
Key Messages
- India accounted for 24 percent of the 5.7 million new and relapse TB cases notified globally in 2010 (WHO, 2011a).
- India had the second highest total number of estimated MDR TB cases (99,000) in 2008, after China (100,000 cases) (WHO, 2010b).
- Drug resistance surveys in several states have indicated that the prevalence of MDR TB in India is 2-3 percent among new cases and 12-17 percent among reinfection cases.
- India’s RNTCP has an overall goal of providing universal access to quality diagnosis and treatment for all TB patients, with an intermediate goal of successfully treating at least 90 percent of all new and at least 85 percent of all previously treated patients.
____________________
1 This chapter is based on the presentations of Ashok Kumar, Deputy Director General and Head, Central TB Division, and Project Director, RNTCP; Kuldeep Singh Sachdeva, Chief Medical Officer, Central TB Division; S. K. Sharma, Chair, Department of Medicine, All India Institute of Medical Sciences (AIIMS); Rohit Sarin, Senior Consultant, Lala Ram Sarup (LRS) Institute of Tuberculosis and Respiratory Diseases; and Aleyamma Thomas, Scientist G and Director-in-Charge, National Institute for Research in Tuberculosis. (Since the workshop, the Tuberculosis Research Centre [TRC] has been renamed the National Institute for Research in Tuberculosis. For the remainder of this workshop summary report, the organization will be referred to by its current name.)
- The RNTCP is scaling up the number of culture and DST laboratories nationwide, along with treatment services, including DOTS-Plus.
- Despite these achievements, India’s efforts to control TB and MDR TB still suffer from too few laboratories, slow diagnostic tools, inadequate management of treatment, insufficient supplies of second-line drugs, and shortages of trained personnel.
- Community-based MDR TB treatment is being implemented as an alternative model of treatment.
- Data from the RNTCP from 2007 to 2010 indicate that the majority of MDR TB cases were undiagnosed in India.
Drug-resistant TB has existed in India virtually since anti-TB drugs were introduced into the country. ICMR carried out state-of-the-art surveys for drug-resistant TB more than 40 years ago (ICMR, 1968, 1969), and surveys have continued since then (Paramasivan and Venkataraman, 2004). Resistance to rifampicin, streptomycin, and other anti-TB drugs has been detected for decades, and MDR TB also was seen in early surveys, although at different levels depending on the place, time, and testing parameters. However, the increasing burden of drug-resistant TB introduces new challenges to TB control and treatment. Ashok Kumar, Deputy Director General and Head, Central TB Division, and Project Director, RNTCP; Kuldeep Singh Sachdeva, Chief Medical Officer, Central TB Division; S. K. Sharma, Chair, Department of Medicine, All India Institute of Medical Sciences (AIIMS); Rohit Sarin, Senior Consultant, Lala Ram Sarup (LRS) Institute of Tuberculosis and Respiratory Diseases; and Aleyamma Thomas, Scientist G and Director-in-Charge, National Institute for Research in Tuberculosis, described the current status of TB and MDR TB in India and the actions taken by government at various levels to combat the disease.
THE BURDEN OF TB AND MDR TB IN INDIA2
India has the highest TB burden of any country in the world, accounting for an estimated one-fifth of global TB cases worldwide (Figure 2-1). It has an estimated prevalence of 3 million TB cases, with 2 million new cases
____________________
2 This section is based on the presentation of Kuldeep Singh Sachdeva, Chief Medical Officer, Central TB Division.
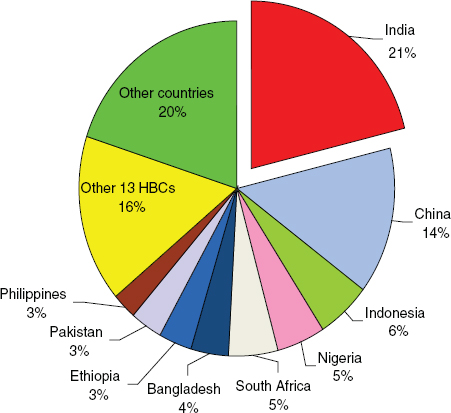
FIGURE 2-1 India has the highest TB burden of any country in the world. As of the date of the workshop, annual incidence was 2 million cases, estimated prevalence was 3 million, annual deaths due to TB totaled 280,000, and approximately 6.4 percent of incident TB cases were also HIV-positive.
NOTE: HBC, high-burden country.
SOURCE: Sachdeva, 2011. Based on data from Global Tuberculosis Control: WHO Report 2010 (WHO, 2010b).
occurring each year. About 280,000 people die from TB in India annually.3 India has the second highest burden of MDR TB in the world after China, with an estimated 99,000 new cases per year (WHO, 2010b).
