
In considering the potential usefulness of information and communications technology (ICT) to violence prevention, speakers at the workshop explored the existing structures and processes within their respective fields and assessed any potential overlap between the two. These papers provide the beginnings of a foundation upon which this new integration can be built.
In the first paper, Cathryn Meurn presents a scan of existing ICT applications to violence prevention. Ms. Meurn explores the design and planning of interventions for various types of violence, the gaps that still exist in designing ICT-enhanced violence prevention interventions, and potential needs for monitoring and evaluation.
The second paper, by Mark L. Rosenberg and colleagues, examines the current status of violence prevention, including a discussion of the idea that violence prevention can be addressed from a public health perspective. This paper also addresses current obstacles and needs in violence prevention, and potential avenues for the inclusion of ICT.
In the third paper, Jody Ranck explores the current state of ICT and how ICT might meet the needs of public health and violence prevention now and in the future. He also discusses how ICT affects the means of data collection, program design, and community-based interventions, a situation that could pose both solutions and challenges for violence prevention practitioners.
In the final paper, William T. Riley describes current and potential evaluation methodologies for determining the success of ICT-enhanced interventions. After examining the gap between the time required to perform
traditional evaluations and the speed at which technology changes, Dr. Riley also suggests several adapted methodologies that might be better suited for rapidly changing environments.
THE ROLE OF INFORMATION AND COMMUNICATIONS TECHNOLOGIES IN VIOLENCE PREVENTION
Introduction
Violence is a global problem that crosses cultural and socioeconomic boundaries. From collective to interpersonal to self-inflicted violence, its impact on health is substantial. Violence is one of the leading causes of death worldwide for people between 15 and 44 years of age (WHO, 2002). However, the actual cost and extent to which violence occurs is difficult to measure. Countless violent acts happen out of public view in offices, homes, or even public institutions.
Violence can be prevented, and this assertion has been proven true within the field of public health. Action to prevent violence has been undertaken at various levels, from the local and community level to the international system. Methods have ranged from primary prevention, aiming to prevent a violent act before it occurs, to the tertiary level, which encompasses approaches that focus on long-term care.
The goal of this background paper is to provide a brief introduction to the current and potential role that ICTs can play in the reduction and prevention of violence. This paper by no means offers an extensive study on the intersection of ICTs and violence prevention. There are many ongoing projects, and a deeper landscape analysis is recommended. Furthermore, the use of ICTs in the field of public health is in its early stages. Much of the research cited in this paper can be classified as pilot projects, and, to date, there have been no in-depth measurements of their impacts. Therefore, this paper is intended to introduce the potential of the area and to encourage collective action going forward.
The Technology and the Debate
Technologies such as the smartphone, crowdsourcing tools, remote diagnostics, and other technological innovations have proliferated over the past decade, and many of them have shifted over to mainstream use. With this technological expansion, debate has also arisen concerning the positive and negative impacts that these innovations have within communities and worldwide.
ICT can be defined as a set of technological tools and resources used to communicate, create, disseminate, store, and manage information. These can include video, radio, television, Internet programs, social media platforms, and mobile phones. Distinctions are emerging between “old” and “new” forms of media and technology—that is, between the use of television, radio, and other forms of traditional media that have been employed for decades and newer forms of media, including social media and the mobile phone.
Particularly in the case of the developing world, the adoption of the mobile phone has created a new avenue for combating longstanding problems. With more than 5 billion mobile subscriptions worldwide, phone ownership has exploded. Two-thirds of these subscriptions are in developing countries, and it is predicted that soon 90 percent of the world’s population will be within the coverage of wireless networks. Furthermore, the number of unique users active on social networks is up nearly 30 percent globally, having risen from 244.2 million in 2009 to 314.5 million in 2010 as reported by the Nielsen Company (Grove, 2010). There are more than 800 million users on Facebook; Twitter is estimated to have more than 200 million users; and more video content is uploaded to YouTube in a 60-day period than three major U.S. television networks created in 60 years (Elliott, 2010). Teens are texting at record rates, and areas such as eLearning, remote diagnostics, and mServices are growing steadily.
Despite the hype, these various technologies are simply tools that can be used either for social good or for harm. The same was true for the invention of paper, the printing press, and the telephone, all of which changed the way in which we interact with each other. These innovations all had a positive impact on society, but these tools were also conduits for such negative things as yellow journalism and mass media campaigns against ethnic groups and certain minorities. It is also important to keep in mind that technology is only a small part of any solution.
Today, these new forms of communication and new technologies have led to some fantastic outcomes, as discussed in the next section. On the other hand, they have also elicited unintended adverse consequences in the pursuit of preventing and reducing violence. Trends in cyberbullying, losses in privacy and security, and stories of perpetrators targeting victims through social media sites—all of these must be kept in mind when we speak of using these tools for social good.
Program and Intervention Designs
Collective Violence
Collective violence is perhaps the most visible type of violence and often receives a high level of public and political attention. Whether arising from violent intrastate conflicts that account for the majority of conflicts today, from the flow of displaced persons, from acts of terrorism, or from genocide, the effects of such violence can be immense. Violent conflicts have profound health effects on civilian society via increased mortality, morbidity, and disability. The World Health Organization (WHO) defines collective violence as
the instrumental use of violence by people who identify themselves as a member of a group—whether this group is transitory or has a more permanent identity—against another group or set of individuals, in order to achieve political, economic or social objectives. (WHO, 2002)
With the rise of new media, and advances in and increased access to technology, opportunities exist to prevent some of this violence. One of the most popular types of programs using mobile phones is based on short message service (SMS) messaging, better known as text messages. The most frequent use of SMS has been the use of one-way messaging for educational awareness, such as in Amnesty International’s SMS urgent-action appeals campaign in the Netherlands. This campaign raised the awareness of torture victims through text campaigns and in turn enabled the agency to collect “signatures” when immediate action from supporters was necessary (New Tactics in Human Rights, n.d.).
One of the most cited cases of the use of SMS, which exemplified its potential beyond simple awareness campaigns, occurred during the 2007 Kenyan election. Although initial results indicated the opposition candidate Raila Odinga was in the lead, incumbent President Mwai Kibaki was announced as the official victor. Six weeks of violence ensued during which the influential role of mobiles became apparent. Through the Ushahidi platform, those with mobile phones were able to send texts to a specific number to report on human rights abuses and incidents, which were then mapped geographically on a website. This use of both texts and online tools not only enabled the reporting of events in real time but also aided the mobilization of groups to prevent further violent outbreaks (Harvard Humanitarian Initiative, 2011). Other examples of the use of the Ushahidi platform have been during the earthquake in Haiti and, more recently, in the protests in Egypt and the crisis in Libya (Ushahidi, 2011). Nevertheless, it is important to note that this mode of communication can also make it
cheap and easy for others to spread hateful messages to incite additional violence, as happened in Kenya.
Traditional types of ICT, such as phone networks, radio, and television, can also play important roles. Radio and television have been used in many forms since their invention. One project of note that used phone networks was devised by Interaction Belfast, which created a mobile phone network to prevent outbreaks of violence between warring neighborhoods in Belfast. Volunteers in both Protestant and Catholic communities were given mobile phones to enable communication with their counterparts when potentially violent crowds gathered or when rumors of violence started to spread, with the goal of resolving the issue peacefully.
Technologies provide not only increased communication but also increased accountability and transparency. The organization Witness works to use the power of video advocacy by documenting and sharing human rights abuses via cameras. By working with constituents to use video to shed light on certain atrocities, the organization has helped to shed light on the repression of ethnic minorities in Burma and has helped to prosecute recruiters of child soldiers in the Democratic Republic of the Congo.1 The organization’s training includes information on how to use video safely, which is important given the complexities to which this type of intervention can give rise.
An opportunity that deserves highlighting, particularly in the developing world, is the increasing role of the health worker. As task shifting continues to progress in these countries, community health workers can help to draw attention to indications of violence. With multiple programs now using these health workers for community outreach, data collection, and reporting via the use of ICTs and mobile phones, opportunities for leveraging technology for violence prevention exist.
Interpersonal Violence
Opportunities for leveraging technology exist with respect to interpersonal violence as well. This category includes sexual violence, intimate partner violence, elder abuse, youth violence, and child abuse.
Sexual violence Sexual violence is defined as “any sexual act, attempt to obtain a sexual act, unwanted sexual comments or advances, or acts to traffic, or otherwise directed, against a person’s sexuality using coercion” (WHO, 2002). Research suggests that at least one in four women in the United States has experienced sexual violence (National Center on Domestic and Sexual Violence, n.d.). Sexual violence is a universal problem, and it
__________________
1 For more information, see www.witness.org/about-us/witness-background.
can have deep impacts on both physical and mental health, including injury, stigma, and even death. One regularly noted aspect of this type of violence is the lack of information surrounding the magnitude of the problem. Data tend to be limited because many women do not report the violent act or seek medical services immediately afterward. Further complicating matters, data come from varying sectors, such as clinical settings, nongovernmental organizations, and the police.
SMS and geocoding can be applied to the prevention of interpersonal violence in much the same way that it has been applied to collective violence, as in the example of the aftermath of the election in Kenya. In Egypt, Medic:Mobile, a text messaging–based system, was used in combination with the Ushahidi platform in a project called Harassmap. In Egypt 83 percent of women are exposed to sexual harassment (Heatwole, 2010). The basic idea behind the program is that if a woman is sexually harassed she can send an SMS to the Harassmap number with corresponding details of the incident. This information will then be mapped on the website, allowing “hot-spots” of harassment to be identified. The project also provides help and information for victims (Heatwole, 2010). This program aims to help break through the silence that surrounds this issue.
Another program aiming to break through cultural barriers is the Mobile Cinema Foundation. This program travels to various soldiers’ camps in the Democratic Republic of the Congo and uses short films to expose soldiers to the consequences of rape. The goal is to educate the soldiers of the Congolese National Army through victim’s testimonies and discussions that are held after the viewing of the film. This form of digital storytelling can be a powerful tool both for empowering the victims and for educating offenders on the effects their actions can elicit.
Other programs are based on confidential hotlines, such as the National Sexual Assault Hotline in the United States, which victims can call for help. In a related use, in 2007 the International Organization for Migration partnered with Ukrainian mobile phone service providers to allow victims to dial a certain number to receive information and advice on migration and trafficking issues (Verclas, 2007).
Often it is an intimate partner that commits sexual violence, making sexual violence dovetail closely with intimate partner violence. Thus many interventions can help with both areas, including programs that promote gender equality, additional awareness campaigns, and microfinance programs and support networks for women.
Intimate partner violence Intimate partner violence is one of the most common forms of violence against women. This category refers to any “behavior within an intimate relationship that causes physical, psychological or sexual harm to those in the relationship” (WHO, 2002). Intimate
partner violence occurs throughout the world and crosses social, economic, and religious divisions. Women who are uneducated, low income, and lack support are most likely to fall victim to this behavior (WHO, 2002).
