
School Environments:
Goal, Recommendation, Strategies, and Actions for Implementation
Goal: Make schools a national focal point for obesity prevention.
Recommendation 5: Federal, state, and local government and education authorities, with support from parents, teachers, and the business community and the private sector, should make schools a focal point for obesity prevention.
Strategy 5-1: Require quality physical education and opportunities for physical activity in schools. Through support from federal and state governments, state and local education agencies and local school districts should ensure that all students in grades K-12 have adequate opportunities to engage in 60 minutes of physical activity per school day. This 60-minute goal includes access to and participation in quality physical education.
For Congress, potential actions include
• strengthening the local wellness policy requirement in Section 204 of the Healthy, Hunger-Free Kids Act of 2010 (Public Law 111-296, 111th Cong.,
2d sess. [December 13, 2010] 124, 3183) or the Elementary and Secondary Education Act (Public Law 89-10, 89th Cong., 1st sess. [April 11,1965] 27, 20) by including a requirement for local education agencies to develop and implement a K-12 quality physical education curriculum with proficiency assessments.
For state legislatures and departments of education, potential actions include
• enacting policies with appropriate funding to ensure the provision of daily quality physical education at school for all students in grades K-12; and
• developing, requiring, and financially supporting the implementation of K-12 curriculum standards for quality physical education that (1) are aligned with guidance from practice and/or professional associations and appropriate instructional practice guidelines, and (2) ensure that at least 50 percent of class time is spent in vigorous or moderate-intensity physical activity.
For local education agencies, potential actions include
• adopting requirements that include opportunities for daily physical activity outside of physical education, such as active transport to school programs, intramural sports and activity programs, active recess, classroom breaks, after-school physical activity programming, and integration of physical activity into curricula lesson plans.
For local school districts, potential actions include
• improving and maintaining an environment that is conducive to safe physical education and physical activity.
Strategy 5-2: Ensure strong nutritional standards for all foods and beverages sold or provided through schools. All government agencies (federal, state, local, and school district) providing foods and beverages to children and adolescents have a responsibility to provide those in their care with foods and beverages that promote health and learning. The Dietary Guidelines for Americans provide specific science-based recommendations for optimizing dietary intake to prevent disease and promote health. Implementation of these guidelines would shift children’s and adolescents’ dietary intake to prevent obesity and risk factors associated with chronic disease risk by increasing the amounts of fruits, vegetables, and high-fiber grains they consume; decreasing their consumption of sugar-sweetened beverages, dietary fat in general, solid fats, and added sugars; and ensuring age-appropriate portion sizes of meals and other foods and beverages. Federal, state, and local decision makers are responsible for ensuring that nutrition standards based on the Dietary Guidelines are adopted by schools; these decision makers, in partnership with regulatory agencies, parents, teachers, and food manufacturers, also are responsible for ensuring that these standards are implemented fully and that adherence is monitored so as to protect the health of the nation’s children and adolescents.
For the U.S. Department of Agriculture (USDA), potential actions include
• adopting nutrition standards for all federal child nutrition programs (i.e., the School Breakfast, National School Lunch, Afterschool Snack, Summer Food Service, and Special Milk programs) that are aligned with guidance on optimal nutrition; and
• adopting nutrition standards for all snacks and beverages sold/served outside of federal child nutrition programs that are aligned with guidance on optimal nutrition.
For state legislatures and departments of education, potential actions include
• adopting nutrition standards for foods sold/served outside of federal child nutrition programs that are aligned with guidance on optimal nutrition.
For school boards and state departments of education, potential actions include
• developing school district policies (including wellness policies for districts participating in federal child nutrition programs) and related regulations that include nutrition standards for foods sold/served outside of the federal programs that are aligned with guidance on optimal nutrition.
Strategy 5-3: Ensure food literacy, including skill development, in schools. Through leadership and guidance from federal and state governments, state and local education agencies should ensure the implementation and monitoring of sequential food literacy and nutrition science education, spanning grades K-12, based on the food and nutrition recommendations in the Dietary Guidelines for Americans.
For the federal government, potential actions include
• USDA developing K-12 food and nutrition curriculum guides that can be used by states and updating information in these guides as appropriate with each periodic revision of the Dietary Guidelines for Americans; and
• as USDA develops regulations to implement Section 204 of the Healthy, Hunger-Free Kids Act of 2010 (Public Law 111-296, December 13, 2010), including a requirement for local education agencies to adopt and implement a K-12 food and nutrition curriculum based on state and federal guidance.
For states, state legislatures, and departments of education, potential actions include
• state legislatures and departments of education adopting, requiring, and financially supporting K-12 standards for food and nutrition curriculum based on USDA guidance;
• state departments of education establishing requirements for training teachers in effectively incorporating nutrition education into their curricula;
• states requiring teacher training programs to include curriculum requirements for the study of nutrition;
• state legislatures and departments of education adopting and requiring proficiency assessments for core elements of their state food and nutrition curriculum standards in accordance with the Common Core State Standards Initiative, and local education agency wellness policies articulating ways in which results of food and nutrition education proficiency assessments can be used to inform program improvement; and
• state and local departments of education working with local education agency wellness policies to link changes in the meals provided through child nutrition services with the food literacy and nutrition education curriculum to the extent possible.
Schools are uniquely positioned to support physical activity and healthy eating and therefore can serve as a focal point for obesity prevention among children and adolescents. Schools can be leaders in reversing trends that have made a physically active lifestyle more difficult and high-calorie, nutrient-poor foods more accessible. Children spend up to half of their waking hours in school. In an increasingly sedentary world, schools therefore provide the best opportunity for a population-based approach to increasing physical activity among the nation’s youth. Likewise, because children and adolescents consume up to one-third or even one-half of their daily calories in school, schools have a unique opportunity to influence the quality of their diets.
The mission of schools is broader than simply teaching academic skills. Schools have an acknowledged responsibility for supporting the health and well-being of their students, for example, by requiring immunizations, providing health screenings, and offering meal programs that support a healthy diet. Both physical activity and a nutritious diet are associated with improved cognitive function and academic performance. Physically active and well-nourished students are better able to learn and less likely to miss school for health reasons (Florence et al., 2008; Taras, 2005a; Trudeau and Shepherd, 2010). Improvements in school physical activity and nutrition also will address social inequities, enabling children and
adolescents with the fewest resources to have improved opportunities to become productive citizens.
Federal, state, and local government and education authorities, with support from parents, teachers, and the business community and the private sector, should make schools a focal point for obesity prevention.
School environments are interrelated with the other areas of focus addressed in this report, such as the physical activity and food and beverage environments, discussed in earlier chapters (see Figure 9-1). For example, schools not only provide physical education and serve foods and beverages to students, but also serve as powerful role models, providing a culture that can support, rather than undermine, the efforts of children and adolescents and parents to promote healthful living. As powerful influences, school food-related policies have been shown to affect not only what students consume at school but also what they and their parents perceive to be healthy choices. Immigrant families in particular look to public institutions to learn about cultural norms and practices (Gordon-Larsen et al., 2003). As far back as 1946, a report of the House Committee on Agriculture during hearings for the National School Lunch Act1 stated that “the educational features of a properly chosen diet served at school should not be under-emphasized. Not only is the child taught what a good diet consists of, but his parents and family likewise are indirectly instructed.”
Structuring school environments to encourage and support physical activity and healthy living offers a unique opportunity to reach nearly all children and adolescents, promoting their health both today and in the future, as lifelong health habits are initiated early in life. Today, the role of the school is more important than ever as fewer families have a parent at home who is not participating in the paid labor force, and children and adolescents are spending more time in before- and after-school programs outside of the home.
The Healthy, Hunger-Free Kids Act of 20102 created an opportunity to improve nutrition for students in the school setting. Recent efforts to change school physical education and food policies have been well received, but they are neither widespread, integrated, nor strong enough to produce the needed reduc-
![]()
1 Public Law 396, 79th Cong., 2d sess. (June 4, 1976), 60, 231.
2 Public Law 111-296, 111th Cong., 2d sess. (December 13, 2010), 124, 3183.
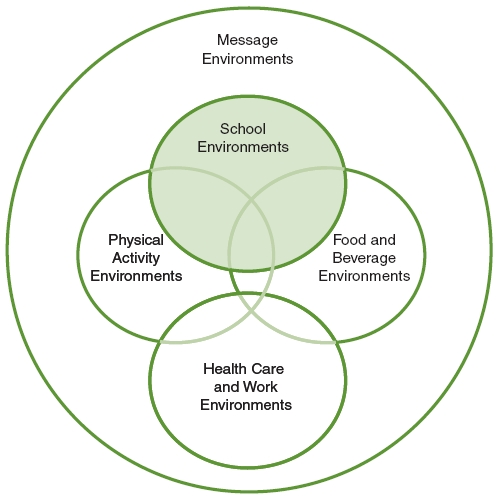
FIGURE 9-1 Five areas of focus of the Committee on Accelerating Progress in Obesity Prevention.
NOTE: The area addressed in this chapter is highlighted.
tion in childhood obesity rates. The committee recommends three strategies and associated actions to address these limitations. These strategies and actions are detailed in the remainder of this chapter. Indicators for measuring progress toward the implementation of each strategy, organized according to the scheme presented in Chapter 4 (primary, process, foundational), are presented in a box following the discussion of that strategy.
The strategies in this chapter are focused on school-aged children because of the broad reach of schools to children and adolescents. Early childhood education is not nationalized, nor is there sufficient evidence for all of the strategies presented in this chapter as applied to preschools to recommend all of them for
younger children. The committee recognizes that the earlier years are critical times to promote children’s health and has offered recommendations for physical activity in child care centers (Chapter 5, Strategy 1-3) and nutrition standards for government-owned and/or -operated child care centers (Chapter 6, Strategy 2-3).
STRATEGIES AND ACTIONS FOR IMPLEMENTATION
Strategy 5-1: Require Quality Physical Education and Opportunities for Physical Activity in Schools
Through support from federal and state governments, state and local education agencies and local school districts should ensure that all students in grades K-12 have adequate opportunities to engage in 60 minutes of physical activity per school day. This 60-minute goal includes access to and participation in quality physical education.
For Congress, potential actions include
• strengthening the local wellness policy requirement in Section 204 of the Healthy, Hunger-Free Kids Act of 2010 (Public Law 111-296, December 13, 2010) or the Elementary and Secondary Education Act (Public Law 89-10, 89th Cong., 1st sess. [April 11, 1965] 27, 20) by including a requirement for local education agencies to develop and implement a K-12 quality physical education curriculum with proficiency assessments.
For state legislatures and departments of education, potential actions include
• enacting policies with appropriate funding to ensure the provision of daily quality physical education at school for all students in grades K-12; and
• developing, requiring, and financially supporting the implementation of K-12 curriculum standards for quality physical education that (1) are aligned with guidance from practice and/or professional associations and appropriate instructional practice guidelines, and (2) ensure that at least 50 percent of class time is spent in vigorous or moderate-intensity physical activity.
For local education agencies, potential actions include
• adopting requirements that include opportunities for daily physical activity outside of physical education, such as active transport to school programs, intramural sports and activity programs, active recess, classroom breaks, after-school physical activity programming, and integration of physical activity into curricula lesson plans.
For local school districts, potential actions include
• improving and maintaining an environment that is conducive to safe physical education and physical activity.
Context
Data from the 2006 School Health Policies and Programs Study (Lee et al., 2007) indicate that nationwide, 78 percent of schools require students to take some physical education as a requirement for graduation or promotion to the next grade or school level (69 percent of elementary schools, 84 percent of middle schools, and 95 percent of high schools). The frequency and length of activity breaks, opportunities for physical education, and adherence to expert guidance and assessment in implementing these requirements vary widely by school district, state, and grade level.
