
Human factors, with its emphasis on user- or person-centered design, can help to ensure that health care in the home suits the people, the tasks, and the environments involved and that the care provided is safe, effective, and efficient. According to the International Ergonomics Association, “[Human factors] is the scientific discipline concerned with the understanding of interactions among humans and other elements of a system, and the profession that applies theory, principles, data, and other methods to design in order to optimize human well-being and overall system performance” (International Ergonomics Association, 2010).
Human factors is therefore concerned with applying what is known about human behavior, abilities, limitations, and other characteristics to the design of systems, tasks/activities, environments, and equipment/technologies. It is also concerned with the design of training programs and instructional materials that support the performance of tasks or the use of technology/equipment.
The focus of human factors is on how people interact with tasks, with equipment/technologies, and with the environment, in order to understand and evaluate these interactions. The goals of human factors are to optimize human and system efficiency and effectiveness, safety, health, comfort, and quality of life. To date, there has been only limited application of human factors knowledge and methods to health care in the home. This report is designed to call attention to the resulting missed opportunities and the great potential advantages of bringing a human factors approach into the center of planning for high-quality and safe home health care.
In this chapter, we discuss some of the tools and methods of human
factors and how their application could improve the design and implementation of home health care.
A HUMAN FACTORS MODEL
Figure 3-1 presents a model of the human factors of health care in the home, based on a systems approach (e.g., Lawton and Nahemow, 1973; Meister, 1989; Czaja et al., 2001; Czaja and Nair, 2006). The components of this system are the person(s) involved in health management (e.g., care recipients and caregivers), the tasks in which they are engaged (e.g., blood glucose monitoring, assistance with activities of daily living), the equipment/technology that they are using to perform these tasks (e.g., blood glucose meter, computer, lifting device), and the environments in which these interactions occur (physical, social, community, and policy environments).
As depicted in the model, people have different characteristics, skills/abilities, education, health conditions, preferences, and attitudes that they
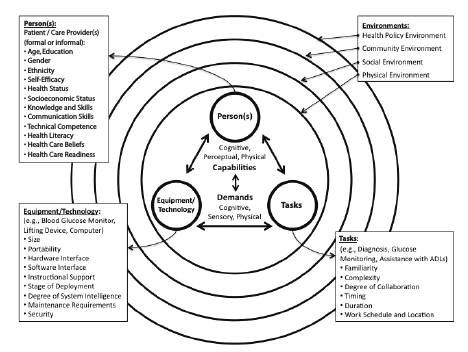
FIGURE 3-1 Model of human factors of health care in the home.
SOURCE: Czaja and Nair [adapted from Czaja et al. (2001)].
bring to the home health care experience. As a result, they vary with respect to their cognitive, perceptual, and physical capabilities with which to interact with tasks and equipment/technology. Interactions are represented by the double arrows in the model. Tasks and equipment/technology also have different characteristics. The type and magnitude of cognitive, sensory, and physical demands placed on people by these tasks and equipment/technology vary and are directly related to personal capabilities. The multiple environments in which the person(s), tasks, and equipment/technology reside interact with each other and are represented by overlapping circles in the model. These environments also have different characteristics and place varying enablers and barriers on a person’s successful completion of tasks and use of equipment/technology. It is also important to note that systems are dynamic and the attributes of the people, tasks, equipment/technology, and environments change over time.
