same time, men showed relatively high levels of depression and suicide ideation. The rates of experiencing depression at least once in the past month ranged from 9 percent in Brazil to a high of 33 percent in Croatia. The percentages of male respondents who reported having suicidal thoughts “sometimes or often” in the past month ranged from 1 percent in Brazil and Mexico to 5 percent in Croatia.
Violence and Criminal Practices
Men reported lifetime rates of physical intimate partner violence ranging from 25 percent to 40 percent, with women reporting slightly higher rates. Factors associated with men’s use of violence were rigid gender attitudes, work stress, experiences of violence in childhood, and alcohol use. Men’s reports of perpetration of sexual violence against women and girls ranged from 6 percent to 29 percent; in India and Mexico the majority of sexual violence took place against a current or former partner. Relatively high percentages of men reported ever having participated in criminal or delinquent acts; between 6 percent and 29 percent of men reported ever having been arrested. In terms of factors associated with
men’s participation in criminal activity, men’s socioeconomic situation was the most significant. Men who owned firearms or carried out violence or criminal behavior were also more likely to report having used intimate partner violence.
Transactional Sex
Between 16 and 56 percent of men surveyed said they have paid for sex at least once. Men with lower educational attainment and less gender-equitable attitudes and men who reported less sexual satisfaction with their current partner were more likely to have paid for sex.
Knowledge and Attitudes About Policies and Laws Related to Gender Equality
Men in all the countries, with the exception of India, were generally supportive of gender equality, with 87 percent to 90 percent agreeing that “Men do not lose out when women’s rights are promoted.” Even when asked about specific policies—quotas for women in executive positions, in university enrollment, or in government—men’s support for such policies was reasonably high, with 40 percent to 74 percent of men supporting such quotas. Among themes related to gender equality, men reported the highest exposure to campaigns about gender-based violence. At the same time, across the sites, men showed negative attitudes toward laws related to gender-based violence.
Conclusion
Overall, IMAGES results affirm that gender equality should be promoted as a gain for women and men. Change seems to be happening as younger men and men with higher levels of education show more gender-equitable attitudes and practices. Men who reported more gender-equitable attitudes are more likely to be happy, to talk to their partners, and to have better sex lives. Women who reported that their partners participate in daily care work report higher levels of relationship and sexual satisfaction. Findings suggest that most men in most of the survey sites accept gender equality in the abstract even if they are not yet living it in their daily practices.
THE SCIENCE OF PREVENTION/
INTERRUPTING THE CYCLE OF VIOLENCE
Claire Crooks, Ph.D.
Centre for Addiction and Mental Health,
Centre for Prevention Science and University of Western Ontario
Overview
This summary describes what we know and, perhaps more importantly, what we don’t know about intervening in the cycle of violence. It encompasses both direct child abuse and exposure to domestic violence. First, the term cycle of violence is clarified, as it is a term that has been adopted into the everyday lexicon without much clarity of concept. Next is a review of some of the key findings from comprehensive review papers summarizing child abuse prevention. Finally, five gaps are identified that indicate possible future directions for research into primary prevention in this domain.
What Is the Cycle of Violence?
The cycle of violence is a phrase used to describe the observed intergenerational pattern by which many children and youth who experience direct or indirect exposure to violence later come to perpetrate violence in their own relationships. For example, children who experience child abuse and are exposed to domestic violence are at an elevated risk for perpetrating dating violence and domestic violence. Essentially, there is a continuity in their relationships such that problems with violence are evident in different ways at different times. Researchers tend to look at this cycle from different vantage points depending on their main areas of interest. Bullying researchers, for example, might note that children who bully others are more likely to perpetrate dating violence as adolescents.3 Dating violence researchers might look at the continuity of violence between dating and adult intimate partner relationships. The investigation of direct and indirect exposure to violence has even been segmented, with child abuse researchers tending to focus on the former and domestic violence researchers tending to take on the latter. The result is a greatly segmented landscape, but one that can be pieced together to depict the cycle shown in Figure 6-1.
________________
3 Bullying prevention programs have been researched quite extensively and are outside the purview of this summary. Bullying/peer aggression was included in the cycle of violence figure as a reminder that children exposed to family violence have difficulties in multiple settings and often perpetrate or experience violence in relationships outside their families. A holistic approach to the impact of violence on children’s lives requires a commitment to beginning to piece together these formerly disparate areas of research.
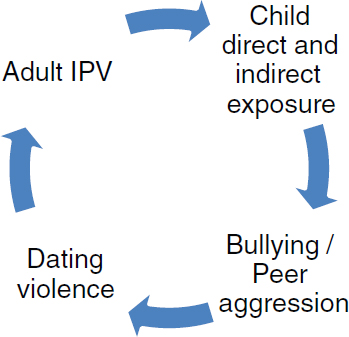
FIGURE 6-1 Cycles of violence.
SOURCE: Crooks, 2011.
It is crucial to understand that the cycle of violence is probabilistic, not determinative. That is, experiencing child abuse increases the risk for subsequently perpetrating violence in relationships, but there is significant variability in trajectories. There are a few important qualifiers for the cycle of violence idea, and they are discussed below.
Abusive Behavior Is Multiply Determined
There is no one pathway to abusive behavior. Rather, it is a final common pathway for a host of social, behavioral, biological, and personality risk factors. Results of a 20-year prospective study show that children’s direct and indirect exposure to violence are important risk factors for perpetration of abusive behavior (Ehrensaft et al., 2001). Furthermore, the risk for experiencing intimate partner violence as an adult (as a victim or perpetrator) increases with the number of types of abuse and additional stressors experienced as a child (Whitfield et al., 2003). At the same time, many children and youth who are abused do not become perpetrators of abuse with their own children. A review of studies suggested that approximately one-third became seriously inept, abusive, or neglectful as parents of their own children; an additional one-third remained at risk for perpetrating child abuse because of their vulnerability to social stress; while the remaining one-third were not abusive (Oliver, 1993).
Experiences of Abuse Show a Dosage Response
The Adverse Childhood Experiences (ACE) Study4 carried out jointly by the Centers for Disease Control and Prevention and Kaiser Permanente has conclusively demonstrated a dosage effect for child maltreatment. This ongoing longitudinal study has been analyzing the relationships between multiple categories of childhood trauma and negative health and behavioral outcomes later in life. David Finkelhor’s work on poly-victimization is also instructive in identifying both the high frequency of poly-victimization and the relationship between multiple forms of abuse and poor outcomes for children (Finkelhor et al., 2009). Research with adolescents has documented this same relationship between multiple forms of abuse and the perpetration of violent delinquency as an adolescent, with each additional form of abuse translating to a 124 percent increase in the relative odds of engaging in violent delinquency (Crooks et al., 2007).
Co-Existing Adversities Increase the Likelihood of Negative Outcomes
Abuse affects different children differently. The ACE Study has documented the additive detrimental effects of experiences such as exposure to woman abuse, a parent with substance abuse or mental health problems, and incarceration of a parent. Low socioeconomic status can further compound difficulties for children who are experiencing child abuse. Conversely, access to protective factors (including at least one stable, nonviolent caregiver) can mitigate these impacts (Herrenkohl et al., 2008).
To summarize what we know about childhood experiences of abuse and exposure to domestic violence as a risk factor for perpetrating violence as an adolescent or adult, it is clear that childhood exposure to violence is a strong risk factor. However, there is still considerable variability among individual outcomes, and additional risk or protective factors can either exacerbate or mitigate the risk conferred by child abuse. Cumulative experiences of child abuse tend to lead to more negative outcomes, both in terms of perpetrating violence and a whole host of other negative social and physical health outcomes. The cycle of violence depicts the what of intergenerational transmission, but it does not explain the how or why. It is important to understand the cycle of violence in terms of how it works, because understanding the mechanisms underlying the intergenerational transmission of violence provides an important basis for understanding intervention opportunities.
________________
4 Results of the study are available at http://www.cdc.gov/ace/index.htm.
How Does the Cycle of Violence Work?
At a superficial level, the intergenerational transmission of violence seems counterintuitive—if someone knows how devastating it is to be abused as a child, how can he or she turn around and do the same thing as a parent? The answer lies in understanding the impact of child abuse on a developing child and understanding how experiences of child direct and indirect exposure to violence change how an individual sees the world and others around him or her. This understanding also explains why child exposure to violence is not something that a person can just “get over.” Three particularly useful frameworks and theories for explaining the intergenerational cycle of violence are attachment, social learning theory, and trauma.
The Role of Attachment
Attachment refers to the quality of the relationship that develops between an infant and his or her primary caregiver(s) (Bowlby, 1980, 1990). Secure attachment emerges within the context of responsive caregiving. The extent to which an infant is fed when she is hungry, changed when she is wet and uncomfortable, and soothed when she is upset or afraid provides a basis for secure attachment. This first relationship becomes a template for future relationships and organizes the way an infant comes to see the world: Is it a safe and predictable place or a scary and bizarrely unpredictable one? Decades of research demonstrate that when attachment develops in a disorganized manner, an individual is at risk for ongoing difficulties in relationships with others. Child abuse and attachment are connected in a number of ways, including the development of attachment, the impacts of abuse, and the later perpetration of abuse (Bacon and Richardson, 2001). Experiences of direct and indirect child exposure to violence undermine the potential for secure attachment and provide an early experience of relationships as dangerous and unpredictable.
Although attachment is most often discussed in the context of parent–infant relationships, it continues to play an important role throughout a youth’s development. Recent longitudinal research demonstrated that youth dually exposed to direct and indirect violence (i.e., child abuse and exposure to domestic violence) were less attached to their parents in adolescence than those who experienced only direct or only indirect exposure (Sousa et al., 2011). Furthermore, attachment to parents during adolescence played an important protective role against antisocial behavior, independent of abuse status.
