
BACKGROUND
The Patient Protection and Affordable Care Act of 2010 (ACA) holds much promise—beyond the expansion of health care coverage—for millions of Americans. The preventive health care services and screenings specified in the legislation will be fully covered without requiring a patient copayment. These include the services with Grade A and B recommendations made by the United States Preventive Services Task Force (USPSTF), the Bright Futures recommendations for adolescents from the American Academy of Pediatrics (AAP) in cooperation with the U.S. Department of Health and Human Services (HHS), and vaccinations specified by the Centers for Disease Control and Prevention’s (CDC’s) Advisory Committee on Immunization Practices (ACIP). These three sets of guidelines provide a list of preventive services, such as blood pressure measurement, diabetes and cholesterol tests, and mammography and colonoscopy screenings. As part of the ACA, the list of preventive services specific to women’s health was requested to be reviewed.
CHARGE TO THE COMMITTEE
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) of HHS provided funds for the Institute of Medicine (IOM) to conduct a review of effective preventive services to ensure women’s health and well-being. The charge to the committee for the project is presented in Box S-1.
BOX S-1
Statement of Task to the Committee on
Preventive Services for Women
The Institute of Medicine will convene an expert committee to review what preventive services are necessary for women’s health and well-being and should be considered in the development of comprehensive guidelines for preventive services for women. The committee will also provide guidance on a process for regularly updating the preventive screenings and services to be considered. In conducting its work, the committee will: conduct a series of meetings to examine existing prevention guidelines, obtain input from stakeholders, identify gaps that may exist in recommended preventive services for USPSTF Grade A and B preventive services guidelines for women and in Bright Futures and USPSTF Grade A and B guidelines for adolescents, and highlight specific services and screenings that could supplement currently recommended preventive services for women. Specifically, the committee will consider the following questions:
- What is the scope of preventive services for women not included in those graded A and B by the USPSTF?
- What additional screenings and preventive services have been shown to be effective for women? Consideration may be given to those services shown to be effective but not well utilized among women disproportionately affected by preventable chronic illnesses.
- What services and screenings are needed to fill gaps in recommended preventive services for women?
- What models could HHS and its agencies use to coordinate regular updates of the comprehensive guidelines for preventive services and screenings for women and adolescent girls?
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) on behalf of the U.S. Department of Health and Human Services (HHS) has been charged to examine recommendations for women’s preventive services. ASPE will use the information and recommendations from the committee’s report to guide policy and program development related to provisions in the Affordable Care Act addressing preventive services for women.
In response, the IOM convened a committee of 16 members—including specialists in disease prevention, women’s health issues, adolescent health issues, and evidence-based guidelines—to develop a set of recommendations for consideration by the ASPE of HHS.
The committee sought clarification from ASPE on a number of issues regarding its charge. In summary:
- Preventive services were specified to be applicable to females aged 10 to 65 years;
- The mammography screenings specified in the ACA legislation used USPSTF guidelines from 2002, which specify that such screenings be performed every one to two years for women aged 40 years and older;
- The cost-effectiveness of screenings or services could not be a factor for the committee to consider in its analyses leading to its recommendations;
- The committee was not intended to duplicate the processes used by the USPSTF and thus should look to other bodies of evidence beyond systematic evidence-based reviews; and
- Preventive services were specified for clinical settings, and thus community-based prevention activities were considered beyond the scope of committee consideration.
COMMITTEE’S APPROACH TO ITS CHARGE
The committee met five times within six months. The committee held three open information-gathering sessions at which the members heard from a diverse group of stakeholders, researchers, members of advocacy organizations, and the public. Box S-2 provides the committee definition of preventive health services.
BOX S-2
Definition of Preventive Health Services
For the purposes of this study, the Committee on Preventive Services for Women defines preventive health services to be measures—including medications, procedures, devices, tests, education and counseling—shown to improve well-being, and/or decrease the likelihood or delay the onset of a targeted disease or condition.
COMMITTEE’S METHODOLOGY
The committee’s methodology to identify preventive services necessary for women’s health and well-being and to identify specific services that could supplement the current list of recommended preventive services for women under the ACA follows.
The committee’s first step was to review and reach an understanding of existing guidelines. The second step was to assemble and assess additional evidence, including reviews of the literature, federal health priority goals
and objectives, federal reimbursement policies, and the clinical guidelines of health care professional organizations. The committee also considered the public comments that it received. Finally, the committee formulated a list of recommendations to be considered by the Secretary of HHS in developing a comprehensive package of preventive services for women to be included under the ACA.