A diabetes management example can be used to illustrate the model. In this case, we examine the interactions involved when an older man with diabetes uses a glucometer in his home to track his glucose level with the goal of maintaining his serum blood glucose within recommended limits in order to prevent complications. The man performing the task may have low health literacy, visual problems, and some mild cognitive impairment, and his caregiver may be his wife, who is close to him in age. The person components of the interactions may also include a nurse at a distant clinic who monitors the medical data of the care recipient via telemonitoring1 and a nurse and home health aide who visit weekly to check on the general health status of the care recipient, measure his vital signs, and assist with personal care. In terms of tasks, the man may be required to monitor his glucose according to a prescribed protocol. Both he and his wife may take several medications on varying schedules. The wife may need to help her husband with various activities and operate the telemonitoring equipment. Use of both the glucometer and the telemonitoring equipment requires the ability to read labels and displays, operate controls, calibrate the equipment, and understand and remember operating procedures. The environment also plays an important role. In this case, the couple may live in a small apartment in a rural location with unreliable Internet access. However, they may have neighbors who check on them and children who visit regularly. A basic tenet of human factors is that “optimization” of this system requires understanding the characteristics of and interactions among all of the components of the system. As illustrated in this example, even relatively modest home health care systems can be complex and may
_____________
1Telemonitoring may involve a personal computer with Internet or e-mail connectivity to send data electronically to the clinic.
involve several people who must interact with a variety of technologies to perform an array of tasks.
Ultimately, the interactions and the degree of “fit” among each of these system components influence the efficiency, effectiveness, and safety of the system and the degree to which the goals of the system can be met. In this example, if the fit is adequate, the man’s diabetes will be successfully managed and he will be able to remain at home. If the fit is poor, he may develop complications that require him be hospitalized. This would increase his risk for comorbidities, such as infection, and also result in a dramatic increase in the cost of care. Misfits among system components may occur at a number of points in the system interactions. For example, the man may not be able to adhere to his medication schedule. He and his wife may have problems using the glucometer and become frustrated and so discontinue using it. They also may have difficulty communicating such problems to caregivers and/or medical providers. The nurse may not be able to adequately monitor the husband’s progress due to problems with the telemonitoring technology or Internet access in the neighborhood. The home health aide may not have adequate training or may be frustrated and/or stressed because of her workload or difficulties accessing the couple’s home. Clearly this is a complex system with many risks for misfit or failure. These risks could be avoided or minimized and the chances for success maximized with the integration of human factors considerations into the design of the system.
HUMAN FACTORS METHODS
Research Methods
Human factors specialists often engage in research to gain a basic understanding of or new knowledge about people and behavior. As with other disciplines, they use a variety of research methods that range from highly controlled laboratory experiments, to less controlled observational studies in real-world contexts, to simulation and modeling. When engaging in research, they also use a variety of data collection techniques that include objective measurement of performance or physiological indices; subjective ratings of satisfaction, comfort, or workload; observational checklists; and interview methods. As with any discipline, the research method chosen and the type of data collected depend on the nature of the problem and other issues, such as feasibility, cost, and time constraints.
For example, in order to design cognitive aids to support the ability of people to engage in Internet-based health information seeking, it is important to understand the cognitive abilities that are required to perform this task successfully. This would typically involve conducting research in a laboratory setting to investigate the relationship between cognition
and information-seeking performance. The research protocol is likely to entail assessing the cognitive abilities of study participants using standard measures of cognition; having the participants perform a sample set of health information search tasks; asking the participants to rate the level of difficulty of the tasks and identify the sources of difficulty; and examining the relationship between the measures of cognition and measures of performance (e.g., task duration or errors). Another example is an observational study, in which the goal is to understand if the prevalence of Internet-based health information seeking varies among age or ethnic subgroups. In this case, telephone or mail surveys or real-time tracking of Internet behavior might be used to gather the needed information. Sometimes the information gathered about behavior is used to develop mathematical models or simulations, which can then be used in the design of tasks or technologies. For example, biomechanical models are often used to evaluate or compare physical demands of tasks or environments. These models might be used to predict the amount of stress on the spines of caregivers to help in the design or selection of mechanical aids for transferring care recipients from a bed to a wheelchair or shower.
System Design and Evaluation
User-Centered Design
Optimally, human factors methods and principles are involved in all aspects of the design process, including the predesign analysis, design expression and prototyping, testing, and evaluation (see Figure 3-2). Human factors methods should also be employed in the evaluation of existing systems and system elements, for example, the evaluation of emergency room protocols after some highly consequential errors, such as patient safety violations, occur, or as part of official “postmarket surveillance” activities required by the U.S. Food and Drug Administration for some medical devices on the market.
