
4
Defining Cognitive Rehabilitation Therapy
In the early part of the 20th century, improvements and advancements in medical care, protective gear, evacuation procedures, and early stabilization in the field began to contribute to the increased survival of brain injured soldiers, enabling even severely injured individuals to survive and attempt to recover from brain injuries. To enhance recovery of brain injury survivors, clinicians and researchers saw the need to provide cognitive as well as physical rehabilitation. They developed a range of therapies for patients with nontraumatic brain injuries, such as stroke, that causes language (aphasia) or visuospatial skill impairments. Likewise, for traumatic brain injury (TBI), clinicians and researchers developed a range of therapies for attention, memory, and executive function impairments; treatments for social and behavioral problems; and programs for adjusting to disability.
In broad terms, rehabilitation principally focuses on the enhancement of human functioning and quality of life. In contrast, other branches of health care focus primarily on prevention and treatment of disease. Rehabilitation accepts the complex correspondence between disease and the ability to function: a disease may be eradicated while disability remains; disability can be reduced in the face of permanent injury or chronic disease. Rehabilitation is often considered in regard to improving physical disabilities. For a person with paralysis, rehabilitation might examine whether the individual’s strength could be improved through exercise, whether the tendons of nonparalyzed muscles could be surgically transferred to a mechanically
useful site, whether braces or a wheelchair might allow the person to navigate the community despite the paralysis, and even whether architectural modifications, urban planning, or transportation services could help overcome barriers to mobility. The treatment interventions used in physical rehabilitation include traditional drug and surgical treatments, as well as physical exercise, technology (e.g., braces, wheelchairs), skill training (e.g., learning how to use a wheelchair), and social policies and services (e.g., accessible transportation).
However, rehabilitation is not limited to improving physical disability. Cognitive rehabilitation attempts to enhance functioning and independence in patients with cognitive impairments as a result of brain damage or disease, most commonly following TBI or stroke. As with physical rehabilitation, cognitive rehabilitation may include interventions that aim to lessen impairments, or interventions that aim to lessen the disabling impact of those impairments. Interventions are applied through technology and other compensatory strategies that may allow the individual with cognitive impairment to accomplish important life activities and more fully participate in society.
Cognitive rehabilitation therapy (CRT) may sometimes be confused with cognitive behavioral therapy. It is important to distinguish between the two. While not mutually exclusive and sometimes delivered conjointly, these two therapies are certainly separate and distinct, differing in both treatment goals and techniques. CRT is used to rehabilitate thinking skills (e.g., attention, memory) impaired by a brain injury. Cognitive behavioral therapy is commonly used for a variety of emotional and psychiatric disorders, including mood, anxiety, and psychotic disorders, as well as sleep disturbance and chronic pain. Cognitive behavioral therapy typically centers on modifying maladaptive thoughts and emotional behaviors and using psychoeducation regarding symptoms and expectations for recovery. The latter technique also may be a component of CRT. Cognitive behavioral therapy includes training in anxiety management and how to recognize and reappraise distorted negative thoughts, and, for some disorders, exposure to anxiety-provoking or distressing stimuli with the intent of forming new adaptive emotional associations with the feared stimuli. The 2008 Institute of Medicine (IOM) report, Treatment of Posttraumatic Stress Disorder: An Assessment of the Evidence, provides a more comprehensive description of cognitive behavioral therapy.
The breadth of treatments included in CRT mirrors that of the World Health Organization’s International Classification of Functioning, Disability, and Health (WHO-ICF). As described in Chapter 1, the WHO-ICF framework recognizes impairments in body structures and functions (e.g., impaired memory) as a result of disease or injury, and limitations in activities and participation, i.e., the ability to carry out important daily activities
(e.g., remembering weekly appointments) and the ability to participate in society (e.g., employment, home, school, or community). Activity and participation limitations result when the person with the impairment(s) interacts with the physical and social environment. For example, an individual with TBI may have difficulty learning and remembering new information. With repeated training, the individual may be able learn some basic routines, such as writing appointments and other important information down in a daily planner and consulting it frequently. These routines enable the person to keep track of a schedule and other important tasks despite memory impairment. Several professional organizations endorse the use of the WHO-ICF for characterizing CRT, including the American Occupational Therapy Association, the American Physical Therapy Association, and the American Speech-Language-Hearing Association (American Occupational Therapy Association 2011; American Physical Therapy Association 2003; American Speech-Language-Hearing Association 2003b).
