
BACKGROUND
The number of people living with HIV/AIDS (PLWHA) in the United States is growing each year largely due both to advances in treatment that allow HIV-infected individuals to live longer and healthier lives and to a steady number of new HIV infections each year. The U.S. Centers for Disease Control and Prevention (CDC) estimates that there were 1.2 million people living with HIV infection in the United States at the end of 2008, the most recent year for which national prevalence data are available. As a disease that disproportionately affects populations who already have a range of care and supportive service needs, now more than ever HIV requires continuous and coordinated quality care. Furthermore, there continue to be challenges to curbing the toll of the epidemic. Each year, approximately 16,000 individuals die from AIDS despite overall improvements in survival, and 50,000 individuals become newly infected with HIV. In 2011, the CDC estimated that about three in four people living with diagnosed HIV infection are linked to care within 3 to 4 months of diagnosis and that only half are retained in ongoing care. Treatment with antiretroviral therapy (ART) can help to reduce the level of HIV virus in the blood, sometimes to viral suppression (i.e., to an undetectable level), resulting in improved health outcomes for PLWHA as well as reduced risk of HIV transmission. Yet, only 19–28 percent of PLWHA are virally suppressed.
______________
1This summary does not include references. Citations to support text, conclusions, and recommendations made herein are given in the body of the report.
The National HIV/AIDS Strategy and the Patient Protection and Affordable Care Act
In the context of the continuing challenges posed by HIV, the White House Office of National AIDS Policy (ONAP) released a National HIV/AIDS Strategy (NHAS) for the United States in July 2010. The primary goals of the NHAS are to
- reduce HIV incidence;
- increase access to care and optimize health outcomes for PLWHA; and
- reduce HIV-related health disparities.
Federally run HIV programs traditionally have been administered in a siloed fashion due to differences in the missions of the agencies within which they originate or in funding stream requirements. Meeting the NHAS objectives will require increased synergy of HIV programs across federal agencies, and among federal agencies, states, and other jurisdictions. As such, the NHAS includes a fourth objective to increase coordination of HIV program activities across levels of government. Subsumed within this objective is the development of improved mechanisms to monitor progress in achieving the NHAS goals. In the agency operational plans for the NHAS, this Institute of Medicine (IOM) report is named as one of the activities that ONAP is undertaking to address existing gaps in the collection, analysis, and integration of data on the care and treatment experiences of PLWHA.
The NHAS is intended to build upon the Patient Protection and Affordable Care Act (ACA), which—if implemented as originally planned—is expected to bring millions of uninsured individuals, including many PLWHA, into the health care system. Examples of provisions of the ACA that may increase access to care for PLWHA include changes in eligibility requirements for public (e.g., Medicaid) and private health insurance, reduced out-of-pocket costs for Medicare Part D prescription drugs, expansion of coverage for preventive health services, and increased care capacity in community health centers.
CHARGE TO THE COMMITTEE
ONAP requested that the IOM convene a committee to identify critical data and indicators related to continuous HIV care and access to supportive services, as well as to monitor the impact of the NHAS and the ACA on improvements in HIV care. In addition, the committee was tasked with identifying public and private data systems that capture the data needed to
estimate these indicators. The committee was also asked to address a series of specific questions related to the collection, analysis, and dissemination of such data (Box S-1). The IOM convened a committee of 17 members with expertise in HIV clinical care and supportive services, health policy, data collection and analysis, informatics, and other relevant areas to respond to this charge.
COMMITTEE’S APPROACH TO ITS CHARGE
NHAS targets for increasing access to care and improving health outcomes for PLWHA and for reducing HIV-related health disparities by 2015 (Box S-2) provided the basis for several of the indicators recommended by the committee.2 The committee also reviewed existing indicators of HIV care and measures of HIV care quality. These include Healthy People 2020 objectives and President’s Emergency Plan for AIDS Relief (PEPFAR) indicators that pertain to HIV care and supportive services, as well as performance measures for HIV care that were endorsed by the National Quality Forum, an organization that sets national consensus standards of performance in health care. The committee also reviewed current guidelines for HIV treatment. The committee identified indicators linked to benchmarks along the continuum of HIV care, from diagnosis through virologic suppression (Figure S-1).