Social Learning Theory
Social learning theory is a well-established paradigm that highlights the importance of reinforcement for promoting certain behavioral responses and inhibiting others (Bandura, 1977, 1986). Furthermore, our experiences with behavior and reinforcement come to shape our attitudes and attributions. One of the key tenets of social learning theory is that humans learn very well from modeling, that is, from what they see others do. This modeling is not indiscriminate. Children do not copy everything around them, but they copy what they see that works. When they are exposed directly and indirectly to violence, they learn harsh but effective lessons about power and may come to see the world as made up of victims and victimizers (Dodge et al., 1994). Given such a dichotomy, they may begin to model after the victimizer to avoid further abuse. These children develop a hostile attribution bias, which is a cognitive framework for expecting the worse, even in threat-neutral situations (Fontaine, 2010). As a result, these children seem hostile and aggressive to their peers, and may be rejected by their more pro-social peers (Dodge et al., 1990). There is some evidence that exposure to family violence is a bigger contributor to later pro-violence attitudes (such as comfort with aggression, aggressive responses to shame, excitement about guns, and violence as means of preserving power) than violence experienced in the school or community (Slovak et al., 2007). In addition to underscoring the importance of what children learn, social learning theory would also draw attention to what these children do not learn, namely, egalitarian relationships, non-violent approaches to conflict resolution, and emotional regulation skills.
Trauma
A third perspective that has been explored for understanding the cycle of violence is the trauma perspective. Based on his work with adolescent boys who have perpetrated lethal violence, James Garbarino has identified a process which he refers to as “hibernation of the soul” (Garbarino, 1999). Essentially, under conditions of severe, early, and chronic violence, these children may come to suppress their more humane aspects as a survival mechanism. The detachment from emotion and compassion that allows a person to survive chronic abuse is the same detachment that facilitates perpetration of severe violence without apparent remorse. Even in less extreme cases of trauma, the dysregulation of anger and arousal that develop create potent risk factors for the intergenerational transmission of violence. A significant literature has emerged to support these processes from a neurobiological perspective, which demonstrates that over-activation of the fight or flight response can result in a weak foundation for the development
of emotional regulation and self-soothing (van der Kolk and Greenberg, 1987).
In considering these three frameworks for understanding the cycle of violence—attachment, social learning, and trauma—it is evident that there are no quick fixes for breaking this cycle. Child abuse does not arise because of a lack of discipline; consequently, get-tough approaches with parents will not redress the risks. Similarly, it does not arise merely from a lack of parental support; as such, increasing support without targeting the underlying causes will not be very successful in preventing and reducing a child’s direct and indirect exposure.
What Programs Are Effective or Promising?
In efforts to prevent child abuse and exposure to domestic violence, there are a number of points for possible intervention. Prevention in other areas is often divided into universal (or primary), selective (or secondary), and indicated (or tertiary). However, an argument can be made that using this type of classification locates the abuse with the victim and pathologizes the experience of abuse. Macmillan and colleagues have proposed an alternative schema for identifying intervention points, presented in Figure 6-2 (Macmillan et al., 2009). With this approach it is clear that one can work to prevent abuse before it occurs, to prevent abuse from recurring, and to prevent impairment following abuse. Each of these targets is necessary in a comprehensive approach, and different strategies will be effective at different points.
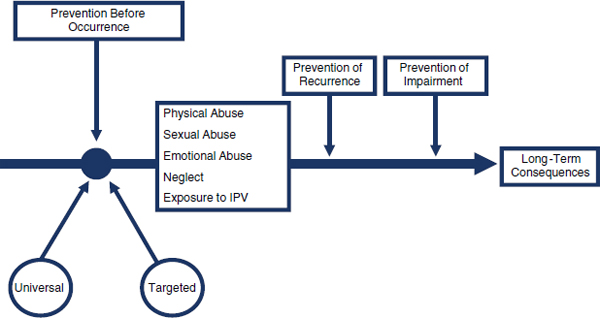
FIGURE 6-2 Intervention to prevent child maltreatment and associated impairment.
SOURCE: Macmillan et al., 2009.
Comprehensive reviews to identify what works to prevent child abuse or recurrence of child abuse follow one of two basic approaches. The first approach is to look across all previous summaries and reviews and amalgamate all of the existing evidence (Mikton and Butchart, 2009). This approach provides a somewhat bleak picture, because when studies are combined, results are generally mixed or disappointing. However, such an approach can be misleading because it includes studies that vary greatly in quality both in terms of the intervention and the research design. By contrast, the review by MacMillan and colleagues looks at high-quality programs that have shown good effects under reasonable research conditions but perhaps have yet to be replicated (Macmillan et al., 2009). Reviewing the existing studies in these two ways finds three approaches that can be considered effective or promising. Additional approaches may improve protective factors or reduce risk factors, but these three are the only ones that have been shown to prevent the occurrence or recurrence of abuse.
Home Visitation
Home visitation is the most effective child maltreatment prevention program to date (Macmillan et al., 2009). There is considerable variability in home-visiting interventions in terms of their models, service delivery, and home staffing. Two models, the Nurse-Family Partnership and the Early Start program, have been shown to be effective in reducing some indicators of child abuse. However, effects have not been uniform across other approaches to home visiting, and there are a few caveats for the success of home visiting. First, most of what we know is based on David Olds’ pioneering work, and efforts to replicate his work have had mixed success. Second, home visitation has proved to be more effective when carried out by nurses than by paraprofessionals. Third, it may be more effective with certain types of families (such as first-time mothers) than others (Macmillan et al., 2009). Finally, the presence of domestic violence may undermine the effectiveness of home visiting. In the Elmira Home Visiting study the intervention reduced reports of child maltreatment, but not for families with mothers reporting more than 28 incidents of domestic violence (Eckenrode et al., 2000).
Parent Training and Education
The results for parent training and education in general are mixed, but there are two programs that have evidence supporting their use. First, the Positive Parenting Program (Triple P) has shown promise in one study for preventing abuse, and replication is currently under way. The Triple P uses multiple levels of social learning–based programs to meet the needs of different families and offers five levels of intervention with increasing intensity
to match higher-needs families (Prinz et al., 2009). Mark Chaffin and colleagues’ work on Parent–Child Interaction Training has also been very promising in that it has been shown effective in lowering recurrence of physical child abuse (Chaffin et al., 2004). Parent–Child Interaction Training uses behavioral conditioning principles and provides immediate and detailed feedback for parents in their interactions with their children. It has been shown to both increase positive interactions and decrease recurrence of child abuse. Both of these programs warrant further investigation, particularly with larger samples of fathers, as most research has focused on mothers.
Educational Prevention of Abusive Head Trauma
The final effective strategy to date is education aimed at preventing abusive head injury (also known as shaken baby syndrome). Offered mainly through hospitals, this education offers normative information about babies’ crying, coping strategies for parents, and the impacts of shaking an infant. There is a one study to date that found that the introduction of this program lowered the rates of abusive head trauma (Dias et al., 2005). Additional trials are under way. This program appears to be a cost-effective way to reduce one specific type of child abuse.
Interventions Lacking Empirical Evidence
Consistent with the general move to positive psychology, there has been much interest in interventions that build on parents’ strengths. Many of these approaches use a mentoring or mutual support model of parents helping other parents in a way to normalize intervention and build informal support networks. The general benefits of mentoring and of encouraging strong social networks are widely accepted, but these approaches have not been found effective in the prevention of child exposure to direct or indirect violence (Macmillan et al., 2009). It is critical to recognize the distinction. A parenting program may increase parents’ satisfaction with parenting, improve their social connections, and even lead to more positive attitudes and skills, and yet it may not reduce direct child abuse or exposure to domestic violence. If a program is being espoused as a child abuse prevention program, then the research must look at child abuse outcomes and not rely on proxies or interpret the promotion of positive parenting attitudes and skills as synonymous with the prevention of abuse.
Preventing Child Exposure to Direct and
Indirect Violence: The Big Picture
A review of the state of the science of child abuse prevention reveals a number of basic facts. First, there are some effective and promising
interventions, but even these have limited evidence compared to many other areas of social and medical science. Second, it obscures the picture to collapse evidence across types of intervention (e.g., with meta-analytic techniques) with no consideration for the quality or features of the program. Quality of implementation matters, training of implementers matters, and matching the intervention to the risk level of the families matters. Third, at this point there is little available evidence concerning programs that are effective for preventing emotional abuse. Finally, there have not been any trials on programs to reduce exposure to domestic violence. Community-based approaches to preventing domestic violence have not been well researched, and there are no studies evaluating strategies for preventing exposure when domestic violence is occurring. On a more hopeful note, there are many innovative interventions in varying degrees of development and evaluation. It takes a long time to reach the point where a randomized controlled trial or multi-site replication is feasible.
Gaps and Challenges
A review of the state of the research shows clearly that while we have an emerging idea of effective practice in some specific areas, there are still many gaps. Below are five gaps in research and practice.
Where Are the Dads?
Much research has focused exclusively on mothers or not included enough fathers for useful subgroup analysis. This lack of representation in research mirrors the child protection policies and practices, which tend to focus on mothers and view fathers as either dangerous or irrelevant. The reality is that men who have perpetrated violence often remain part of their children’s lives and require specific and intentional strategies to change attitudes and beliefs that support their abusive behavior, particularly when these men have also abused the children’s mothers (Scott and Crooks, 2004). Furthermore, there is a dearth of programs that both address the gendered nature of violence and address men’s abuse of their intimate partners and children concurrently. The Fathering After Violence initiative5 for men who have been abusive to intimate partners and the Caring Dads program6 for men who have been abusive to their partners and their children are exceptions to the rule.
________________
5 See http://endabuse.org/section/programs/children_families/_breaking_cycle.
Is Stopping the Violence Enough for Positive Child Outcomes?
When we look for successful outcomes in research, we often use the idea of recidivism or repeat violence as a sign of failure, but the corollary to that is that success is equated with no further violence. The reality is that, in the life of a child who has been victimized, just stopping the violence might not be good enough. There has been some discussion about restorative parenting and applying restorative justice models to the parent–child relationship, but we do not actually have a good sense yet about what that looks like or the implications for the child. Some work has been done in this area of child sexual abuse, but very little has been carried out that looks at father–child relationship restoration after domestic violence. There is a significant need to develop and evaluate protocols for deciding when it is safe to restore parent–child relationships post-violence and how this can be achieved with minimal risk to children.
