
An Operational Definition of Resilience
In response to the project’s statement of task, the workshop series explored the issue of how to define long-term resilience for the Department of Homeland Security (DHS). Experts from different fields of research were brought together to discuss resilience and its relevance to the DHS workforce. The multidisciplinary panel of experts were drawn from the fields of community resilience, individual resilience, and resilience from an occupational health and safety perspective. Fran Norris, an investigator at the National Consortium for the Study of Terrorism and Responses to Terrorism and a professor at Dartmouth University, is an expert in community resilience. She presented findings from a comprehensive interdisciplinary literature review that sought to identify common threads across different ecological levels and to draw some conclusions for the emerging field of community resilience. Robert Ursano is the chair of the department of psychiatry and founding director of the Center for the Study of Traumatic Stress (CSTS) at the Uniformed Services University of the Health Sciences; he is also a leading expert in individual psychiatric responses to trauma, particularly within the first-responder community. Dori Reissman is a senior medical advisor at the National Institute for Occupational Safety and Health and is an expert in the integration of behavioral health and resilience into occupational safety and health policy and practice. Each speaker presented his or her perspective on the issue and then participated in a panel discussion.
Although each speaker presented a nuanced perspective on resilience, there were several common themes that emerged across disciplines (see Box 3-1).
BOX 3-1
Themes from Individual Speakers on Operational Definition of Resilience
- Resilience is a multi-component process
- Resilience is affected by professional and personal factors
- Organizational and individual resilience
- Critical incident-specific and long-term resilience
- Barriers to utilization of services
- The role of leadership
- The use of evidence in developing interventions
DEFINING RESILIENCE FOR COMMUNITIES AND ORGANIZATIONS
The basic notion of resilience is the capacity to bounce back from stress, pressure, or disturbance. Fran Norris proposed that resilience is more than simply a capacity; rather it is a process through which, after a disturbance, a set of adaptive capacities is linked to a positive trajectory of functioning and adaptation. She suggested that the advantage of this definition is that it emphasizes process, patterns of change, and adaptability. Additionally, it works across different ecological levels, such as the community, the organization, and the individual, because it is not context specific. With this definition, the associated outcomes, adaptive capacities, and interventions may vary, but the focus remains on functioning and process.
Norris’s process-oriented definition of resilience includes three layers—adaptation, adaptive capacities, and intervention—and is applicable to individual, community, and organizational resilience (see Figure 3-1). The first layer of the process details the predisaster level of functioning or adaptation and the occurrence of a stressor. Within this model, there are two pathways. Either there is resistance, and in turn, stability and no change, or there is transient dysfunction. Over time, the model shows that, when transient dysfunction occurs, there is either a readaptation, a return to baseline levels of functioning, or continued dysfunction, which indicates some vulnerability to longer-term problems.
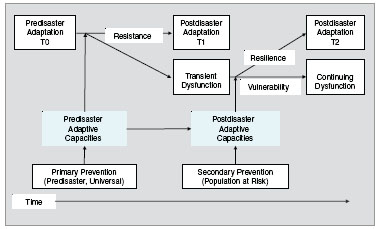
FIGURE 3-1 Proposed model of resilience.
SOURCE: Norris et al., 2008.
The second layer of this model includes the adaptive capacities. These capacities are the focus of much ongoing resilience research. This research seeks to determine which resources, characteristics, and conditions influence the resilience process and affect the trajectory toward postdisaster adaptation described in layer one. Figure 3-2 maps the adaptive capacities for community resilience.
The third layer of the model is the interventions. An intervention prior to an event can target boosting adaptive capacities for resistance. Additionally there are interventions at the time of the event/stressor or afterward. Interventions after the event do not boost resistance but they can support resilience. Norris indicated that there is a longer version of the model that includes longer-term issues and tertiary interventions for recovery that she did not present at the workshop.