Human factors specialists use a variety of methods to support the design process. The overriding principle is to center the design process on the person or persons in the system; in other words, human factors practitioners adopt a user-centered design approach. User-centered design, as a design philosophy, has been around for several decades (e.g., Norman and Draper, 1986; Norman, 1988; Morales, Casper, and Brennan, 2007) and has been shown to increase user safety, performance, efficiency and effectiveness, cost-effectiveness, and user satisfaction. In fact, user-centered design has been elevated to a standard (International Organization for Standardization, 2010 [ISO 9241-210:2010]).
Generally, user-centered design involves understanding user needs, task/
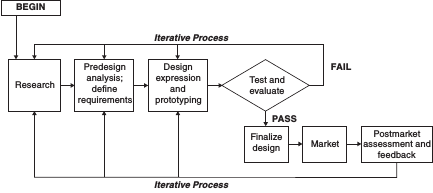
FIGURE 3-2 Conceptual model of the design process.
activity flows and environments, focusing early and continually on users, basing the design of the user interface on known human behavior principles, usability testing and empirical measurement, participatory design in which users are actively involved throughout the process (Wickens et al., 2004), and iterative design.
The term “iterative” applied to the design process refers to the fact that the process should not be a one-way linear progression from concept to product. As needs are determined and design features conceptualized, it is useful to develop prototypes of the design at each point in its development and to test these prototypes with the intended user population. Often the information gained from such prototyping and testing will need to be fed back to inform changes in design that will improve the product or system. This repeated prototyping, testing, and revisiting of the design, shown by the recursive arrows in Figure 3-2, is the best way to ensure good fit with user needs, expectations, and capabilities. Even after the product or system is marketed, it is useful to solicit and analyze feedback on it from users to inform updates or new designs.2
User and Environment Analyses
The design of a system or equipment/technology generally begins with an analysis of the potential user groups (which may include care recipients, informal and formal caregivers, and professional health care providers) to understand their characteristics, needs, preferences, and goals with respect
_____________
2A more extensive description of prototyping and some of its uses can be found in National Research Council (2007, pp. 235-239).
to a system/device. The user-needs analysis usually includes such characteristics as age, education, gender, culture and ethnicity, physical and cognitive abilities, relevant skills, language, and literacy, among others. It also involves descriptions of the users’ needs and preferences, goals, and past experiences. Gathering this information might involve conducting interviews with potential users to understand their goals and objectives with respect to a particular system or system component, such as a device, where it will be used, how often it will be used, experiences with similar devices, etc. It is important to recognize that, for health care in the home, the users are heterogeneous and include people who engage in self-care or receive care and both lay and professional caregivers who vary widely in their skills, abilities, and characteristics (see Chapter 2).
It is also important to gather information on the characteristics of the environment in which the system/device will be used. As noted in Figure 3-1, the environment is multifaceted and not restricted to its physical characteristics. Thus, information should be gathered on all aspects of the environment relevant to the system/device: the immediate physical environment (e.g., home, work, school, travel), the social environment (e.g., family, friends, colleagues, neighbors), the community environment (e.g., weather, sidewalks, parks, shops, transportation), and policy environments (e.g., building codes, social services, insurance policies, reimbursement mechanisms; see Chapter 6).
Task Analysis
Task analysis is a fundamental method in human factors and is used in the design of systems, devices/technologies, training protocols, instruction manuals, jobs or activities, and activity environments. It is also used in the evaluation of existing systems to help identify design problems and sources of mismatches between system demands and user-group capabilities. The basic elements of a task analysis include defining the task or activities that a person will be performing, dividing these activities into subtasks or steps, and specifying the sensory/perceptual, cognitive, and physical demands associated with these subtasks (Chapanis, 1996). It also typically involves identifying the equipment/technology that may be involved in the performance of these activities and the demands associated with the environment in which the activities will occur. The results of task analyses are typically used to develop system requirements for the design/redesign of systems, as well as to develop checklists, training procedures, and performance aids (see Chapter 4).
