
Additive Manufacturing Is Changing Surgery
ANDREW M. CHRISTENSEN
Medical Modeling Inc.
ABSTRACT
Additive manufacturing (AM) is changing how surgery is performed. Over the past two decades relatively small, continuous advances have pushed forward the concept of using AM as part of the surgical treatment of conditions ranging from arthritis of the hip or knee to ablation of malignant tumors of the head and neck. Historical uses of AM in medicine have been primarily limited to custom anatomical models based on medical imaging data and prototyping instruments for new designs (Figure 1). Today’s trend for treatment is toward surgery that is not “one size fits all” but surgery that is now tailored to the exact needs of each patient. AM plays a key role in making this happen in a time- and cost-efficient manner based on its built-in ability to create objects of almost unlimited complexity. This is evidenced by new applications for patient-specific surgical instrumentation whose design is driven by that patient’s surgical plan and AM techniques that allow for direct output of implantable metals.
BACKGROUND
Historically the use of additive manufacturing as applied to surgery was mostly related to manufacturing of surgical planning models based on patientspecific medical image data (Mankovich et al., 1990). These “3D x-rays” allow surgeons to more closely evaluate complex anatomical structures before they enter the operating room. Most times these models depict hard-tissue anatomy (i.e., bone structures) and are used (a) to visualize anatomy preoperatively, (b) to allow for surgical simulation such as creation of bone cuts, or (c) for prebending
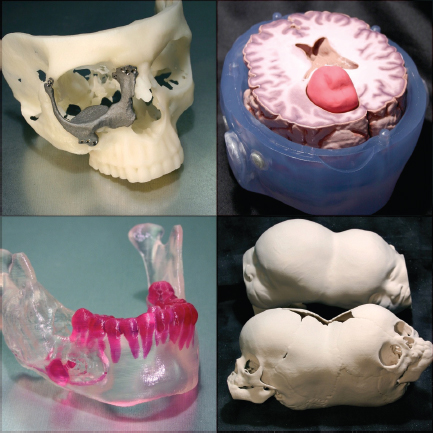
FIGURE 1 Images of typical medical-image-based models used in planning for surgery of the head and neck. Source: Courtesy of Medical Modeling Inc.
or sizing of off-the-shelf implant components, which can be “customized” to fit the bone model.
In the late 1980s came the introduction of the first commercial additive manufacturing process called stereolithography (SL or sterolithography apparatus [SLA]). Stereolithography offered immediate access to creating models of almost unlimited complexity from a three-dimensional computer-aided design (CAD) file in a translucent resin material. Immediately those surgeons who had previously been using subtractively manufactured models created from computedtomography (CT) scans started experimenting with this new additive fabrication technology. SLA allowed not only the creation of the external anatomy but also a
precise depiction of internal anatomy, including bony voids. Case reports immediately surfaced and head and neck surgical applications became the mainstay of use of this technology. Historically many have asked why head and neck surgery was leading this area and why not orthopedics. The answer seemed to lie in the fact that for orthopedic procedures, which were far more numerous (by two orders of magnitude, give or take), the surgeons cared more about function and less about form. If you imagine a hip joint reconstruction, the primary focus surrounds its biomechanical function and optimization of concentric wear from ball to cup. The reconstruction could look awful from an aesthetic standpoint but be perfectly functional from a biomechanical perspective. Reconstructive surgery of the head and neck, by contrast, has probably more to do with form than function. There are exceptions, such as reconstruction of the temporomandibular joint, but for the most part surgery of the facial skeleton has to do with restoring or creating symmetry. This pushes surgeons to agonize about fairly insignificant details such as forehead projection, symmetry between the left and right sides of the face, and interaction between the upper and lower teeth. This is probably why anatomical modeling technology by additive techniques found a home supporting surgical specialties such as oral and maxillofacial surgery, neurosurgery, and craniofacial surgery.
ADDITIVE MANUFACTURING MATERIALS
Additive manufacturing methods exist today allowing one to directly output CAD models in many different types of materials. For surgical applications the interesting materials of late fall into one of two categories: (1) strong and durable plastics for use as instruments in surgery and (2) implantable metals. Strong and durable plastics are now used in surgical settings as one-time-use instruments on a daily basis around the globe. These have found great application in surgeries such as total knee replacement and reconstruction of the mandible using virtual surgical planning techniques. The main technologies that play a role in providing durable plastic parts are laser sintering (or selective laser sintering) and SL or SLA. A key to these materials being usable is the fact that they are biocompatible for limited in vivo use during surgery and can be sterilized for use in a sterile field, including contact with the patient’s body fluids and tissues. All materials for these applications need to be tested to some portion of the standard for materials biocompatibility, ISO 10993.