Sachdeva noted that the RNTCP carried out a drug resistance surveillance survey in accordance with global guidelines in the states of Gujarat and Maharashtra in 2007 and in Andhra Pradesh in 2009 (Table 2-1). The results of these selected surveys indicate an MDR TB prevalence of about
____________________
3 Since the workshop took place, an updated WHO report (2011a) cited new provisional estimates of the TB burden in India in 2010. India has an estimated prevalence of 3.1 million TB cases, with 2.3 million new cases occurring each year, and 320,000 deaths due to TB each year.
TABLE 2-1 Drug Resistance Surveillance in Three Indian States
|
|
|||
| State (survey year) | Population | MDR TB Among New Cases (%) |
MDR TB Among Previously Treated Cases (%) |
|
|
|||
| Gujarat (2007–2008) | 56 million | 2.4 | 17.4 |
| Maharashtra (2008) | 108 million | 2.7 | 14.0 |
| Andhra Pradesh (2009) | 86 million | 1.8 | 11.8 |
|
|
|||
| SOURCE: Sachdeva, 2011. | |||
2–3 percent among new cases and 12–17 percent among previously treated cases.
According to Sharma and colleagues (2011a), the prevalence of MDR TB among 177 cases of newly diagnosed pulmonary TB patients in New Delhi in 2008–2009 was lower—about 1.1 percent. Among 196 patients with pulmonary TB diagnosed in New Delhi between 2005 and 2008 who had failed previous TB treatment, relapsed after treatment, or defaulted during treatment, 20.4 percent had MDR TB (Sharma et al., 2011b).
Population-based data are highly limited for second-line drug resistance among MDR TB patients, according to Sachdeva. According to drug resistance surveillance data from Gujarat, fluoroquinolone resistance occurred in 24 percent and kanamycin resistance in 3 percent of 219 MDR TB cases detected. XDR TB was observed in about 3 percent of MDR TB isolates, and all 7 of these cases were in previously treated patients.
Accurate estimates of drug resistance require that results come from well-qualified and accredited laboratories. The reliability of the data and quality control issues are essential considerations both in estimating current levels and in making historical comparisons, noted Sharma.
PLANS OF THE REVISED NATIONAL TB CONTROL PROGRAM4
Initiated in 1997, the RNTCP has been implementing all of the components of the WHO STOP TB Partnership, including early diagnosis, quality smear microscopy, and prompt treatment with DOTS using quality first-line drugs, said A. Kumar. Sachdeva noted that the RNTCP’s overriding goal is to provide universal access to quality diagnosis and treatment for all patients. Intermediate goals (by 2015) are to achieve early detection of at least 90 percent of all TB cases, including HIV-associated TB; perform initial screening of all smear-positive patients for drug-resistant TB; provide
____________________
4 This section is based on the presentations of Kuldeep Singh Sachdeva, Chief Medical Officer, Central TB Division; and Ashok Kumar, Deputy Director General and Head, Central TB Division, and Project Director, RNTCP.
HIV counseling and testing for all TB patients; and successfully treat at least 90 percent of all new and at least 85 percent of all previously treated TB patients. A national strategy for the RNTCP for the next Five-Year Plan, which extends from 2012 to 2017, is currently being developed. Since the RNTCP’s inception, more than 12 million TB patients have been initiated on DOTS, and approximately 2 million lives have been saved, A. Kumar noted.
Preventing Drug-Resistant TB
To combat drug-resistant TB, the RNTCP has developed a multiphase response plan, said A. Kumar. With regard to prevention, the plan calls for improving and sustaining high-quality DOTS implementation, promoting the rational use of anti-TB drugs, and implementing infection control measures. The RNTCP is also seeking to improve laboratory capacity, effectively treat MDR TB patients, initiate and rapidly scale up MDR TB services, and evaluate the extent of second-line anti-TB management strategies.
Airborne infection control is crucial for preventing the spread of TB from person to person, as well as reducing the risk of TB among health workers in institutional settings, said A. Kumar. The National Airborne Infection Control Committee was established in 2008 with representatives from the medical profession, the National Center for Disease Control, the National Center for TB Resistance, WHO, architects, and engineers. The committee has developed provisional guidelines on airborne infection control in health care and other settings. These guidelines are expected to augment the infection control measures undertaken by the RNTCP. Workshops on airborne infection control have been organized by the RNTCP with the support of the U.S. Centers for Disease Control and Prevention (CDC), WHO, and others, and pilot implementation programs have been initiated. The RNTCP also has disseminated provisional airborne infection control guidelines to all states in India.
A. Kumar noted that the national guidelines for infection control still need to be operationalized, not just for TB but for the general health system and at the community level. Chapter 4 of this report summarizes several workshop presentations specifically addressing infection control.
