
Aging, Health, and Chronic Conditions in China and India: Results from the Multinational Study on Global AGEing and Adult Health (SAGE)1
Paul Kowal, Sharon Williams, Yong Jiang, Wu Fan, P. Arokiasamy, and Somnath Chatterji
China and India are the two most populous countries in the world. Combined, they were home to more than 34% of the world’s 784 million people aged 60 and older in 2011. China’s proportion of older people will grow from over 12% of its total population currently to 34% in 2050. Meanwhile, India’s older population will grow from close to 8% to almost 20% over the same time period. The proportion of people aged 60 and older will exceed that of people aged 0-14 years by 2019 in China and by 2050 in India (United Nations, 2011a). In 2050, more than three-quarters of 1 billion people aged 60 and older will live in China and India, constituting 38% of the world’s 60-plus population.
Population aging in China and India will likely be accompanied by an increase in chronic disease burden. An estimated 66% of the Chinese health burden and 45% of the Indian health burden are expected to be in older adults by 2030 (Chatterji et al., 2008). Furthermore, population aging will result in an estimated 200% increase in deaths from cardio-
____________
1 The World Health Organization’s Study on Global AGEing and Adult Health (SAGE) is supported by the U.S. National Institute on Aging through Interagency Agreements (OGHA 04034785; YA1323-08-CN-0020; Y1-AG-1005-01) and through an NIH research grant (R01-AG034479). The National Institute on Aging’s Division of Behavioral and Social Research, under the directorship of Dr. Richard Suzman, has been instrumental in providing continuous intellectual and other technical support to SAGE and has made the entire endeavor possible. The Chinese government and the Shanghai Metropolitan Center for Disease Control and Prevention contributed financial and in-kind support for SAGE China. The China and India SAGE teams conducted the interviews and produced high-quality results. We would like to acknowledge Jesse Cramer, who assisted with the literature search for this chapter.
vascular disease in China between 2000 and 2040 (Leeder et al., 2005). In addition, the rapid economic growth in these countries accompanied by rapid urbanization may also contribute to the increase of noncommunicable diseases. Urbanization is associated with unhealthy nutrition and physical inactivity, leading to obesity and increases in the prevalence of chronic diseases such as diabetes (Wang et al., 2005, 2007). The number of people with diabetes in China is estimated to be more than 92 million, with another 148 million pre-diabetic (Yang et al., 2010). India has the second largest estimated number of people with diabetes currently, at 51 million (International Diabetes Federation, 2009).
Mean life expectancies at birth and age 60 were higher in China (74 years and 20 years) than India (65 years and 17 years) in 2010, with the differences between the countries projected to shrink over the next two decades (see Table 17-1). The most recent healthy life expectancy (HALE) at birth estimates for China were 65.0 years for men and 67.8 years for women in 2007 (World Health Organization, 2008). At age 60, HALE is 13.7 years for Chinese men and 15.5 years for women. HALE at birth in India is 55.9 years for men and 56.7 years for women. The difference in HALE between the genders at age 60 in India is small, with years for men and 11.9 years for women. In comparison to HALE at 60 years for both sexes combined of 14.6 years in China and 11.5 years in India, older people living in Indonesia can expect 11.9 years of healthy life remaining at age 60; in the United States, 17.3 years; and in Japan, 20.2 years.
Recent Global Burden of Disease estimates show a higher age-standardized overall disease burden in India than China, but with a higher proportion of noncommunicable disease (NCD) burden to overall burden in China than India (Abegunde et al., 2007; World Health Organization, 2008) (see Figure 17-1). The composition of NCDs across the countries is also notable, with considerable differences in cerebrovascular and ischemic heart diseases and unipolar depressive disorders. It is estimated that 44% of the total burden of disease in China in 2004 was from adults aged 45 and older (Chatterji, 2008), which is expected to increase to more than 65% by 2030. In India, the figure was 26% in 2004, rising to 46% by 2030.
In light of the demographic and health changes occurring in China and India, and in response to conferences in 2010 and 2011 to address population aging in Asia hosted by five national science academies, including the Chinese Academy of Social Sciences and Indian National Science Academy, this chapter summarizes selected health results from the World Health Organization’s (WHO) Study on Global AGEing and Adult Health (SAGE) Wave 1 for the two nations with the largest numbers of older persons. Health state and chronic condition patterns are compared and contrasted across the two countries to further improve the understanding
TABLE 17-1 Population Aged 60 and Older, Life Expectancy (LE) at Birth and Age 60, China and India, 2010 and 2030
| 2010 | 2030 | |||||||||
| Country | Total, N* | Median Age | 60+, N*(%) | LE at birth (yrs) | LE at 60 (yrs) | Total, N* | Median Age | 60+, N* (%) | LE at birth (yrs) | LE at 60 (yrs) |
| World | 6 895 | 29.2 | 759.0 (11.0) | 68.9 | 20.1 | 8 321 | 34.1 | 1 378 (16.6) | 73.1 | 21.6 |
| China | 1 341 | 34.5 | 165.2 (12.3) | 74.0 | 19.9 | 1 393 | 42.5 | 340 (24.4) | 77.4 | 21.6 |
| India | 1 224 | 25.1 | 92.7 (7.6) | 65.2 | 17.4 | 1 523 | 31.2 | 188 (12.3) | 70.5 | 19.0 |
NOTE: * in millions (000,000).
SOURCES: Data from United Nations (2011a) and World Health Organization (2008).
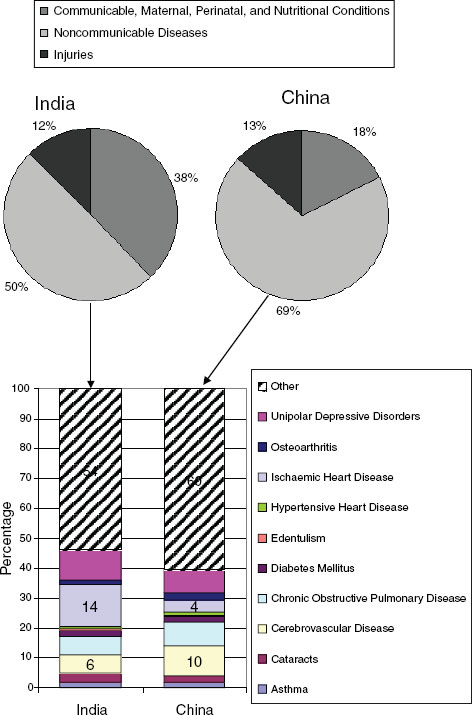
FIGURE 17-1 Percentage of age-standardized Disability-Adjusted Life Years (DALY) by Global Burden of Disease cause categories and percentage of overall noncommunicable disease burden contributed by selected health conditions in China and India, 2004.