Specific cognitive and communication needs of patients with brain injury propelled the parallel development of CRT within multiple professional disciplines, including clinical psychology, neuropsychology, speech-language pathology, occupational therapy, physical therapy, and physiatry (i.e., rehabilitation medicine) (Prigatano 2005). Collaboration with academic colleagues in other disciplines such as cognitive psychology also occurred. The various disciplines share a common goal: each intends to help patients with cognitive impairments function more fully, either by focusing on the impairment itself or the activities affected by the impairment (as described by the WHO-ICF framework). Chapter 5 provides full descriptions of the disciplines and providers of CRT, and their approaches to treatment.
The heterogeneity of the possible interventions makes it challenging to narrowly define the concept of CRT, or how to effectively apply it. Current definitions of CRT focus on the intention to improve or accommodate one or more impaired cognitive functions, rather than on the contents or active ingredients of treatment. Intentional definitions can limit the interpretation of CRT evidence since treatment efficacy and effectiveness depend more on the contents and processes of treatment than the intention of the clinician providing it. Table 4-1 includes assembled definitions of CRT based on intent.
The most commonly referenced definition of CRT is interdisciplinary, endorsed by the Brain Injury Interdisciplinary Special Interest Group (BI-ISIG) of the American Congress of Rehabilitation Medicine (ACRM). This description allows for comprehensive, interdisciplinary rehabilitation programs with interventions to restore or reorganize function, compensate
TABLE 4-1 Definitions of Cognitive Rehabilitation Therapy by Organization
| Organization | Definition |
| Brain Injury Association of America | “Cognitive rehabilitation is a systematically applied set of medical and therapeutic services designed to improve cognitive functioning and participation in activities that may be affected by difficulties in one or more cognitive domains…. Cognitive rehabilitation is often part of comprehensive interdisciplinary programs” (Katz et al. 2006). |
| Brain Injury Interdisciplinary Special Interest Group (BI-ISIG) | “Cognitive rehabilitation is a systematic, functionally oriented service of therapeutic cognitive activities, based on an assessment and understanding of the person’s brain-behavior deficits. Services are directed to achieve functional changes by (1) reinforcing, strengthening, or reestablishing previously learned patterns of behavior, or (2) establishing new patterns of cognitive activity or compensatory mechanisms for impaired neurological systems” (Harley et al. 1992). |
| U.S. Veterans Administration (VA) | “Cognitive rehabilitation is one component of a comprehensive brain injury rehabilitation program. It focuses not only on the specific cognitive deficits of the individual with brain injury, but also on their impact on social, communication, behavior, and academic/vocational performance. Some of the interventions used in cognitive rehabilitation include modeling, guided practice, distributed practice, errorless learning, direct instruction with feedback, paper-and-pencil tasks, communication skills, computer-assisted retraining programs, and use of memory aids. The interventions can be provided on a one-on-one basis or in a small group setting” (Benedict et al. 2010). |
for impaired function through new cognitive patterns or external devices, and enable individuals to adapt to their new level of functioning. CRT may target specific cognitive domains (e.g., attention, reasoning, planning), and may be delivered in various contexts.
Differences across definitions of CRT are based on theoretical differences regarding the underlying cognitive mechanisms that result in behavioral changes. The Brain Injury Association of America, the largest U.S. advocacy organization for individuals with brain injury, summarizes this issue: “Theoretical models of cognitive rehabilitation vary along several different dimensions. Treatments may be process specific, focused on improving a particular cognitive domain such as attention, memory, language, or executive functions. Alternatively, treatments may be skill-based, aimed at improving performance of particular activities. The overall goal may be restoring function in a cognitive domain or set of domains or teaching compensatory strategies to overcome domain specific problems, improving
performance of a specific activity, or generalizing to multiple activities” (Katz et al. 2006).
