
HEALTH LITERACY AND PATIENT-CENTERED CARE
Ana Pujols-McKee, M.D.
The Joint Commission
McKee began her presentation with an anecdote that illustrates how health literacy challenges can be hidden. She was engaged in a telephone conversation with a man who is in his nineties, and she happened to ask, “What are you doing?” The man laughed and responded that he was trying to file something but that he had forgotten the alphabet. Had she not asked what the man was doing when she called, she would not have realized that he was struggling.
The Joint Commission, McKee said, accredits and certifies 19,000 organizations and programs throughout the United States, including hospitals, homecare, nursing homes, and ambulatory health care facilities. The purpose of the accreditation process is to ensure safety and improve outcomes within the organization. The Joint Commission has had experience with health literacy as far back as 2002 when it, in conjunction with the Centers for Medicare and Medicaid Services (CMS), launched the national Speak UpTM campaign.1 Other efforts have included the following:
![]()
1 “In March 2002, The Joint Commission, together with the Centers for Medicare and Medicaid Services, launched a national campaign to urge patients to take a role in preventing health care errors by becoming active, involved, and informed participants on the health
• Hospitals, Language, and Culture: A Snapshot of the Nation (2004)
• What Did the Doctor Say?: Improving Health Literacy to Protect Patient Safety (2007)
• Exploring Cultural and Linguistic Services in the Nation’s Hospitals: A Report of Findings (2007)
• One Size Does Not Fit All: Meeting the Health Care Needs of Diverse Populations (2008)
• Approval of new standards for patient-centered communication (2009)
• Advancing Effective Communication, Cultural Competence, and Patient- and Family-Centered Care: A Roadmap for Hospitals (2010)
• Health Equity Advisory Group—internal to the Joint Commission and supported by a grant from the California Endowment
More recently, the Joint Commission has expanded its scope from health literacy to include effective communication, cultural competencies, and patient- and family-centered care. Effective communication is viewed as a two-way process, where messages are negotiated until information is fully understood by both parties. Cultural competency values diversity and assessments, manages the dynamics of difference, and adapts to diversity. Patient- and family-centered care is an innovative approach to planning, delivering, and evaluating health care. In providing such care organizations establish mutually beneficial partnerships with providers, families, and patients, of all ages.
Joint Commission standards are principles that are based on concepts which drive patient safety, process improvement, and protection of patient rights. For every standard, there are elements of performance that an organization must demonstrate. Four key areas of standards are applicable to the attributes of a health literate organization described in the paper, McKee said: leadership, human resources or workforce, provision of care, and the rights and responsibilities of individuals.
The standards related to leadership are focused on making sure that the mission, vision, and goals of the hospital support the safety and quality of care, treatment, and services. The more one focuses on concerns of patient safety, the more likely patient safety will capture the attention, imagination, and innovation of the organization’s leadership. Another element of leadership is ensuring that patients with comparable needs receive the same standard of care, treatment, and services throughout the organization.
care team. The program features brochures, posters, and buttons on a variety of patient safety topics.” http://www.jointcommission.org/facts_about_speak_up_initiatives/ (accessed February 4, 2012).
A second area of standards relevant to attributes of health literacy are the human resources standards. The Joint Commission allows the organization to define the qualifications of its staff. That means there is an opportunity, if the organization wishes, to include education in health literacy as a qualification. Staff do participate in ongoing education and training, some of which is required on an annual basis, and this is another area where health literacy could be included. Finally, staff are evaluated to ensure that they are competent to perform their responsibilities. Health literacy could be included here as well.
The third area in which health literacy can be found in the Joint Commission Standards is in the standards that define provision of care. The hospital is expected to provide assessesments and reassessments of all patients. Some of this may be especially pertinent to health literacy, for example, if nurses are asked to assess a patient’s learning preferences. There are many opportunities within this standard of assessment to identify issues of health literaacy. The hospital is also expected to provide education and training, based on each patient’s needs and abilitities. One of the elements of performance for this standard is that every patient should identify his or her needs, which could potentially include issues of health literacy.
The fourth area of standards concerns the rights and responsibilities of individuals. A hospital must honor the patient’s right to give or withold informed consent. However, if one were to closely examine the informed consent process, one might find that many patients do not understand what they are being told. Some of this is due to the way in which information is presented, some is due to time constraints that foster quick interaction, and some is due to the fact that the time at which the discussion is taking place is a very emotional time for the patient.