NOTE: DALY is a health gap measure that combines the time lived with disability and the time lost due to premature mortality.
SOURCE: Data from World Health Organization (2008).
of age gradients and gender differences in health outcomes in China and India. The results also describe the approach to measurement of health and chronic diseases used by WHO, to highlight differences in reporting bias across countries and the methods SAGE employs to account for these biases.
STUDY METHODS
SAGE Wave 1
SAGE is a longitudinal study with nationally representative cohorts of persons aged 50 and older in China, Ghana, India, Mexico, the Russian Federation, and South Africa, with comparison samples of younger adults aged 18-49 years in each country. The study focuses on health and health-related outcomes and their determinants.
SAGE was implemented as a face-to-face household interview in China (2008-2010) and India (2007-2008). The samples were drawn from a current frame using a stratified, multistage cluster design so as to allow each household and individual respondent to be assigned a known nonzero probability of selection. Half the interviews in China were completed using a computer-assisted personal interview. In both China and India, the samples were selected to be nationally representative, using multistage sampling plans. In China, the survey was carried out in Guandong, Hubei, Jilin, Shaanxi, Shandong, Shanghai, Yunnan, and Zhejiang, covering four regions. The entire sample of India was followed up from households included in SAGE Wave 0 conducted in 2003, and was collected in the states of Assam, Karnataka, Maharashtra, Rajasthan, Uttar Pradesh, and West Bengal.
The SAGE survey instruments cover a broad range of topics, including health and its determinants, disability, subjective well-being, emotional and financial well-being, health care utilization, and health systems responsiveness. SAGE has included methodologies to improve cross-population comparability of self-reported health and well-being data through the inclusion of biomarkers, performance tests, anchoring vignettes, and additional validation studies. The anchoring vignettes approach included a short story that describes a concrete level of health in a given health domain, such as mobility (King et al., 2004; Salomon, Tandon, and Murray, 2004). Respondents are asked to rate the vignettes using the same questions and response categories that they use to describe their own health state along the same domain.
SAGE2 has also worked to harmonize methods and results with a number of studies, including the U.S. Health and Retirement Study, Chinese Health and Retirement Longitudinal Study, and Longitudinal Aging Study in India.
Variables
Gender and age were collected, as well as area of residence, education, marital status, and income and consumption information. Four age groups were used for the analyses, 18-49, 50-59, 60-69, and 70-plus years. Education variables were mapped to an international standard classification in each country to improve comparability (United Nations Educational, Scientific and Cultural Organization, 2006). Income or wealth quintiles were derived from the household ownership of durable goods, dwelling characteristics (type of floors, walls, and cooking stove), and access to services for the dwelling, such as improved water, sanitation, and type of cooking fuel used. Durable goods included number of chairs, tables, or cars, and if, for example, the household has electricity, a television, fixed line or mobile phone, and a bucket or washing machine. A total of 21 assets and wealth indicators were included with overlaps and differences in the asset lists by country.
The income and wealth data were recoded into dichotomous variables, with the resulting data set being reshaped, as though each household had multiple observations for wealth (each item being one observation). A pure random effect model was fit based on the multiple items per household. The result provides indicator-specific thresholds on the latent income scale such that a household is more likely to respond affirmatively than not when its permanent income exceeds this threshold (Ferguson et al., 2003). This “asset ladder” was generated and is country-specific. Using a Bayesian post-estimation (empirical Bayes) method, households were arranged on the asset ladder, where the raw continuous income estimates are transformed in the final step into quintiles.
The survey instrument asked about difficulties in functioning in eight domains of health (mobility, self-care, pain/discomfort, cognition, interpersonal activities, vision, sleep/energy, and affect) and related vignettes, behavioral risk factors (tobacco use, alcohol use, physical inactivity, diet), disability, happiness, chronic conditions (asthma, angina, arthritis, depression, and diabetes), and healthcare utilization. In addition, objectively observed performance tests (including grip strength and a four-meter timed walk) and anthropometric measurements (including weight,
____________
2 More information, survey materials and results for SAGE are available at http://www.who.int/healthinfo/systems/sage/en/index.html.
height, and waist circumference) were conducted. However, the latter results are not reported in this chapter.
OVERALL SELF-REPORTED GENERAL HEALTH
A single overall self-rated general health question is used in SAGE: “In general, how would you rate your health today?” with a five-point response scale from very good to very bad. A single general health question has been shown to be a good predictor of numerous health outcomes, but raises concerns about comparability and inconsistency of results, which is why a multidimensional approach to measuring health state, combined with vignette methodologies, is also used in SAGE (Bowling, 2005; Fayers and Sprangers, 2002; Salomon et al., 2009; Sen, 2002; Subramanian et al., 2009).
Health State
The 16 questions asked about difficulties in functioning across multiple health domains. In this approach to measuring health, an individual’s health state is considered a vector of capacities to function across a parsimonious set of domains in day-to-day life. As noted above, these domains included mobility, self-care, pain/discomfort, cognition, interpersonal activities, vision, sleep/energy, and affect. Examples of the questions asked about one domain (mobility) are below:
Q2002: Overall in the last 30 days, how much difficulty did you have moving around?
Q2003: Overall in the last 30 days, how much difficulty did you have in vigorous activities (“vigorous activities” require hard physical effort and cause large increases in breathing or heart rate)?