CRT Attributes
This section includes descriptions of the key distinctions within CRT, which may be useful in clarifying the contents of treatment and analyzing efficacy for different types of patients. These dichotomies include modular versus comprehensive, restorative versus compensatory, and contextualized versus decontextualized treatments. These dichotomies are not mutually exclusive categories by which to classify CRT treatments; they serve as important distinctions at understanding underlying cognitive processes and ways providers have attempted to treat cognitive deficits. These approaches to CRT evolved somewhat differently, from different philosophical perspectives and for different purposes, such as treating focal versus diffuse injuries, although considerable overlap exists. Focal brain injuries, such as stroke or brain tumors, may result in one or a small number of cognitive impairments and largely spare other cognitive processes. In contrast, diffuse (i.e., multifocal) brain injuries resulting from trauma often result in multiple cognitive and behavioral impairments. Hence, an emphasis on interdisciplinary CRT for individuals with TBI is warranted.
Modular Versus Comprehensive Treatments
In modular models of CRT, treatments are generally aimed at a single cognitive impairment, such as memory (“memory remediation”) or language (“aphasia therapy”). Such treatments, when delivered alone, might be expected to enhance activities and participation most effectively in patients with a single or predominant impairment (i.e., patients with a more focal impairment). In contrast, patients with multiple impairments (i.e., deficits in attention and memory, along with impulsivity and depression) may receive a comprehensive program also referred to as “holistic,” “multi-modal,” or “neuropsychological rehabilitation.” Comprehensive programs typically contain a mix of modular treatments that target specific cognitive impairments, treatments that address self-awareness of the impact of cognitive deficits, and individual or group therapies that facilitate coping with residual deficits and their social consequences. For example, a comprehensive program for patients with moderate or severe TBI might begin with a comprehensive neuropsychological assessment, along with a patient and family interview of current difficulties in activities, social behavior, and mood. From this assessment, certain patient-specific modules might be selected. Consider a female patient who frequently becomes stalled in complex tasks and often forgets appointments and commitments. She might
receive specific individualized treatment focusing on task-related problem solving, along with training in the effective use of a daily planner. In addition, she might participate in daily group discussions with other patients about the ways in which their lives have changed; group members receive feedback and support for their attempts to cope with and adapt to those life changes. She might also receive individual psychotherapy to address depression, along with periodic joint sessions with her husband to help him understand the sources of her unreliability as well as address his own sense of the loss of his familiar partner. Specific adaptations of CRT for patients with TBI reflect the domains most commonly impaired, notably attention, memory, social communication, and executive function. Figures 4-1 and 4-2 illustrate the differences and overlap in these dichotomies.
Restorative Versus Compensatory Treatments
Restorative treatments are aimed directly at improving, strengthening, or normalizing specific impaired cognitive functions. Such treatments frequently have an “exercise-like” aspect in that they may involve intensive and repetitive use of a particular cognitive process while gradually increasing the level of difficulty or the processing demands. Patients with attention deficits may, for example, be provided with a series of computer tasks that require detection of targets on the screen at an increasing pace. Such tasks may increase in difficulty along a number of dimensions (e.g., pacing, to focus on speeded processing, or task duration, to focus on sustained attention), and the difficulty along each dimension increases as performance improves.
Compensatory treatments, in contrast, seek to provide alternative strategies for carrying out important activities of daily living despite residual cognitive impairment. The compensations may be internal, as when a person with memory impairment learns mental strategies for organizing material for better recall (e.g., learning to group items to be remembered in categories as an aide to retrieval), or external, as when such a person adopts the use of electronic reminder technology. Compensatory treatments are typically more tailored to specific needs of the individual, to the person’s willingness to use the strategy, and to the demands of specific activities. For example, strategies for remembering a list of groceries are likely to differ from strategies for retaining class material at school. In both cases, writing may be used (a grocery list versus taking notes), but the form may differ. Paper and pencil may be sufficient for a grocery list, but taking notes may need to be supplemented by audio recordings of the lecture.
