
Chronic diseases are common and costly, yet they are also among the most preventable health problems (CDC, 2008). Comprehensive and accurate disease surveillance systems are needed to implement successful efforts to reduce the burden of chronic diseases on the U.S. population. A number of sources of surveillance data—including population surveys, cohort studies, disease registries, administrative health data, and vital statistics—contribute important and critical information about chronic disease. But no organized surveillance system provides the information needed to analyze how chronic disease impacts various U.S. populations by race, ethnicity, and locale; to identify public health priorities; or to track the progress of preventive efforts.
The National Heart, Lung, and Blood Institute of the National Institutes of Health and the Division for Heart Disease and Stroke Prevention of the Centers for Disease Control and Prevention (CDC) asked the Institute of Medicine (IOM) to form a committee that would develop a framework for building a national chronic disease surveillance system. This system would focus primarily on cardiovascular and chronic lung disease and be able to provide data for analysis of race, ethnic, socioeconomic, and geographic region disparities in incidence and prevalence, functional health outcomes, measured risk factors, and clinical care delivery. Questions for the committee to consider included:
- Given what seems to be an existing consensus within the clinical and public health communities that national surveillance should be a high priority, is there a need for a new surveillance system and infrastructure? How might different types of surveillance systems (e.g., standard and sentinel) be included in a national system?
- Might existing surveillance data collection efforts and cohort studies be strengthened or integrated to provide necessary surveillance information?
- How might surveillance efforts include associated conditions, such as chronic lung disease, that contribute to cardiovascular disease and outcomes?
- How could surveillance data be used to enhance research to address health disparities?
- Given that fundamentally different approaches to national surveillance could be implemented, what general comments might be made on the relative efficiencies of an entirely new infrastructure versus one built upon currently existing systems?
- How might local communities participate in the collection and use of data?
- How might various federal, state, and local agencies collaborate in surveillance of cardiovascular and pulmonary disease data collection, determination of research priorities, and development of public policy?
- What degree of validation is needed for cardiovascular disease (CVD) and pulmonary events identified through records systems?
- Are there new initiatives that might be exploited for new national chronic disease surveillance efforts, such as:
a. The Public Health Information Network (http://www.cdc.gov/phin/index.html), including BioSense, a real-time disease detection and monitoring system designed primarily for infectious disease surveillance (http://www.cdc.gov/phin/library/documents/pdf/111759_biosense2.pdf);
b. The National Electronic Disease Surveillance System project to establish a network of interoperable systems for “national integrated surveillance” (http://www.cdc.gov/phin/library/documents/pdf/111759_NEDSS.pdf);
c. The Food and Drug Administration’s (FDA’s) Sentinel System;
d. Local community surveys; or
e. Efforts to increase use of electronic medical records (EMRs) nationally?
10. Can any existing data sources, such as Veterans Administration systems, health maintenance organization networks, or the Department of Defense systems, be used?
11. What can be learned from chronic disease surveillance in other developed countries?
The committee interpreted its charge as entailing a fairly broad approach with a focus on developing the overarching framework and the infrastructure required to create such a framework. While the committee determined it could identify kinds of data necessary for a framework (e.g., behavioral risk factors), identifying the specific data elements and the ways in which those elements are to be measured, collected, and verified is at a much more detailed level of specificity and requires greater resources than those available to the committee.
In considering the extent to which the framework should focus on chronic diseases in general, the committee concluded that the focus, as stated in the charge, should be “primarily on cardiovascular and chronic lung disease.” An enlarged focus on chronic diseases would require an expanded committee, a lengthier study process, and additional resources that were not available. However, the committee resolved to devise a framework and infrastructure that could, to the extent possible, be applicable to other chronic diseases. The committee also recognized the rich history and accomplishments of existing surveillance resources, which can be leveraged in designing a national surveillance framework that would be timely, reliable, and comprehensive for current users of surveillance information.
