
The purpose of this chapter is to examine the available evidence on barriers to (that is, factors that reduce use of) and facilitators of (that is, factors that increase use of) high-quality care for posttraumatic stress disorder (PTSD) in military and veteran populations. The chapter first provides an overview of the types of barriers to high-quality PTSD care followed by a historical overview of research on barriers to and facilitators of PTSD treatment and related comorbid conditions for veterans in previous wars, beginning with Vietnam. The chapter then reviews the empirical literature on barriers to and facilitators of care, distinguishing between barriers experienced by service members and veterans in three markedly different health care service delivery environments: in the theater of war, in military treatment facilities in the United States, and in the Department of Veteran Affairs (VA) health care system.
Although the existence of barriers to PTSD care (such as stigma) is widely recognized, empirical evidence on some aspects of these barriers remains sparse. In this chapter, the committee chose to review and place an emphasis on peer-reviewed materials. It also chose to augment peer-reviewed literature with information from military reports (for example, the Mental Health Advisory Team [MHAT] reports), presentations to the committee, and site visit meetings.
A 2008 study by the RAND Corporation of psychologic injuries and associated treatment in military and veteran populations found that 14% of Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) veterans had screened positive for PTSD. The study also found that only slightly more than half the veterans who had psychologic injuries, including
PTSD, received “minimally adequate” treatment for these injuries (Tanielian and Jaycox, 2008). The authors of the report were unable to determine the percentage of veterans with a PTSD diagnosis who received high-quality care for PTSD, but their research strongly suggested that there was a large gap between the number of service members and veterans who had PTSD and the number who received high-quality care for it. That gap represents extensive human suffering and lost productivity. One possible reason for the gap between those who need care and those who are receiving high-quality care is the existence of barriers that prevent access to high-quality care.
Research on posttraumatic care for active-duty service members and veterans has identified a large number of possible barriers to and facilitators of care. Barriers to care exist at the patient, provider, and institutional levels. For example, patient barriers could include concern about the employment effects of seeking treatment for PTSD, a perception that mental health care is ineffective, a lack of information on resources for care, financial concerns, and logistical problems, such as travel distance (Hoge et al., 2004, 2006; Milliken et al., 2007; Warner et al., 2011). For providers, barriers could include lack of training, lack of time, and treatment location issues, such as transportation in the theater of war (MHAT VII, 2011a, b; Sayer et al., 2009b; Warner et al., 2011). At the organizational level, barriers could include rigid organizational requirements for screening and treatment and the competing demands of force readiness in the Department of Defense (DoD). Treatment programs requiring significant time commitments, such as the 3-week Functional and Occupational Rehabilitation Treatment program, are a challenge to receiving treatment because commanders may be hesitant to approve leave for such long periods of time.
Although such external barriers as logistics and financial pressures exist, barriers to care may also be internal and be related to a person’s attitudes and beliefs (Curry et al., 2011). Some internal barriers are closely related to the construct of stigma. Stigma has been defined as a negative and erroneous stereotype about a person (Corrigan and Penn, 1999). The stigma process has been further described as consisting of cues, prejudice, and discrimination (Corrigan, 2004) and may be categorized as public stigma or self-stigma. In public stigma, a naive public exhibits prejudice toward a stigmatized group; self-stigma occurs when members of a stigmatized group internalize public stigma (Corrigan and Watson, 2002). The stigma attached to having a mental illness and receiving a psychiatric diagnosis has been the subject of extensive study in military and in civilian contexts (Britt et al., 2007; Corrigan, 2004; Corrigan and Penn, 1999; Corrigan and Watson, 2002; Hoge et al., 2004; Warner et al., 2011).
An additional type of barrier in the DoD and the VA occurs in the translation of research findings into practice. Factors that contribute to this kind of barrier include application to target settings, research-design issues, and a combination of these (Glasgow and Emmons, 2007). From a public-health perspective, such barriers result from an inability to generalize the results of research studies to representative samples of patients, providers, and practice settings (Zatzick and Galea, 2007).
Another barrier to accessing care is that active-duty service members may have difficulty in keeping regularly scheduled appointments for treatment or may not be able to complete a full treatment regimen because of deployment, transfer of duty station, or work schedule. On the basis of such variations, the committee decided to structure its analysis around separate considerations of the barriers and facilitators in the three most common service sectors for PTSD care: in the theater of war, in domestic DoD settings, and in VA facilities, as illustrated in Figure 9-1.
Adding to the complexity of treating some cases of PTSD, are the high rates of co-occurring medical and psychosocial conditions. Some treatments, however, such as prolonged exposure therapy, are effective for both PTSD and for frequently co-occurring conditions such as depression, other anxiety disorders, alcohol and drug use disorders, and mild traumatic brain injury (TBI). In addition, there is ample evidence that community mental health providers who are not expert in cognitive behavior therapy or PTSD can deliver these treatments effectively.
There have been several assessments of barriers to the use of mental health care in military and veteran populations. As part of the National Vietnam Veterans Readjustment Study, conducted during the 1980s, Kulka (1990) asked veterans about their reasons for not seeking treatment for
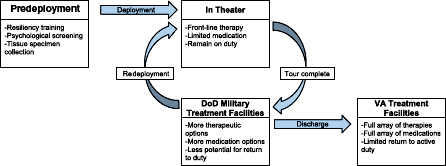
FIGURE 9-1 PTSD services throughout the military life cycle.
their mental health issues. The most frequently cited reasons were the “hope or belief that the individual could solve the problem on his own” and “the hope or belief that the problem would get better on its own.” Vietnam veterans who had PTSD sought mental health care at a higher rate than other veterans, but the authors cautioned that this finding did not support claims that the PTSD programs at that time were sufficient in either quality or accessibility (Kulka, 1990). A report from the Institute of Medicine described barriers to delivery of adequate mental health service for 1990–1991 Gulf War veterans who had unexplained physical symptoms (IOM, 2000). They outlined barriers at the provider level, such as competing demands on provider time. They also identified more tacit barriers, such as lack of provider recognition of the symptom complex as a diagnosable entity and reluctance of patients to discuss their illness. Embedding mental health treatment in primary care settings might help to ameliorate specific barriers, particularly the stigma associated with presenting to specialty mental health settings (IOM, 2000).
A 2008 RAND report on treatment for and the burden of psychologic and cognitive injuries in OEF and OIF, The Invisible Wounds of War, looked at inadequacies in access to care and in the quality of mental health care for the current Iraq and Afghanistan cohort of veterans (Burnam et al., 2008). Burnam et al. (2008) identified two categories of barriers: the first are structural or financial barriers, and include limited availability of services and financial limitations; the second are personal or social barriers, which include personal values and military culture (Figure 9-2).
