
KEY FINDINGS
This report highlights findings and analyses in two broad categories: potential exposure to burn pit emissions at Joint Base Balad (JBB) and other U.S. military bases in Iraq and Afghanistan and potential health effects of that exposure. From the starting points outlined in Figure 3-2, the committee’s data collection and analysis led to the expanded and interactive processes shown in Figure 7-1. Those processes draw on several information sources, such as air monitoring data from JBB, results of health-effects studies in military reports, and results of health-effects studies of related exposure scenarios in the medical and scientific literature, including literature on health effects associated with combustion products individually and in the aggregate. Although those sources yielded substantial amounts of information, the available database is marked by numerous data gaps and uncertainties that point to the need for additional studies and analysis, particularly an epidemiologic study of populations exposed to burn pit emissions. The committee summarizes below its findings presented in the previous chapters and synthesizes its findings into an assessment of the potential long-term health consequences for military and other personnel stationed at JBB and other sites that have burn pits.
Burn Pit Basics
Background information on the use of military burn pits was available from several sources, including the Department of Defense (DoD), particularly the U.S. Army Center for Health Promotion and Preventive Medicine (CHPPM, now the U.S. Army Public Health Command), the Government Accountability Office, and the RAND Corporation. In spite of air-monitoring data from JBB, incomplete information on the burning practices and on the materials burned in the pits hampered the committee’s ability to determine the chemical composition and amount of emissions from the burn pits at JBB and elsewhere. For example, burning of tires was banned at some bases and apparently permitted at others. The committee asked the DoD for specific information pertaining to burn pit locations on the bases and in Iraq and Afghanistan, the number of burn pits in use by the military in those countries, their frequency of use, and the average burn times for the pits. The DoD was unable to provide specific information to characterize waste streams at large and small forward operating bases but it did provide generic data on waste-stream content, for example, percentages of plastics, wood, and miscellaneous noncombustible, metal, and combustible materials at bases in Iraq and Afghanistan (Faulkner 2011). Nonhazardous solid waste generated by bases in Kosovo, Bosnia, and Bulgaria was better characterized (Faulkner 2011), but the extent of similarity
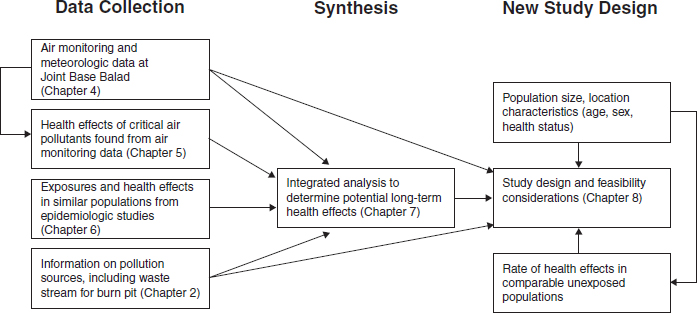
FIGURE 7-1 Committee’s process for assessing the long-term consequences of exposure to burn pit emissions and the design of an epidemiologic study.
between the burn pits in these countries and in Iraq and Afghanistan, and in particular at JBB, is unknown. Available information suggests that burn pit practices varied among bases and over time; the amount of waste burned daily at JBB is estimated to have varied by an order of magnitude over its years of operation.
Combustion Products and Exposure Considerations
Air samples were collected upwind of the burn pit and downwind in an open area and in a housing and work area. The sampling targeted several chemical categories, including particulate matter (PM) and metals, volatile organic compounds (VOCs), polycyclic aromatic hydrocarbons (PAHs), and polychlorinated dibenzodioxins and furans (PCDDs/Fs). It is notable that some U.S. criteria air pollutants, such as sulfur dioxide, nitrogen dioxide, carbon monoxide, and ozone, were not analyzed for at JBB. CHPPM found measurable concentrations of many of the chemicals for which the samples were analyzed, albeit at concentrations below those typically observed in urban airsheds outside the United States. However, the samples contained contributions from other sources of air pollution in the area, so measured air contaminants could not be directly attributed to the JBB burn pit. Based on its analysis of the CHPPM data, the committee concluded that:
- Background ambient air concentrations of PM at JBB are high, with average concentrations above the U.S. air pollution standards, and are most likely derived from local sources;
- PCDDs/Fs were detected at low concentrations in nearly all samples (although high compared with even polluted urban areas), and the burn pit was likely the major source of these chemicals; and
- Ambient VOC and PAH concentrations were similar to those reported for polluted urban environments outside the United States, and the major sources of these pollutants are regional background, ground transportation, stationary power generation, and the JBB airport.