A new Joint Commission requirement attempts to address some of these issues by calling for patient-centered communication, bilateral communication, or negotiating information until both parties understand fully. The expanded standards now allow a family member, friend, or other individual to be present with the patient for emotional support during the course of the patient’s stay. There is also a requirement that the hospital provide language interpretation and translation services.
The Joint Commission has published a document titled Advancing Effective Communication, Cultural Competence, and Patient- and Family-Centered Care: A Roadmap for Hospitals. One chapter provides a checklist on how to assess an organization’s readiness to make the kinds of cultural changes and competency changes that improve health literacy in the organization, including the ability to use data in an effective way and the readiness of the leadership and the workforce.
McKee said two attributes were most important. The first is “Promot-
ing health literacy as an organization’s responsibility.” When an organization’s leadership is able to recognize a failure in communication with a patient as a system failure, that is a very sophisticated organization. But it probably also means that the organization has a culture of safety well embedded throughout.
The second key attribute is the one that involves identifying high-risk treatments and transitions. Relevant to this is the area of informed consent discussed earlier. Improving health literacy capabilities in this area offers a tremendous opportunity to improve safety.
All of the attributes should be integrated into the operational functions of the organization—into patient safety initiatives, into patient experience initiatives, and into intiatives that involve community outreach or employee engagement.
Those attributes that are potentially unfeasible are the ones that require rich resources. Until there is information about the return on investment for health literacy interventions, it will be difficult to convince organizations, particularly those that are stuggling financially, that it is valuable and important to move forward in those areas.
The Joint Commission is developing a method of evaluation called the Tracer Method. Such a method will trace a patient’s journey throughout the organization, from the point of admission or the emergency room to the patient discharge. In this world of important transitions of care, it is recognized that the tracer must also extend into the patient’s home, with homecare, or into the long-term care facility. Evaluating an organization’s ability to communicate confidently with the patients would be a component in that tracer method.
It is the vision of the Joint Commission that all people, regardless of their level of education, their ability to read, or their ability to understand English should always experience the safest, highest-quality, best-value health care across all settings. That statement is relevant to what makes an organization health literate, McKee said.
John Neuberger
QuadGraphics
QuadGraphics was founded in 1971 and is the second largest printer in the Western Hemisphere, Neuberger said. It has 28,000 employees in 80 facilities in North America, Latin America, and Europe. In the United States the facilities are located in very different kinds of areas—some very large and urban, others small and rural—and language issues arise in
many areas. About 20 years ago QuadGraphics started providing medical care to its employees, including
• primary care clinics with selected subpecialties;
• wellness and preventive medicine programs;
• an occupational medicince program;
• onsite rehabilitation clinics;
• full-services laboratories, X-rays, pharmacies, and dental services;
• third-party benefit administration and utilitzation review;
• robust information systems; and
• telemedicine.
Health literacy is a cornerstone of a successful health care model, Neuberger said. QuadGraphics, as is the case with any employer, needs a healthy and productive workforce that works every day if the company is to remain competitive in a very competitive market. The organization is also concerned about population health for the 50,000 lives covered under its health plan. If the consumers of care are not health literate, it will cost both the company and the patient money. Health literacy is not just an expense, it is an investment. The indirect costs of poor health literacy include low productivity, absenteeism, presenteeism,2 and increased workers compensation claims. The company sees health literacy as one of the cornerstones of managing costs, health, and wellness in consumer-driven care.
Of the eighteen attributes discussed in the commissioned paper, several are important to an employer such as QuadGraphics. One is “Provide an infrastructure to avail frontline providers with educational supports and resources.” It is important to have have reinforcements at the point of service for what the provider (e.g., the physician, the dentist, the pharmacist, or the physical therapist) has just told the patient. It is not enough just to provide a brochure. It is important to work with the patient to be sure that both patient and provider understand the issues involved in care and agree on what needs to be done to take care of the condition. In the company’s clinics 30 minutes per provider is allowed for each visit. The company is willing to pay for this because it believes that allowing that amount of time is effective in promoting health. It provides time for the patient to focus not only on their ailment, but on prevention and wellness issues, such as losing weight, stopping smoking, and family problems.
![]()
2 Presenteeism is “the measure of lost productivity cost due to employees actually showing up for work, but not being fully engaged and productive mainly because of personal health and life issue distractions.” http://ezinearticles.com/?Presenteeism-The-Hidden-Costs-of-Business&id=40408 (accessed February 5, 2012).