Respondents could answer using a five-point scale: 1 = None; 2 = Mild; 3 = Moderate; 4 = Severe; 5 = Extreme/Cannot do. A single health state score is generated using the Binormal Hierarchical Ordered Probit (BiHOPIT) method. Vignette adjustments of the composite health state scores were used to improve comparability of results across the two countries. The anchoring vignette technique used the same questions and response categories as used for self-assessment. The vignettes are used to fix the level of ability on a given health domain so that when analyzing the results, the variation in categorical responses can be attributed to variation in response category cut-points: that is, at what point a respondent moves from mild to moderate, or severe to extreme on the categorical response scales (Hopkins and King, 2010; Salomon et al., 2004). The additional information provided by the vignette ratings helps to describe the effects of different covariates on two important issues: (1) the level of the underlying latent variable
and (2) the cut-points on the latent variable scale. Scores were normalized and then transformed to a scale of 0 to 100, with zero representing worst health and 100, best health.
Chronic Conditions
In this chapter, five chronic conditions are summarized. Respondents were asked if they had been diagnosed with any of the following chronic medical conditions: angina, arthritis, asthma, diabetes, or depression. The question format used was, “Have you ever been told by a health professional that you have…?”, or “Have you ever been diagnosed with…?” for each health condition.
In addition to self-reported diagnosis, a set of symptomatic questions based on each condition was also asked, except for diabetes where a validated set of symptomatic questions are not currently available. The set of symptoms for each condition was derived from standard instruments, such as the World Mental Health Survey version of the Composite International Diagnostic Interview for the diagnosis of depression (Kessler and Ustun, 2004) or the Rose questionnaire for angina (Rose, 1962). The pattern of responses to the symptom questions for the four conditions (angina, arthritis, asthma, and depression) was combined with results from a separate diagnostic item probability study implemented in 2003 by WHO (Moussavi et al., 2007). This study used Receiver Operating Characteristic (ROC) analysis to create the symptom-reporting algorithm-based estimates. The method describes the sensitivity and specificity of an instrument, in this case an algorithm combining responses to different symptomatic questions. The ROC curve combines the true-positive rate and the false-positive rate of each algorithm, and the one with the highest area under the curve (“AUC statistic”) is ultimately selected to derive the estimated rates.
Respondents were also asked if they were ever treated for each chronic condition they reported, if they had received treatment in the past one year (an estimate of being on longer-term regular therapy for the chronic condition), and if they were currently on treatment at the time of the interview. These two combined give an estimate of healthcare coverage and disease chronicity.
Statistical Analyses
The analyses focused on sex and age differences in health and chronic conditions. For the single overall general health question, an ordered logistic regression produced proportional odds ratios. A composite health state score in SAGE was generated using the 16 questions asked in eight
health domains. A BiHOPIT model, a modification of the Compound Hierarchical Ordered Probit (CHOPIT) (Tandon et al., 2003), was used to take into account the responses to the vignettes that adjusted for response biases across the countries. BiHOPIT and CHOPIT are both generalizations of the ordered probit model, and allow the model cut-points to vary by the same covariates that the ordinal health response variables do. This means that the covariates have a two-way effect, one from the model and one from the cut-points. The latter is driven by the vignette responses. This more analytically intensive approach enables modeling to account for different health expectations, for example based on wealth, and corresponding health. BiHOPIT is computationally more efficient than CHOPIT, but provides similar results.
The prevalence of each condition was estimated separately and was generated using probability weights based on WHO’s World Standard Population and the UN Statistical Division (Ahmad et al., 2001; United Nations, 2009). Results were age-standardized to improve the validity of comparisons across the two countries. Cases with age, gender, or residence variables missing were dropped from the analyses. STATA 11.2 was used for all analyses.
RESULTS
The samples included 14,793 respondents in China and 11,230 respondents in India (see Table 17-2). The Indian sample included a large number of younger (18-49) women from SAGE Wave 0 added to the Wave 1 sample as part of a nested study to meet the add-on sampling targets and study objectives. Otherwise, the percentages of men and women at older ages were similar in the two countries. A higher percentage of respondents in India resided in rural areas as compared to China; the India sample also had a slightly lower percentage in the lowest wealth quintile and slightly higher percentage in the highest wealth quintile.
The weighted results are also included in Table 17-2, with more men than women and more than 80% currently married/cohabiting in both countries. China had more older and wealthier adults than India.
Overall Health
Using the single overall self-rated general health question, male sex, younger age, urban residence, higher wealth, and living in China had significantly higher log odds of better health (see Table 17-3). Differences in the odds of good health categories, as compared to the lowest level health category, were statistically significant between the countries, as well as
TABLE 17-2 Demographic Characteristics, Weighted and Unweighted Sample Sizesa with Percentage, SAGE China and India, 2007-2010.