A small number of schools provide physical education opportunities at all grade levels every day or even a few days a week. In 2006, nearly 4 percent of all elementary schools (excluding kindergarten), 8 percent of all middle schools, and 2 percent of all high schools provided daily physical education or its equivalent for the entire school year for students in all grades. More schools provide physical education or its equivalent at least 3 days per week for the entire school year— almost 14 percent of elementary schools (excluding kindergarten), 15 percent of middle schools, and 3 percent of high schools (Lee et al., 2007).
Apart from physical education opportunities, the number and length of physical activity breaks required throughout the school day vary by state, district, and grade. Among all school districts, 39 percent require or recommend 30 minutes or more of recess per day, 23 percent require or recommend 20-29 minutes per day, and 16 percent require or recommend 10-19 minutes per day in elementary schools. Among all districts, 16 percent require and 25 percent recommend that elementary schools provide regular physical activity breaks; 10 percent of all dis-
tricts require and 24 percent recommend that middle schools provide such breaks; and 4 percent of all districts require and 9 percent recommend that high schools provide such breaks (Lee et al., 2007). Among all states, 14 percent have a policy encouraging districts or schools to support or promote walking or biking to and from school, and nearly 18 percent of all districts have a policy that supports or promotes walking or biking to and from school.
Significant improvement has been seen in state and district policies to follow expert guidelines in implementing physical education policies. Between 2000 and 2006, the percentage of states that required or encouraged districts or schools to follow standards or guidelines based on the National Standards for Physical Education increased from 59 percent to 76 percent. In addition, the percentage of districts with a policy stating that schools must follow national, state, or district physical education standards or guidelines increased from 67 percent to 81 percent (Lee et al., 2007).
Finally, state assessment and graduation proficiency requirements for physical education are limited. The 2010 Shape of the Nation report (NASPE and AHA, 2010) found that 27 percent of states require that grades be given for physical education classes, but few include physical education in comprehensive assessment tests, if given. Of the 40 states that have an education “report card” for schools, only 5 include physical education in that report. Of the 45 states that require high school physical education, 75 percent specify the number of credits needed for graduation (12 states require 0.5 credit; 15 states require 1 credit; 3 states require 1.5 credits; 7 states requires 2 credits; and New Jersey requires 3.75 credits per year, the highest in the nation). In addition, 9 states require a health or wellness course to fulfill graduation requirements. Physical education is required only in grades K-12 in five states (Illinois, Iowa, Massachusetts, New Mexico, and Vermont) and is required in grades 1-12 in two states (New Jersey and Rhode Island).
The inconsistencies in frequency, duration, assessments, and requirements for physical education and opportunities for physical activity breaks throughout the day indicate that states and local education agencies can improve policies to help students achieve 60 minutes of physical activity per day.
Evidence
The 2005 Institute of Medicine (IOM) report Preventing Childhood Obesity: Health in the Balance recommends that children and adolescents participate in a minimum of 30 minutes of physical activity during the school day and that opportunities for physical activity and physical education be expanded. In addition, the
report recommends that health curricula be enhanced to devote adequate attention to physical activity, reducing sedentary behaviors, nutrition, and energy balance, with a focus on behavioral skills (IOM, 2005). Many of these recommendations were based on a systematic review of the effectiveness of increasing the amount of time students spend in physical education, as well as large-scale school-based interventions that have been successful in increasing activity levels. Likewise, the Task Force on Community Preventive Services concluded that there is strong evidence that school-based physical education increases levels of physical activity, although evidence indicates minimal or inconsistent effects on body mass index (BMI) (Kahn et al., 2002). Another review found that two elementary school-based interventions—SPARK (Sports, Play, and Active Recreation for Kids) and CATCH (Coordinated Approach To Child Health)—and a small number of interventions involving older students were effective in increasing activity levels, with some interventions being associated with positive improvements in BMI (IOM, 2005). Reviews also have concluded that attending longer physical education classes did not affect academic performance (Kahn et al., 2002).
Schools’ interest in physical activity begins with the brain (Trudeau and Shepherd, 2010). Movement and exercise increase breathing and heart rate so that more blood flows to the brain, thus enhancing energy production and waste removal. Physical activity oxygenates the brain, which is why taking a walk can help people “clear their head” and think better. Exercise has effects as well on higher mental executive functions involving memory, planning, organization, and the capability to juggle different intellectual tasks (Sibley and Etnier, 2003). Exercise also helps youth who have difficulty with impulse control (Kelder, 2010). A recent meta-analysis studying the impact of combinations of school-based interventions focused on increasing physical activity among children and adolescents aged 6-18 found “good evidence that school-based physical activity interventions have a positive impact on” duration of physical activity, television viewing, VO2 max,3 and blood cholesterol (Dobbins et al., 2009, p. 24). The authors also report that, in addition to the positive outcomes they studied, “the current evidence suggests that school-based physical activity interventions may be effective in the development of healthy lifestyle behaviors among children and adolescents, which will then translate into reduced risk for many chronic diseases and cancers in adulthood. The evidence also suggests that the best primary strategy for improving the long-term health of children and adolescents through exercise may be creating lifestyle patterns of regular physical activity that carry over to the adult years” (Dobbins et al., 2009, p. 2).
![]()
3 Maximal oxygen uptake.
Mounting evidence shows a positive relationship between physical activity and academic performance. A systematic review of observational and longitudinal studies (Singh et al., 2012) suggests that there is a significant positive relationship between physical activity and academic performance, although just 2 of the 14 studies included in the review were judged as being of “high methodological quality.” Nonetheless, this cautious conclusion was supported by two earlier reviews (Taras, 2005b; Trudeau and Shephard, 2008). A Centers for Disease Control and Prevention (CDC) synthesis of the literature on the association between school-based physical activity (including physical education, recess, classroom physical activity, and extracurricular physical activity) and academic performance (based on measures of academic achievement, academic behavior, and cognitive skills and attitudes) (CDC, 2010b) found 251 associations between the two. Of these, 50.5 percent were positive, 48 percent were not significant, and 1.5 percent were negative. In the context of school-based physical education, the available studies (n = 14) show that overall, increased time in physical education appears to have a positive or no relationship with academic achievement, and not a negative relationship. A review by Woodward-Lopez and colleagues (2010a) reports that physical activity is critical for optimal brain function and the ability to learn; positively influences academic performance; and can improve classroom behavior, attendance, and students’ psychological well-being.
Implementation
It is important to encourage young people to participate in physical activities that are appropriate for their age, that are enjoyable, and that offer a wide variety of options. The focus at schools for decades has been on physical education and after-school extracurricular activities and sports. As described earlier, current district and state physical education policies and programs vary nationwide. At the national level, the Healthy, Hunger-Free Kids Act of 20104 requires, at a minimum, that goals for physical activity be included in all school wellness policies. The 1965 Elementary and Secondary Education Act,5 which provides support for the development and improvement of physical education programs in schools, offers opportunities to encourage the development and adoption of consistent quality physical education at all grade levels across the country.
General physical education opportunities and after-school activities and sports usually are guided by a qualified instructor or coach. However, this is not always
![]()
4 Public Law 111-296 (December 13, 2010).
5 Public Law 89-10 (April 13, 1965).
the case. Noncurricular programs can contribute to increases in the frequency (daily), duration (60+ minutes), and intensity (vigorous or moderate or weight bearing) of activity (Kelder, 2010). A number of noncurricular physical activity strategies have been reviewed and are recommended as promising ways to increase physical activity throughout the school day (California Project LEAN, 2009; Jago and Baranowski, 2004; NASPE, undated). As reviewed by Kelder (2010, pp. 30-34), these evidence-based strategies include
• daily classroom physical activity breaks,
• organized physical activity during after-school programs,
• walking trails and active commuting (i.e., walking or biking) to/from school,
• access to the kind of equipment found in fitness clubs at school,
• walking programs or “open gym” in the morning before school begins,
• intramural sport teams for students not interested in competitive sports,
• evening events that provide a safe place for students to play, and
• annual campus or community events to heighten community awareness of physical activity and health.
Additionally, redesigned and renovated school playgrounds have been found to increase overall playground utilization and improve the physical activity levels of children and adults during school as well as after-school hours (Anthamatten et al., 2011; Brink et al., 2010; Colabianci et al., 2009; Ridgers et al., 2007). Combining quality physical education curriculum standards (i.e., guidelines of the National Standards for Physical Education) and proficiency assessments guided by professional experts with such additional noncurriculum opportunities for physical activity (before, during, and after school) will be necessary to help students achieve the recommended activity levels (i.e., 60 or more minutes of physical activity each day) and create a lifestyle pattern that will continue into their adult lives. Although these quality standards may pose a challenge given core curriculum requirements, combining physical education time with noncurricular physical activity strategies is a critical step in ensuring that children receive the recommended 60 minutes of daily physical activity and should be the goal for all schools.
Indicators for Assessing Progress in Obesity Prevention for Strategy 5-1
Primary Indicator
• Increase in the prevalence of children and adolescents meeting physical activity guidelines of 60 minutes per day of vigorous or moderate-intensity physical activity.*
Sources for measuring indicator: YRBSS and NHANES (additional sources needed for measurement of indicator)
Process Indicators
• Increase in the proportion of school-aged children and adolescents enrolled in school physical education.
Sources for measuring indicator: YRBSS and NYPANS (additional sources needed for measurement of indicator)
• Increase in the proportion of states with policies requiring that at least 50 percent of physical education time be spent in vigorous or moderate-intensity physical activity for each grade level.
Sources for measuring indicator: CLASS (NCI), CDC’s State School Health Profiles, CDC’s School Health Policies and Programs Study
• Increase in the proportion of districts with policies requiring that at least 50 percent of physical education time be spent in vigorous or moderate-intensity physical activity for each grade level.
Sources for measuring indicator: CDC’s School Health Policy and Programs Study and Bridging the Gap District Wellness Policy Study
• Increase in the proportion of schools with policies requiring that at least 50 percent of physical education time be spent in vigorous or moderate-intensity physical activity for each grade level.
Source for measuring indicator: CDC’s School Health Policy and Programs Study
• Increase in the proportion of schools providing opportunities for school-based physical activity outside of physical education.
Source for measuring indicator: CDC’s School Health Policy and Programs Study
Foundational Indicators
• Increase in the frequency of CDC’s School Health Policy and Programs Study to every 2 years.
Source needed for measurement of indicator.
• Increase in the frequency of CDC’s National Youth Physical Activity and Nutrition Survey to every 2 years.
Source needed for measurement of indicator.
• Development of monitoring systems to capture objectively measured and context-specific data on participation in physical activity for all grade levels.
Source needed for measurement of indicator.
NOTE: CDC = Centers for Disease Control and Prevention; CLASS = Classification of Laws Associated with School Students; NCI = National Cancer Institute; NHANES = National Health and Nutrition Examination Survey; NYPANS = National Youth Physical Activity and Nutrition Survey; YRBSS = Youth Risk Behavior Surveillance System.
![]()
*See Box B-1 in Appendix B.
All government agencies (federal, state, local, and school district) providing foods and beverages to children and adolescents have a responsibility to provide those in their care with foods and beverages that promote health and learning. The Dietary Guidelines for Americans provide specific science-based recom-
mendations for optimizing dietary intake to prevent disease and promote health. Implementation of these guidelines would shift children’s and adolescents’ dietary intake to prevent obesity and risk factors associated with chronic disease risk by increasing the amounts of fruits, vegetables, and high-fiber grains they consume; decreasing their consumption of sugar-sweetened beverages, dietary fat in general, solid fats, and added sugars; and ensuring age-appropriate portion sizes of meals and other foods and beverages. Federal, state, and local decision makers are responsible for ensuring that nutrition standards based on the Dietary Guidelines are adopted by schools; these decision makers, in partnership with regulatory agencies, parents, teachers, and food manufacturers, also are responsible for ensuring that these standards are implemented fully and that adherence is monitored so as to protect the health of the nation’s children and adolescents.