EXISTING SURVEILLANCE EFFORTS
In health, surveillance systems are constructed to routinely provide information on the scope, magnitude, and cost of a health problem in order to regularly influence priority setting, program development, and evaluation of services or policies. While surveillance has been historically concentrated on notifiable1 conditions or diseases, more recent surveillance efforts have expanded to track chronic diseases (Goodman et al., 2006). But surveillance of these conditions is difficult because of the challenges of disease definition, ascertainment, and differences in access to care, changes in clinical practice, multiple care providers, and lack of perceived threat of disease transmission. Surveillance of chronic conditions is also complicated by the need to provide data from several distinct domains (e.g., environment, income, education, race, ethnicity, and genetics) whose interaction leads to disparities in health and health care. A uniform framework for a nationwide surveillance system for these chronic conditions
____________
1 A notifiable disease is “a disease that, by statutory requirements, must be reported to the public health authority in the pertinent jurisdiction when the diagnosis is made. A disease deemed of sufficient importance to the public health to require that its occurrence be reported to health authorities” (Last, 2001). The Council of State and Territorial Health Epidemiologists works with the CDC to regularly update the list of notifiable diseases.
must also address the challenges that arise from the long-term nature of the risk and conditions, the large number of stakeholders involved in prevention and control, and the many potential objectives to be met.
A number of surveys, registries, cohort studies, administrative data, and vital statistics are used by different stakeholders to gather different kinds of information about these diseases. (See Appendix A for details.) Routine surveys are particularly valuable for obtaining information about prevalence and distribution of chronic diseases as well as about associated risk factors that may contribute to the diseases and their consequences. Major strengths of surveys include the breadth of information they offer and their ability to achieve representation through careful sampling. Such information may be helpful in tracking distributions, changes in rates, and comparisons among subgroups. In-person surveys, although costly, are widely considered to be most inclusive of the population because they select people based on where they are rather than whether they answer their telephone or respond to mail surveys, and because they often have high response rates. A limitation of many surveys is that they rely exclusively on respondent self-reporting to questionnaire items. Surveys are perhaps most valid for measuring many health behaviors, mental health conditions, perceived barriers to accessing health services, and reporting of symptoms.
A registry is one of the most powerful tools employed to record chronic diseases. Disease-specific registries are useful for capturing patient-specific data for individuals with selected conditions. Registries have significant advantages; the most important is that needed data are collected prospectively in the exact format required. Registries allow calculation of incidence rates and, if the cases are followed up regularly, a registry can also provide information on remission, exacerbation, prevalence, and survival. Despite the advantages of using registries for surveillance, they have some inherent limitations. Registries miss patients who visit healthcare providers not participating in the registry as well as individuals who do not receive care. Registries can also suffer bias due to unmeasured confounders and misclassification of patients into a registry. Furthermore, because of the time and effort required to enter data into a registry, clinicians may be reluctant to register patients or collect and record data on busy days, and busier clinicians may be less inclined to participate in registries altogether.
Another approach to surveillance is the cohort study. A cohort study is an epidemiological study which observes a group of individuals over time. The cohort design can be either prospective or retrospective. Retrospective cohort studies are less costly, shorter in duration, and useful for examining prior exposures; however, the resulting information is less complete and accurate than with the prospective approach. In general, the prospective cohort design offers several advantages, including the ability to provide incidence rates, determine a temporal sequence of events (exposure precedes disease), and examine multiple outcomes from the same exposure simultaneously. Additional advantages of the cohort design are the emphasis on systematic data collection and uniformly conducted measurements; however, a major weakness is the potential for differences between study volunteers and the general population. Other disadvantages include subject attrition, inability to produce prevalence data, and relative expense.
Claims data and medical record data obtained from manual chart abstraction or emerging electronic health records (EHRs) are two other sources of information that can be used for surveillance. Claims data can be used to enumerate each person’s encounter or service. They can be collected for hospitalizations, outpatient visits, public program coverage, or private health insurance. Claims data may include sufficiently detailed information to analyze the incidence rate of a chronic condition, the social characteristics of people who receive services for the condition, and the types of services they receive. Claims data may also include geographic identifiers for persons or service providers and may be used to map geographic patterns of the incidence of hospitalizations, other services provided, and healthcare costs, which can be used in analyses of healthcare disparities. Although administrative claims data are useful at the macro level to describe patterns of use and mortality, limitations do exist, including coding errors, limited clinical information, and diagnostic misclassification such as underdiagnosis, overdiagnosis, and misdiagnosis common with cardiovascular and chronic lung diseases.
Data abstracted from medical records and EHRs can provide a detailed record of the history of health services for persons with chronic conditions and can be used to assess quality of care provided to persons with chronic conditions. If they include characteristics of the individual patients, the data also can be used to assess disparities in care. These data can be abstracted for use in registries and for combination into other data sets such as the Healthcare Cost and Utilization Project. However, like registry data, health services data exclude information extraneous to the healthcare delivery system.