| China | India | |||
| Gender | Unweighted Nb (%) | Weighted Nb (%) | Unweighted Nb (%) | Weighted Nb (%) |
| Men | 6 883 (46.5) | 7 525 (50.9) | 4 349 (38.7) | 5 714 (50.9) |
| Women | 7 910 (53.5) | 7 268 (49.1) | 6 881 (61.3) | 5 516 (49.1) |
| Age Group | ||||
| 18-49 | 1 636 (11.1) | 10 980 (74.2) | 4 670 (41.6) | 8 448 (75.2) |
| 50-59 | 5 701 (38.5) | 1 713 (11.6) | 2 939 (26.2) | 1 353 (12.0) |
| 60-69 | 3 919 (26.5) | 1 215 (8.2) | 2 235 (19.9) | 860 (7.7) |
| 70-79 | 2 770 (18.7) | 709 (4.8) | 1 058 (9.4) | 445 (4.0) |
| 80+ | 773 (5.2) | 176 (1.2) | 328 (2.9) | 126 (1.1) |
| Residence | ||||
| Urban | 7 205 (48.7) | 7 172 (48.5) | 2 845 (25.3) | 2 861 (25.5) |
| Rural | 7 588 (51.3) | 7 621 (51.5) | 8 385 (74.7) | 8 369 (74.5) |
| Marital Status | ||||
| Never married | 279 (1.9) | 849 (5.7) | 621 (5.5) | 1 057 (9.4) |
| Currently married | 12 295 (83.1) | 13 116 (88.7) | 8 715 (77.6) | 9 194 (81.9) |
| Cohabiting | 27 (0.2) | 36 (0.2) | — | — |
| Separated or divorced | 267 (1.8) | 225 (1.5) | 79 (0.7) | 60 (0.5) |
| Widowed | 1 911 (12.8) | 554 (3.7) | 1 814 (16.2) | 917 (8.2) |
| Missing | 14 (0.1) | 15 (0.1) | 1 (0.0) | 2 (0.0) |
| Wealth Quintile | ||||
| Lowest | 2 948 (19.9) | 1 531 (10.4)) | 2 232 (19.9) | 2 565 (22.8) |
| Second | 2 949 (19.9) | 2 477 (16.8) | 2 232 (19.9) | 2 431 (21.7) |
| Middle | 2 948 (19.9) | 2 672 (18.1) | 2 232 (19.9) | 2 269 (20.2) |
| Fourth | 2 947 (19.9) | 3 290 (22.2) | 2 234 (19.9) | 1 887 (16.8) |
| Highest | 2 948 (19.9) | 4 764 (32.2) | 2 229 (19.9) | 2 028 (18.1) |
| Missing | 53 (0.4) | 59 (0.4) | 71 (0.6) | 50 (0.4) |
| Total | 14 793 (100) | 14 793 (100) | 11 230 (100) | 11 230 (100) |
aSAGE samples are representative of the 50+ population, with a smaller group of younger adults selected for comparison purposes. In India, the sample of 18-to 49-year-old women was supplemented to meet the objectives of a nested study.
bIn millions (000,000).
SOURCE: Data from SAGE Wave 1.
clear differences by gender and gradients by age and income quintiles. Marital status did not significantly impact health reporting.
Using the continuous composite health state measure, a decline in health state with increasing age is seen in both countries; however, the level of health is higher at all age points in China as compared to India (see Figure 17-2). The differences were more pronounced between the countries in the ages from about 40 to 60 years, possibly indicating a cohort effect.
TABLE 17-3 Ordered Logistic Regression Results for Overall Self-Rated General Health
| Independent Variables (referent group) | Ordered Logit Coefficient | Standard Error |
| Gender (male) | 1.45* | 0.04 |
| Age Group (18-49) | ||
| 50-59 | 2.59* | 0.09 |
| 60-69 | 3.90* | 0.14 |
| 70+ | 5.97* | 0.25 |
| Residence (urban) | 1.10* | 0.03 |
| Marital Status (married/cohabiting) | 1.05 | 0.03 |
| Wealth Quintile (lowest) | ||
| Second | 0.75* | 0.03 |
| Middle | 0.65* | 0.03 |
| Fourth | 0.56* | 0.02 |
| Highest | 0.40* | 0.02 |
| Country (China) | 1.25* | 0.03 |
NOTE: * denotes p = 0.00. N = 25640; chi-square (df = 11) = 3169; pseudo R-squared = 0.05.
SOURCE: Data from SAGE Wave 1.
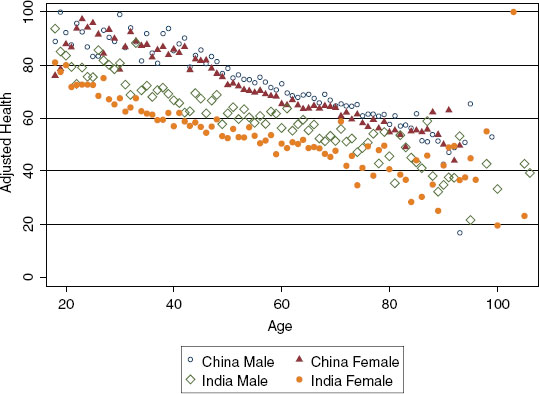
FIGURE 17-2 Vignette-adjusted health scores by age, gender, and country.
SOURCE: Data from SAGE Wave 1.
Health was better (higher health scores) in men than women in both countries, with greater differences between the genders in the health scores in India than China. An analysis of the contributions of the different domains to the overall health state score may help to better understand the determinants and drivers of health between the genders and at different ages.
Chronic Conditions
Overall, 33% of Chinese and 49% of Indian respondents aged 50 and older reported at least one chronic condition. The percentage of people with a chronic condition increased with increasing age in both countries. At each age group, Chinese men and women had lower levels of reported chronic conditions than their Indian counterparts. Comparing the youngest (18-49) to oldest (70+) age groups, women had a 33 percentage-point difference in both countries (52% versus 85% in China and 41% versus 74% in India). The age-group difference between younger and older men was 28 percentage points in China, but 36 percentage points in India, which was the largest difference in rates of reported health conditions.
In general, men reported lower levels of chronic conditions than women in both China and India, with some differences between the sexes by age. For those with no chronic conditions, the largest differences between the genders were seen in the 50-59 and 60-69 age groups in China, and the 60-69 age group in India (see Figure 17-3). For those with one condition, the largest differences were in the 50- to 59-year-old men versus women in China and the 60- to 69-year-old men and women in India. For those with two or more chronic conditions, the biggest differences between the gendrs were seen in the older two cohorts in China and the 50-59 age group in India.
Angina
The percentage of Indians (19.6%) reporting angina through the Rose questionnaire was double that in China (10%) for the 50-plus population. However, Indians were far less likely to have received recent (in the two weeks prior to interview) or longer-term (over the past 12 months) treatment.
China
Angina increased with age in both genders in China. The percentages with angina by self-report and symptom-reporting were not dissimilar by age group but with larger differences between the two methods of assessment in women than men. For instance, 3.0% of men aged 50-59 had angina
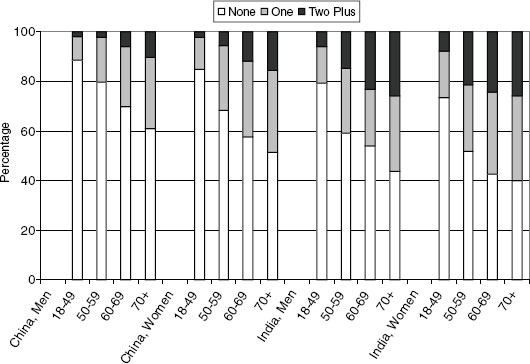
FIGURE 17-3 Percentage (%) with chronic conditions and co-morbidities by age, gender, and country.