There is debate over whether true restoration ever occurs or whether the behavioral improvements simply become more like the norm and thus, less visible. Because there is no “window into the brain,” it is difficult to
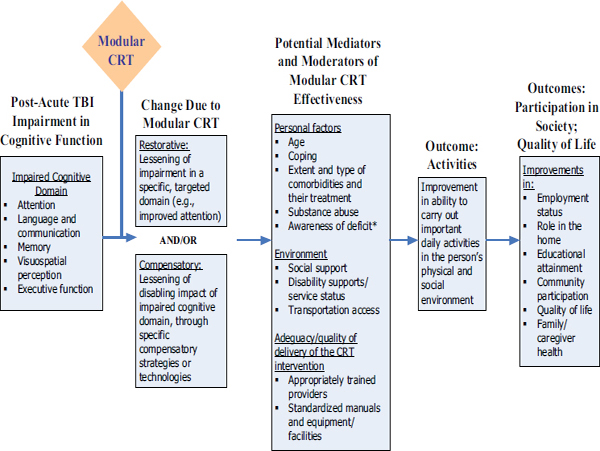
FIGURE 4-1 Model for modular CRT.
* For some domains, the CRT intervention may also target deficit awareness; for example, videotape of a social interaction followed by a critique will increase awareness of deficit in language and communication.
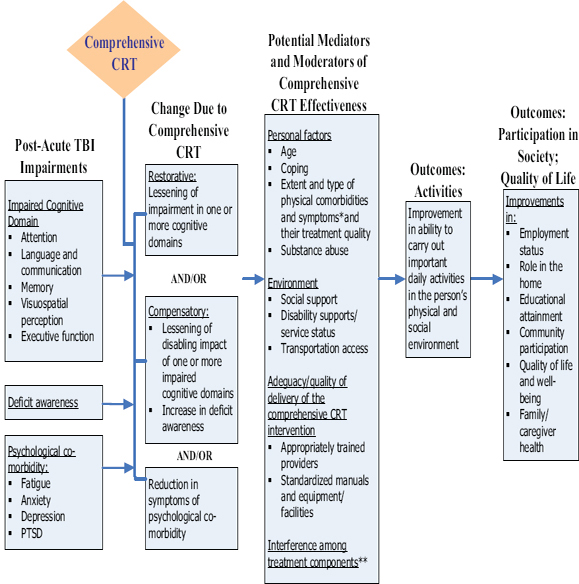
FIGURE 4-2 Model for multi-modal/comprehensive CRT.
* For example: visual impairment, headache, dizziness.
** For example: side effect of medication for depression interferes with attention.
determine if restoration of a cognitive process is possible. The ability to translate a treatment task to real-world applications is largely dependent on the circumstances of the individual with cognitive deficits. The lure of restorative approaches is that, if effective, they could impact a broad range of activities affected by the same impairment. For example, if attention capacity can truly be restored, then all of the activities suffering from inattention would likely improve. Compensatory strategies tend to be designed around important activities rather than around the impairment itself and, therefore, tend to be more local solutions. However, the impact of compensatory strategies may be more visible, since task accomplishment serves as direct evidence of the success of the strategy.
Contextualized Versus Decontextualized Treatments
CRT interventions also differ in the degree to which they take place in the real world or use materials and tasks from the patient’s everyday life. Decontextualized assessment and treatment targets specific cognitive processes often using artificial treatment tasks, such as pressing a key when a computer presents a number but not a letter. This artificial task attempts to enhance attention. Another artificial task is repeating words in lists of increasing length in attempt to improve working memory span. Decontextualized approaches provide more opportunity for pure manipulation of a single dimension, on the assumption that specific cognitive processes can be isolated and treated somewhat independently from each other. However, attempting to train attention during a cooking task may reveal obstacles related to manual coordination in slicing and chopping, planning and sequencing of the cooking steps, and reading the instructions (Adamovich 1998; Sohlberg and Mateer 2001).
Contextualized therapy addresses cognitive impairments as they disrupt activities and skills in various milieus (American Speech-Language-Hearing Association 2003a; Hartley 1995; Ylvisaker and Feeney 1998). For example, a contextualized treatment may include a focus on driving to observe the occasions in which the patient appears to be distracted from the driving task, allowing for an opportunity to provide specific feedback about how to manage these difficulties (e.g., “When you approach an intersection, you should stop talking to your passenger.”). It has been argued that contextualized treatments that occur within a familiar environment, or deal with personally important tasks, are likely to enhance motivation for treatment, improve self-awareness of strengths and weaknesses, and ensure that the strategies learned are applicable to the patient’s personal situation. However, such treatments are more cumbersome to deliver than those based on standardized materials that can be delivered in a clinic or office.