While interaction at the time of service is key, it is also important for the patient to leave with appropriate written materials or a website reference that reinforces the information exchanged between provider and patient. Even if the patient understands the information at the time of the visit, it is likely that memory and understanding will fade with time. Reinforcement of information is especially important for patients with chronic conditions that need to continue to be managed.
Another important attribute is “Fosters an augmented and prepared workforce to promote health literacy.” From the company’s perspective this means the presence of integrated health teams to support the provider, including reception staff, the nurse, or others that work in the setting. These staff need to be trained in health literacy and to be sensitive to and understanding of the patient’s needs. With such a team the provider can refer the patient to the appropriate staff for continued support—to the dietician to talk about diet, the hygienist to discuss dental care, or the receptionist to make the call to set up needed tests.
The team should reflect the socio-demographic profiles of the population. Members should be prepared to translate the provider’s directions into language that the patient understands, to check on understanding and comprehension, to encourage questioning, and to focus on actionable information.
Another important attribute is to “Make health plan and health insurance products more transparent.” During open enrollment employees are being asked to make tough choices. They need clear and plain communication. Before any vendor can send information to its employees, QuadGraphics must first review it to make sure it is understandable for the population served. Plan descriptions need to be made more comprehensible so that families choose the right plan for themselves. The company counsels employees who are having difficulty understanding which plan to choose. Employers have a major role to play in health literacy. They need to engage the employee all year, not just at the time of enrollment, and to encourage employees to take resonsibility for their personal health.
“Make systems more navigable for families working through the health care system” is another important attribute for employers. There are huge challenges in attemping to navigate the complicated and fragmented health care environment. Patients need to feel comfortable asking for help.
There are major challenges to implementing policies and programs aimed at becoming a more health literate organization, Neuberger said. There are no immediate financial incentives for health care organizations. Are health care providers really interested in reducing utilization of services under the current fee-for-service basis? Are they serious about reducing emergency room visits, testing, and so on?
Information needs to be easily accessible to employees. QuadGraphics is in the process of creating a webpage that will provide employees with a variety of information related to their health benefits, including medical and pharmacy benefits, flexible spending accounts, and claims information. With such a page employees will no longer have to navigate multiple sites in order to obtain needed information. Employers also need to develop an advocacy role so as to assist patients in choosing and navigating their health plans. Furthermore, employers can assure that all health care materials are properly geared to various populations. That is what QuadGraphics is doing—making sure that the information is relevant to its different populations of employees. Employers have the financial incentives to ensure that their populations are literate and can navigate the health care system.
Employers are willing to work with providers in their communities in order to create healthier populations. For example, there is one small clinic in one of the QuadGraphic communities that wants to become a medical home. To do so requires a nurse care manager to, among other things, monitor patients. But the clinic cannot pay for a full-time care manager. So the clinic approached QuadGrahics asking if the company would be willing to pay half the salary, and it appears that the company will do this because it is a good investment in employee health.
Neuberger concluded by saying that employers are incentivized and can be partners in working with health care organizations to become more health literate. Employers are willing to pay for better outcomes and better care. However, it is important to have a system for documenting improvements—a system that can monitor patients’ understanding of their medical conditions and provide information to develop better practices in order to improve outcomes through improved health literacy.
THE CENTERS FOR MEDICARE AND MEDICAID SERVICES (CMS) PERSPECTIVE
Shari Ling, M.D.
Office of Clinical Standards and Quality
Health literacy is an important topic at a critical time when the country is facing limited resources, Ling said. All of the attributes discussed in the paper are important. They speak to different parts of the system and different issues. Rather than discuss individual attributes separately, Ling bundled them into a few categories and said she thought that it may be worth considering the bundles in terms of what can be done immediately using existing resources versus what requires more long-term solutions. One could also think about them in terms of what is actionable rather
than what is ideal. Finally, perhaps those attributes that require health system redesign could be reframed in terms of what can be accomplished or achieved without a complete redesign—that is, what can be tackled now.
The first of the attributes that is critically important—“Promoting health literacy as an organizational responsibility”—falls into the bundle of culture change and the acknowledgment that culture matters. Culture matters for the patients and for the families; it is the filter through which all information flows. This attribute is fundamental but is also the greatest challenge. Other attributes in this bundle include the following:
• Encourage active inquiry, innovation, evaluation, and improvements.
• Encourage and expect question asking.
• Assess the communication climate.
• Recognize and overcome communication barriers.
• Target population health literacy advisory group.
