
2
Nutrition Issues of Concern in the Community
Presenters during the first session provided background on nutrition issues that characterize the needs of older adults who would benefit from community-based nutrition services, said moderator Connie W. Bales, professor of medicine at the Duke University School of Medicine and associate director for education/evaluation at the Durham Veterans Adminstration’s Geriatric Research, Education, and Clinical Center. Attention to the issues of nutrition screening, food insecurity, sarcopenic obesity, and dietary patterns, along with supportive community resources, can contribute to improved functionality, independence, and quality of life for older adults.
NUTRITION SCREENING AT DISCHARGE AND IN THE COMMUNITY
Joseph Sharkey, professor of social and behavioral health at the Texas A&M Health Sciences Center, drew on his research with home-delivered meal participants and providers in North Carolina and Texas to discuss nutrition screening and its role in community-based programs within the Aging Network and potential partners. Screening can be a vital part of reaching the national goal of eliminating nutritional health disparities, preventing and delaying chronic disease and disease-related consequences, and improving postdischarge recovery, daily functioning, and quality of life. He
discussed nutrition screening versus assessment, challenges associated with screening, determinants of nutritional risk, and uses for nutrition screens.
Nutrition Screening Versus Assessment
Sharkey began by clarifying the difference between nutrition screening and assessment. Screening is used to identify characteristics associated with dietary or nutrition problems, and to differentiate those at high risk for nutrition problems who should be referred for further assessment or counseling. Assessment is a measurement of dietary or nutrition-related indicators, such as body mass index or nutrient intake, used to identify the presence, nature, and extent of impaired nutritional status. This information is used to develop an intervention for providing nutritional care.
Sharkey presented the pathway from the presence of a health condition, to impairment, functional limitations, disability, and adverse outcomes (Nagi, 1976; Verbrugge and Jette, 1994) and noted the role that nutrition and screening could play throughout that progression in preventing advancement to the next stage. Additional reasons for conducting nutrition screening are listed in Box 2-1.
Who Should Be Screened?
In the past, the only people screened were nutrition program participants and those seeking nutrition services. “Is that enough,” asked Sharkey, “or should screening be used more broadly to identify and pre-empt some individuals’ needs?” While screening people in the community may iden-
BOX 2-1
Reasons for Conducting Nutrition Screening
• Determine potential need/demand for community programs
• Prioritize services
• Define short- and long-term outcomes
• Identity or develop interventions
• Prepare nutrition care plans
• Make referrals
• Build basis tor additional funding
• Engage community partners
SOURCE: Sharkey, 2011.
tify more high-risk individuals, doing so is made difficult by the following contextual challenges:
• Geography. Screening and follow-up may be conducted differently in rural versus urban areas.
• Population shifts. The population of older adults in rural areas is increasing due to older adults choosing those locations to retire and younger adults leaving to find jobs.
• Culture and context. Immigration may result in the development of new communities that require screening to be conducted within the context of that population’s culture.
• Language. Nutrition providers should employ people who speak the languages of the populations being screened and can translate materials into those languages. For example, there are nuances to the Spanish language that should be considered when the population includes people from different Spanish-speaking countries.
• Literacy. Both educational and health literacy should be considered, especially in the context of various immigrant populations.
He also discussed community challenges for the use of screening:
• Spectrum of vulnerability. Screening can be used to identify those individuals at the frail end of the spectrum as well as to prevent people from moving along the continuum to that point. Screeners should be trained to provide people at all points with the appropriate nutrition information, counseling, or referrals.
• Rapid hospital discharge. Hospital discharge plans may not take into account challenges associated with high-risk individuals’ home and community environments or provide linkages to communitybased services.
• Limited/reduced funding. Community programs have limited resources so it may be challenging for individuals to locate programs that provide the services they need, such as access to healthy food and transportation.
• Engagement of nontraditional partners. How can nontraditional partners, such as the Special Supplemental Nutrition Program for Women, Infants, and Children and Federally Qualified Health Centers be engaged to assist with screening?
Determinants of Nutritional Risk
As previously mentioned, the main purpose of nutrition screening is to identify those at high risk for nutritional problems. Screening for nutri-
tional risk includes gathering information on topics that may be thought of as only partially related or unrelated to food and nutrition, such as social support and transportation. Table 2-1 identifies what are or should be components of nutrition screening and determinants of nutritional risk.
In closing, Sharkey encouraged people to consider the use of screening as a component of prevention as well as the associated ethics of screening, “How can one determine someone to be at risk for poor nutritional health and do nothing?”
TABLE 2-1 Components of Nutrition Screening
| Component | Determinants of Risk |
| Material resources |
• Adequacy of income and competing demands (other household members and financial demands) |
|
• Household environment (e.g., adequate refrigeration and storage) |
|
|
• Food security |
|
|
• Money, resources, and access |
|
|
• Frequency and duration |
|
|
• Individual components |
|
|
• Energy security (e.g., heating oil, air conditioning) |
|
| Individual resources |
• Individual capacity and complexity of tasks |
|
• Social support: familial and extrafamilial |
|
|
• Partnership status |
|
|
• Food preparation and consumption tasks (e.g., opening a jar, lifting a glass) |
|
|
• Depressive symptoms |
|
|
• Life stresses |
|
|
• Meal patterns (e.g., eating breakfast) |
|
| Health |
• Disease burden |
|
• Medications |
|
|
—Multiple prescribed and over the counter (number and therapeutic categories) —Practices to reduce or restrict cost —Adherence |
|
|
• Oral and chemosensory health (e.g., problems with chewing and swallowing) |
|
|
• Depressive symptoms |
|
|
• Life stresses |
|
| Other |
• Acculturation |
|
• Transportation |
|
|
• Access to affordable, healthy foods |
|
|
• Access to food programs |
|
SOURCE: Sharkey, 2011.
FOOD INSECURITY AMONG OLDER ADULTS
James Ziliak, chair of microeconomics at the University of Kentucky, presented data from research that he and Craig Gundersen, from the University of Illinois, conducted on food security and food assistance among older Americans. Their research examined the extent, distribution, and determinants of food insecurity among older adults, including differences by age, poverty status, race, and presence of grandchildren, and the health and nutritional consequences of food insecurity.
Households are assigned to food security categories based on responses to 18 questions in the Core Food Security Module (CFSM) developed by the U.S. Department of Agriculture (USDA) and administered as part of a supplement to the Current Population Survey. The CFSM includes questions related to conditions and behaviors experienced by households having trouble meeting basic food needs, such as, “Did you or other adults in your household ever cut the size of your meals or skip meals because there wasn’t enough money for food?” (FNS, 2000). The number of affirmative responses dictates the household’s food security category (see Table 2-2).
Trends in Food Insecurity Among Older Adults, 2001–2009
Ziliak presented analyses of nationally representative data from the December 2001–2009 Supplements to the Current Population Survey (CPS)
TABLE 2-2 Categories of Food Security
| Category | Description of Household Condition | Number of Affirmative Responses to CFSM |
| Fully food secure | No reported indications of food access problems or limitations | 0 |
| Marginal food insecurity | One or two reported indications—typically of anxiety over food sufficiency or shortage of food in the house |
1 or more |
| Food insecurity | Reports of reduced quality, variety, or desirability of diet |
3 or more |
| Very low food security | Reports of multiple indications of disrupted eating patterns and reduced food intake |
8 or more in households with children 5 or more in households without children |
NOTE: CFSM, Core Food Security Module.
SOURCE: Ziliak and Gundersen, 2011.
(U.S. Census Bureau, 2011a) to provide an overview of food insecurity rates among adults ages 40 years and older. CPS data represent the full set of questions from the CFSM and are used to establish official estimates of food insecurity in the United States.
Background on Adult Food Insecurity in the United States
Between 2001 and 2007, food insecurity rates for adults over age 50 years remained relatively constant. There were spikes in the rates after 2007, which Ziliak suggested is a result of the recession (see Figure 2-1). However, while the rates remained relatively constant in the early 2000s, the actual number of people affected by food insecurity increased at a greater rate; the numbers of people who are food insecure and very low food secure increased 40 and 52 percent, respectively. This is probably a reflection of the “aging society” and the growing number of people 50 years and older, said Ziliak.