Conventional forms of technology and media have been used to prevent intimate partner violence. Examples include hotlines and awareness campaigns through both traditional and new media. Bell Bajao!, or Ring the Bell!, is an Indian program that provides a series of public service announcements urging men and boys to stand against domestic violence. The idea is that if one is hearing violence in progress, one should ring the bell and ask a simple question, such as “Can I borrow a cup of sugar?” It is likely the perpetrator recognizes that the person has heard the violence, which will interrupt the action. The organization also hosts a blog for victims to voice their experiences and access information and guidance (Bell Bajao!, n.d.).
In the United States the company Liz Claiborne initiated a Love Is Not Abuse program, which provides information and tools for men, women, and children (including teens) to learn more about the issue of domestic violence. In August 2011 it launched the Love Is Not Abuse iPhone application, which helps teach parents about teen dating abuse and demonstrates how technology, such as text messages, e-mails, and phone calls, can be conduits for committing abuse. Parents receive real-time communication that mimics the abusive and controlling behaviors teens might face in their relationships.2 This program illuminates the negative role technology can play.
On the other hand, texting can be a cheap and effective way to prevent intimate partner violence, as demonstrated by a case in Ohio in which a texting service allowed victims to report incidents silently via a simple SMS message and to make contact with a crisis intervention worker or the police without making an actual phone call. The total cost to set up the program, which used the Medic:Mobile platform, was about $380. FamilyFirst, as it was termed, processed between 6,000 to 8,000 texts per month during its first year and helped convict 18 abusers whose victims were able to report confidentially (Papillon, n.d.).
Technology can also play a role in helping to transform some of the underlying causes of intimate partner violence. Helping women gain access to both economic and societal support, such as is done through the Village Phone project by Grameen Phone Foundation, can lead to positive outcomes. The idea behind the Village Phone model is to provide a small loan and a “business in a box” to enable an aspiring entrepreneur to provide customers with access to a mobile phone and to sell mobile airtime. In March 2011, the program reports, 85 percent of the 6,876 entrepreneurs
__________________
who had been recruited into the network were women (Grameen Foundation, n.d.). This idea of women having access to a mobile device can also be found in the report Women & Mobile: A Global Opportunity, published in 2010. This report states that 9 out of every 10 women surveyed who had a mobile phone felt safer, and 85 percent felt more independent (Vital Wave Consulting, n.d.). With the rise of mobile payments and mobile money, or mFinance, and with increasing access to mobile devices, women are beginning to gain more economic independence in areas where they have traditionally been limited.
Finally, social support is important for women who have found themselves in domestic violence situations. In the developed world, such support may be derived from in-person working groups or community groups as well as from social media platforms and the Internet, which allow women to connect and share their experiences. In the developing world, however, mobile phones can play a unique role in garnering this type of support. In Senegal, the organizations Tostan and UNICEF launched the Jokko Initiative. Using SMS technology, the program allows community members to send out messages on various topics, including information on vital events, service announcements, and income-generating activities (Vital Wave Consulting, n.d.). This allows women the opportunity to promote their goods and to provide information about events they organize. Not only does this provide a chance for women to connect with each other and provide support, but also the program is also tied into Tostan’s literacy and math program.
Elder Abuse
Elder abuse has received the least public attention among the various forms of violence, having historically been defined as a “private matter.” Today it is seen as an important problem that is likely to grow because of the rise in aging populations in many countries (see Figure 6-1). Elder abuse can be “either an act of commission or of omission,” and it may be either intentional or unintentional (WHO, 2002). The elderly can experience violence physically, sexually, or psychologically, and they are also susceptible to economic abuse.
Again, the use of hotlines and the sharing of information via the Internet are integral to dealing with this type of violence. The National Center on Elder Abuse has state resources such as helplines and hotlines listed directly on its website in addition to listing where to report nursing home abuses and providing information about Adult Protective Services. There are also National Elder Abuse Awareness public service announcements that call attention to the issue.
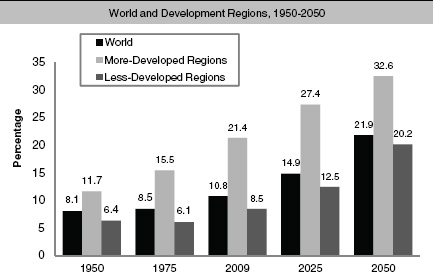
FIGURE 6-1 Percentage of population aged 60 or over.
SOURCE: United Nations, 2009.
Some sources state that a key prevention tactic could be the further use of intervention programs in hospital settings, which are currently lacking because of an absence of training in this area (WHO, 2002). Recently there has been an increase in the use of electronic checklists within the hospital setting concerning surgical procedures. Certain elements, such as signs and symptoms of abuse, could be integrated into these checklists. As tablets and electronic records become more common, a unique opportunity will appear to progress to a more holistic approach in health care. Furthermore, with the ability to train remotely, technology can be used to keep those in the health care industry abreast of the proper diagnosis of elder abuse and what to do about it.
The role of social media should also be mentioned. Social media platforms such as Facebook and Twitter, along with communications tools such as Skype, allow those traditionally cut off from the outside world to connect with both family and the wider community. According to a 2009 study by AARP, about one-third of people 75 or older live alone (Clifford, 2009). MyWay Village, a social network installed in nursing homes, allows residents to connect with new people and share their memories and experiences. Training sessions make it easy to pick up, and residents can send messages, play games, and, most important, not feel that they are isolated (Clifford, 2009).
Youth Violence
Youth violence is closely linked with other forms of violence, because youths who are exposed to other types of violence have an increased propensity toward committing violent acts themselves. Adolescents and young adults are often both victims and perpetrators of youth violence. The WHO says that violence involving youth greatly adds to the costs of welfare and health services, decreases productivity, and “undermines the fabric of society” (WHO, 2002).
Technology, particularly social media, is frequently thought to have a negative effect on youth. From online bullying to violent YouTube videos and video games, the various technologies are often cited as leading to increased violence among youth. The type of harassment that occurs through e-mail, instant messaging, and websites or via the mobile phone has even been given a name: “electronic aggression” (Hertz and David-Ferdon, 2008).
Regardless of the potential harm, youth are increasingly using social media, and there are ways in which it can be used positively. The increase in use of mobile phones by teens makes it possible to reach each one on an individual basis. A program in South Africa called loveLife launched a Web-based mobile program called MYMsta. This mobile social network allows the youth population to access information about HIV, employment opportunities, scholarships, and tips to improve their lives (Ngcobo, 2010). It also allows them to talk about concerns relating to sexual health and get responses from trained counselors.
loveLife employs other services to reach youth, such as its call-back service, which offers users free mobile connectivity to counselors. A user sends a message to the service saying, “Please call me,” and the automated system calls back and links the caller to a trained counselor.3 A similar program exists in the United States. The National Dating Abuse Helpline recently made its services available via text message by providing teens who text “loveis” to 77054 with help from trained peer advocates.4
In another effort to reach out to teens, particularly in cases of intimate partner violence or dating violence, Futures Without Violence developed the online campaign That’s Not Cool. The campaign encourages teenagers to decide for themselves what is okay and what is not okay in their relationships through the use of videos, interactive games, and an online forum for teens to share their stories and receive advice. That’s Not Cool recently launched an avatar application that lets teens create their own personalized mobile phone characters in response to animated videos addressing digital
__________________
3 See www.lovelife.org.za/what/call_me.php.
4 See www.loveisrespect.org.
dating abuse. Using text-to-speech technology, the character speaks the teen’s response, and the result is a speaking avatar video that can be posted and shared with peers on Facebook and Twitter.5
To deal with youth gangs, an innovative partnership involving the Chicago-based organization CeaseFire had been developed that combines science and street outreach to track where violence is heating up and to interrupt in order to calm the situation down. With Ushahidi, Medic:Mobile, and PopTech, the project PeaceTXT will look at how mobile tools, such as those used by other crisis-mapping organizations, and mobile messaging can accelerate CeaseFire’s existing success in decreasing deaths (Meier, 2010).
Child Abuse
Child abuse includes infanticide, mutilation, abandonment, and other forms of physical and sexual violence (WHO, 2002). It is a universal problem and often increases the likelihood of adverse health outcomes in adulthood. There is also a cultural aspect to child abuse because the standards and expectations of proper parenting can vary in different countries and societies. More often than not, the term “technology” combined with the idea of child abuse conjures up images of child pornography on the Internet and other negative ways in which recent innovations have harmed children. But technology also offers unique ways to prevent this type of abuse.
One underlying risk factor for a parent committing child abuse is a lack of education concerning a child’s development (WHO, 2002). There has been a recent rise in health text messaging programs geared toward reaching traditionally underserved groups with important health information. For instance, in the United States the Text4Baby program piloted by the Department of Health and Human Services (HHS) is a public–private partnership that provides pregnant women and new mothers with free health text messages. The messages range from tips on how to care for a baby to information on what to expect during pregnancy. Evaluations of the program are scheduled to be made available in 2013, and the model is already being taken abroad with interactive voice response technology, which relies on voice instead of text. Another text program that HHS is expected to roll out next year is Text4KidsHealth. The Health Resources and Services Administration (HRSA) will develop text messages on nutrition and physical activity to be used for future programs targeting the parents of children from 1 to 5 years of age (HHS, n.d.).
The mobile phone can act as a reporting tool for cases of child abuse. As seen with regard to collective violence, there is power is capturing
__________________
5 See www.loveisrespect.org.
images of typically ignored issues and bringing them to light in the mainstream media. Using one’s mobile phone in combination with community reporting is an easy way for stories to hit the Web that will be shared across masses of people through YouTube, blogs, and other social media channels (Nyirubugara, 2010). One can do a simple Google search online and find numerous online campaigns, blogs, and other videos calling for action and for attention to the issue of child abuse.
The traditional hotlines available to children, such as the National Child Abuse Hotline that is run via Childhelp, offer another approach to assistance and prevention. Childhelp also has information on its website to help children determine if they are being abused and what actions to take.6 Also, because health professionals play a key role in identifying any signs of child abuse in their patients, incorporating such identification as part of their training—or including information and prompts in the tools they use, such as checklists or reminders—could help prevent additional cases of abuse.
Self-Directed Violence
Violent acts that a person inflicts upon himself or herself are classified as self-directed violence. This includes both suicidal behavior and self-abuse. In the United States more than 35,000 people commit suicide every year, not including suicide attempts or self-abuse. Annually more than 1 million people attempt to take their own lives, and approximately 60 million Americans experience a mental health disorder, including post-traumatic stress disorder (PTSD) and depression, which can be risk factors for self-directed violence (National Alliance on Mental Health, 2010).
The WHO says that proper diagnosis of mental disorders is important, as is support for those who are contemplating destructive acts. Again, Telehelp lines and call centers are influential. Numerous lifelines, hopelines, and other crisis services are available. Opportunities now also exist for easy access to information and therapies online. The rise of online support groups also allows for those who are suffering to reach out and connect with others, which helps them understand that they are not alone. Awareness and access to services permits many to move past the social stigma often attached to depression and suicide.