A task analysis begins with a “task description,” which involves a description of the overall system objectives and of the tasks/activities required by the person to meet these objectives and the linkages among
these tasks. Following the task description, the task demands for each task level, whether they are physical, sensory/perceptual, cognitive, social, or emotional, are specified. These demands are then compared with the capabilities of the planned user population to determine where errors and inefficiencies are likely to arise. The result is a list of potential mismatches keyed to each task and subtask, which is the basis for deriving design requirements for a usable system.
The current standard task analysis methodology is hierarchical task analysis (HTA), although many methods are available. HTA starts from system goals and uses a systematic goal decomposition methodology until a sufficient level of detail is reached to solve the problem at hand. The result of the analysis is generally a hierarchical structure that can be represented either graphically or in an outline-like formatted table that organizes tasks as sets of actions used to accomplish higher level goals. Chapter 4 presents several examples of this methodology.
In health care, many tasks, especially those relying on the use of technology, draw heavily on cognitive capabilities with users required to receive, understand, evaluate, and act on information. For these, one might perform a cognitive task analysis, which can be conceptualized as task analysis applied to the cognitive domain. In this case the demands focus on the knowledge structures (e.g., domain knowledge of a disease or medications, basic knowledge of information-seeking strategies) and the cognitive processes (e.g., working memory, reasoning) that underlie decisions that must be made by the person. Often, the analysis is performed by assuming a computational model of the relevant cognitive processes, and the specific analysis approaches depend on the model adopted.
Many techniques are used for the collection of task data, including observation, interviews, questionnaires, and review of instruction manuals. A task analysis might also involve the use of verbal or “think-aloud” protocols, in which people are asked to verbalize what they are doing and the steps they are taking when engaging in a task or an activity or immediately on completion of that activity (National Research Council, 2007). The human factors literature is often used to find the range of capabilities in the appropriate population to compare with the task demands. The success of task analysis applied to health care in the home depends on the analyst’s human factors expertise, domain knowledge regarding health care and health management in the home, accurate knowledge and descriptions of activities and activity requirements, and knowledge of user capabilities and other characteristics.
Usability Testing
A critical human factors method that is particularly appropriate for the design of components of health care systems is user testing. These tests may take the form of focus groups or usability testing with early mock-ups or mid-stage prototypes or final system components. Often in usability testing, a variety of prototypes or mock-ups are used. For example, in the early stages of usability testing, two-dimensional representations of a device or user interface (a graphical, nonfunctioning version of a system) or storyboards (that describe in a series of images the steps involved in execution of a task) may be used, whereas working prototype devices or fully interactive systems may be used in later stages of testing. Frequently, especially in software engineering, human factors specialists use iterative prototyping, involving a series of tests with rough prototypes and short revision cycles (National Research Council, 2007).
In usability testing it is important to ensure that the participants are representative of the anticipated user groups and that the data collection techniques capture both the demands associated with the activities they will be performing and the relevant environmental contexts. This is especially important with respect to health care systems for the home, for which the potential user groups are broad and diverse. Failing to understand the appropriate range of user abilities, needs, and preferences and the characteristics of and demands imposed by the tasks, equipment/technologies, and environments often results in technology-centered, rather than user-centered, designs that are much more likely to fail (Norman, 1988; Reason, 1990; Casey, 1993; see medical examples in Morrow, North, and Wickens, 2006, pp. 259-265).
Usability metrics include measures of effectiveness (e.g., percentage of tasks completed, ratio of successes to failures, number of applications or features of a product/device used), efficiency (e.g., time to complete a task, time to learn, number of errors, number of help requests), and user satisfaction (e.g., ratings of usefulness, usability, satisfaction with features, number of times user expresses frustration) (Wickens et al., 2004).