Drawing on her research on community resilience and the model described above, Norris outlined several items she felt could contribute to DHS’s definition of organizational resilience. DHS leadership should first identify the desired outcomes. For example, is the department concerned with burnout, absenteeism, and other typical workforce issues, or are there more comlex issues to consider? Secondly what are the primary
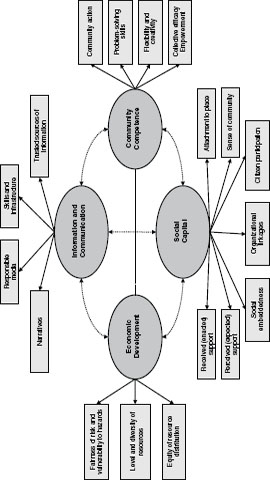
FIGURE 3-2 Adaptive capacities for community resilience.
SOURCE: Norris et al., 2008.
stressors of concern? Has DHS examined what resources matter in these settings? What are the adaptive capacities of the various groups within DHS? Finally, Norris suggested considering what interventions influence each of those adaptive capacities, which in turn may influence the outcomes.
Norris gave examples from the literature of the definitional process for individual and community resilience. The outcome of interest for individual resilience could be wellness. Wellness goes beyond the absence of psychopathology. It also means good behavioral health, quality of life, and effective functioning in role performance. For communities, the primary outcome of interest is population wellness. Population wellness is defined as high and nondisparate levels of mental and behavioral health in the community with good quality of life, as well as effective role functioning and performance.
The research on individual and community resilience can inform DHS’s definition of organizational resilience. Norris suggested that a starting place would be to consider workforce wellness and its similarity to individual wellness and community wellness. Workforce wellness could imply things such as low turnover and absenteeism, and effective role functioning and performance. She pointed out that the basic questions for organizational resilience remain the same as in individual and community resilience. What are the desired outcomes? What are the adaptive capacities in organizations that produce the desired outcomes? What are the interventions that support these adaptive capacities?
Lessons Learned from Community Resilience Research
Norris highlighted several components of community resilience that would be applicable to organizational resilience. One such component is social capital, including social support and social participation.
Social Support
In terms of social support, she pointed to the importance of “buddies” within military communities for social support and wellness. Norris also noted the importance of social participation or the sense of being imbedded within the organization. Social participation can be seen in terms of bonds, roots, and commitments. For an example, she mentioned that although she had not lived there for many years, she still
felt a deep sense of attachment to her hometown of Louisville, Kentucky. In a similar vein, individuals can also have attachments to their organizations.
Communication
Norris suggested that another potentially applicable component is information and communication. This is an area of tremendous importance to communities. When building community resilience, there is an emphasis on “trusted sources of information,” and Norris proposed that the same applies within organizations.
Competency
Community competency is the ability of people to work together, use information, and then make decisions and act. Community competency is dependent on leadership. The leadership on which it is dependent is not just hierarchal leadership—it includes collective action and participatory decision making.
Beyond Psychopathology
Norris emphasized the need to stop thinking of resilience as a personal trait but rather as a process. This shift in thinking has occurred in the field of mental health and has broadened the perspective on resilience beyond psychopathology; the role of stressors and the impact they have on individuals and organizations is important.
Building on Existing Research
Norris also noted that although this workshop series focuses on DHS organizational resilience, it is not necessary for scholars and practitioners in the realm of organizational resilience to start from scratch. They can build on progress in the realms of individual and community resilience. Additionally, there is the long-standing field of organizational psychology and other areas that have performed a great deal of research and have background knowledge, yet they may have never used the word resilience in the literature. Researchers have studied resilience for decades; however, terminology differs across fields.
In his remarks, Robert Ursano agreed with Norris’s assertion that resilience is a process with multiple factors. He identified the four primary factors within the process as (1) mission, (2) organizational function, (3) individual, and (4) time.
Ursano suggested that these factors form a matrix in which all four are interrelated and that a comprehensive program for resilience requires consideration for each section of the matrix. For example, within DHS there are operational and law enforcement missions. Imbedded within each mission there may be response teams, decontamination teams, or administrative tasks such as budgeting. Each of these roles requires different types of personnel and operates on varying timelines. All of these factors vary between missions, and all influence the specific situation.
When considering the four quadrants within the resilience matrix, several significant mediators can serve as risk or protective factors for building resilience. Three of these mediators are leadership, family, and sleep.
Ursano stated that leadership should be considered at all levels and can be a tool for overcoming stigma within law enforcement communities. Leadership also is a means for teaching individuals how to ask for help. Strengthening families is key to sustaining a resilient workforce. Sleep patterns could play a significant role in resilience.