Implantable metals created using additive manufacturing have only been available for the past five years or so and represent a major step forward for the industry. Now, not only can one mock up a prototype of the implant or create a mold to create the implant in an indirect fashion, but one could directly output the implant in an implantable metal. There are a few companies making additive manufacturing equipment that can directly output parts in implantable metals including titanium, titanium alloys, cobalt-chrome alloy, and other metals. If the
parts can be certified to a surgical implant material standard (many ASTM and ISO standards exist), then it is possible for these materials to be used in the body. In Europe, parts created by Electro Optical Systems direct metal laser sintering process (www.eos.info) and Arcam AB’s electron beam melting process (EBM; www.arcam.com) are CE (Conformité Européenne) marked for sale. One of those, an acetabular cup system offered by Italian orthopaedic company Lima Orthopaedics, has been used clinically (i.e., implanted) in more than 15,000 patients in the past 3 years (Marin et al., 2010). This still represents a very small number of the total of hip-replacement surgeries used—the 2010 number worldwide is 1.4 million hip replacements—but for additive manufacturing it is an impressive number. The U.S. market has been slower to adopt this new technology as a mainstream manufacturing technique, but in the past year there are at least four devices that have been cleared by the U.S. Food and Drug Administration that involve metallic implants for spine and hip reconstruction made using additive manufacturing methods. The known clearances are all for implants created using the EBM process. Several custom implant concepts have been reported, including work at Walter Reed Army Medical Center and National Naval Medical Center on reconstruction for war veterans with large cranial defects. In this case a customized porous titanium implant is fabricated with integrated fixation for adherence to the surrounding skull with standard titanium screws.
VIRTUAL SURGICAL PLANNING
The advent of easier access to medical images has given rise to a whole new area of medicine that involves virtual planning in a CAD-type environment for the upcoming surgery. Imagine planning for the surgery of your knee (Figure 2) or hip or jaw with your surgeon before surgery to allow for optimization of the surgical plan and creation of custom instruments to help precisely guide this plan into reality. This sounds like science fiction but across the globe today thousands of patients per year are getting this “customized” treatment (Davis et al., 2010; Hirsch et al., 2009).
The major step forward here, in this author’s opinion, has been the combination of surgical planning software with online collaborative environments such as those popularized by WebEx and GoToMeeting. Two methods exist for virtual surgical planning today and many methods are in the gray area between. The first is the “off-line method,” whereby the surgeon sends a service company his patient’s medical images and an order form with detailed instructions and awaits the surgical plan for approval. The surgical plan is developed by an engineering team using the inputs provided by the surgeon in conjunction with their proven workflow for treating the particular type of surgical situation. The second approach involves the surgeon sending a service company the medical images and the same detailed instructions. The difference is that the design of the surgical procedure is done in real-time collaboration between the surgeon and the engineering team during a

FIGURE 2 Customized, disposable instrument developed from a CT scan to guide total knee arthroplasty. Source: Courtesy of DePuy Orthopaedics.
web meeting conducted over the Internet (the “real-time” method). If we imagine the surgery being planned is a total knee replacement, the result of either technique is the development of a surgical plan for how the surgery will be performed, where bone cuts will be placed, what bone will be moved around or taken out, and where the prosthetic implant(s) will be placed. Once the surgical plan is created, the output of that surgical plan could go down one of two major pathways: (1) creation of a one-of-a-kind custom implant based on the surgical plan, or (2) creation of custom, disposable surgical instrument(s) that would facilitate placing an off-the-shelf implant into its desired, predetermined position.