Food insecurity among older adults is associated with age, poverty level, race, presence of grandchildren in the household, and geography. Among adults over age 40 years, food insecurity is inversely related to age; the highest rates are among persons 40–49 years (15.2 percent) and the lowest rates are among those 60 years and older (7.3 percent). Among adults ages 50 years and older whose incomes are below 200 percent of the poverty line,1 about 40 percent are marginally food insecure, 23 percent are food insecure, and 10 percent are very low food secure. There was a linear long-term increase in these rates between 2001 and 2009 and no spike in rates after 2007. There was, however, a spike in rates among people whose incomes were greater than 200 percent of the poverty line, suggesting that income is not the only factor affecting an individual’s food security status. Food insecurity rates among those living below the poverty line are two to three times higher than the rates among those living above it.
In 2009, food insecurity rates were highest among Hispanics and African Americans age 50 years and older (about 18 percent) and lowest among whites (7 percent). The spike in rates after 2007 was seen among Hispanics, whites, and Asian and Pacific Islanders, while the rates among African Americans exhibited linear increases. There remains a large gap in food insecurity rates between racial groups even after accounting for income differences (Ziliak and Gundersen, 2011).
Discussing the results from his research on multigenerational hunger,
____________________
1 In 2009, the Poverty Thresholds were $11,161 for one person under 65 years of age, $10,289 for one person 65 years of age and over, $14,787 for two people, including a householder under 65 years of age, and $14,731 for two people, including a householder 65 years of age and over (U.S. Census Bureau, 2010).
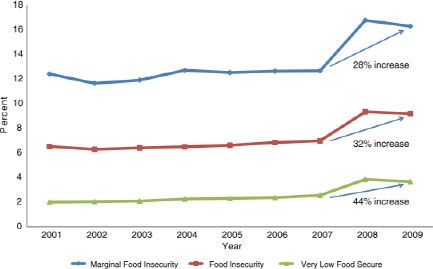
FIGURE 2-1 Food insecurity rates for people ages 50 years and older by level of food insecurity.
SOURCE: Adapted from Ziliak and Gundersen, 2011.
Ziliak showed that the presence of grandchildren in the households of adults 60 years and older is associated with higher rates of food insecurity. In 2009, about 20 percent of adults 60 years and older who had grandchildren in their households were food insecure compared to 7 percent without grandchildren in their households. While these data are more volatile due to the small sample size, rates of food insecurity are on average about three times higher in older adult households with a grandchild present than in those without grandchildren. Ziliak also illustrated the potential destabilizing effect that the presence of a grandchild can have on a food-secure household (see Table 2-3). Regardless of income level, the added presence of a grandchild greatly increases the predicted risk of food insecurity among food secure and insecure households.
“Geographically…[food insecurity] is a southern problem,” said Ziliak. Rates of food insecurity among adults 50 years and older are highest in the South (7.78 to 12.99 percent) and lowest in the northern Midwest (2.53 to 5.50 percent) (Ziliak and Gundersen, 2011), following the same trend as poverty levels.
After reviewing the data and controlling for other factors, Ziliak and Gundersen found that food insecurity is more likely to affect older adults who
TABLE 2-3 Destabilizing Effect of a Grandchild on Food-Secure and Food-Insecure Households
| Food-Secure Household | Food-Insecure Household | |||
| Income | Adult over 80 years old, white, retired, married, with a college degree, living in a metro area | Adult 60–64 years old, African American, retired, divorced/separated, did not finish high school, living in a metro area | ||
|
Predicted risk of food insecurity with and without a grandchild present |
||||
| No | Yes | No | Yes | |
| < 50% Poverty line | 5.8 | 36.9 | 53.8 | 69.6 |
| 50–100% Poverty line | 5.2 | 25.8 | 51.6 | 57.9 |
| 100–200% Poverty line | 2.8 | 21.0 | 40.5 | 51.7 |
| > 200% Poverty line | 0.6 | 5.7 | 19.9 | 23.2 |
SOURCE: Analysis of December 2001–2009 Supplements to the Current Population Survey (CPS) data (U.S. Census Bureau, 2011a).
• are living at or below the poverty level,
• do not have a high school degree,
• are African American or Hispanic,
• are divorced or separated,
• have a grandchild living in the household, and
• are younger.
Health Consequences of Food Insecurity
Ziliak and Gundersen reviewed nutrient intake data from the National Health and Nutrition Examination Survey (NHANES) to identify nutrients of concern among adults over 40 years of age. The differences in nutrient intake between food-secure and food-insecure adults in different age groups varies. There are no statistically significant differences in nutrient intake between 40–49-year-old food-secure and food-insecure individuals. Statistically significant differences in nutrient intake in the 50–59-year-old age group were identified for vitamin A, thiamin, vitamin B6, calcium, phosphorus, magnesium, and iron. However, the differences are not large in magnitude and were no longer present when the sample was restricted to adults below 200 percent of the poverty line. Food-insecure adults over age 60 years have substantially lower intakes of food and all nutrients as compared to food-secure adults in the same age group.
Food-insecure adults ages 50–59 years are more likely than food-secure
adults to have limitations in their activities of daily living (ADLs); to be depressed; or to have diabetes; and are less likely to describe their health status as good, very good, or excellent. The gap in health outcomes between food-secure and food-insecure individuals in this age group narrows when the sample is restricted to individuals whose income is below 200 percent of the poverty level. This is due to the increased number of individuals, both food secure and insecure, who have relatively poor health outcomes in this age group and income level.
When controlling for all other factors, Ziliak and Gundersen’s multivariate regression models indicate that food-insecure individuals
• ages 50–59 years do not have lower nutrient intakes;
• ages 60 years and older have statistically significant lower nutrient intakes; and
• ages 50 years and older are
— less likely to be in excellent or very good health,
— more likely to be depressed, and
— more likely to have ADL limitations (roughly equivalent to being 14 years older) (Ziliak and Gundersen, 2011).
Concluding Remarks
Ziliak concluded by reiterating the effects that various factors have on food-insecurity rates among older adults in the community and suggesting that they need to be taken into account when developing policy. Rates are highest among 40–49-year-olds, something that should be considered when developing policies for the Supplemental Nutrition Assistance Program (SNAP) since SNAP participation declines with age. Food-insecure individuals over the age of 50 years face serious health consequences; therefore, constructing policies that meet the needs of this population may reduce their risk of negative health outcomes and result in lower health care costs.
SARCOPENIC OBESITY AND AGING
When the first research on obesity and aging was published over 15 years ago, researchers needed to overcome resistance from geriatricians, said Gordon Jensen, head of the Department of Nutritional Sciences at the Pennsylvania State University. Geriatricians were trained to treat frail older adults in skilled nursing facilities who were underweight, undernourished, and suffering from functional limitations and disability; the idea of obese
older adults was new. A great deal has changed in the past 15 years and now many older adults in acute care, transitional care, chronic care, and the community are obese, representing a new population with different health care and nutrition needs.
Obesity and Function Among Older Adults
As with other age groups, obesity is a growing concern among older adults. Data from NHANES 1999–2004 show that the prevalence of obesity among men and women ages 40–79 years is over 30 percent, with rates higher than 40 and 50 percent among Mexican American and black women, respectively (Ogden et al., 2007). The rates may be higher among women because, as Jensen noted, “obese [middle-aged] men tend not to live to be obese older men.” Particularly concerning is the relationship between obesity and functional limitations. Elevated current or past body mass index (BMI) has been linked with increased self-reported functional limitations, physical performance testing has confirmed a strong relationship between elevated BMI and functional impairment, and elevated BMI has been associated with increased self-reported homebound status (Jensen, 2005). Predictors of reporting homebound status include
• 75 years of age and older,
• BMI of 35 or greater,
• poor appetite,
• income less than $6,000 a year, and
• limitations in activities of daily living and instrumental activities of daily living (Jensen, 2005).
“These days many older persons in need of services are not tiny and frail; they are large and frail,” said Jensen.
Whereas body composition studies have found positive associations between total body fat mass and functional limitations, links between muscle mass and functional limitations have been inconsistent. However, with appropriate adjustment for body size, an association may be detected between relative loss of muscle mass and increased functional limitations (Villareal et al., 2004; Zoico et al., 2004). Obesity is a proxy for sedentary living among older adults because it negatively impacts function. Contributing factors are likely to include obesity’s associated medical comorbidities such as diabetes mellitus, hypertension, dyslipidemia, metabolic syndrome, heart disease, and osteoarthritis of the knee. Recent findings further implicate inflammation, sarcopenia, and impairment of muscle function and strength as possibly contributing to functional limitations (Jensen, 2005).