SOURCE: Data from SAGE Wave 1.
by self-report and 3.6% by symptom reporting, compared to 5.9% and 7.9%, respectively, for women. Women had higher rates of angina than men at all age groups. Current and longer-term treatment levels were similar in men and women and increased with age.
India
The percentages of men with angina increased with increasing age in both men and women in India. Angina self-report versus symptom-reporting in India resulted in significantly different rates for men and women. Using the 50-59 age group as an example, the differences by method of ascertainment between men (5.9% by self-report and 12.3% by symptom-reporting) and women (4.0% and 20.4%) in India were large. Using self-report, men had higher rates of angina than women; however, using symptom-reporting, a larger percentage of women had angina than men. In addition, men were more likely to be on longer-term and current (in past two weeks) therapy than women.
Arthritis
Twenty-two percent of Chinese and 25% of Indians aged 50 and older had arthritis based on symptom-reporting. Using this method, rates of arthritis were slightly higher in India than China but lower in India than China using self-report. Percentages receiving current or ongoing therapies for arthritis were higher in China than India.
China
Arthritis increased steadily with age in China for men and women. Both methods of assessing arthritis prevalence produced similar results in both men and women. Rates of arthritis were higher in women (30.3%) than men (20.6%) for the 70-plus age group, but similar in the 18-49 age group (10.3% in women and 8.3% in men). Levels of treatment were again similar for the genders across the different age groups, with slightly more men receiving longer-term treatments in the 70-plus age group.
India
Levels of arthritis increased with age in men in India, but remained at about 28% across the older three age groups (50-59, 60-69, and 70-plus) in women. The percentage with arthritis for both genders was slightly higher using the symptom-reporting method as compared to self-report. The differences between men and women were similar using either method. The percentage of men aged 50-59 with arthritis was 19.5%; it was 28.4% for women. Women reported higher levels of ongoing treatment over the past year compared to men. Younger men were more likely to be on current therapy (in the two weeks prior to interview) than younger women.
Asthma
The percentage with asthma in the 50-plus population was lower in China (3.9%) than in India (11.0%). Asthma increased with age in both countries, and higher levels were reported in India than China at all age groups using either method. Longer-term and current treatment levels were typically higher in India than China for asthma.
China
Younger (18-49) and older (70-plus) women in China reported lower levels of asthma compared to men in the same age groups. Less than 1%
(0.6%) of younger women and 6.0% of older women had asthma as compared to 1.4% of younger men and 7.7% of older men. The middle-age groups had similar percentages for both genders. Levels were higher in the symptom-reporting method than the self-report at all ages and in both sexes. The percentages receiving current (more than 20%) and longer-term (more than 30%) treatment were similar in men and women.
India
The percentage with asthma increased from 4.9% in younger men to 16.9% in older men in India, and from 3.5% in younger women to 11.1% in older women. Men in India reported higher levels of asthma than women across all age groups, based on either self-report or symptom-reporting. Levels of current (close to 30%) and longer-term (over 40%) treatment of asthma were similar in both genders.
Diabetes
The percentage reporting diabetes was similar in China (6.6%) and India (6.9%) in the 50-plus population. The patterns of diabetes by age and gender between the two countries were more mixed than for any of the other conditions. Diabetes rates increased with age in China but showed somewhat variable patterns in India. Rates are higher in the younger two age groups for Indian men (2.9% in the 18-49 age group and 8.8% in the 50-59 group) compared to Chinese men (1.4% and 3.3%, respectively), but the percentages were similar for older Indians (7.2% in the 60-69 and 8.2% in the 70-plus age groups) and Chinese men (7.5% and 8.4%, respectively). A higher percentage of women than men in China had diabetes, but a lower percentage of women than men in India had diabetes. Current and longer-term treatment rates for diabetes are higher in China than in India.
China
The percentage with diabetes increased with age for Chinese men and women: from 1.4% of younger men to 8.4% of older men, and from 1.8% of younger women to 10.0% of older women. The percentage of younger men receiving current (94.2%) or longer-term (86.4%) treatment was higher than in younger women (75.7% and 67.6%, respectively); otherwise, the treatment rates were high (more than 80%) and comparable between the genders.
India
The age pattern for diabetes was less clear for both men and women in India, with a higher percentage reporting diabetes in the 50-59 age group for men (8.8%) and women (5.5%) than the 60-69 age group for men (7.2%) and women (5.1%). As with asthma, a higher percentage of Indian men reported diabetes as compared to Indian women. Longer-term treatment rates were typically above 70% for men and women and current treatment rates above 50%.
Depression
Compared with the other conditions, depression showed the largest differences in reporting by country, with much lower reported levels in China than in India. Just 2.0% of Chinese people aged 50-plus reported depression using the CIDI questions, while 19.3% of Indians had depression. The differences in depression by age were small in both countries. Not surprisingly, the levels of depression by symptom-reporting were much higher than by self-report. Undertreatment of depression was rife: the percentage on current or longer-term therapy was less than 20% in each age group for men and women in China and India.
China
The percentage of women reporting depression was slightly higher than men, with only slight differences in depression by age group. Treatment levels were low overall, with higher rates in younger age groups than older age groups.
India
Depression increased with increasing age in India, with slightly higher percentages in women than men in each age group. For example, 15.8% of men aged 50-59 and 21.2% of men aged 70 and older had depression, as compared to 18.9% and 25.3% of women. Current and ongoing treatment levels were low at all ages and in men and women.
Co-Morbidity
A substantially larger proportion of Indian respondents reported multiple morbidities than Chinese respondents at each age group for both men and women. For example, 5.7% of Chinese men and 11.9% of Chinese women aged 60-69 reported multiple chronic diseases, compared to 23.3%
of Indian men and 24.3% of Indian women in the same age group. The two countries had similar percentages of persons reporting one chronic condition at each age group, for both males and females.