Several barriers to and facilitators of mental health care in the DoD and the VA health care systems were identified through focus groups and interviews with health providers and OEF and OIF service members and veterans, including reservists and National Guardsmen. Service members rarely considered seeking mental health care in the military health care system because of privacy concerns related to perceived stigma. Many people stated that if they needed care, they would choose to see an off-base provider or seek counseling from a peer or chaplain. The potential loss of a security clearance, loss of professional opportunities, and the adverse judgment of peers were among the feared outcomes most commonly identified. Another barrier was the tendency to not immediately report mental health problems after deployment so as to avoid delay in reuniting with their families. In the words of one focus group participant, “I lied on my post-deployment forms. Whatever got me back to my family quicker” (Burnam et al., 2008). One facilitator of care was the availability of fellow OEF and OIF veterans with whom to share mental health concerns.
Burnam et al. (2008) used the Institute of Medicine (IOM) definition of high-quality care as safe, effective, patient-centered, timely, efficient, and equitable (IOM, 2001). They concluded that a substantial gap existed
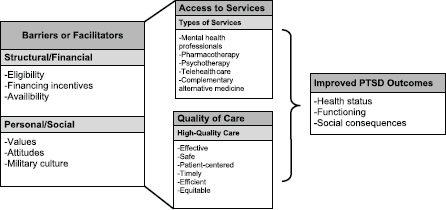
FIGURE 9-2 Barriers to, facilitators of, and access to care for PTSD and related comorbid presentations.
SOURCE: Tanielian and Jaycox, 2008; adapted with permission from RAND Corporation.
between the need for and the use of mental health services for active-duty service members. For veterans who were receiving services in the VA system, the report suggested that improving access would require addressing two major challenges: expanding service capacity and appealing to younger veterans. The authors concluded that both the VA and the DoD should undertake substantial efforts to monitor and enhance the quality of care received by patients who have PTSD.
In the Department of Defense
As discussed in Chapter 4, service members and veterans who have PTSD live, work, and receive mental health care in various settings, ranging from combat zones to specialized PTSD treatment facilities in the VA. Each setting may have specific barriers to and facilitators of care. For example, the use of pharmacotherapy varies markedly depending on the treatment setting (in the theater of war, on U.S. military bases, and in the VA). There are many restrictions on psychiatric medications that a service member may use because of potentially hazardous side effects. Lithium, for example, may not be used in the theater of war, although it is prescribed stateside for service members and is routinely prescribed by the VA. Serotonin reuptake inhibitors, especially selective serotonin and serotonin/ norepinephrine—prescribed for depression, anxiety, PTSD, and some other disorders—are prescribed in the VA and in the DoD, but long-term use
may adversely affect a service member’s career. In the Navy, sailors and marines on selective serotonin reuptake inhibitors cannot carry firearms or deploy unless granted a waiver by their prescribing provider. For other types of psychiatric medications, waivers may be issued case by case by psychiatrists, but the waivers must be consistent with DoD or service-specific guidelines (U.S. Navy, 2009). For some job categories, such as pilot, the use of psychiatric medications while one is on flight status is prohibited (U.S. Air Force, 2009).
In the Theater of War
In the context of service delivery in the theater of war, the best available sources of information on barriers to and facilitators of mental health care are MHAT reports. The series of reports documents improvements in access to mental health treatment in combat settings and the increased need for this treatment for service members who have had multiple deployments. The MHAT reports also show there is persistent stigma and logistical barriers to accessing PTSD care for service members in the theater of war.
In 2003, the first MHAT was assembled and surveyed 756 OIF soldiers, 82% of whom had engaged in combat (MHAT I, 2003). Almost half the soldiers surveyed reported they did not know how to obtain needed mental health services. Only one-third of soldiers who reported they wanted mental health services received the care they needed. That initial MHAT survey recommended immediate improvements in delivery of mental health services, including appointment of in-theater behavioral health consultants and provision of services closer to soldiers’ units (MHAT I, 2003).
Later MHAT surveys have continued to document improvements, but they also have identified barriers to receiving high-quality mental health care in the theater of war. For example, the MHAT II survey, conducted in 2005, found that 40% of soldiers who had mental health problems reported receiving some formal mental health services during their deployment, but stigma and organizational barriers, such as time off to receive care and location of facilities, continued to limit access for many soldiers in the theater of war (MHAT II, 2005).
The MHAT VI survey, conducted in 2009 in Iraq and Afghanistan, differed from previous MHAT surveys in a number of ways. The MHAT VI survey was designed to randomly sample preselected platoons, and sampled units were from both support and sustainment units, and maneuver battalions. Current data were compared with data collected in earlier MHAT surveys to investigate service delivery trends. Of enlisted soldiers in Iraq who reported mental health problems, an estimated 7% (support and sus-tainment sample) and 15% (maneuver sample) did not know that mental health services were available, 16% of support and sustainment soldiers
and 29% of maneuver soldiers thought that it was difficult to get an appointment, 36% and 50% thought that it would be difficult to get time off from work for treatment, 9% and 29% had logistic barriers to obtaining treatment, 15% and 24% were discouraged by their leaders from using mental health services, and 13% and 12% did not know where to get help (MHAT VI, 2009). Sampling of support and sustainment units, and maneuver units deployed to Afghanistan yielded similar results (MHAT VI, 2009). Undertaken in 2010, the joint MHAT VII (surveyed soldiers and marines) extended the findings and assessment methods of previous MHAT surveys. MHAT VII respondents reported the highest level of combat exposures of any MHAT respondents. MHAT VII also reported higher numbers of multiple deployments than MHAT VI. Soldiers on their third and fourth deployments reported increased psychologic problems and use of psycho-tropic medications than soldiers on their first and second deployments, and overall 4% of respondents reported using psychotropic medications. Although enlisted soldiers who screened positive for any mental health problem reported substantial reductions in barriers to mental health care from what was found in MHAT VI, 29% still reported embarrassment as a factor in not seeking mental health services, 29% reported that it would harm their career, 42% reported that their units would have less confidence in them, 46% reported that their leaders might treat them differently, 34% thought that their leaders might blame them for the problem, and approximately 50% reported that they would be seen as weak. Furthermore, 27% reported that mental health services were not available, 29% reported difficulty in getting appointments, 48% reported that it would be difficult to get time off from work for appointments, and 32% reported that it would be too difficult to get to the mental health specialists’ locations. The number of soldiers who reported “I did not know where to get help” (16%) and “my leaders discouraged me from getting services” (14%) were relatively similar to those in the MHAT VI survey. Marines had more mental health concerns in 2010 than in 2006 or 2007 and perceived fewer barriers to mental health care, including reduced stigma associated with receiving mental health care. Mental health providers noted that outreach efforts had been successful in providing behavioral health services outside combat stress control unit locations. Multiple barriers to telehealth delivery were noted by service members and mental health providers (MHAT VII, 2011a, b). Those results show that barriers to seeking care improved but remained.
In Garrison
In one of the earliest studies of soldiers and marines serving in OEF and OIF, Hoge et al. (2004) described mental health service use, stigma, and other barriers to care in four active-duty combat infantry units returning
to the United States after deployment. Soldiers and marines who screened positive for mental health problems reported significantly higher rates of perceived barriers than those who screened negative. Of those who screened positive for PTSD, depression, or anxiety disorders, 38% of soldiers deployed to Afghanistan, 43% of soldiers deployed to Iraq, and 45% of marines deployed to Afghanistan expressed interest in receiving help; 23%, 40%, and 29% of persons in these respective groups had seen a health care provider in the preceding year, and those that had seen a mental health provider in the past year ranged from 13% in soldiers deployed to Afghanistan to 27% for soldiers deployed to Iraq. Hoge et al. (2004) concluded that efforts to address barriers to and stigma surrounding mental health treatment in the military should include outreach, education, and changes in service-delivery models, such as integration of mental health services into primary care settings in garrison (that is, on permanent military installations).