The data thus indicate that military personnel were exposed to a mixture of combustion products from the burn pit and to other air pollutants from local and regional sources, including other combustion sources, industry, and wind-blown soil. It is likely that people who worked at or near burn pits were exposed to combustion emissions and
products of incomplete combustion at concentrations higher than those measured at the CHPPM monitoring sites, but the available information is insufficient to estimate the concentrations to which they might have been exposed.
Potentially Related Health Effects and Hazard Considerations
Most of the pollutants detected at JBB were present at concentrations lower than health-based reference values of individual pollutants that are considered to be protective of the general U.S. population. The exceptions were PM and acrolein, neither of which could be attributed primarily to the burn pit. Measured PM concentrations substantially exceeded U.S. standards, and increased cardiovascular and respiratory morbidity and mortality have been observed in many epidemiologic studies of PM exposures at lower concentrations (IOM 2010). Although acrolein was poorly measured with the analytic techniques used, the concentrations were above a health-based reference concentration of 2 × 10-5 mg/m3 (EPA 2003) although still far below any concentration observed to cause the nasal lesions and lung damage in laboratory animal experiments from which the reference value is derived. Exceedances of the health-based reference value of acrolein are common in U.S. monitoring data.
However, information on health effects of exposure to mixtures specific to burn pits is minimal. There is a larger dataset for health effects of exposure to combustion products from the open burning of waste and of exposure to combustion products from the burning of cooking and heating fuels, such vehicle fuels as JP-8, and household and municipal waste. The committee therefore turned to studies of firefighters and workers at municipal incinerators as populations exposed to combustion products likely to be similar in chemical composition to burn pit emissions. It was hoped that those populations would provide information useful for assessing possible long-term health effects of exposure to such mixtures.
That approach was based on several considerations. The DoD had labeled the waste stream for the military burn pits as containing “household waste,” what is known of its composition is similar to that of such waste, and the dioxin congener profiles measured at JBB are similar to those seen in open burning of household waste. Firefighters are exposed to burning homes, commercial properties, and wildfires that might also contain materials similar to burn pit material, such as wood, electronics, and particularly plastics. Municipal waste-incinerator workers would be expected to be exposed to similar combustion products. Because the military personnel at JBB not only worked on the base but lived there, the committee also sought information on reported long-term health effects in residents who live near municipal waste incinerators.
Those studies did not yield conclusive results about long-term health effects associated with exposure to combustion products in the populations studied, but several health outcomes deserve further investigation. Respiratory outcomes should be assessed further because such air pollutants as PM, which are generally present in burn pit emissions, are known to have respiratory effects. Pulmonary function should be monitored to track changes and diagnose respiratory diseases, including asthma, bronchitis, and emphysema. Although there are reports of constrictive bronchiolitis in military personnel returning from JBB, it is difficult to conduct studies to assess this effect because the diagnosis is based on lung biopsy and ascertainment of cases for followup studies is therefore problematic. Nevertheless, the presentation of several cases in military personnel who have been deployed to bases that have burn pits warrants continuing study.
Many neurologic outcomes are associated with chemicals potentially present in emissions from burn pits. However, studies involving firefighters and others exposed to incinerator emissions provide little information on neurologic outcomes that might be associated with exposure to mixtures of combustion products.
Cardiovascular outcomes were observed in some studies; however, no increase in any specific cardiovascular outcome was reported consistently. Increased ischemic heart disease, arteriosclerosis, aortic aneurysm, and diseases of arteries and veins were reported in studies of firefighters but not in studies of other populations. Most of the studies of firefighters and other populations lacked adjustment for the acknowledged risk factors of cardiovascular disease, such as diet, physical activity, smoking, and a family history of heart disease. Nevertheless, although the evidence provided by those epidemiologic studies did not allow the committee to reach definitive conclusions about the risk of cardiovascular disease, an increase in risk caused by exposure to combustion products cannot be ruled out. Future followup pertaining to cardiovascular disease should develop data on risk factors, such as smoking, and should investigate disease incidence rather than focus on mortality. Better exposure assessment is critical.