USPSTF Recommendations
The USPSTF process for developing recommendations is a disease-focused one. The intent of its recommendations has been to provide guidance to primary care providers. The IOM committee’s approach to identifying gaps in existing services accounts for contextual issues beyond traditional research evidence used by the USPSTF. The committee looked at women’s preventive service needs more broadly to account for women’s health and well-being. The committee found that its interpretation of the Grade A and B recommendations was important in those cases in which ambiguity was found regarding periodicity of screenings. Furthermore, the committee compared USPSTF guidelines with those of numerous health care professional organizations to identify potential gaps.
The committee recognized that USPSTF Grade C recommendations and I statements warranted further analysis because the USPSTF did not develop and has not used these grades as support to offer or deny coverage of a preventive service. The USPSTF Grade C recommendations are made when the balance of potential benefits and harms does not strongly favor the clinician recommending the preventive service to all patients, although it may be appropriate in some cases.
The USPSTF I statements identify services for which the evidence is insufficient to suggest the effectiveness of a service because evidence is lacking, of lower quality, or conflicting. The committee notes that from a coverage perspective, the evidence supporting many clinical interventions in common use, whether in prevention or in general medical practice, is insufficient or unclear, and coverage decisions may be or have been made on the basis of other factors.
For example, although physician knowledge of the evidence of the benefits associated with a counseling service will inform a physician’s decision for each patient, in many instances, it is difficult for researchers to show or conclude that outcomes are positive. Many preventive interventions that are intended to be conducted early in the life span (e.g., skin cancer prevention) require decades to demonstrate effectiveness.
Thus, each of the USPSTF Grade C and I statement recommendations and the evidence supporting them were collected and reviewed. The committee’s evaluation included reviewing relevant supporting USPSTF
publications, other peer-reviewed research and clinical articles, and clinician fact sheets. Additional literature searches were conducted to identify randomized control trials published after the USPSTF recommendation was released. Furthermore, the committee compared the Grade C and I statement guidelines with guidelines from other professional organizations. The committee did not reexamine the services with Grade D recommendations, because the USPSTF recommends against providing these services.
Bright Futures Recommendations
The committee reviewed all Bright Futures guidelines and compared them with the USPSTF guidelines for adolescents. The committee noted that the methodology that Bright Futures uses is quite different from that which the USPSTF uses. Bright Futures makes decisions through a consensus-driven process; thus, expert opinion is at the core of its development of recommendations.
The committee interpreted the sample questions and advice suggested in the anticipatory guidance section of the Bright Futures report (AAP, 2008) to describe topics to be covered as preventive services under the ACA and addressed in an annual health care visit of sufficient length to cover age- and sex-appropriate topics in the health domain. The committee assumes that physicians will identify priorities from this section of the Bright Futures report on the basis of the unique circumstances of each patient.
ACIP Recommendations
The committee reviewed ACIP General Recommendations on Immunizations, which include all of the Food and Drug Administration-approved immunizations recommended for the general population of adolescent and adult women. Although literature searches were conducted to identify areas where supplemental immunization recommendations might be warranted, the committee identified little evidence to clearly indicate deficiencies in existing ACIP recommendations.
Further Committee Considerations
The committee reviewed oral and written comments submitted throughout the course of the study. The committee also invited researchers and leaders of organizations to deliver presentations in areas in which the committee believed that it could benefit from their expertise. In addition, the committee reviewed HHS documents relating to prevention priorities and reimbursement policies. It also reviewed the existing coverage practices of national, state, and private health plans. In some cases, current practice
in clinical care was also identified. Finally, the committee used the 2011 IOM report Leading Health Indicators for Healthy People 2020 as a tool to perform horizon scanning or examine priority goals and/or persistent trends relating to women’s health and well-being to identify potential gaps (IOM, 2011).
COMMITTEE ANALYSIS
The product of these reviews was an array of potential areas where supplemental preventive measures might be warranted. Some of these areas were identified on the basis of traditional indicators, such as morbidity and mortality, whereas others were identified as being more generally supportive of a woman’s well-being. The committee focused on conditions unique to women or that affected women in some specific or disproportionate way. The committee moved forward using criteria adapted from the USPSTF that considered frequency, severity, morbidity, mortality, and quality of life to bring consistency to the analyses.