Diagnosing Drug-Resistant TB
Sachdeva reported that a staggered approach is currently being used to diagnose MDR TB in India. MDR TB is suspected in all patients who fail the first-line drug regimen, all patients whose sputum is positive after 4 months of treatment, and all smear-positive contacts of MDR TB patients. These
criteria will be changed over the years as laboratory capacity expands. DST is conducted at an accredited laboratory, with the line probe assay (LPA) being the preferred testing method if available. Treatment is initiated on the basis of results for rifampicin resistance, since resistance only to rifampicin is rare.
Edward Nardell, Associate Professor of Medicine, Harvard Medical School, pointed out that because previously untreated TB cases are much more numerous than those previously treated,5 more than half of MDR TB cases globally are new. However, more effort is required to detect such cases.6 A strategy that focuses on smear-positive patients for MDR TB testing will be more likely to miss these new cases. Sharma noted that sometimes it is unclear whether patients were previously treated or not.
Treating Drug-Resistant TB
To combat MDR and XDR TB, a national DOTS-Plus committee of experts, established in 2005, developed national DOTS-Plus guidelines for India aligned with the WHO guidelines for treatment of drug-resistant TB. DOTS-Plus services for programmatic management of MDR TB were introduced as a pilot in the states of Gujarat and Maharashtra in 2007 and since then have gradually been expanded.
The model of DOTS-Plus care includes inpatient and community care. Sachdeva explained that patients are identified at the community level and then referred to the district TB officer, who collects a sample from the patient and sends it to the culture and DST laboratory. The culture and DST laboratory communicates the results to the district. The district TB officer traces the patient and sends him or her to a DOTS-Plus site for about a week for an initial workup. The patient then is placed on treatment at the DOTS-Plus site. After a week of treatment, the patient is referred back to the community, and the rest of the treatment is carried out on an outpatient basis.
The DOTS-Plus program employs a decentralized and integrated model of care. The DOTS provider at the community level sees the patient through the course of treatment. At the health facility, the doctors and paramedics
____________________
5 Of the 6.2 million people diagnosed with TB in 2010, 5.4 million had TB for the first time, and 0.3 million had a recurrent episode. In a small number of cases the treatment history was not recorded, and 0.4 million had already been diagnosed with TB but had their treatment changed to a retreatment regimen after treatment failure or interruption. In 2010, an estimated 3.4 percent of new TB cases globally were MDR TB and an estimated 20 percent of retreatment TB cases were MDR TB (WHO, 2011a).
6 Trends in global MDR TB rates remain largely unclear because of a lack of nationally representative data in many large countries, including India and several African countries (Zignol et al., 2012).
are trained to supervise the DOTS provider, as well as to manage and monitor minor side effects. At the district level, the district TB officer coordinates case findings, follow-up examinations, and reporting.
The standardized treatment regimen for MDR TB in India is a 6-drug regimen, with an intensive phase of 6–9 months and a continuation phase of 18 months; the total duration of treatment is about 24–27 months. The six drugs are kanamycin, levofloxacin, cycloserine, ethionamide, pyrazinamide, and ethambutol. P-aminosalicylic acid (PAS) is kept as a reserve drug in the event of intolerance of or a reaction to any one of the other drugs. The regimen involves daily DOT, with kanamycin given for 6 days in a week. Patients are treated according to 3 weight bands: 16–25 kg, 26–45 kg, and more than 45 kg.
In the discussion period, Sachdeva noted that because many patients were unwilling to be admitted to the hospital for a month, the period of hospitalization was reduced to about a week. Also, many MDR TB patients die in the time it takes for them to be traced, diagnosed, counseled, and put on treatment. Therefore, the goal is to diagnose patients as early as possible, in part through scale-up of the country’s laboratory capacity. Another problem is that transporting sputum from patients to the culture and DST laboratories has been difficult, especially in remote areas. Accordingly, greater involvement by private-sector laboratories is being sought.
Sachdeva also noted that reports of patients with XDR TB are surfacing. Specifications for drugs for these patients are being analyzed, which will generate guidance for DOTS facilities.7
Procuring Drugs
The RNTCP’s system of drug logistics and event-tree management is integrated with first-line anti-TB management. There are two sources of procurement: the GLC and the government of India. Quality-assured second-line drugs are being procured by the government of India with financial support from the World Bank, UNITAID,8 and the Global Fund,
____________________
7 In January 2012, following the workshop summarized herein, the emergence of TDR TB in India was reported at Hinduja Hospital in Mumbai (Udwadia et al., 2012). The reporting authors indicated that three of the four TDR TB patients had received erratic, unsupervised second-line drugs, often in incorrect doses and from a variety of private practitioners, in an effort to cure their MDR TB. The term “TDR TB” is not currently recognized by WHO or the RNTCP, which instead refer to these cases as XDR TB. For more information on this terminology, visit http://www.who.int/tb/challenges/mdr/tdrfaqs/en/index.html (accessed April 17, 2012).