Death records are an important source of information on mortality trends and patterns. Death certificate data, which include underlying and contributing causes of death, are compiled at the local and state levels in nearly all states and then shared with the National Center for Health Statistics. However, death certificates have been found to have relatively low sensitivity and specificity compared with medical chart review or autopsy findings. Coronary heart disease, for example, is overreported as a cause of death (Agarwal et al., 2010; Coady et al., 2001; Lloyd-Jones et al., 1998; Sington and Cottrell, 2002), and chronic obstructive pulmonary disease (COPD) is under-reported (Camilli et al., 1991; Mitchell et al., 1971).
Currently, these surveys (some standardized and many non-standardized), registries, cohort studies, health services data, and mortality vital statistics provide an incomplete patchwork of information used by different stakeholders, often with inconsistent findings (Goff et al., 2007; Yeh and Go, 2010).
EMERGING SOURCES OF SURVEILLANCE DATA
Emerging experience with use of health information technologies (HITs) by both patients and providers suggests that, in addition to current sources of surveillance information, there will be expanding and potentially more efficient approaches to generating data for surveillance. Of particular interest is the potential, via the EHR, to economically and completely capture care events and processes and efficiently organize them into robust population- and condition-based registries. The healthcare reform goal of universal coverage, along with broad promotion of HITs (especially the EHR), may markedly increase the value of the medical record for disease surveillance. When an electronic medical record is suitably designed, analyses can be performed without duplicative data generation and handling. EHR data can also be used to generate lists of potential patients for a registry and prospectively register patients or to identify potentially eligible patients during healthcare visits. Challenges to using EHRs for surveillance include (1) a relatively small number of hospitals and practices currently use EHRs; (2) data collected in EHRs may not include the data necessary for effective surveillance; (3) sicker patients are likely to be overrepresented in EHRs due to more visits and more data per visit; (4) inaccurate coding occurs; and (5) patients with significant barriers will likely be underrepresented in EHRs. Despite these difficulties, EHRs have an important role to play in CVD and COPD surveillance, and their growth requires their inclusion when planning for a national surveillance system.
In addition to provider-generated EHR data, the generation and sharing of personal health data by individuals themselves (a trend that has its root in the emergence of the Internet) is a growing health data phenomenon with potential implications for timely, robust, and relevant surveillance. Recording of data by patients in HIT systems is being facilitated by a range of online personal health records. These may be provided by health insurers, integrated delivery systems, commercial providers of health information tools and support, and freestanding personal health records. Timely access to personally relevant information has been a driving force for patients to form, join, and share experiences and data within a range of organizations independent from historically defined public health, healthcare delivery, and health research entities. A new tool that has the potential to modify the future of surveillance and population-based research is the development of registries that integrate social networking, such as those registries currently recruiting in Kentucky2 and Illinois.3 An advantage of registries linked to social networking capabilities is that it creates the potential to follow people easily as they move around the country and even abroad, but their voluntary and non-randomized participation makes generalizing the data obtained from them challenging. Registries linked to social networking sites also produce privacy issues.
LEVELS AND USES OF SURVEILLANCE
Information and knowledge needs vary by perspective, and resources are rarely available to support all needs. Furthermore, the types of information and level of detail required will vary among users of surveillance data. A nationwide surveillance system will, therefore, involve consideration of a range of user groups. Table S-1 provides