In a cross-sectional investigation of mental health problems in active-duty service members returning from Iraq and Afghanistan, Hoge et al. (2006) reported that 19% of OIF and 11% of OEF service members reported a mental health problem and that 31% of OIF veterans had at least one mental health visit in the first year after deployment. Approximately 56% of OIF and 48% of OEF service members who were referred for mental health treatment received it. In a follow-up longitudinal assessment of mental health problems and service use, Milliken et al. (2007) found that 20.3% of active-duty and 42.4% of reserve component soldiers required mental health treatment based on their responses to the post-deployment health assessment (PDHA) and post-deployment health reassessment (PDHRA) after returning from Iraq. Furthermore, soldiers were much more likely to report PTSD symptoms on the PDHRA than on the PDHA, and about half of those who reported PTSD symptoms on the PDHA had improved by the time they took the PDHRA.
Warner et al. (2011) assessed reporting of mental health symptoms and needs for care in 2,500 returning OEF and OIF veterans. Study participants completed both the PDHA and an anonymous survey. Items in both surveys were used to assess the presence of PTSD, depression, and suicidal ideation. Reported symptoms of depression, PTSD, and suicide were 2–4 times higher on the anonymous survey than on the PDHA. More than 20% of soldiers who screened positive for PTSD or depression reported discomfort in answering routine PDHA screening items honestly. Those who screened positive for PTSD or depression also had increased perceptions of stigma and barriers. Those results empirically demonstrate the potential effect of stigma on the reporting of mental health symptoms and care seeking. McGeary et al. (2011) documented that persistent concerns of stigma and fear of potential long-term implications, including separation from the military, also inhibit reporting.
A series of other studies examined barriers and stigma associated with receiving mental health care in active-duty military populations. Wright et al. (2009) found that improved unit leadership ratings and high unit cohesion were associated with lower perceptions of stigma and diminished barriers to care; the association persisted after adjustment for mental health symptom levels. Kim et al. (2010) found that active-duty soldiers who reported a mental health problem perceived greater stigma and had significantly lower rates of service use than did National Guard soldiers. Negative beliefs about mental health care and diminished perceptions of unit social support were associated with decreased visits for mental health counseling and education (Pietrzak et al., 2009). Olmsted et al. (2011) determined that soldiers in treatment perceived greater stigma than soldiers not receiving treatment. Two common barriers to receiving care were not being able to ask for help and not being able to admit to having a problem (Stecker et al., 2007).
Research on barriers to, stigma associated with, and facilitators of PTSD care for active-duty service members seeking care stateside has focused on DoD facilities or has not specified the source of care, but service members can also receive care through the TRICARE purchased-care program. Multiple reports have raised concerns about access to and adequacy of mental health services available from TRICARE contract network providers, including the availability of providers who are willing to see TRICARE beneficiaries, the familiarity of TRICARE mental health providers with military culture, and the training and expertise of TRICARE mental health providers (APA, 2007; DoD, 2007; IOM, 2010). The 2010 IOM report on TRICARE and licensed professional counseling found an absence of guidelines or designated scope of practice for a wide array of behavioral health providers who treat TRICARE patients; this led to a recommendation that TRICARE evaluate its goals for level of preparedness and training of all its health care providers. A GAO report (2011a) reviewed access to TRICARE Standard and Extra providers, including an analysis of concerns about access to mental health providers. The report acknowledged the DoD’s efforts in response to earlier reports to address access problems but concluded that serious barriers to access mental health providers, particularly psychiatrists, nevertheless continue. Data for accurately assessing the shortfall in providers or the success of recent DoD initiatives to improve access are still inadequate. Data for determining the degree to which providers have the appropriate training and expertise to treat combat-related PTSD are also lacking.
In its reports to Congress, the DoD has noted the increased use of TRICARE contract mental health providers (GAO, 2011a), which is consistent with what the committee found on its site visit to Fort Hood in September 2011. During the site visit, mental health staff acknowledged
to the committee that a substantial and increasing number of active-duty personnel have been referred to TRICARE contract providers because of inadequate staffing in the military mental health clinics to meet the needs of service members seeking PTSD care.
In the Department of Veterans Affairs
Sayer et al. (2009a, b) used qualitative interviews with patients and providers to document barriers to and facilitators of care for veterans who have PTSD and are seen in the VA. They conducted in-depth interviews with veterans who were filing claims related to service-connected disability. The investigation identified multiple barriers to treatment, including beliefs that discouraged seeking mental health treatment, concerns about the ability of the health care system to meet a patient’s needs, lack of knowledge about PTSD, treatment access, and trauma-related avoidance. Facilitators of VA services included recognition and acceptance of PTSD, availability of help, beliefs that encouraged seeking treatment, system facilitation (such as promotion of help-seeking by primary care providers), and encouragement of treatment seeking by members of a patient’s social network.
In a study of barriers experienced by providers, Sayer et al. (2009b) interviewed 40 providers in VA clinical teams that provide specialized services for TBI or PTSD. Providers were asked questions about referral processes, assessment and treatment challenges, terminology, comorbidities, and collaborations. They found screening and referral challenges that included false negative TBI screening results; assessment challenges derived from retrospective evaluations of TBI, PTSD, and functional impairments; secondary gain issues; high no-show rates; uncertainty about evidence-based PTSD treatments for mild TBI; lack of coordination of care with other VA services; and questionable availability of services, including psychiatric staffing. Although these two studies are small, they could serve as a model for assessing barriers to PTSD care in the VA.
In 2011, the GAO identified four key barriers that might prevent veterans from seeking mental health care at VA facilities: stigma and beliefs about mental health care, lack of understanding or awareness of mental health care, logistical challenges to accessing mental health care, and concerns about VA health care in general (GAO, 2011b). On the basis of a literature review and interviews with officials of the VA and veteran service organizations, particular concerns included perception by veterans that seeking help would negatively affect their careers, that treatment may be painful and bring up bad memories, and that they would be able to solve their problems without treatment. The VA and veteran service organization officials also noted that barriers affected different demographic groups differently, for example, younger veterans might think that only older veterans
go to the VA for health care, women may perceive the VA health care system as primarily male-oriented, National Guard and reservists may have more concerns about privacy and stigma, and veterans who live in rural locations may have greater distances to travel to receive care.