The epidemiologic literature on cancer in firefighters and incinerator workers is inconsistent; reports link work in these occupations with brain, testicular, colon, and prostate cancers. Because many of the studies are marked by failure to control for confounding factors, have infrequent or inadequate exposure assessment, and do not have sufficient information to show dose–response relationships, the committee was unable to determine whether any increased risks of brain, testicular, colon, or prostate cancer were associated with combustion products or with other characteristics specific to the study populations. Because of the carcinogenic nature of many of the chemicals potentially associated with burn pit emissions, it is prudent to continue investigations of cancer end points and other health outcomes that have long latency in exposed military populations.
The DoD or the Department of Veterans Affairs (VA) may also consider investigating other health outcomes seen in personnel deployed to JBB, such as birth defects, rheumatoid arthritis, and lupus.
SYNTHESIS AND IMPLICATIONS
The starting point for the committee’s work was a series of military reports and individual observations related to combustion products and possible health effects associated with military service at JBB, mainly from 2006 to 2009. Those reports and observations, which include videos and photographs, clearly establish that smoke from the burn pits drifted over the base at various times. However, the absence of atmospheric sampling data describing more fully the nature and extent of exposure to smoke by military personnel limits the availability of critical information, such as the concentration, composition, frequency, or duration of smoke episodes at the site. Similarly, although medical data on the health status of military personnel who served at JBB are available, the epidemiologic studies that have been conducted by the DoD do not provide sufficient information for evaluating an any association between exposure to burn pit emissions and long-term health effects in exposed military personnel. The DoD studies do not have sufficient followup to identify latent health effects, such as cancer and cardiovascular disease. The studies also do not provide any information on the degree of exposure that people may have experienced at JBB, such as how long they were at the base, where on the base they worked or lived, and whether they had more than one deployment to JBB or to other bases that had operating burn pits; nor do the studies adjust for confounding factors, such as smoking. The committee recognizes that the DoD studies did categorized deployed personnel as being with a 3- or 5-mile radius at some bases and compared them with deployed personnel stationed at bases without burn pits or with nondeployed personnel. The major limitations that the committee found in characterizing the waste stream at JBB and in the air monitoring data collected there and in assessing exposure and likely health effects of exposure to the burn pit emissions are given in Box 7-1.
Although air monitoring was conducted twice at JBB in 2007 and once in 2009, the locations of the sampling sites were not optimal for determining ambient concentrations of the air pollutants to which residents of the base might be exposed, and did not target smoke episodes. Only PM and acrolein were detected in the air samples at JBB at concentrations above reference concentrations intended for application for the general population in the United States. The committee understood that the limitations in the JBB air monitoring data would affect its work and that developing the analyses requested in the statement of task would require data from nonmilitary sources in addition to those collected previously at JBB and other military sites. These other sources, although useful, also had substantial limitations and did not permit the committee to determine precisely all the chemicals that might be in the burn pit emissions or their concentrations.
Nevertheless, the committee developed useful information on three categories of combustion products—PCDDs/Fs, VOCs and PAHs, and PM—and on their association with long-term health effects. The observed smoke from burn pits undoubtedly implies a contribution to the PM at JBB, but the committee was unable to distinguish any effects of the burn pit emissions on measured PM. The high PM concentrations come primarily from local sources, such as traffic and jet emissions, and from regional sources, including long-range anthropogenic emissions and dust storms. Health effects associated with PM exposure include cardiovascular and respiratory morbidity and mortality. Chronic cardiovascular and respiratory effects have been associated with PM concentrations substantially below those found at JBB, and this suggests that continued health monitoring of military personnel deployed to JBB would be appropriate.