Contextualized treatments also are more difficult to evaluate, standardize, and disseminate because doing so requires the therapist to have the skills necessary to design and execute them, and generally requires more availability/effort from the patient. A decontextualized attention training program can be a specific computer program with internal rules for task progression, which is disseminated in standard form. In contrast, contextualized attention training would be an approach to finding out what activities are most disrupted by inattention from the individual patient, how to simplify those activities during training, and how to assess progress.
Application of CRT Attributes
Attributes of CRT are not mutually exclusive options, and various attributes can be combined in a multitude of ways. Modular treatments, for example, can be aimed at either restoration or compensation. One treatment might consist of a hierarchical set of “attention exercises” designed to strengthen attentional capacities. Alternatively, one might provide compensations such as unpredictable auditory tones to alert an inattentive patient, training the patient to ask a speaker to repeat a point, or having the patient work in a quiet environment. Comprehensive programs may contain a mix of both restorative and compensatory treatment types. Modular treatments can also be either contextualized or decontextualized. As noted, modular treatments aimed at restoration, in particular, are likely to be decontextualized, in that they may seek to abstract the essence of a cognitive process from its natural context to more tightly focus the treatment. Compensatory modular treatments, however, such as training in memory strategies, are often applied to the real-world activities the patient faces.
Implications of CRT Attributes on Treatment and Research
Practitioners and researchers acknowledge that the ultimate goal of treatment should be functionally meaningful improvements in the patient (i.e., activities, participation, or quality of life), and there may be many approaches to reaching this goal (Sohlberg and Mateer 2001). A one-size-fits-all method of treatment may not be effective because of the heterogeneity of injuries, differences in premorbid personal, social, and environmental circumstances, and differences in the activities of importance to individual patients. Heterogeneity of TBI further complicates studies of CRT impact and may mask benefit in subgroups that the study cannot detect due to small sample size or other limitations in study design.
In general, CRT attributes may shape expectations about the types of possible treatment outcomes and the types of patients most likely to benefit, and therefore may be useful for clinical reasoning; however, rehabilitation
professionals often use a variety of therapy approaches, providing interventions that target activities and participation while systematically addressing the underlying cognitive impairment(s). For example, individuals may benefit from intensive practice of memory encoding strategies (modular, decontextualized, compensatory) to bolster remembering new information, while also practicing applying these strategies to various types of material and in various contexts (modular, contextualized, compensatory). Alternatively, a modular treatment may not have substantial impact on activities and participation in a patient with multiple impairments unless other coexisting cognitive and emotional factors are concurrently addressed, as in a comprehensive program. Likewise, a contextualized, compensatory treatment may not restore an underlying cognitive impairment or even impact behavior change in an environment beyond where the strategy was taught.
These treatment attributes also affect the feasibility and design of research that might advance the evidence regarding CRT. For patients with multifocal or diffuse injuries, evaluation of the effectiveness of CRT in terms of real clinical impact faces a particular challenge. Even highly efficacious modular treatments may have impact on specific measures of the targeted impairment, but may fail to show improvement in real-world activities, participation, or quality of life. For example, if attention can be substantially improved in a patient who still has memory deficits, difficulty solving problems, and inappropriate social behavior, this may have little impact on employment or the development of social relationships. Comprehensive treatment programs, by targeting multiple impairments as well as skills for coping with residual impairments, may have more substantial life impact, but they provide no insight into the necessary or sufficient ingredients for a successful treatment outcome.
These attributes also affect the experimental designs that are most applicable and feasible for advancing the science of CRT. Specifically, modular restorative treatments are relatively amenable to randomized controlled trials (RCTs). In an RCT, therapists can design similar appearing treatments that differ in the active ingredients and deliver one treatment or the other at random to research subjects. For example, to assess whether “continued attention deficits” is a critical attention challenge, a study may compare a program with static attention exercises with a progressive program that advances with patient improvement.