____________
2 See https://www.mc.uky.edu/kyhealthregistry/ (accessed August 2, 2011).
3 See https://whr.northwestern.edu/ (accessed August 2, 2011).
TABLE S-1 Levels and Users of Decision Making
| Place and Roles | Place | Type | Who | What | Implementation Levers | Linkage to 2010 Reforms | |||
| Macro |
• Federal • National • Nationwide |
• Business coalitions • Benefit associations • National employer |
• Federal government organizations • Medical society |
Priority setting for
• Regulation • Research and development • Objectives/ targets (e.g., Healthy People 2020) |
• Legislation • Funding institutions (e.g., National Institutes of Health) • Communications |
PPACAa
• Comparative effectiveness • Meaningful use |
|||
| Meso |
• Region • State • County • City • Community |
• Regional/state employer • Small business |
• State board • Medical society • Multispecialty medical group • Hospital medical staff • Public health workers • Local advocates |
• Strategies • Programs and initiatives • Business planning and development • Performance reporting |
• Budgets • Institutions and departments • Communications incentives |
ACOs HIT funding
• Beacon sites • Meaningful use • HIEe Chronic care Prevention |
|||
| Micro |
• Neighborhood • ZIP+4 • Home |
• Schools • “Mom and Pop” |
• Medical practice • Clinician • Family • Individual |
• Interventions • Care and action plans • Outcomes |
• Guidelines • Programs and initiatives • Communications • Payment or coverage |
Insurance reform
• Access • Free prevention services • Payment reform • Pay for performance • ACOs; medical home |
|||
a PPACA = Patient Protection and Affordable Care Act.
b ACO stands for Accountable Care Organization. According to the Medicare Payment Advisory Commission, “The defining characteristic of ACOs is that a set of physicians and hospitals accept joint responsibility for the quality of care and the cost of care received by the ACO’s panel of patients” (MedPac, 2009).
c ARRA = American Recovery and Reinvestment Act of 2009.
d HIT stands for health information technology. ONC is the Office of the National Coordinator for Health Information Technology.
e HIE stands for health information exchange.
examples of different users of surveillance information that can be found at the micro, meso, and macro levels of surveillance.
Surveillance design will require explicit trade-offs in what is included and which user needs are addressed because resources are constrained by time, funding, data accessibility, and acceptability of use. For example, cost constraints may result in sampling rather than assessment of an entire population or force a trade-off between detailed biological examinations versus self-reported information. To protect the confidentiality of individual patient data, sample-size thresholds may be required for reporting. Strategies for improving surveillance will need to balance a number of challenges, including the tension between cost and granularity, and the differing needs of the various user constituencies of data.
CONCLUSIONS AND RECOMMENDATIONS
The committee concluded that a coordinated surveillance system is needed to integrate and expand existing information across the multiple levels of decision making in order to generate actionable, timely knowledge for a range of stakeholders at the local, state or regional, and national levels. The committee further concluded that existing surveillance data collection efforts and cohort studies can and should be strengthened and integrated to provide the basis of the system. Successful implementation of a framework for nationwide surveillance of cardiovascular and chronic lung diseases requires a mechanism to coordinate, monitor, and support the multiple data collection systems that contribute to the surveillance system. Furthermore, the system must provide ways to ensure that the elements collected by the system can evolve along with new knowledge about emerging risk factors, advancing technologies, and new understanding of the basis for disease.
Given that the mission of the Department of Health and Human Services (HHS) is to protect the health of and provide essential health services to Americans,4 that HHS is already responsible for the funding and conduct of numerous surveillance efforts, and that it is in a position to bring together stakeholders from both the public and private sectors as well as those from multiple geographic levels, the committee concluded that HHS is in the best position to lead the development and implementation of the recommended framework and system. Because the recommended framework is based upon existing data collection approaches, it is crucial that those organizations responsible for the conduct of those activities be involved in determining ways to use and integrate existing approaches. The committee believes strongly that federal agencies should collaborate with the many state and local public agencies and the national and state-level nongovernmental organizations that conduct components of the proposed system.
Recommendation 1
The committee recommends that the Secretary of HHS establish and provide adequate resources for a standing national working group to oversee and coordinate cardiovascular and chronic pulmonary disease surveillance activity. This working group should include representatives from HHS (CDC, NIH, AHRQ, CMS, IHS, ONCHIT, FDA), other relevant federal agencies (e.g., VA and DOD), and tribal, state, and local public health agencies, as well as nongovernmental organizations with relevant roles in surveillance.
In a coordinated surveillance system, data are needed that can provide information on incidence and prevalence of relevant conditions over time; behavioral, clinical, and environmental risk factors (e.g., smoking); primary prevention (i.e., elimination of exposures that cause these diseases); secondary prevention efforts (i.e., early detection and intervention); tertiary prevention (i.e., management of symptomatic disease); health outcomes; costs; and, importantly, disparities in these factors by race or ethnicity, geographic region, and socioeconomic status.