Sources of Human Factors Data
Human factors specialists rely on a variety of sources of information to guide their involvement in the design process. This may initially include review of the existing literature, data compendiums, and design standards and guidelines. Several peer-reviewed journals are devoted to the topic of human factors, including Human Factors, Human Factors in Manufacturing, Ergonomics, Applied Ergonomics, Ergonomics in Design, International Journal of Industrial Ergonomics, Journal of Cognitive Engineering and
Design Making, and Journal of Experimental Psychology: Applied. Databases that contain information on human capabilities are also available (e.g., Boff and Lincoln, 1988; Boff, Kaufman, and Thomas, 1994; Wickens et al., 2004; Salvendy, 2006; Fisk et al., 2009).
The Human Factors and Ergonomics Society (HFES) offers best practice documents. For example, HFES 300, Guidelines for Using Anthropometric Data in Product Design, provides guidance for using data on the dimensions of the human body in the design process. The document provides human dimension data and explains proper techniques for applying these data, which may vary depending on the complexity of the population to be accommodated. The guide describes basic and advanced methods for applying anthropometric data, illustrated with examples, and explains the methods’ advantages and disadvantages. The guide includes a long list of resources and references (Human Factors and Ergonomics Society, 2004). In addition, a number of design standards and guidelines are available to guide the design process of medical devices and systems (see Chapter 5).
APPLICATION OF HUMAN FACTORS
Human factors methods and knowledge can be applied to any stage of design or implementation of a system. This includes the initial design of systems and system components to avoid problems and deficiencies, as well as the diagnosis and identification of problems with existing systems. Thus, the concepts and methods of human factors have broad applicability to health care in the home.
For example, human factors techniques can be applied to the design of health care equipment and technologies, such as medication dispensers, glucometers, nebulizers, blood pressure monitors, telemedicine technologies, and software interfaces for Internet health applications. These techniques can also be applied to the design of instruction manuals and training programs to ensure that individuals or their caregivers have the information and skills they need to operate equipment and perform health care tasks. Human factors techniques can be used to inform the design of a home environment to ensure that lighting, layout, and space are adequate for the tasks being performed or the design of a neighborhood to help ensure that there is adequate and effective signage. Human factors approaches are also relevant to the design of jobs for health care workers. For example, human factors methods can be used to determine workflow, to coordinate work, to maintain scheduling and communication protocols, and to determine work requirements to ensure worker productivity, safety, and health. Human factors can have input into the broader organizational environment to help design and implement safety programs, certification protocols, or program evaluation methods.
Human factors techniques can also be used to help understand the sources of human errors and safety violations in the health care domain. In fact, the goals of human factors are commensurate with the goals stated in the report Crossing the Quality Chasm (Institute of Medicine, 2001) for health system reform: safety, effectiveness, patient-centeredness, timeliness, efficiency, and equality. There are numerous examples in the health care domain in which the application of human factors has resulted in reduced errors and cost, increased safety, efficiency, and effectiveness, and personal satisfaction. These examples include efforts to enhance safety and reduce medical errors (e.g., Karsh et al., 2006), medication management (e.g., Lin, Vincente, and Doyle, 2001; Murray et al., 2007), communication among health care providers (e.g., Donchin et al., 2003; Leonard, Graham, and Bonacum, 2004), and the workflow of health care workers (e.g., Carayon and Gurses, 2005). Human factors methods have also been applied to the design of medical equipment and devices (e.g., Lin et al., 1998; Ginsburg, 2005), technology systems to support health management (e.g., Czaja, Sharit, and Nair, 2008; Sharit et al., 2008), and environments in which health care occurs (e.g., Donchin et al., 2003).
From a human factors perspective, optimization of a system’s effectiveness and reduction of adverse outcomes require that all of the components of a system be considered in the design process. This is in contrast to a more traditional reductionist approach, which focuses on one component of a system in isolation from the other components. Using a traditional approach, the focus is typically on the physical or technical components of a system, with little regard for the human. For example, glucometer or medication instructions may be designed without considering how the persons using these instructions might vary in terms of age, cognitive and sensory capabilities, English literacy, health literacy, or stage of illness acceptance.
