
The Committee’s charge was to explore the feasibility and need for “a New Taxonomy of human disease based on molecular biology” and to develop a potential framework for creating one. Clearly, the motivation for this study is the explosion of molecular data on humans, particularly those associated with individual patients, and the sense that there are large, as-yet-untapped opportunities to use these data to improve health outcomes. The Committee agreed with this perspective and, indeed, came to see the challenge of developing a New Taxonomy of Disease as just one element, albeit an important one, in a truly historic set of health-related challenges and opportunities associated with the rise of data-intensive biology and rapidly expanding knowledge of the mechanisms of fundamental biological processes. Hence, many of the implications of the Committee’s findings and recommendations ramify far beyond the science of disease classification and have substantial implications for nearly all stakeholders in the vast enterprise of biomedical research and patient care.
Given the scope of the Committee’s deliberations, it is appropriate to start this report by tracing the logical thread that unifies the Committee’s major findings and recommendations and connects them to its statement of task. The Committee’s charge highlights the importance of taxonomy in medicine and the potential opportunities to use molecular data to improve disease taxonomy and, thereby, health outcomes. Taxonomy is the practice and science of classification, typically considered in the context of biology (e.g., the Linnaean system for classifying living organisms). In medical practice, taxonomy often refers to the International Classification of Diseases (ICD), a system established more than 100 years ago that the World Health Organization uses to track disease incidence, physicians use as a basis for standardized diagnoses, and the health-care industry (specifically, clinicians, hospitals, and payers) uses to
determine reimbursement for care. Although the Committee was cognizant that any new-taxonomy initiative must serve the needs of the ICD and related classification systems, it concluded that this goal could best be met by rooting future improvements in disease classification in an “Information Commons” and “Knowledge Network” that would play many other roles, as well. The Committee envisions these data repositories as essential infrastructure, necessary both for creating the New Taxonomy and, more broadly, for integrating basic biological knowledge with medical histories and health outcomes of individual patients. The Committee believes that building this infrastructure—the Information Commons and Knowledge Network—is a grand challenge that, if met, would both modernize the ways in which biomedical research is conducted and, over time, lead to dramatically improved patient care (see Figure S-1).
The Committee envisions this ambitious program, which would play out on a time scale of decades rather than years, as proceeding through a blend of top-down and bottom-up activity. A major top-down component, initiated by public and private agencies that fund and regulate biomedical research, would be required to ensure that results of individual projects could be combined to
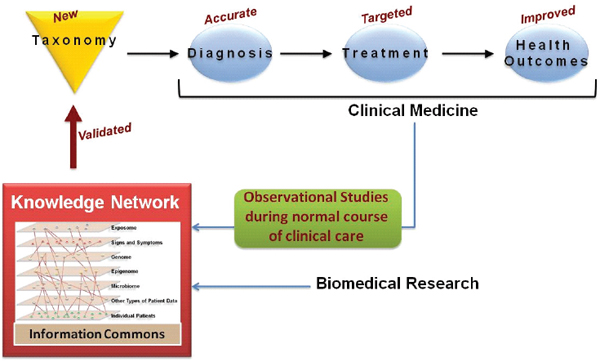
FIGURE S-1 Creation of a New Taxonomy first requires an “Information Commons” in which data on large populations of patients become broadly available for research use and a “Knowledge Network” that adds value to these data by highlighting their inter-connectedness and integrating them with evolving knowledge of fundamental biological processes.
SOURCE: Committee on A Framework for Developing a New Taxonomy of Disease.
create a broadly useful and accessible Information Commons and to establish guidelines for handling the innumerable social, ethical, and legal issues that will arise as data on individual patients become widely shared research resources. However, as is appropriate for a framework study, the Committee did not attempt to design the Information Commons, the Knowledge Network, or the New Taxonomy itself and would discourage funding agencies from over-specifying these entities in advance of initial efforts to create them. What is needed, in the Committee’s view, is a creative period of bottom-up research activity, organized through pilot projects of increasing scope and scale, from which the Committee is confident best practices would emerge. Particularly given the size and diversity of the health-care enterprise, no one approach to gathering the data that will populate the Information Commons is likely to be appropriate for all contributors. As in any initiative of this complexity, what will be needed is the right level of coordination and encouragement of the many players who will need to cooperate to create the Information Commons and Knowledge Network and thereby develop a New Taxonomy. If coordination is too rigid, much-needed innovation and adaptation to local circumstances will be stifled, while if it is too lax, it will be impossible to integrate the data that are gathered into a whole whose value greatly exceeds that of the sum of its parts, an objective the Committee believes is achievable with effective central leadership.