There has been some debate over the creation and use of suicide prevention applications on mobile platforms. To have the applications verified and appropriate for the user, in addition to the possibility of producing any impact, is challenging. The QPR Institute released an Android app that turned the book The Tender Leaves of Hope: Helping Someone Survive
__________________
6 See www.childhelp.org.
a Suicide Crisis into a digital booklet in hopes of reaching more families and individuals.7 Some mobile applications let users track their moods and experiences, providing supplemental information for them as well as for their therapists. An app called “mobile therapy” has a “mood map” that pops up on a user’s screen that allows the user to indicate how he or she is feeling. The app responds by offering “therapeutic exercises” ranging from “breathing visualizations to progressive muscle relaxation” as well as ways to disengage from a stressful situation (Trudeau, 2010).
Again, there are risks involved. Technology and media are often blamed for suicide, particularly teen suicides related to cyberbullying. It is difficult to determine how great a role media and technology play in these deaths. Some instances become sensationalized, such as the 2008 case of a Florida teenager who posted online a live-stream video that showed his suicide, as he was encouraged by others he was chatting with online at the time (Friedman, 2008). With more than 87 percent of teens (ages 12 to 17) using the Internet and 19 million teens sharing their lives through text messages, this is definitely a cause for concern. As much as mobile phones, chat rooms, and other forms of communication can help teens work through their issues, they can also push teens in the opposite direction.
Overarching Gaps and Trends
From the program implementation cases above, several overarching gaps and trends begin to emerge, many similar to other fields using similar tools. In this section we will examine some of these gaps and what can be done about them.
Data Collection and Surveillance
A common problem in the field is the collection, analysis, and distribution of valid and useful data. As stated in the first WHO World Report on Violence and Health, countries around the world are at different stages of capacity for collecting data (WHO, 2002). There is a lack of quality and uniformity in the data. In addition, the problem of only knowing “the tip of the iceberg” remains, as research indicates many instances of violent acts remain unreported.
The use of ICTs can create certain efficiencies in data collection as well as improving its quality and associated information flows (Ranck, 2011a). Currently, in part because of the need for donor reporting, data collection is fragmented and siloed. Opportunities to increase the collection of and access to data and health information have increased, in large part because
__________________
7 See https://market.android.com/details?id=qprinstitute.crisis.
of the use of mobile phones in the developing world. Electronic capture of data can decrease human error and increase the speed of analysis.
Increasingly, people in the field of ICTs and their uses have been talking about the use of unique identifiers, such as biometric data, and the use of electronic health records to track patients has become increasingly commonplace. This type of data capture and storage can create better co-ordination across health systems and allow them to share data horizontally (Ranck, 2011a). Having access to broader data could lead to different actions and outcomes. Furthermore, the use of ICTs and mobile devices could aid health professionals, from doctors to community healthcare workers, in accessing and retrieving information.
EpiSurveyor and Commcare are examples of tools that have just started to be used in this area. EpiSurveyor allows anyone to create an account, design forms, and download the forms to a mobile phone in order to collect data for free. Commcare is free and open-source software that provides community healthcare workers with aid in case management through their mobile phones. The software contains registration forms, checklists, danger sign monitoring, and educational prompts and is designed to help manage the enrollment, support, and tracking of all of a community health worker’s clients and activities. The data that are collected are sent to the cloud for easy analysis and retrieval.
Another project, ChildCount+, is a platform designed and used by the Millennium Villages Project. ChildCount+ uses SMS to assist and coordinate the activities of community-based healthcare providers such as community health workers. These workers can use text messages to register patients and report on their health status. This information is sent to a central Web-based dashboard that can then provide a real-time view of the current status of the community.8 There are also numerous other software kits being used in the developing world, such as EpiInfo, OpenXdata, Open Data Kit, Open Dream, Open MRS, OpeneLIS, Open-Clinica, District Health Information System, Managing News, Sahana, Geo-Chat, Riff/Evolve, Mesh4x, Ushahidi, and Epidefender.
Research and Evaluation
Along with the needs listed above for data collection and surveillance, there is also a lack of common metrics for monitoring and evaluation, especially for programs using ICTs and mobile devices. There are serious insufficiencies in rigorous evaluation of the many pilot programs that are using these new mediums of communication and determining their overall impact.
__________________
8 See www.childcount.org.
A unique advantage of ICTs is that they offer the possibility of real-time evaluation. Furthermore, linking data from one program to others could lead to a clearer view of where the field is and where it is heading. This could have important effects. However, issues remain, including a lack of understanding of the capabilities around the use of ICTs, a lack of common data standards that support interoperability, and the need to develop information-sharing policies (Ranck, 2011a). Conversations concerning the “enterprise architecture”—the “plumbing” of systems—are in the early stages. We have yet to hit a point where projects are no longer functioning in siloes and where sharing data leads to a leveraging of each other’s results. “Interoperability,” or the ability to share data quickly and accurately across different application and through the health system, will be an important property to develop in the coming years if the full potential of ICTs and mobile devices is to be realized.
A final issue related to sharing data across silos is the problem of privacy and security. Concern about the ability of users to retain anonymity, especially given the nature of collective violence or intimate partner violence, is understandable, and such concerns should remain at the forefront of any project implementation. Data ownership is another issue that raises various concerns, particularly as projects strive for scale in implementation or begin to share data between programs or with the health system at large.
Dissemination and Implementation
ICTs can play a pivotal role in the implementation of violence prevention programs throughout the program and intervention design section. Multiple modes of telecommunications exist, but the mobile explosion both within and outside the United States provides additional opportunities for impact (see Figure 6-2). Common elements of program implementation can include the use of electronic forms and checklists, remote training for healthcare professionals, the use of crowdsourcing and social media platforms, and the use of SMS and video or television.
A larger issue remains, however, which is the exchange of information and lessons learned throughout not only the violence prevention community but also the public health field at large. Online platforms can aid in the dissemination and sharing of knowledge. Although not yet widely instituted, GHD Online and the mHealth Alliance’s Healthunbound platforms offer a peek into what is possible. With the rise of webinars and remote access to meetings, and with the ability to share presentations online through websites such as slideshare, avenues for information sharing and collaboration have increased.
Finally, institutions should not overlook these platforms for supporting their advocacy campaigns and their ability to raise funds for the
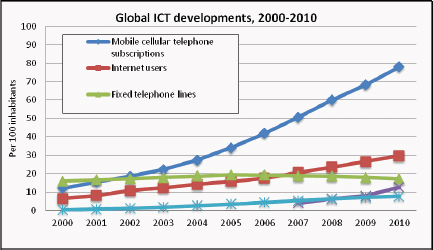
FIGURE 6-2 Global ICT developments, 2000–2010.
SOURCE: ITU, 2011.
implementation of programs. Multiple programs now use e-cards and online petitions or request advocates to share program information with their social networks. Text campaigns have become particularly popular over the past few years, allowing individuals to donate to certain causes via their mobile phones. Eight days after the earthquake in Haiti in 2011, the American Red Cross had raised approximately $22 million via text messaging (Heath, 2010). Donors texted the word “Haiti” to 90999, and a $10 pledge was automatically added to the person’s phone bill.
Recommendations
1. Undertake a full-landscape analysis of the use of ICTs in violence prevention.
Time and resources should be dedicated to a full-landscape analysis on the intersection between ICTs and the field of violence prevention, with particular emphasis on the mobile phone in relation to the developing world.
2. Learn from other fields and each other.
The mServices and mHealth spaces in particular have a lot to offer in terms of uses of new innovations and lessons learned. Conversations about the employment of electronic health records, interoperability, and the development of common metrics to evaluation are being explored. Furthermore, the types of violence outlined in this paper are interrelated
and interdependent in various ways. Using new platforms for information sharing and collaboration as well as sharing data and lessons learned could greatly push the field forward.
3. Develop common metrics for monitoring and evaluation.
With the ever-pressing need to know if these technologies are making a positive impact, the development of common metrics for monitoring and evaluation is important. With the ability for near real-time analysis of data, and given the infancy of this field, collaboration on metrics and the evaluation of programs will be vital for knowing what works and what does not.
4. Further explore privacy issues.
Given the sensitivities that surround certain types of violence, such as intimate partner violence, the need for anonymity is of utmost importance. Issues concerning user privacy, the sharing of data, reporting, and so forth need to be further explored. The technologies themselves must be investigated to make certain that they are not allowing sensitive information to be leaked to a wider public, for example via GIS mapping or forums on the Internet.
5. Address development factors—move beyond intervention.
Emphasis must be given to many of the underlying development factors that can lead to the instigation and continued perpetration of violence. Factors such as poverty, lack of access to the health care system, lack of access to education, and economic inequality can make any person or society ripe for violence. ICTs can be pivotal in addressing these issues, as with the use of mFinance to address poverty or with community health workers using computers or mobile phones to help expand access to health care and education.
THE STATE OF GLOBAL VIOLENCE PREVENTION:
PROGRESS AND CHALLENGES
Mark L. Rosenberg, M.D., M.P.P.
The Task Force for Global Health
Frances Henry, M.B.A.
Advisor, F. Felix Foundation
Alexander Butchart, Ph.D., M.A.
Department of Violence and Injury Prevention,
World Health Organization9
The field of global violence prevention has made some tremendous advances in the past 35 years. In some very important ways, however, it remains “stuck,” facing a number of serious obstacles, some that are generic for global health and others that are unique to the field of violence prevention. This paper sets the stage by describing some of these advances and then presenting the obstacles in order to explore whether ICT—including the new social media—can inspire ways to surmount these obstacles.
Perhaps the most important advance the field has made is to have helped people understand that violence is not inevitable, that it is not just an unavoidable aspect of daily life, and that it is not just one aspect of the existence of evil in this world. The importance of this advance can be seen in the story of smallpox, a disease that for centuries killed tens of millions of people every year. For many people, smallpox was seen as a recurring and unavoidable plague—until it became the first and the only human disease that has ever been eradicated (Foege, 2010). In 1806 President Thomas Jefferson wrote to congratulate Edward Jenner on his discovery that inoculating an individual with cowpox vaccine could confer immunity to smallpox. Jefferson told Jenner that within a few years his discovery would make smallpox a disease known only to history. It took a few more years than Jefferson thought. In 1973 Dr. Bill Foege was sent to India, where there were 87,000 cases of smallpox and the situation appeared quite hopeless. Foege shifted the strategy from mass immunization to the containment of outbreaks by vaccinating only those within or exposed to infected villages. This led to the eradication of smallpox in India and then the rest
__________________
9 One of the authors is a staff member of the World Health Organization. The authors alone are responsible for the views expressed in this publication, and they do not necessarily represent the decisions, policy, or views of the World Health Organization.
of the world. Smallpox eradication was the holy grail of global health, and this was an extraordinary achievement.
Sometimes tremendous leaps are made with a disruptive innovation; smallpox eradication was achieved when the containment strategy replaced mass immunization. The Swedish strategy for eliminating road traffic deaths was inspired by the eradication of smallpox. In Vision Zero, Claus Tingval put forward the idea that road traffic injuries are not “accidents”—not unpredictable and unpreventable acts of fate—but rather are very predictable and preventable events, and he suggested that we do not have to accept any number over zero. He was at first ridiculed for this idea, but now Sweden is well on its way to achieving this goal, and the European Union has adopted the Vision Zero goal for 2050. The idea that violence can be prevented is a similar sort of paradigm shift that can change the future.