For each potential supplemental preventive measure considered, the committee conducted an extensive comparison of the guidelines of professional organizations to understand the development of the guidelines and the evidence that the organizations used to reach their conclusions. The committee also performed targeted literature searches. However, it should be noted that the committee did not have adequate time or resources to conduct its own meta-analyses or comprehensive systematic review of each preventive service.
Supplemental Preventive Measures
The committee attempted to identify preventive measures that were aimed at filling the gaps that it had identified. In most cases, the committee found that measures had already been proposed in the guidelines of other professional organizations. The committee also eliminated preventive measures that, even at this early stage in the analysis, were clearly not developed, tested, or known well enough to have a measurable impact. The resulting product of this step was a series of preventive service areas with gaps in coverage and the accompanying preventive measure or measures that could be considered by HHS. The core of the committee’s task was to assemble the evidence that would allow it to recommend consideration of a preventive service.
Coverage Decisions
As noted above, the USPSTF, Bright Futures, and ACIP guidelines focus on guidance for primary care providers and patients. Coverage decisions
often consider a host of other issues, such as established practice; patient and clinician preferences; availability; ethical, legal, and social issues; and availability of alternatives. Further complicating matters, special population groups such as minority populations, disabled women, recent immigrants, lesbians, prisoners, and those employed in high-risk environments, may have different health needs or benefit from different preventive services. High-risk groups, population subsets, and special populations are unevenly identified and addressed to varying degrees in current guidelines. Finally, cost-effectiveness was explicitly excluded as a factor that the committee could use in developing recommendations, and so the committee process could not evaluate preventive services on this basis.
Committee Approach
The committee developed a hybrid approach that collected relevant evidence for each measure. Four categories of evidence—posed in the form of questions—to be examined for each potential preventive measure were developed. The committee did not formally rank or assign weights to the categories, nor did it stipulate that evidence in any one category would automatically result in a recommendation for a measure or service to be considered. Instead, the queries and categories were used to consider the range of evidence and to ensure consistency in the committee’s analysis and deliberations. Many of the recommendations are supported by more than one category of evidence.
Category I. Are high-quality systematic evidence reviews available indicating that the service is effective in women?
Category II. Are quality peer-reviewed studies available demonstrating effectiveness of the service in women?
Category III. Has the measure been identified as a federal priority to address in women’s preventive services?
Category IV. Are there existing federal, state, or international practices, professional guidelines, or federal reimbursement policies that support the use of the measure?
RECOMMENDATIONS
Subcommittees were formed, and each subcommittee reviewed the available evidence applicable to its identified potential preventive measure(s) and assigned the evidence to one or more of the above categories. Each subcommittee then brought its analysis of the range of evidence before the full committee for deliberation. The committee then combined the burden of the condition and its potential impact on health and well-being with the array of available evidence and support to reach a consensus regarding
whether to recommend a specific preventive measure for that condition. As is true in most analytical processes in decision making, evidence and expert judgment are inextricably linked; thus, the expert judgments of the committee members also played a role in decision making.
In general, the preventive measures recommended by the committee for consideration of coverage (see Table S-1) met the following criteria:
- The condition to be prevented affects a broad population;
- The condition to be prevented has a large potential impact on health and well-being; and
- The quality and strength of the evidence is supportive.
Ultimately, the decision to develop a recommendation for a preventive service to be considered was made after a thoughtful review and debate of each of the subcommittee reports and when the committee found the evidence to be compelling.