Sarcopenic Obesity
Sarcopenia, the loss of muscle mass with aging, can affect both under-and overweight adults. It can be a major concern for obese older adults since they require more muscle mass to move and function. Loss of α-motor neuron input, changes in anabolic hormones, and malnutrition may lead to loss of muscle mass. However, inflammation-driven erosion of muscle mass and a vicious cycle of physical inactivity, increased body fat, and disease burden are likely to culminate in sarcopenic obesity (Jensen and Hsiao, 2010; Stenholm et al., 2008, Zamboni et al., 2008).
Weight Loss Among Obese Older Adults
Although a growing body of research supports consideration of weight loss for some obese older adults, the practice remains controversial. Jensen identified the following reasons (Jensen and Hsaio, 2010):
• Involuntary weight loss usually reflects a serious underlying disease or injury associated with adverse outcomes (Huffman, 2002; McMinnctal., 2011).
• Overweight and mild obesity may be associated with reduced mortality risk (Bouillannc ct al., 2009; Curtis ct al., 2005).
• Some extra weight may provide a metabolic reserve needed to survive illness or injury {Davenport ct al., 2009; Flcgal ct al., 2007).
• There are concerns for potential losses of muscle and bone mineral density during weight reduction (Chao ct al., 2000; Miller and Wolf, 2008; Shapscs and Ricdt, 2006).
However, findings from weight loss studies suggest that weight loss through exercise and dietary interventions can result in improvements in physical performance testing and functional assessments (Villareal et al., 2006a); reductions in coronary heart disease risk factors such as waist circumference, blood pressure, and glucose, triglyceride, C-reactive protein, and interleukin-6 levels (Villareal et al., 2006b); reductions in the diagnosis of metabolic syndrome (Villareal et al., 2006b); and improvements in systemic and adipose tissue inflammatory states, including reduced levels of C-reactive protein, interleukin-6, and other inflammatory cytokines (Dalmas et al., 2011). A study conducted by Villareal and colleagues (2011) found that a combination of diet and exercise resulted in the greatest improvements in physical function (see Figure 2-2) and diet or a combination of diet and exercise resulted in the most weight loss (see Figure 2-3).
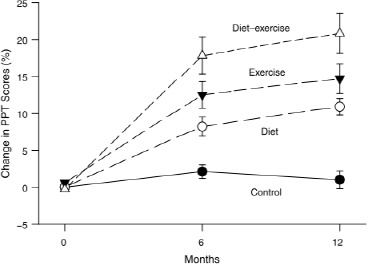
FIGURE 2-2 Mean percent changes in Physical Performance Test (PPT) during intervention.
SOURCE: Villareal et al., 2011. © Massachusetts Medical Society. Reprinted with permission.
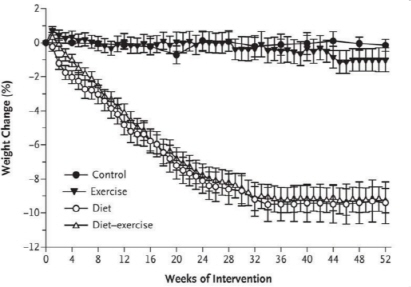
FIGURE 2-3 Mean percent changes in body weight during intervention.
SOURCE: Villareal et al., 2011. © Massachusetts Medical Society. Reprinted with permission.
Weight Status and Nutrient Intake
Jensen presented data from a community-based study of nutrition risk in older persons, further supporting the presence of malnutrition characterized by nutrient deficiencies in obese older adults. Both men and women had inadequate intakes of folate, magnesium, vitamin E, vitamin B6, zinc, vitamin D, and calcium (Ledikwe et al., 2003). Despite having similar nutrient intakes after adjusting for other factors, only for women were BMI and waist circumference positively associated with intakes of fat and saturated fat and negatively associated with Healthy Eating Index scores and intakes of carbohydrates, fiber, folate, magnesium, iron, and zinc. One explanation for why obese older women were less likely than men to meet nutrient requirements and to have healthy eating patterns may be that older women often live alone whereas men reside with a significant other.
Research Priorities Related to Weight Loss Among Older Adults
In closing, Jensen posed the following questions related to research priorities (Jensen and Hsaio, 2010):
• Which obese older people should be selected for weight reduction?
• What program of prudent diet, behavior modification, and/or exercise is appropriate for which audience?
• What degree of weight loss is appropriate for which audience?
• Are there better approaches to preservation of muscle and bone mineral density during weight reduction?
• For whom is an emphasis on strength and flexibility rather than weight loss the best option?
• Can benefits of weight reduction be maintained in aging subjects?
• Are there anti-inflammatory, resistance training, hormonal, nutritional, or other interventions that may be helpful in preventing or treating sarcopenic obesity?
• Should priority for obese older persons be on diet quality, protein, and micronutricnts?
DIETARY INTAKE PATTERNS IN OLDER ADULTS
Katherine Tucker, professor and chair of the Department of Health Sciences at Northeastern University, explained that individuals’ dietary needs change with aging. Older adults may require less energy, experience less effi-
cient absorption and utilization of many nutrients, and have different nutrient requirements due to chronic conditions and medications. These changes result in older adults needing a nutrient-dense diet. Unfortunately, it can be challenging for this population to obtain such a nutrient-dense diet because it involves overcoming barriers such as loss of appetite, changes in taste and smell, oral health decline, mobility constraints, and lower incomes.
Inadequate Intake
Data from the 2003–2004 NHANES were used by the Institute of Medicine Committee to Review Child and Adult Care Food Program Meal Requirements to identify the prevalence of inadequacy of protein and select nutrients among adults 60 years and older (IOM, 2011a) (see Table 2-4). Using NHANES data for adults 70 years and older, Lichtenstein and colleagues (2008) reported calcium, potassium, fiber, and vitamins D, E, and K as shortfall nutrients. In addition to those nutrients, Tucker emphasized the importance of adequate protein intake for prevention of sarcopenia and noted the controversy regarding the current recommendation for protein intake among older adults; should it be the same as the recommendation for younger adults or should it be higher?
TABLE 2-4 Estimated Prevalence of Inadequacy (%) of Protein and Selected Vitamins and Minerals Among Adults ≥ 60 Years Based on Usual Nutrient Intakes from NHANES 2003–2004a
| Nutrient | Males | Females |
| Protein | 12 | 20 |
| Vitamin A | 54 | 43 |
| Vitamin C | 49 | 40 |
| Vitamin E | 92 | 98 |
| Thiamin | 6.0 | 12 |
| Riboflavin | 2.8 | 3.7 |
| Niacin | 1.8 | 4.6 |
| Vitamin B6 | 19 | 39 |
| Folate | 11 | 24 |
| Vitamin B12 | 2.4 | 9.0 |
| Phosphorus | 1.2 | 4.8 |
| Magnesium | 78 | 73 |
| Iron | 1.0 | 1.5 |
| Zinc | 26 | 21 |
a All nutrients in this table have an Estimated Average Requirement (EAR).
SOURCES: Adapted from IOM, 2011a. Intake data from NHANES 2003–2004. Estimated Average Requirements from Dietary Reference Intake reports (IOM, 1997, 1998, 2000, 2001, 2002/2005).
Tucker highlighted several nutrients of concern in the older adult population.
• Protein. The current Estimated Average Requirement for protein for all adults 19 years and older is 0.66 g/kg/day; however, Tucker indicated that a moderately higher protein intake (1.0–1.3 g/kg/day) may be required for older adults to maintain nitrogen balance due to decreased efficiency of protein synthesis and impaired insulin action. Need for increased protein intake is further supported by the Health, Aging, and Body Composition Study, which found that older adults with the highest intake of protein lost less lean body mass than those with lower protein intakes (Houston et al., 2008). However, there is some concern that higher protein intake may increase risk of toxicity or impaired renal function (Paddon-Jones et al., 2008).
• Vitamin E. Vitamin E is important because of its role as an antioxidant and in immune function. There is some controversy over whether the current Recommended Daily Allowance, 15 mg of α-tocopherol, is too high, as very few individuals are able to meet this recommendation from diet alone. Vitamin E supplements increase α-tocopherol levels while reducing γ-tocopherol, so supplements may not be the healthiest option for increasing intake. Some literature suggests that other tocopherols (found in nuts, seeds, and plant oils) are also important (Saldeen and Saldeen, 2005); however, there are no current nutrient recommendations for other forms of vitamin E.