Compartmentalization of Efforts
There have been some big strides in breaking down silos between types of abuse since the “Greenbook” was published as a model for collaboration between child protection and domestic violence sectors (Schecter and Edleson, 1999), but there is still too much compartmentalization within fields. Often researchers emphasize one type of abuse without looking at the complexities of poly-victimization or, what is even trickier, the co-occurrence of perpetration and victimization. For example, most research and programming for children exposed to domestic violence still does not inquire about the direct victimization experience of the children, particularly for abuse perpetrated by the victim parent. There are philosophical and practical reasons for these practices, but they hinder a fuller understanding and more effective response to children.
What Do Culturally Relevant Programs Look Like?
Virtually every paper or chapter ends with a plea for more culturally diverse and appropriate services, yet we have only scratched the surface in exploring what this really means. Is it merely resources translated into different languages? Is it trained therapists from the same ethnic or cultural background as the families? Is it program manuals that have different faces on them? It can be argued that we need to go much further than these superficial changes and that we have not done a good job of documenting or evaluating these processes of cultural adaptation. The challenge for cultural adaptation is further complicated when we look at implementing promising practices on a global scale, particularly in countries with less developed child protection or mental health systems.
What Is an Effective Specialized Response in the Highest Risk Cases?
Finally, for the most high-risk families, there is a complexity in terms of system involvement and information sharing that can only be addressed by collaboration across systems. Any comprehensive approach to preventing violence against children requires specialized responses that can be activated in the most high-risk cases. With the advent of domestic violence homicide review committees, a clearer picture of the risk factors for lethality to women and their children is emerging (Jaffe et al., 2003; Campbell, 2005; Jaffe and Juodis, 2006). In these cases, home visiting and parent education are not sufficient or appropriate for the degree of risk. In addition to developing clinical interventions for a wide range of families, we need to develop specialized collaborative protocols for the highest-risk cases.
In closing, although reviews that combine all interventions of a certain type tell a disheartening story, there are some bright spots in our search for effective interventions. Home visiting, parent education and training, and education approaches to abusive head trauma have all shown promise and a solid degree of evidence. The science is at the point where we know enough to know that there are no easy answers and no quick fixes. Different families need different types of support and intervention at different points in time, and we need to develop a comprehensive and coordinated system of care to ensure that no children fall between the cracks. It is a colossal task, but a vital one, because at the end of the day our children need to be safe from abuse and violence to develop to their full potential and grow into the type of adults who will contribute to a compassionate and productive society.
TRAUMA-INFORMED CARE: A VALUES-BASED
CONTEXT FOR PSYCHOSOCIAL EMPOWERMENT
Roger D. Fallot, Ph.D.
Community Connections
We make a fundamental distinction between trauma-informed care and trauma-specific services (Harris and Fallot, 2001). Psychosocially empowering, trauma-specific interventions take as their primary goals ameliorating trauma-related difficulties and facilitating trauma recovery and healing. The Trauma Recovery and Empowerment Model, Seeking Safety, Trauma Affect Regulation: Guide for Education and Therapy (TARGET), the Boston Consortium Model, and Beyond Trauma, among others, are manualized approaches to helping women (and sometimes men as well) develop the skills necessary to cope more effectively with the impact of violence and abuse and to avoid revictimization (Harris, 1998; Najavits, 2002;
Covington, 2003; Ford and Russo, 2006; van Lier et al., 2009; Amaro, 2011). These interventions and many individual ones that focus primarily on post-traumatic stress disorder, such as exposure therapy, cognitive processing therapy, and other cognitive-behavioral approaches (e.g., Mueser et al., 2008), are an important component of trauma-informed care (Resick et al., 2008; Powers et al., 2010).
However, “cultures of trauma-informed care” refer to the programmatic, organizational, and community contexts that are necessary and valuable in supporting survivors and the staff who serve them. Any setting can be trauma-informed when it takes fully into account what we know about trauma, its impact, and the diverse, individualized paths to trauma recovery. In this way, not only behavioral health care settings but also primary care institutions, schools, and even correctional facilities can be trauma-informed. When an organizational culture becomes trauma-informed, it becomes more welcoming and hospitable for trauma survivors (as well as the rare individual who does not have a history of exposure to violence); it minimizes the possibility of revictimization; it indirectly facilitates healing, recovery, and empowerment; and it builds collaborations throughout the service system.
Trauma-informed care is important for a number of reasons:
- Trauma and, in particular, violent victimization are pervasive.
- The impact of trauma is broad, extending well beyond the post-traumatic stress disorders frequently perceived to be the most common outcome.
- The impact of trauma is often deep and life-shaping.
- Trauma, especially caused by interpersonal violence, is often self-perpetuating.
- Violence is even more common in the lives of those who are socially and politically vulnerable, including the poor, many racial and ethnic minorities, women and children, those diagnosed with mental health or substance abuse problems, and people who are developmentally disabled.
- Trauma affects the way people approach the human service setting, heightening fear and suspiciousness.
- The service system itself has too often been retraumatizing.
Retraumatization in the behavioral health care setting is one of the experiences that originally fueled awareness of the need for trauma-informed care (Jennings, 1998). Two types of retraumatization are noteworthy. First are the many ways in which traumagenic dynamics may be replicated in service provision. Examples include providers’ lack of interest in traumatic violence or their disbelief of individuals’ reports of violent victimization; both of these patterns may replicate earlier experiences, in which signs and
reports of violence were minimized or denied. Coercive approaches involving involuntary medication and hospitalization are still too common in many settings. And the presumption of incompetence (e.g., the inability to handle one’s own finances) may be a part of standard operating procedure in many programs, a visible reminder of the ways in which survivors’ skills are overlooked.
Second are instances of “sanctuary harm” (Robins et al., 2005). Consumers surveyed about their experiences in behavioral health care settings report violence and the fear of violence (including physical restraint and seclusion) as well as negative interactions with staff involving disrespect and humiliation. Taken as a whole, then, it is not surprising that one prominent psychiatrist has written that the past 30 years has evinced a continuing story of “destroying sanctuary” in the human services system (Bloom and Farragher, 2010).
As a counter to this destructive organizational culture, we have developed a model of trauma-informed care that builds on core values of safety, trustworthiness, choice, collaboration, and empowerment (Fallot and Harris, 2008, 2009). These values are key antidotes to the toxic effects of violence in the lives of consumers and staff members in human service delivery settings. For those who have been exposed to violence repeatedly and unpredictably, physical and emotional safety is a high priority. For those individuals affected by violence perpetrated by those who were supposed to be family or institutional caretakers, trustworthiness is a high priority. For those whose sense of voice and control has been attenuated by violent victimization, choice is a high priority. For those who have experienced the world as consistently arrayed in one-up, one-down relationships in which they have been the one down, the realistic offer to share power in a collaborative way is a high priority. And for those who have felt powerless to do anything about these other realities, empowerment is a high priority.
As a change in organizational culture, then, trauma-informed care extends far beyond any new service; it involves the physical setting, each contact, each activity, and each relationship in the organization. It extends beyond the training of clinical staff by engaging with all staff (including administrators, service staff, and support staff) and, importantly, all consumers to direct and monitor this change. Finally, trauma-informed care represents an opportunity to make these values into a routine part of the setting; it is broader than simply being “trained” in this approach.
Cultures of trauma-informed care balance trauma-specific emphases on individual empowerment and skills development with organizational emphases on safety, trustworthiness, choice, collaboration, and empowerment. This approach is consistent with other values-based approaches that have become prominent in the past two decades in behavioral health: recovery orientation, gender responsiveness, and cultural competence (Farkas et al.,
2005; Covington, 2007; Whitaker et al., 2007a). Furthermore, the core values of trauma-informed care are consistent with, and strongly supportive of, many evidence-based interventions, such as motivational interviewing, shared decision making, and psychosocial empowerment groups.
Basic shifts in both understanding and practice are fundamental in changing a traditional human service or community culture to one that is trauma-informed. Our protocol for developing a culture of trauma-informed care thus emphasizes both a paradigm shift in understanding and a thoroughly collaborative way to change practice (Harris and Fallot, 2001; Fallot and Harris, 2009). For instance, one of the key changes in understanding is establishing a “trauma first” mode of thinking about a consumer or staff member. Thus, we adopt a “trauma lens” through which other aspects of a person’s life may be viewed. Rather than asking, implicitly or explicitly, “What is wrong with you?” or “What is your problem?” we ask “What have you been through?” and “How have you tried to cope with it?” This basic change in orientation affects the organization’s view of not only consumers and staff members but also the nature of trauma itself, the services provided, and the relationship between consumer and provider. As the basic questions change, so do the approaches, from “Here is what I can do to fix you,” to “How can you and I work together to further your goals for recovery and healing?” Collaborative decision making and planning pervade trauma-informed cultures; not only are consumers’ opinions frequently sought and incorporated into individual service planning and organizational strategies, but also staff perspectives become central to administrators’ thinking as well.
In putting these ideas into practice, we address six domains of organizational culture in human service settings; three are service-level domains, and three are at the systems-level (Fallot and Harris, 2009):
Services-level changes in a culture of trauma-informed care:
- Informal service procedures and settings
- Formal service policies
- Trauma screening, assessment, service planning, and trauma-specific services
Systems-level changes in a culture of trauma-informed care:
- Administrative support for developing and sustaining this culture
- Staff training and education
- Human resources practices
As an example, let us examine our approach to informal service procedures and settings. Here we ask agency workgroups representing all constituencies (upper-level administrators, supervisors and middle management, service staff, support staff, and consumers) to review the sequence of
settings, activities, and people to whom consumers are likely to be exposed from the time of their first call to their final visit. We sometimes recommend a walk-through, in which staff literally put themselves in the place of consumers by going through the same procedures as a new consumer would in entering the agency. Once each physical setting, activity, contact, and relationship has been outlined, we ask key questions related to the core values:
- How can we ensure physical and emotional safety for consumers throughout our organization and larger system of care?