The substantial changes that this paradigm shift brought about can be seen in the area of child sexual abuse. This was a problem to which the response used to be denial until it happened, and then perpetrators were sent to jail and victims to therapy. However, Fran Henry, through Stop It Now, helped to change the paradigm and demonstrated that identifying people at risk for perpetration and providing them help could actually prevent abuse from occurring. She made the case for prevention, and it has now become commonplace for the public to expect that preventive steps be taken. The failure to prevent child sexual abuse associated with the Catholic Church has provoked huge protests, and the most recent scandal involving a football coach at Penn State resulted in high-level firings. These are the results of a change in the paradigm—of a new and widespread belief that child sexual abuse can and must be prevented. Many believe that media attention to the Penn State case contributed to the response. This raises the possibility that change happens more quickly when the whole world is watching and suggests that ICT can help to spread the notion that violence is preventable and can accelerate positive change.
Significant Progress
Significant progress has been made in making it clear that violence is not “evil in the world” through the clarification of a definition of violence developed by the Centers for Disease Control and Prevention (CDC) and the WHO. The agencies have defined violence as “the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment, or deprivation” (WHO, 2002). The agencies have also helped to identify specific categories of violence: child maltreatment, intimate partner violence, youth violence, collective violence, sexual violence, elder abuse,
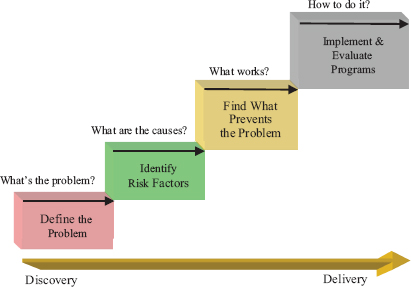
FIGURE 6-3 CDC Public Health Model.
SOURCE: CDC, 2008.
suicide, and self-directed violence. And they have helped to make substantial progress in each of these areas by asking and answering four questions: What is the problem? What are the causes? What works to prevent it? How do you do it? (Figure 6-3). We can see substantial progress has been made in answering each of these questions.
Progress Has Been Made in Achieving a Better Understanding of the Problem
We have developed a substantial science base ranging from knowledge generation (research) and knowledge integration to knowledge dissemination and knowledge application (delivery). We have demonstrated that the burden of violence is large and truly global; there are an estimated 1.5 million deaths each year, with more than 90 percent of the burden born by low- and middle-income countries. We also now understand that the burden of violence is exacerbated by its impact on other health and social problems. Exposure to violence increases the risk of mental health issues (e.g., depressions and anxiety) and physical health problems (e.g., diabetes, heart disease, and cancer) across the lifespan (Repetti et al., 2002). Exposure can also compromise cognitive development as well as the social development of communities and nations (WHO, 2008). Most important,
we have generated important knowledge about what works to prevent violence (Rosenberg et al., 2006; Mercy et al., 2008; WHO, 2010), although we have much to learn about how this can be applied in low- and middle-income countries.
We Also Have Made Progress in Understanding the Causes and Connections Among Different Types of Violence
There are identifiable risk factors and protective factors for each type of violence, many of which affect more than one type of violence, e.g., alcohol-related, child maltreatment, and exposure to violence (Rosenberg et al., 2006). We have learned that different types of violence are connected in many ways. A cycle of violence can begin, for example, with child neglect at birth, leading to hypervigilant children who are less likely to be calmed and more likely to participate in youth violence, and then intimate partner violence, elder abuse, and suicide when they get older.
We have a much better understanding of how to implement violence prevention programs and interventions. We have learned the value of collaboration among different sectors and disciplines, and we have seen the value that is added when police and public health, instead of fighting for control, work to collaborate effectively (Rosenberg et al., 2010). We have seen the important role that advocacy groups, often led by survivors, can play in program design and delivery. Advocacy groups have made substantial progress in many areas of violence prevention as they have expanded from treatment only to treatment and prevention, with prevention and treatment components working together rather than competing for funds. The place of public health in violence prevention has been well established, with the CDC and WHO providing leadership. The WHO has adapted the CDC model for use around the world. The organizations’ success is reflected in a substantial worldwide demand for technical assistance for violence prevention, with 44 countries around the world receiving WHO technical support as of September 2011 (A. Butchart, personal communication, 2011). The institutions that work in the field of violence prevention have also been strengthened: The WHO established a growing network of officially appointed Ministry of Health focal points for violence prevention, with a global total of more than 130 focal points in 2011.
The Challenges Before Us
But in some important ways we are still stuck. In fact, we are still stuck getting answers to the “four questions”:
1. What is the problem? There is much more work to do in overcoming the sense of fatalism that pervades so much of our thinking about violence, in countering the notion that violence is an inevitable part of human life and thus not preventable. We also need to overcome the separation of different types of violence into silos, so that researchers and practitioners in different fields of violence prevention can benefit from understanding the common roots and interconnections among different types of violence across the lifespan. We need more resources for a better understanding of the social and economic determinants of violence. One consequence of these root causes is that violence affects the most needy, poor, and vulnerable disproportionately but they do not set the spending priorities. There is still a need for more interdisciplinary collaboration. Many people still do not believe that violence is really a public health problem, but instead feel that it “belongs” to criminal justice. We need to overcome the “privacy ruse”—the belief that interpersonal or self-directed violence is a family affair and that what happens in the family (or nation) stays in the family (or nation). Stigma and shame keep people and countries from reporting many kinds of victimization, such as rape. Nations do not want to stigmatize themselves by saying they hurt their children, their women, their elderly, or themselves.
We are also hindered in our understanding of violence prevention because we use the wrong calculus to identify costs and benefits. Traditionally the biggest threats to our own health have been traditional infectious diseases, such as smallpox, polio, MDRTB, HIV/AIDS, and cholera. Most people do not realize that the well-known philosopher Martin Buber was really the first philosopher of surveillance. His work tells us that there are two types of surveillance. The first is “I and IT surveillance,” which follow the principle, “My country is at the center of the universe, and I relate to others only insofar as they contribute to my own little agendas or pose threats to my own health.” The second type of surveillance is “I and THOU” surveillance: “We flourish best when we treat others with respect, care, and equality. We add value to this global human endeavor by understanding the needs and contributing to the lives of others. We are compassionate” (Buber, 1923). The International Health Regulations look at I and IT surveillance, taking account only of those conditions that pose a direct threat to the security of other countries. But if we let this guide our efforts, then we fail to account for the costs to the people who suffer in the developing world from interpersonal and self-directed violence because this is not seen as contagious and importable into our own countries. Using “I and It” surveillance will mislead our efforts in formulating policy and setting our priorities if we fail to see that interpersonal violence is intimately connected to group violence and in the end it will pose a threat to our own security.
ICT may help facilitate “I and THOU” surveillance by contributing to the breakdown of the walls and borders that separate us as residents of
countries. They open whole new possibilities for conducting surveillance and open up the participation of many new groups and types of people to the process of surveillance, to analysis, and to the application of surveillance data.
2. What are the causes? Positive relationships are crucial for violence prevention. There is much more work to be done in understanding how to improve relationships and break the cycle of violence. Additionally, there is a particular risk that faces all of us: becoming disconnected while believing that we are becoming more connected. There is a risk that increased reliance on indirect communication methods such as cell phones and e-mail may diminish direct personal communications and thereby make it more likely that violence will be employed against someone whose face and persona are not known. Thus, we must also be cognizant of the limitations of these new technologies and realize that they may also be used to cause or facilitate violence.
3. What works to prevent it? Although much progress has been made in understanding what works to prevent violence, we lack sufficient proof of effectiveness for many interventions in low- and middle-income countries, and, without the proof of effectiveness, donors do not want to invest in preventive interventions. Ideally we should be able to provide a short list of specific interventions or “best buys” that have been proven to be effective and are ready for application in developing countries. However, few interventions have been implemented in developing countries with the capacity to evaluate the outcomes and collect the data needed to measure cost-effectiveness. This is a vicious cycle because without the necessary investment, we cannot develop the evaluation capacity needed to demonstrate effectiveness. The strongest case possible must therefore be made for investing in building the capacity to take interventions that have proven effective in developed countries and systematically implement and evaluate them in developing countries (WHO, 2008). What role can new information and communications technologies play in preventing violence in low- and middle-income countries? These technologies may enable us to accelerate progress in finding viable and effective strategies in low-resource environments.
4. How do you do it? One fundamental obstacle to progress is the absence of commitment by decision makers to enact solutions and try ideas. This field is markedly under-resourced. The consequences of this include an intense rivalry among organizations that compete for the same limited pool of dollars and a lack of resources to build the violence prevention foundations that, at a country level, are required to ensure that prevention activities are sustained over time. We need to overcome skepticism about the feasibility of delivering complex social interventions in resource-poor settings, and we struggle with the large time lag between prevention program delivery and reduced rates of violence for interventions such as parent
training and life skills training. Those working in global violence prevention also have to deal with the significant cost of preventive interventions. In the current economic climate, with increasing cut-backs in foreign aid, people want to stick with what we have already started (i.e., programs dealing with AIDS, tuberculosis, malaria, and infectious diseases) and not get into something that is new and therefore a lower priority. We also do not know how to reach out to high-risk groups. In addition, we have a lot to learn about scalability—we can do demonstration projects, but we have had little experience with scaling up programs that work. We also need to do a better job at integrating the different phases of the public health model. Ideally, surveillance, evaluation, and response would be closely linked. Instead, we collect the data, analyze it, and then 3 years later perhaps it is applied or used. We have not developed the capacity to implement solutions to overcome the many bottlenecks that occur here. This is a universal problem for global health and one where ICT may be of great help.
INFORMATION AND COMMUNICATIONS TECHNOLOGIES
AND THE FUTURE OF GLOBAL HEALTH
Jody Ranck, Dr.P.H.
Public Health Institute
Introduction
The past decade has witnessed a remarkable and truly global technology revolution unlike virtually any other. The mobile phone has placed more computing power in the hands of more people than even telecommunications experts in the 1980s thought would be possible. An executive from AT&T predicted that the global market for cell phones would peak at approximately 100,000. But by the end of 2011, according to the International Telecommunications Union, almost 6 billion people had access to mobile phones (ITU, 2011). The average smartphone today contains more computing power than all of NASA’s computing resources at the time the first man was sent to the moon. Social media is an important driver of this growth.
In contrast to most public health practitioners’ perspectives, Africa is one of the fastest-growing markets for Facebook. In fact, Facebook is becoming an important driver of Internet growth in Africa, because it has now become the leading site visited by Internet users on the African continent (Jidenma, 2011). Although Africa has become the continent with the fastest growth in Facebook use, there are important disparities in access and growth rates. Nevertheless, the developing world has rapidly become a major focus of the marketing departments of most major social media
platforms, such as Twitter, Facebook, and Google. The role that these platforms played in the Arab Spring of 2011 can certainly be overstated, but there is little denying that access to social media platforms that are essentially many-to-many self-publishing platforms, mostly accessible by mobile phones, is having a major impact on the way ideas are communicated, new knowledge is generated, and, as we will soon see, new research on the understanding of human behavior is being conducted.