The committee compiled a list of 32 public and private data systems and data collection agencies, including ones highlighted in the project proposal from ONAP and others identified by the committee as potentially important sources of information on HIV care and supportive services. The committee reviewed both HIV-specific data systems and data collection activities, such as epidemiologic studies of PLWHA and Ryan White HIV/AIDS Program data, and those that are not HIV specific but capture information on care received by PLWHA, such as Medicaid and Medicare claims data. The committee requested information from individuals who are familiar with the data systems and data collection activities in the areas of HIV testing and linkage to care, clinical care, access to care, treatment and adherence, financial security, need for supportive services, demographics, risk behavior assessment, and patient experience with care. The committee then compared the compiled information against the data elements needed to estimate the indicators to identify the best sources of
______________
2The committee interpreted its charge as focusing on the population of people living with HIV/AIDS (PLWHA) who have been diagnosed with HIV. Therefore, the committee did not identify indicators to monitor the National HIV/AIDS Strategy (NHAS) objective related to reducing the occurrence of new HIV infections, although some of the indicators promote reduced HIV transmission as well as improved health outcomes for PLWHA.
The White House Office of National AIDS Policy has requested that the Institute of Medicine (IOM) convene a committee of experts to assess available public and private data systems that capture information about HIV care to investigate ways to maximize their usefulness and recommend approaches for supplementing current data sources and to identify and provide recommendations for the most critical data and indicators to gauge the impact of the National HIV/AIDS Strategy and the Patient Protection and Affordable Care Act in improving HIV/AIDS care.
1. What are the best sources of data (and which data elements should be used) from public and private HIV care databases to assess core indicators related to continuous care and access to support services, such as housing, for people living with HIV?
a. What data collection items need to be revised or reconsidered in existing databases of care and services provided to people living with HIV and in demographic data about populations receiving these services? Are there proposed changes that can provide necessary data without adding additional burden to data collection?
b. What is the difference between claims data and clinical data found in medical records and do these differences encompass gaps in measures for HIV care?
2. What similar data collection or standardization efforts are currently under way by public agencies or private industry that should be tapped?
3. How do we regularly obtain data (core indicators) that capture the care experiences of people living with HIV without substantial new investments?
4. What situations may impose barriers to the collection of core indicators?
a. What policies, reimbursement issues or reporting issues need to be addressed to collect necessary data?
b. How can data be collected in a way that will not significantly increase provider burden?
5. How can federal agencies efficiently analyze care indicators and disseminate data to improve HIV care quality?
6. What models or best practices in data system integration can be gleaned from public agencies or private industry to make existing data systems and core indicators interoperable?
a. Which among these models or combination of models would be most cost effective?
7. How should health information technology (including electronic medical records) be utilized or configured in order to improve the collection of comprehensive data describing the care experiences of people living with HIV?
BOX S-2
National HIV/AIDS Strategy Targets
Targets for Increasing Access to Care and Improving Health Outcomes for People Living with HIV
By 2015,
- increase the proportion of newly diagnosed patients linked to clinical care within 3 months of their HIV diagnosis from 65 to 85 percent.
- increase the proportion of Ryan White HIV/AIDS Program clients who are in care (at least two visits for routine HIV medical care in 12 months at least 3 months apart) from 73 to 80 percent.
- increase the percentage of Ryan White HIV/AIDS Program clients with permanent housing from 82 to 86 percent.
Targets for Reducing HIV-Related Health Disparities and Inequities
By 2015,
- increase the proportion of HIV diagnosed gay and bisexual men with undetectable viral load by 20 percent.
- increase the proportion of HIV-diagnosed Black Americans with undetectable viral load by 20 percent.
- increase the proportion of HIV diagnosed Latinos with undetectable viral load by 20 percent.
data for gauging the impact of the NHAS and ACA on improvements in HIV care.