A 2011 survey of VA mental health care providers in five Veteran Integrated Service Networks (VISNs) found many perceived system barriers to veterans’ seeking mental health care (VA, 2011). Of the 272 providers surveyed (a mixture of social workers, psychologists, psychiatrists, and nurses), 63% could schedule an appointment for a new patient within 14 days in their clinic, but 18% could not see a new veteran for at least 30 days, and 7% thought the waiting time would be longer than 60 days. Some also noted long waiting times for established patients: 25% could see an established patient at the earliest preferred date, 36% within 14 days of the preferred date, 22% within a month, 11% in more than a month, and 7% in more than 60 days. Providers also noted there were waiting times for referrals to specialty mental health care, such as for PTSD or substance abuse. Most (71%) of the providers thought that current staffing levels were inadequate. When they were asked about other system barriers to provision of mental health care, 46% cited a need for more off-hours appointments (evenings and weekends), 27% said that participating in compensation and pension examinations took time they could otherwise spend with patients, and 25% cited shortages of other staff (clerical and scheduling) (VA, 2011).
In a nonrandomized study of rural veterans of all eras who had never enrolled for VA health benefits or had not used VA health services in the preceding 2 years, the primary veteran-reported barrier to accessing health care of any kind was perceived cost (Davis et al., 2011). Of veterans whose last deployment was in Iraq, Afghanistan, or Kuwait, 22% reported a delay in obtaining or an inability to obtain mental health care compared with 5.6% of veterans who had been deployed elsewhere. The study authors suggested that lack of mental health screening and evaluation may also be a barrier to obtaining mental health care.
BARRIERS TO DELIVERY OF EVIDENCE-BASED CARE
As noted in Chapter 7, the VA/DoD clinical practice guideline and other practice guidelines have identified psychosocial treatments—specifically prolonged exposure (PE) and cognitive processing therapy (CPT)—and pharmacologic treatments as having the strongest evidence base for treatment for PTSD. The VA has trained over 4,000 clinicians who provide care in many settings (such as specialized programs, mental health clinics, and Vet Centers) in PE and CPT. The VA has reported adequate capacity to provide CPT or PE for all OEF and OIF veterans who have PTSD and are enrolled in the Veterans Health Administration, and it plans to train
an additional 400 staff in these therapies in 2012 to have the capacity to treat veterans of all eras who have PTSD (Schiffner, 2011). Recently, the VA announced that it plans to hire 1,600 nurses, psychiatrists, psychologists, social workers, and other mental health staff and about 300 administrative support staff (VA, 2012b). Challenges and barriers to delivering CPT and PE identified through surveys of trained providers and program evaluations include the need to modify training to be intensive and experiential with interaction between trainers and trainees, the need to allow continuing consultation and mentorship with experts for at least 6 months after initial training, the need to monitor and quantify treatment provided, the need for adequate time to deliver treatment according to protocol, and the need to be supported by local management (Karlin et al., 2010; Schiffner, 2011).
To address some of those barriers, the VA has trained master trainers to deliver the initial training in each VISN and to serve as local mentors and consultants. By augmenting the VA computerized clinical record to document the number of veterans who have PTSD and are given at least 8 hours of psychotherapy within a 14-week period, the VA will be able to assess performance measures, such as availability and adequacy of CPT and PE treatment at local facilities and in the overall VA system (Schiffner, 2011). Some of the same challenges to implementing VA training initiatives for psychotherapies are relevant to evidence-based pharmacologic treatment for PTSD. Pharmacologic treatment for PTSD can be prescribed by clinicians in multiple venues—including specialized programs, mental health clinics, and primary care practices—and pharmacologic training must be broadly implemented for these providers.
Similar challenges to and solutions for training VA providers in evidence-based treatments for PTSD may be applicable to DoD mental health care. These challenges include the barriers experienced in specific populations (such as deployed troops), comorbid PTSD presentations, substance abuse and dependence, and the need for stabilization and engagement through stepped-care treatment protocols (see Chapter 8).
Some specific active-duty and veteran subpopulations experience different barriers to PTSD care from the veteran population as a whole. For example, Westermeyer et al. (2002) reported that American Indian veterans were less likely to use VA mental health services than other mental health services because of barriers to accessing care, such as lack of VA outreach to them, distrust of the VA, and lack of resources to access the VA. Similarly, women, racial- and ethnic-minority populations, victims of sexual assault sustained during military service, severely wounded veterans, residents of rural areas, and National Guard and reserve populations may all encounter additional barriers to care (Stecker et al., 2007). Data on the prevalence and causes of these population-specific barriers are lacking, but treatment programs and other interventions need to take them into account for optimal
effectiveness. The committee recognizes the importance of barriers to high-quality care experienced by various populations and anticipates further examination of this subject in phase 2 of its study.
As documented in other chapters, evidence-based treatment for PTSD should be provided as soon as feasible, before the disorder becomes chronic or symptoms worsen. The DoD and the VA have made progress in early screening of service members and veterans, respectively, who have or are at risk for PTSD. That progress should be followed by timely access to evidence-based care that integrates evidence-based treatments into a stepped-care, multimodal treatment plan, for example, combining cognitive behavioral therapy with couples therapy. During early engagements with service members or veterans, mental health providers need to be able to treat those who are in crisis while assessing the need for long-term, evidence-based treatment.
This chapter has focused primarily on barriers to accessing care for PTSD. In this section, the committee discusses new approaches that are being used or studied to improve the delivery of mental health services to military and veteran populations. The DoD and the VA are in the forefront of exploring innovative methods for reaching service members, veterans, and their families who are in need of PTSD treatment but for whom the traditional office visit to a mental health provider is not possible. Among the approaches is the use of computers to deliver high-quality person-to-person therapy.
Computing and information technology can address logistical barriers and stigma issues that are present in all service-delivery settings. It has been implemented to different degrees by both the DoD and the VA, which have given users opportunities to access and interact with computing applications (and care providers) for the delivery of clinical services, to participate in anonymous mental health screening, and to access tools that are designed to foster self-awareness and promote a sense of urgency in seeking care. Those opportunities are available to users regardless of their physical location or the time of day. The challenge is to create technologic tools that can provide benefits to users in ways that are ethically sound.
Treatment Delivery Technologies
The rapid and broad adoption of computing and mobile technologies may be opportune in view of the demands that the OEF and OIF conflicts have placed on the DoD and the VA health care systems. Since 2004, numerous recommendations (APA, 2007; DoD, 2007; Dole and Shalala, 2007;
IOM, 2007; Tanielian and Jaycox, 2008) have cited two major needs for improvement: support for randomized controlled trials (RCTs) that assess the efficacy, effectiveness, and implementation of treatment methods and lead to wider dissemination of evidenced-based approaches; and identification and implementation of ways to enhance health care dissemination and delivery for military personnel and their families in ways that provide better awareness of and access to care while reducing stigma.
Telemental Health-Based Interventions
Telemental health (TMH or telemedicine) approaches take advantage of recent advances in computer and information technology that support user interaction with clinicians or clinical applications via low-cost, high-bandwidth connectivity with the Internet. TMH methods constitute more of a delivery medium for providing services to users in remote locations and are not specific to any one model of assessment or treatment. The core methods of TMH delivery are videoteleconferencing (real-time synchronous interaction with a live provider over the Internet), interaction with Internet-based sites that can provide screening assessments and general clinical information (for example, DCoE, 2012, or VA, 2012a), and in some cases programmed guides that allow users to embark on self-managed mental health programming, sometimes supported by additional synchronous or asynchronous interaction with a clinical provider.