Recommendation 2
The committee recommends that HHS place priorities for surveillance on systems that can overtly
- Track progress on nationally recognized goals and indicators regarding cardiovascular disease and chronic pulmonary disease incidence, prevalence, and prevention (e.g., Healthy People);
- Evaluate and inform national, state, and local efforts to control, reduce, and prevent these chronic diseases;
- Enable effective public health actions and policies;
- Improve treatment outcomes;
- Monitor and enhance quality of life; and
- Reduce disparities in risk and burden of these diseases.
____________
4 See http://govinfo.library.unt.edu/npr/library/status/mission/mhhs.htm (accessed August 2, 2011).
Many chronic cardiovascular and lung conditions have common risk factors and follow a broadly similar natural history within patients and populations, which enabled the committee to adapt for its purposes a conceptual framework developed by Wingo and colleagues (2005) for cancer surveillance. In this framework (Figure S-1), the trajectory of chronic disease is integrated with the logic and practices of primary, secondary, and tertiary prevention to provide the core of the framework. The framework organizes data from traditional, evolving, and novel surveillance sources to reflect the development and progression of chronic conditions over a life course. It is critical to collect data on these risk factors in order to identify precursors prior to or at the very earliest states of disease. The design also captures the impact of prevention as both a goal and an interventional intent. Information emerging from this core can be assembled into both cross-cutting and stage-specific metrics to inform the actions of decision makers in multiple roles and at the macro, meso, and micro levels of the health and healthcare systems. This general framework, while evolved specifically for chronic heart and lung diseases, is anticipated to be broadly applicable to other chronic health conditions, including the increasingly common co-occurrence of multiple chronic health conditions in the same individual.
Recommendation 3
The committee recommends that HHS adopt the framework illustrated in Figure S-1 as a guide for national surveillance of cardiovascular and chronic lung diseases.
Impressive gains have been achieved in life expectancy for the overall American population, as well as distinct subpopulations defined by race and ethnicity. However, inequities in health status and health systems remain in many neighborhoods, cities, states, and regions. The committee explored the need for data that would facilitate understanding of the effects of race and ethnicity on health and health outcomes and concluded that it would endorse the recommendations of the IOM report Race, Ethnicity, and Language Data: Standardization for Health Care Quality Improvement (2009). That report recommends that organizations collecting data related to health and heath
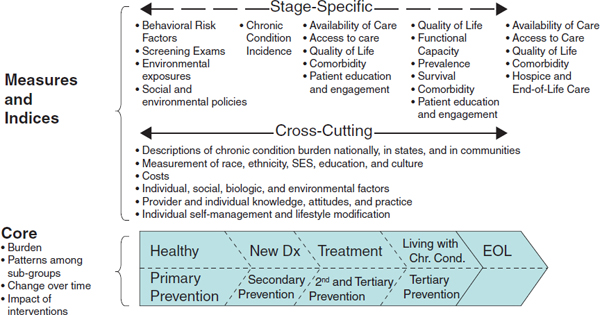
FIGURE S-1 Framework for a national surveillance system for cardiovascular and chronic lung diseases.
SOURCE: Adapted from Wingo et al. (2005).
care should not only use the OMB race and Hispanic ethnicity categories but also select other ethnicity categories to include from a national standard set.
An effective national surveillance system will require more effective and efficient linkages of conventional surveillance data to contextually relevant information, such as socioeconomic status, birthplace, acculturation, geography, language, and health insurance. Also, to the extent possible, there should be standard definitions of key risk factors, outcomes, and interventions as well as a mechanism to link subjects and providers across the different data sources. The committee believes that serious consideration should be given to the scientific and cost considerations as well as the ethical and privacy issues associated with the use of a unique personal health identifier and the use of standardized case definitions and data collection elements so that results can be compared within and across different geographical areas. Furthermore, the integrated system should be able to evolve to allow for recognition of new disease entities, for understanding how changes in public policy affect the disease being studied, and for determining how risk factors can have a major impact on incidence and prevalence of other diseases. Functional capacity, quality of life, and patient engagement and action measures are needed. Enhancing the use of current data sources requires coordination of data collection efforts, harmonization of some elements, expansion to include patient outcomes, and community-tailored items. Coordination of data collection efforts across federal, state, and local systems and healthcare delivery organizations requires, to the extent possible, standard definitions of key risk factors and outcomes, interventions, and a mechanism to link subjects and providers across the different data sources.