For the U.S. Department of Agriculture (USDA), potential actions include
• adopting nutrition standards for all federal child nutrition programs (i.e., the School Breakfast, National School Lunch, Afterschool Snack, Summer Food Service, and Special Milk programs) that are aligned with guidance on optimal nutrition; and
• adopting nutrition standards for all snacks and beverages sold/served outside of federal child nutrition programs that are aligned with guidance on optimal nutrition.
For state legislatures and departments of education, potential actions include
• adopting nutrition standards for foods sold/served outside of federal child nutrition programs that are aligned with guidance on optimal nutrition.
For school boards and state departments of education, potential actions include
• developing school district policies (including wellness policies for districts participating in federal child nutrition programs) and related regulations that include nutrition standards for foods sold/served outside of the federal programs that are aligned with guidance on optimal nutrition.
Context
The relationship between access to healthy foods and dietary behaviors is well established (Larson et al., 2009; see also Chapter 6). Studies demonstrate that individuals with access to a greater abundance of healthy foods consume more fresh produce and other healthful items, and individuals with less access to these foods are less likely to eat a healthy diet (Treuhaft and Karpyn, 2010). Those institutions entrusted with caring for the nation’s children and adolescents have an opportunity to provide food options for children and adolescents that will not promote obesity and compromise their health, but promote their health and learning.
Numerous government agencies at the federal, state, and local levels provide foods served to children and adolescents in schools. These agencies contribute financial and/or material resources to feed children and adolescents in schools, in after-school programs, and in summer feeding programs. Because of the scale of these programs, they are a critical partner in efforts to prevent obesity. The foods provided in school settings serve two purposes: nourishing children and adolescents, and educating them and their parents about healthy dietary patterns. “If a school’s setting is intended to be a learning environment for children, the issue [of] healthful food choices needs to be a priority” (Pilant, 2006, p. 125). Currently, schools must offer meals consistent with the National School Lunch and Child Nutrition Act Amendments.6 These regulations require that school meals provide a minimum percentage of the Recommended Dietary Allowances (RDAs) to protect against nutritional deficiencies that would impair children’s growth and development.
Both the National School Lunch Program and the original national RDAs were created to foster the nutritional health of America’s youth during the decade of World War II. Guidance on kinds and amounts of foods to be provided at each meal was institutionalized. In the decades that followed, less nutritious foods outside of the meal program began being sold at schools, providing additional revenues for school groups or food service departments. Although disputes about providing foods with little nutritional value to compete with school meals arose, these foods, termed competitive foods, remained. As the body of evidence about the dietary crisis among children and adolescents in the United States grew, so, too, did understanding of the association between the diets of children and adoles-
![]()
6 Public Law 94-105, 94th Cong., 1st sess. (October 7, 1975). Amendments: Public Law 95-166, 95th Cong., 1st sess. (November 10, 1977); Public Law 97-35, 97th Cong., 1st sess. (August 13, 1981); Public Law 99-591, 99th Cong., 1st sess. (October 30, 1986).
cents and not only nutritional deficiencies, but also health problems (IOM, 2005, 2007, 2010; NRC, 1989). In recognition of the importance of providing foods to children and adolescents that will promote their health and reduce their risk of obesity, the Healthy, Hunger-Free Kids Act of 20107 gave USDA the mandate to develop regulations governing all foods sold and served on school campuses, including foods and beverages sold outside of school meal programs.
The guidance on school food for the Healthy, Hunger-Free Kids Act is found in two IOM reports. The first, Nutrition Standards for Foods in Schools: Leading the Way Toward Healthier Youth (IOM, 2007), recommends that competitive foods offered on school campuses contribute to rather than compete with an overall healthful eating environment. Based on the nutrition evidence in the Dietary Guidelines for Americans, the report outlines specific food and nutrition standards for all foods and beverages sold in schools outside of school meal programs. Soon afterward, the IOM Committee on School Meals was tasked with reviewing and assessing the food and nutrition needs of school-aged children and adolescents using the most recent Dietary Guidelines in order to recommend updates to the guidance regarding the foods and beverages served in the National School Lunch and School Breakfast Programs (IOM, 2010). The recommendations in both of these reports serve as the foundation for current school food strategies to accelerate progress toward preventing obesity.
Given that school breakfast and lunch programs may account for more than half of a child’s daily calorie intake (IOM, 2010), their dietary impact can be substantial. Further, as noted above, the potential reach of school-based nutrition interventions is unparalleled, extending to nearly all children and adolescents in the United States, including the most difficult-to-reach, underserved populations (IOM, 2010).
Evidence
The 2010 Dietary Guidelines for Americans provide evidence-based dietary recommendations encompassing two concepts: helping individuals achieve and maintain a healthy weight and focus on consuming nutrient-dense foods and beverages. They include the following:
• Individuals should prepare, serve, and consume smaller portions at home, and eat smaller portions while eating out.
• Consumption of fruits and vegetables should be increased in childhood.
![]()
7 Public Law 111-296 (December 13, 2010).
• Children should consume recommended levels of low-fat and fat-free dairy products.
• Children should consume more and a greater variety of high-fiber foods.
• Total fat should not exceed IOM-recommended ranges and should consist of primarily mono- and polyunsaturated fatty acids.
• Consumption of sugar-sweetened beverages should be discouraged.
• The intake of surplus energy in the form of empty calories from added sugars and solid fats should be controlled.
The guidance provided in the two above-cited IOM reports addresses each of these recommendations. It identifies the amount of each food group (fruits, vegetables, whole grains, milk, meat and other protein foods, and oils) needed by children and adolescents in each age category, and recommends that competitive foods contribute to meeting these specific food requirements as well. Appendix 7 in the 2010 Dietary Guidelines for Americans shows recommended average daily intake amounts for each food group or subgroup at all calorie levels. The last three recommendations listed above are addressed in the 2005 Dietary Guidelines as discretionary calories (calories from any source that can be used flexibly after nutrient needs have been fulfilled) and in the 2010 Dietary Guidelines as solid fats and added sugars. The 2005 and 2010 Dietary Guidelines (HHS, 2005, 2010) recommend specific daily limits on the amounts of solid fats and added sugars in the diets of children and adolescents in accordance with health standards (see 2010 Dietary Guidelines, Appendix 7). Assuming that children and adolescents eat at least one-third of their calories during the school day, the limit on calories from added solid fats and added sugars obtained during the school day ranges from 40 calories for the 1,600-calorie/day plan, to 86 calories for the 2,000-calorie/day plan, to 110 calories for the 2,400-calorie/day plan. An understanding of the trade-off between snack foods and whole foods, including fruits, vegetables, whole grains, and protein foods, informs the standards for competitive foods. Snack foods and beverages sold in schools have been displacing the foods needed for a healthy diet. Both of the above-cited IOM reports (2007, 2010) are grounded in evidence demonstrating that school meals influence children’s overall daily dietary intake (USDA, 2007).
There is evidence that nutrition standards for foods sold in schools can be implemented by schools, garner positive responses from students, and reduce students’ intake of less healthy foods, and may be associated with reductions in children’s BMI increases. Recent studies examining state and local implementation
of nutrition standards have demonstrated that schools are able to comply with new food and beverage standards (Cullen and Watson, 2009; Long et al., 2010; Phillips et al., 2010; Woodward-Lopez et al., 2010b) and that students respond favorably to the provision of more healthy foods in school (Gosliner et al., 2011). Limiting access to the least healthy foods and beverages in schools has been shown to lead to a reduction in students’ overall consumption of these items (Schwartz et al., 2009; Woodward-Lopez et al., 2010b). In addition to changes in the school food environment that impact children’s dietary intake (CDC, 2010a; Cullen et al., 2008; Mendoza et al., 2010), there is evidence of an association, although not necessarily causal, between policies limiting competitive foods and beverages and a reduction in child BMI increases over the past 10 years (Sanchez-Vaznaugh et al., 2010).
There may be concern that reduced revenues from competitive foods (including those sold in vending machines) will adversely affect a school’s financial status. Woodward-Lopez and colleagues (2010b) assessed the impact of legislation in California that instituted nutrition standards for competitive foods and beverages. They report a decrease in competitive food and beverage sales from vending machines, snack bars and stores, and school fundraisers. Although food service à la carte sales decreased by 60 percent, increases in meal sales increased enough to compensate for the reduction in à la carte sales and lead to an increase in total school food revenues. Overall, the school food service bottom line deteriorated because food service expenditures outpaced revenue increases during the time period under study, but the food service directors who were interviewed for the study did not believe the increased costs were attributable to their wellness efforts (Woodward-Lopez et al., 2010b). In Seattle, recent anecdotal evidence shows that revenues from vending machine sales sharply decreased when healthier items replaced other foods in response to a school policy, leaving high school-associated student body governments with less funding than before. School officials are considering new vending machine offerings that still meet the nutrition standards, but are expected to garner increased sales (Wood, 2011).
Implementation
Implementation of this strategy and associated actions will have to occur at the federal, state, and local (district) levels. Box 9-1 details additional actions that can be taken to implement this strategy.
Federal level With the adoption of the Child Nutrition and WIC Reauthorization Act of 2004,8 USDA was given the mandate to propose new meal patterns and nutrition standards for foods served in the National School Lunch Program and School Breakfast Program to align them with the Dietary Guidelines for Americans. The Healthy, Hunger-Free Kids Act of 20109 specified that schools would receive an additional reimbursement of 6 cents for each meal served that adheres to the new standards. USDA issued proposed revisions (USDA/FNS, 2011) in line with the IOM recommendations for school meals (IOM, 2008, 2010), which generated approximately 130,000 comments. In January 2012, USDA issued a final rule for the nutrition standards (USDA/FNS, 2012).
Also with the adoption of the Healthy, Hunger-Free Kids Act of 2010,10 USDA was given the mandate to regulate competitive foods and beverages sold in schools, which would include foods sold in à la carte lines in the cafeteria, vending machines, in snack bars and stores, and for fundraisers. At the time that this report went to press, USDA was gathering evidence on this issue and developing a proposed rule for public comment. The act does not preempt stronger standards at the state or district level, so the federal standards are expected to provide a floor rather than a ceiling.
State level The federal government can create broad policies designed to encourage schools to provide healthier foods, but it is up to state and local governments to implement those policies in ways that promote healthful eating. Currently, most states have standards for competitive foods and beverages, but they vary greatly and tend to be weak overall. Most state standards focus specifically on foods and beverages sold outside of school meal programs (i.e., competitive foods and beverages) and do not address foods/beverages sold or served during summer months or in before- and after-school settings. Implementation studies in states with relatively strong standards—Arkansas, California, and Texas, in particular—have shown positive impacts of these standards on food/beverage availability and consumption and net energy intake.
After Arkansas Act 1220 was implemented, annual surveys of principals and superintendents showed that schools were more likely to require healthy food options at student parties and concession stands and to offer skim milk in the cafeteria, and less likely to make vending machines available during lunch periods
![]()
8 Public Law 108-265, 108th Cong., 2d sess. (June 30, 2004), 118, 729.
9 Public Law 111-296 (December 13, 2010).
10 Public Law 111-296 (December 13, 2010).
BOX 9-1
Additional Potential Actions for Implementing School Nutritional Standards Based on the Dietary Guidelines for Americans
Guideline 1: Increase the contribution of fruits, vegetables, whole grains, low-fat and fat-free milk and milk products, and protein foods to the diets of children and adolescents aged 2 and older.
For Congress:
• Support full implementation of the Healthy, Hunger-Free Kids Act of 2010 (Public Law 11-296, December 13, 2010).
• Upwardly adjust meal reimbursement rates as necessary for full implementation of nutrition requirements.