- How can we maximize trustworthiness? Make tasks clear? Maintain appropriate boundaries?
- How can we enhance consumer choice and control?
- How can we maximize collaboration and the sharing of power with consumers?
- How can we prioritize consumer empowerment and skill-building at every opportunity?
Agencies have taken this task on with enthusiasm, developing creative solutions to identified problems in these domains. For example, one residential substance abuse setting had a large sign that read “Denial stops here” over the entrance to the residential areas of its building. Deciding that this sign did not create a hospitable or emotionally safe first impression of their setting, they replaced it with a “Welcome” sign that was much more inviting. Clearer and more positive signs, more comfortable waiting rooms (with adequate space and with minimal intrusion of security staff), more positive first contacts via phone or in person, better lighting in hallways and outdoors, and more private intake procedures—among many others—are examples of the sorts of changes organizations have made in efforts to create safer and more welcoming environments.
Once this process is completed, we ask organizational workgroups to follow the same procedure, this time with a focus on the staff’s experiences of safety, trustworthiness, choice, collaboration, and empowerment. We have seen this “parallel process” with regard to trauma-related concerns played out repeatedly in a wide variety of settings. Simply put, only when staff members’ experiences of physical and emotional safety, of trustworthy relationships (with their co-workers and with supervisors and administrators), of choice in how they go about their daily work, of collaborative power-sharing with administrators and supervisors (so that staff input is weighed significantly), and of empowerment (so that staff members have the resources they need to do their jobs well) are in place is the staff able to create similar experiences for consumers.
Trauma-informed cultures of care develop over time with the collaboration and support of administrators who recognize the invaluable
perspectives of both staff and consumers. We have gathered qualitative data in support of this shift in organizational cultures. Consumers report that they feel more accepted. One woman said, for example, “Before this initiative, I had to leave an important part of myself on the doorstep to this agency; now I can bring my whole self inside.” Consumers, staff, and administrators frequently comment that the initiative fostered more collaborative relationships among them. Built on safety and trustworthiness and supported by valuing choice and empowerment, the capacity to share power meaningfully has become a hallmark of trauma-informed care.
As a values-based context strongly supportive of evidence-based trauma-specific interventions, trauma-informed organizational cultures represent a powerful source of engagement for women and their children who have been exposed to violence (Cocozza et al., 2005; Morrissey et al., 2005). (Also see the Substance Abuse and Mental Health Services Administration’s Women, Co-Occurring Disorders, and Violence Study for related discussions and findings.7) To the extent that secondary and tertiary prevention of such violence relies on creating settings that are welcoming and engaging for individuals with complex histories of violent victimization, trauma-informed care is an increasingly central requirement for programs designed to assist women and children.
ENHANCING EMOTION REGULATION:
A FRAMEWORK FOR PSYCHOLOGICAL EMPOWERMENT
OF WOMEN AND CHILDREN EXPOSED TO VIOLENCE
Julian D. Ford, Ph.D.
University of Connecticut School of Medicine
The health care and social service professions tend to approach the question of how to assist women and children who are victims of violence by doing research on, and developing practice guidelines for, the treatment of posttraumatic stress disorder (PTSD) (Forbes et al., 2010). Extensive surveys of scientifically validated and clinically promising PTSD treatments have been compiled by the International Society for Traumatic Stress Studies, the U.S. Department of Veterans Affairs, the Clinical Resource Efficiency Support Team (part of the Northern Ireland Health Service), the American Psychiatric Association, the British National Institute for Clinical Excellence, the Institute of Medicine, and the Australian Centre for Posttraumatic Mental Health at the University of Melbourne (CREST, 2003; APA, 2004; VA, 2004; NICE, 2005; IOM, 2006; Australian Centre
________________
7 Available at http://pathprogram.samhsa.gov/Resource/Women-Co-Occurring-Disordersand-Violence-Study-Program-Summary-21101.aspx.
for Posttraumatic Mental Health, 2007; Foa et al., 2009). These guidelines were developed to address diagnostic criteria for PTSD in the Diagnostic and Statistical Manual (APA, 1997).
Although laudable in that they have made the possible benefits of carefully developed therapies for PTSD increasingly known to professionals who treat victims of violence, this medicalized approach to helping victims recover from violence has several key limitations. First, the very terms, “victim” and “treatment” suggest a degree of passivity and deficiency that does a grave injustice to the typically extremely courageous and resilient survivors of violence. Violence temporarily disempowers those who must survive it, but even prolonged and horrific violence does not strip the survivor of the capacity to be empowered. Being viewed as broken or defective and therefore in need of corrective treatment as a result of having suffered violence adds injury (as well as insult) to injury. Although therapeutic treatments can be empowering, this is the case only to the extent that they emphasize helping the violence survivor restore or build their strengths. PTSD therapies definitely have been shown through both scientific and clinical research to empower children and adults who have experienced violence (Courtois et al., 2009; Ford and Cloitre, 2009). However, PTSD treatments tend to provide education and therapy based primarily on a view of PTSD as a breakdown of courage (i.e., avoidance of trauma reminders or memories) or deficits in arousal and anxiety management (i.e., hyperarousal, hypervigilance).
Recent research provides a basis for a paradigm shift from a pathology/deficit perspective to a framework of psychological empowerment for interventions for survivors of violence. Women and children who have been exposed to violence often suffer from aftereffects that either do not fit the criteria for PTSD or that involve symptoms and difficulties in daily living that go well beyond PTSD (Rayburn et al., 2005; Schumm et al., 2006; Ford et al., 2008, 2009, 2010, in press-b; Gill et al., 2008; Mongillo et al., 2009; Briggs-Gowan et al., 2010; Seng et al., in review). Although these sequelae might at first glance seem to be consistent with the pathology perspective (e.g., depression, panic, dissociation, addiction, oppositional–defiance, eating disorders, personality disorders, guilt, shame, complicated bereavement), in fact what they demonstrate is the extreme degree of biological, psychological, and interpersonal adaptation required to survive violence (Ford, 2005; Ford and Cloitre, 2009; Ford et al., 2009). These adaptations require substantial strength and resilience, rather than being markers for or the results of pathology or deficiencies (Herman, 1992; Courtois et al., 2009).
As a result of this paradigm shift, in the past decade an impressive array of psychological empowerment interventions has been developed for children and adults who have experienced violence and related forms of complex trauma (Courtois et al., 2009; Ford and Cloitre, 2009). As summarized
by Courtois and colleagues, psychological empowerment interventions are built upon the following two central philosophical foundations:
- Recognizing the uniqueness of the individual. The model is organized around recognition of the primacy and uniqueness of the individual and the maintenance of his/her welfare. Treatment is not one-size-fits-all; rather, each client is assessed, and treatment is planned differentially according to the specific needs of the individual. This is a phenomenological approach…. A “whole person” philosophy prevails: Although symptoms, deficits, and distress are reasons for seeking treatment and generally become the targets for intervention, the individual’s strengths, resources, resilience, personalized needs, values, and contexts are identified and reinforced.
- Personal empowerment. A strengths- and resilience-based philosophy of personal empowerment and self-determination encourages the therapist to seek to understand the individual’s unique phenomenological experience and its specific meaning and its relationship to symptoms, distress, and treatment goals. The individual has authority over the meaning and interpretation of his/her personal life history, current needs and preferences, and goals for the future. The therapist functions as an active, empathic, and responsive listener and a guide to enable the client to openly voice, examine, and therapeutically work through feelings of confusion, shame, or other emotions that have been suppressed or forbidden. The therapist seeks to create relational conditions where the client is emotionally validated and is “seen” and appreciated, to counter the invalidiation experiences typically associated with attachment trauma and subsequent victimization and to encourage emotional expression and development. The therapist strives to create conditions within the treatment that are as egalitarian as possible and that encourage collaboration with and empowerment of the client; however, the responsibilities and inherent power differences in the treatment relationship are explicitly acknowledged. The therapist seeks to use power effectively on the individual’s behalf while simultaneously encouraging the client’s development and autonomy. Importantly, the therapist conveys an openness to the client’s questioning of authority (including that of the therapist) and supports the client’s ultimate authority over his/her life, memories, and therapeutic engagement and progress. Moreover, the therapist is careful to maintain appropriate boundaries and limitations and is responsible for avoiding dual relationships and situations in which the client might be subject to pressure, coercion, or exploitation intentionally or inadvertently by the therapist. Treatment should be based in a shared plan that is systematic (not laissez-faire), utilizes effective strategies … organized around a careful assessment and a planned sequence of interventions that are hierarchically ordered and sequenced (86-87; italics in original).
A recent meta-analysis of therapy outcome studies with adult survivors of childhood sexual abuse found that cognitive behavior therapy was superior to other modalities for anxiety, depression, and other internalizing problems but not for problems more specifically related to emotion dysregulation (e.g., externalizing or interpersonal problems) (Taylor and Harvey, 2010). Thus, some violence survivors, particularly those with extensive victimization histories, may respond best to therapy focused on enhancing emotion regulation. Survivors who have severe difficulties with emotion regulation and their therapists also may prefer not to engage in trauma memory processing or to not do so until the client has acquired emotion regulation skills (Cook et al., 2004; Cloitre et al., 2010). Three manualized psychosocial intervention models that do not include trauma memory processing have been designed to enhance skills for emotion regulation, anxiety management, and interpersonal functioning. Skills Training for Emotion and Interpersonal Regulation (STAIR) has shown promise in reducing PTSD and depression symptoms and in enhancing emotion regulation with women survivors of violence (Cloitre et al., 2010). Seeking Safety has shown promise in reducing PTSD and substance use problems with girls and women (Najavits et al., 2006; Zlotnick et al., 2009). Although STAIR and Seeking Safety address emotion regulation, they emphasize becoming more assertively aware and expressive of emotions as a way to overcome excessively negative emotion states and dysfunctional avoidance of trauma memories or reminders of those memories.