On the basis of the CHPPM air monitoring data from JBB, PCDDs/Fs were detected at low concentrations
BOX 7-1
Limitations of and Uncertainties in Burn Pit Information
- Waste stream characterization unknowns
![]() Content
Content
![]() Volume
Volume
![]() Burn rate
Burn rate
![]() Variability
Variability
![]() Specific location and dimensions of pit
Specific location and dimensions of pit
- Air monitoring and meteorologic data
![]() Lack of monitoring for criteria air pollutants
Lack of monitoring for criteria air pollutants
![]() Meteorologic data not location-specific (not linked to sampling sites)
Meteorologic data not location-specific (not linked to sampling sites)
![]() Lack of specificity of data (no longitude and latitude for sampling sites or burn pits, airport, all housing areas, and local sources of pollutants)
Lack of specificity of data (no longitude and latitude for sampling sites or burn pits, airport, all housing areas, and local sources of pollutants)
![]() No monitoring conducted close to burn pit, so no direct sampling of burn pit emissions
No monitoring conducted close to burn pit, so no direct sampling of burn pit emissions
![]() Lack of simultaneous sampling at all sites
Lack of simultaneous sampling at all sites
![]() Lack of coordination between emissions and burn pit activities, particularly for smoke events
Lack of coordination between emissions and burn pit activities, particularly for smoke events
- Exposure information
![]() Lack of information on personnel at JBB (such as how many people worked in or near the pits, for how long, and how frequently)
Lack of information on personnel at JBB (such as how many people worked in or near the pits, for how long, and how frequently)
![]() No characterization of where people lived, ate, and worked
No characterization of where people lived, ate, and worked
![]() Highly variable characterization of how long people were at JBB
Highly variable characterization of how long people were at JBB
![]() Other sources of exposure to air pollutants (such as from kerosene heaters, cooking appliances, and airport activities)
Other sources of exposure to air pollutants (such as from kerosene heaters, cooking appliances, and airport activities)
![]() No information on possible ingestion or dermal exposures (no soil-surface samples or indoor air samples)
No information on possible ingestion or dermal exposures (no soil-surface samples or indoor air samples)
- Health effects
![]() Lack of characterization of PM to permit identification of possible health effects
Lack of characterization of PM to permit identification of possible health effects
![]() Use of surrogate populations and many uncertainties comparing exposures, duration, and frequency
Use of surrogate populations and many uncertainties comparing exposures, duration, and frequency
![]() Surrogate-population studies lack dose–response information and exposure characterization
Surrogate-population studies lack dose–response information and exposure characterization
![]() DOD epidemiologic studies:
DOD epidemiologic studies:
• Insufficient time for followup
• Looked at some relatively rare diseases for this population for long-term effects, such as birth defects, chronic multisymptom illness, lupus, and rheumatoid arthritis
in all samples, and the JBB burn pit was probably the major source of these chemicals, to judge by the measured gradient of concentrations with distance from the burn pit. The toxic equivalents of the dioxin concentrations are high compared with locations in the United States and are higher than those found in many polluted urban environments outside the United States. Health effects associated with exposure (of higher magnitudes) to dioxins and dioxin-like compounds include cancer, diabetes and other endocrine system effects, immunologic responses, neurologic effects, and reproductive and developmental effects.
The major sources of VOCs and PAHs at JBB were regional background, ground transportation, stationary power generation, and the airport on the base. The presence of these chemicals was not demonstrably associated with the burn pit, although the burn pit probably contributed to the ambient concentrations. VOC and PAH concentrations in the CHPPM monitoring study were similar to those reported in polluted urban areas outside the United
States. The measured concentrations were, in general and chemical by chemical, well below those expected to cause health effects in a population of healthy people. However, the effect of the overall mixture is not predictable with current methods.
The committee focused its literature review on long-term health outcomes in populations that were considered by the committee to have exposure to chemical mixtures that were similar to burn pit emissions: firefighters, municipal incinerator workers, and residents who lived near municipal incinerators. Although there was a wealth of epidemiologic information on health outcomes seen in firefighters, it was unclear how applicable it was to the military personnel at JBB and other military bases that had burn pits. The committee considered the risk potential for long-term health outcomes associated with combustion products in those surrogate populations and found limited or suggestive evidence of an association only for decreased pulmonary function in firefighters. Such a categorization warrants further study to develop the evidence base and support a reassessment of the strength of the association. There was insufficient or inadequate evidence of an association between exposure to combustion products and any other health effects in those surrogate populations. For all the other outcomes, the committee found inadequate or insufficient evidence of an association between long-term exposure to combustion products and specific health outcomes in the populations studied. That category can be used for a number of situations, for example, when the evidence is contradictory—that is, some well-conducted studies found an association but others did not—or when there are no key studies on which to base a conclusion and the supporting studies have substantial limitations.