For the U.S. Department of Agriculture (USDA) and other federal agencies:
• Implement school meal standards consistent with Institute of Medicine (IOM) recommendations.
• Adopt the strictest IOM recommendations for all foods and beverages sold/ provided outside of school meal programs to allow only foods that contribute to meeting the nutritional requirements of children and adolescents (fruits, vegetables, whole grains, low-fat and fat-free dairy products, and other protein foods) to ensure that less healthy foods and beverages do not compete with those foods.
• Require programs to monitor compliance with nutrition standards.
• Amend local wellness policies to include strategies that support the implementation of nutrition standards in school meal and competitive food venues.
For state legislatures and departments of education:
• Evaluate programs aimed at improving students’ intake of the above foods to highlight innovations and barriers to implementation.
• Support federal standards for school meals and competitive foods.
• Create professional development modules to help school nutrition professionals implement nutrition standards.
For local school districts and schools:
• Adopt supportive policies that encourage schools to adhere to updated federal nutrition standards.
• Develop and distribute a resource list to help school groups raise money without selling foods that fail to meet nutrition standards.
• Allocate adequate space and other necessary resources for the procurement, provision, and preparation of foods that meet nutrition standards.
• Encourage the participation of students and parents in menu development and product selection so that foods served are appealing to the student population.
• Maintain active wellness policy councils to support healthy food environments.
Guideline 2: Reduce the percentage of total energy in the diets of children and adolescents derived from added sugars and solid fats (fat intake should come primarily from mono- and polyunsaturated fatty acids).
For Congress:
• Support full implementation of the Healthy, Hunger-Free Kids Act of 2010 (Public Law 11-296, December 13, 2010).
For USDA and federal agencies:
• Adopt the strictest interpretation of the IOM school meal and competitive food standards.
• Provide guidance to schools and the food and beverage industry regarding the importance of the new standards and how to implement them to ensure that calories from sugars and solid fats are replaced with healthier calories.
• Require programs to monitor compliance with nutrition standards.
• Amend local wellness policies to include strategies that support the implementation of nutrition standards in school meal and competitive food venues.
For state legislatures and departments of education:
• Promote adequate school funding and suggestions for alternative school fundraisers to reduce the need for food sales to support school groups and programs.
• Develop monitoring systems to ensure that child care and recreation programs sponsored by the state but not participating in the National School Lunch Program comply with standards limiting foods and beverages with added sugars and solid fats.
For local school districts and schools:
• Work with students to develop a selection of appealing foods and beverages that do not include items high in added sugars and solid fats.
• Implement the strictest interpretation of the IOM school meal and competitive food standards.
• Create budgets that do not rely on snack food and beverage sales to support important school programs.
Guideline 3: Ensure that portion sizes as served are age-appropriate for children and adolescents.
For Congress:
• Support implementation of the Healthy, Hunger-Free Kids Act of 2010 (Public Law 11-296, December 13, 2010).
For USDA and federal agencies:
• Develop guidance that establishes adequate but not excessive food portions for children and adolescents. Include maximum allowances for calories in school meals.
For state legislatures and departments of education:
• Develop portion size standards for foods and beverages served to children and adolescents in programs not within the reach of the National School Lunch, School Breakfast, and Summer Food Service programs.
For local school districts and schools:
• Ensure that food service staff are trained in and knowledgeable about appropriate portion sizes for children and adolescents of various ages.
• Develop strategies for monitoring portion sizes and ensuring that they are consistent with recommendations for children and adolescents of various ages. These may include relatively simple strategies such as offering smaller portions, using smaller dishware, or removing trays from the school lunchroom (Fischer et al., 2003; Just and Wansink, 2009; Rolls et al., 2004; Wansink, 2010).
or to include sodas in vending machines (Phillips et al., 2010). Woodward-Lopez and colleagues (2010b) observed in California an increase in standards-compliant items, a decrease in noncompliant items, and a reduction in at-school consumption of noncompliant items without an increase in home consumption of those items. They called the improvements modest, recognizing that many compliant items were fat- and sugar-modified products of low nutritional value. And an evaluation of the Texas School Nutrition Policy, an unfunded mandate, showed that post-policy changes included significant reductions in high-fat vegetable items served by school cafeterias and sales of large bags of chips at snack bars, and increases in sales of baked chips (Cullen and Watson, 2009).
A difference between adherence to nutrition standards for beverages and to nutrition standards for foods has been observed, and there are a number of possible reasons for this inconsistency. Samuels and colleagues (2009), Wood and colleagues (2010), and Woodward-Lopez and colleagues (2010b) explain that the way standards are written may make it easier to identify beverages that meet standards than foods that do so. A California policy specifies categories of compliant beverages (e.g., water, sports drinks, or milk with a certain fat percentage), but for foods, specifies nutrient limits instead of categories. Thus, determining whether a food is compliant requires multiple calculations to determine whether the amounts of calories, saturated fat, and other nutrients are compliant. Samuels and colleagues (2009) suggest that specifying compliant categories of foods would make policies easier for personnel to implement, but they acknowledge that establishing criteria for such categories would be a more complex task than it is for beverages. In addition, similar food products (for example, different flavors of similar products from the same brand) from the same manufacturer may vary in compliance because of slightly different nutrient compositions, causing confusion among personnel responsible for implementing the standards.
District level Beginning with the 2006-2007 school year, all local education agencies (i.e., school districts) participating in the federal child nutrition programs were required to adopt and implement a school wellness policy. As of school year 2009-2010, nearly all districts nationwide had such a policy, but they were fairly vague. The standards for competitive foods and beverages were one of the weakest elements, particularly in policies focused at the middle and high school levels (Chriqui et al., 2010). Box 9-1 provides additional suggested action steps for implementing this strategy.
Indicators for Assessing Progress in Obesity Prevention for Strategy 5-2
Primary Indicators
• Increase in the percentage of energy intake in schools attributable to the consumption of foods and beverages recommended by the Dietary Guidelines for Americans for children and adolescents aged 2 and older.*
Sources for measuring indicator: NHANES, NYPANS, and YRBSS
• Reduction in the percentage of total energy in the diets of children and adolescents consumed at school derived from added sugars and solid fats (fat intake should come primarily from mono- and polyunsaturated fatty acids).
Sources for measuring indicator: NHANES, NYPANS, and YRBSS
Process Indicators
• Adoption of regulations by the USDA that require all foods and beverages sold/served in schools to be aligned with the Dietary Guidelines for Americans recommendations.*
Sources for measuring indicator: CLASS (NCI), CDC State School Health Profiles, and SHPPS
• Increase in the proportion of states with laws and regulations requiring that all foods sold/served in schools be aligned with the Dietary Guidelines for Americans recommendations.*
Sources for measuring indicator: CLASS (NCI), CDC State School Health Profiles, and SHPPS
• Increase in the proportion of school districts with policies requiring that all foods sold/served in schools be aligned with the Dietary Guidelines for Americans recommendations.*
Sources for measuring indicator: SHPPS and Bridging the Gap District Wellness Policy Study
• Increase in the percentage of public and private schools that adhere to the IOM’s (2007) Tier 1 and Tier 2 food standards.
Sources for measuring indicator: SNDA, USDA program monitoring/ reporting, and SHPPS
Foundational Indicators
• Increase in the frequency of CDC’s School Health Policy and Programs Study to every 2 years.
Source needed for measurement of indicator.
• Increase in the frequency of CDC’s National Youth Physical Activity and Nutrition Survey to every 2 years.
Source needed for measurement of indicator.
• Addition of dietary questions to CDC’s Middle School Youth Risk Behavior Surveillance System, particularly questions related to sugar-sweetened beverages and access to such beverages in schools.
Source needed for measurement of indicator.
• Conduct of USDA’s School Nutrition Dietary Assessment Study every 5 years.
Source needed for measurement of indicator.
• Inclusion of population-representative subgroups of children and adolescents aged 2-5, 6-12, and 13-18 in CDC’s NHANES.
Source needed for measurement of indicator.
NOTE: CDC = Centers for Disease Control and Prevention; CLASS = Classification of Laws Associated with School Students; IOM = Institute of Medicine; NCI = National Cancer Institute; NHANES = National Health and Nutrition Examination Survey; NYPANS = National Youth Physical Activity and Nutrition Survey; SHPPS = School Health Policies and Practices Study; SNDA = School Nutrition Dietary Assessment Survey; USDA = U.S. Department of Agriculture; YRBSS = Youth Risk Behavior Surveillance System.
![]()
*See Box B-1 in Appendix B.
Strategy 5-3: Ensure Food Literacy, Including Skill Development, in Schools
Through leadership and guidance from federal and state governments, state and local education agencies should ensure the implementation and monitoring of sequential food literacy and nutrition science education, spanning grades K-12, based on the food and nutrition recommendations in the Dietary Guidelines for Americans.
For the federal government, potential actions include
• USDA developing K-12 food and nutrition curriculum guides that can be used by states and updating information in these guides as appropriate with each periodic revision of the Dietary Guidelines for Americans; and
• as USDA develops regulations to implement Section 204 of the Healthy, Hunger-Free Kids Act of 2010 (Public Law 111-296, December 13, 2010), including a requirement for local education agencies to adopt and implement a K-12 food and nutrition curriculum based on state and federal guidance.
For states, state legislatures, and departments of education, potential actions include
• state legislatures and departments of education adopting, requiring, and financially supporting K-12 standards for food and nutrition curriculum based on USDA guidance;
• state departments of education establishing requirements for training teachers in effectively incorporating nutrition education into their curricula;
• states requiring teacher training programs to include curriculum requirements for the study of nutrition;
• state legislatures and departments of education adopting and requiring proficiency assessments for core elements of their state food and nutrition curriculum standards in accordance with the Common Core State Standards Initiative, and local education agency wellness policies articulating ways in which results of food and nutrition education proficiency assessments can be used to inform program improvement; and
• state and local departments of education, working with local education agency wellness policies, to link changes in the meals provided through child nutrition services with the food literacy and nutrition education curriculum to the extent possible.
Context
Current data on the efficacy of new programs designed to teach food and nutrition to children and adolescents in a school setting provide critical support for changes in the food environment to prevent obesity and promote health. The 2010 Dietary Guidelines for Americans recommend providing nutrition education programs in educational settings. The content of food and nutrition education should be based on the Dietary Guidelines, which provide the current evidence linking nutrition to the prevention of disease and promotion of health. During the last decade, however, despite an increased focus on efforts to prevent childhood obesity and evidence supporting the impact of nutrition education on dietary behaviors and weight outcomes, school programs providing nutrition education have remained inconsistent and underemphasized. Today, few schools offer the necessary intensity or quality of such education or a coordinated grade-level curricular approach. While 74 percent of elementary, 73 percent of middle, and 24 percent of high schools provided some nutrition content in every grade during the 2004-2005 school year (Briefel et al., 2009), data from CDC’s School Health Policies and Practices Study illustrate the limitations of current practices. The median number of hours of required instruction that teachers provided on the topic of nutrition and dietary behavior during 2006 was 3.4 for elementary school students, 4.2 for middle school students, and 5.9 for high school students (Kann et al., 2007). Further, curriculum continuity often is absent from nutrition education—lessons taught in one grade are not coordinated/reinforced in subsequent school years as is the case for other subjects. A greater investment of educational time, as well as a K-12 curriculum based on the latest science on preventing disease and promoting nutritional health, would maximize opportunities for imparting the information needed to influence students’ knowledge of nutrition and dietary behaviors.