DISCUSSION
WHO’s SAGE, Wave 1 data provide cross-country comparable health results. Differences in levels of health states are evident when comparing China and India, even after correcting for possible reporting biases using vignette methodologies. A striking result is that health state scores for women aged 50-59 were similar to men aged 60-69, and women aged 60—69 similar to men aged 70+ in both countries. This finding suggests a decade difference in health levels for women as compared to men. This difference may shrink drastically because of highly skewed gender ratios in both countries and the positive impact of women on men’s longevity and health (Economist, 2010a, 2010b). Given the difference in morbidity, women still live longer than men in both countries.
Differences in self-reported health levels between the genders have been well documented but inconsistent (Bath, 2003; Benyamini et al., 2003; Fang et al., 2003; Hairi et al., 2010). Here the differences were significant within the countries, as well as between China and India. Some of this could be due to the differences in composition of the sample in each country, with a higher proportion of rural dwellers in the India sample, more people in the wealthier income quintiles in China, and more people in the poorer income quintiles in India. The reporting of health conditions was also different by gender and country, with the biggest difference seen for the reporting of depression. Despite the measures taken in SAGE to overcome reporting biases, the well-documented low reporting of depression in China was also found here, and will prompt a revisit of the measurement technique used for depression for Wave 2 in China in 2012 (Bromet et al., 2011).
The declines in overall self-reported health with increasing age were clear using either the single overall general health question or the multidimensional approach to measuring health. A more consistent gradient was clearly shown using the continuous measure, and can be deconstructed to identify the determinants driving the differences at different ages, levels of income, and between the two countries. The health status of respondents in China, for both males and females, was consistently better across all ages as compared to respondents in India. The vignette adjustment narrows this difference somewhat as compared to the unadjusted results. Respondents in China report fewer difficulties in health domains as compared to respondents in India; however, respondents in India have vignette-rating patterns suggesting that they identify health problems at
lower thresholds, that is, they have stricter standards (detailed results not shown, available from authors). Nonetheless, the differences in health status between China and India are validated by the levels and differences in healthy life expectancy (HALE) at age 60 in China (14.6 years) and India (11.5 years). With increasing longevity in China and India, and the rise in obesity and NCDs so striking that even large multinational corporations are taking note (JWT Intelligence, 2010), the steady decline in health using the health state measures has implications for disability in older age and the compression or expansion of morbidity in these middle-income countries (Gu et al., 2009; Tyagi and Kapoor, 2010). Longitudinal data and improved measurement methods are needed to provide valid measures of health and to disentangle the complexities of health in older age (National Research Council, 2001). SAGE is providing the data and methodologies to address aging and health across a number of countries, including health measures, modifiable risk factors, and health-related outcomes that will form the basis of future studies.
It is estimated that 80% of cardiovascular disease deaths occur in lower- and middle-income countries, including China and India (Bonow et al., 2002). Considerable underreporting of the five chronic diseases presented here was demonstrated through comparing self-reports and symptom-reporting. For example, the low levels and under-reporting of mental health conditions and depression in China, through a variety of measurement techniques, is noted (Lee et al., 2006; Parker, Gladstone, and Chee, 2001; Shen et al., 2006). The rate of major depressive disorder in SAGE (2.0%) matches that found in a study in metropolitan China (Shen et al., 2006). The technique used in SAGE to measure this affective disorder was informed by the World Mental Health Survey Initiative (http://www.hcp.med.harvard.edu/wmh/). Understanding the limitations of the current estimates and employing methods to improve measurement have further implications for the true burden of NCDs in China and India, and the health systems’ response to chronic conditions.
Furthermore, co-morbidity has a large impact on health and well-being (Haagsma et al., 2011; Moussavi, 2007), yet complexities of multiple chronic conditions are understudied and not well understood (Tinetti and Studenski, 2011). In an effort to improve the evidence base for planning and policymaking, SAGE measures are attempting to reduce well-known reporting biases for chronic conditions in epidemiological health studies to improve the understanding about impacts of co-morbidity on health. India currently has much higher levels of people with multiple chronic conditions than China; however, China’s underreporting of conditions, particularly mental health conditions, is well documented.
China’s levels of treatment for the different chronic health conditions were generally higher than India, with the highest levels of treatment for
angina and diabetes. Overall though, and in particular for depression, the healthcare coverage for patients with these NCDs is strikingly low. The levels and treatment of NCDs will need to be tracked over time to assess the burden on governments, the labor force, and healthcare systems. SAGE has incorporated biomarker measurements to independently assess risks for and levels of chronic disease (from height, weight and waist circumference, to glycosylated hemoglobin and C-reactive protein from dried blood spots) and will be reported separately.
The concern over NCDs in lower- and middle-income countries was raised in WHO’s Moscow Declaration (World Health Organization, 2011) in April 2011 with specific statements about the huge burden in developing countries. Moving towards universal health coverage (Gwatkin and Ergo, 2010; World Health Organization, 2010a), especially targeting poorer and vulnerable population groups at the outset, and addressing the burden of increasing urbanization (Dobbs and Sankhe, 2010; WHO, 2010b) and the social determinants of health (Marmot, 2009) are mechanisms to shift the ongoing health transitions. The topics raised in this chapter are also a timely follow-up to the United Nations General Assembly High-level Meeting on Non-communicable Diseases (United Nations, 2011b) held in September 2011.
SAGE has many strengths, including nationally representative samples with large numbers in different older age groups, a method for measuring health and related techniques for improving cross-national comparability, and assessment of angina, arthritis, asthma, and depression through self-report and validated symptom-reporting methods (Moussavi et al., 2007; Tandon, Murray, and Shengalia, 2004). While the accuracy of self-reported health conditions is robust in high-income countries and wealthier populations, the same is not true in situations where low access to healthcare and low literacy levels reduce the reliability of self-report (Sen, 2002). In low- and middle-income countries, validated algorithms of disease symptoms offer a method to generate reliable prevalence estimates (Rose, 1962; Sembajwe et al., 2010). SAGE has also included biomarker and anthropometric measurements to help minimize biases in prevalence rates based on self-report and will complement these results in future studies. Increasingly, objective health outcomes, such as grip strength, timed walk, and results from collected blood samples, are used to improve our understanding of subjective or perceived health, although they may also mirror or deviate from the self-reported measures (Cooper et al., 2011). In this case, the results from the blood tests and performance tests are forthcoming from each country team. The need for improved data collection has been noted as an issue for healthcare equity even in high-income countries (Weissman and Hasnain-Wynia, 2011). SAGE
provides one such data collection platform across a number of countries, including China and India.