8 UNITAID is an international purchase facility for medicines and diagnostics for HIV/AIDS, malaria, and TB. Started in 2006 by Brazil, Chile, France, Norway, and the United Kingdom, UNITAID generates program financing through a tax on airline tickets. Ninety-four countries currently receive UNITAID funding. For more information, visit http://www.unitaid.eu/.
with technical assistance from WHO and the GLC. The procurement of 23,000 drug doses for MDR TB for 2011-2012 has been initiated through the GLC and the Global Drug Facility (GDF) mechanism. Loose drugs are supplied to state drug stores and repackaged into three monthly boxes. These boxes are supplied to the districts, with loose drugs being provided to DOTS-Plus sites.
Scaling Up Laboratory Capacity
As of March 2011, India had 25 accredited culture and DST laboratories, noted Sachdeva (Figure 2-2). As of December 2010, 12 states were implementing basic DOTS-Plus services, and all planned to do so by the end of 2011. At the end of 2010, the DOTS-Plus program covered about 24 percent of the population in the 141 of the country’s 658 districts that at that point had MDR TB diagnostic and treatment services available.
Sachdeva reported that as of December 2010, more than 19,000 patients suspected of having MDR TB had been examined and about 3,600 had been initiated on treatment. The number of patients placed on treatment has been increasing each year.
The RNTCP is currently scaling up the number of accredited culture and DST laboratories nationwide to at least 43 by 2013, with the potential for 65–70 laboratories, including private-sector and medical college laboratories, to be accredited under the program, said Sachdeva. Capacity will be increased at each laboratory through investments in sputum processing capacity, the introduction of high-throughput molecular DST, automated liquid culture systems, stronger specimen transport systems, and electronic reporting of results. By 2013, access to laboratory-based, quality-assured MDR TB diagnosis and treatment will be available to all smear-positive retreatment TB cases and new cases that have failed an initial first-line drug treatment, said Sachdeva. Also by 2013, the expected annual DST capacity will grow from 35,000 in 2010–2011 to 220,000, and at least 30,000 MDR TB patients are projected to enter treatment annually. By 2015, all smear-positive TB cases, whether new or retreatment cases, will have access to MDR TB diagnosis and treatment. UNITAID, the Global Fund, the World Bank, and WHO have all supported the laboratory scale-up effort.
Sachdeva described several components of the strategy for scaling up treatment services. Human resource capacity will be strengthened by having a DOTS-Plus coordinator in every district and additional staff at laboratories and DOTS-Plus sites. By 2012, the number of DOTS-Plus sites is slated to increase from about 24 currently to 200 sites covering all states across the country—the equivalent of 1 site per 10 million people (RNTCP Status Report, 2011). All DOTS-Plus sites will be upgraded to national airborne infection control standards. The RNTCP is advocating that drug

FIGURE 2-2 Distribution of Revised National TB Control Program (RNTCP) culture and drug susceptibility testing (DST) laboratories across India as of March 2011. As of that date, there were 25 accredited laboratories (4 national reference laboratories, 12 intermediate reference laboratories, 9 other laboratories) and 8 laboratories whose accreditation was pending. The line probe assay (LPA) was available in 4 laboratories. The RNTCP is also encouraging a number of private-sector laboratories and medical college laboratories to obtain accreditation (i.e., “preparatory” status in the legend above).
SOURCE: Sachdeva, 2011.
manufacturers adhere to WHO prequalification and GDF quality assurance programs and develop second-line drug production plans that take account of the nation’s demand for the drugs. The RNTCP also is advocating with professional associations and physicians for rational use of the fluoroqui-nolones, especially in respiratory diseases, so that resistance to this class of drugs does not become a major challenge in the management of MDR TB.9 Finally, an integrated national online electronic recording and reporting system will be instituted, based on the E-TB Manager model used in Brazil.
Outcomes for patients who received standardized treatment through DOTS-Plus have been mixed, said Sharma. In a retrospective analysis of 66 patients, 53 (80.3 percent) became culture-negative, 77.3 percent of these within 3 months (Arora et al., 2007); 4 failed to convert within 9 months; and the rest died or defaulted. Among 28 patients completing 2 years of treatment, 67.9 percent were cured, 14.3 percent died, 17.9 percent defaulted, and none failed treatment. Cycloserine had to be stopped in 5 patients and kanamycin was stopped in 3 patients because of adverse effects. Other drugs were better tolerated.
By contrast, in another 2007 study of 172 MDR TB patients and 1 XDR TB patient described by Sharma, only 41.6 percent were cured, 38.7 percent failed, 15 percent defaulted, and 4.6 percent died, although this study preceded the DOTS-Plus era. During the discussion period, in response to a question about this cure rate, Sachdeva noted that many of these patients had undergone second-line treatment multiple times, and the risk of failure was greater because they were treatment experienced. Subsequent cohorts are showing better results, but they have not yet completed the full course of treatment. Earlier diagnosis and treatment could boost cure rates, said Sachdeva, but globally the treatment success rate for MDR TB is only about 60–65 percent.