The implementation of academic proficiency standards, including those of No Child Left Behind Act (Public Law 107-110, 107th Cong., 1st sess. [January 8, 2002], 115, 1425), has resulted in a narrowing of curriculum to fit specific standardized testing. Research suggests that teachers are limiting their curricula to content listed in curriculum frameworks and tested on examinations, while untested subjects such as social studies and science increasingly are excluded (Au, 2007; Grant, 2001; Kolbe, 2002; McNeil, 2000; Vogler and Virtue, 2007). Despite the widely recognized child obesity epidemic, nutrition education is among the subjects often omitted as a result of this narrowed focus. The committee recommends that proficiency standards for knowledge of food and nutrition parallel those for physical education and other core academic topics. These proficiency
standards and associated measurements should be based on evidence of school nutrition education programs with demonstrated effectiveness in changing nutrition knowledge and behavioral outcomes among students.
Evidence
Although traditional education has not been solidly proven to change behavior, the type of nutrition education recommended by the committee is not the exclusively didactic nutrition education of the past, but is interactive and couples experiential education techniques with education on food systems, marketing, food literacy, and other elements integral to the development of healthful eating habits. This type of education has shown promise in impacting students’ knowledge and behaviors.
Recently developed methods for teaching food and nutrition, in some cases using techniques based on experiential education (including food preparation, fruit and vegetable gardening, food tasting, and other hands-on approaches) can produce changes in knowledge without evidence of behavior change (Abood et al., 2008; DeVault et al., 2009; Gower et al., 2010; Katz et al., 2011; McGaffey et al., 2010; Moore et al., 2009, Morgan et al., 2010; Somerset and Markwell, 2009; Tuuri et al., 2009). Other studies have reported changes in students’ dietary intake patterns as well (Contento et al., 2010; Day et al., 2008; Dunton et al., 2009; Fahlman et al., 2008; He et al., 2009; Heim et al., 2009; Kristjansdottir et al., 2010; Lo et al., 2008; Muth et al., 2008; Parmer et al., 2009; Wang et al., 2010) and in some cases, positive impacts on changes in their weight or BMI (Hatzis et al., 2010; Mihas et al., 2010; Plachta-Danielzik et al., 2011). Further, nutrition education when reinforced by the school food environment has been shown to lead to changes in behavior and/or weight status (Burgess-Champoux et al., 2008; Davis et al., 2009; Foster et al., 2008; Hollar et al., 2010a,b; Hoppu et al., 2010; Muckelbauer et al., 2009; Reinaerts et al., 2008; Taylor et al., 2008). These studies were conducted with students ranging from the kindergarten level through high school, with education doses varying by program. Those education interventions associated with demonstrated changes in student BMI were conducted with either elementary or middle school students and included variable numbers of classroom hours, from only a few during a 1-year period to up to 17 per year over a 6-year period.
In 2006, Knai and colleagues (2006) conducted a review of 15 nutrition education interventions (11 in primary schools and 4 in secondary schools) designed to increase fruit and vegetable intake in children and adolescents aged 5-18. To qualify for this review, a study had to measure fruit and vegetable intake at a follow-up of at least 3 months. Using a variety of methods to measure fruit and
vegetable intake, 10 of the 15 interventions included in the review reported statistically significant positive change in consumption among intervention students compared with control students (Knai et al., 2006). Even using evidence drawn from an earlier period (1982-2004), the authors of the Academy of Nutrition and Dietetics position paper on individual-, family-, school-, and community-based interventions for pediatric overweight concluded: “There is fair evidence to support using nutrition education to change the type of food eaten, food preferences, or eating patterns as part of a school-based primary prevention program to effect changes in weight status/adiposity in elementary school and particularly in secondary school students” (Ritchie et al., 2006, p. 934).
The federal nutrition education programs that are administered to students in some selected grade levels and schools provide corroborating evidence for the efficacy of food and nutrition education in changing knowledge and behaviors. The Food Stamp Nutrition Education Program conducted a review of nationwide food and nutrition education programs in 2006. Fifty percent of implementing agencies (n = 22) believed that their outcome evaluations found positive behavior change among participants (Bell et al., 2006). Similarly, the National Institute of Food and Agriculture’s 2010 annual report on the Expanded Food and Nutrition Education Program (EFNEP) shows that the majority of youth receiving nutrition education improved knowledge and skills in nutrition (USDA, 2010). And a USDA evaluation of a Team Nutrition pilot study for fourth graders in seven school districts around the country showed a significant positive impact on students’ knowledge of the Food Guide Pyramid and healthy food choices (USDA, 1996). Multivariate analysis revealed that students exposed to more intervention components demonstrated the most significant changes in dietary behavior.
Implementation
The evidence is clear that nutrition education can positively influence children’s food and nutrition knowledge and behaviors, but research indicates that more instructional time is needed. The total number of classroom hours for programs studied and found to be effective varied widely, but nearly always was more than the current average of 4-6 hours per year, which translates to just 1-2 minutes per day. This amount of instruction stands in contrast to physical activity, for which daily instructional time, opportunities, and positive messages are more likely to exist during the school day. Students are exposed to unhealthy foods virtually everywhere they go, and they must have the knowledge necessary to make informed choices. In the face of the extensive food marketing to which children and
adolescents are exposed and must be able to interpret, a foundation of food and nutrition knowledge is important. It is difficult to imagine how children and adolescents can be expected to make healthy food choices in or out of school with so little instructional time spent on education about healthy foods and eating habits.
The amount of time schools should devote to nutrition education is not well defined. If quality nutrition education were a core subject area, it would receive 30 to 60 minutes per day, or 87 to 171 hours per year, of instructional time, similar to other academic subjects. It has been suggested that 50 hours/school year of instruction in nutrition is required to effect positive changes in eating behavior, but this number is not well substantiated and is based on best-practice estimates (Connell et al., 1985; Contento et al., 1995). The committee’s recommendation is 20 to 50 hours per year. Fifty hours per year is approximately 15 minutes per day, which is considerably less time than is devoted to other subjects taught in schools, as well as physical education classes. It should be noted that, although nutrition education could be viewed as taking time away from core educational requirements, no evaluations of nutrition education have demonstrated a negative effect on academic performance. Furthermore, one nutrition education intervention showed a positive effect on academic test scores (Shilts et al., 2009).
Multicomponent school-based programs utilizing a variety of methods, such as nutrition education, changes in school food offerings, social marketing, school gardens, and parent involvement, have been shown to be effective in reducing the prevalence of obesity in at least some participants. Doak and colleagues (2006) reviewed the literature and assessed 25 school-based obesity prevention programs. They found that 68 percent of the programs (17 of the 25) were successful in reducing the BMI or skin-fold measurements of program participants. Gortmaker and colleagues (1999) evaluated a school-based health behavior intervention known as Planet Health, in which sessions were included within existing school curricula, among students in grades 6-8. The intervention reduced obesity (based on BMI and triceps skin fold) in girls in intervention schools compared with controls, but no differences were found among boys. One example of a multicomponent school health program that is accompanied by a large body of work is the CATCH program, which achieved positive results with respect to nutrition knowledge, intention, and food preferences and intake with approximately 12 to 20 hours of nutrition education per year (Edmundson et al., 1994; Luepker et al., 1996; Perry et al., 1990, 1997). The CATCH program provides compelling evidence of the multiple benefits of school-based food, nutrition, and physical education programs (Box 9-2).
BOX 9-2
The CATCH School-Based Food, Nutrition, and Physical
Education Program
Background
The Coordinated Approach To Child Health (CATCH) program* was designed in the 1980s to improve physical activity and diet and to prevent the onset of tobacco use (Perry et al., 1990). In recent years, the CATCH program has aligned with the Centers for Disease Control and Prevention’s coordinated school health model, in which eight components work interactively to educate young people about and provide support for a healthful lifestyle. The five main components of CATCH are (1) K-8 classroom curricula focusing on food, nutrition, and physical activity; (2) physical education activities; (3) child nutrition services; (4) family involvement; and (5) community involvement. An evidence base supports the program’s efficacy in improving diet and increasing physical activity and preventing the onset of obesity in children.
Results and Evidence
• Results of long-term follow-up indicate that changes in diet and physical activity were maintained 3 years postintervention, until the children were in eighth grade (Nader et al., 1999).
• CATCH has been proven effective in promoting health among inner-city, border, rural, privileged, and underprivileged children. A school randomized replication study of CATCH in El Paso found significant effects in reducing the rate of increase of overweight and risk of overweight among a cohort of children in grades 3-5. By fifth grade, the rate of increase was 2 percent for girls and 1 per-
cent for boys in intervention schools, compared with 13 and 9 percent, respectively, in control schools (Coleman et al., 2005).
• PASS & CATCH, a version of CATCH making extensive use of classroom physical activities, has been shown to improve disadvantaged children’s Stanford math and reading scores (Murray et al., under review).
• CATCH augments existing school health programming by inviting local community youth organizations to participate in the process of creating a healthier school environment. The effects of community support cannot be underestimated.
• An El Paso demonstration study of CATCH plus community support found a 7 percent reduction in child obesity prevalence (Hoelscher et al., 2010a).
• A recent Travis County demonstration study of CATCH showed an 8 percent reduction in overweight and obesity among fourth graders (Hoelscher et al., 2010b).
• According to a recent cost-effectiveness study of CATCH, the program’s cost-effectiveness ratio was approximately $900 (representing the intervention cost per quality-adjusted life-year saved), and the net benefit was $68,125 (based on a comparison of the present value of averted future costs due to obesity with the cost of the CATCH intervention) (Brown et al., 2007).
![]()
*Formerly known as the Child and Adolescent Trial for Cardiovascular Health.
Indicators for Assessing Progress in Obesity Prevention for Strategy 5-3
Process Indicators
• Increase in the adoption of age-appropriate, sequential food and nutrition curriculum standards and performance measures for grades K-12 in all schools.
Source for measuring indicator: SHPPS
• Increase in students’ knowledge of nutrition, consistent with the Dietary Guidelines for Americans.*
Source needed for measurement of indicator.
• Increase in the proportion of states with policies requiring a sequential food and nutrition curriculum for grades K-12.
Sources for measuring indicator: CLASS (NCI) and SHPPS
• Increase in the proportion of states with nutrition education training requirements for teachers.
Source needed for measurement of indicator.
Foundational Indicators
• Increase in the priority of advocacy efforts (among professional associations related to schools and nutrition) regarding the implementation of 20-50 hours of classroom nutrition education.
Source needed for measurement of indicator.
NOTE: CLASS = Classification of Laws Associated with School Students; NCI = National Cancer Institute; SHPPS = School Health Policies and Practices Study.
![]()
*See Box B-1 in Appendix B.
INTEGRATION OF STRATEGIES FOR ACCELERATING PROGRESS IN OBESITY PREVENTION
Evidence outlined in this chapter points to opportunities to accelerate progress in preventing obesity among children and adolescents in three school-related areas: physical education, school foods, and food and nutrition education. During the past decade, states and municipal governments have implemented policies regarding competitive foods; many schools have made improvements in school meals and others in physical education programs. Some schools have added nutrition education programs in particular classrooms or grade levels. These programs and policies differ by class, grade, school, district and state.
Physical activity, school foods, and nutrition education generally have been treated separately within schools, and interdisciplinary obesity prevention efforts thus have rarely been realized. The breaking down of these silos began in many schools in fall 2006 when local education agencies sponsoring USDA-funded school meal programs were required to establish local wellness policies. A three-state USDA-funded Team Nutrition Local Wellness Demonstration Project reported that wellness committees brought together principals, food service directors, physical education teachers, school nurses, superintendents, parents, curriculum directors, school board members, and students (Wood et al., 2010). While none of the districts studied reported changes in all areas—including improvements in physical activity environments, implementation of physical education programs that meet state standards, increased opportunities for and participation by students and staff in physical activity, school food environments, and implementation of nutrition education in classes—most schools had made some improvements in some of these areas. Classroom nutrition instruction implemented concurrently with changes in meal program offerings was associated with improved healthy food choices (Wood et al., 2010). Thus school wellness policies can be a vehicle for change, suggesting comprehensive approaches to school wellness and providing consistent messages to school stakeholders. The report of the Wellness Demonstration Project goes on to say that local wellness policies have created a culture of change in schools that, coupled with the beginnings of an integrated approach to physical and food and nutrition and education, promises to provide momentum for the changes needed to accelerate progress toward obesity prevention in school environments (Wood et al., 2010).