CONCLUSIONS
The Committee hosted a two-day workshop that convened diverse experts in both basic and clinical disease biology to address the feasibility, need, scope, impact, and consequences of creating a “New Taxonomy of human diseases based on molecular biology”. The information and opinions conveyed at the workshop informed and influenced an intensive series of Committee deliberations (in person and by teleconference) over a six-month period, which led to the following conclusions:
1. A New Taxonomy will lead to better health care. Because new information and concepts from biomedical research cannot be optimally incorporated into the disease taxonomy of today, opportunities to define diseases more precisely and to inform health-care decisions are being missed. Many disease subtypes with distinct molecular causes are still classified as one disease and, conversely, multiple different diseases share a common molecular cause. The failure to incorporate optimally new biological insights results in delayed adoption of new practice guidelines and wasteful health-care expenditures for treatments that are only effective in specific subgroups.
2. The time is right to modernize disease taxonomy. Dramatic advances in molecular biology have enabled rapid, comprehensive and
cost-efficient analysis of clinical samples, resulting in an explosion of disease-relevant data with the potential to dramatically alter disease classification. Fundamental discovery research is defining at the molecular level the processes that define and drive physiology. These developments, coupled with parallel advances in information technologies and electronic medical records, provide a transformative opportunity to create a new system to classify disease.
3. A New Taxonomy should be developed. A New Taxonomy that integrates multi-parameter molecular data with clinical data, environmental data, and health outcomes in a dynamic, iterative fashion, is feasible and should be developed. The Committee envisions a comprehensive disease taxonomy that brings the biomedical-research, public health, and health-care-delivery communities together around the related goals of advancing our understanding of disease pathogenesis and improving health. Such a New Taxonomy would
• Describe and define diseases based on their intrinsic biology in addition to traditional physical “signs and symptoms.”
• Go beyond description and be directly linked to a deeper understanding of disease mechanisms, pathogenesis, and treatments.
• Be highly dynamic, at least when used as a research tool, continuously incorporating newly emerging disease information.
4. A Knowledge Network of Disease would Enable a New Taxonomy. The informational infrastructure required to create a New Taxonomy with the characteristics described above overlaps with that required to modernize many other facets of biomedical research and patient care. This infrastructure requires an “Information Commons” in which data on large populations of patients become broadly available for research use and a “Knowledge Network” that adds value to these data by highlighting their inter-connectedness and integrating them with evolving knowledge of fundamental biological processes.
5. New models for population-based research will enable development of the Knowledge Network and New Taxonomy. Current population-based studies of disease are relatively inefficient and can generate conclusions that are not relevant to broader populations. Widespread incorporation of electronic medical records into the health-care system will make it possible to conduct such research at “point-of-care” in conjunction with the routine delivery of medical services. Moreover, only if the linked phenotypic data is acquired in the ordinary course of clinical care is it likely to be economically feasible to characterize a sufficient number of patients and ultimately to create a self-sustaining system (i.e., one in which the costs of gathering molecular data on individual patients can be medically justified in cost-benefit terms).
6. Redirection of resources could facilitate development of the Knowledge Network of Disease. The initiative to develop a New Taxonomy—and its underlying Information Commons and Knowledge Network—is a needed modernization of current approaches to integrating molecular, environmental, and phenotypic data, not an “add-on” to existing research programs. Enormous efforts are already underway to achieve many of the goals of this report. In the Committee’s view, what is missing is a system-wide emphasis on shifting the large-scale acquisition of molecular data to point-of-care settings and the coordination required to ensure that the products of the research will coalesce into an Information Commons and Knowledge Network from which a New Taxonomy (and many other benefits) can be derived. In view of this conclusion, the Committee makes no recommendations about the resource requirements of the New Taxonomy initiative. Obviously, the process could be accelerated with new resources; however, the basic thrust of the Committee’s recommendations could be pursued by redirection of resources already dedicated to increasing the medical utility of large-scale molecular datasets on individual patients.