• Vitamin B12. Although the daily intake of total vitamin B12 does not appear to be low for most older adults, dietary intake data may underestimate the number of people who are vitamin B12 deficient given that atrophic gastritis and loss of stomach acid prevent some older adults from absorbing it. As a result, the Institute of Medicine (IOM, 2011a) recommended that older adults get their vitamin B12 in crystalline form such as from fortified foods or supplements. The Framingham Offspring Study found that nonsupplement users had a higher prevalence of low B12 (less than 250 μmol/L) than those who were taking a supplement containing vitamin B12 (Tucker et al., 2000). Vitamin B12 deficiency can lead to peripheral neuropathy, balance disturbances, cognitive disturbances, physical disability, and increased risk of heart disease from high homocysteine. Tucker stated, “It’s critical that more attention be given to this important nutrient as many of these symptoms are nonspecific and not always diagnosed correctly.”
• Vitamin B6. Vitamin B6 is important for numerous metabolic reactions and health outcomes. Inadequacy may lead to high homo-
cysteine and impaired immune function and has been associated with impaired cognitive function and depression. Data from the Massachusetts Hispanic Elders Study showed that 30 percent of Hispanics and 28 percent of non-Hispanic whites had plasma pyridoxal 5’-phosphate (PLP; the active form of vitamin B6 used as a biomarker for vitamin B6 status) concentrations less than 30 nmol/L (indicator of inadequate status), and 11 percent of Hispanics and 16 percent of nonwhite Hispanics had concentrations less than 20 nmol/L (clinical cutoff level indicating deficient concentrations). Furthermore, PLP was associated with depressive symptomatology in this population-based study of older adults (Merete et al., 2008).
• Omega-3 fatty acids. Among adults 60 years and older, the median intake of α-linolenic acid by women was above the Adequate Intake (AI), whereas the median intake by men was not (IOM, 2011a). Omega-3 fatty acids are associated with protection against heart disease, diabetes, and cognitive decline. Low intake may be partially due to the limited sources in the diet (e.g., fatty fish, flax seeds, and walnuts).
• Dietary fiber. Fiber is important for intestinal health and protection against heart disease and metabolic syndrome; however, the median intakes of neither men nor women 60 years and older meet the AI (IOM, 2011a).
• Vitamin D. Tucker reported that older adults’ poor vitamin D intake and status may be due to low intakes of fortified dairy foods and fatty fish, low sun exposure, reduced dermal synthesis of vitamin D3 (IOM, 2011b), and decreased capacity of kidneys to convert 25OHD into 1,25-OH2-D. A study of homebound older adults found that about 65 percent had suboptimal concentrations of 25OHD in their blood (less than 50 nmol/L) and 48 percent had intakes below 400 International Units (Buell et al., 2009). In addition to its importance to bone status, vitamin D deficiency has been associated with neurological conditions, diabetes, and other metabolic conditions. Increasingly, more nutritionists are recommending that older adults take a vitamin D supplement.
Excessive Intakes
Excessive intake of some nutrients is also a concern among older adults as it is for the general population.
• Sodium. The Tolerable Upper Intake Level for sodium is 2.3 g/day; however, the 2010 Dietary Guidelines Advisory Committee (DGAC)
recommended it should be lowered to 1.5 g/day (HHS and USDA, 2010) to reduce the risk of hypertension and heart disease. Men and women over the age of 70 years are exceeding both recommendations; the usual daily mean intake for men and women is 3.0 and 2.4 g, respectively (IOM, 2010; NHANES 2003–2006).
• Saturated fat. The DGAC’s 2010 interim recommendation for saturated fat intake is less than 10 percent of energy intake, with the goal of reducing that recommendation to 7 percent (HHS and USDA, 2010). However, most adults have intakes greater than 10 percent of their energy intake (NHANES 2001–2004, 2005–2006).
• Folic acid. Whereas some adults do not meet the recommended intake levels of folic acid (400 μg), research shows that others are at risk of exceeding the upper level of 1,000 μg per day due to intake of fortified flour and breakfast cereals, and supplement use. More research is needed but high folic acid may contribute to the progression of neurological diseases associated with vitamin B12 deficiency (IOM, 1998) and lead to increased risk of some cancers (Cole et al., 2007; Mason et al., 2007; Stolzenberg-Solomon et al., 2006).
Food Intakes
In order to determine why older adults’ nutrient intakes are inadequate, one must review their food intake patterns. The 2011 IOM report Child and Adult Care Food Programs: Aligning Dietary Guidance for All presented the mean daily food group intakes by adults ages 60 years and older as compared to the 2,000-calorie MyPyramid food group pattern. It showed that older adults are not meeting any of the MyPyramid food group recommendations and are exceeding the recommendations for daily intake of solid fats and added sugar (see Table 2-5).
Baltimore Longitudinal Study of Aging
The Baltimore Longitudinal Study of Aging collected dietary intake data from 7-day diet records of adults ages 30–80 years old. Five dietary patterns were derived from the data and labeled as follows: “white bread,” “healthy,” “meat and potatoes,” “sweets,” and “alcohol.” The patterns were based on the foods that contributed the greatest amount of energy to the group; for example, individuals consuming a healthy diet ate more fruit, reduced-fat dairy, and high-fiber cereal. On average, those in the meat and potatoes group had the most gains in BMI over time, those in the white bread group had the largest gains in waist circumference, and those in the healthy group had the smallest gains in both (Newby et al., 2003).
TABLE 2-5 2,000-Calorie MyPyramid Food Group Pattern and Mean Daily Amounts Consumed by Adults ≥ 60 Years of Age
|
≥ 19 Years |
≥ 60 Years |
|
| Food Group or Component | 2,000-kcal Patterna | Mean Intakeb |
| Total fruit (cup eq) | 2.0 | 1.1 |
| Total vegetables (cup eq) | 2.5 | 1.7 |
| Whole grains (oz eq) | 3.0 | 0.86 |
| Total milk group (8 fl oz eq) | 3.0 | 1.3 |
| SoFAS (kcal) | 267 | 570 |
NOTES: eq, equivalent; fl, fluid; kcal, calories; oz, ounce; SoFAS, solid fats and and sugar.
a Britten et al., 2006.
b NHANES 2003–2004.
SOURCES: Adapted from IOM, 2011a.
Jackson Heart Study
Using similar methods as the Baltimore Longitudinal Study, this study of African Americans in the southern United States identified different patterns than those listed above. The most common pattern was the “fast food pattern”—characterized by fast food, salty snacks, soft drinks, and meat—which was high in energy, fat, trans fat, and saturated fat. The second most common pattern was the “Southern pattern,” which consisted of more cornbread and was high in fat and lower in dietary fiber. The “prudent pattern” was the least common, reported by only 17 percent of participants, the majority of which were women (Talegawkar et al., 2008).
Recommendations for Older Adults
Tucker concluded her presentation by recommending some dietary changes based on the available data. Older adults should be encouraged to eat
• more fruits and vegetables, especially orange and dark green vegetables, to increase intakes of vitamin C, carotenoids, folate, vitamin B6, magnesium, potassium, and dietary fiber;
• more low-fat dairy to improve intakes of magnesium, calcium, potassium, and vitamins B12 and D;
• more whole grains, including more fortified breakfast cereals, to increase intakes of vitamin B6, crystalline vitamin B12, magnesium, and dietary fiber;
• fewer foods high in sugar, solid fats, sodium; and
• fewer refined grains.
ECONOMIC AND RESOURCE ISSUES SURROUNDING
NUTRITION SERVICES FOR OLDER PERSONS
IN THE COMMUNITY SETTING
Kathryn Larin presented information from two congressionally requested reports developed by the Government Accountability Office (GAO) that focus on nutrition assistance available to older adults. The first report reviewed all of the federally funded nutrition programs in the United States and highlighted the effectiveness of the programs (GAO, 2011a), and the second focused on the Older Americans Act (OAA) Nutrition Program (GAO, 2011b).
Nutrition Assistance Programs Available to Older Adults
GAO’s review of the 18 nutrition assistance programs identified four programs that target older adults and three more that are available to the general population but can be accessed by older adults.2 These programs are listed in Box 2-2.