In recent years, there has been growing recognition of the value of TMH technologies—such as videoconferencing, Internet use, or telephone use—to conduct therapy for patients who have PTSD (Frueh et al., 2007a). These approaches decrease the burdens of travel time, costs, and time away from work or family and could improve access to services for traditionally underserved populations (for example, patients in rural settings and people who have transportation difficulties or physical disabilities) and people in regions that may be difficult for therapists to reach (such as combat zones). Continuing advances in low-cost, faster, and more sophisticated Internet technologies have led to a substantial investment in TMH infrastructure by government agencies (Godleski et al., 2008), and a growing literature details the structure and mechanics of a variety of TMH applications, as well as research into their effectiveness and efficiency (Frueh et al., 2000; Monnier et al., 2003; Norman, 2006; Richardson et al., 2009).
Videoconferencing
Early research has shown that videoconferencing can be implemented cost-effectively (Bose et al., 2001; Elford et al., 2000; Fortney et al., 2005). Much attention has focused on this medium for providing evidence-based
treatments to veterans, and the VA is promoting telemedicine as an important means of providing care to veterans who live in remote areas (IOM, 2005). Several uncontrolled studies have indicated that telemedicine has resulted in a reduction in PTSD symptoms in veterans (Deitsch et al., 2000; Germain et al., 2009; Morland et al., 2004). For example, Tuerk et al. (2011) administered PE to veterans via videoconferencing and compared responses with those in a sample of veterans who were treated with PE in a standard clinical setting. There were few differences between the two formats, apart from the weekly express posting of the audiorecording of the PE session to the patient. Although the trial was not an RCT, it demonstrated that this delivery mode was safe and resulted in effect sizes comparable with those observed in patients treated the traditional way.
In an initial group-based RCT that compared videoconferencing with standard PE treatment, Frueh et al. (2007b) reported videoconferencing and face-to-face therapy resulted in comparable reductions in symptoms; however, patients who had videoconferencing reported less comfort with therapy and poorer adherence to homework exercises than their counterparts who received treatment in person. A larger nonrandomized study of 89 patients found that whereas telemedicine-delivered PE resulted in significant symptom reduction, it was not as effective as face-to-face treatment (Gros et al., 2011b). Encouraging findings also came from a strongly designed RCT that found comparable results in treating anger in veterans who had PTSD via telemedicine and with in-person therapy (Morland et al., 2010). Such results have supported a growing recognition of the potential usefulness of delivering PE via a telemedicine approach. Large well-controlled trials with OIF and OEF veterans that will permit more definitive conclusions about the effectiveness of this medium are under way (Gros et al., 2011a).
Internet-Based Interventions
Several RCTs of Internet-based treatments for PTSD have been conducted. Litz et al. (2007) assessed DE-STRESS, an 8-week Internet-delivered CBT program, in a military population. Participants were randomly assigned to the DE-STRESS group or an Internet-based supportive counseling program. DE-STRESS entailed therapist-guided exploration of self-monitoring triggers, development of a hierarchy of trauma triggers, stress management, in vivo exposure, trauma writing sessions, and relapse prevention. The treatment group had significantly greater decreases in symptoms of PTSD, depression, and anxiety 6 months after treatment; however, the overall dropout rate was 30%, which is high and reduces the benefit of the intervention (Cukor et al., 2009).
Another Internet-based treatment, Interapy (Lange et al., 2000, 2001, 2003), is a CBT approach that uses exposure and cognitive restructuring
techniques. Interapy involves 2 sessions a week for 5 weeks, during which participants have 10 writing sessions lasting 45 minutes each to describe their trauma in detail, work on cognitive reappraisal, and address their perception of the effect of the trauma on their lives. The largest assessment of Interapy was conducted in a community sample of 69 subjects and 32 wait list controls (Lange et al., 2003). The treatment group improved significantly more than the controls, and there were large effect sizes for PTSD symptoms and general psychopathologic conditions. However, many of the traumas reported in this population may not have met criterion A for PTSD (such as losing a loved one, divorce, or a personal attack). Interapy and DE-STRESS share several intervention components, including repeated writing about the traumatic experience and provision of various levels of therapist assistance (Cukor et al., 2009).
Hirai and Clum (2005) used an Internet-based, 8-week self-help program for traumatic event-related consequences (SHTC) to compare people who had experienced a traumatic event, but had only subclinical PTSD symptoms, with a wait list control group. No therapist aid was provided. SHTC consisted of CBT modules, such as psychoeducation; relaxation training, including breathing retraining, muscle relaxation, and imagery-induced relaxation; cognitive restructuring; and exposure. Participants had to master the material in each module independently before proceeding to the next module. Treatment decreased avoidance behavior, frequency of intrusive symptoms, state anxiety, and depressive symptoms and increased coping skills and coping self-efficacy significantly more than the wait list condition. However, given the low symptom severity in the sample, it is not possible to determine whether a person who has more severe PTSD would benefit from the program without some provider contact.
A recent meta-analysis of outcomes of Internet-based programs for anxiety disorders found that among four wait-list–controlled studies of PTSD yielded preliminary support for the use of Internet-based approaches for PTSD (Reger and Gahm, 2009). In a literature review, Richardson et al. (2009) also found strong evidence of patient satisfaction and successful clinical assessment with Internet-based programs. However, both groups of authors concluded that more evidence is needed on the effectiveness of these approaches for specific mental health diagnoses, such as depression and anxiety disorders. Future research on such Internet-based therapies as DE-STRESS, Interapy, and SHTC should focus on the effectiveness of CBT techniques delivered online to more severely traumatized populations, factoring in ethical and legal considerations regarding the amount of provider contact (Tate and Zabinski, 2004). It should be noted that evidence from research on other mental health problems indicates that rates of attrition after Internet-based interventions are higher in the absence of provider contact to facilitate completion (Gros et al., 2011b).
The pressure of increased demands on the DoD and the VA health care systems and the need to break down barriers to care and to reduce costs will probably support continued interest and research in TMH. From an economics perspective, research has demonstrated cost reductions in providing care with telemedicine and Internet-based applications (Harley, 2006; Jong, 2004; Persaud et al., 2005; Shore et al., 2007a), and this trend will probably continue with advances in low-cost, high-fidelity computer and information technology. However, large-scale studies using robust design and sampling methodology is needed to identify the clinical interventions that can be delivered in this format effectively and ethically. Richardson et al. (2009) report that several telemedicine services for mental health care have been operating for more than 12 years, such as Virginia’s Appal-Link network, South Australia’s Rural and Remote Mental Health Service, and services at the University of Arizona; the University of California, Davis; the University of Michigan; and the University of Nebraska. More robust quantitative indicators of the success or failure of large-scale programs like those may soon be available.
Telemedicine programs will necessarily demand attention to ethical and practice issues. Practice guidelines are gradually emerging (Rizzo et al., 2004; Shore and Manson, 2004; Shore et al., 2007b) to address such issues as protection of privacy and security, standard-of-care assurances, cross-state licensure, practice behavior and treatment approaches, and clinical risk management. Those issues will inform decision making with respect to when care can be delivered via computer and information technology or in person safely and effectively (Hyler and Gangure, 2004; McGinty et al., 2006; Miller et al., 2005; Schopp et al., 2006; Shore et al., 2007b).