Salmaan Keshavjee, Harvard Medical School, observed that a high failure rate probably points to strains that are more resistant than is commonly held. Moreover, default rates of 20 percent indicate that there is much work
____________________
9 At the 2010 IOM workshop in Moscow (IOM, 2011b), Peter Cegielski, CDC, shared results from the Preserving Effective TB Treatment Study (PETTS), a prospective follow-up study of MDR TB patients in nine countries aimed at determining the frequency of and risk factors for acquired resistance to second-line drugs in a diverse group of MDR TB programs. A large number of MDR TB patients already had resistance to second-line drugs at the start of treatment: 11 percent for the fluoroquinolones, 11–18 percent for injectable agents, close to 20 percent for ethionamide, and almost 10 percent for para-aminosalycylic acid. Cegielski suggested that the high level and diversity of drug resistance found at baseline suggests that standardized treatment approaches for MDR TB are not advisable. The 2010 IOM workshop in South Africa (IOM, 2011a) also included a discussion of the sensitivity of the various strains of M.tb. to the fluoroquinolones. Nesri Padayatchi, University of KwaZulu-Natal, shared that moxifloxacin has been one of the most commonly used fluoroquinolones for treating patients in South Africa.
to be done in India and elsewhere to strengthen the health system’s capacity to deliver care. High death rates mean that greater capacity is needed to diagnose people quickly and place them on appropriate treatment. A 42 percent success rate is disturbing, he said, suggesting that the goal should be 60–80 percent. In the Tomsk prison system in Russia, for example, where inmates are resistant to all first-line drugs plus some second-line drugs, the cure rate approaches 80 percent under a collaborative DOTS-Plus program that includes the penitentiary system and the civilian health service and serves a combination of incarcerated and civilian patients, as well as vulnerable populations such as the homeless, unemployed, and disabled (Shin et al., 2006). Keshavjee explained that the reason for this success is the presence of a health system within the prison that can deliver drugs to patients each day and ensure that they take them.
Keshavjee also noted that MDR TB is a highly complex problem and that India is attempting to incorporate a complex health intervention into a health system that needs strengthening at multiple levels. Involvement of the private sector is being sought to make these efforts more feasible (see the next section and Chapter 7).
INVOLVEMENT OF THE PRIVATE SECTOR10
Indiscriminate use of anti-TB drugs, especially outside the RNTCP, has contributed significantly to the emergence of drug-resistant TB in India, said A. Kumar. In India, drugs available by prescription elsewhere are available over the counter in any pharmacy, which complicates the management of MDR TB. For example, fluoroquinolones are available over the counter and are commonly used in households for fevers and infections. In 2006, prior to the implementation of the DOTS-Plus program in India, based on the total amount of money available for anti-TB drugs sold in India, 75 percent of first-line drugs and 100 percent of second-line drugs were being used outside the RNTCP.
The National Center for Disease Control under the Indian Ministry of Health has sought to restrict the sale of anti-TB drugs without a written prescription. The Drug and Cosmetic Act of India also contains a clause restricting the sale of anti-TB drugs. A. Kumar noted that meetings organized by the GDF, WHO, and the RNTCP have brought Indian drug manufacturers together to educate them and encourage them to adhere to established standards.
An important component of the DOTS-Plus program has been the establishment of partnerships with the private sector, including nongovernmental
____________________
10 This section is based on the presentation of Ashok Kumar, Deputy Director General and Head, Central TB Division, and Project Director, RNTCP.
organizations (NGOs), medical colleges, and other private institutions. Such partnerships are critical, said A. Kumar, because it is not possible to achieve control through the actions of a single agency. The partnerships are designed to achieve community awareness, improve access to TB care, reduce patient costs and inconvenience, detect cases early, promote the rational use of anti-TB drugs, and ensure sustained funding. For example, the Indian Medical Association and other private-sector professional societies, particularly those for chest physicians, have endorsed the application of international standards of TB care.
Partners are also needed at the national and global levels. For example, Sachdeva noted that the Foundation for Innovative New Diagnostics (FIND) has aligned its work plans with India’s national scale-up plan, and the Clinton Foundation has conducted an independent external validation of the national plan.
CHALLENGES TO THE REVISED NATIONAL
TB CONTROL PROGRAM11
India’s efforts to control TB and MDR TB face a number of challenges and roadblocks, which were described by A. Kumar and Thomas.
Laboratories
For a variety of reasons, the establishment and accreditation of laboratories in some states have been delayed. The RNTCP plans to link these states with an accredited laboratory elsewhere so that services will not be affected, said A. Kumar.