The committee’s information gathering for the remaining aspects of its charge consisted of presentations before the committee during its open sessions and review of the research literature.
COMMITTEE’S RECOMMENDATIONS
Core Indicators Related to Continuous HIV Care and Access to Supportive Services
The committee concluded that the primary challenges to optimal health outcomes for PLWHA include late diagnosis, delayed linkage to care for HIV, poor retention in care, delayed initiation of ART, and poor adherence to ART (i.e., discontinuing or intermittent use of ART), as well as untreated non-HIV comorbidities (e.g., substance abuse, hepatitis C), and unmet basic needs (e.g., housing, food, or transportation assistance needs). The commit-
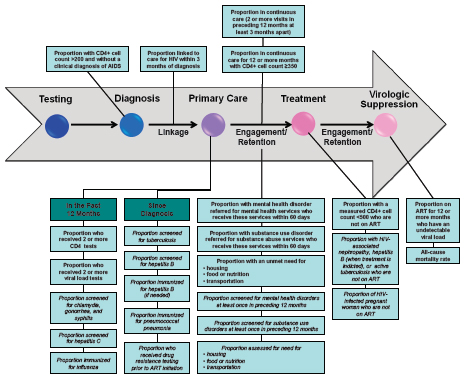
FIGURE S-1 Continuum of HIV care arrow mapped to indicators of HIV care and supportive services.
NOTE: Indicators in bold text correspond with the committee’s recommended core indicators, while the indicators in italics correspond with the additional indicators. More information on the committee’s selection of both core and additional indicators can be found in Chapter 2.
tee identified a set of core indicators that can be used to measure the degree to which these challenges are being addressed across the continuum of HIV care and to monitor the impact of the NHAS and ACA on improvements in HIV care (Table S-1 provides the committee’s rationale for each of the core indicators).
Recommendation 2-1. The Department of Health and Human Services should use the following core indicators to assess the impact of the National HIV/AIDS Strategy and the Patient Protection and Affordable Care Act on improving HIV/AIDS care and access to supportive services for individuals with HIV:
Core Indicators for Clinical HIV Care
Proportion of people newly diagnosed with HIV with a CD4+ cell count >200 cells/mm3 and without a clinical diagnosis of AIDS
Proportion of people newly diagnosed with HIV who are linked to clinical care for HIV within 3 months of diagnosis
Proportion of people with diagnosed HIV infection who are in continuous care (two or more visits for routine HIV medical care in the preceding 12 months at least 3 months apart)
Proportion of people with diagnosed HIV infection who received two or more CD4 tests in the preceding 12 months
Proportion of people with diagnosed HIV infection who received two or more viral load tests in the preceding 12 months
Proportion of people with diagnosed HIV infection in continuous care for 12 or more months and with a CD4+ cell count. 350 cells/mm3
Proportion of people with diagnosed HIV infection and a measured CD4+ cell count <500 cells/mm3 who are not on ART
Proportion of people with diagnosed HIV infection who have been on ART for 12 or more months and have a viral load below the level of detection
All-cause mortality rate among people diagnosed with HIV infection
Core Indicators for Mental Health, Substance Abuse, and Supportive Services3
Proportion of people with diagnosed HIV infection and mental health disorder who are referred for mental health services and receive these services within 60 days4
Proportion of people with diagnosed HIV infection and substance use disorder who are referred for substance abuse services and receive these services within 60 days5
Proportion of people with diagnosed HIV infection who were homeless or temporarily or unstably housed at least once in the preceding 12 months6
Proportion of people with diagnosed HIV infection who experienced food or nutrition insecurity at least once in the preceding 12 months7
______________
3As discussed in Chapter 2, the committee found that the indicators for supportive services may be particularly difficult to measure. However, there is evidence from research that addressing need for housing, food security, and other supportive services is effective for retention in care and improving health outcomes among people with HIV. In addition, the committee was specifically asked to address core indicators relating to “access to support services, such as housing,” as well as those relating to continuous care. The fact that indicators for supportive services may be difficult to estimate did not preclude the committee from including them as core indictors.