Global health experts can no longer afford to view social media as trivial playthings of adolescents. These are major platforms with which to engage the public and to innovate in areas such as civic engagement, public policy, and technology development, and they are transforming the way we think about education, technology development, the media, politics, social movements, and science. These are all critical dimensions of public health, more largely, and for developing the next generation of global violence prevention tools and policies.
In this paper I will outline some of the most important technological innovations involving the mobile and social media platforms and provide some preliminary examples of the key lessons and impacts that these tools have had. There have been many early research studies on mHealth and social media tools, but these often suffer from small sample sizes and various other methodological shortcomings, so there are relatively few robust evaluations of the technologies (Mechael et al., 2010). In the discussion that follows, I will focus on innovations in mHealth and social media and how these have created the enabling conditions for open data, crowdsourcing, citizen science, new visual cultures and advocacy, the gamification of health, and open innovation, all of which can lead to a new approach called “open health.” I will conclude with some observations on how these may lead to new strategies for global violence prevention efforts.
Social Media: Amplifying the Self and New Forms of Cooperation
Since the early 2000s, social media tools have grown dramatically in use and scope, becoming mainstream communications tools that have helped foster what some have termed “new economies and cultures of sharing.” From Flickr to Facebook, the demographics of the adoption of these tools have grown in unexpected ways, and they have become important, if not central tools, for companies, nongovernmental organizations, and governments to share information and communicate. Early on, platforms such as Flickr proved to be virtual spaces where acts of resistance to gender norms could be acted out by youth; for example, in the Arabian Gulf states, where public spaces are strictly segregated by gender, teenagers used Flickr as a space for interacting across gender lines. Such examples illustrate how the use of many-to-many communications platforms can take on distinctly
political tones. The Arab Spring was just one of many instances in recent history in which mobile devices and social media were used to amplify voices of dissent and tell compelling oppositional narratives in public life. The Orange Revolution in the Ukraine and the toppling of Philippine president Joseph Estrada are further examples of the use of SMS or text messaging to coordinate resistance movements or what Howard Rheingold has termed “smart mobs” (Rheingold, 2003).
In January 2008 one of the most powerful examples of the use of social media and mobile devices and of the new forms of cooperation that they entail occurred. During the Kenyan electoral violence, bloggers critical of the national government’s media blackout created an open-source platform for crowdsourcing information about both violence and counter-violence via SMS messages that could be mapped on the platform called Ushahidi (Swahili for “Testimony” or “Witness”). Blogger Ory Okolloh suggested the need for a platform for information gathering, and a network of bloggers created the site in approximately 1 week. Incidents could be reported via mobile devices using a short code and were then verified by local groups on the ground and mapped in order to provide a visualization of the violence. Today this platform is used globally from Russia to Washington, DC, by groups involved in a variety of humanitarian and human rights issues. In its wake, a number of similar tools have been developed to raise awareness of gender harassment in Egypt (HarassMap) and violence against girls; in one example, a reporting tool similar to Ushahidi was even merged with open data initiatives in order to map murder rates (Evans, 2011). Social media have been a major driver in the move toward greater transparency and in the growing area of open data initiatives that have taken place in a number of formerly closed institutions, such as the World Bank.
Such examples point to the sorts of roles that the phenomenon of crowdsourcing that has arisen from the social media landscape can play in global health. Several years ago the pharmaceutical giant Eli Lilly launched an open innovation platform called InnoCentive to tackle difficult-to-solve scientific problems. The firm, after spending millions of dollars and many person-years without solving specific problems, began to reach beyond its own walls and disciplines to find assistance in solving these challenges. It placed problems on the site, which allowed potential solution finders to register and submit approaches to solving the problems. Frequently the company discovered to its surprise that the problems were easily solved by scientists halfway around the world who approached the problem through a different paradigm or discipline that made the challenge quite easy to solve. The success of InnoCentive has unleashed a wave of platforms and strategies to drive innovation and solve difficult scientific and health challenges by recognizing that our traditional forms of knowledge creation have not necessarily kept up with the technologies and new forms of sociality
that they engender. A new science of asking questions has arisen, and platforms are now being used to “micro-task” problems and work into smaller pieces that can be easily solved, often providing income to micro-taskers using platforms such as Amazon’s Mechanical Turk or the developing world platform, Jana. An example of such work that has taken place in developing countries is the group of Trinidadian and Brazilian students who developed a micro-tasking tool for performing medical diagnostics of digitized X-rays on mobile phones that users would scan for eye conditions; this was the winner of InfoDev’s microwork challenge, “m2work” (InfoDev, 2012).
Cooperation and the Commons
Elinor Ostrom won the 2009 Nobel Prize in economics for her path-breaking work on the commons and the strategies and tools used to manage the commons in the area of natural resources. Her work is all the more salient in our new world of ICT, because the examples demonstrate the power of the tools of cooperation. The commons can become an invaluable companion to these tools through creating a basis for shared resources. From open-source software to innovation commons such as the Science Commons or public goods such as health, we see a growing movement to deploy commons-based assets alongside the tools of cooperation in order to drive innovation and problem solving. As much of the world enters a period of prolonged financial crises, global health experts will need to become more literate and skilled in strategies for commons-based approaches that rest on an economics of sharing that can be disruptive to traditional approaches. In the biological sciences we have examples such as the ProteomeCommons, which involves protocols for sharing terabytes of data over the Web (Weinberger, 2012).
mHealth and Public Health 2.0
The near-ubiquity of cell phones in most low- and middle-income countries has created an unprecedented opportunity to extend the reach of community health workers as well as to provide a channel for public health messages and two-way communications. Mobile devices are increasingly playing an important role in data collection with open-source tools such as DataDyne’s Epi-Surveyor or INSTEDD’s Geochat, which enable the creation of forms and the transmission of data. The Praekelt Foundation and organizations such as Cell Life in South Africa have pioneered the use of SMS for HIV prevention, testing, and drug-adherence regimens. Beyond texting, there are new tools for eye exams, infectious diseases, vital signs measurement, and microscopy that are in various stages of development and that will be able to take advantage of the augmented computing power
of smartphones. Smartphones are coming down in price as well, as exemplified by the $80 offering that HTC has developed for the Kenyan market. In countries such as Kenya and the Philippines, where the mobile industry has made extensive inroads, there are new possibilities for mHealth to piggy back on the mobile industry to enable micro-insurance schemes, such as the one by Changamka aimed at enabling pregnant women to cover antenatal care, child delivery, and postnatal care. These systems can also be extended to vouchers for supplementary feeding, cash incentives, and the payment of health workers (Gencer and Ranck, 2011).
Beyond mobile devices, the broader social media system is increasingly playing a public health role in the areas of epidemiology, participatory planning, and biosurveillance. Public Health 2.0 offers a new paradigm that democratizes the way science is practiced. In February 2011 a mysterious fever appeared among participants at the DomainFest Global Conference (Garrity, 2011). One of the attendees used Facebook to reach out to other participants to inquire about their symptoms. Within a few days, before the Los Angeles County health department and the Centers for Disease Control and Prevention had even launched an investigation, the participants had diagnosed the outbreak themselves as legionellosis and had entered the diagnosis on Wikipedia. HealthMap and Google’s Flu Tracker, along with Twitter, are some of the more robust mapping/crowdsourcing tools that are becoming increasingly prevalent in public health science and practice. Rumi Chanara of Harvard used Twitter to track the 2010 cholera outbreak in Haiti (Chunara et al., 2012). These platforms are in essence large repositories of data which new data-mining tools can use that to make sense of much faster than is possible with traditional methods.
Big Data and Data Mining
Given the proliferation of mobile devices and data-collection devices, particularly with the emerging Internet of things including the billions of devices that can collect data and send them to the Internet, the major challenge has been to make sense of all of this data (Ranck, 2011b). The combination of cloud computing and big-data analytical tools such as Hadoop has enabled data scientists to take vast volumes of data, too big to fit on the typical server, and parse these data very rapidly. Tools such as IBM’s Watson can now scan several hundred million pages of medical text in seconds or fractions of a second. These tools are capable of sorting through hundreds of millions of tweets and making sense out of this chaos, often at a much lower price than conventional approaches. Such tools have already been used to analyze data about violence, such as shootings in Camden, New Jersey. Jeffry Brenner used big-data analytics to sort through 8 years of medical billing records and to discover that 80 percent
of costs were associated with 13 percent of patients, and that much of the care was neither medically effective nor cost-effective. This discovery created the foundation for a new partnership to address violence prevention efforts. Another research effort, this one carried out by Harvard University researchers, uncovered indicators of risks of domestic violence in patients’ electronic medical records that may help clinicians identify early risk factors that can prompt earlier interventions (Joelving, 2009).
Gamification
A final area where social media and ICTs can play a role in the future of global health is gaming. Gamification refers to the deployment of gaming tools, incentives, and technologies within the worlds of business, research, creativity, and innovation. In 2011 a major breakthrough in the area of HIV research came to light through the success of the online research and gaming platform Fold.it (Marshall and Nature, 2012). Researchers from the University of Washington created an online game that allowed users to manipulate three-dimensional structures of proteins on their home computers, which were then scored for the best (lowest-energy) configurations of the enzyme critical to some HIV drug therapies. For several years bench scientists had failed to come up with better configurations and thus had sought to crowdsource alternatives. Within several weeks amateur gamers had solved a problem that had plagued these scientists for years. There is growing use of games such as this designed for mobile devices to use the incentives and critical thinking fostered by game dynamics in order to encourage public participation in citizen science or behavioral change (Fogg, 2002; Bogost, 2010).
ICTs and Global Violence Prevention: Lessons
for the Future of Global Health
In this paper I have outlined some of the key technology trends that are likely to play a significant role in general public health efforts in the future. Although many of the examples are from developed countries, we are seeing a dramatic growth of these tools for global health efforts. Some of the tools have been developed with violence prevention efforts in mind, but the violence prevention arena lags significantly and could explore these tools in more detail. For example, the United Nations Global Pulse platform is a big-data project that seeks to stimulate data philanthropy, sharing, and analytics in order to predict political crises much earlier through finely tuned analyses of the “data exhaust” from media, NGOs, evaluations, and so forth. A number of mapping tools for visualizing violence against women exist, such as HarassMap and Map4Aid’s Fighting Violence Against
Women in India campaign, and text messaging is being used for a number of campaigns aimed at preventing domestic violence and violence against women. Take Back the Tech! is an effort mobilized during the 16 Days of Activism Against Gender-Based Violence that has developed various innovations in the use of SMS for public awareness campaigns.