THE FUTURE
If we can provide “designer” surgeries today and create fully custom surgical interventions, where might we go next? The answer probably lies in two major areas, both having to do with the implants themselves. Additive manufacturing plays a key role in the first next logical step: functional elements driving design. Today’s implants, while custom-fit or truly custom, are only custom in form. Their shape mimics the patient’s shape and they are meant to fit in a more stable manner than “off-the-shelf” interventions. It is commonly known that the more stable the implant, the longer it will last because loosening is the number one cause of failure for certain artificial joints like the hip or knee. Apart from something that
fits well, however, we need something that is designed just for you, something that takes your form and your function requirements and marries the two to create an implant that takes the shape that it needs to take, not the shape that an engineer predetermines it should take. As an example, we look at a hip stem implant. Typically this implant fills the intramedullary canal (marrow space) of the femur with a large amount of solid titanium material, either cemented or press-fit for stability. The issue with the current designs involves a one-size-fits-all mentality where this works for most, but people at the ends of the bell curve end up with problems with the stem being either too large or too small. Furthermore, working in conjunction with the size issue is a biomechanical issue called “stress shielding,” whereby the bone surrounding this large mass of metal is not stressed the way it was originally. There is a risk that this bone will resorb because it is not under appropriate levels of stress. In this instance, if we let form follow the functional requirements, we end up with a stem that fits the intramedullary canal but instead of being a large solid mass of metal it might look more like a combination of solid areas and patches of metallic mesh that vary based on the surrounding bone and the function required at that particular point along the canal. This idealized hip stem might allow just the right amount of flexural modulus so that the bone surrounding the implant not only does not die off but actually thrives. This concept is powerful, and additive manufacturing is ideal for its implementation based on the ability to create objects of almost unlimited complexity with a lot size of one being just as easy to fabricate as a lot size of 1,000.
Today’s alloplastic (man-made) biomaterials have not changed much in many years. Sure, there are newer variations of things and new categories such as ceramics that are becoming more and more a mainstay for articulating surfaces. The next frontier for biomaterials involves moving toward regenerative medicine, whereby the materials we put into the body eventually help regenerate the body’s own natural tissues. Much work is going on today to look at creating artificial tissues of many types, from simple bone structures all the way up to complex organ systems like the kidney and lung (Mironov et al., 2009). Additive manufacturing is known to be an ideal fit for the future of these projects, such as printing a kidney, because of the way that you can control the internal structure of an object built up in three dimensions by creating it in thin, cross-sectional two-dimensional layers.
CONCLUSIONS
Major advances in applications and materials have led to additive manufacturing (AM) playing a key role shaping the way surgery is performed today. Output of customized surgical instruments via AM and direct AM-fabricated implants will continue to expand into many other anatomical areas and surgical specialties. The future is bright for direct metallic implant production via AM technologies because they are fundamental to eventually creating truly “customized” devices that will focus on functional elements and restoring biomechanical stability in
replaced joints. Additive manufacturing plays a key role in progressing these advanced treatments, based on its core abilities to produce complex objects and to produce these objects with a lot size of one just as easily as producing a lot size of 100. This flexibility will allow for more personalization of care in the areas of joint replacements and, farther in the future, organs as the numbers of people needing these therapies will continue to grow dramatically over the coming decades.
REFERENCES
Davis, J. J., J. V. Bono, and B. G. Lindeque. 2010. Surgical strategies to achieve a custom-fit TKA with standard implant technique. Orthopedics 33(8):569–576.
Hirsch, D. L., E. S. Garfein, A. M. Christensen, K. A. Weimer, P. B. Saddeh, and J. P. Levine. 2009. Use of computer-aided design and computer-aided manufacturing to produce orthognathically ideal surgical outcomes: A paradigm shift in head and neck reconstruction. Journal of Oral and Maxillofacial Surgery 67(10):2115–2122.
Mankovich, N. J., A. M. Cheeseman, and N. G. Stoker. 1990. The display of three-dimensional anatomy with stereolithographic models. Journal of Digital Imaging 3(3):200–203.
Marin, E., S. Fusi, M. Pressacco, L. Paussa, and L. Fedrizzi. 2010. Characterization of cellular solids in Ti6Al4V for orthopaedic implant applications: Trabecular titanium. Journal of the Mechanical Behavior of Biomedical Materials 3(5):373–381.
Mironov, V., R. P. Visconti, V. Kasyanov, G. Forgacs, C. J. Drake, and R. R. Markwald. 2009. Organ printing: Tissue spheroids as building blocks. Biomaterials 30(12):2164–2174.
This Page is Blank