The literature provides evidence of the benefits of multicomponent nutrition interventions, many specifically combining changes in the school food environment with food and nutrition education (Knai et al., 2006; Livingstone et al.,
2006; Peters et al., 2009). If well coordinated, a school lunch program can serve as an important adjunct to nutrition education. When multicomponent nutrition programs have been coupled with physical activity and physical education programs, even more dramatic changes have occurred, in some cases, changes in student adiposity (Brown and Summerbell, 2009; Coleman et al., 2005; Foster et al., 2008; Hollar et al., 2010a,b; Katz et al., 2008; Ritchie et al., 2006). In addition to achieving improvements in school meals and competitive foods, these programs often have included physical education and physical activity during the school day, strong nutrition education and promotion components, and family involvement, and some have included related community events.
Along with changes in the school environment and implementation of sequential food and nutrition education, it is important for teachers and other school staff to model healthy behaviors, and there is progress to be made in this area (Eaton et al., 2007; Hartline-Grafton et al., 2009). The Alliance for a Healthier Generation encourages school employee wellness programs in the belief that the conditions that affect the health of these employees influence the health and learning of students, and that protecting the health of school employees is essential to protecting student health and fostering students’ academic success (Alliance for a Healthier Generation, 2011). Employee wellness programs are discussed further in Chapter 8 (Strategy 4-3) and have demonstrated positive outcomes in other settings. For example, a staff wellness intervention conducted in selected Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) sites showed that intervention group staff were more likely than control group staff to report that the workplace environment supported their efforts to choose healthy foods and be physically active, and improved their counseling for WIC clients related to physical activity and weight (Crawford et al., 2004). In a staff wellness program in child care centers, employees in intervention sites reported providing more fresh fruits and vegetables to children and experiencing more positive changes in their comfort level with respect to discussing physical activity and nutrition with parents relative to employees in control sites (Gosliner et al., 2010). The committee believes that ensuring that school staff support the strategies set forth in this chapter—with words and actions—in the presence of students is likely critical for success.
The committee expects that changes in the school environment, implemented concurrently with this report’s recommended changes in the rest of the system in which children live and play, will act synergistically to accelerate progress in obesity prevention (as illustrated by Figure 9-1, presented at the beginning of this chapter). Even if the effect of school-based interventions were to be relatively
small, schools are an ideal setting in which to expose children and adolescents to knowledge and behaviors related to physical activity and nutrition. As shown in New York City (Berger et al., 2011) and by past interventions in CATCH schools (Box 9-2), changes in schools accompanied by changes in the community are associated with positive health outcomes. Furthermore, school-based interventions could have positive effects on children’s behaviors outside of school, such as time spent viewing television (Robinson and Borzekowski, 2006) and consumption of healthy foods (IOM, 2010; Wang et al., 2010).
Objections to physical education and nutrition education programs coupled with changes in school foods will undoubtedly arise. The most serious objection is less likely to be lack of funding as it is to be concern about reduced time for academic subjects, with the potential result of lower test scores. With regard to reducing time spent on academic subjects, the committee acknowledges that integrating nutrition education with existing school curricula has shown limited success in reducing obesity (Austin et al., 2005; Gortmaker et al., 1999); however, this approach would need further testing at various grade levels before its use could be recommended in place of sequential nutrition education, in which knowledge and skills are reinforced and expanded each year as a stand-alone subject. The committee could find no evidence that such sequential programs lower academic test scores. To the contrary, some evidence indicates that school-based physical education (CDC, 2010b; Singh et al., 2012) and nutrition curriculum (Shilts et al., 2009) can positively influence academic achievement. Furthermore, well-nourished children are more able to learn and less likely to miss school for health reasons (Florence et al., 2008; Taras, 2005a). Studies have shown that students participating in school breakfast programs score higher on standardized tests and have better school attendance than similar children not participating in the program (Hoyland et al., 2009; Kleinman et al., 2002; Meyers et al., 1989; Powell et al., 1983, 1998). Assessments of recent interventions to improve school physical activity and nutrition environments have shown that these efforts can lead to an improvement in children’s academic performance and to improved classroom behavior and attentiveness (Hollar, 2010a,b; Murphy et al., 1998; Nansel et al., 2010). As far back as 1904, Robert Hunter wrote about the need for students to have adequate physical activity and nutrition: “It is utter folly, from the point of view of learning, to have a compulsory school law which compels children, in that weak physical and mental state … to sit at their desks, day in and day out for several years, learning little or nothing … because hungry stomachs and languid bodies and thin blood are not able to feed the brain” (Hunter, 1965).
Abood, D. A., D. R. Black, and D. C. Coster. 2008. Evaluation of a school-based teen obesity prevention minimal intervention. Journal of Nutrition Education and Behavior 40(3):168-174.
Alliance for a Healthier Generation. 2011. School employee wellness. http://www.healthiergeneration.org/schools.aspx?id=3393 (accessed December 28, 2011).
Anthamatten, P., L. Brink, S. Lampe, E. Greenwood, B. Kingston, and C. Nigg. 2011. An assessment of schoolyard renovation strategies to encourage children’s physical activity. International Journal of Behavior Nutrition and Physical Activity 8:27.
Au, W. 2007. High-stakes testing and curricular control: A qualitative metasynthesis. Educational Researcher 36(5):258.
Austin, S. B., A. E. Field, J. Wiecha, K. E. Peterson, and S. L. Gortmaker. 2005. The impact of a school-based obesity prevention trial on disordered weight-control behaviors in early adolescent girls. Archives of Pediatrics and Adolescent Medicine 159(3):225-230.
Bell, L., F. Tao, J. Anthony, C. Logan, R. Ledsky, M. Ferreira, and A. Brown. 2006. Food stamp nutrition education systems review: Final report. Alexandria, VA: USDA/FNS, Office of Analysis, Nutrition, and Evaluation.
Berger, M., K. Konty, S. Day, L. D. Silver, C. Nonas, B. D. Kerker, C. Greene, T. Farley, and L. Harr. 2011. Obesity in K-8 students—New York City, 2006-2007 to 2010-2011 school years. Morbidity and Mortality Weekly Report 60(49):1673-1678.
Briefel, R. R., M. K. Crepinsek, C. Cabili, A. Wilson, and P. M. Gleason. 2009. School food environments and practices affect dietary behaviors of U.S. public school children. Journal of the American Dietetic Association 109(2):S91-S107.
Brink, L. A., C. R. Nigg, S. M. Lampe, B. A. Kingston, A. L. Mootz, and W. van Vliet. 2010. Influence of schoolyard renovations on children’s physical activity: The Learning Landscapes Program. American Journal of Public Health 100(9):1672-1678.
Brown, H. S., A. Perez, Y.-P. Li, D. Hoelscher, S. Kelder, and R. Rivera. 2007. The cost-effectiveness of a school-based overweight program. International Journal of Behavioral Nutrition and Physical Activity 4(1):47.
Brown, T., and C. Summerbell. 2009. Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: An update to the obesity guidance produced by the National Institute for Health and Clinical Excellence. Obesity Reviews 10(1): 110-141.
Burgess-Champoux, T. L., H. W. Chan, R. Rosen, L. Marquart, and M. Reicks. 2008. Healthy whole-grain choices for children and parents: A multi-component school-based pilot intervention. Public Health Nutrition 11(8):849-859.
California Project LEAN (Leaders Encouraging Activity and Nutrition). 2009. Maximizing opportunities for physical activity during the school day. Sacramento, CA: California Project LEAN.
CDC (Centers for Disease Control and Prevention). 2010a. Effects of switching from whole to low-fat/fat-free milk in public schools—New York City, 2004-2009. Morbidity and Mortality Weekly Report 59(3):70-73.
CDC. 2010b. The association between school based physical activity, including physical education, and academic performance. Atlanta, GA: HHS, CDC.
Chriqui, J. F., L. Schneider, F. J. Chaloupka, C. Gourdet, A. Bruursema, K. Ide, and O. Pugach. 2010. School district wellness policies: Evaluating progress and potential for improving children’s health three years after the federal mandate: School years 2006-07, 2007-08 and 2008-09, Volume 2. Chicago, IL: Bridging the Gap Program, Health Policy Center, Institute for Health Research and Policy, University of Illinois.
Colabianchi, N., A. E. Kinsella, C. J. Coulton, and S. M. Moore. 2009. Utilization and physical activity levels at renovated and unrenovated school playgrounds. Preventive Medicine 48(2):140-143.
Coleman, K. J., C. L. Tiller, J. Sanchez, E. M. Heath, O. Sy, G. Milliken, and D. A. Dzewaltowski. 2005. Prevention of the epidemic increase in child risk of overweight in low-income schools: The El Paso coordinated approach to child health. Archives of Pediatrics and Adolescent Medicine 159(3):217-224.
Connell, D. B., R. R. Turner, and E. F. Mason. 1985. Summary of findings of the School Health Education Evaluation: Health promotion effectiveness, implementation, and costs. Journal of School Health 55(8):316-321.
Contento, I., G. I. Balch, Y. L. Bronner, D. M. Paige, S. M. Gross, and L. Bisignani. 1995. Nutrition education for school-aged children. Journal of Nutrition Education 27(6):298-311.
Contento, I. R., P. A. Koch, H. Lee, and A. Calabrese-Barton. 2010. Adolescents demonstrate improvement in obesity risk behaviors after completion of choice, control & change, a curriculum addressing personal agency and autonomous motivation. Journal of the American Dietetic Association 110(12):1830-1839.
Crawford, P. B., W. Gosliner, P. Strode, S. E. Samuels, C. Burnett, L. Craypo, and A. K. Yancey. 2004. Walking the talk: Fit WIC wellness programs improve self-efficacy in pediatric obesity prevention counseling. American Journal of Public Health 94(9):1480-1485.
Cullen, K. W., and K. B. Watson. 2009. The impact of the Texas public school nutrition policy on student food selection and sales in Texas. American Journal of Public Health 99(4):706-712.
Cullen, K. W., K. Watson, and I. Zakeri. 2008. Improvements in middle school student dietary intake after implementation of the Texas Public School Nutrition Policy. American Journal of Public Health 98(1):111-117.
Davis, E. M., K. W. Cullen, K. B. Watson, M. Konarik, and J. Radcliffe. 2009. A fresh fruit and vegetable program improves high school students’ consumption of fresh produce. Journal of the American Dietetic Association 109(7):1227-1231.
Day, M. E., K. S. Strange, H. A. McKay, and P. J. Naylor. 2008. Action schools! BC— Healthy Eating: Effects of a whole-school model to modifying eating behaviours of elementary school children. Canadian Journal of Public Health. Revue Canadienne de Sante Publique 99(4):328-331.
DeVault, N., T. Kennedy, J. Hermann, M. Mwavita, P. Rask, and A. Jaworsky. 2009. It’s all about kids: Preventing overweight in elementary school children in Tulsa, OK. Journal of the American Dietetic Association 109(4):680-687.
Doak, C. M., T. L. S. Visscher, C. M. Renders, and J. C. Seidell. 2006. The prevention of overweight and obesity in children and adolescents: A review of interventions and programmes. Obesity Reviews 7(1):111-136.
Dobbins, M., K. DeCorby, P. Robeson, H. Husson, and D. Tirilis. 2009. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6-18. Cochrane Database of Systematic Reviews (1).