Recommendation 4
The committee recommends that the group that oversees and coordinates surveillance activity be charged with:
- Selecting surveillance indicators and, periodically, undertaking a review of the surveillance system in order to identify and incorporate necessary modifications;
- Improving collaboration and coordination among federal, tribal, state, and local agencies and nongovernmental organizations around the collection, compilation, and dissemination of surveillance information;
- Collecting and making available all types of surveillance data (survey, registry, EHR) at the most granular level consistent with protection of data privacy and confidentiality and, when feasible, linked with other data sources (i.e., clinical databases, public health data);
- Formation of public–private partnerships with the nongovernmental health sector; and
- Development of data sets for surveillance sources that can be made broadly accessible to a variety of users to support and guide action to improve health at the national, state, and local levels.
While the working group functions are as outlined above, a mechanism is needed to facilitate implementation of the enhanced and integrated system as it evolves. To further an understanding of the basis and trajectories of cardiovascular and chronic lung diseases, the information collected by the system must be available and accessible to a variety of stakeholders. While data from national surveys conducted by the federal, state, or local governments are usually readily available, private sources of data are frequently inaccessible or accessible only with great difficulty. A greater national investment is needed to ensure that chronic disease surveillance data are accessible to potential data users with a wide range of technical capacities.
Recommendation 5
The committee recommends that the Secretary of HHS designate a federal office with the following responsibilities:
- Producing and disseminating regular surveillance reports and key indicators of progress that support and stimulate action aimed at improving health and reducing disparities at the national, state, and local levels;
- Assuring that the surveillance data are accessible to a broad spectrum of users (e.g., public health agencies, health systems, researchers, policy makers, and advocacy groups) at all levels while protecting privacy and documenting the extent of that use; and
- Implementing the recommendations of the national working group.
As discussed earlier, the life course perspective is important to understanding the trajectory of chronic diseases. Also needed are comparable data that enable analysis across different subpopulation groups and geographic levels and that can be linked across data sources. The committee concluded that existing data collection mechanisms provide valuable information that, with enhancements, can serve to meet the surveillance needs for CVD and chronic lung disease.
Recommendation 6
The committee recommends that HHS coordinate with voluntary bodies operating disease registries to promote collection and harmonization of data.
Recommendation 7
The committee recommends that governmental and nongovernmental organizations enhance existing national data sources in the following manner:
- Information on all elements of the recommended framework should be collected on the U.S. population across the life span, with special attention paid to collecting information on diverse and changing populations, including information on disparities.
- A minimum subset of actionable indicators as identified by the working group should be collected using comparable measures at the national, state, and local levels.
- Data should be increasingly linked across health domains and data sources.
Effective interventions to prevent CVD and chronic lung disease, many of which take place at the local level, require tracking information at multiple geographic levels—local and state as well as national. Community-tailored survey items will be necessary to understand the extent to which conditions vary by characteristics such as socioeconomic status, race/ethnicity, or geographic setting (e.g., urban versus rural). To foster efforts to reduce these disparities, a surveillance system must be capable of providing data for analysis of disparities not only at the national level but also at the regional, state, and local levels. Furthermore, the system will be most beneficial if comparisons can be made between and among various communities; this requires collection of comparable data.
Recommendation 8
The committee recommends that HHS develop a cardiovascular and chronic pulmonary disease survey question bank and technical support for use by tribal, state, and local agencies; nongovernmental organizations; and individual researchers for the purpose of enhancing the quality and comparability of population health surveys in order to identify trends in risk factors, diseases, treatments, and outcomes.
There is great potential for the use of electronic health records (EHRs) as sources of surveillance information. Currently, those records focus primarily on recording clinical information (e.g., diagnoses, laboratory work, and treatments). However, behavioral, social, and physical environmental risk factors in the development of cardiovascular and chronic lung diseases are key to understanding the development of these diseases. The Office of the National Coordinator for Health Information Technology (ONCHIT) is responsible for identifying the minimum data to be collected for EHRs. ONCHIT is in a position to take action that would significantly enhance the surveillance information contained in EHRs.
Recommendation 9
The committee recommends that the Office of the National Coordinator for Health Information Technology expand the minimum data for electronic health records to include behavioral, social, and environmental risk factors for cardiovascular and chronic lung diseases in validated, interoperable ways in order to enhance the quality of surveillance data for these conditions.