4Receipt of care within 30 days would reflect optimal care, but 60 days is more realistic given the current limited capacity of many providers to see new patients within a shorter time frame. Urgent cases should be seen as soon as possible.
5See footnote 4 above.
6The U.S. Department of Housing and Urban Development’s Homeless Management Information System (HMIS) Data Standards provide guidance for classifying housing status in four categories: literally homeless (e.g., lack a regular nighttime residence, staying in an emergency shelter), following the McKinney-Vento Homeless Assistance Act (42 U.S.C. 11302, Sec. 103) definition of homelessness, as amended by the Homeless Emergency Assistance and Rapid Transition to Housing (HEARTH) Act of 2009 (P.L. 111-22, div. B, Sec. 1003); imminently losing housing (e.g., being evicted or being discharged from an institution with no housing options identified); unstably housed and at-risk of losing housing (e.g., temporarily doubled up with others, moving frequently for economic reasons); and stably housed (http://www.hudhre.info/documents/FinalHMISDataStandards_March2010.pdf, accessed March 12, 2012).
7According to the U.S. Department of Agriculture, households with high food security have “no reported indications of food-access problems or limitations”; households with marginal food security have “one or two reported indications—typically of anxiety over food sufficiency or shortage of food in the house [with] little or no indication of changes in diets or food intake”; households with low food security have “reports of reduced quality, variety, or desirability of diet [with] little or no indications of reduced food intake”; and households with very low food security have “reports of multiple indications of disrupted eating patterns and reduced food intake.” The lower two levels indicate food insecurity (http://www.ers.usda.gov/briefing/foodsecurity/labels.htm#cnstat, accessed March 12, 2012).
Proportion of people with diagnosed HIV infection who had an unmet need for transportation services to facilitate access to medical care and related services at least once in the preceding 12 months
In addition to the core indicators, the committee identified a set of additional indicators based on more granular process measures to provide a comprehensive assessment of the quality of HIV care. These additional indicators are included in Figure S-1 and discussed in detail in Chapter 2 of the report.
Demographic data on PLWHA have to be collected to monitor the impact of the NHAS and ACA on improvements in HIV-related health disparities. The committee found that many crucial data elements, such as gender identity, sexual orientation, sexual risk behaviors, geographic marker of residence, income, primary means of reimbursement for medical services, and level of acculturation as reflected in primary language are not routinely collected in many of the federal data systems that it reviewed. Data on race and ethnicity often are not collected with a sufficient level of detail to make nuanced distinctions among the health needs of different racial and ethnic groups. On October 31, 2011, the U.S. Department of Health and Human Services (HHS) issued new guidance on minimum standards for collection of data on race, ethnicity, sex, primary language, and disability status in national population health surveys that are sponsored or conducted by HHS. The guidance mandates the collection of more granular data on race and ethnicity, as well as data on “biologic sex” and English proficiency as a measure of primary language. HHS is also developing a plan to integrate the collection of data on sexual orientation and gender identity into HHS national surveys, and to collect data on socioeconomic status.
Recommendation 2-2. The Department of Health and Services and the Office of Management and Budget should continue to expand the demographic data elements to be captured by federal data systems relevant to HIV care to permit calculation of the indicators for subgroups of the population of people with diagnosed HIV infection, including, but not limited to, the following:
Age
Race
Ethnicity
Sex (assigned at birth)
Gender identity (e.g., male, female, transgender [male-to-female, female-to-male], bigender, gender queer)
Core Indicators for HIV Clinical Care
Proportion of people newly diagnosed with HIV with a CD4+ cell count >200 cells/mm3 and without a clinical diagnosis of AIDS
Rationale: Improve health outcomes by reducing the number of people living with HIV/AIDS (PLWHA) with late diagnosis.
Proportion of people newly diagnosed with HIV who are linked to clinical care for HIV within 3 months of diagnosis
Rationale: Timely linkage to care improves individual health outcomes and reduces transmission of the virus to others.