Dunton, G. F., R. Lagloire, and T. Robertson. 2009. Using the RE-AIM framework to evaluate the statewide dissemination of a school-based physical activity and nutrition curriculum: “Exercise Your Options.” American Journal of Health Promotion 23(4):229-232.
Eaton, D. K., E. Marx, and S. E. Bowie. 2007. Faculty and staff health promotion: Results from the school health policies and programs study 2006. Journal of School Health 77(8):557-566.
Edmundson, E. W., S. C. Luton, S. A. McGraw, S. H. Kelder, A. K. Layman, M. H. Smyth, K. J. Bachman, S. A. Pedersen, and E. J. Stone. 1994. CATCH: Classroom process evaluation in a multicenter trial. Health Education Quarterly (Suppl. 2):S27-S50.
Fahlman, M. M., J. A. Dake, N. McCaughtry, and J. Martin. 2008. A pilot study to examine the effects of a nutrition intervention on nutrition knowledge, behaviors, and efficacy expectations in middle school children. Journal of School Health 78(4):216-222.
Fisher, J. O., B. J. Rolls, and L. L. Birch. 2003. Children’s bite size and intake of an entrée are greater with large portions than with age-appropriate or self-selected portions. American Journal of Clinical Nutrition 77(5):1164-1170.
Florence, M. D., M. Asbridge, and P. J. Veugelers. 2008. Diet quality and academic performance. Journal of School Health 78(4):209-215.
Foster, G. D., S. Sherman, K. E. Borradaile, K. M. Grundy, S. S. Vander Veur, J. Nachmani, A. Karpyn, S. Kumanyika, and J. Shults. 2008. A policy-based school intervention to prevent overweight and obesity. Pediatrics 121(4):e794-e802.
Gordon-Larsen, P., K. M. Harris, D. S. Ward, and B. M. Popkin. 2003. Acculturation and overweight-related behaviors among Hispanic immigrants to the US: The National Longitudinal Study of Adolescent Health. Social Science and Medicine 57(11):2023-2034.
Gortmaker, S. L., K. Peterson, J. Wiecha, A. M. Sobol, S. Dixit, M. K. Fox, and N. Laird. 1999. Reducing obesity via a school-based interdisciplinary intervention among youth: Planet health. Archives of Pediatrics and Adolescent Medicine 153(4):409-418.
Gosliner, W. A., P. James, A. K. Yancey, L. Ritchie, N. Studer, and P. B. Crawford. 2010. Impact of a worksite wellness program on the nutrition and physical activity environment of child care centers. American Journal of Health Promotion 24(3):186-189.
Gosliner, W., K. A. Madsen, G. Woodward-Lopez, and P. B. Crawford. 2011. Would students prefer to eat healthier foods at school? Journal of School Health 81(3):146-151.
Gower, J. R., L. J. Moyer-Mileur, R. D. Wilkinson, H. Slater, and K. C. Jordan. 2010. Validity and reliability of a nutrition knowledge survey for assessment in elementary school children. Journal of the American Dietetic Association 110(3):452-456.
Grant, S. G. 2001. An uncertain lever: Exploring the influence of state-level testing in New York state on teaching social studies. Teachers College Record 103(3):398-426.
Hartline-Grafton, H. L., D. Rose, C. C. Johnson, J. C. Rice, and L. S. Webber. 2009. Are school employees role models of healthful eating? Dietary intake results from the ACTION worksite wellness trial. Journal of the American Dietetic Association 109(9):1548-1556.
Hatzis, C. M., C. Papandreou, and A. G. Kafatos. 2010. School health education programs in Crete: Evaluation of behavioural and health indices a decade after initiation. Preventive Medicine 51(3-4):262-267.
He, M., C. Beynon, M. Sangster Bouck, R. St Onge, S. Stewart, L. Khoshaba, B. A. Horbul, and B. Chircoski. 2009. Impact evaluation of the northern fruit and vegetable pilot program: A cluster-randomised controlled trial. Public Health Nutrition 12(11):2199-2208.
Heim, S., J. Stang, and M. Ireland. 2009. A garden pilot project enhances fruit and vegetable consumption among children. Journal of the American Dietetic Association 109(7):1220-1226.
HHS/USDA (U.S. Department of Health and Human Services/U.S. Department of Agriculture). 2005. Dietary guidelines for Americans. Washington, DC: U.S. Government Printing Office.
HHS/USDA. 2010. Dietary guidelines for Americans. Washington, DC: U.S. Government Printing Office.
Hoelscher, D. M., S. H. Kelder, A. Perez, R. S. Day, J. S. Benoit, R. F. Frankowski, J. L. Walker, and E. S. Lee. 2010a. Changes in the regional prevalence of child obesity in 4th, 8th, and 11th grade students in Texas from 2000-2002 to 2004-2005. Obesity 18(7):1360-1368.
Hoelscher, D., A. Springer, N. Ranjit, S. Perry, A. Evans, M. Stigler, and S. Kelder. 2010b. Reductions in child obesity among disadvantaged school children with community involvement: The Travis County CATCH trial. Obesity (Silver Spring) 18(Suppl. 1):S36-S44.
Hollar, D., M. Lombardo, G. Lopez-Mitnik, T. L. Hollar, M. Almon, A. S. Agatston, and S. E. Messiah. 2010a. Effective multi-level, multi-sector, school-based obesity prevention programming improves weight, blood pressure, and academic performance, especially among low-income, minority children. Journal of Health Care for the Poor and Underserved 21(Suppl. 2):93-108.
Hollar, D., S. E. Messiah, G. Lopez-Mitnik, T. L. Hollar, M. Almon, and A. S. Agatston. 2010b. Effect of a two-year obesity prevention intervention on percentile changes in body mass index and academic performance in low-income elementary school children. American Journal of Public Health 100(4):646-653.
Hoppu, U., J. Lehtisalo, J. Kujala, T. Keso, S. Garam, H. Tapanainen, A. Uutela, T. Laatikainen, U. Rauramo, and P. Pietinen. 2010. The diet of adolescents can be improved by school intervention. Public Health Nutrition 13(6A):973-979.
Hoyland, A., L. Dye, and C. L. Lawton. 2009. A systematic review of the effect of breakfast on the cognitive performance of children and adolescents. Nutrition Research Reviews 22(02):220-243.
Hunter, R. 1965 (originally published in 1904). Poverty, Harper Torchbooks edition. New York: Harper & Row.
IOM (Institute of Medicine). 2005. Preventing childhood obesity: Health in the balance, edited by J. P. Koplan, C. T. Liverman, and V. A. Kraak. Washington, DC: The National Academies Press.
IOM. 2007. Nutrition standards for foods in schools: Leading the way toward healthier youth. Washington, DC: The National Academies Press.
IOM. 2008. Nutrition standards and meal requirements for national school lunch and breakfast programs: Phase I. Proposed approach for recommending revisions. Washington, DC: The National Academies Press.
IOM. 2010. School meals: Building blocks for healthy children. Washington, DC: The National Academies Press.
Jago, R., and T. Baranowski. 2004. Non-curricular approaches for increasing physical activity in youth: A review. Preventive Medicine 39(1):157-163.
Just, D. R., and B. Wansink. 2009. Smarter lunchrooms: Using behavioral economics to improve meal selection. Choices 24(3).
Kahn, E. B., L. T. Ramsey, R. C. Brownson, G. W. Heath, E. H. Howze, K. E. Powell, E. J. Stone, M. W. Rajab, and P. Corso. 2002. The effectiveness of interventions to increase physical activity. A systematic review. American Journal of Preventive Medicine 22(Suppl. 4):73-107.
Kann, L., S. K. Telljohann, and S. F. Wooley. 2007. Health education: Results from the School Health Policies and Programs Study 2006. Journal of School Health 77(8):408-434.
Katz, D. L., M. O’Connell, V. Y. Njike, M. C. Yeh, and H. Nawaz. 2008. Strategies for the prevention and control of obesity in the school setting: Systematic review and meta-analysis. International Journal of Obesity (London) 32(12):1780-1789.
Katz, D. L., C. S. Katz, J. A. Treu, J. Reynolds, V. Njike, J. Walker, E. Smith, and J. Michael. 2011. Teaching healthful food choices to elementary school students and their parents: The Nutrition Detectives program. Journal of School Health 81(1):21-28.
Kelder, S. 2010. Stuck in the middle: The false choice between health and education in Texas middle schools. Austin, TX: RGK Foundation.
Kleinman, R. E., S. Hall, H. Green, D. Korzec-Ramirez, K. Patton, M. E. Pagano, and J. M. Murphy. 2002. Diet, breakfast, and academic performance in children. Annals of Nutrition and Metabolism 46(Supp1. 1):24-30.
Knai, C., J. Pomerleau, K. Lock, and M. McKee. 2006. Getting children to eat more fruit and vegetables: A systematic review. Preventive Medicine 42(2):85-95.
Kolbe, L. J. 2002. Health and the goals of modern school health programs. The State Education Standard August:1-11.
Kristjansdottir, A. G., E. Johannsson, and I. Thorsdottir. 2010. Effects of a school-based intervention on adherence of 7-9-year-olds to food-based dietary guidelines and intake of nutrients. Public Health Nutrition 13(8):1151-1161.
Larson, N. I., M. T. Story, and M. C. Nelson. 2009. Neighborhood environments: Disparities in access to healthy foods in the U.S. American Journal of Preventive Medicine 36(1):74-81.
Lee, S. M., C. R. Burgeson, J. E. Fulton, and C. G. Spain. 2007. Physical education and physical activity: Results from the School Health Policies and Programs Study 2006. Journal of School Health 77(8):435-463.
Livingstone, M. B., T. A. McCaffrey, and K. L. Rennie. 2006. Childhood obesity prevention studies: lessons learned and to be learned. Public Health Nutrition 9(8A):1121-1129.
Lo, E., R. Coles, M. L. Humbert, J. Polowski, C. J. Henry, and S. J. Whiting. 2008. Beverage intake improvement by high school students in Saskatchewan, Canada. Nutrition Research 28(3):144-150.
Long, M. W., K. E. Henderson, and M. B. Schwartz. 2010. Evaluating the impact of a Connecticut program to reduce availability of unhealthy competitive food in schools. Journal of School Health 80(10):478-486.
Luepker, R. V., C. L. Perry, S. M. McKinlay, P. R. Nader, G. S. Parcel, E. J. Stone, L. S. Webber, J. P. Elder, H. A. Feldman, C. C. Johnson, S. H. Kelder, M. Wu, and CATCH Collaborative Group. 1996. Outcomes of a field trial to improve children’s dietary patterns and physical activity. The Child and Adolescent Trial for Cardiovascular Health. CATCH Collaborative Group. Journal of the American Medical Association 275(10):768-776.
McGaffey, A., K. Hughes, S. K. Fidler, F. J. D’Amico, and M. N. Stalter. 2010. Can Elvis Pretzley and the Fitwits improve knowledge of obesity, nutrition, exercise, and portions in fifth graders? International Journal of Obesity (London) 34(7):1134-1142.
McNeil, L. M. 2000. Contradictions of school reform: Educational costs of standardized testing. New York: Routledge.
Mendoza, J. A., K. Watson, and K. W. Cullen. 2010. Change in dietary energy density after implementation of the Texas Public School Nutrition Policy. Journal of the American Dietetic Association 110(3):434-440.
Meyers, A. F., A. E. Sampson, M. Weitzman, B. L. Rogers, and H. Kayne. 1989. School breakfast program and school performance. American Journal of Diseases of Children 143(10):1234-1239.
Mihas, C., A. Mariolis, Y. Manios, A. Naska, A. Arapaki, T. Mariolis-Sapsakos, and Y. Tountas. 2010. Evaluation of a nutrition intervention in adolescents of an urban area in Greece: Short- and long-term effects of the VYRONAS study. Public Health Nutrition 13(5):712-719.