Although the field is in its nascent stages, the time is ripe to begin building the evidence base for these tools and the lessons learned, with particular attention paid to the various cultural contexts. For example, some SMS campaigns to prevent domestic violence have actually backfired in some contexts because of the particular power and gender dynamics at the household level. This is an important element that often gets overlooked in the rush to deploy technologies, and it will be critical for the field to have more case studies seen through the prism of gender and power as it moves forward. Furthermore, the same technologies used for interventions can also help in evaluating these technologies. Data-collection tools used for health and human rights, such as the KoBo Project (KoboProject.org), provide open-source data-collection tools that also offer the encryption functionality that can protect users in conflict or human rights situations while also building the capacity of local organizations. Directories of these tools and case studies are in great need at the moment. Furthermore, the public health field itself can no longer afford to fall behind in its thinking about technology. Increasingly one’s ability to realize one’s capabilities, in the sense articulated by Amartya Sen, will require technological literacy that many in our field do not have. This emerging notion of technological citizenship (Barry, 2001) is likely to play a determining role in the social divides of the future as well as in the growing one within public health ranks, where new techno-political thinking is desperately needed.
William T. Riley, Ph.D.
National Heart, Lung, and Blood Institute, National Institutes of Health
The past decade has witnessed an explosion of mobile technologies. Eighty-three percent of U.S. adults own cell phones (Pew Internet and American Life Project, 2010). Worldwide there are approximately 6 billion cell phone subscriptions, and the rapidly growing rates in developing countries, where wireless technologies have leapfrogged the wired infrastructure, have made it possible to reach people in remote villages and communities (ITU, 2011). The public health community has begun to leverage these mobile devices in order to perform real-time assessments and to intervene at the times when these interventions would be most useful (e.g., in the context of the behavior).
Despite the rapid growth of mobile technologies applied to health (mHealth), the evaluation of mobile technologies has not kept pace with the development and deployment of these technologies. Although there also needs to be considerable emphasis on the reliability, validity, and sensitivity of measurements in mHealth, the focus of this summary is on research evaluations of mHealth interventions.
Randomized Controlled Trials
The randomized controlled trial (RCT) is the standard for intervention research. Meta-analyses such as those performed by the Cochrane Review routinely include only RCTs in their reviews (Higgins, 2011). The U.S. Preventive Services Task Force (USPSTF) recommendations are developed predominately from the findings of RCTs (USPSTF, 2010). The Institute of Medicine relies heavily on RCTs as the basis for its consensus reports (IOM, 2011). Given the reliance on RCTs as the accepted standard for biomedical and behavioral evidence, mHealth interventions, including violence prevention programs delivered via mobile devices, need to be subjected to this same standard if they are to be accepted as a valid and effective method.
Appropriate Comparison Conditions in mHealth
One challenge of evaluating the efficacy of mobile interventions via RCTs is the choice of a comparison condition. How the mHealth intervention is intended to be used is an important consideration for determining an appropriate comparison condition. If the mHealth intervention fills a gap where no other viable intervention exists, then a no-treatment or usual care condition is appropriate. If the mHealth intervention is intended to augment an existing intervention, then an additive design in which the existing intervention is compared to the existing intervention plus the mHealth intervention would be used. If the mHealth intervention is intended to supplant or replace an existing low-tech equivalent interventions, then the low-tech intervention may be the appropriate comparison condition.
The comparison condition in which the mHealth intervention is intended to augment or supplant the existing intervention is a high outcome standard to exceed. One solution to this dilemma is to use or develop a minimal-contact version of the low-tech intervention (e.g., a self-help book or non-interactive Web pages) as the comparison condition, but this dilutes the effect of the low-tech intervention and often delivers it in a form that was never intended. Therefore, it becomes critical to ask in what way the mobile intervention is hypothesized to be better than the other interventions currently available. In many cases, it may not be the case that the mobile intervention is expected to produce better outcomes, but rather that it is
expected to provide comparable outcomes while delivering the intervention either more consistently across individuals (e.g., with less variability in outcomes) or at less cost. For many mobile health applications, the hypothesis should not be that the mobile intervention will produce better outcomes than its low-tech equivalent, but rather that it will produce comparable outcomes at a lower cost. As a result, a cost-per-unit change is often a better indicator of mHealth intervention outcomes. Furthermore, because most mobile or other technology intervention costs are fixed (e.g., initial development and equipment) while most of the low-tech intervention costs are variable (e.g., professional time), extrapolating cost-per-unit changes across large numbers of individuals, not just those in the study, gives a better estimate of the reach possible from the high- vs. low-tech intervention.
Technology Outpacing RCTs
A more substantive issue regarding the fit of RCTs and mobile health interventions is the length of time required to perform an RCT. Previous research has shown that the median time from start of enrollment to publication is 5.5 years and substantially longer for negative trials (Ioannidis, 1998). From the initiation of a grant submission, an RCT can be expected to take 7 or more years to complete, a timeframe that does not keep pace with recent technological advances. As shown in Figure 6-4, an RCT with the primary results published at the end of 2011 would have required developing the initial project idea and submitting the grant application by 2005, prior to the advent of many Internet, mobile, and wireless advances, including YouTube, iPhone, Android, and iPad. As a result, most of the
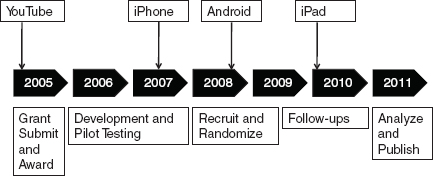
FIGURE 6-4 Mobile technology advances outpace traditional research design. SOURCE: Riley, 2011.
mobile health research published today was developed on dated technologies and mobile platforms.
Fortunately, mobile technologies can be used not only to provide interventions but also to streamline the RCT process. Mobile technologies can be used to recruit participants rapidly and to conduct the trial remotely. In one of the first uses of mobile phones for smoking cessation, Rodgers et al. (2005) recruited participants and conducted the study remotely across the continent of Australia. By being able to recruit with a text message to all mobile phone users and to conduct the study remotely, the researchers were able to make the study convenient for participants (e.g., no travel for in-person visits) and to reduce study costs (e.g., fewer research staff and facilities were required). This remote study capability is based in part on leveraging the mobile phone to deliver not only the intervention but also the study outcome measures. The frequent longitudinal assessments and the automated reminder prompts to complete the study assessments also potentially reduce missing data and the number of participants needed to find the hypothesized effect. The value of technology in streamlining the RCT process and performing remote RCTs has extended beyond those doing mobile interventions. Pfizer’s REMOTE trial uses technology to evaluate medication for overactive bladder disorder without requiring the patient to visit a health clinic (Pharmacy Times, 2009). As a result, not only will Pfizer be able to perform this RCT faster and at less cost, but also it will be able to include patients who would otherwise not be able to participate.
By leveraging the capabilities of mobile technologies to streamline RCTs and by selecting the appropriate control condition and outcomes for comparison, RCTs can be conducted on mHealth interventions. RCTs, however, are not the only method—or even the most appropriate method in some cases—for evaluating mHealth interventions. The remainder of this paper discusses alternative methodologies that can be used to evaluate the development and dissemination of an mHealth intervention.
Evaluating While Developing mHealth Interventions
Evaluation During Development
The empirical evaluation of mobile health interventions should be integrated throughout the development process. The initial design and content should be based on theory and on prior empirical literature on the effectiveness of various interventions for the target problem (Riley et al., 2011). Because mobile technologies can deliver some intervention components better than others, an in-depth understanding of the mechanisms or components of an intervention and their relative contribution to intervention effectiveness is critical to mobile health intervention development. In addition to
its theoretical and empirical underpinnings, the core of the software development process is iterative and incremental development (Larman and Basili, 2003), which utilizes qualitative methodologies to obtain user input throughout the development process. A range of qualitative methods, both from health informatics (Borycki et al., 2011) and from violence research (e.g., Testa et al., 2011), can be used to elicit end-user perspectives on the usability and functionality of various design features during the development process.
Prototype Evaluations
As prototypes or components of the mHealth intervention are developed and tested (e.g., debugged), a number of research methodologies are available to evaluate efficacy prior to any full-scale RCT. These preliminary evaluations are particularly important for newly developed mHealth interventions in order to insure that the interventions have been optimized before subjecting them to an RCT. Although a single-arm pre-post pilot trial with a small sample is commonly used to determine if the mHealth intervention produces a significant change and to test the procedures for a subsequent RCT, this design may not provide the flexibility needed to test and further optimize the intervention before subjecting it to an RCT.
N-of-1 designs Instead of testing a group of participants pre- and post-trial, detailed testing of individuals longitudinally throughout the intervention period (AB) provides the development team with important information on how the intervention is used by each user and the effect on the target problem during the intervention. By staggering these N-of-1 trials, mHealth developers can detect potential improvements after a few users have been evaluated, modify the program, and then test the new version on the next N-of-1 users. (See Lillie et al., 2011, for a review of N-of-1 trials in personalized medicine and utilizing wireless and mobile devices for N-of-1 trials.)
To increase the internal validity of these N-of-1 studies, reversal and interrupted time series designs can be considered. When the effects of the intervention are expected to quickly dissipate once the intervention is withdrawn, a reversal design (ABA) can be considered. Although the improvement in the target behavior from baseline (A) to intervention (B) can be the result of a number of confounders, many of these confounders can be eliminated from consideration if the individual returns to baseline levels of the target behavior after the intervention has been withdrawn (A).
If the intervention is expected to have an enduring effect after the intervention is withdrawn (or if the intervention continues for as long as the user wants to use it), then an interrupted time series design can be considered (Biglan et al., 2000). This design is essentially an AB design, but the baseline
values are used to predict future values of the outcome variable. If after the intervention is introduced, the values for the target problem exceed what would have been predicted from baseline, then it is reasonable to conclude that the intervention produced this effect. Of course, extraneous variable outside of the researcher’s control (e.g., a significant life event) could also have produced this effect, but such confounders can be minimized by staggering the initiation of the intervention across multiple users. If the improvement is seen for each user following interventions that are initiated at different times for different individuals, then the causal inference is stronger.
N-of-1 designs were commonly used in early behavioral intervention research and are still used regularly in many applied behavior analysis settings (e.g., developmental disabilities). The challenge with these designs is the frequent outcome assessments required to establish a stable baseline and to determine if the intervention affects the subsequent assessments. Mobile health interventions, however, are uniquely suited to generate the frequent longitudinal assessments needed to conduct these various N-of-1 designs. For example, an mHealth intervention is likely to have some specified baseline period (e.g., 7 days) and can be designed to continue the baseline period until a stable baseline has been achieved. The mHealth intervention can then introduce the intervention and continue frequent assessments and fully automate these N-of-1 designs so that every user of the mHealth intervention also contributes efficacy data.
Intervention optimization designs Even with a solid empirical basis, the development of mobile health interventions still involves guesswork. Which components should get a higher or lower dose in the mHealth intervention? Which modality would be best for delivering a specific intervention component? Should all of the intervention components be delivered simultaneously or in some pre-specified order? To address these questions, there are a number of intervention optimization design issues to consider. For N-of-1 designs, systems modeling, such as control systems engineering modeling, can be used to test the model (Rivera et al., 2007). For example, if the intervention model indicates that an intervention to identify potential violence or victimization will result in the avoidance of these situations and thereby reduce violence, the process of this change can be assessed and modeled. The intervention can then be revised based on how well the model fits.