REFERENCES
Abegunde, D.O., C.D. Mathers, T. Adam, and M. Ortegon. (2007). The burden and costs of chronic diseases in low-income and middle-income countries. The Lancet 370:1,9291,938.
Ahmad, O.B., C. Boschi-Pint, A.D. Lopez, C.J.L. Murray, R. Lozano, and M. Inoue. (2001). Age Standardization of Rates: A New WHO Standard. Geneva: World Health Organization.
Bath, P.A. (2003). Differences between older men and women in the self-rated health-mortality relationship. The Gerontologist 43(3):387-395.
Benyamini, Y., T. Blumstein, A. Lusky, and B. Modan. (2003). Gender differences in the self-rated health-mortality association: Is it poor self-rated health that predicts mortality or excellent self-rated health that predicts survival? Gerontology 43(3):396-405.
Bonow, R.O., L.A. Smaha, S.C. Smith, G.A. Mensah, and C. Lenfant. (2002). The international burden of cardiovascular disease: Responding to the emerging global epidemic. Circulation 206:1,602-1,605.
Bowling, A. (2005). Just one question: If one question works, why ask several? Journal of Epidemiology & Community Health 59:342-345. doi:10.1136/jech.2004.021204.
Bromet, E., L.H. Andrade, I. Hwang, N.A. Sampson, J. Alonso, G. de Girolamo, R. de Graaf, K. Demyttenaere, C. Hu, N. Iwata, A.N. Karam, J. Kaur, S. Kostyuchenko, J.P. Lépine, D. Levinson, H. Matschinger, M.E. Mora, M.O. Browne, J. Posada-Villa, M.C. Viana, D.R. Williams, and R.C. Kessler. (2011). Cross-national epidemiology of DSM-IV major depressive episode. BMC Medicine 26(9):90.
Chatterji, S., P. Kowal, C. Mathers, N. Naidoon, J.P. Smith, and R. Suzman. (2008). The health of aging populations in China and India. Health Affairs 27(4):1,052-1,063.
Cooper, R., D. Kuh, C. Cooper, C.R. Gale, D.A. Lawlor, F. Matthews, R. Hardy, and the FALCon and HALCyon Study Teams. (2011). Objective measures of physical capability and subsequent health: A systematic review. Age Ageing 40:14-23.
Dobbs, R., and S. Sankhe. (2010, July). Comparing urbanization in China and India. McKinsey Quarterly.
Economist. (2010a, 4 May). Gendercide. The worldwide war on baby girls: Technology, declining fertility and ancient prejudice are combining to unbalance societies. Available: http://www.economist.com/node/15636231.
Economist. (2010b, 11 August). Health and the sex ratio. A healthy relationship: The mere presence of women seems to bring health benefits to men. Available: http://www.economist.com/node/16789152.
Fang, X.H., C. Meng, X.H. Liu, X.G. Wu, H.J. Liu, L.J. Diao, and Z. Tang. (2003). Study on the relationship between self-rated health situation and health status in the elderly—an 8-year follow-up study from the Multidimensional Longitudinal Study of Aging in Beijing. Zhonghua Liu Xing Bing Xue Za Zhi 24(3):184-188.
Fayers, P.M., and M.A.G. Sprangers. (2002). Understanding self-rated health. The Lancet 359: 187-188.
Ferguson, B., A. Tandon, E. Gakidou, and C.J.L. Murray. (2003). Estimating permanent income using indicator variables. In Health Systems Performance Assessment: Debates, Methods and Empiricism, C.J.L. Murray and D.B. Evans (Eds.). Geneva: World Health Organization.
Gu, D., M.E. Dupre, D.F. Warner, and Y. Zeng. (2009). Changing health status and health expectancies among older adults in China: Gender differences from 1992-2002. Social Science & Medicine 68(12):2,170-2,179.
Gwatkin, D.R., and A. Ergo. (2010). Universal health coverage: Friend or foe of health equity? The Lancet 377(9,784):2,160-2,162.
Haagsma, J.A., E.F. van Beeck, S. Polinder, H. Toet, M. Panneman, and G.J. Bonsel. (2011). The effect of comorbidity on health-related quality of life for injury patients in the first three years following injury: Comparison of three comorbidity adjustment approaches. Population Health Metrics 9:10.
Hairi, N.N., A. Bulgiba, R.G. Cumming, V. Naganathan, and I. Mudla. (2010). Prevalence and correlates of physical disability and functional limitation among community dwelling older people in rural Malaysia, a middle income country. BMC Public Health 10:492.
Hopkins, D.J., and G. King. (2010). Improving anchoring vignettes: Designing surveys to correct interpersonal incomparability. Public Opinion Quarterly:1-26. doi: 10.1093/poq/nfq011.
International Diabetes Federation. (2009). Diabetes Atlas, 4th Edition. Available: http://www.idf.org/diabetesatlas.
JWT Intelligence. (2010). Spotlight on marketers as obesity rises in China and India. Available: http://www.jwtintelligence.com/2010/08/spotlight-on-marketers-as-obesity-rises-in-china-and-india/.
Kessler, R.C., and T.B. Ustun. (2004). The World Mental Health (WMH) Survey initiative version of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). International Journal of Methods in Psychiatric Research 13:93-121.
King, G., C.J.L. Murray, J.A. Salomon, and A. Tandon. (2004). Enhancing the validity and cross-cultural comparability of measurement in survey research. American Political Science Review 98(1):191-207.
Lee, A., M.Y.L. Chiu, A. Tsang, H. Chui, and A. Kleinman. (2006). Stigmatizing experience and structural discrimination associated with the treatment of schizophrenia in Hong Kong. Social Science & Medicine 62:1,685-1,696.