Trauma Affect Regulation: Guide for Education and Therapy (TARGET) acknowledges the extreme emotional distress (e.g., depression, anxiety, anger, guilt, shame, and grief) or emotionally numbed and shutdown feelings (e.g., dissociation) that violence survivors often suffer (Ford and Russo, 2006). However, these PTSD or trauma-related “symptoms” are currently viewed as adaptive, rather than maladaptive or dysfunctional, reactions which reflect a change in the stress response system in the body that is protective of the individual. TARGET teaches a single sequential skill set described by the mnemonic FREEDOM, designed based on research showing that emotion regulation involves recognizing, modulating, and recovering from negative emotion states as well as accessing and sustaining positive emotion states (Eisner et al., 2009; Kessler and Staudinger, 2009). Restoring affect regulation is described as requiring seven practical steps or skills denoted by FREEDOM: Focusing the mind on one thought at a time; Recognizing current triggers for emotional reactions; distinguishing dysregulated (“reactive”) versus adaptive (“main”) Emotions; Evaluations (thoughts); goal Definitions; behavioral Options; and self-statements affirming that taking responsibility for recovering from intense emotions is crucial not only to one’s own personal well-being but also to Making a positive contribution to primary relationships (e.g., as a parent) and the community.
TARGET has been evaluated in a series of real-world effectiveness studies as a group therapy for women and men in substance abuse treatment as well as for incarcerated women, as a one-to-one therapy for low-income women with complex trauma histories and girls involved in delinquency, and as a combined group and milieu intervention for girls and boys placed in juvenile detention centers (Frisman et al., 2008, Ford et al., in press-b, in preparation; Ford and Hawke, in review). Group and milieu interventions enable participants to provide one another with peer modeling, support, and guidance as well as potentially enabling the program or community in which they take place to become “trauma informed” (Fallot and Harris, 2008). Consistent with this view, TARGET was found to enable women and men recovering from substance abuse to maintain a sense of realistic confidence and optimism (“sobriety self-efficacy”), where others who received substance abuse treatment as usual showed a marked decline in this important resilience factor (Frisman et al., 2008). The benefits to the entire setting were evident in findings from the evaluation of TARGET in youth detention centers, in which every session of TARGET received by a girl or boy was associated with a reduction in the number of behavioral incidents and punitive sanctions imposed by staff during the first two weeks of youths’ stay in the facilities (Ford and Hawke, in review). On the other hand, many girls or women who have experienced violence may prefer the privacy of a one-to-one therapy intervention, and TARGET showed evidence of helping both underserved women and girls to not only reduce their PTSD symptoms but also to increase their ability to regulate emotions (Ford et al., in press-a, in press-b).
Implications of a Psychological Empowerment
Approach for Violence Survivors
To the extent that knowledge is power, providing women and children who have experienced violence with de-stigmatizing explanations of why they are struggling with persistent emotional distress and how they can draw upon their inherent personal strengths to regain their emotional balance is a very direct and essential form of psychological empowerment. Equally, if not more, important is bringing this same knowledge to the many professionals, advocates, policy makers, funders, jurists, and regulators who determine how scarce societal resources will be allocated both to prevent violence and to restore the lives and well-being of survivors of violence. If violence changes how survivors’ bodies respond to subsequent stressors (non-violent as well as violent), then traumatic stress disorders such as PTSD and its more complex variants are simply extreme versions of the out-of-balance emotional states that everyone experiences. Therefore, if recovery from the aftereffects of violence involves regaining or restoring
innate capacities for re-setting the body’s stress reaction systems—and, in so doing, regaining or restoring the innate ability to regulate emotions and maintain a generally healthy balanced emotional state despite expectable perturbations—it is essential that not only violence survivors but also the public at large (including those key determiners and providers of services) are informed about why and how emotion regulation is essential not only for survivors of violence but also on a larger scale to prevent violence. With this perspective, it becomes possible to understand not only the aftereffects of violence but also violence itself as resulting at least in part from emotion dysregulation on a broad scale (e.g., uncivil discourse in politics or extreme economic and social disparities). Knowledge and skills regarding emotion regulation are essential not just for violence survivors, but for everyone.
REFERENCES
Adegoke, T. G., and D. Oladeji. 2008. Community norms and cultural attitudes and beliefs factors influencing violence against women of reproductive age in Nigeria. European Journal of Scientific Research 20:265-273.
Adi, Y., A. Killoran, K. Janmohamed, and S. Stewart-Brown. 2007. Systematic review of the effectiveness of interventions to promote mental wellbeing in children in primary education. Report 1: Universal approaches: non-violence related outcomes. London: National Institute for Health and Clinical Excellence.
Ahmed, S. M. 2005. Intimate partner violence against women: Experiences from a woman-focused development programme in Matlab, Bangladesh. Journal of Health, Population and Nutrition 23(1):95-101.
Amaro, H. 2011. The Boston Consortium Model: Treatment of trauma among women with substance use disorders. Paper presented at Workshop on Preventing Violence against Women and Children, Institute of Medicine, Washington, DC. January 28.
Amoakohene, M. I. 2004. Violence against women in Ghana: A look at women’s perceptions and review of policy and social responses. Social Science and Medicine 59:2373-2385.
Anderson, L. A., and S. C. Whiston. 2005. Sexual assault education programs: A meta-analytic examination of their effectiveness. Psychology of Women Quarterly 29:374-388.
Anderson, P., D. Chisholm, and D. C. Fuhr. 2009. Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. The Lancet 373(9682):2234-2246.
APA (American Psychiatric Association). 1997. Diagnostic and statistical manual of mental disorders (DSM), fourth edition. Washington, DC: American Psychiatric Association.
APA. 2004. Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Washington, DC: American Psychiatric Association.
Australian Centre for Posttraumatic Mental Health. 2007. Australian guidelines for the treatment of adults with acute stress disorder and posttraumatic stress disorder. Melbourne, Australia: Australian Centre for Posttraumatic Mental Health.
Bacon, H., and S. Richardson. 2001. Attachment theory and child abuse: An overview of the literature for practitioners. Child Abuse Review 10:377-397.
Bair-Merritt, M. H., J. M. Jennings, R. Chen, L. Burrell, E. MacFarlane, L. Fuddy, and A. K. Duggan. 2010. Reducing maternal intimate partner violence after the birth of a child: A randomized controlled trial of the Hawaii Healthy Start home visitation program. Archives of Pediatrics & Adolescent Medicine 164(1):16-23.
Baldry, A. C., and D. P. Farrington. 2007. Effectiveness of programs to prevent school bullying. Victims and Offenders 2(2):183-204.
Bandura, A. 1977. Social learning theory. Englewood Cliffs, NJ: Prentice Hall.
Bandura, A. 1986. Social foundations of thought and action: A social cognitive theory. Upper Saddle River, NJ: Prentice Hall.
Barker, G., C. Ricardo, and M. Nascimento. 2007. Engaging men and boys in changing gender based inequity in health: Evidence from programme interventions. Geneva, Switzerland: World Health Organization.
Basile, K. C., M. F. Hertz, and S. E. Back. 2009. Intimate partner violence and sexual violence victimization assessment instruments for use in healthcare settings: Version 1. Atlanta, GA: Centers for Disease Control and Prevention.
Bilukha, O., R. A. Hahn, A. Crosby, M. T. Fullilove, A. Liberman, E. Moscicki, S. Snyder, F. Tuma, P. Corso, A. Schofield, P. A. Briss, and Task Force on Community Preventive Services. 2005. The effectiveness of early childhood home visitation in preventing violence: A systematic review. American Journal of Preventive Medicine 28:11-39.
Bloom, S., and B. Farragher. 2010. Destroying sanctuary: The crisis in human service delivery systems. New York: Oxford University Press.
Bowlby, J. 1980. Attachment and loss. New York: Basic.
Bowlby, J. 1990. A secure base: Parent-child attachment and healthy human development. London: Routledge.
Breitenbecher, K. H., and C. A. Gidycz. 1998. Empirical evaluation of a program designed to reduce the risk of multiple sexual victimization. Journal of Interpersonal Violence 13:472-488.
Breitenbecher, K. H., and M. Scarce. 2001. An evaluation of the effectiveness of a sexual assault education program focusing on psychological barriers to resistance. Journal of Interpersonal Violence 16:387-407.
Briggs-Gowan, M. J., J. D. Ford, L. Fraleigh, K. McCarthy, and A. S. Carter. 2010. Prevalence of exposure to potentially traumatic events in a healthy birth cohort of very young children in the northeastern United States. Journal of Traumatic Stress 23(6):725-733.
Bruce, S. 2002. The “A Man” campaign: Marketing social norms to men to prevent sexual assualt. The Report on Social Norms, Working paper, No. 5. Little Falls, NJ: PaperClip Communications.
Campbell, J. C. 2005. Assessing dangerousness in domestic violence cases: History, challenges, and opportunities. Criminology & Public Policy 4:653-672.
Chaffin, M., J. F. Silovsky, B. Funderburk, L. A. Valle, E. V. Brestan, T. Balachova, S. Jackson, J. Lensgraf, and B. L. Bonner. 2004. Parent–child interaction therapy with physically abusive parents: Efficacy for reducing future abuse reports. Journal of Consulting and Clinical Psychology 72(3):500-510.
Chaloupka, F. J., M. Grossman, and H. Saffer. 2002. The effects of price on alcohol consumption and alcohol-related problems. Alcohol Research and Health 26(1):22-34.
Champion, H. L., and R. H. Durant. 2001. Exposure to violence and victimization and the use of violence by adolescents in the United States. Minerva Pediatrics 53:189-197.
Cloitre, M., K. C. Stovall-McClough, K. Nooner, P. Zorbas, S. Cherry, C. L. Jackson, W. Gan, and E. Petkova. 2010. Treatment for PTSD related to childhood abuse: A randomized controlled trial. American Journal of Psychiatry 167(8):915-924.