If there is a mismatch between an individual’s capabilities and those required to perform a task, it is likely that the individual will fail to complete that task successfully or will make errors that may pose a threat to health and well-being. For example, such errors could include lapses in performing health promotion and disease prevention behaviors, not adhering to a prescribed treatment, ignoring warning signs of complications, and not sharing important information about health history, symptoms, or response to treatment with caregivers. Other examples include potentially life-threatening events, such as misreading output from health monitoring equipment, altering equipment settings, turning off alarms, sustaining injuries due to poor body mechanics during lifting and transfers, or continuing intravenous (IV) antibiotic infusion in a person who is showing signs of allergic reaction.
There are many types of human error, and the causes and consequences of these errors vary. Although some errors may be inconsequential, others
may result in preventable disease (i.e., physical or psychological illness or injury), inadequate disease detection and treatment (i.e., too little, too much, or too late), poor symptom control, development of complications, excessive use of health resources, long-term disability, psychological distress, and even death. Some errors and their consequences are preventable via good device or environmental design, whereas others must be handled through procedural or administrative solutions or through user education and training.
In general, optimal system design and error prevention require knowledge about the people, tasks, technologies/equipment, and environments that are involved in the system. They also require knowledge of whether the fit among these system elements is adequate.
In summary, applying human factors knowledge and techniques to the design of health care systems intended for use in the home can make the systems safer, more effective, and more efficient. By optimizing the relationships among the people, the health care tasks and technologies, and the environments in which health care occurs and ensuring that the demands placed on users by the system are within those individuals’ capabilities, these goals can be achieved.
REFERENCES
Boff, K.R., Kaufman, L., and Thomas, J. (1994). Handbook of perception and human performance. Volume II. Cognitive processes and performance. New York: John Wiley and Sons. Available: http://www.dtic.mil/cgi-bin/GetTRDoc?AD=ADA289587&Location=U2&doc=GetTRDoc.pdf [April 2011].
Boff, K.R., and Lincoln, J.E. (1988). Engineering data compendium of human perception and performance. Volume 1. Available: http://www.dtic.mil/cgi-bin/GetTRDoc?AD=ADB345187&Location=U2&doc=GetTRDoc.pdf [April 2011].
Carayon, P., and Gurses, A. (2005). Nursing workload and patient safety in intensive care units: A human factors engineering evaluation of the literature. Intensive and Critical Care Nursing, 21, 284-301.
Casey, S. (1993). Set phasers on stun, and other true tales of design, technology, and human error (2nd ed.). Santa Barbara, CA: Aegean.
Chapanis, A. (1996). Human factors in systems engineering. New York: John Wiley and Sons. Czaja, S.J., and Nair, S.N. (2006). Human factors engineering and systems design. In G. Salvendy (Ed.), Handbook of human factors and ergonomics (3rd ed). New York: John Wiley and Sons.
Czaja, S.J., Sharit, J., Charness, N., and Fisk, A.D. (2001). The Center for Research and Education on Aging and Technology Enhancement (CREATE): A program to enhance technology for older adults. Gerontechnology, 1, 50-59.
Czaja, S.J., Sharit, J., and Nair, S.N. (2008). Usability of the Medicare health web site. Journal of the American Medical Association, 300, 790.
Donchin, Y., Gopher, D., Olin, M., et al. (2003). A look into the nature and causes of human errors in the intensive care unit, 1995. Quality & Safety in Health Care, 12(2), 143-147.
Fisk, A.D., Rogers, W., Charness, N., Czaja, S.J., and Sharit, J. (2009). Designing for older adults: Principles and creative human factors approaches (2nd ed.). Boca Raton, FL: CRC Press.