RECOMMENDATIONS
To create a New Taxonomy and its underlying Information Commons and Knowledge Network, the Committee recommends the following:
- Conduct pilot studies that begin to populate the Information Commons with data. Pilot observational studies should be conducted in the health-care setting to assess the feasibility of integrating molecular parameters with medical histories and health outcomes in the ordinary course of clinical care. These studies would address the practical and ethical challenges involved in creating, linking, and making broadly accessible the datasets that would underlie the New Taxonomy. Best practices defined by the pilot studies should then be expanded in scope and scale to produce an Information Commons and Knowledge Network that are adequately powered to support a New Taxonomy. As this process evolves, there should be ongoing assessment of the extent to which these new informational resources actually contribute to improved health outcomes and to more cost-effective delivery of health care.
- Integrate Data to Construct a Disease Knowledge Network. As data from point-of-care pilot studies, linked to individual patients, begin to populate the Information Commons, substantial effort should go into integrating these data with the results of basic biomedical research
in order to create a dynamic, interactive Knowledge Network. This network, and the Information Commons itself, should leverage state-of-the-art information technology to provide multiple views of the data, as appropriate to the varying needs of different users (e.g., basic researchers, clinicians, outcomes researchers, payers).
- Initiate a process within an appropriate federal agency to assess the privacy issues associated with the research required to create the Information Commons. Because these issues have been studied extensively, this process need not start from scratch. However, in practical terms, investigators who wish to participate in the pilot studies discussed above—and the Institutional Review Boards who must approve their human-subjects protocols—will need specific guidance on the range of informed-consent processes appropriate for these projects. Subject to the constraints of current law and prevailing ethical standards, the Committee encourages as much flexibility as possible in the guidance provided. As much as possible, on-the-ground experience in pilot projects carried out in diverse health-care settings, rather than top-down dictates, should govern the emergence of best practices in this sensitive area, whose handling will have a make-or-break influence on the entire Information Commons/Knowledge Network/New Taxonomy initiative. Inclusion in these deliberations of health-care providers, payers, and other stakeholders outside the academic community will be essential.
- Ensure data sharing. Widespread data sharing is critical to the success of each stage of the process by which the Committee envisions creating a New Taxonomy. Most fundamentally, the molecular and phenotypic data on individual patients that populate the Information Commons must be broadly accessible so that a wide diversity of researchers can mine them for specific purposes and explore alternate ways of deriving Knowledge Networks and disease taxonomies from them. Current standards developed and adopted by federally sponsored genome projects have addressed some of these issues, but substantial barriers, particularly to the sharing of phenotypic and health-outcomes data on individual patients, remain. Data-sharing standards should be created that respect individual privacy concerns while enhancing the deposition of data into the Information Commons. Importantly, these standards should provide incentives that motivate data sharing over the establishment of proprietary databases for commercial intent. Resolving these impediments may require legislation and perhaps evolution in the public’s expectations with regard to access and privacy of health-care data.
- Develop an efficient validation process to incorporate information from the Knowledge Network of Disease into a New Taxonomy.
Insights into disease classification that emerge from the Information Commons and the derived Knowledge Network will require validation of their reproducibility and their utility for making clinically relevant distinctions (e.g., regarding prognosis or choice of treatment) before adoption into clinical use. A process should be established by which such information is validated for incorporation into a New Taxonomy to be used by physicians, patients, regulators, and payers. The speed and complexity with which such validated information emerges will undoubtedly accelerate and will require novel decision-support systems for use by all stakeholders.
- Incentivize partnerships. The Committee envisions that a New Taxonomy incorporating molecular data could become self-sustaining by accelerating delivery of better health through more accurate diagnosis and more effective and cost-efficient treatments. However, to cover initial costs associated with collecting and integrating data for the Information Commons, incentives should be developed that encourage public–private partnerships involving government, drug developers, regulators, advocacy groups, and payers.
A major beneficiary of the proposed Knowledge Network of Disease and New Taxonomy would be what has been termed “precision medicine.” The Committee is of the opinion that realizing the full promise of precision medicine, whose goal is to provide the best available care for each individual, requires that researchers and health-care providers have access to vary large sets of health and disease-related data linked to individual patients. These data are also critical for the development of the Information Commons, the Knowledge Network of Disease, and the development and validation of the New Taxonomy.