Novel technologies being developed to enhance TMH systems will require both clinical and ethical scrutiny. For example, advanced online systems have recently been developed that leverage artificially intelligent “virtual humans” to serve as health care guides and personal screening agents (Rizzo et al., 2011). These systems are undergoing evaluations with service members, veterans, and their families to determine whether such interactive virtual human representations that can be anonymously accessed and interacted with will promote awareness of service options. Such awareness may help people who otherwise might not seek care to jump-start the search for help with a live provider.
Other Facilitators
A recent development has the potential to expand treatment opportunities for service members who have PTSD at bases without large hospitals or mental health care. The National Defense Authorization Act for 2012 lifted a restriction against mental health consultations across state lines and
exempts the requirement that health care providers be licensed in the state in which their patients are treated. Although the state licensure requirements for military health care providers providing care in federal facilities are exempt, the new exemption includes care provided at any location.
A further facilitator to care is the incorporation of PTSD screening, diagnosis, and treatment into primary care settings at military treatment facilities. For example, the U.S. Army RESPECT-Mil model (see Chapters 4 and 6) provides service members with an annual opportunity to discuss any PTSD symptoms with a primary care clinician without the stigma of going to a mental health clinic. Integrated primary care and mental health teams are also being used by the other services such as the Air Force Behavioral Health Optimization Program. Similar collaborative care models are also being implemented in the VA. The development of such models has the potential to greatly expand access to and the acceptability of mental health care for service members and veterans.
Many service members and veterans have PTSD, so there is a growing demand for PTSD treatment services in the DoD and the VA. However, many of the service members and veterans do not seek or successfully access those services. Although there are some published studies of the use of PTSD services and programs in the DoD and the VA, the committee found there is a need for more empirical data on barriers to accessing high-quality PTSD care for military and veteran populations. Information and data related to barriers experienced by service members transitioning from the DoD into the VA health care system and the nature and impact of stigma that is perceived by service members and veterans are lacking.
An overarching goal of the committee’s analysis of barriers and facilitators is to identify ways of improving access to high-quality care. In phase 2, the committee will continue to assess barriers to PTSD care, including barriers that are sex specific, race specific, or ethnicity specific. The committee believes that a sound conceptual framework that comprehensively elucidates barriers to and facilitators of access to high-quality PTSD services can result in effective change.
APA (American Psychological Association). 2007. The psychological needs of U.S. military service members and their families: A preliminary report. Presidential Task Force on Military Deployment Services for Youth, Families and Service Members. Washington, DC: American Psychological Association.
Bose, U., P. McLaren, A. Riley, and A. Mohammedali. 2001. The use of telepsychiatry in the brief counseling of non-psychotic patients from an inner-London general practice. Journal of Telemedicine and Telecare 7:S8-S10.
Britt, T. W., T. M. Greene-Shortridge, and C. A. Castro. 2007. The stigma of mental health problems in the military. Military Medicine 172(2):157-161.
Burnam, M. A., L. S. Meredith, T. C. Helmus, R. M. Burns, R. A. Cox, E. D’Amico, L. T. Martin, M. E. Vaiana, K. M. Williams, and M. R. Yochelson. 2008. Systems of care: Challenges and opportunities to improve access to high-quality care. In Invisible wounds of war: Psychological and cognitive injuries, their consequences, and services to assist recovery, edited by T. L. Tanielian and L. Jaycox. Arlington, VA: RAND Corporation.
Corrigan, J. D. 2004. How stigma interferes with mental health care. American Psychologist 59(7):614-625.
Corrigan, P. W., and D. L. Penn. 1999. Lessons from social psychology on discrediting psychiatric stigma. American Psychologist 54(9):765-776.
Corrigan, P. W., and A. C. Watson. 2002. The paradox of self-stigma and mental illness. Clinical Psychology—Science and Practice 9(1):35-53.
Cukor, J., J. Spitalnick, J. Difede, A. Rizzo, B. O. Rothbaum. 2009. Emerging treatments for PTSD. Clinical Psychology Review 29(8):715-726.
Curry, M. A., P. Renker, S. Robinson-Whelen, R. B. Hughes, P. Swank, M. Oschwald, and L. E. Powers. 2011. Facilitators and barriers to disclosing abuse among women with disabilities. Violence & Victims 26(4):430-444.
Davis, L. L., S. Kertesz, A. Mahaney-Price, M. Martin, K. Tabb, K. Pettey, S. McNeal, U. Granstaff, K. Hamner, M. Powell, M. Hilgeman, A. Snow, M. Stanton, P. Parmelee, M. Litaker, and M. Hawn. 2011. Alabama veterans rural health initiative: A preliminary evaluation of unmet health care needs. Journal of Rural Social Sciences 26(3):74-100.
DCoE (Defense Centers of Excellence). 2012. Afterdeployment.org. http://www.afterdeployment.org/ (accessed January 24, 2012).
Deitsch, S. E., B. C. Frueh, and A. B. Santos. 2000. Telepsychiatry for post-traumatic stress disorder. Journal of Telemedicine and Telecare 6(3):184-186.
DoD (Department of Defense). 2007. An achievable vision: Report of the Department of Defense Task Force on Mental Health. Falls Church, VA: Defense Health Board.
Dole, B., and D. Shalala. 2007. Report of the President’s Commission on Care for America’s Returning Wounded Warriors. Washington, DC: White House.
Elford, R., H. White, R. Bowering, A. Ghandi, B. Maddiggan, K. St John, M. House, J. Harnett, R. West, and A. Battcock. 2000. A randomized, controlled trial of child psychiatric assessments conducted using videoconferencing. Journal of Telemedicine and Telecare 6(2):73-82.
Fortney, J. C., D. E. Steffick, J. F. Burgess, M. L. Maciejewski, and L. A. Petersen. 2005. Are primary care services a substitute or complement for specialty and inpatient services? Health Services Research 40(5):1422-1442.
Frueh, B. C., S. E. Deitsch, A. B. Santos, P. B. Gold, M. R. Johnson, N. Meisler, K. M. Magruder, and J. C. Ballenger. 2000. Procedural and methodological issues in telepsy-chiatry research and program development. Psychiatric Services 51(12):1522-1527.
Frueh, B. C., A. L. Grubaugh, J. D. Elhai, and T. C. Buckley. 2007a. US Department of Veterans Affairs disability policies for posttraumatic stress disorder: Administrative trends and implications for treatment, rehabilitation, and research. American Journal of Public Health 97(12):2143-2145.
Frueh, B. C., J. Monnier, E. Yim, A. L. Grubaugh, M. B. Hamner, and R. G. Knapp. 2007b. A randomized trial of telepsychiatry for post-traumatic stress disorder. Journal of Tele-medicine and Telecare 13(3):142-147.
GAO (U.S. Government Accountability Office). 2011a. Defense health care: Access to civilian providers under TRICARE standard and extra. Washington, DC: GAO.