Ursano observed that the type of critical incident that occurs affects the resilience process. He commented that it is always a challenge in first-responder communities to think about fostering operations before an incident versus dealing with the consequences after the fact. To illustrate the effects of critical incidents, Ursano discussed a study of responders to an airplane crash. A month after the crash, the rates of acute stress disorder, post-traumatic stress disorder (PTSD), early dissociative symptoms, depression, and health care utilization among the responders were examined. These rates were compared to a similar group of responders located 90 miles away who were not involved in the incident. The study group of responders experienced higher rates of emotional problems and physical problems, and they were more likely not to obtain needed medical care than the comparison group (Fullerton et al., 2004). Other studies have looked at similar populations (Fullerton et al., 2004; McFarlane and Papay, 1992; North et al., 2002). These studies indicate that first responders develop disaster-specific disorders. First responders
seek care for emotional problems at higher rates. Interestingly they also report needing medical care but not seeking it. These studies are informative, but they do not explain the full picture because they only examined psychiatric disorders and did not include distress or sleep disorders.
Ursano suggested that a key component of DHS’s mission is continuity. Continuity has three Rs embedded in it—redundancy, reliability, and resilience—and specific policies are necessary to sustain all three. An example of redundancy is using three computers instead of one. To ensure reliability, people back up those computers, and people are usually more resilient than organizations. Therefore, it is necessary to sustain individuals because individuals will sustain the organization when all else fails.
When building resilience in individuals, mental and behavioral health issues must be considered. The following list from a 2002 Institute of Medicine (IOM) report illustrates issues related to critical incident responses of individuals (IOM, 2002):
- Mourning
- PTSD
- Depression
- Unexplained somatic symptoms
- Sleep disturbances
- Increased use of alcohol and cigarettes
- Traumatic/complex grief
- Increased family violence and conflict
- Over-dedication to the group
- Helplessness and guilt
- Identification with the victim
Ursano suggested that, when planning to sustain the surge capability in responders, this list also provides insight into individual responses and possible areas to target, such as psychiatric health and behavioral health. One behavioral health problem specific to DHS that was mentioned by multiple workshop speakers and participants was over-dedication. Over-dedication is an issue in nearly every workforce and is a particular issue in DHS and the military. Organizations such as DHS foster over-dedication. Ursano observed that it might be more productive for the
organization to help personnel achieve more balance between their work and personal lives.
Ursano asserts that the key points for DHS to consider in developing its resilience program are defining DHS’s mission in terms of resilience, thinking about organizational versus individual resilience, and considering employee work-life balance needs.
INTEGRATING RESILIENCE INTO HEALTH AND SAFETY
The capacity of individuals to be resilient is tied to the organization’s mission success and productivity and is an element of organizational culture. Dori Reissman suggested that resilience is the ability to adjust rapidly to adversity in a healthy manner and is an integral component of occupational health and safety. She agreed with many of the previous speakers’ comments including concepts such as resilience as a process with a trajectory. She further elaborated on the previous definitions by stating that resilience is connected with preventing injury and illness and making sure individuals are functioning well on the job. This type of public health prevention is much more than a focus on suicide prevention, which represents the most extreme end of the spectrum.
Reissman noted that almost all definitions of resilience are anchored in stressors, and almost all resilience programs target stressors. She noted, however, that certain types and levels of stress can sometimes be helpful when it reasonably motivates individuals to get their work done and to be productive. However, along the concept of continuum, at some point stress levels or types of distress may become pathological and need intervention. In 2002 the National Institute of Mental Health (NIMH) defined stressors as events or conditions that may cause physiological and behavioral reactions and present coping difficulties for the individual experiencing them (NIMH, 2002).
Reissman suggested that work stress must be viewed in context to the employment environment and the psychological fit between worker and supervisor or manager. Therefore, it is intimately tied to the organization’s mission success and productivity. There are several factors in how a job, tasks, or negotiating position are organized that are associated with job stress:
- Job design (task complexity, skill/effort, worker control)
- Scheduling (work-rest schedules, hours of work, shift work)
- Career concerns (job security, growth opportunities)
- Management style (participatory management practices, teamwork)
- Interpersonal relationships (with supervisors and coworkers)
- Organizational characteristics (climate, culture)
Job design is central to many of these factors. Reissman suggested that organizations should consider how they are matching individuals to the tasks, the requirements, pressure, and resources needed to do their job.