Proportion of people with diagnosed HIV infection who are in continuous care (two or more visits for routine HIV medical care in the preceding 12 months at least 3 months apart)
Rationale: Continuous HIV care results in better outcomes, including decreased mortality, and reduced transmission of the virus to others.
Proportion of people with diagnosed HIV infection who received two or more CD4 tests in the preceding 12 months
Rationale: Regular CD4 testing permits providers to monitor individuals’ immune function, determine when to start antiretroviral therapy (ART), and assess the need for prophylaxis for opportunistic infections.
Proportion of people with diagnosed HIV infection who received two or more viral load tests in the preceding 12 months
Rationale: Regular viral load (plasma HIV RNA) testing is important for monitoring clinical progression of the disease and therapeutic response in individuals on ART.
Proportion of people with diagnosed HIV infection in continuous care for 12 or more months and with a CD4+ cell count ≥350 cells/mm3
Rationale: Achieving and maintaining a CD4+ cell count ≥350 cells/mm3 reduces the risk of complicating opportunistic infections and cancers.
Proportion of people with diagnosed HIV infection and a measured CD4+ cell count ∠500 cells/mm3 who are not on ART*
Rationale: Appropriate initiation of ART improves individual health outcomes and reduces transmission of the virus to others.
Proportion of people with diagnosed HIV infection who have been on ART for 12 or more months and have a viral load below the level of detection
Rationale: The goal of ART is durable virologic suppression, which improves health outcomes and reduces transmission of the virus.
All-cause mortality rate among people diagnosed with HIV infection*Rationale: Mortality rate is the ultimate outcome measure for people diagnosed with HIV infection. Mortality among PLWHA should be inversely related to the quality of overall care delivered.
Core Indicators for Mental Health, Substance Abuse, and Supportive Services
Proportion of people with diagnosed HIV infection and mental health disorder who are referred for mental health services and receive these services within 60 days**
Rationale: Untreated mental health disorders can negatively affect maintenance in care, adherence to treatment, and health outcomes for PLWHA and may increase the risk of transmitting the virus to others.
Proportion of people with diagnosed HIV infection and substance use disorder who are referred for substance abuse services and receive these services within 60 days**
Rationale: Untreated substance use disorders can negatively affect maintenance in care, adherence to treatment, and health outcomes for PLWHA and may increase the risk of transmitting the virus to others.
Proportion of people with diagnosed HIV infection who were homeless or temporarily or unstably housed at least once in the preceding 12 months*
Rationale: Homelessness and housing instability negatively affect maintenance in care, adherence to treatment, and health outcomes for PLWHA and may increase the risk of transmitting the virus to others.
Proportion of people with diagnosed HIV infection who experienced food or nutrition insecurity at least once in the preceding 12 months*
Rationale: Food insecurity affects maintenance in care, adherence to treatment, and health outcomes for PLWHA and may increase the risk of transmitting the virus to others. Poor nutrition affects absorption of medications and can contribute to diet-sensitive comorbidities.
Proportion of people with diagnosed HIV infection who had an unmet need for transportation services to facilitate access to medical care and related services at least once in the preceding 12 months*
Rationale: Unmet need for transportation to access HIV health care and related services negatively affects treatment access, service utilization, and health outcomes for PLWHA and may increase the risk of transmitting the virus to others.
*In contrast to the other indicators, the estimates for these indicators should decrease with improved access to care and supportive services.
**Receipt of care within 30 days would reflect optimal care, but 60 days is more realistic given the current limited capacity of many providers to see new patients within a shorter time frame. Urgent cases should be seen as soon as possible.
Sexual orientation (e.g., heterosexual, homosexual, bisexual)
Current geographic marker of residence (e.g., current address, zip code, partial zip code, census block)
Income or poverty level
Primary means of reimbursement for medical services (including Medicaid, Medicare, Ryan White HIV/AIDS Program, private insurance or health maintenance organization, no coverage)
In addition, HHS should, to the extent practicable, extend its expanded data collection standards beyond national population-based health surveys to all HHS-sponsored data collection activities.