These programs range in size, reach, amount of federal spending, and types of services provided. Table 2-6 lists the approximate participation in and federal spending on these programs.
Research on the Effectiveness of the Nutrition Assistance Programs
As a part of the report, GAO reviewed the programs’ purposes, goals, and the extent to which the goals were being met. While research on these programs is limited, GAO did identify some information on the effectiveness of SNAP and the OAA Nutrition Program.
The goals of the OAA Nutrition Program are to (1) reduce hunger and food insecurity, (2) promote socialization of older individuals, and (3) promote the health and well-being of older individuals through access to nutrition and other disease prevention and health promotion services (AoA, 2011). Studies found that participation in the OAA Nutrition Program resulted in reduced likelihood of food insecurity (Edwards et al., 1993), higher levels of socialization and nutrient intake (Millen et el., 2002), and lower nutrient intakes on days when their meals were not delivered (Sharkey, 2003). Larin said these results are only suggestive because some of
____________________
2 Some older adults may be eligible for services through the Community Food Projects Competitive Grant Program; the Food Distribution Program on Indian Reservations; Grants to American Indian, Alaska Native, and Native Hawaiian Organizations for Nutrition and Supportive Services; and the Nutrition Assistance of Puerto Rico.
BOX 2-2
Nutrition Assistance Programs Available to Older Adults
Programs Targeted to Older Adults
• Older Americans Act (OAA) Nutrition Program
• Senior Farmers’ Market Nutrition Program
• Commodity Supplemental Food Program (CSFP): adults age 60 years and older who meet income eligibility requirements
• Child and Adult Care Food Program (CACFP): chronically impaired disabled adults and adults age 60 years and older in adult day care centers
Programs That Allow Older Adult Participation
• Supplemental Nutrition Assistance Program (SNAP)
• The Emergency Food Assistance Program (TEFAP)
• The Emergency Food and Shelter National Board Program
TABLE 2-6 Primary Nutrition Assistance Programs Available to Older Adults, FY 2008
| Program | Federal Spending (in millions of dollars) | Participation (approximate) |
| SNAP | 37,645.4 | 28.4 million people 12.7 million householdsa |
| CACFP | 2,394.1 | 108,000 adults and 3.1 million childrenb |
| OAA Nutrition Program | 745.0 | More than 2.5 million seniors |
| TEFAP | 230.6 | |
| Emergency Food and Shelter National Board Program | 140.1 | 73 million meals served |
| CSFP | 100.4 | 440,000 elderly and 31,000 women, infants, and childrena |
| Senior Farmers’ Market Nutrition Program | 20.1 | 953,000 low-income seniors |
NOTES: CACFP, Children and Adult Care Food Program; CSFP, Commodity Supplemental Food Program; FY, fiscal year; OAA, Older Americans Act; SNAP, Supplemental Nutrition Assistance Program; TEFAP, The Emergency Food Assistance Program.
a Average per month.
b Average per day.
SOURCE: Consolidated Federal Funds Report, FY 2008.
this research was conducted on pilot or demonstration programs that may not reflect the manner in which the program operates at the national level.
Studies on SNAP found that participation increases household food expenditures (ERS, 2004), increases nutrient availability to households (ERS, 2004), and may reduce anemia and other nutritional deficiencies (Lee et al., 2006). However, research on SNAP generally finds impact at the household level and has found little impact of participation on individuals’ dietary or nutrient intake, possibly because not all individuals share equally in SNAP benefits. Furthermore, there has been no SNAP research focused on older adult participants.
Despite the minimal research on the effectiveness of the OAA Nutrition Program, that which is available identifies possible ways to strengthen the program. Research suggests that providing home-delivered breakfast in addition to lunch may increase levels of food security and result in increased intake of calories, protein, carbohydrates, fiber, and minerals by participants (Gollub and Weddle, 2004). In addition, participants’ calorie and nutrient intakes could also be increased by delivering “enhanced” energy-dense meals (Silver et al., 2008). However, Larin reiterated that research is limited and dated and that further research on both congregate and home-delivered meals is needed to determine effectiveness. Research on pilot programs may also be beneficial to identify model programs.
Overlap, Duplication, and Fragmentation in Nutrition Assistance Programs
In response to a federal mandate (GAO, 2011c), GAO reviewed nutrition assistance programs to identify areas of program overlap, duplication, and fragmentation. Overlap and duplication are evidenced by multiple programs providing similar services to the same population, while fragmentation is the provision of services through multiple agencies at the federal, state, and local levels. GAO found that the OAA Nutrition Program and Commodity Supplemental Food Program (CSFP) both target older adults, CSFP and The Emergency Food Assistance Program provide similar benefits, and older adults may participate in several programs simultaneously. While providers perceive overlap and duplication as beneficial because it provides multiple points of access and increases the chance that those needing services will obtain them, it may also result in increased administrative costs, inefficient use of federal funding, and confusion among participants and providers.
GAO Report on the OAA Elderly Nutrition Program
GAO analysis of the December Current Population Survey Food Security Supplement shows that among low-income older adult households (age
60 years and older with incomes less than 185 percent of the poverty level), 8.6 percent are food insecure; of these, 5.3 percent have low food security, and 3.3 percent have very low food security (GAO, 2011a). Larin suggested that these numbers likely reflect older adults who need nutrition assistance but are not participating in the programs. Table 2-7 shows the percentage of low-income adults that had characteristics associated with need for nutrition services and the percentages who did and did not receive those services. Larin highlighted the approximately 89 percent of food-insecure older adults that received neither home-delivered nor congregate meals.
Larin suggested that older adults may not be participating in the programs because they
• have limited awareness of available services;
• live in areas with limited available services;
• receive informal services through friends, family, or other organizations;
• choose not to obtain government assistance; or
• receive nutrition assistance through other federal programs, such as SNAP.
Increased Demand for OAA Elderly Nutrition Program Services
A GAO survey of local agencies conducted in the summer of 2010 reports that requests for home-delivered and congregate meals have increased 79 and 47 percent, respectively, since the start of the economic downturn in late 2007. Officials suggest that the increased requests for meals reflects the growing number of adults 60 years and older (greater than than 11 million more Americans were 60 years and older in 2010 than in 2000 [U.S. Census Bureau, 2011b]) and the increasing number of older adults staying in their homes rather than moving to assisted living facilities.
Unfortunately, Larin stated, the growing need for meal services, particularly home-delivered meals, surpasses available resources. While the congregate meal program served more clients in fiscal year (FY) 2008 than the home-delivered meal program, data reflect increasing requests for homedelivered meals. Twenty-two percent of the agencies surveyed by GAO reported being unable to serve all the clients who requested home-delivered meals compared to 5 percent of agencies expressing the same concern about congregate meals. This is in line with data from the Congressional Research Service showing that between 1999 and 2008 the number of congregate meals served decreased by 34 percent while the number of home-delivered meals increased by 44 percent (CRS, 2010). In order to meet this changing need, local programs are shifting funding from congregate meals to homedelivered meals; each year between FY 2000 and FY 2008 the states collec-
TABLE 2-7 Percentage of Low-Income Older Adultsa with Each Characteristic of Likely Need for Meals Services and Percentages Who Did and Did Not Receive Meals Services
| Characteristic of Likely Need | Have Each Characteristic | Received Home-Delivered Meals | Did Not Receive Home-Delivered Meals | Received Congregate Meals | Did Not Receive Congregate Meals | Received Either Type of Meal | Received Neither Type of Meal |
| Food security | |||||||
|
Food secure |
81.4 | 3.3 | 96.7 | 5.7 | 94.3 | 8.3 | 91.7 |
|
Food insecure |
18.6 | 7.4 | 92.6 | 4.9 | 95.1 | 11.1 | 88.9 |
| Numbers of difficulties with daily activities | |||||||
|
None |
65.2 | 2.3 | 97.7 | 5.1 | 94.9 | 6.9 | 93.1 |
|
One |
18.0 | 3.6 | 96.4 | 6.3 | 93.7 | 8.8 | 91.2 |
|
Two or more |
16.8 | 11.5 | 88.5 | 6.4 | 93.6 | 16.7 | 83.3 |
| Social isolationb | |||||||
|
Less isolated |
31.8 | 2.5 | 97.5 | 6.1 | 93.9 | 7.9 | 92.1 |
|
More isolated |
41.4 | 5.0 | 95.0 | 5.0 | 95.0 | 9.0 | 91.0 |
|
Missingc |
26.8 | 4.5 | 95.5 | 5.8 | 94.2 | 9.7 | 90.3 |
a Adults over the age of 60 years whose incomes were below 185 percent of the poverty level.
b Likely need for more social interactions was defined as a response of “no” to all Current Population Survey civic engagement supplement questions about the older adult’s participation in social activities. However, such survey data cannot capture more qualitative aspects of an individual older adult’s likely need.
cApproximately 27 percent of the older adults with low incomes in the sample provided information about participation in meals programs, but not about participation in social groups.