Scheduling is an important component of job design, and it not only includes the hours individuals are at work but also the time they spend away from work to recover. Some individuals choose to work long hours because they prefer to and have developed coping skills to deal with the overtime. However, individuals’ coping mechanisms can be overwhelmed by the amount of shift work or high-intensity project work that they have to respond to on an ongoing basis without time to recover.
Reissman noted that career concerns are also an important contributor to job stress. In the current economic climate, job security as well as growth opportunities are primary concerns of many employees.
Management style and interpersonal relationships at work matter. If employees dislike their supervisor, they tend to work around them. When employees step outside the lines of command, it creates an environment ripe for scapegoating. Leaders set the tone for resilience for the workforce, and it is important that the tone is in line with workforce needs.
Organizational characteristics, such as climate and culture, should be assessed to find out what workers think about safety and employee support, and whether appropriate policies are in place to protect and support workers. As mentioned by the previous speakers, DHS operates under many different types of situations. The department responds to events such as extreme weather, man-made disasters like the Deepwater Horizon accident, terrorists’ actions, and calls from concerned citizens. Because of the diversity of activities to which DHS is required to respond, there are two distinct cultures within the department-the law enforcement culture and the emergency management culture. She noted that in order to address resilience for DHS as a whole, it is necessary to consider the different operating principles and values of these two very different cultures.
While it is important to consider the differences between organizational and individual resilience, Reissman emphasized that workforce resilience
feeds into the resilience of the organization. These stressors and subsequent issues with long-term resilience of the workforce can affect DHS at several levels. Long-term exposure to certain types of stressors may not only have negative consequences for the health and welfare of the workforce, but also affect their performance, morale, and motivation as well. The resilience of the workforce can affect the success of the mission.
Reissman suggested that workers’ compensation claims could result from employees working too much and becoming stressed out. For example, cardiovascular complications or accidents can arise from fatigue, and these problems can create cascading effects for years.
Emergency Responder Communities
The National Institute for Occupational Safety and Health (NIOSH) created a logic model for researching work stress that can be applied to homeland security and emergency response entities (see Figure 3-3). The items on the left are inputs into the system. To the right are groups representing work organization and potential exposures. The work organization grouping attempts to capture the stress related to the job and how the work is designed. Reissman modified the model to include issues related to critical incidents and stressors. Although traumatic exposures and experiences appear to be straightforward, in reality, they are not always obvious. There are several important questions to consider: What constitutes psychological trauma? Does this include ongoing exposure to routine everyday stress, or is it narrowly defined as a sudden critical incident? Where do you draw the line?
Riessman suggested that there are many potentially traumatic experiences for first responders and law enforcement personnel. There are threats to personal safety, the inability to control or predict their circumstances, and incongruent events such as witnessing death, mutilation, mass casualties, and violence. There are also personal factors such as the loss of personal attachments, loved ones, a job, or home. These exposures are compounded by sensory overload and sometimes information overload or conflict. Sensory overload can happen if workers are exposed to things that are not typical. For example, at the 9/11 World Trade Center disaster construction workers had to pick up body parts (human remains), which was extremely taxing, outside their occupational training or experience, and resulted in higher rates of PTSD.
The mechanisms included in Figure 3-3 are all interactive. To explain the differences between resistance and resilience, Reissman uses the metaphor that resistance is like a steel bar that is stiff enough to overcome most things until it is broken; resilience is a rubber bar that can be bent out of shape and snap back. The NIOSH model attempts to look at resilience, resistance, and recovery in the face of all the other outcomes related to normal functions of health, illness, injury, dysfunction, and disease.
Reissman noted a couple of resources that have been developed to broaden the understanding of the role of resilience in emergency responder communities. The IOM’s 2002 report on the psychological consequences of terrorism inspired a further evolution of thinking by a federal interagency group considering impacts of an influenza pandemic, which includes building blocks for improving disaster response, mental health, and human behavior. For instance, people’s distress response may be buffered by their resilience capabilities. Those capabilities can depend on (1) how their employer prepares them for success and (2) learning how to help themselves.