Sources of Data on HIV Care to Assess Core
Indicators and Access to Supportive Services
Data on HIV care and supportive services are currently being collected by a number of public and private data systems. Although no single data system on its own provides all of the data needed to estimate the indicators recommended by the committee (listed above), these data systems as a whole are collecting relevant information that can serve as a collective platform for evaluating access to continuous and high-quality care in all populations of PLWHA. The committee identified 12 data systems in particular that collect data of use for estimating the core indicators to monitor progress toward meeting the goals of the NHAS and ACA:
National HIV Surveillance System (CDC)
Medical Monitoring Project (CDC)
Ryan White Services Report (Health Resources and Services Administration [HRSA])
Ryan White AIDS Drug Assistance Program Reports (HRSA)
Medicaid Statistical Information System (Centers for Medicare and
Medicaid Services [CMS])
Chronic Condition Data Warehouse (CMS)
North American AIDS Cohort Collaboration on Research and Design
CFAR Network of Integrated Clinical Systems
HIV Research Network
Clinical Case Registry: HIV (Department of Veterans Affairs)
Kaiser Permanente
National Vital Statistics System
The committee identified two additional data systems that provide information of use in tracking the impact of the NHAS and ACA on care for two small but important subpopulations of PLWHA (American Indians and Alaskan Natives; federal prisoners), and a third that provides information relevant to housing assistance and other supportive services for PLWHA:
Resource and Patient Management System (Indian Health Service)
Bureau of Prisons Electronic Medical Record
Housing Opportunities for Persons with AIDS (U.S. Department of Housing and Urban Development)
The committee’s review showed that each data system has limitations. For example, few contain all of the data elements needed to estimate all of the indicators recommended by the committee, especially those for mental health, substance abuse, and supportive services (housing, food security, transportation). In addition, most of the data systems are not fully representative of the population of PLWHA in the United States. In many cases (e.g., Ryan White HIV/AIDS Program, Medicaid Statistical Information System [MSIS], Chronic Condition Data Warehouse [CCW], Clinical Case Registry: HIV), the population represented in the data system is defined by program eligibility and cannot be expanded. Similarly, the purposes for which the data systems were designed preclude expansion of the data elements they collect to include all of those needed to estimate all of the indicators identified by the committee. Modest changes in individual data systems, however, could improve the usefulness of their data for tracking changes in HIV care and access to supportive services for PLWHA. For example, a given data system might add one or more data elements or modify an existing data element to allow the system to provide data for estimating a subgroup of the indicators identified by the committee, such as those pertaining to supportive services, or to simplify identification of data representing HIV-infected individuals (e.g., flagging HIV/AIDS as a chronic condition in the CCW). In cases where the population represented in a data system is not constrained by the program it serves (e.g., Medical Monitoring Project), steps might be taken either to make the population more representative of the national population of PLWHA or to include groups (e.g., homeless) who are less apt to be represented in other data systems.
Recommendation 3-1. The Department of Health and Human Services, the Department of Veterans Affairs, the Department of Housing and Urban Development, and other relevant federal agencies should review and, to the extent practicable, modify the federal data systems identified by the committee to better enable them to be used for monitoring progress toward achieving the goals of the National HIV/AIDS Strategy.
Currently there is variation among CDC reporting areas with respect to longitudinal reporting of CD4 and viral load test dates and results. Uniform longitudinal reporting of CD4 and viral load test dates and results from all jurisdictions would facilitate the use of data from the National HIV Surveillance System (NHSS) to estimate the core indicators for HIV care identified by the committee. In addition, collection of longitudinal data on the initiation and ongoing prescription or dispensing of antiretroviral therapy for individuals diagnosed with HIV would provide the remaining data elements necessary to use the NHSS as a source of data to estimate all of the core clinical HIV care indicators. Use of NHSS data would permit estimation of the indicators for the majority of the population diagnosed with HIV in the United States, as well as for subpopulations based on race, ethnicity, sex, gender, age, geographic area, and country of origin. Capturing information on sexual orientation, sources of coverage for medical treatment, and current geographic area of residence would facilitate use of NHSS data for evaluation of indicators for specific subpopulations identified in the NHAS.