TABLE S-1 Summary of the Committee’s Recommendations on Preventive Services for Women
|
|
|||
| Preventive Service | USPSTF Grade | Supporting Evidence | Recommendations |
|
|
|||
| Screening for gestational diabetes | I | The evidence provided to support a recommendation for screening for gestational diabetes is based on current federal practice policy from the U.S. Indian Health Service, the U.S. Department of Veterans Affairs, as well as current practice and clinical professional guidelines such as those set forth by the American Academy of Family Physicians and the American Congress of Obstetricians and Gynecologists. | Recommendation 5.1 The committee recommends for consideration as a preventive service for women: screening for gestational diabetes in pregnant women between 24 and 28 weeks of gestation and at the first prenatal visit for pregnant women identified to be at high risk for diabetes. |
|
|
|||
|
|
|||
| Preventive Service | USPSTF Grade | Supporting Evidence | Recommendations |
|
|
|||
| Human papillomavirus testing (HPV) | I | The evidence provided to support a recommendation to support testing for HPV is based on federal practice policy from the U.S. Department of Defense. Peer-reviewed studies demonstrate that improved testing technologies, particularly combined screening using both conventional cytology and high-risk HPV DNA testing, may significantly improve the rate of detection of cervical cancer precursors and facilitate the safe lengthening of the interval for screening. | Recommendation 5.2 The committee recommends for consideration as a preventive service for women: the addition of high-risk human papillomavirus DNA testing in addition to cytology testing in women with normal cytology results. Screening should begin at 30 years of age and should occur no more frequently than every 3 years. |
| Counseling for sexually transmitted infections (STIs) | I | The evidence provided to support a recommendation related to STI counseling is based on federal goals from the Centers for Disease Control and Prevention and Healthy People 2020, as well as recommendations from the American Medical Association and the American College of Obstetricians and Gynecologists. | Recommendation 5.3 The committee recommends for consideration as a preventive service for women: annual counseling on sexually transmitted infections for sexually active women. |
|
|
|||
| Preventive Service | USPSTF Grade | Supporting Evidence | Recommendations |
|
|
|||
| Counseling and screening for human immuno-deficiency virus (HIV) | C | The evidence provided to support a recommendation for expanding screening for HIV is based on federal goals from the Centers for Disease Control and Prevention, as well as clinical professional guidelines, such as those from the American College of Physicians, the Infectious Diseases Society of America, the American Medical Association, and the American College of Obstetricians and Gynecologists. | Recommendation 5.4 The committee recommends for consideration as a preventive service for women: counseling and screening for human immunodeficiency virus infection on an annual basis for sexually active women. |
| Contraceptive methods and counseling | Not Addressed | The evidence provided to support a recommendation related to unintended pregnancy is based on systematic evidence reviews and other peer-reviewed studies, which indicate that contraception and contraceptive counseling are effective at reducing unintended pregnancies. Current federal reimbursement policies provide coverage for contraception and contraceptive counseling, and most private insurers also cover contraception in their health plans. Numerous health professional associations recommend family planning services as part of preventive care for women. Furthermore, a reduction in unintended pregnancies has been identified as a specific goal in Healthy People 2010 and Healthy People 2020. | Recommendation 5.5 The committee recommends for consideration as a preventive service for women: the full range of Food and Drug Administration-approved contraceptive methods, sterilization procedures, and patient education and counseling for women with reproductive capacity. |
|
|
|||
| Preventive Service | USPSTF Grade | Supporting Evidence | Recommendations |
|
|
|||
| Breastfeeding support, supplies, and counseling | B | The evidence provided to support a recommendation regarding the inclusion of breastfeeding services is based on systematic evidence reviews, federal and international goals (such as the U.S. Surgeon General, Health Resources and Services Administration [HRSA], Healthy People 2020, World Health Organization and UNICEF) and clinical professional guidelines such as those set forth by the American Academy of Family Physicians, the American Academy of Pediatrics, and the American College of Obstetricians and Gynecologists. | Recommendation 5.6 The committee recommends for consideration as a preventive service for women: comprehensive lactation support and counseling and costs of renting breastfeeding equipment. A trained provider should provide counseling services to all pregnant women and to those in the postpartum period to ensure the successful initiation and duration of breastfeeding. (The ACA ensures that breastfeeding counseling is covered; however, the committee recognizes that interpretation of this varies.) |
| Screening and counseling for interpersonal and domestic violence | I | The evidence provided to support a recommendation related to increasing detection of and counseling for domestic violence and abuse is based on peer-review studies and federal and international policies, in addition to clinical professional guidelines from organizations, such as the American Medical Association and the American College of Obstetricians and Gynecologists. | Recommendation 5.7 The committee recommends for consideration as a preventive service for women: screening and counseling for interpersonal and domestic violence. Screening and counseling involve elicitation of information from women and adolescents about current and past violence and abuse in a culturally sensitive and supportive manner to address current health concerns about safety and other current or future health problems. |
|
|
|||
| Preventive Service | USPSTF Grade | Supporting Evidence | Recommendations |
|
|
|||
| Well-woman visits | Not Addressed | The evidence provided to support a recommendation for including well-woman visits is based on federal and state policies (such as included in Medicaid, Medicare and the state of Massachusetts), clinical professional guidelines (such as those of the American Medical Association and the American Academy of Family Practitioners), and private health plan policies (such as those of Kaiser Permanente). | Recommendation 5.8 The committee recommends for consideration as a preventive service for women: at least one well-woman preventive care visit annually for adult women to obtain the recommended preventive services, including preconception and prenatal care. The committee also recognizes that several visits may be needed to obtain all necessary recommended preventive services, depending on a woman’s health status, health needs, and other risk factors. |
|
|
|||
UPDATING GUIDELINES
Developing and maintaining a comprehensive list of covered preventive services for women is not currently under the specific purview of any HHS entity. Thus, the committee believes that it will be necessary to develop structures, accountability, and processes to ensure that preventive services meeting evidence-based standards are considered in the context of the general approach taken to identify and update preventive services for women.