Cocozza, J. J., E. W. Jackson, K. Hennigan, J. P. Morrissey, B. G. Reed, R. D. Fallot, and S. Banks. 2005. Outcomes for women with co-occurring disorders and trauma: Program-level effects. Journal of Substance Abuse Treatment 28(2):109-119.
Cook, J. M., P. P. Schnurr, and E. B. Foa. 2004. Bridging the gap between posttraumatic stress disorder research and clinical practice. Psychotherapy: Theory, Research, Practice, Training 41:374-387.
Courtois, C. A., J. D. Ford, and M. Cloitre. 2009. Best practices in psychotherapy for adults. In C. A. Courtois and J. D. Ford, eds., Treating complex traumatic stress disorders: An evidence-based guide (pp. 82-103). New York: Guilford Press.
Covington, S. 2003. Beyond trauma: A healing journey for women. City Center, MN: Hazelden.
Covington, S. 2007. Women and addiction: A gender-responsive approach. Clinical innovators series. City Center, MN: Hazelden.
CREST. 2003. The management of post traumatic stress disorder in adults. Belfast, Ireland: Clinical Resource Efficiency Support Team.
Crooks, C. V. 2011. Cycles of violence. Paper presented at Workshop on Preventing Violence Against Women and Children, Institute of Medicine, Washington, DC. January 28.
Crooks, C. V., K. L. Scott, D. A. Wolfe, D. Chiodo, and S. Killip. 2007. Understanding the link between childhood maltreatment and violent delinquency: What do schools have to add? Child Maltreatment 12(3):269-280.
Dahlberg, L. L., and A. Butchart. 2005. State of the science: Violence prevention efforts in developing and developed countries. International Journal of Injury Control and Safety Promotion 12(2):93-104.
Dias, M. A., K. Smith, K. deGuehery, P. Mazur, V. Li, and M. L. Shaffer. 2005. Preventing abusive head trauma among infants and young children: A hospital-based, parent education program. Pediatrics 115:e470-477.
Dodge, K. A., J. D. Coie, G. S. Pettit, and J. M. Price. 1990. Peer status and aggression in boys’ groups: Developmental and contextual analyses. Child Development 61(5):1289-1309.
Dodge, K. A., G. S. Pettit, and J. E. Bates. 1994. Effects of physical maltreatment on the development of peer relations. Development and Psychopathology 6:43-55.
Douglas, M. 1998. Restriction of the hours of sale of alcohol in a small community: A beneficial impact. Australian and New Zealand Journal of Public Health 22:714-719.
Du Mont, J., and D. Parnis. 2000. Sexual assault and legal resolution: Querying the medical collection of forensic evidence. Medicine and Law 19:779-792.
Duailibi, S., W. Ponicki, J. Grube, I. Pinsky, R. Laranjeira, and M. Raw. 2007. The effect of restricting opening hours on alcohol-related violence. American Journal of Public Health 97:2276-2280.
Dusenbury, L., M. Falco, A. Lake, R. Brannigan, and K. Bosworth. 1997. Nine critical elements of promising violence prevention programs. Journal of School Health 67:409-414.
Eckenrode, J., B. Ganzel, C. R. Henderson, Jr., E. Smith, D. L. Olds, J. Powers, R. Cole, H. Kitzman, and K. Sidora. 2000. Preventing child abuse and neglect with a program of nurse home visitation: The limiting effects of domestic violence. JAMA 284(11):1385-1391.
Ehrensaft, M. K., P. Cohen, J. Brown, E. Smailes, H. Chen, and J. G. Johnson. 2001. Intergenerational transmission of partner violence: A 20-year prospective study. Journal of Consulting and Clinical Psychology 71:741-753.
Eisner, L. R., S. L. Johnson, and C. S. Carver. 2009. Positive affect regulation in anxiety disorders. Journal of Anxiety Disorders 23(5):645-649.
Ellsberg, M., J. Liljestrand, and A. Winkwist. 1997. The Nicaraguan Network of Women Against Violence: Using research and action for change. Reproductive Health Matters, 5(10):82-92.
Fabiano, P., H. W. Perkins, A. Berkowitz, J. Linkenbach, and C. Stark. 2003. Engaging men as social justice allies in ending violence against women: Evidence for a social norms approach. Journal of American College Health 52:105-112.
Fagan, J., and A. Browne. 1994. Violence between spouses and intimates: Physical aggression between women and men in intimate relationships. In A. J. Reiss, Jr., and J. A. Roth, eds. Understanding and preventing violence, Volume 3: Social Influences (pp. 115-292). Washington, DC: National Academy Press.
Fallot, R. D., and M. Harris. 2008. Trauma-informed services. In G. Reyes, J. D. Elhai and J. D. Ford, eds. The Encyclopedia of Psychological Trauma. Hoboken, NJ: John Wiley.
Fallot, R. D., and M. Harris. 2009. Creating cultures of trauma-informed care: A self-assessment and planning protocol. Washington, DC: Community Connections.
Farkas, M., C. Gagne, W. Anthony, and J. Chamberlin. 2005. Implementing recovery oriented evidence based programs: Identifying the critical dimensions. Community Mental Health Journal 41(2):141-158.
Farrington, D. P., and M. M. Ttofi. 2009. School-based programs to reduce bullying and victimization. Campbell Systematic Reviews. Oslo, Norway: Campbell Collaboration.
Finkelhor, D. 2009. The prevention of childhood sexual abuse. The Future of Children 19(2):169-194.
Finkelhor, D., N. Asdigian, and J. Dziuba-Leatherman. 1995. The effectiveness of victimization prevention instruction: An evaluation of children’s responses to actual threats and assaults. Child Abuse and Neglect 19:141-153.
Finkelhor, D., R. K. Ormrod, and H. A. Turner. 2009. Lifetime assessment of poly-victimization in a national sample of children and youth. Child Abuse and Neglect 33(7):403-411.
Finnish Foundation for Alcohol Studies. 2003. Alcohol in developing societies: A public health approach. Helsinki and Geneva: Finnish Foundation for Alcohol Studies and World Health Organization.
Fisher, G. J. 1986. College student attitudes toward forcible date rape: Changes after taking a human sexuality course. Journal of Sex Education and Therapy 12:42-46.
Foa, E. B., T. Keane, M. J. Friedman, and J. A. Cohen, eds. 2009. Effective treatments for PTSD, 2nd ed. New York: Guilford.
Fontaine, R. G. 2010. New developments in developmental research on social information processing and antisocial behavior. Journal of Abnormal Child Psychology 38(5):569-573.
Forbes, D., M. Creamer, J. I. Bisson, J. A. Cohen, B. E. Crow, E. B. Foa, M. J. Friedman, T. M. Keane, H. S. Kudler, and R. J. Ursano. 2010. A guide to guidelines for the treatment of PTSD and related conditions. Journal of Traumatic Stress 23(5):537-552.
Ford, J. D. 2005. Treatment implications of altered neurobiology, emotion regulation and information processing following child maltreatment. Psychiatric Annals 35:410-419.
Ford, J. D., and M. Cloitre. 2009. Best practices in psychotherapy for children and adolescents. In C. Courtois and J. D. Ford, eds., Treating complex traumatic stress disorders: An evidence-based guide (pp. 59-81). New York: Guilford.
Ford, J. D., D. F. Connor, and J. Hawke. 2009. Complex trauma among psychiatrically impaired children: A cross-sectional, chart-review study. Journal of Clinical Psychiatry 70(8):1155-1163.
Ford, J. D., J. D. Elhai, D. F. Connor, and B. C. Frueh. 2010. Poly-victimization and risk of posttraumatic, depressive, and substance use disorders and involvement in delinquency in a national sample of adolescents. Journal of Adolescent Health 46(6):545-552.
Ford, J. D., J. K. Hartman, J. Hawke, and J. Chapman. 2008. Traumatic victimization, posttraumatic stress disorder, suicidal ideation, and substance abuse risk among juvenile justice-involved youths. Journal of Child and Adolescent Trauma 1:75-92.
Ford, J. D., and J. Hawke. In review. Trauma emotion regulation psychoeducation group attendance is associated with reduced disciplinary incidents and sanctions in juvenile detention facilities. Journal of Child and Adolescent Trauma.
Ford, J. D., and E. Russo. 2006. Trauma-focused, present-centered, emotional self-regulation approach to integrated treatment for posttraumatic stress and addiction: Trauma Adaptive Recovery Group Education and Therapy (TARGET). American Journal of Psychotherapy 60(4):335-355.
Ford, J. D., K. Steinberg, J. Hawke, J. Levine, and W. Zhang. In press-a. Evaluation of trauma emotion regulation—Guide for education and therapy (TARGET) with traumatized girls involved in delinquency. Journal of Clinical Child and Adolescent Psychology.
Ford, J. D., K. Steinberg, and W. Zhang. In press-b. Emotion regulation and social problem-solving psychotherapies for high-risk mothers with PTSD. Behavior Therapy.
Foshee, V. A., G. F. Linder, K. E. Bauman, S. A. Langwick, X. B. Arriaga, J. L. Health, P. M. McMahon, and S. Bangdiwala. 1996. The Safe Dates project: Theoretical basis, evaluation design, and selected baseline findings. American Journal of Preventive Medicine 12(5):39-47.
Foshee, V. A., K. E. Bauman, X. B. Arriaga, R. W. Helms, G. G. Koch, and G. F. Linder. 1998. An evaluation of Safe Dates, an adolescent dating violence prevention program. American Journal of Public Health 88(1):45-50.
Foshee, V. A., K. E. Bauman, W. F. Greene, G. G. Koch, G. F. Linder, and J. E. MacDougall. 2000. The Safe Dates program: 1-year follow-up results. American Journal of Public Health 90(10):1619-1622.
Foshee, V. A., K. E. Bauman, S. T. Ennett, G. F. Linder, T. Benefield, and C. Suchindran. 2004. Assessing the long-term effects of the Safe Dates program and a booster in preventing and reducing adolescent dating violence victimization and perpetration. American Journal of Public Health 94(4):619-624.