GAO. 2011b. VA mental health: Number of veterans receiving care, barriers faced, and efforts to increase access. Washington, DC: GAO.
Germain, V., A. Marchand, S. Bouchard, M.-S. Drouin, and S. Guay. 2009. Effectiveness of cognitive behavioural therapy administered by videoconference for posttraumatic stress disorder. Cognitive Behaviour Therapy 38(1):42-53.
Glasgow, R. E., and K. M. Emmons. 2007. How can we increase translation of research into practice? Types of evidence needed. Annual Review of Public Health 28:413-433.
Godleski, L., J. E. Nieves, A. Darkins, and L. Lehmann. 2008. VA telemental health: Suicide assessment. Behavioral Sciences & the Law 26(3):271-286.
Gros, D. F., M. Strachan, K. J. Ruggiero, R. G. Knapp, B. C. Frueh, L. E. Egede, C. W. Lejuez, P. W. Tuerk, and R. Acierno. 2011a. Innovative service delivery for secondary prevention of PTSD in at-risk OIF-OEF service men and women. Contemporary Clinical Trials 32(1):122-128.
Gros, D. F., M. Yoder, P. W. Tuerk, B. E. Lozano, and R. Acierno. 2011b. Exposure therapy for PTSD delivered to veterans via telehealth: Predictors of treatment completion and outcome and comparison to treatment delivered in person. Behavior Therapy 42(2):276-283.
Harley, J. 2006. Economic evaluation of a tertiary telepsychiatry service to an island. Journal of Telemedicine & Telecare 12(7):354-357.
Hirai, M., and G. A. Clum. 2005. An Internet-based self-change program for traumatic event related fear, distress, and maladaptive coping. Journal of Traumatic Stress 18(6):631-636.
Hoge, C. W., C. A. Castro, S. C. Messer, D. McGurk, D. I. Cotting, and R. L. Koffman. 2004. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. New England Journal of Medicine 351(1):13-22.
Hoge, C. W., J. L. Auchterlonie, and C. S. Milliken. 2006. Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. Journal of the American Medical Association 295(9):1023-1032.
Hyler, S. E., and D. P. Gangure. 2004. Legal and ethical challenges in telepsychiatry. Journal of Psychiatric Practice 10(4):272-276.
IOM (Institute of Medicine). 2000. Protecting those who serve: Strategies to protect the health of deployed U.S. forcess. Washington, DC: National Academy Press.
IOM. 2001. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
IOM. 2005. Quality through collaboration: The future of rural health. Washington, DC: The National Academies Press.
IOM. 2007. PTSD compensation and military service. Washington, DC: The National Academies Press.
IOM. 2010. Provision of mental health counseling services under TRICARE. Washington, DC: The National Academies Press.
Jong, M. 2004. Managing suicides via videoconferencing in a remote northern community in Canada. International Journal of Circumpolar Health 63(4):422-428.
Karlin, B. E., J. I. Ruzek, K. M. Chard, A. Eftekhari, C. M. Monson, E. A. Hembree, P. A. Resick, and E. B. Foa. 2010. Dissemination of evidence-based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration. Journal of Traumatic Stress 23(6):663-673.
Kim, P. Y., J. L. Thomas, J. E. Wilk, C. A. Castro, and C. W. Hoge. 2010. Stigma, barriers to care, and use of mental health services among active duty and national guard soldiers after combat. Psychiatric Services 61(6):582-588.
Kulka, R. A. 1990. Trauma and the Vietnam War generation: Report of findings from the National Vietnam Veterans Readjustment Study. New York: Brunner/Mazel.
Lange, A., B. Schrieken, J.-P. van de Ven, B. Bredeweg, P. M. G. Emmelkamp, J. van der Kolk, L. Lydsdottir, M. Massaro, and A. Reuvers. 2000. “Interapy”: The effects of a short protocolled treatment of posttraumatic stress and pathological grief through the Internet. Behavioural and Cognitive Psychotherapy 28(02):175-192.
Lange, A., J. P. van de Ven, B. Schrieken, and P. M. G. Emmelkamp. 2001. Interapy. Treatment of posttraumatic stress through the Internet: A controlled trial. Journal of Behavior Therapy and Experimental Psychiatry 32(2):73-90.
Lange, A., D. Rietdijk, M. Hudcovicova, J. P. van de Ven, B. Schrieken, and P. M. G. Emmelkamp. 2003. Interapy: A controlled randomized trial of the standardized treatment of posttraumatic stress through the Internet. Journal of Consulting and Clinical Psychology 71(5):901-909.
Litz, B. T., C. C. Engel, R. A. Bryant, and A. Papa. 2007. A randomized, controlled proof-of-concept trial of an Internet-based, therapist-assisted self-management treatment for posttraumatic stress disorder. American Journal of Psychiatry 164(11):1676-1683.
McGeary, D., M. Moore, C. A. Vriend, A. L. Peterson, and R. J. Gatchel. 2011. The evaluation and treatment of comorbid pain and PTSD in a military setting: An overview. Journal of Clinical Psychology in Medical Settings 18(2):155-163.
McGinty, K. L., S. A. Saeed, S. C. Simmons, and Y. Yildirim. 2006. Telepsychiatry and e-mental health services: Potential for improving access to mental health care. Psychiatric Quarterly 77(4):335-342.
MHAT I (Mental Health Advisory Team). 2003. Operation Iraqi Freedom (OIF) mental health advisory team (MHAT). Washington, DC: Office of the Surgeon General, United States Army Medical Command.
MHAT II. 2005. Operation Iraqi Freedom (OIF-II) mental health advisory team (MHAT-II). Washington, DC: Office of the Surgeon General, United States Army Medical Command.
MHAT VI. 2009. Mental health advisory team (MHAT) VI Operation Iraqi Freedom 07-09. Washington, DC: Office of the Surgeon, Multinational Force-Iraq and Office of the Surgeon General, United States Army Medical Command.
MHAT VII. 2011a. Joint mental health advisory team 7 (J-MHAT 7) Operation Iraqi Freedom 2010. Washington, DC: Office of the Surgeon General, United States Army Medical Command, Office of the Command Surgeon HQ, USCENTCOM, Office of the Command Surgeon, US Forces Afghanistan (USFOR-A). MHAT VII. 2011b. Joint mental health advisory team 7 (J-MHAT 7) Operation Enduring Freedom 2010. Washington, DC: Office of the Surgeon General, United States Army Medical Command, Office of the Command Surgeon HQ, USCENTCOM, Office of the Command Surgeon, US Forces Afghanistan (USFOR-A).
Miller, T. W., D. C. Burton, K. Hill, G. Luftman, L. J. Veltkemp, and M. Swope. 2005. Tele-psychiatry: Critical dimensions for forensic services. Journal of the American Academy of Psychiatry and the Law 33(4):539-546.
Milliken, C. S., J. L. Auchterlonie, and C. W. Hoge. 2007. Longitudinal assessment of mental health problems among active and reserve component soldiers returning from the Iraq war. Journal of the American Medical Association 298(18):2141-2148.