Group-level randomized optimization designs include factorial, fractional factorial, and sequential multiple assignment randomized trials (SMARTs) (Collins et al., 2007). Fractional factorial designs mix and match the various intervention components and modes of delivery that need to be evaluated and determine which components in which combination produce the largest effect. SMART designs are similar in analysis but isolate the sequence of the components according to various considerations. For
example, if a user responds well to the first phase of the intervention, what should be the next phase? If the user responds poorly, should the first phase be repeated or should the user move on to a different phase of treatment, and, if so, which one? These optimization designs take time and resources to conduct, but they are important to consider before subjecting an intervention to a standard two-arm RCT, especially if considerable questions about how best to deliver the various components of the intervention remain.
Evaluating While Disseminating
Although an RCT to establish the efficacy of an mHealth intervention in a controlled study is an important step to take before disseminating and implementing the intervention, it is not always feasible to conduct an RCT. There may, for example, be inadequate resources to conduct an RCT, or the mHealth intervention may have been developed for a pressing public health need and the intervention needs to be deployed immediately. The organization employing the mHealth intervention may not want a random selection of those it serves to not receive the intervention. In these cases, the mHealth intervention should, at the very least, have been developed empirically and evaluated on some small scale (e.g., pilot or N-of-1) before implementation. There are, however, a number of designs that can be employed to evaluate the intervention while it is being disseminated and implemented. Many of these designs have been used in community-based interventions in which it is impractical to randomize communities to an intervention.
The same interrupted time series design described above for single subject users can be used for groups. The community or setting in which the intervention is being implemented is evaluated recurrently to obtain a stable baseline. This stable baseline can come from routinely collected public health data, but it can also be generated via the mHealth intervention itself by incorporating a baseline assessment prior to intervention initiation. Once the baseline is established, the intervention can be implemented with continued assessment to determine if the intervention is associated with a significant change in the outcome variable.
For example, if a community-based youth violence prevention program (e.g., Vivolo et al., 2011) incorporated a mobile or wireless intervention component, then the addition of this component could be evaluated in a single community by monitoring the relevant outcomes over time before and after the addition of the mobile or wireless component. An illustration of an interrupted time series design applied to a technological solution (radio-frequency identification, or RFID) for improving workflow and reducing hospital service wait times is shown in Figure 6-5. By tracking wait times for weeks before and after the implementation of the RFID
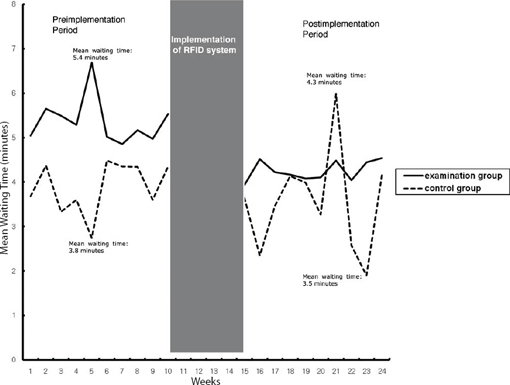
FIGURE 6-5 Interrupted time series example.
SOURCE: Kim et al., 2010.
system, Kim and colleagues (2010) were able to show that wait times were significantly reduced. Greater confidence in the causal inference from this design can obtained by using a matched control (e.g., a health service that did not receive the intervention, as shown in Figure 6-5), by staggering the intervention across communities, or by applying propensity-score weightings (Linden and Adams, 2011). Given that an RCT is often not feasible for community, hospital, or school-based interventions, the interrupted time series design provides a quasi-experimental alternative that requires only one (or slightly more than one) community for evaluation.
The stepped-wedge design rolls out the intervention in a staggered or sequential manner to individuals or clusters of individuals over a number of assessment periods (see Figure 6-6, adapted from Brown and Lilford, 2006, for a graphical representation of this design). This design is particularly appropriate if there are well defined cohorts (i.e., communities), all of whom should receive the intervention for ethical reasons, and especially if there are insufficient resources to introduce the intervention to all of the groups at once. The groups are defined a priori and randomized as to when they will
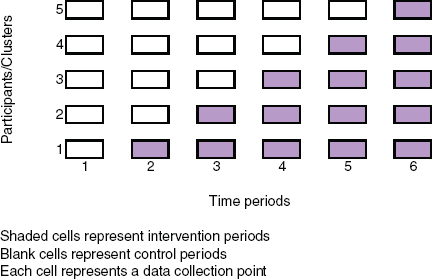
FIGURE 6-6 Stepped-wedge design.
SOURCE: Brown and Lilford, 2006.
receive the intervention. Compared to interrupted time series, the stepped-wedge design typically requires less frequent assessments (i.e., one for each new rollout) but more cohorts (e.g., communities, schools, or hospitals).
To see how the stepped-wedge design might be applied to mobile applications to prevent violence, consider a mobile intervention developed to reduce youth violence in schools. The schools receiving the intervention collect monthly data on violent behavior throughout the school year. The schools are randomly assigned to the order of intervention initiation. After a baseline month, the first randomly selected school receives the intervention and continues to use it throughout the school year. In each subsequent month the intervention is rolled out in the next randomly selected school until all of the schools have received the intervention, and violent behavior within and between schools can then be compared. In contrast to an RCT, every school eventually receives the intervention. The stepped-wedge design also makes better use of staff to roll out the intervention because the initial orientation, training, and deployment are performed at a different school each month instead of simultaneously. Newer technologies that have not been fully field-tested are often rolled out sequentially to detect problems before fully deploying, which fits a stepped-wedge model well. (See Handley et al., 2011, for a more detailed description of the stepped-wedge design.)
The regression discontinuity design assigns participants to an intervention based on a cutoff variable and then analyzes the change in slope or intercept at the cutoff between those receiving and those not receiving the intervention. The design is often used when only those deemed more in need or at risk are provided the intervention. For example, if only those at risk for dating violence are referred to receive a mobile application to change dating violence attitudes, the intervention can be evaluated by comparing dating violence attitudes of those referred with the attitudes of those not referred by analyzing differences in the prediction of dating violence attitudes from the risk variable used as the cutoff for referral. It is critical in the regression discontinuity design, however, that the cutoff criteria remain unchanged. Any variation in referral cutoff based on the risk score will introduce bias. Performed rigorously, the regression discontinuity design produces results similar to those of an RCT (Linden and Adams, 2011; Shadish et al., 2011). Regression discontinuity is preferable to an RCT when the referring agency wants all of those referred, not just those randomly assigned to the treatment group, to receive the intervention.
These examples of evaluating interventions during dissemination clearly show that dissemination should not represent the end of the research evaluation process. These methodologies do allow for evaluation during dissemination, and often these designs are more externally valid than RCTs because the intervention is being evaluated in actual users and, if well designed, the internal validity of these designs is comparable to RCTs (Shadish et al., 2011). The frequent longitudinal assessments often integrated into mHealth interventions can be leveraged to perform automated evaluations of the intervention while it is being disseminated and implemented using these designs.
Conclusion
Interventions delivered via mobile technologies (mHealth) have many potential advantages over traditional interventions. The mobile and wireless infrastructure already exists, so the costs of intervention delivery are greatly reduced. mHealth and other computerized interventions are completely standardized (i.e., they never deviate from the intervention protocol). They can be tailored and adapted over time to the user’s needs. mHealth interventions can be more engaging, especially for younger users, because of their graphics and gaming modalities. There are no time or space constraints: mHealth interventions can be delivered at any time or any place. mHealth interventions are fully scalable, which greatly improves their reach when compared with traditional intervention delivery. The ability for frequent and real-time monitoring provides both a base for research and program
evaluation as well as for interventions that can adapt to ongoing changes in the users’ responses.
All of these advantages, however, are more promise than proven. Public health has a long history of assuming that new technologies will improve public health. The Health Belief Model was developed in response to the failure of a new technology, mobile tuberculosis screenings in the 1950s, to substantially increase these screenings (Rosenstock, 1974). The mobile delivery of violence prevention interventions—and, indeed, of all public health interventions—requires rigorous evaluation. Although RCTs are the standard by which most of these interventions are judged, numerous other research designs can be used throughout the development and dissemination of mHealth interventions.
REFERENCES
Barry, A. 2001. Political machines: Governing a technological society. New York: Athlone Press.
Biglan, A., D. Ary, and A. C. Wagenaar. 2000. The value of interrupted time-series experiments for community intervention research. Prevention Science 1(1):31–49.
Bogost, I. 2010. Persuasive games. The expressive power of videogames. Cambridge, MA: MIT Press.
Borycki, E. M., M. Househ, A. W. Kushniruk, and C. Kuziemsky. 2011. Use of qualitative methods across the software development lifecycle in health informatics. Studies in Health Technology Information 164:293–297.
Bell Bajao! n.d. Breakthrough. My cause. www.bellbajao.org/my-cause/ (accessed October 1, 2012).
Brown, C. A., and R. J. Lilford. 2006. The stepped wedge trial design: A systematic review. BMC Medical Research Methodology 6:54.
Buber, M. 1923. I and thou, translated by Walter Kaufman in 1996. New York: Touchstone.
CDC (Centers for Disease Control and Prevention). 2008. The public health approach to violence prevention. http://www.cdc.gov/ViolencePrevention/overview/publichealthapproach.html (accessed March 7, 2012).
Chunara, R., J. R. Andrews, and J. S. Brownstein. 2012. Social and news media enable estimation of epidemiological patterns early in the 2010 Haitian cholera outbreak. American Journal of Tropical Medicine and Hygiene 86(1):39–45.
Clifford, S. 2009. Online, “a reason to keep on going.” New York Times, June 2. www.nytimes.com/2009/06/02/health/02face.html (accessed October 1, 2011).
Collins, L. M., S. A. Murphy, and V. Strecher. 2007. The Multiphase Optimization Strategy (MOST) and the Sequential Multiple Assignment Randomized Trial (SMART): New methods for more potent eHealth interventions. American Journal of Preventive Medicine 32(Suppl 5):S112–S118.
Elliott, A. 2010. YouTube facts: 10 things you may not have known. Mashable Business, February 19. www.mashable.com/2011/02/19/youtube-facts/ (accessed October 1, 2011).
Evans, L. 2011. Mapping murder throughout the world. The Guardian. October 10, 2011.
Foege, W. H. 2010. House on fire: The fight to eradicate smallpox. Berkeley: University of California Press.
Fogg. 2002. Persuasive technology: Using computers to change what we think and do. Elsevier. http://public.eblib.com/EBLPublic/PublicView.do?ptiID=294303 (accessed April 2, 2012).
Friedman, E. 2008. Florida teen live-streams his suicide online. ABCNews, November 21. www.abcnews.go.com/Technology/MindMoodNews/story?id=6306126 (accessed October 1, 2011).
Garrity, B. 2011. Social media join toolkit for hunters of disease. New York Times, June 13.
Gencer, M., and J. Ranck. 2011. Advancing the dialogue on mobile finance and mobile health. Country Case Studies. mHealth Alliance, Washington, DC. http://www.slideshare.net/mpayconnect/mpay-connect-mhealth-mfnance-country-studies-dec-2011 (accessed February 20, 2012).
Grameen Foundation. n.d. Mobile livelihoods. www.grameenfoundation.org/what-we-do/mobile-phone-solutions/livelihoods (accessed October 1, 2011).