Although it is not always possible to prevent mental illness, there are things that can be done to maximize coping and reduce the severity of mental distress and stress-related disorders. From the human behavior side, resilience can affect the productivity of the individual. NIOSH developed the Emergency Responder Health Monitoring and Surveillance Guidebook to implement enhancements for monitoring emergency
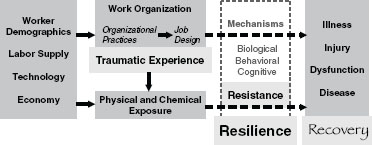
FIGURE 3-3 Causal pathways affecting worker safety and health.
SOURCE: Adapted from NIOSH, 2009.
workers. The guidebook contains lessons learned from large disasters and their affect on workers (NIOSH, 2011). This may be useful for DHS. Although the guidebook is based on lessons from emergency responders, it looks at many issues that are relevant for the entire workforce. These include factors such as the status of an individual, if they are medically fit for the job, and types of services that can support them, such as an employee assistance program.
A key point in Reissman’s presentation was that when the requirements of a job are a poor match to the capabilities, resources, or needs of the worker resilience is compromised. Reissman reiterated that safety and resilience have to be a part of work design and is ultimately a function of leadership.
DEFINING LONG-TERM RESILIENCE PANEL DISCUSSION
At the conclusion of the individual presentations, the speakers participated in a panel discussion. Planning committee member David Sundwall moderated the panel discussion. Questions and comments were taken from all of the workshop participants including the planning committee, summary panelists, and audience members.
Long-Term Resilience Versus Incident-Specific Resilience
Summary panelist Joseph Hurrell suggested that focusing on specific events or disturbances makes it possible to miss the bigger picture. He asked the panelists to comment on resilience in terms of adaptation to disturbances compared to resilience in the context of chronic exposure to stressors on the job. Norris responded that, to some extent, there is an ongoing level of adaptation to the environment that is always stressful. In the field of community resilience, the primary focus is understanding what happens when the environment suddenly and dramatically shifts and the types of stressors change. Ursano added that in the study on critical incidents, ongoing daily hassles, adversities, and disrupted resources contribute to stress in a workplace. Reissman commented that these are all issues that have been examined in other fields of study, including work organization and design, and the problem is that the
different fields often have subtly different jargon, which can create issues finding and translating the information.
Workforce Capacity
Sundwall asked the panelists to comment on the adequacy of the workforce, especially in the treatment of resilience or disaster problems. Reissman agreed that the adequacy of the workforce is a huge issue, and that ongoing demands are taxing the existing staff. She suggested leadership needs to think about workforce adequacy at an organizational level in order to protect the workers. At the basic level, this means understanding what the work demands are, intelligently reformulating how teams meet the demands of the job, and being more flexible in job assignments. Additionally, to avoid silos within the organization, it is good to bring individuals from different teams together for a project. This can be very productive, but it is often problematic because agencies assign people to tasks but then do not relieve them of existing responsibilities. Management of these issues requires effective leadership.
Expanding View of Workforce Supports
There is the perception that there is a grave problem with the adequacy of the workforce, noted Norris. She believes this is largely because people are only thinking about psychiatrists and psychologists. There are other groups who can support individuals, the workforce, and communities. For example, the FEMA-funded crisis counseling program is a step-care model that includes not only professional providers but also peers and others who can provide various types of emotional support. The logic of the model is that resilience requires different levels of interventions, and early intervention can decrease the likelihood that professional interventions are needed later.
Stigma
The issue is not always the availability of services but getting people to utilize the resources, noted Norris. She commented that each of the speakers discussed the problem of stigma and how it affects utilization of mental health and related services. It is important to make sure that the services provided fit the way individuals view their health care needs. Ursano mentioned there are several new programs looking at how to embed
mental health care within primary care, which may help to alleviate the stigma as well.