Foshee, V. A., K. E. Bauman, S. T. Ennett, C. Suchindran, T. Benefield, and G. F. Linder. 2005. Assessing the effects of the dating violence prevention program “Safe Dates” using random coefficient regression modeling. Prevention Science 6:245-258.
Foshee, V. A., K. J. Karriker–Jaffe, H. L. Reyes, S. T. Ennett, C. Suchindran, K. E. Bauman, and T. Benefield. 2008. What accounts for demographic differences in trajectories of adolescent dating violence? An examination of intrapersonal and contextual mediators. Journal of Adolescent Health 42(6):596-604.
Foshee, V. A., M. L. Reyes, and S. Wyckoff. 2009. Approaches to preventing psychological, physical, and sexual partner abuse. In D. O’Leary and E. Woodin, eds., Psychological and physical aggression in couples: Causes and interventions (pp. 165-190). Washington, DC: American Psychological Association.
Fox A. M., S. S. Jackson, N. B. Hansen, N. Gasa, M. Crewe, and K. J. Sikkema. 2007. In their own voices: A qualitative study of women’s risk for intimate partner violence and HIV in South Africa. Violence Against Women 13:583-602.
FPH (U.K. Faculty of Public Health). 2008. Alcohol and public health. Faculty of Public Health position statement: U.K. Faculty of Public Health.
Frisman, L., J. D. Ford, H. Lin, S. Mallon, and R. Chang. 2008. Outcomes of trauma treatment using the TARGET model. Journal of Groups in Addiction and Recovery 3:285-303.
Garbarino, J. 1999. Lost boys: Why our sons turn violent and how we can save them. New York: The Free Press.
Garner, J., J. Fagan, and C. Maxwell. 1995. Published findings from the Spouse Assault Replication Program: A critical review. Journal of Quantitative Criminology 11:3-28.
Gibson, L. E., and H. Leitemberg. 2000. Child sexual abuse prevention programs: Do they decrease the occurrence of child sexual abuse? Child Abuse & Neglect 24:1115-1125.
Gill, J. M., G. G. Page, P. Sharps, and J. C. Campbell. 2008. Experiences of traumatic events and associations with PTSD and depression development in urban health care-seeking women. Journal of Urban Health 85(5):693-706.
Go, V. F., S. C. Johnson, M. E. Bentley, S. Sivaram, A. K. Srikrishnan, D. D. Celentano, and S. Solomon. 2003. Crossing the threshold: Engendered definitions of socially acceptable domestic violence in Chennai, India. Culture, Health and Sexuality 5:393-408.
Hahn, R., D. Fuqua-Whitley, H. Wethington, J. Lowy, A. Crosby, M. Fullilove, R. Johnson, A. Liberman, E. Moscicki, L. Price, S. Snyder, F. Tuma, S. Cory, G. Stone, K. Mukhopadhaya, S. Chattopadhyay, and L. Dahlberg. 2007. Effectiveness of universal school-based programs to prevent violent and aggressive behavior: A systematic review. American Journal of Preventive Medicine 33(2 Suppl):S114-S129.
Harris, M. 1998. Trauma recovery and empowerment: A clinician’s guide for working with women in groups. New York: The New Press.
Harris, M., and R. D. Fallot, eds. 2001. Using trauma theory to design service systems. San Francisco: Jossey-Bass.
Heise, L., and C. García-Moreno. 2002. Violence by intimate partners. In E. G. Krug, ed., World report on violence and health (pp. 87-121). Geneva, Switzerland: World Health Organization.
Herman, J. L. 1992. Trauma and recovery. New York: Basic Books.
Herrenkohl, T. I., C. Sousa, E. A. Tajima, R. C. Herrenkohl, and C. A. Moylan. 2008. Intersection of child abuse and children’s exposure to domestic violence. Trauma Violence Abuse 9(2):84-99.
Hussain, R., and A. Khan. 2008. Women’s perceptions and experiences of sexual violence in marital relationships and its effect on reproductive health. Health Care for Women International 29:468-483.
Ilika, A. L. 2005. Women’s perception of partner violence in a rural Igbo community. African Journal of Reproductive Health 9:77-88.
IOM (Institute of Medicine). 2006. Posttraumatic stress disorder: Diagnosis and assessment. Washington, DC: The National Academies Press.
Jaffe, P. G., and M. Juodis. 2006. Children as victims and witnesses of domestic homicide: Lessons learned from domestic violence death review committees. Juvenile and Family Court Journal 57(3):13-28.
Jaffe, P. G., N. K. D. Lemon, and S. E. Poisson. 2003. Child custody and domestic violence: A call for safety and accountability. Thousand Oaks, CA: Sage.
Jennings, A. 1998. On being invisible in the mental health system. In B. L. Levin, A. K. Blanch, and A. Jennings, eds. Women’s mental health services: A public health perspective (pp. 326-347). Thousand Oaks, CA: Sage Publications.
Jewkes, R., M. Nduna, J. Levin, N. Jama, K. Dunkle, A. Puren, and N. Duwury. 2008. Impact of Stepping Stones on incidence of HIV and HSV-2 and sexual behaviour in rural South Africa: Cluster randomised controlled trial. British Medical Journal 337:383-387.
Jewkes, R., P. Sen, and C. García-Moreno. 2002. Sexual violence. In E. G. Krug, ed. World report on violence and health (pp. 149-181). Geneva, Switzerland: World Health Organization.
Kabeer, N. 2001. Conflicts over credit: Re-evaluating the empowerment potential of loans to women in rural Bangladesh. World Development 29(1):63-84.
Katz, J. 2006. The macho paradox: Why some men hurt women and how all men can help. Napierville, IL: Sourcebooks.
Kessler, E. M., and U. M. Staudinger. 2009. Affective experience in adulthood and old age: The role of affective arousal and perceived affect regulation. Psychology and Aging 24(2):349-362.
Kim, J. C., G. Ferrari, T. Abramsky, C. H. Watts, J. R. Hargreaves, L. A. Morison, G. Phetla, J. D. H. Porter, and P. Pronyk. 2009. Assessing the incremental benefits of combining health and economic interventions: Experience from the IMAGE study in rural South Africa. Bulletin of the World Health Organization 87:824-832.
Knox K. L., D. A. Litts, G. W. Talcott, J. C. Feig, and E. D. Caine. 2003. Risk of suicide and related adverse outcomes after exposure to a suicide prevention programme in the US Air Force: Cohort study. British Medical Journal 327:1376-1381.
Koenig, M. A., A. Saifuddin, H. Mian Bazle, and A. B. M. Khorshed-Alam-Mozumder. 2003. Women’s status and domestic violence in rural Bangladesh: Individual- and community-level effects. Demography 40(2):269-288.
Lankester, T. 1992. Setting up community health programmes: A practical manual for use in developing countries. London: Macmillan Press.
Laranjeira, R., and D. Hinkly. 2002. Evaluation of alcohol outlet density and its relation with violence. Revista de Saude Publica 36(4):455-461.
Liu, M., and C. Chan. 1999. Enduring violence and staying in marriage: Stories of battered women in rural China. Violence Against Women 5:1469-1492.
Lösel, F., and A. Beelmann. 2003. Effects of child skills training in preventing antisocial behaviour: A systematic review of randomized evaluations. Annals of the American Academy of Political and Social Science 587:84-109.
Macmillan, H. L., C. N. Wathen, J. Barlow, D. M. Fergusson, J. M. Leventhal, and H. N. Taussig. 2009. Interventions to prevent child maltreatment and associated impairment. Lancet 373(9659):250-266.
Markowitz, S. 2000. The price of alcohol, wife abuse, and husband abuse. Southern Economic Journal 67:279-303.
Meltzer, H., R. Gatward, T. Corbin, R. Goodman, and T. Ford. 2003. Persistence, onset, risk factors and outcomes of childhood mental disorders. London: Office for National Statistics, HMSO.
Mikton, C., and A. Butchart. 2009. Child maltreatment prevention: A systematic review of reviews. Bulletin of the World Health Organization 87(5):353-361.
Mitra, A., and P. Singh. 2007. Human capital attainment and gender empowerment: The Kerala paradox. Social Science Quarterly 88:1227-1242.
Mongillo, E. A., M. Briggs-Gowan, J. D. Ford, and A. S. Carter. 2009. Impact of traumatic life events in a community sample of toddlers. Journal of Abnormal Child Psychology 37(4):455-468.
Morrison, A., M. Ellsberg, and S. Bott. 2004. Addressing gender-based violence in the Latin American and Caribbean region: A critical review of interventions. Washington, DC: World Bank Policy Research.
Morrissey, J. P., E. W. Jackson, A. R. Ellis, H. Amaro, V. B. Brown, and L. M. Najavits. 2005. Twelve-month outcomes of trauma-informed interventions for women with co-occurring disorders. Psychiatric Services 56(10):1213-1222.
Mueser, K. T., S. D. Rosenberg, H. Xie, M. K. Jankowski, E. E. Bolton, W. Lu, J. L. Hamblen, H. J. Rosenberg, G. J. McHugo, and R. Wolfe. 2008. A randomized controlled trial of cognitive-behavioral treatment for posttraumatic stress disorder in severe mental illness. Journal of Consulting and Clinical Psychology 76(2):259-271.
Najavits, L. M. 2002. Seeking safety: A treatment manual for PTSD and substance abuse. New York: Guilford Press.
Najavits, L. M., R. J. Gallop, and R. D. Weiss. 2006. Seeking safety therapy for adolescent girls with PTSD and substance use disorder: A randomized controlled trial. Jounal of Behavioral Health Services and Research 33(4):453-463.
National Collaborating Centre for Mental Health. 2007. Antenatal and postnatal mental health. NICE Clinical Guideline No 45. London: National Institute for Clinical Excellence.
NICE (National Institute for Clinical Excellence.). 2005. Posttraumatic stress disorder (PTSD): The management of PTSD in adults and children in primary and secondary care. London, UK: National Institute for Clinical Excellence.