Diagnosis
A. Kumar noted that conventional tests to detect drug-resistant TB are slow, tedious, and difficult to perform under field conditions. Timely availability of results is crucial for prompt patient management to reduce morbidity and mortality. Newer tools are being introduced into the RNTCP in a phased manner. The LPA, when available, is the preferred DST method in India.12 These tools need to undergo rigorous field evaluation before they are used in populations with a significant burden of drug-resistant TB, and
____________________
11 This section is based on the presentations of Ashok Kumar, Deputy Director General and Head, Central TB Division, and Project Director, RNTCP; and Aleyamma Thomas, Scientist G and Director-in-Charge, National Institute for Research in Tuberculosis.
12 Capacity for DST with the LPA in India was less than 0.1 laboratories per 10 million population in 2010 (WHO, 2011b).
technologies that provide rapid diagnosis require staff support and training. Operational research to reduce these delays is ongoing in the state of Andhra Pradesh, supported by UNITAID.
Management
Successful management of TB patients is the responsibility of health systems, said Thomas. First-line DOTS regimens need to be followed strictly. The default rate in retreatment cases, a major source of drug-resistant TB, remains quite high. Management of drug-resistant TB is a therapeutic challenge that needs to be undertaken by experienced clinicians at centers equipped with quality-assured, accredited laboratories and inpatient and surgical facilities. Improving the efficiency with which suspected MDR TB cases are referred and tracing patients who are lost to follow-up are both critical, since the best treatment for MDR TB is to prevent it from developing. The irrational use of first- and second-line drugs needs to be discouraged, including in education and training provided at medical colleges. Patients and their relatives need to receive standardized counseling because of the long duration of treatment. And infection control measures are essential to keep the disease from spreading.
Drug Access and Supply
Ensuring an uninterrupted supply of quality-assured second-line drugs is a key issue. A. Kumar noted that the diagnostic capacity for MDR TB exceeds the number of patients who can be placed on treatment because of the limited availability of drugs. Rising costs reduce the use of these drugs. Addressing this problem will require intervention from the GLC and incentives for Indian drug manufacturers to build their capacity to produce better-quality prequalified drugs.
Human Resources
Thomas noted that the dramatic demands on program staff for supervision and treatment are posing human resource challenges in India. Staff need adequate training in management and supervision. Specifically, Thomas suggested that training should also focus on problem solving, management skills, and planning to facilitate program expansion and performance, as well as specialized training for dealing with MDR TB among vulnerable populations. Nonprogram providers and communities also need to be involved in diagnosis and management.
Data
A robust system is needed to monitor and evaluate multiple program indicators, said Thomas. Better performance will require good data collection and analysis, as well as timely dissemination of findings to end users for further improvement.
TREATMENT OF DRUG-RESISTANT TB13
Before 1998, most treatment of drug-resistant TB was still being provided by individual clinicians, said Sarin. These clinicians treated very few patients, and not all clinicians provided effective treatments. In 1998, WHO and international partners adopted a different strategy for dealing with the burden of drug-resistant TB, which included shifting to a community-based programmatic approach. This decision contributed to the genesis of the DOTS-Plus program, as well as the GLC.
WHO’s Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis: Emergency Update includes a hierarchy of the five groups of anti-TB drugs and instructions for building a treatment regimen (WHO, 2008, Table 7.1 and Figure 7.2):
- Group 1—first-line oral anti-TB drugs (isoniazid [H], rifampicin [R], ethambutol [E], pyrazinamide [Z]; rifabutin [Rfb]);
- Group 2—injectable anti-TB drugs (kanamycin [Km], amikacin [Am], capreomycin [Cm], streptomycin [S]);
- Group 3—fluoroquinolones (moxifloxacin [Mfx], levofloxacin [Lfx], ofloxacin [Ofx]);
- Group 4—oral bacteriostatic second-line anti-TB drugs (ethion-amide [Eto], protionamide [Pto], cycloserine [Cs], terizidone [Trd], p-aminosalicylic acid [PAS]); and
- Group 5—agents with unclear efficacy or an unclear role in MDR TB treatment not recommended for routine use in MDR TB patients (clofazimine [Cfx], linezolid [Lzd], amoxicillin/clavulanate [Amx/ Clv], thioacetazone [Thz], imipenem/cilastatin [Ipm/Cln], high-dose isoniazid [high-dose H], clarithromycin [Clr]).
WHO (2008) also has established basic guiding principles for designing a treatment regimen for drug-resistant TB:
____________________
13 This section is based on the presentation of Rohit Sarin, Senior Consultant, LRS Institute of Tuberculosis and Respiratory Diseases.
- Regimens should be based on the history of drugs taken by the patient.
- Drugs commonly used in the country and the prevalence of resistance to first- and second-line drugs should be considered in developing a regimen.