Ginsburg, G. (2005). Human factors engineering: A tool for medical device evaluation in hospital procurement decision-making. Journal of Biomedical Informatics, 38(3), 213-219.
Human Factors and Ergonomics Society. (2004). Guidelines for using anthropometric data in product design. Santa Monica, CA: Author.
Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Committee on the Quality of Health Care in America. Washington, DC: National Academy Press.
International Ergonomics Association. (2010). What is ergonomics? Available: http://www.iea.cc/01_what/What%20is%20Ergonomics.html [March 30, 2011].
International Organization for Standardization. (2010). ISO 9241-210:2010 Ergonomics of human-system interaction Part 210: Human-centered design for interactive systems. Available: http://www.iso.org/iso/iso_catalogue/catalogue_tc/catalogue_detail.htm?csnumber=52075 [April 2011].
Karsh, B., Holden, R., Alper, S.J., and Or, C.K.L. (2006). A human factors engineering paradigm for patient safety—Designing to support the performance of the health care professional. Quality and Safety in Health Care, 15(Suppl I), i59-i65.
Lawton, M.P., and Nahemow, L. (1973). Ecology and the aging process. In C. Eisdorfer and M.P. Lawton (Eds.), The psychology of adult development and aging. Washington, DC: American Psychological Association.
Leonard, M., Graham S., and Bonacum, D. (2004). The human factor: The critical importance of effective teamwork and communication in providing safe care. Quality and Safety in Health Care, 13(Suppl 1), i85-i90.
Lin, L., Isla, R., Doniz, K., Harkness, H., Vicente, K.J., and Doyle, D.J. (1998). Applying human factors to the design of medical equipment: Patient-controlled analgesia. Journal of Clinical Monitoring and Computing, 14(4), 253-263.
Lin, L., Vicente K.J., and Doyle, D.J. (2001). Patient safety, potential adverse drug events, and medical device design: A human factors engineering approach. Journal of Biomedical Informatics, 34(4), 274-284.
Meister, D. (1989). Conceptual aspects of human factors. Baltimore, MD: Johns Hopkins University Press.
Morales R.M., Casper, G., and Brennan P.F. (2007). Patient-centered design. The potential of user-centered design in personal health records. Journal of the American Health Information Management Association, 78(4), 44-46, quiz 49-50.
Morrow, D., North, R., and Wickens, C.D. (2006). Reducing and mitigating human error in medicine. In R. Nickerson (Ed.), Reviews of human factors and ergonomics, Volume 1 (pp. 254-296). Santa Monica, CA: Human Factors and Ergonomics Society.
Murray, M.D., Young, J., Hoke, S., et al. (2007). Pharmacist intervention to improve medication adherence in heart failure: A randomized trial. Annals of Internal Medicine, 146(10), 714-725.
National Research Council. (2007). Human-system integration in the system development process; A new look. Committee on Human-System Design Support for Changing Technology, R.W. Pew and A.S. Mavor, Eds. Committee on Human Factors, Division of Behavioral and Social Sciences and Education. Washington, DC: The National Academies Press.
Norman, D.A. (1988). The psychology of everyday things. New York: Basic Books.
Norman, D.A., and Draper, S.W. (1986). User-centered system design: New perspectives on human-computer interaction. Hillsdale, NJ: Lawrence Erlbaum Associates.
Reason, J. (1990). Human error. Cambridge, UK: Cambridge University Press.
Salvendy, G. (2006). Handbook of human factors and ergonomics (vol. 3). Hoboken, NJ: John Wiley and Sons.
Sharit, J., Hernández, M.A., Czaja S.J., and Pirolli, P. (2008). Investigating the roles of knowledge and cognitive abilities in older adult information seeking on the web. ACM Transactions on Computer-Human Interaction, 15(1), 3.
Wickens, C.D., Gordon, S.E., and Liu, Y. (2004). An introduction to human factors engineering. Upper Saddle River, NJ: Pearson Prentice Hall.