Oliver, J. E. 1993. Intergenerational transmission of child abuse: Rates, research, and clinical implications. American Journal of Psychiatry 150(9):1315-1324.
Paine, K., G. Hart, M. Jawo, S. Ceesay, M. Jallow, L. Morison, G. Walraven, K. McAdam, and M. Shaw. 2002. Before we were sleeping, now we are awake: Preliminary evaluation of the Stepping Stones sexual health programme in the Gambia. African Journal of AIDS Research 1(1):39-40.
Petersen, I., A. Bhana, and M. McKay. 2005. Sexual violence and youth in South Africa: The need for community based prevention interventions. Child Abuse & Neglect 29:1233-1248.
Powers, M. B., J. M. Halpern, M. P. Ferenschak, S. J. Gillihan, and E. B. Foa. 2010. A meta-analytic review of prolonged exposure for posttraumatic stress disorder. Clinical Psychology Review 30(6):635-641.
Prinz, R. J., M. R. Sanders, C. J. Shapiro, D. J. Whitaker, and J. R. Lutzker. 2009. Population-based prevention of child maltreatment: The U.S. Triple P system population trial. Prevention Science 10(1):1-12.
Rahman, A. 1999. Women and microcredit in rural Bangladesh: Anthropological study of the rhetoric and realities of Grameen Bank lending. Boulder, CO: Westview Press.
Rayburn, N. R., S. L. Wenzel, M. N. Elliott, K. Hambarsoomians, G. N. Marshall, and J. S. Tucker. 2005. Trauma, depression, coping, and mental health service seeking among impoverished women. Journal of Consulting and Clinical Psychology 73(4):667-677.
Resick, P. A., T. E. Galovski, M. O’Brien Uhlmansiek, C. D. Scher, G. A. Clum, and Y. Young-Xu. 2008. A randomized clinical trial to dismantle components of cognitive processing therapy for posttraumatic stress disorder in female victims of interpersonal violence. Journal of Consulting and Clinical Psychology 76(2):243-258.
Rhyne, E. 2001. Mainstreaming microfinance: How lending to the poor began, grew, and came of age in Bolivia. Green Haven, CT: Kumarian Press.
Robins, C. S., J. A. Sauvageot, K. J. Cusack, S. Suffoletta-Maierle, and B. C. Frueh. 2005. Consumers’ perceptions of negative experiences and “sanctuary harm” in psychiatric settings. Psychiatric Services 56(9):1134-1138.
Schecter, S., and J. Edleson. 1999. Effective intervention in domestic violence and child maltreatment cases: Guidelines for policy and practice. Reno, NV: National Council of Juvenile and Family Court Judges.
Schewe, P. A. 2007. Interventions to prevent sexual violence. In L. Doll, ed. Handbook of injury and violence prevention (pp. 183-201). New York: Springer.
Schopper, D., J.-D. Lormand, and R. Waxweiler. 2006. Developing policies to prevent injuries and violence: Guidelines for policy-makers and planners. Geneva, Switzerland: World Health Organization.
Schuler, S. R., S. M. Hashemi, A. P. Riley, and S. Akhter. 1996. Credit programs, patriarchy and men’s violence against women in rural Bangladesh. Social Science and Medicine 43(12):1729-1742.
Schumm, J. A., M. Briggs-Phillips, and S. E. Hobfoll. 2006. Cumulative interpersonal traumas and social support as risk and resiliency factors in predicting PTSD and depression among inner-city women. Journal of Traumatic Stress 19(6):825-836.
Scott, K. L., and C. V. Crooks. 2004. Effecting change in maltreating fathers: Critical principles for intervention planning. Clinical Psychology: Science and Practice 11:95-111.
Seng, J., W. D’Andrea, and J. D. Ford. In review. Psychological trauma history and empirically derived psychiatric syndromes in a community sample of women in prenatal care. Psychological Trauma.
Sheehan, D. 2008. Alcohol, health and wider social impact. SE Regional Public Health Group Information Series No. 1. London: Department of Health.
Skowron, E. A., and D. H. S. Reinemann. 2005. Psychological interventions for child maltreatment: A meta-analysis. Psychotherapy: Theory, Research, Practice, and Training 42:52-71.
Slovak, K., C. Carlson, and L. Helm. 2007. The influence of family violence on youth attitudes. Child and Adolescent Social Work Journal 24:77-99.
Smith, J. D., B. H. Schneider, P. K. Smith, and K. Ananiadou. 2004. The effectiveness of whole-school antibullying programs: A synthesis of evaluation research. School Psychology Review 33:548-561.
Smith, P. H., J. W. White, and L. J. Holland. 2003. A longitudinal perspective on dating violence among adolescent and college-age women. American Journal of Public Health 93(7):1104-1109.
Solórzano, I., H. Abaunza, and C. Molina. 2000. Evaluación de impacto de la campaña contra las mujeres un desastre que los hombres si podemos evitar [impact evaluation of the campaign violence against women: A disaster we can prevent as men]. Managua: CANTERA.
Sousa, C., T. I. Herrenkohl, C. A. Moylan, E. A. Tajima, J. B. Klika, R. C. Herrenkohl, and M. J. Russo. 2011. Longitudinal study on the effects of child abuse and children’s exposure to domestic violence, parent-child attachments, and antisocial behavior in adolescence. Journal of Interpersonal Violence 26(1):111-136.
Stuart, G. L., S. E. Ramsey, T. M. Moore, C. W. Kahler, L. E. Farrell, P. R. Recupero, and R. A. Brown. 2003. Reductions in marital violence following treatment for alcohol dependence. Journal of Interpersonal Violence 18:1113-1131.
Taylor, J. E., and S. T. Harvey. 2010. A meta-analysis of the effects of psychotherapy with adults sexually abused in childhood. Clinical Psychology Review 30(6):749-767.
Usdin, S., E. Scheepers, S. Goldstein, and G. Japhet. 2005. Achieving social change on gender-based violence: A report on the impact evaluation of Soul City’s fourth series. Social Science and Medicine 61(11):2434-2445.
VA (U.S. Department of Veterans Affairs). 2004. Management of posttraumatic stress. Washington, DC: Department of Veterans Affairs.
van der Kolk, B. A., and M. S. Greenberg. 1987. The psychobiology of the trauma response: Hyperarousal, constriction, and addition to traumatic reexposure. In B. A. van der Kolk, ed. Psychological trauma (pp. 63-87). Arlington, VA: American Psychiatric Publishing.
van Lier, P., F. Vitaro, E. Barker, H. Koot, and R. Tremblay. 2009. Developmental links between trajectories of physical violence, vandalism, theft, and alcohol-drug use from childhood to adolescence. Journal of Abnormal Child Psychology 37(4):481-492.
Welbourn, A. 2009. Stepping Stones—List of surveys and reports to 2006 and some quotes from Stepping Stones users around the world. Some brief notes prepared for the UNAIDS pre-think tank meeting on Evaluation Strategies for Prevention Interventions, Geneva. Available at http://www.steppingstonesfeedback.org/resources/22/Welbourn_Quotes_UNAIDS_Presentation_2009.pdf (accessed April 29, 2011).
Welsh, P. 1997. Hacia una masculinidad sin violencia en las relaciones de pareja [toward masculinity without partner violence]. Managua: CANTERA.
Whitaker, D. J., C. K. Baker, and I. Arias. 2007a. Interventions to prevent intimate partner violence. In L. Doll, ed., Handbook of injury and violence prevention (pp. 203-223). New York: Springer.
Whitaker, D. J., C. K. Baker, C. Pratt, E. Reed, S. Suri, C. Pavlos, B. J. Nagy, and J. Silverman. 2007b. A network model for providing culturally competent services for intimate partner violence and sexual violence. Violence Against Women 13(2):190-209.
Whitaker, D. J., S. Morrison, C. Lindquist, S. R. Hawkins, J. A. O’Neil, and A. M. Nesius. 2006. A critical review of interventions for the primary prevention of perpetration of partner violence. Aggression and Violent Behavior 11(2):151-166.
Whitfield, C. L., R. F. Anda, S. R. Dube, and V. J. Felitti. 2003. Violent childhood experiences and the risk of intimate partners violence in adults: Assessment in a large health maintenance organization. Journal of Interpersonal Violence 18:166-185.
Wolfe, D. A., C. Crooks, P. Jaffe, D. Chiodo, R. Hughes, W. Ellis, L. Stitt, and A. Donner. 2009. A school-based program to prevent adolescent dating violence: A cluster randomized trial. Archives of Paediatrics & Adolescent Medicine 163(8):692-699.
Wolfe, D. A., C. Wekerle, K. Scott, A. L. Straatman, C. Grasley, and D. Reitzel-Jaffe. 2003. Dating violence prevention with at-risk youth: A controlled outcome evaluation. Journal of Consulting and Clinical Psychology 71(2):279-291.
WHO (World Health Organization) and International Society for Prevention of Child Abuse and Neglect. 2006. Preventing child maltreatment: A guide to taking action and generating evidence Geneva, Switzerland: World Health Organization.
WHO and LSHTM (London School of Hygiene and Tropical Medicine). 2010a. The nature, magnitude and consequences of intimate partner and sexual violence. In Preventing intimate partner and sexual violence against women: Taking action and generating evidence. Geneva, Switzerland: World Health Organization.
WHO and LSHTM. 2010b. Preventing intimate partner and sexual violence against women: Taking action and generating evidence. Geneva, Switzerland: World Health Organization.
WHO and LSHTM. 2010c. Risk and protective factors for intimate partner and sexual violence. In Preventing intimate partner and sexual violence against women: Taking action and generating evidence. Geneva, Switzerland: World Health Organization.
Zlotnick, C., J. Johnson, and L. M. Najavits. 2009. Randomized controlled pilot study of cognitive-behavioral therapy in a sample of incarcerated women with substance use disorder and PTSD. Behavior Therapy 40(4):325-336.




































