The committee recommends a process supported by guiding principles that separates evidence assessment and coverage decisions.
Recommendation 6.1: The committee recommends that the process for updating the preventive services for women be:
- Independent;
- Free of conflict of interest;
- Evidence-based;
- Gender-specific;
- Life-course oriented;
- Transparent;
- Informed by systematic surveillance and monitoring;
- Cognizant of the need to integrate clinical preventive services with effective interventions in public health, the community, work place, and environment; and
- Appropriately resourced to meet its mandate.
Recommendation 6.2: The committee recommends that the Secretary of HHS establish a commission to recommend coverage of new preventive services for women to be covered under the ACA.
In carrying out its work the commission should:
- Be independent of bodies conducting evidence reviews, free of conflict of interest, and transparent;
- Set goals for prevention (it may use available HHS reports and products or commission its own at its discretion);
- Design and implement a coverage decision making methodology to consider information from evidence review bodies (and other clinical guideline bodies) and coverage factors (e.g., cost, cost-effectiveness, legal, ethical);
- Conduct horizon scanning or examine priority goals and/or persistent trends relating to women’s health and well-being to identify new information on significant health conditions, preventive interventions, new evidence regarding efficacy, effectiveness, periodicity, and safety;
- Focus on the general population, but also search for conditions that may differentially affect women and high-risk subpopulations of women;
- Assign evidence review topics and set review priorities for the bodies reviewing clinical effectiveness;
- Set timetables and processes for updating clinical practice guidelines and coverage recommendations; and
- Submit its coverage recommendations to the Secretary of HHS.
Recommendation 6.3: The committee recommends that the Secretary of HHS identify existing bodies or appoint new ones as needed to review the evidence and develop clinical practice guidelines to be reviewed by a preventive services coverage commission.
Bringing clinical preventive services into rational alignment with the coverage for other health care services under the ACA will be a major task. The committee notes that many of the individual components for review of the evidence are already managed within HHS but currently lack effective coordination for the purposes outlined in the ACA and that some functions are entirely new. The structure might be effectively built over time by using
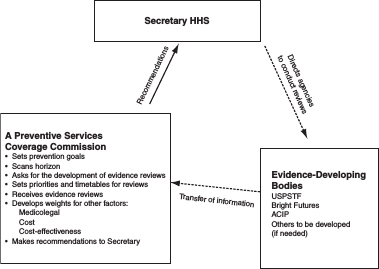
FIGURE S-1 Suggested structure for updating preventive services under the ACA.
some current bodies and adding new ones as resources permit. The committee does not believe that it has enough information to recommend which unit in HHS should implement the recommendations. Figure S-1 illustrates the committee’s suggested structure.
In view of the critical importance of community-based preventive services in achieving clinical aims, the committee encourages the Secretary to consider widening the scope of authority to include public health efforts to more comprehensively address prevention. It will be critical for a preventive services coverage commission to coordinate with the new and existing committees that are charged with overseeing other elements of the ACA.
Finally, the committee notes that it would make the most sense to consider preventive services for women, men, children, and adolescents in the same way. Thus, although the committee’s recommendations address women’s preventive services, a parallel approach could be equally useful for determining covered preventive services for men, children, and male adolescents.
REFERENCES
AAP (American Academy of Pediatrics). 2008. Bright Futures: Guidelines for health supervision of infants, children and adolescents, 3rd ed. (J. F. Hagan, J. S. Shaw, and P. M. Duncan, eds.). Elk Grove Village, IL: American Academy of Pediatrics.
IOM (Institute of Medicine). 2011. Leading health indicators for Healthy People 2020 Report. Washington, DC: The National Academies Press.