Grove, J. 2010. Social networking usage surges globally. Mashable Business, March 19. www.mashable.com/2010/03/19/global-social-media-usage/ (accessed October 1, 2011).
Handley, M. A., D. Schillinger, and S. Shiboski. 2011. Quasi-experimental designs in practice-based research settings: Design and implementation considerations. Journal of American Board of Family Medicine 24(5):589–596.
Harvard Humanitarian Initiative. 2011. Disaster relief 2.0: The future of information sharing in humanitarian emergencies. Washington, DC: UN Foundation and Vodafone Technology Partnership.
Heath, T. 2010. U.S. Cellphone users donate $22 million to Haiti earthquake relief via text. Washington Post, January 18. www.washingtonpost.com/wp-dyn/content/article/2010/01/18/AR2010011803792.html (accessed April 2, 2012).
Heatwole, A. 2010. Harassmap: Tracking sexual harassment in Egypt with SMS. http://mobileactive.org/harassmap-plan-track-sexual-harassment-egypt (accessed October 1, 2011).
Hertz, M. F., and C. David-Ferdon. 2008. Electronic media and youth violence: A CDC issue brief for educators and caregivers. Atlanta, GA: Centers for Disease Control and Prevention.
HHS (U.S. Department of Health and Human Services). n.d. HHS text4health projects: Open government at HHS. www.hhs.gov/open/initiatives/mhealth/projects.html (accessed October 1, 2011).
Higgins, J. P. T. 2011. Cochrane handbook for systematic reviews of interventions, Version 5.1.0 (updated March 2011). Cochrane Collaboration. www.cochrane.org/training/cochrane-handbook (accessed April 2, 2012).
InfoDev. 2011. Student from Trinidad wins m2work’s first spot prize. www.infodev.org/en/Article.798.html (accessed on February 20, 2012).
Ioannidis, J. P. 1998. Effect of the statistical significance of results on the time to completion and publication of randomized efficacy trials. Journal of American Medical Association 279(4):281–286.
IOM (Institute of Medicine). 2011. Finding what works in health care: Standards for systematic reviews. Washington, DC: The National Academies Press.
ITU (International Telecommunications Union). 2011. Key global telecom indicators for the telecommunications service sector. www.itu.int/ITU-D/ict/statistics/at_glance/KeyTelecom.html (accessed February 20, 2012).
Jidenma, N. 2011. Facebook’s explosive growth in Africa. The next web. http://thenextweb.com/africa/2011/05/02/facebooks-explosive-growth-in-africa/ (accessed February 20, 2012).
Joelving, F. 2009. Data mining records could predict domestic violence. Wired Science, September. www.wired.com/wiredscience/2009/09/domestic-abuse-prediction/ (accessed February 20, 2012).
Kim, J. Y., H. J. Lee, N. S. Byeon, H. C. Kim, K. S. Ha, and C. Y. Chung. 2010. Development and impact of radio-frequency identification-based workflow management in health promotion center: Using interrupted time-series analysis. IEEE Transactions Information Technology in Biomedicine 14(4):935–940.
Larman, C., and V. R. Basili. 2003. Iterative and incremental development: A brief history. Computer 36(6):2–11.
Lillie, E. O., B. Patay, J. Diamant, B. Issell, E. J. Topol, and N. J. Schork. 2011. The N-of-1 clinical trial: The ultimate strategy for individualizing medicine? Personalized Medicine 8(2):161–173.
Linden, A., and J. L. Adams. 2011. Applying a propensity score-based weighting model to interrupted time series data: Improving causal inference in programme evaluation. Journal of Evaluation in Clinical Practice 17(6):1231–1238.
Marshall, J., and Nature. 2012. Online gamers achieve first crowd-sourced redesign of protein. Scientific American, January 22. www.scientifcamerican.com/article.cfm?id=victory-for-crowdsourced-biomolecule2 (accessed February 20, 2012).
Mechael, P., H. Batavia, N. Kaonga, S. Searle, A. Kwan, A. Goldberger, L. Fu, and J. Ossman. 2010. Barriers and gaps affecting mHealth in low and middle income countries. Washington, DC: mHealth Alliance and Earth Institute.
Meier, P. 2010. Launching peacetxt. The Ushahidi Blog, October 29. http://blog.ushahidi.com/index.php/2010/10/29/peacetxt (accessed October 1, 2011).
Mercy, J. A., A. Butchart, M. L. Rosenberg, L. Dahlberg, and A. Harvey. 2008. Preventing violence in developing countries: A framework for action. International Journal of Injury Control and Safety Promotion 15(4):197–208.
National Alliance on Mental Health. 2010. Election 2010: Will candidates address the facts? Check out state suicide rates and new Obama administration numbers; unemployed persons and veterans are especially at risk. Washington, DC: National Alliance on Mental Illness.
National Center for Health Statistics. n.d. Facts and figures. www.afsp.org/index.cfm?fuseaction=home.viewpage (accessed October 1, 2011).
National Center on Domestic and Sexual Violence. n.d. Sexual assault statistics. http://www.ncdsv.org/images/sexualassaultstatistics.pdf (accessed October 1, 2011).
New Tactics in Human Rights. n.d. Wk 214 mobile phones: Communicating for action. www.newtactics.org/wk214 (accessed October 1, 2011).
Ngcobo, N. 2010. Mobile lovelife goes global. Daily Sun. November 1. www.lovelife.org.za/press/media/article.php?uid=2982 (accessed October 1, 2011).
Nyirubugara, O. 2010. Unmasking child abuse with mobile phones. Haarlem, The Netherlands: Voices of Africa Media Foundation.
Papillon, A. n.d. Developing a text messaging based community domestic violence response system using FrontlineSMS. www.frontlinesms.com/_PREV/user-resources/download/Building-Community-Based-SMS-System-Using-FrontlineSMS.pdf (accessed October 1, 2011).
Pew Internet and American Life Project. 2010. Americans and their cell phones. www.pewin-ternet.org/~/media//Files/Reports/2011/Cell%20Phones%202011.pdf (accessed February 6, 2012).
Pharmacy Times. 2009. Pfizer announces “virtual” clinical trial pilot in US. November 6. www.pharmatimes.com/article/11-06-09/Pfizer_announces_virtual_clinical_trial_pilot_ in_US.aspx (accessed February 6, 2012).
Ranck, J. 2011a. Health information and health care: The role of technology in unlocking data and wellness—discussion paper. Washington, DC: United Nations Foundation and Vodafone Foundation Technology Partnership.
Ranck, J. 2011b. The Internet of things: Creating tomorrow’s healthcare. http://pro.gigaom.com/2011/11/the-internet-of-things-creating-tomorrows-health-care/ (accessed February 20, 2012).
Repetti, R. L., S. E. Taylor, and T. E. Seeman. 2002. Risky families: Family social environments and the mental and physical health of offspring. Psychological Bulletin 128(2):330–366.
Rheingold, H. 2003. Smart mobs: The next social revolution. Cambridge, MA: Basic Books.
Riley, W. T. 2011. Evaluation of mHealth. Presentation at Workshop on Communications and Technology for Violence Prevention, Institute of Medicine, Washington, DC. December 9.
Riley, W. T., D. E. Rivera, A. A. Atienza, W. Nilsen, S. M. Allison, and R. Mermelstein. 2011. Health behavior models in the age of mobile interventions: Are our theories up to the task? Translational Behavioral Medicine 1(1):53–71.
Rivera, D. E., M. D. Pew, and L. M. Collins. 2007. Using engineering control principles to inform the design of adaptive interventions: A conceptual introduction. Drug and Alcohol Dependency 88(Suppl 2):S31–S40.
Rodgers, A., T. Corbett, D. Bramley, T. Riddell, M. Wills, R. B. Lin, and M. Jones. 2005. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tobacco Control 14(4):255–261.
Rosenberg, M. L., A. Butchart, J. Mercy, V. Narasimhan, H. Waters, and M. Marshall. 2006. Interpersonal violence. In Disease control priorities in developing countries (2nd ed.), edited by D. T. Jamison, J. G. Breman, A. R. Measham, G. Alleyne, M. Claeson, D. B. Evans, J. Prabhat, A. Mills, and P. Musgrove. Washington, DC: Oxford University Press and the World Bank.
Rosenberg, M. L., E. S. Hayes, M. H. McIntyre, and N. Neill. 2010. Real collaboration: What it takes for global health to succeed. Berkeley: University of California Press.
Rosenstock, I. M. 1974. Historical orgins of the health belief model. Health Education Monographs 2:328–335.
Shadish, W. R., R. Galindo, V. C. Wong, P. M. Steiner, and T. D. Cook. 2011. A randomized experiment comparing random and cutoff-based assignment. Psychological Methods 16(2):179–191.
Testa, M., J. A. Livingston, and C. VanZile-Tamsen. 2011. Advancing the study of violence against women using mixed methods: Integrating qualitative methods into a quantitative research program. Violence Against Women 17(2):236–250.
Trudeau, M. 2010. Mental health apps: Like a “therapist in your pocket.” National Public Radio, May 24. www.npr.org/templates/story/story.php?storyId=127081326 (accessed October 1, 2011).
United Nations. 2010. World population aging 2009. New York: United Nations, Department of Economic and Social Affairs, Population Division. http://www.un.org/esa/population/publications/WPA2009/WPA2009-report.pdf.
Ushahidi. 2011. Mapping the Egypt protests and Libya crisis. The Ushahidi Blog, April 7. www.blog.ushahidi.com/index.php/2011/04/07/mapping-egypt-and-libya/ (accessed October 1, 2011).
USPSTF (U.S. Preventive Services Task Force). 2010. The guide to clinical preventive services 2010-2011: Recommendations of the U.S. Preventive Services Task Force. No. 10-05145. Rockville, MD: Agency for Healthcare Research and Quality.
Verclas, K. 2007. Human trafficking hotline: Mobile phones in the fight against slavery. http://mobileactive.org/human-trafficking-hotlin (accessed October 1, 2012).
Vital Wave Consulting. n.d. Women & mobile: A global opportunity: A study on the mobile phone gender gap in low- and middle-income countries. Cherie Blair Foundation.
Vivolo, A. M., J. L. Matjasko, and G. M. Massetti. 2011. Mobilizing communities and building capacity for youth violence prevention: The National Academic Centers of Excellence for Youth Violence Prevention. American Journal of Community Psychology 48(1–2):141–145.
Weinberger, D. 2012. Too big to know: Rethinking knowledge now that the facts aren’t the facts, experts are everywhere, and the smartest person in the room is the room. New York: Basic Books.
WHO (World Health Organization). 2002. World report on violence and health. Geneva: WHO.
WHO. 2008. Preventing violence and reducing its impact: How developing agencies can help. http://whqlibdoc.who.int/publications/2008/9789241596589_eng.pdf (accessed February 28, 2012).
WHO. 2010. Violence prevention: The evidence. http://www.who.int/violenceprevention/publications/en/index.html (accessed February 28, 2012).












