RCTs involving comprehensive treatments are more difficult to design and execute, because of the need to distill a multifaceted treatment, often individually tailored, into standard form. A study evaluating comprehensive treatment programs ideally will include a manual specifying the rules that link assessment to selection of specific treatment elements, and how those elements will be advanced or tailored to individual performance. It is difficult to deliver a control treatment in this case, since plausible but
inert treatments of a compensatory nature are modified to the person or environment and are more likely to be tailored to each patient’s specific task priorities. Furthermore, such treatment programs are expensive to provide without clinical revenue, which would preclude intentionally designing an ineffective comparison treatment.
CRT is an umbrella term for a group of interventions that are used to support or ameliorate cognitive impairments, as well as the changes that occur in everyday functioning as a result of these impairments. Patients with TBI often have multiple identifiable cognitive impairments, coupled with mood or other behavioral disturbances, a reduced awareness of their own cognitive and behavioral limitations, and reductions in social competence. Although some patients with isolated impairments may achieve substantial treatment benefits in terms of activities and participation from treatment of a single deficit, others may require a combination of treatments aimed at multiple problems to achieve comparable outcomes. The heterogeneous array of treatments available, as well as the lack of a unified theoretical framework for defining and quantifying them, makes definitive evaluation of their effectiveness particularly challenging.
Adamovich, B. B. 1998. Functional outcome assessment of adults with traumatic brain injury. Seminars in Speech & Language 19(3):281–290.
American Occupational Therapy Association. 2011. Occupational Therapy’s Role in Adult Cognitive Disorders. http://www.aota.org/Practitioners/PracticeAreas/Rehab/Tools/Cognition.aspx?FT=.pdf (accessed May 26, 2011).
American Physical Therapy Association. 2003. What types of tests and measures do physical therapists use? In Interactive Guide to Physical Therapist Practice. American Physical Therapy Association. Pp. 43–53.
American Speech-Language-Hearing Association. 2003a. Code of Ethics (revised). ASHA Supplement 23:13–15.
———. 2003b. Rehabilitation of Children and Adults with Cognitive-Communication Disorders After Brain Injury [technical report]. http://www.asha.org/docs/html/TR2003-00146.html (accessed May 26, 2011).
Benedict, S. M., H. G. Belanger, S. D. Ceperich, D. X. Cifu, M. Cornis-Pop, H. L. Lew, and K. Meyer. 2010. Veterans Health Initiative on Traumatic Brain Injury. U.S. Department of Veterans Affairs.
Harley, J. P., C. Allen, T. L. Braciszewski, K. D. Cicerone, C. Dahlberg, S. Evans, M. Foto, W. A. Gordon, D. Harrington, W. Levin, J. F. Malec, S. Millis, J. Morris, C. Muir, J. Richert, E. Salazar, D. A. Schiavone, and J. S. Smigelski. 1992. Guidelines for cognitive rehabilitation. NeuroRehabilitation 2(3):62–67.
Hartley, L. L. 1995. Cognitive-Communicative Abilities Following Brain Injury: A Functional Approach. San Diego: Singular Publishing Group.
IOM (Institute of Medicine). 2008. Treatment of Posttraumatic Stress Disorder: An Assessment of the Evidence. Washington, DC: The National Academies Press.
Katz, D. I., M. Ashley, G. J. O’Shanick, and S. H. Connors. 2006. Cognitive Rehabilitation: The Evidence, Funding, and Case for Advocacy in Brain Injury. McLean, VA: Brain Injury Association of America.
Prigatano, G. P. 2005. A history of cognitive rehabilitation. In The Effectiveness of Rehabilitation for Cognitive Deficits. Edited by P. W. Halligan and D. T. Wade. New York: Oxford University Press. Pp. 3–11.
Sohlberg, M. M., and C. A. Mateer. 2001. Improving attention and managing attentional problems: Adapting rehabilitation techniques to adults with ADD. Annals of the New York Academy of Sciences 931:359–375.
Ylvisaker, M., and T. Feeney. 1998. Collaborative Brain Injury Intervention: Positive Everyday Routines. 1st ed. San Diego: Singular Publishing Group.
This page intentionally left blank.