- At least four anti-TB drugs that are certain, or almost certain, to be effective should be used. When evidence of effectiveness is unclear, a drug can be included in the regimen, but it should not be depended upon for success.14
- Drugs with cross-resistance should not be used. (For example, amikacin and kanamycin have high levels of cross-resistance, as do capreomycin and viomycin.)
- Adverse drug effects should be treated immediately and adequately so as to minimize the risk of treatment interruptions and prevent increased morbidity and mortality due to serious adverse effects.
- Drugs that are not safe in the patient should be eliminated.
Each dose of a drug is provided as DOT throughout the treatment regimen and recorded.
In addition to the above guidelines, WHO has established principles for the selection of drugs. The first is to perform DST and use a drug considered to be effective on the basis of the results. The patient should have no previous history of treatment failure with a drug and no known close contact with resistance to a drug, and drug resistance patterns should indicate that resistance to a drug is rare among the population. Finally, the regimen should include at least one injectable and one fluoroquinolone.
Drugs usually are administered at least 6 days a week. Dosage should be linked to body weight, with a preference for the higher dosage within a weight range. Injectables need to be administered for a minimum of 6 months (intensive phase), with treatment for a minimum of 18 months beyond sputum culture conversion.15
The entire regimen should be administered under DOTS, but different treatment options are available. One is an empirical treatment strategy, in which a DST report is not available, but a course of treatment is devised on the basis of a patient’s history of drug intake and other factors. In an individualized treatment strategy, a DST report is available for a patient for all
____________________
14 A recent WHO (2011c) report updates this guideline to state that MDR TB treatment regimens should include at least four second-line anti-TB drugs likely to be effective, plus pyrazinamide (Z), in the intensive phase of treatment.
15 An updated WHO report (2011c) changes the guideline for duration of treatment for MDR TB patients to at least 8 months of intensive-phase treatment (an increase of 2 months relative to the 2008 guidelines). A total treatment duration of at least 20 months is recommended for MDR TB patients with no previous MDR TB treatment.
first- and second-line drugs, and the regimen is based on the susceptibility pattern. In a standardized treatment strategy, drug resistance surveillance data from representative patient populations are used to design a treatment regimen in the absence of individual drug susceptibility results. Patients in a defined group or category then receive the same standardized treatment regimen.
The advantages of a standardized treatment strategy are that the cost of the regimen is lower than that of the other two strategies, DST is not required for all drugs, the technical capacity of the physician need not be high, the regimen can be applied on a large scale, implementation is less complicated, drug ordering and training are easier, and mismanagement is less likely. The disadvantages of a standardized treatment strategy are that it is not as effective as an individualized strategy in all cases; it can amplify resistance; the drug susceptibility pattern within a community needs to be well documented; and organisms may be resistant to some of the drugs in the regimen, resulting in an avoidable increase in both cost and toxicity.
Countries can adopt MDR TB treatment strategies on the basis of the laboratory method used to confirm MDR TB. If the method involves a long time gap before results are obtained, patients can be placed on an empirical treatment regimen. If the results then demonstrate drug resistance, the patient can be placed on an individualized or standardized treatment regimen. If rapid detection methods are available, such that results are available within 1–2 days, the patient can be placed on an individualized or standardized treatment regimen as soon as results are available.
Surgery can be an adjunct to chemotherapy, but it is not indicated when the disease is extensive and bilateral. About 2 months of anti-TB therapy must be administered before surgical resection is attempted. And even with surgery, the duration of treatment still must be a minimum of 2 years.
In India, a particular treatment regimen followed as national policy is an intensive phase of 6–9 months and a continuation phase of 18 months. As specified in the DOTS-Plus guidelines, patients are monitored through sputum smears, cultures, x-rays, and some blood and laboratory investigations.
XDR TB treatment follows similar guidelines but is of longer duration since it is more difficult. A later generation of fluoroquinolones needs to be used, with greater reliance on category IV and V drugs rather than category II and III drugs; surgical resection also needs to be considered. Underlying HIV infection must be treated if present, and side effects demand comprehensive monitoring and treatment.
Predictors of success in the treatment of MDR TB are the use of pyrazinamide and ethambutol if the strain of TB is susceptible to these drugs, the use of a fluoroquinolone, the use of more than 5 drugs, sputum conversion within 2 months, and surgical resection. Predictors of failure are
previous therapy, resistance to the fluoroquinolones, resistance to inject-ables, the presence of cavitation, low body mass index, HIV infection, poor adherence, and positive culture at 2–3 months.
WHO also has issued recommended strategies for different programmatic situations. In India, for example, all category I failures are placed on category II treatments, and the regimen is adjusted to category IV if DST reveals drug resistance. In some countries, category I failures are started immediately on category IV treatments. In India, treatment choices for category II failures depend on results of DST and overall drug resistance patterns.