Monnier, J., R. G. Knapp, and B. C. Frueh. 2003. Recent advances in telepsychiatry: An updated review. Psychiatric Services 54(12):1604-1609.
Morland, L. A., K. Pierce, and M. Y. Wong. 2004. Telemedicine and coping skills groups for Pacific Island veterans with post-traumatic stress disorder: A pilot study. Journal of Telemedicine and Telecare 10(5):286-289.
Morland, L. A., C. J. Greene, C. S. Rosen, D. Foy, P. Reilly, J. Shore, Q. He, and B. C. Frueh. 2010. Telemedicine for anger management therapy in a rural population of combat veterans with posttraumatic stress disorder: A randomized noninferiority trial. Journal of Clinical Psychiatry 71(7):855-863.
Norman, S. 2006. The use of telemedicine in psychiatry. Journal of Psychiatric and Mental Health Nursing 13(6):771-777.
Olmsted, K. L. R., J. M. Brown, J. R. Vandermaas-Peeler, S. J. Tueller, R. E. Johnson, and D. A. Gibbs. 2011. Mental health and substance abuse treatment stigma among soldiers. Military Psychology 23(1):52-64.
Persaud, D. D., S. Jreige, C. Skedgel, J. Finley, J. Sargeant, and N. Hanlon. 2005. An incremental cost analysis of telehealth in Nova Scotia from a societal perspective. Journal of Telemedicine & Telecare 11(2):77-84.
Pietrzak, R. H., D. C. Johnson, M. B. Goldstein, J. C. Malley, and S. M. Southwick. 2009. Perceived stigma and barriers to mental health care utilization among OEF-OIF veterans. Psychiatric Services 60(8):1118-1122.
Reger, M. A., and G. A. Gahm. 2009. A meta-analysis of the effects of Internet- and computer-based cognitive-behavioral treatments for anxiety. Journal of Clinical Psychology 65(1): 53-75.
Richardson, L. K., B. C. Frueh, A. L. Grubaugh, L. Egede, and J. D. Elhai. 2009. Current directions in videoconferencing tele-mental health research. Clinical Psychology-Science and Practice 16(3):323-338.
Rizzo, A. A., D. Strickland, and S. Bouchard. 2004. The challenge of using virtual reality in telerehabilitation. Telemedicine Journal & E-Health 10(2):184-195.
Rizzo, A., T. D. Parsons, B. Lange, P. Kenny, J. G. Buckwalter, B. Rothbaum, J. Difede, J. Frazier, B. Newman, J. Williams, and G. Reger. 2011. Virtual reality goes to war: A brief review of the future of military behavioral healthcare. Journal of Clinical Psychology in Medical Settings 18(2):176-187.
Sayer, N. A., G. Friedemann-Sanchez, M. Spoont, M. Murdoch, L. E. Parker, C. Chiros, and R. Rosenheck. 2009a. A qualitative study of determinants of PTSD treatment initiation in veterans. Psychiatry 72(3):238-255.
Sayer, N. A., N. A. Rettmann, K. F. Carlson, N. Bernardy, B. J. Sigford, J. L. Hamblen, and M. J. Friedman. 2009b. Veterans with history of mild traumatic brain injury and post-traumatic stress disorder: Challenges from provider perspective. Journal of Rehabilitation Research & Development 46(6):703-716.
Schiffner, S. 2011. Data request on mental health providers in the VA, provider training, and the use of complementary and alternative medicine and treatments. Response to data request by the Committee on the Assessment of Ongoing Efforts in the Treatment of PTSD. October 18, 2011. Washington, DC.
Schopp, L. H., G. Demiris, and R. L. Glueckauf. 2006. Rural backwaters or front-runners? Rural telehealth in the vanguard of psychology practice. Professional Psychology: Research and Practice 37(2):165-173.
Shore, J. H., and S. M. Manson. 2004. Telepsychiatric care of American Indian veterans with post-traumatic stress disorder: Bridging gaps in geography, organizations, and culture. Telemedicine Journal (now Telemedicine and E-Health) 10:64-69.
Shore, J. H., E. Brooks, D. M. Savin, S. M. Manson, and A. M. Libby. 2007a. An economic evaluation of telehealth data collection with rural populations. Psychiatric Services 58(6):830-835.
Shore, J. H., D. M. Hilty, and P. Yellowlees. 2007b. Emergency management guidelines for telepsychiatry. General Hospital Psychiatry 29(3):199-206.
Stecker, T., J. C. Fortney, F. Hamilton, and I. Ajzen. 2007. An assessment of beliefs about mental health care among veterans who served in Iraq. Psychiatric Services 58(10):1358-1361.
Tanielian, T. L., and L. Jaycox. 2008. Invisible wounds of war: Psychological and cognitive injuries, their consequences, and services to assist recovery. Arlington, VA: RAND Corporation.
Tate, D. F., and M. F. Zabinski. 2004. Computer and Internet applications for psychological treatment: Update for clinicians. Journal of Clinical Psychology 60(2):209-220.
Tuerk, P. W., M. Yoder, A. Grubaugh, H. Myrick, M. Hamner, and R. Acierno. 2011. Prolonged exposure therapy for combat-related posttraumatic stress disorder: An examination of treatment effectiveness for veterans of the wars in Afghanistan and Iraq. Journal of Anxiety Disorders 25(3):397-403.
U.S. Air Force. 2009. Medical examinations and standards. Air Force Instruction 48-123. Washington, DC: U.S. Air Force.
U.S. Navy. 2009. Subject: Small arms training and qualification. OPNAVINST 3591.1F. Washington, DC: U.S. Navy.
VA (Department of Veterans Affairs). 2011. A query of VA mental health professionals. http://graphics8.nytimes.com/packages/pdf/opinion/editorial/VAMentalHealth.pdf (accessed January 8, 2012).
VA. 2012a. Mission and overview. National Center for PTSD. http://www.ptsd.va.gov/about/mission/mission-and-overview.asp (accessed March 3, 2012).
VA. 2012b. VA to increase mental health staff by 1,900. http://www.va.gov/opa/pressrel/pressrelease.cfm?id=2302 (accessed April 12, 2012).
Warner, C. H., G. N. Appenzeller, T. A. Grieger, S. Belenkly, J. Breitback, J. Parker, C. M. Warner, and C. W. Hoge. 2011. Importance of anonymity to encourage honest reporting in mental health screening after combat deployment. Archives of General Psychiatry 68:1065-1071.
Westermeyer, J., J. Canive, P. Thuras, D. Chesness, and J. Thompson. 2002. Perceived barriers to VA mental health care among upper midwest American Indian veterans—description and associations. Medical Care 40(1):62-71.
Wright, K. M., O. Cabrera, P. D. Bliese, A. B. Adler, C. W. Hoge, and C. A. Castro. 2009. Stigma and barriers to care in soldiers postcombat. Psychological Services 6(2):108-116.
Zatzick, D. F., and S. Galea. 2007. An epidemiologic approach to the development of early trauma focused intervention. Journal of Traumatic Stress 20(4):401-412.
