Recommendation 3-2. The Centers for Disease Control and Prevention should take steps to enhance the National HIV Surveillance System including
• issuing guidelines or criteria for National HIV Surveillance System reporting to include all CD4 and viral load test results
• capturing longitudinal data pertaining to the initiation and ongoing prescription or dispensing of antiretroviral therapy for individuals diagnosed with HIV (e.g., through pharmacy-based reporting)
• obtaining information on sexual orientation and sources of coverage for medical treatment (including, but not limited to, Medicaid, Medicare, Ryan White HIV/AIDS Program, other public funding, private insurance or health maintenance organization, no coverage) and obtaining and employing current geographic marker of residence (e.g., current address, zip code, partial zip code, census block) for individuals in the National HIV Surveillance System
Clinically based electronic health record (EHR) systems, such as those used by the Veterans Health Administration (VHA) and Kaiser Permanente, capture all, or most, of the data elements needed to estimate the clinical HIV care indicators recommended by the committee. They also generally capture at least some of the information needed to estimate the indicators pertaining to mental health and substance abuse, but they do not routinely capture data needed to estimate the indicators pertaining to supportive services. Another limitation of provider-based EHR systems is that individually each represents only one segment of the population of PLWHA in the United States (e.g., those who receive care in the VHA system, Kaiser Permanente enrollees). Other data systems represent larger proportions of PLWHA nationally (e.g., NHSS, MSIS) and may contain information on mental health, substance abuse, and supportive services (e.g., Ryan White HIV/AIDS Program, MSIS), but they contain limited or no clinical data. The National Health Information Network Exchange is an example of a partnership between public and private entities to exchange health information for a variety of purposes. It could serve as a model for or a foundation upon which to build a broader data sharing partnership among public and private data systems both to permit better estimation of the indicators identified by the committee and to return information to private health care systems and providers for the purpose of improving health care for individuals with HIV. Building upon existing data sharing partnerships would help to reduce costs associated with implementation of such partnerships for the exchange of information relevant to the provision of HIV care.
Recommendation 3-3. The Department of Health and Human Services, the Department of Veterans Affairs, the Indian Health Service, the Federal Bureau of Prisons, and other relevant federal agencies should use existing data from private data systems, including data from electronic health records, to monitor the impact of the National HIV/AIDS Strategy and the Patient Protection and Affordable Care Act on improving HIV care. Federal agencies also should share data pertaining to HIV care with private health care systems and providers to improve the quality of care for individuals with HIV. Methods might include the development of a data sharing partnership between public and private data systems that include data pertaining to HIV care.
Barriers to the Collection of HIV Care Data
Grantees of federally funded HIV/AIDS programs are a vital source of HIV care and supportive services data, but are currently overburdened by the many reporting obligations they are required to fulfill as a condition of program funding. The reporting requirements for core and supplemental
HIV/AIDS programs administered by health departments are often project specific, even across related programming (e.g., HIV prevention and HIV/AIDS care), requiring staff to modify their reporting practices for each grant. Reporting is further complicated by the fact that programs operate on different grant cycles so that reports for related programs are due at different times during the year. According to the Presidential Advisory Council on HIV/AIDS, the current reporting requirements for grantees of federally funded HIV/AIDS programs have not resulted in a set of metrics by which to thoroughly monitor the HIV epidemic or to evaluate federal HIV/AIDS programs. A smaller number of metrics that are aligned with NHAS goals could be used across federal agencies to monitor progress in managing the epidemic. As it was preparing this report, the committee learned that there is an effort under way by HHS to identify a set of HIV-related metrics to be used across funding agencies and reduce reporting burden for program grantees. The committee supports this current effort and recommends that it be maintained so that data needs can be periodically reprioritized based on changes in the HIV epidemic and to facilitate continued minimization of grantee reporting burden.