Designing treatment regimens for MDR TB is highly challenging, said Sarin. In resource-limited settings, standardized treatment regimens may be necessary instead of individualized regimens. Different options for standardized regimens are available, depending on drug resistance patterns in the country. Decisions on regimens also are linked to the availability of resources, quality-assured DST, and drugs.
IMPROVING HEALTH SYSTEM PERFORMANCE TO
ADDRESS THE CHALLENGE OF DRUG-RESISTANT TB16
From 2007 to 2010, the staff of DOTS-Plus sites in India examined 19,178 MDR TB suspects, diagnosed 5,365 cases of MDR TB, and initiated treatment for 3,610 MDR TB patients (RNTCP Status Report, 2011). There is an estimated annual incidence of 99,000 cases of MDR TB in the country (RNTCP Status Report, 2011); thus, the majority of MDR TB patients are undiagnosed. Scale-up of the DOTS-Plus program is essential to increase the number of MDR TB patients receiving treatment, but strengthening of the health care system also is necessary, said Thomas. Health system strengthening is defined as an array of initiatives and strategies that improves one or more functions of the system. It leads to better health through improvements in access, coverage, quality, or efficiency. TB remains a high priority for health system strengthening, especially in view of the threat of drug-resistant forms of the disease.
With regard to human resources, Thomas continued, the goal is to have the right number of people with the right skills in the right place at the right time, who are motivated and supported to provide the right services to the right people. Health workers at all levels—from physicians and administrators to grassroots-level workers—need to be trained. Academic institutions, including medical colleges, schools of nursing, and other allied health institutions, need greater capacity. Beyond initial training, there
____________________
16 This section is based on the presentation of Aleyamma Thomas, Scientist G and Director-in-Charge, National Institute for Research in Tuberculosis.
is a need for retraining, on-the-job training, continuing education, and advanced training in management. Training in problem solving, supervision, management, and planning is needed to supplement core training in TB management. Specialized training should focus on operations research, drug management, treatment of drug-resistant TB, TB and HIV coinfection, and infection control, said Thomas.
Training should be followed by in-service monitoring and supervision to detect performance deficiencies, identify new staff in need of training, and identify additional staff needed for current and new interventions. Innovative strategies, some of which were described during the workshop (see the next section), are needed to develop the appropriate competencies to deliver services for drug-resistant TB effectively. Strategies for optimal use of shared resources and coordination of different sectors, both governmental and nongovernmental, also are needed.
Advocacy, communication, and social mobilization are important aspects of TB control, said Thomas. Policy makers and administrators should be sensitized to the need for
- adequate and sustained funding for TB control;
- sharing of resources with other public health programs;
- training of staff at different levels and retention of trained staff;
- periodic reviews to identify gaps and take corrective steps;
- communication with patients to improve adherence;
- communication with people to encourage them to demand free diagnosis and care so that TB control becomes a people’s movement; and
- dissemination of the national plan for advocacy, communication, and social mobilization to field staff.
Finally, the scope for research on drug-resistant TB is broad. To improve the performance of the health system, Thomas said, research is particularly needed in the areas of
- epidemiology;
- newer tools for diagnosis and newer drugs for treatment;
- clinical trials to find ways to shorten the duration of treatment; and
- health system structure and operations, to identify constraints on the effective use of resources and quality services.
More and better research can inform evidence-based decision making at the policy level.
In conclusion, A. Kumar emphasized that antimicrobial resistance is a major threat to humanity and the fight against communicable diseases.
This vital issue requires an integrated and practical response guided by principles adopted by all countries. Without action today, there will be no cures tomorrow.
POTENTIAL INNOVATIONS AND ACTION ITEMS
Through the presentations provided in this session and the subsequent discussions, individual workshop speakers and participants noted key innovations and action items. They include the following:
- Based on lessons learned from recent Indian experience, inpatient care was reduced from 1 month to 1 week where possible.
- Because diagnoses were taking such a long time, in part because of a lack of laboratory capacity, private laboratories are now being accredited and utilized for more rapid diagnoses.
- All types of health care providers, including private-sector laboratories, NGOs, medical colleges, other private institutions, and professional societies, are now being incorporated into TB treatment.
- More and better managerial capacity in training programs for all types of health care workers is needed.
- Greater attention needs to be focused on vulnerable populations, especially pediatric populations, for whom there is currently a lack of adequate research data and information.
- Community-based care is a key strategy to reach patients early, initiate treatment, and help them stay on treatment.
- Decentralized and integrated models of care should be considered to reduce the time from diagnosis to treatment, bring treatment closer to patients, and increase the numbers of patients who complete treatment.
- An integrated national online electronic recording and reporting system will be instituted in India, based on the e-TB Manager model in Brazil.
- Advocacy, communication, and social mobilization are important aspects of TB control, and policy makers should be sensitized about the multiple needs for TB treatment.
This page intentionally left blank.




