As a result, the committee is unable to say whether exposures to emissions from the burn pit at JBB have caused long-term health effects. In particular, as summarized below, none of the individual chemical constituents among the combustion products emitted by the burn pit at JBB and measured in the monitoring campaigns appears to have been present at concentrations likely to be responsible for the adverse health outcomes studied in this report. However, the committee’s review of the literature and the data from JBB suggests that service in Iraq or Afghanistan—that is, a broader consideration of air pollution than exposure only to burn pit emissions—might be associated with long-term health effects, particularly in susceptible (for example, those who have asthma) or highly exposed subpopulations (such as those who worked at the burn pit). Such health effects would be due mainly to high ambient concentrations of PM from both natural and anthropogenic sources, including military sources. If that broader exposure to air pollution turns out to be relevant, potentially related health effects of concern are respiratory and cardiovascular effects and cancer. Susceptibility to the PM health effects could be exacerbated by other exposures, such as stress, smoking, local climatic conditions, and coexposures to other chemicals that affect the same biologic or chemical processes.
Individually, the chemicals measured at JBB were generally below concentrations of health concern for general populations in the United States. However, the possibility of exposure to mixtures of the chemicals raises the potential for health outcomes associated with cumulative exposure to combinations of the constituents of burn pit emissions and emissions from other sources. As a preliminary step towards understanding possible long-term health effects of multiple contaminants or cumulative exposures, the committee looked at all the detected pollutants and the target organs or specific effects associated with them. The rationale for that approach is that when multiple pollutants contribute to a common outcome, the outcome may be more likely to occur, particularly if the pollutants have the same mechanisms of action. Many of the chemicals detected at JBB have the same toxic end points; for example, several are associated with liver toxicity or respiratory effects. Some of the health effects associated with five or more of the chemicals detected at JBB include some cancers, liver toxicity and reduced liver function, kidney toxicity and reduced kidney function, respiratory toxicity and morbidity, neurologic effects, blood effects (anemia and changes in various blood-cell types), cardiovascular toxicity and morbidity, and reproductive toxicity.
As summarized above, the studies reviewed for this report provide information about chemical agents found in burn pit emissions, some at very low concentrations and some at higher concentrations, and about related health outcomes, some of little potential concern and some of greater potential concern. But the limitations and uncertainties associated with the studies cannot be overlooked. In particular, the available epidemiologic studies are inconsistent in quality, were conducted with various degrees of methodologic rigor, and had considerable variations in design and sample size. Most critical, the database on the nature and extent of exposure to combustion products is incomplete.
Those considerations should be instructive for any future epidemiologic studies of JBB and other burn pit populations or other military personnel serving in Iraq and Afghanistan. In that regard, with awareness of the data gaps and analytic limitations in the studies reviewed here, the committee recommends that the DoD and the VA give special attention to several important aspects of the studies: uncertainties and limitations in exposure assessment, the scarcity of data on the long-term health effects resulting from exposure to relevant combustion products, and differences between the best surrogate populations described in the epidemiologic literature (firefighters and municipal incinerator workers) and military personnel stationed at JBB. Related feasibility and design elements for a future epidemiologic study are discussed in Chapter 8.
REFERENCES
EPA (U.S. Environmental Protection Agency). 2003. Toxicological profile for acrolein. CASRN 107-02-8. Integrated Risk Information System (IRIS) database. http://www.epa.gov/iris/subst/0364.htm (accessed July 12, 2011).
Faulkner, W.M. 2011. Exposure to toxins produced by burn pits: Congressional data request and studies. Memorandum for the assistant secretary of defense for health affairs. Washington, DC: The Joint Staff. March 28, 2011. Enclosure: ASD(HA) Memorandum, 17 Feb 11. Response to ASD(HA) Request for Information.
IOM (Institute of Medicine). 2010. Gulf War and health: Volume 8: Update of health effects of serving in the Gulf War. Washington, DC: The National Academies Press.