Leeder, S., S. Raymond, H. Greenberg, H. Liu, and K. Esson. (2005). A Race Against Time: The Challenge of Cardiovascular Disease in Developing Economies. New York: Columbia University.
Marmot, M. (2009). Closing the health gap in a generation: The work of the Commission on Social Determinants of Health and its recommendations. Global Health Promotion 16:23-27.
Moussavi, S., S. Chatterji, A. Tandon, V. Patel, and B. Ustun. (2007). Depression, chronic diseases, and decrements in health: Results from the World Health Surveys. The Lancet 370(9590):851-858.
National Research Council. (2001). Preparing for an Aging World: The Case for Cross-National Research. Panel on a Research Agenda and New Data for an Aging World. Committee on Population and Committee on National Statistics, Division of Behavioral and Social Sciences and Education. Washington, DC: National Academy Press.
Parker, G., G. Gladstone, and K.T. Chee. (2001). Depression in the planet’s largest ethnic group: The Chinese. American Journal of Psychiatry 158:857-864.
Rose, G.A. (1962). The diagnosis of ischemic heart pain and intermittent claudication in field surveys. Bulletin of the World Health Organization 27:645-658.
Salomon, J.A., A. Tandon, and C.J.L. Murray for the World Health Survey Pilot Study Collaborating Group. (2004). Comparability of self-rated health: Cross sectional multi-country survey using anchoring vignettes. British Medical Journal 328:258-261.
Salomon, J.A., S. Nordhagen, S. Oza, and C.J.L. Murray. (2009). Are Americans feeling less healthy? The puzzle of trends in self-rated health. American Journal of Epidemiology 170:343-351.
Sembajwe, G., M. Cifuentes, S.W. Tak, D. Kriebel, R. Gore, and L. Punnett. (2010). National income, self-reported wheezing and asthma diagnosis from the World Health Survey. European Respiratory Journal 35:279-286.
Sen, A. (2002). Health: Perception versus observation. British Medical Journal 324:860-861.
Shen, Y.C., M.Y. Zhang, Y.Q. Huang, Y.L. He, Z.R. Liu, H. Cheng, A. Tsang, S. Lee, and R. Kessler. (2006). Twelve-month prevalence, severity, and unmet need for treatment of mental disorders in metropolitan China. Psychological Medicine 26:257-267.
Study on Global AGEing and Adult Health, Wave 1. (2010). World Health Organization. Available: http://www.who.int/healthinfo/systems/sage/en/index1.html.
Subramanian, S.V., M.A. Subramanyam, S. Selvaraj, and I. Kawachi, I. (2009). Are self-reports of health and morbidities in developing countries misleading? Evidence from India. Social Science Medicine 68(2):260-265.
Tandon, A., C.J.L. Murray, J.A. Salomon, and G. King. (2003). Statistical models for enhancing cross-population comparability. In Health Systems Performance Assessment. Debates, Methods and Empiricism, C.J.L. Murray and D.B. Evans (Eds.). Geneva: World Health Organization.
Tandon, A., C.J.L. Murray, and B. Shengalia. (2004). Measuring health care need and coverage on a probabilistic scale in population surveys. Population Association of America. Available: http://paa2004.princeton.edu/download.asp?submissionId=41208.
Tinetti, M.E., and S.A. Studenski. (2011). Comparative effectiveness research and patients with multiple chronic conditions. New England Journal of Medicine 364(26):2,478-2,481.
Tyagi, R., and S. Kapoor. (2010). Functional ability and nutritional status of Indian elderly. Open Anthropology Journal 3:200-205.
United Nations. (2009). World Population Prospects: The 2008 Revision. New York: United Nations, Department for Economic and Social Information, Population Division.
United Nations. (2011a). World Population Prospects: The 2010 Revision (medium variant). New York: United Nations, Department for Economic and Social Information, Population Division.
United Nations. (2011b). General Assembly resolution A/RES/65/238. New York, USA. United Nations Educational, Scientific and Cultural Organization. International Standard Classification of Education, 1997. (1997). Available: http://www.unesco.org/education/information/nfsunesco/doc/isced_1997.htm.
United Nations Educational, Scientific and Cultural Organization. (2006). ISCED 1997: International Standard Classification of Education (May 2006 re-edition). New York: United Nations. Available: http://www.uis.unesco.org/Library/Documents/isced97-en.pdf.
Wang, H., S. Du, F. Zhai, and B.M. Popkin. (2007). Trends in the distribution of body mass index among Chinese adults, aged 20-45 years (1989-2000). International Journal of Obesity 31(2):272-278.
Wang, L., L. Kong, F. Wu, Y. Bai, and R. Burton. (2005). Preventing chronic diseases in China. The Lancet 366(9,499):1,821-1,824.
Weissman, J.S., and R. Hasnain-Wynia. (2011). Advancing health care equity through improved data collection. New England Journal of Medicine 364:2,276-2,277.
World Health Organization. (2008). Global Burden of Disease: 2004 Update. Geneva: World Health Organization.
World Health Organization. (2010a). World Health Report 2010. Health Systems Financing: The Path to Universal Coverage. Geneva: World Health Organization.
World Health Organization. (2010b). World Health Day 2010. Why Urban Health Matters. Geneva: World Health Organization. Available: http://www.who.int/world-health-day/2010/media/whd2010background.pdf.
World Health Organization. (2011, 29 April). Moscow Declaration. First Global Ministerial Conference on Healthy Lifestyles and Noncommunicable Disease Control. Available: http://www.who.int/nmh/events/moscow_ncds_2011/conference_documents/moscow_declaration_en.pdf.
Yang, W., J. Lu, J. Weng, W. Jia, L. Ji, J. Xiao, Z. Shan, J. Liu, H. Tian, Q. Ji, D. Zhu, J. Ge, L. Lin, L. Chen, X. Guo, Z. Zhao, Q. Li, Z. Zhou, G. Shan, and J. He. (2010). China National Diabetes and Metabolic Disorders Study Group. Prevalence of diabetes among men and women in China. New England Journal of Medicine 362:1,090-1,101.