SOURCE: GAO, 2011a. Analysis of December 2008 Current Population Survey Food Security Supplement data.
tively transferred $67 million out of the congregate meal program and into other OAA programs, such as home-delivered meals and support services (GAO, 2011b). Despite the growing need for nutrition services, funding decreased for all programs in 2010, resulting in many programs reducing operational and administrative costs and services.
Closing Comments
Over $90 billion a year is currently spent on nutrition assistance programs, including multiple programs providing services to older adults. Research shows that some of these programs are effectively addressing older adults’ nutritional and social needs, yet more updated research is needed to provide additional effectiveness data and to identify services to meet older adults’ changing needs. Unfortunately, while need for these programs continues to increase, funding will only continue to decrease in the current budgetary environment. Therefore, it is important that further research identifies and reduces overlap, duplication, and fragmentation of services so funds can be used efficiently.
DISCUSSION
During the discussion, points raised by participants included the importance of breakfast, vitamin B12 intake, food insecurity, the role of SNAP, and socioeconomic status and food patterns.
The Importance of Breakfast
In response to a request from Robert Miller, Sharkey expanded on the importance of breakfast by stating that consumption of a regular breakfast “jump-started the metabolism for the day” and resulted in increased intake of calcium, vitamin D, magnesium, and phosphorus. Older adults who received breakfast and lunch delivered to their homes consumed more calories, protein, carbohydrates, fiber, and minerals than those who only received lunch, said Larin. Nancy Wellman said that breakfast is one of the easier meals for older adults to assemble; therefore, they should be encouraged to eat that meal at some point during the day.
Crystalline Vitamin B12 Intake
Melanie Polk raised the issue of vitamin B12 absorption among individuals who are on chronic use of proton pump inhibitors for gastroesophageal reflux disease. Tucker noted that one of the reasons so many older adults are diagnosed as vitamin B12 deficient is due to the use of these proton pump inhibitors. However, studies show that some crystalline vitamin B12 will be absorbed even in those taking proton pump inhibitors if given in large enough doses.
Food Insecurity Among Older Adult Households with Grandchildren Present
Elizabeth Walker asked why the presence of a grandchild in an older adult’s household is associated with higher food insecurity. She wondered whether it was related to the grandparents acting as the primary caregivers or simply due to children being given first choice of the available foods before the adults? Ziliak explained that he and Gundersen are currently examining the health consequences associated with multigenerational food insecurity and will have more results in the near future. The results he presented during the workshop are based solely on the presence of a grandchild, and findings suggest that food insecurity is associated with “the additional anxiety of trying to provide for multiple other individuals [on] a very fixed income.” After controlling for income, “on average the presence of a grandchild increases that risk [of food insecurity] by about 50 percent, whether the parent is there or not.”
Wellman said that the percent of grandparents caring for a grandchild is fairly low, and Ziliak confirmed that it is probably around 3 to 5 percent; however, there are substantial differences between races and the rate is probably closer to 15 percent in African American households. Sharkey suggested further research to determine food distribution in households where grandparents are present but are not the primary caregivers for the children.
Role of SNAP Among Older Adults
In response to a request from Julie Locher for more information on the role of SNAP in addressing food security among older adults, Larin noted that SNAP is underutilized by older adults. They have the lowest participation rates in SNAP, possibly since they are only eligible for the minimum benefit ($14–$16 per month). Ziliak said, although he cannot prove causality, SNAP participants are at a greater risk of food insecurity and more research needs to be done on that relationship.
Socioeconomic Status and Food Patterns
Charlene Compher inquired about the association between socioeconomic status and dietary patterns. Tucker confirmed this association; she noted that people with limited resources are more likely to choose high-calorie, highly refined, high-sugar foods because they are generally less expensive. Diets comprising fruits and vegetables, low-fat dairy foods, and lean meats are more expensive, less widely available, and heavier to carry, all of which may prevent low-income older adults from purchasing them.
NUTRITION ISSUES RELATED TO AGING IN THE COMMUNITY:
PERSPECTIVES AND DISCUSSION
In the final session of the morning, several speakers representing the workshop sponsoring agencies provided perspectives on nutrition issues of concern related to aging in the community. The moderator, Gordon Jensen, encouraged presenters to discuss important nutritional needs for older adults that differ from those of the community, gaps in services for older adults choosing to stay in their homes, and promising actions for addressing the unique needs to this population.
A Perspective from Abbott Nutrition
Robert Miller, Divisional Vice President of Global Research and Development and Scientific Affairs at Abbott Nutrition, asked “how does [the industry] get nutrition to those people that most need it?” He pointed to the lack of data from intervention studies needed to demonstrate nutrition’s impact and stressed the importance of more research to track the effects of nutrition education and supplementation.
In 2010, about 15 percent of hospital patients received nutrition supplementation, the same percent as in 2000. Initial reviews of data suggest that people receiving nutritional supplementation have shorter hospital stays and lower rates of readmission, resulting in lower health care costs. Clinical trials should be used to translate research into something that can be implemented by industry, Miller said. For example, Abbott conducted a pilot study to determine the effect of a nutrition screening and education initiative on hospital readmission rates. The 30-day readmission rate of the 1,000 people followed over 6 months was 8.7 percent, compared to about 24 percent for the area average and 26 percent for the national average. “One of the most simple things in a doctor’s bag is education and nutrition
…and how do we bring everything from payer, industry, manufacturer, academics, [and] government together to tackle this,” Miller concluded.
A Perspective from the Administration on Aging
Jean Lloyd, national nutritionist for the Administration on Aging (AoA), expanded on previous presentations’ discussion of the OAA Nutrition Programs. “Although we’ve talked primarily about the fact that meals are our primary service, it’s not just a meals program; it is a nutrition program…not a malnutrition program.” In efforts to meet the program’s three goals (see earlier discussion in this chapter), each year about 50 million meals are home delivered (about 170 meals per participant) and 92.5 million congregate meals are served (about 55 meals per participant). Due to limited government funding, the number of meals served each year has declined; federal funds account for only about 28 percent of the expenditure for home-delivered meals and 41 percent for congregate meals.
In addition to providing meals that meet the current dietary guidelines, the OAA Nutrition Program also includes nutrition education and counseling. The OAA, Lloyd said, provides the opportunity for collaboration among various assistance programs in parallel systems, such as Medicaid waiver programs and the Veterans Administration, in order to develop “comprehensive and coordinated service systems” to meet the nutrition needs of older adults. Despite the success of the program in meeting the needs of this complex and vulnerable population, AoA still faces funding and service cuts and limited nutrition expertise in sites across the country. However, AoA is committed to continuing to improve the way it provides services by conducting research to better understand the needs of its service population. Future plans include conducting outcomes research in the field, administration of process improvement surveys, and research of short-term methods for reducing food insecurity. As a long-term goal, AoA will be conducting impact studies that include reviews of Medicare records for data on emergency room visits and hospitalizations among participants and nonparticipants.
A Perspective from Meals On Wheels Association of America and
Meals On Wheels Association of America Research Foundation:
The Hidden Hungry
“Over the past 21 years, which is as long as I have been with [Meals On Wheels Association of America], I have become something of an authority on what we at Meals On Wheels Association of America call the ‘hidden hungry,’” said Enid Borden, president and Chief Executive Officer. She travels across the country, speaks with people who are “living behind
closed doors,” gives them meals, and, most important, listens to their stories. These older adults may live in the community, but they often stand apart from it and are overlooked. She hoped her presentation would help the audience get to know the population being served by giving these older adults a “human face and voice.”
Older adults needing nutrition services are often overlooked by the community in which they live. She described a trip to a town in Arkansas with a population of 117 that had become a food desert.3 She met an 86-year-old woman that had lived there all her life in the house where she was born. This woman was all alone except for the Meals On Wheels volunteer who delivered her meals. Borden said, “She told me that if it weren’t for Meals On Wheels, she would be dead. She was right.”