Because EHRs are currently in use in only a minority of hospitals and practices, several interim steps are needed before their potential can be realized. Expansion of EHRs to the majority of clinical care settings will require significant investment in purchasing necessary equipment and software as well as staff training. Additional resources will need to be devoted to major issues such as interoperability of EHR systems and harmonization of data standards.
Many existing sources of surveillance information provide high-quality data that are critical to understanding the trajectory of cardiovascular and chronic lung diseases. However, those data lack standardization and cannot be linked across sources, and many of them are not readily accessible. Furthermore, there is a need for collection of data that can be analyzed by demographic variables such as race/ethnicity, socioeconomic status, and geography. The committee believes the recommendations provided in this report lay the foundation or framework and the basics of the infrastructure needed for integrating and enhancing current CVD and COPD surveillance activities so that they can evolve into the complex, interdependent system needed.
REFERENCES
Agarwal, R., J. M. Norton, K. Konty, R. Zimmerman, M. Glover, A. Lekiachvili, H. McGruder, A. Malarcher, M. Casper, G. A. Mensah, and L. Thorpe. 2010. Overreporting of deaths from coronary heart disease in New York City hospitals, 2003. Preventing Chronic Disease 7(3):A47.
Camilli, A. E., D. R. Robbins, and M. D. Lebowitz. 1991. Death certificate reporting of confirmed airways obstructive disease. American Journal of Epidemiology 133(8):795-800.
CDC (Centers for Disease Control and Prevention). 2008. Chronic disease prevention and health promotion. http://www.cdc.gov/nccdphp/ (accessed April 1, 2011).
Coady, S. A., P. D. Sorlie, L. S. Cooper, A. R. Folsom, W. D. Rosamond, and D. E. Conwill. 2001. Validation of death certificate diagnosis for coronary heart disease: The Atherosclerosis Risk in Communities (ARIC) study. Journal of Clinical Epidemiology 54(1):40-50.
Goff, D. C., Jr., L. Brass, L. T. Braun, J. B. Croft, J. D. Flesch, F. G. R. Fowkes, Y. Hong, V. Howard, S. Huston, S. F. Jencks, R. Luepker, T. Manolio, C. O’Donnell, R. Marie Robertson, W. Rosamond, J. Rumsfeld, S. Sidney, and Z. J. Zheng. 2007. Essential features of a surveillance system to support the prevention and management of heart disease and stroke: A scientific statement from the American Heart Association councils on epidemiology and prevention, stroke, and cardiovascular nursing and the interdisciplinary working groups on quality of care and outcomes research and atherosclerotic peripheral vascular disease. Circulation 115(1):127-155.
Goodman, R. A., S. Loue, and F. E. Shaw. 2006. Epidemiology and the law. In Applied epidemiology: Theory to practice. 2nd ed, edited by R. C. Brownson and D. B. Petitti. New York: Oxford University Press. Pp. 289-326.
IOM (Institute of Medicine). 2009. Race, ethnicity, and language data: Standardization for health care quality improvement. Washington, DC: The National Academies Press.
Last, J. M. 2001. A dictionary of epidemiology. 4th ed. New York: Oxford University Press.
Lloyd-Jones, D. M., D. O. Martin, M. G. Larson, and D. Levy. 1998. Accuracy of death certificates for coding coronary heart disease as the cause of death. Annals of Internal Medicine 129(12):1020-1026.
MedPac. 2009. Improving incentives in the medicare program. Washington, DC: Medicare Payment Advisory Commission.
Mitchell, R., J. Maisel, G. Dart, and G. Silvers. 1971. The accuracy of the death certificate in reporting cause of death in adults. With special reference to chronic bronchitis and emphysema. American Review of Respiratory Disease(104):844-850.
Sington, J. D., and B. J. Cottrell. 2002. Analysis of the sensitivity of death certificates in 440 hospital deaths: A comparison with necropsy findings. Journal of Clinical Pathology 55(7):499-502.
Wingo, P. A., H. L. Howe, M. J. Thun, R. Ballard-Barbash, E. Ward, M. L. Brown, J. Sylvester, G. H. Friedell, L. Alley, J. H. Rowland, and B. K. Edwards. 2005. A national framework for cancer surveillance in the United States. Cancer Causes and Control 16(2):151-170.
Yeh, R. W., and A. S. Go. 2010. Rethinking the epidemiology of acute myocardial infarction: Challenges and opportunities. Archives of Internal Medicine 170(9):759-764.