Work Rewards
Most of what is written about resilience is centered on stressors. Ursano liked that Norris’ presentation and comments shift the resilience discussion out of the pathology mode and asked the panelists to discuss the role of work rewards. Reissman and Norris both felt that work rewards are a valuable component. As an example, Norris discussed a study of individual resilience and the key role of meaning. Being part of an event because you have a role in that event and can make a difference is very different from being part of an event in which you feel victimized by your presence there. Law enforcement or public health personnel know from the outset of an event that they are there for a reason and generally believe they can make a difference. Ursano discussed the concept of “mattering,” which asks “Do I matter to my organization, and does my work have meaning for me?”
Surveillance and Measuring Resilience
Sundwall asked about the role of surveillance and measurement in developing a resilience program, and how to build baseline measures of resilience. Ursano suggested health surveillance in primary care is intended to be a health intervention model. This model is in contrast to models for embedded mental health care within primary care. He went on to say that health surveillance falls into two different categories. One category is the dashboard or the elements of health surveillance information to which an individual already has access. There are a number of items to consider, including accident rates, the number of health visits, absenteeism, and suicide. The other category is active health surveillance that spans everything from postdeployment health assessments to survey health assessments, and from interviews to requiring annual physicals. The World Trade Center is one of the largest health surveillance activities, as is the Deepwater Horizon oil spill. The question of instituting mental health surveillance is on the cutting edge. There are all kinds of health surveillance programs for a variety of conditions, but health surveillance for depression is different. Health surveillance for smoking is linked to smoking cessation programs. Although the Department of Defense is able to do health surveillance for
PTSD, other organizations probably cannot. In addition, primary care providers need to be trained to identify resilience-related health needs and be aware of resources that are available.
Norris commented it is necessary to differentiate between the individual and organization and then the variables or outcomes that can be changed. For instance, self-reported stress is a good marker and could capture information from both individual and collective levels.
Reissman commented that, from an organizational perspective, a key piece to surveillance is management. At the management level, it is possible to get at the presenteeism/absenteeism ratio. However, some of the other metrics mentioned earlier are more difficult, such as disability and injury, because these are typically paid by workers’ compensation. They are important and should be part of the dashboard used by leadership to understand their workforce. On top of that, some issues might happen outside of a formal survey. For instance, do they have management team meetings to raise awareness? What’s the tension level? Is productivity dropping off? Are groups meeting deadlines? It is also important to compare the views of leaders to workers to see if they are concordant. Additionally, there is a program sponsored by the Washington Business Group on Health that puts together an index for corporations assessing health care at work and the kinds of resources required.
Fullerton, C. S., R. J. Ursano, and L. Wang. 2004. Acute stress disorder, post-traumatic stress disorder, and depression in disaster or rescue workers. American Journal of Psychiatry 161(8):1370-1376.
IOM (Institute of Medicine). 2002. Preparing for terrorism: Tools for evaluating the Metropolitan Medical Response System Program. Washington, DC: The National Academies Press.
McFarlane, A. C., and P. Papay. 1992. Multiple diagnosis in posttraumatic stress disorder in the victims of a natural disaster. Journal of Nervous and Mental Disease 180:498-504.
NIMH (National Institute of Mental Health). 2002. Post-traumatic stress disorder (PTSD). Washington, DC: U.S. Department of Health and Human Services.
NIOSH (National Institute of Occupational Safety and Health). 2009. Causal pathways affecting worker safety and health. Modified from Steering Committee on Work Organization and Health. http://www.cdc.gov/niosh/programs/workorg/ (accessed February 16, 2012).
NIOSH. 2011. Emergency responder health monitoring and surveillance. http://www.cdc.gov/niosh/docket/review/docket223/ (accessed February 16, 2012).
Norris, F., S. Stevens, B. Pfefferbaum, K. Wyche, and R. Pfefferbaum. 2008. Community resilience as a metaphor, theory, set of capacities, and strategy for disaster readiness. American Journal of Community Psychology 41(1):127-150.
North, C. S., L. Tivis, J. C. McMillen, B. Pfefferbaum, E. L. Spitznagel, J. Cox, S. Nixon, K. P. Bunch, and E. M. Smith. 2002. Psychiatric disorders in rescue workers after the Oklahoma City bombing. American Journal of Psychiatry 159(5):857-859.
This page is blank


