DISCUSSION
During the discussion, points raised by participants included information for case managers, research steps, and aging in place.
Information for Case Managers
Heather Keller inquired about information that case managers should have to help them determine if they are missing people at nutrition risk. Lloyd responded that many tools used by case managers do not include a nutrition component, with the exception of obtaining information on special diets or nutrition needs based on ADLs. She suggested that case managers find out more about a person’s weight history, appetite, income, oral conditions, and instrumental ADLs (e.g., shopping for and preparing meals) and correlate them with responses to food insecurity and functionality questions.
Research Gaps
Robert Russell noted that a real research gap is the lack of analysis of Medicare and Medicaid records to track the effectiveness of interventions on preventing hospital admissions and readmissions. He asked how
____________________
3 The Food, Conservation, and Energy Act of 2008 (also known as the Farm Bill) (HR 6124, Sec. 7527) defines a food desert as “an area in the United States with limited access to affordable and nutritious food, particularly such an area composed of predominantly lower-income neighborhoods and communities.”
this would be done by AoA considering differences between programs in various regions of the country; would it be a nationwide evaluation or a review of a selection of similar programs? Lloyd responded that it will be a nationwide evaluation that includes process surveys conducted in all state units on aging, about half of the area agencies on aging, and local providers. The statistical method is still being finalized, but the evaluation will include meal cost at the local level to compare the cost of preparing meals different ways in various parts of the country and a comparison of Medicare data from participants and nonparticipants with different racial and ethnic backgrounds in the same community.
Aging in Place
Katherine Tallmadge pointed out that many communities are organizing groups focusing on aging in place, but wondered if there were any regulations ensuring that people in those groups receive appropriate nutritional care, such as having them track their weight and food intake for consultation with a dietitian. Since those organizations are locally funded and organized and receive no federal funds, the community decides on the requirements, said Lloyd.
Lloyd also addressed the larger issue of programs designed to help keep older adults in their homes. Medicaid funds home- and community-based waivers that are used to keep people out of nursing homes. It is a personcentered program and there are no nutrition or food requirements; however, the states have the option of including them. Over half the states offer a meal service under the waiver program and some states include nutritional supplements and other nutrition services.
REFERENCES
AoA (Administration on Aging). 2011. Home & Community Based Long-Term Care: Nutrition Services (OAA Title IIIC). http://www.aoa.gov/aoaroot/aoa_programs/hcltc/nutrition_services/index.aspx (accessed November 14, 2011).
Bouillanne, O., C. Dupont-Belmont, P. Hay, B. Hamon-Vilcot, L. Cynober, and C. Aussel. 2009. Fat mass protects hospitalized elderly persons against morbidity and mortality. American Journal of Clinical Nutrition 90(3):505–510.
Britten, P., K. Marcoe, S. Yamini, and C. Davis. 2006. Development of food intake patterns for the MyPyramid Food Guidance System. Journal of Nutrition Education and Behavior 38(6 Suppl):S78–S92.
Buell, J. S., T. M. Scott, B. Dawson-Hughes, G. E. Dallal, I. H. Rosenberg, M. F. Folstein, and K. L. Tucker. 2009. Vitamin D is associated with cognitive function in elders receiving home health services. Journal of Gerontology—Series A Biological Sciences and Medical Sciences 64(8):888–895.
Chao, D., M. A. Espeland, D. Farmer, T. C. Register, L. Lenchik, W. B. Applegate, and W. H. Ettinger Jr. 2000. Effect of voluntary weight loss on bone mineral density in older overweight women. Journal of the American Geriatrics Society 48(7):753–759.
Cole, B. F., J. A. Baron, R. S. Sandler, R. W. Haile, D. J. Ahnen, R. S. Bresalier, G. McKeown-Eyssen, R. W. Summers, R. I. Rothstein, C. A. Burke, D. C. Snover, T. R. Church, J. I. Allen, D. J. Robertson, G. J. Beck, J. H. Bond, T. Byers, J. S. Mandel, L. A. Mott, L. H. Pearson, E. L. Barry, J. R. Rees, N. Marcon, F. Saibil, P. M. Ueland, and E. R. Greenberg. 2007. Folic acid for the prevention of colorectal adenomas: A randomized clinical trial. Journal of the American Medical Association 297(21):2351–2359.
CRS (Congressional Research Service). 2010. Older Americans Act: Title III Nutrition Services Program. http://aging.senate.gov/crs/nutrition1.pdf (accessed October 10, 2011).
Curtis, J. P., J. G. Selter, Y. Wang, S. S. Rathore, I. S. Jovin, F. Jadbabaie, M. Kosiborod, E. L. Portnay, S. I. Sokol, F. Bader, and H. M. Krumholz. 2005. The obesity paradox: Body mass index and outcomes in patients with heart failure. Archives of Internal Medicine 165(1):55–61.
Dalmas, E., C. Rouault, M. Abdennour, C. Rovere, S. Rizkalla, A. Bar-Hen, J. L. Nahon, J. L. Bouillot, M. Guerre-Millo, K. Clément, and C. Poitou. 2011. Variations in circulating inflammatory factors are related to changes in calorie and carbohydrate intakes early in the course of surgery-induced weight reduction. American Journal of Clinical Nutrition 94(2):450–458.
Davenport, D. L., E. S. Xenos, P. Hosokawa, J. Radford, W. G. Henderson, and E. D. Endean. 2009. The influence of body mass index obesity status on vascular surgery 30-day morbidity and mortality. Journal of Vascular Surgery 49(1):140–147, 147.e1.
Edwards, D. L., E. A. Frongillo Jr., B. A. Rauschenbach, and D. A. Roe. 1993. Homedelivered meals benefit the diabetic elderly. Journal of the American Dietetic Association 93(5):585–587.
ERS (Economic Research Service). 2004. Effects of Food Assistance and Nutrition Programs on Nutrition and Health: Volume 3, Literature Review. Washington, DC: ERS, USDA. http://www.ers.usda.gov/publications/fanrr19-3/fanrr19-3.pdf (accessed November 15, 2011).
Flegal, K. M., B. I. Graubard, D. F. Williamson, and M. H. Gail. 2007. Cause-specific excess deaths associated with underweight, overweight, and obesity. Journal of the American Medical Association 298(17):2028–2037.
FNS (Food and Nutrition Service). 2000. Guide to Measuring Household Food Security. Alexandria, VA: FNS, USDA. http://www.fns.usda.gov/fsec/files/fsguide.pdf (accessed November 15, 2011).
GAO (Government Accountability Office). 2011a. Nutrition Assistance: Additional Efficiencies Could Improve Services to Older Adults. Washington, DC: GAO. http://www.gao.gov/new.items/d11782t.pdf (accessed November 15, 2011).
GAO. 2011b. Older Americans Act: More Should Be Done to Measure the Extent of Unmet Need for Services. Washington, DC: GAO. http://www.gao.gov/new.items/d11237.pdf (accessed December 15, 2011).
GAO. 2011c. Opportunities to Reduce Potential Duplication in Government Programs, Save Tax Dollars, and Enhance Revenue. Washington, DC: GAO. http://www.gao.gov/new.items/d11318sp.pdf (accessed November 29, 2011).
Gollub, E. A., and D. O. Weddle. 2004. Improvements in nutritional intake and quality of life among frail homebound older adults receiving home-delivered breakfast and lunch. Journal of the American Dietetic Association 104(8):1227–1235.
HHS and USDA (U.S. Department of Health and Human Services and U.S. Department of Agriculture). 2010. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010. http://www.cnpp.usda.gov/Publications/DietaryGuidelines/2010/DGAC/Report/2010DGACReport-camera-ready-Jan11-11.pdf (accessed November 15, 2011).
Houston, D. K., B. J. Nicklas, J. Ding, T. B. Harris, F. A. Tylavsky, A. B. Newman, S. L. Jung, N. R. Sahyoun, M. Visser, and S. B. Kritchevsky. 2008. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: The Health, Aging, and Body Composition (Health ABC) study. American Journal of Clinical Nutrition 87(1):150–155.
Huffman, G. B. 2002. Evaluating and treating unintentional weight loss in the elderly. American Family Physician 65(4):640–650.
IOM (Institute of Medicine). 1997. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington, DC: National Academy Press.
IOM. 1998. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington, DC: National Academy Press.