Recommendation 4-1. The Department of Health and Human Services should maintain and institutionalize the existing effort to streamline data collection and reduce reporting requirements for federally funded HIV/AIDS programs. This will allow for periodic reprioritization of data needs, based on changes in the HIV epidemic that occur over time, and ensure the continuous availability of data to effectively monitor HIV care while minimizing reporting requirements for grantees. The data reprioritization should involve health departments, HIV provider organizations, and federal agencies that are major funders of HIV/AIDS programs, including HHS, the Department of Veterans Affairs, and the Department of Housing and Urban Development.
Providers of HIV care and supportive services contend with numerous federal laws and state statutes and regulations on the proper use and disclosure of patient information. Although important to patient privacy, the often inconsistent nature of these protections, which leave the decision of whether or not to disclose requested patient information open to various interpretations, may result in discrepancies in data sharing and reporting across states and providers. Such discrepancies may influence the availability and quality of data needed to estimate indicators of HIV care and supportive services.
Recommendation 4-2. The Department of Health and Human Services should issue guidance to the HIV care community to clarify what is permissible patient information to share given federal and state privacy laws.
The Role of Health Information Technology and Data
System Integration in the Collection of HIV Care Data
Increased exchange of health-related information across providers of HIV care and supportive services has the potential to improve care coordination and longitudinal tracking of care. Some integrated health care systems, such as the VHA and Kaiser Permanente, effectively manage information across providers within their networks, but most PLWHA receive care and supportive services outside of these networks, and many receive care across multiple organizations. The committee identified local efforts in health information exchange that have resulted in improved monitoring of patient care and outcomes. However, these efforts have not been scaled broadly among entities serving PLWHA.
Recommendation 5-1. The Department of Health and Human Services should review existing mechanisms for the confidential and secure exchange of health information to provide a platform to increase the exchange of such information among entities serving individuals with HIV. These entities may include, but are not limited to, state and local health departments, government agencies, and community-based organizations funded to provide medical care, substance use and mental health services, and housing and other supportive services.
Interoperability—the ability of different IT systems and software applications to communicate, exchange, and use information—is not fully possible in the United States at this time due to a lack of infrastructure to support it. For the most part, the various sources of care and care coverage for PLWHA have their own health IT systems with disparate architectures and vocabularies, posing a challenge to the exchange of data across systems.
Recommendation 5-2. The Department of Health and Human Services and the Office of the National Coordinator for Health Information Technology should provide technical assistance and policy guidance to state and local health departments, clinical providers, and other agencies serving individuals with HIV to improve the interoperability of data systems relevant to monitoring HIV care and supportive services.
Efficient Analysis of HIV Care Indicators and
Dissemination of Data by Federal Agencies
Estimation of the committee’s recommended indicators for clinical HIV care and mental health, substance abuse, and supportive services will often require combining data from multiple data systems. Making valid inferences about the indicators across different populations and over time using data from multiple data systems presents a range of analytic and logistical challenges. Such challenges will change over time and will have to be reevaluated periodically.
Recommendation 6-1. At least once every 2 years, the Department of Health and Human Services should reevaluate mechanisms for combining data elements to estimate key indicators of HIV care and access to supportive services, analyze the combined data, and identify and address barriers to the efficient analysis of such data, including relevant statistical methodologies. To facilitate this process, HHS should engage a center of excellence representing broad areas of expertise that include information technology, statistical methodologies for combining data, and data system content.
Information on the indicators recommended by the committee will be of interest to a variety of stakeholders, including policy makers, health departments, HIV care providers, patients, and researchers. The disseminated information can be used in numerous ways—from informing policy decisions to supporting the development of research projects—that have the potential to improve HIV care quality.
Recommendation 6-2. The Department of Health and Human Services should report to the public at least once every 2 years on indicators of HIV care and access to supportive services to foster improvements in the quality of HIV care and in monitoring progress toward meeting the goals of the National HIV/AIDS Strategy.
The reporting interval of at least once every 2 years allows for regular reporting of the indicator data to monitor the NHAS while minimizing reporting burden and associated costs.

