Moore, J. B., L. R. Pawloski, P. Goldberg, M. O. Kyeung, A. Stoehr, and H. Baghi. 2009. Childhood obesity study: A pilot study of the effect of the nutrition education program Color My Pyramid. Journal of School Nursing 25(3):230-239.
Morgan, P. J., J. M. Warren, D. R. Lubans, K. L. Saunders, G. I. Quick, and C. E. Collins. 2010. The impact of nutrition education with and without a school garden on knowledge, vegetable intake and preferences and quality of school life among primary-school students. Public Health Nutrition 13(11):1931-1940.
Muckelbauer, R., L. Libuda, K. Clausen, A. M. Toschke, T. Reinehr, and M. Kersting. 2009. Promotion and provision of drinking water in schools for overweight prevention: Randomized, controlled cluster trial. Pediatrics 123(4):e661-e667.
Murphy, J. M., M. E. Pagano, J. Nachmani, P. Sperling, S. Kane, and R. E. Kleinman. 1998. The relationship of school breakfast to psychosocial and academic functioning: Cross-sectional and longitudinal observations in an inner-city school sample. Archives of Pediatrics and Adolescent Medicine 152(9):899-907.
Murray, N. G., J. C. Garza, P. M. Diamond, M. Stigler, D. Hoelscher, S. Kelder, and J. Ward. under review. PASS & CATCH improves academic achievement. http://www.nemours.org/content/dam/nemours/www/filebox/service/preventive/nhps/pep/pass%2Bcatch.pdf (accessed December 12, 2011).
Muth, N. D., A. Chatterjee, D. Williams, A. Cross, and K. Flower. 2008. Making an IMPACT: Effect of a school-based pilot intervention. North Carolina Medical Journal 69(6):432-440.
Nader, P. R., E. J. Stone, L. A. Lytle, C. L. Perry, S. K. Osganian, S. Kelder, L. S. Webber, J. P. Elder, D. Montgomery, H. A. Feldman, M. Wu, C. Johnson, G. S. Parcel, and R. V. Luepker. 1999. Three-year maintenance of improved diet and physical activity: The CATCH cohort. Archives of Pediatrics and Adolescent Medicine 153(7):695-704.
Nansel, T. R., T. T. K. Huang, A. J. Rovner, and Y. Sanders-Butler. 2010. Association of school performance indicators with implementation of the healthy kids, smart kids programme: Case study. Public Health Nutrition 13(1):116-122.
NASPE (National Association for Sport and Physical Education). Undated. Integrating physical activity into the complete school day. Reston, VA: American Alliance for Health, Physical Education, Recreation and Dance.
NASPE and AHA (American Heart Association). 2010. Shape of the nation report: Status of physical education in the USA. Reston, VA: NASPE.
NRC (National Research Council, Committee on Diet and Health). 1989. Diet and health: Implications for reducing chronic disease risk. Washington, DC: National Academy Press.
Parmer, S. M., J. Salisbury-Glennon, D. Shannon, and B. Struempler. 2009. School gardens: An experiential learning approach for a nutrition education program to increase fruit and vegetable knowledge, preference, and consumption among second-grade students. Journal of Nutrition Education and Behavior 41(3):212-217.
Perry, C. L., E. J. Stone, G. S. Parcel, R. C. Ellison, P. R. Nader, L. S. Webber, and R. V. Luepker. 1990. School-based cardiovascular health promotion: The Child and Adolescent Trial for Cardiovascular Health (CATCH). Journal of School Health 60(8):406-413.
Perry, C. L., D. E. Sellers, C. Johnson, S. Pedersen, K. J. Bachman, G. S. Parcel, E. J. Stone, R. V. Luepker, M. Wu, P. R. Nader, and K. Cook. 1997. The Child and Adolescent Trial for Cardiovascular Health (CATCH): Intervention, implementation, and feasibility for elementary schools in the United States. Health Education and Behavior 24(6):716-735.
Peters, L. W., G. Kok, G. T. Ten Dam, G. J. Buijs, and T. G. Paulussen. 2009. Effective elements of school health promotion across behavioral domains: A systematic review of reviews. BMC Public Health 9:182.
Phillips, M. M., J. M. Raczynski, D. S. West, L. Pulley, Z. Bursac, C. H. Gauss, and J. F. Walker. 2010. Changes in school environments with implementation of Arkansas Act 1220 of 2003. Obesity (Silver Spring) 18(Suppl. 1):S54-S61.
Pilant, V. B. 2006. Position of the American Dietetic Association: Local support for nutrition integrity in schools. Journal of the American Dietetic Association 106(1):122-133.
Plachta-Danielzik, S., B. Landsberg, D. Lange, J. Seiberl, and M. J. Muller. 2011. Eight-year follow-up of school-based intervention on childhood overweight—the Kiel Obesity Prevention Study. Obesity Facts 4(1):35-43.
Powell, C., S. Grantham-McGregor, and M. Elston. 1983. An evaluation of giving the Jamaican government school meal to a class of children. Human Nutrition. Clinical Nutrition 37(5):381-388.
Powell, C. A., S. P. Walker, S. M. Chang, and S. M. Grantham-McGregor. 1998. Nutrition and education: A randomized trial of the effects of breakfast in rural primary school children. American Journal of Clinical Nutrition 68(4):873-879.
Reinaerts, E., R. Crutzen, M. Candel, N. K. De Vries, and J. De Nooijer. 2008. Increasing fruit and vegetable intake among children: Comparing long-term effects of a free distribution and a multicomponent program. Health Education Research 23(6):987-996.
Ridgers, N. D., G. Stratton, S. J. Fairclough, and J. W. Twisk. 2007. Children’s physical activity levels during school recess: A quasi-experimental intervention study. International Journal of Behavior, Nutrition, and Physical Activity 4:19.
Ritchie, L. D., P. B. Crawford, D. M. Hoelscher, and M. S. Sothern. 2006. Position of the American Dietetic Association: Individual-, family-, school-, and community-based interventions for pediatric overweight. Journal of the American Dietetic Association 106(6):925-945.
Robinson, T. N., and D. L. G. Borzekowski. 2006. Effects of the SMART classroom curriculum to reduce child and family screen time. Journal of Communication 56(1):1-26.
Rolls, B. J., L. S. Roe, T. V. E. Kral, J. S. Meengs, and D. E. Wall. 2004. Increasing the portion size of a packaged snack increases energy intake in men and women. Appetite 42(1):63-69.
Samuels, S. E., S. Lawrence Bullock, G. Woodward-Lopez, S. E. Clark, J. Kao, L. Craypo, J. Barry, and P. B. Crawford. 2009. To what extent have high schools in California been able to implement state-mandated nutrition standards? Journal of Adolescent Health 45(Suppl. 3):S38-S44.
Sanchez-Vaznaugh, E. V., B. N. Sánchez, J. Baek, and P. B. Crawford. 2010. “Competitive” food and beverage policies: Are they influencing childhood overweight trends? Health Affairs 29(3):436-446.
Schwartz, M. B., S. A. Novak, and S. S. Fiore. 2009. The impact of removing snacks of low nutritional value from middle schools. Health Education and Behavior 36(6):999-1011.
Shilts, M. K., C. Lamp, M. Horowitz, and M. S. Townsend. 2009. Pilot study: EatFit impacts sixth graders’ academic performance on achievement of mathematics and English education standards. Journal of Nutrition Education and Behavior 41(2):127-131.
Sibley, B. A., and J. L. Etnier. 2003. The relationship between physical activity and cognition in children: A meta-analysis. Pediatric Exercise Science 15:243-256.
Singh, A., L. Uijtdewilligen, J. W. R. Twisk, W. van Mechelen, and M. J. M. Chinapaw. 2012. Physical activity and performance at school: A systematic review of the literature including a methodological quality assessment. Archives of Pediatrics and Adolescent Medicine 166(1):49-55.
Somerset, S., and K. Markwell. 2009. Impact of a school-based food garden on attitudes and identification skills regarding vegetables and fruit: A 12-month intervention trial. Public Health Nutrition 12(2):214-221.
Taras, H. 2005a. Nutrition and student performance at school. Journal of School Health 75(6):199-213.
Taras, H. 2005b. Physical activity and student performance at school. Journal of School Health 75(6):214-218.
Taylor, R. W., K. A. McAuley, W. Barbezat, V. L. Farmer, S. M. Williams, and J. I. Mann. 2008. Two-year follow-up of an obesity prevention initiative in children: The APPLE project. American Journal of Clinical Nutrition 88(5):1371-1377.
Treuhaft, S., and A. Karpyn. 2010. The grocery gap: Who has access to healthy food and why it matters. Oakland, CA and Philadelphia, PA: PolicyLink and The Food Trust.
Trudeau, F., and R. J. Shephard. 2008. Physical education, school physical activity, school sports and academic performance. International Journal of Behavioral Nutrition and Physical Activity 5.
Trudeau, F., and R. J. Shephard. 2010. Relationships of physical activity to brain health and the academic performance of school children. American Journal of Lifestyle Medicine 4:138-150.
Tuuri, G., M. Zanovec, L. Silverman, J. Geaghan, M. Solmon, D. Holston, A. Guarino, H. Roy, and E. Murphy. 2009. “Smart Bodies” school wellness program increased children’s knowledge of healthy nutrition practices and self-efficacy to consume fruit and vegetables. Appetite 52(2):445-451.
USDA (U.S. Department of Agriculture). 1996. The story of team nutrition: Executive summary of the pilot study. Alexandria, VA: USDA/FNS, Office of Evaluation, Nutrition, and Evaluation.
USDA. 2007. School Nutrition Dietary Assessment Study—III: Volume I: School food service, school food environment, and meals offered and served. Alexandria, VA:USDA.
USDA. 2010. FY 2010: NIFA-national data: The Expanded Food and Nutrition Education Program. Washington, DC: USDA.
USDA/FNS (Food and Nutrition Service). 2011. Nutrition standards in the National School Lunch and Breakfast Programs: Proposed rule. Federal Register 76(9):2494-2570.
USDA/FNS. 2012. Nutrition standards in the National School Lunch and School Breakfast Programs: Final rule. Federal Register 77(17):4088-4167.
Vogler, K. E., and D. Virtue. 2007. “Just the facts, ma’am”: Teaching social studies in the era of standards and high-stakes testing. Social Studies 98(2):54-58.
Wang, M. C., S. Rauzon, N. Studer, A. C. Martin, L. Craig, C. Merlo, K. Fung, D. Kursunoglu, M. Shannguan, and P. Crawford. 2010. Exposure to a comprehensive school intervention increases vegetable consumption. Journal of Adolescent Health 47(1):74-82.
Wansink, B. 2010. From mindless eating to mindlessly eating better. Physiology and Behavior 100(5):454-463.
Wood, S. 2011. Losing money, Seattle schools may ease ban on junk foods. http://usnews.msnbc.msn.com/_news/2011/12/12/9394147-losing-money-seattle-schools-may-ease-ban-on-junk-foods (accessed December 12, 2011).
Wood, Y., M. M. Cody, and M. F. Nettles. 2010. Team nutrition local wellness demonstration project report. University, MS: National Food Service Management Institute.
Woodward-Lopez, G., H. Diaz, and L. Cox. 2010a. Physical Education Research for Kids (PERK) report. Orangevale, CA: The California Task Force on Youth and Workplace Wellness.
Woodward-Lopez, G., W. Gosliner, S. E. Samuels, L. Craypo, J. Kao, and P. B. Crawford. 2010b. Lessons learned from evaluations of California’s statewide school nutrition standards. American Journal of Public Health 100(11):2137-2145.


















