IOM. 2000. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids. Washington, DC: National Academy Press.
IOM. 2001. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. Washington, DC: National Academy Press.
IOM. 2002/2005. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington, DC: The National Academies Press.
IOM. 2010. Strategies to Reduce Sodium Intake in the United States. Washington, DC: The National Academies Press.
IOM. 2011a. Child and Adult Care Food Program: Aligning Dietary Guidance for All. Washington, DC: The National Academies Press.
IOM. 2011b. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: The National Academies Press.
Jensen, G. L. 2005. Obesity and functional decline: Epidemiology and geriatric consequences. Clinics in Geriatric Medicine 21(4):677–687.
Jensen, G. L., and P. Y. Hsiao. 2010. Obesity in older adults: Relationship to functional limitation. Current Opinion in Clinical Nutrition and Metabolic Care 13(1):46–51.
Ledikwe, J. H., H. Smiciklas-Wright, D. C. Mitchell, G. L. Jensen, J. M. Friedmann, and C. D. Still. 2003. Nutritional risk assessment and obesity in rural older adults: A sex difference. American Journal of Clinical Nutrition 77(3):551–558.
Lee, B. J., L. Mackey-Bilaver, and M. Chin. 2006. Effects of WIC and Food Stamp Program Participation on Child Outcomes. In Contractor and Cooperator Report, 27. Washington, DC: ERS, USDA. http://ddr.nal.usda.gov/bitstream/10113/33688/1/CAT31012177.pdf (accessed November 15, 2011).
Lichtenstein, A. H., H. Rasmussen, W. W. Yu, S. R. Epstein, and R. M. Russell. 2008. Modified MyPyramid for older adults. Journal of Nutrition 138(1):5–11.
Mason, J. B., A. Dickstein, P. F. Jacques, P. Haggarty, J. Selhub, G. Dallal, and I. H. Rosenberg. 2007. A temporal association between folic acid fortification and an increase in colorectal cancer rates may be illuminating important biological principles: A hypothesis. Cancer Epidemiology Biomarkers and Prevention 16(7):1325–1329.
McMinn, J., C. Steel, and A. Bowman. 2011. Investigation and management of unintentional weight loss in older adults. British Medical Journal 342(7800):754–759.
Merete, C., L. M. Falcon, and K. L. Tucker. 2008. Vitamin B6 is associated with depressive symptomatology in Massachusetts elders. Journal of the American College of Nutrition 27(3):421–427.
Millen, B. E., J. C. Ohls, M. Ponza, and A. C. McCool. 2002. The Elderly Nutrition Program: An effective national framework for preventive nutrition interventions. Journal of the American Dietetic Association 102(2):234–240.
Miller, S. L., and R. R. Wolfe. 2008. The danger of weight loss in the elderly. Journal of Nutrition, Health and Aging 12(7):487–491.
Nagi, S. Z. 1976. An epidemiology of disability among adults in the United States. Milbank Memorial Fund Quarterly, Health and Society 54(4):439–467.
Newby, P. K., D. Muller, J. Hallfrisch, N. Qiao, R. Andres, and K. L. Tucker. 2003. Dietary patterns and changes in body mass index and waist circumference in adults. American Journal of Clinical Nutrition 77(6):1417–1425.
Ogden, C. L., S. Z. Yanovski, M. D. Carroll, and K. M. Flegal. 2007. The epidemiology of obesity. Gastroenterology 132(6):2087–2102.
Paddon-Jones, D., K. R. Short, W. W. Campbell, E. Volpi, and R. R. Wolfe. 2008. Role of dietary protein in the sarcopenia of aging. American Journal of Clinical Nutrition 87(5):1562S–1566S.
Saldeen, K., and T. Saldeen. 2005. Importance of tocopherols beyond α-tocopherol: Evidence from animal and human studies. Nutrition Research 25(10):877–889.
Shapses, S. A., and C. S. Riedt. 2006. Bone, body weight, and weight reduction: What are the concerns? Journal of Nutrition 136(6):1453–1456.
Sharkey, J. R. 2003. Risk and presence of food insufficiency are associated with low nutrient intakes and multimorbidity among homebound older women who receive home-delivered meals. Journal of Nutrition 133(11):3485–3491.
Sharkey, J. 2011. Nutrition screening at discharge and in the community. Presented at the Institute of Medicine Workshop on Nutrition and Healthy Aging in the Community. Washington DC, October 5–6.
Silver, H. J., M. S. Dietrich, and V. H. Castellanos. 2008. Increased energy density of the home-delivered lunch meal improves 24-hour nutrient intakes in older adults. Journal of the American Dietetic Association 108(12):2084–2089.
Stenholm, S., T. B. Harris, T. Rantanen, M. Visser, S. B. Kritchevsky, and L. Ferrucci. 2008. Sarcopenic obesity: Definition, cause and consequences. Current Opinion in Clinical Nutrition and Metabolic Care 11(6):693–700.
Stolzenberg-Solomon, R. Z., S. C. Chang, M. F. Leitzmann, K. A. Johnson, C. Johnson, S. S. Buys, R. N. Hoover, and R. G. Ziegler. 2006. Folate intake, alcohol use, and postmenopausal breast cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. American Journal of Clinical Nutrition 83(4):895–904.
Talegawkar, S. A., E. J. Johnson, T. C. Carithers, H. A. Taylor Jr., M. L. Bogle, and K. L. Tucker. 2008. Serum carotenoid and tocopherol concentrations vary by dietary pattern among African Americans. Journal of the American Dietetic Association 108(12):2013–2020.
Tucker, K. L., S. Rich, I. Rosenberg, P. Jacques, G. Dallal, P. W. F. Wilson, and J. Selhub. 2000. Plasma vitamin B-12 concentrations relate to intake source in the Framingham Offspring Study. American Journal of Clinical Nutrition 71(2):514–522.
U.S. Census Bureau. 2010. Poverty Thresholds 2009. http://www.census.gov/hhes/www/poverty/data/threshld/thresh09.html (accessed January 11, 2012).
U.S. Census Bureau. 2011a. Current Population Survey. http://www.census.gov/cps/ (accessed November 29, 2011).
U.S. Census Bureau. 2011b. Age and Sex Composition: 2010. Washington, DC: U.S. Census Bureau. http://www.census.gov/prod/cen2010/briefs/c2010br-03.pdf (accessed November 15, 2011).
Verbrugge, L. M., and A. M. Jette. 1994. The disablement process. Social Science and Medicine 38(1):1–14.
Villareal, D. T., M. Banks, C. Siener, D. R. Sinacore, and S. Klein. 2004. Physical frailty and body composition in obese elderly men and women. Obesity Research 12(6):913–920.
Villareal, D. T., M. Banks, D. R. Sinacore, C. Siener, and S. Klein. 2006a. Effect of weight loss and exercise on frailty in obese older adults. Archives of Internal Medicine 166(8):860–866.
Villareal, D. T., B. V. Miller III, M. Banks, L. Fontana, D. R. Sinacore, and S. Klein. 2006b. Effect of lifestyle intervention on metabolic coronary heart disease risk factors in obese older adults. American Journal of Clinical Nutrition 84(6):1317–1323.
Villareal, D. T., S. Chode, N. Parimi, D. R. Sinacore, T. Hilton, R. Armamento-Villareal, N. Napoli, C. Qualls, and K. Shah. 2011. Weight loss, exercise, or both and physical function in obese older adults. New England Journal of Medicine 364(13):1218–1229.
Zamboni, M., G. Mazzali, F. Fantin, A. Rossi, and V. Di Francesco. 2008. Sarcopenic obesity: A new category of obesity in the elderly. Nutrition, Metabolism and Cardiovascular Diseases 18(5):388–395.
Ziliak, J., and C. Gundersen. 2011. Food Insecurity Among Older Adults: Policy Brief. Washington, DC: AARP. http://drivetoendhunger.org/downloads/AARP_Hunger_Brief.pdf (accessed November 15, 2011).
Zoico, E., V. Di Francesco, J. M. Guralnik, G. Mazzali, A. Bortolani, S. Guariento, G. Sergi, O. Bosello, and M. Zamboni. 2004. Physical disability and muscular strength in relation to obesity and different body composition indexes in a sample of healthy elderly women. International Journal of Obesity 28(2):234–241.


