Another important bundle of attributes relates to attention to content. This is particularly crucial in the area of medication safety and communication about medication safety. Conversations around this issue must balance the risks versus the benefits of the recommended interventions. That conversation is dependent upon the patient understanding and believing what is being said, and understanding requires health literacy.
Infrastructure is another important bundle of attributes. There are long-term and short-term infrastructure requirements. “Provider, patient, and family technical assistance” could be provided immediately by offering educational materials that can actually be read and understood. “Enhancing health care system navigability,” particularly across transitions, could be addressed in the short term. Longer-term infrastructure requirements include “Leveraging health information technology,” “Providing personal health records,” and, again, “Enhancing health care system navigability.”
In an earlier presentation, Darren Townzen had offered a surprising but informative piece of information when he said that even when personal health records are available, they are not necessarily used. What can be done to make them usable? That is a longer term effort that needs to be undertaken, Ling said.
The final bundle of attributes relates to developing needed skills and tools for the workforce, the individual, and the community. There is an opportunity for private and public partnerships to develop and apply techniques that are never taught in medical school, for example, techniques that are based on learning theories. What motivates an individual to learn? How can understanding this motivation be applied in the medi-
cal setting? What lessons can be learned by both providers and patients? The bundle includes the following attributes:
• Assess and track patient comprehension, skills, and problem solving.
• Community resource awareness.
• Provider, patients, and family education resources.
• Promoting health plan and insurance transparency and comprehensibility—access and use.
• Curricula and threshold for health skills.
There are a number of implementation challenges. What will encourage corporations and the health care system to embrace the idea of improving health literacy? From the perspective of the CMS, this requires an evidence base. It also requies acknowledging that perception and perspective matter: A message has to be perceived and understood in order to be acted upon. At a system level it must be recognized that there are burdens on the providers and the system. A provider has a specified number of minutes to collect a patient history, conduct the examination, and develop a plan with recommendations. And this is true even in a system that has powerful electronic health records. Resources are a huge challenge. How can these interventions be paid for? And finally, policy change requires due process. Organizations are usually slow to change. Stakeholder and public engagement and input are critical.
Encouraging the implementation of the attributes starts with a vision and requires both strategy and resources. CMS is a major force and a trustworthy partner for the continued improvement of health and health care for all Americans, Ling said. Figure 6-1 ilustrates the “three-part aim” of CMS. At the center are the patient and the family, which means that the challenge of achieving health literacy is itself at the center.
As for strategy, there is no “silver bullet,” Ling said. Many incentives are needed to change behavior. Changing patient behavior relies on literacy, on comprehension, and on understanding. Changing provider behavior has a different set of challenges, but theories of behavioral intervention apply there, too. Intensive support must be offered for the painstaking work needed to improve.
Figure 6-2 shows the various implementation levers for change. This slide has been presented before with quality at the center, but the concepts apply equally well with health literacy at the center. There are numerous opportunities. The conditions of participation, or COP, can be seen at the bottom of the diagram. CMS writes conditions of participation for all providers. If they want to participate, they must abide by the rules. Perhaps the COP offers an opportunity for encouraging the attributes.
SOURCE: Ling, 2011.
Quality-improvement organizations are a potential lever for observing, studying, planning, and demonstrating improvement, and public acknowlegment of a job well done can provide incentive. Existing quality-improvement sites include Hospital Compare, Home Health Compare, ESRD (End Stage Renal Disease) Compare, and Physician Compare. Perhaps aspects of what matters in health literacy can be integrated into the quality measurement and reporting schemes in these organizations. Can some of the concepts embodied in these attributes, for example, be extracted from the electronic health record in order to support a quality measure construct? If so, that would support an operational and implementation strategy.
Patient safety is another avenue for incentives. Perhaps some of the attributes could be integrated into the patient safety data formats offered by the Agency for Healthcare Research and Quality. Other projects include improving health literacy as a key component. Partnership for Patients, which is focused on reducing hospital readmissions, is predicated on the idea that such reductions can be achieved with increased patient understanding and comprehension. The CMS diabetes disparities project
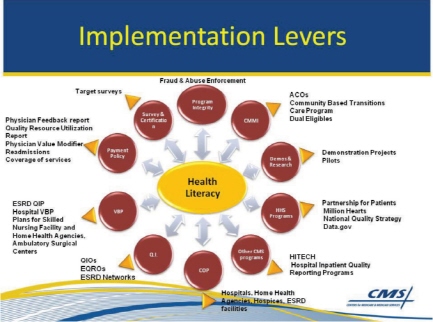
FIGURE 6–2 Implementation levers.
NOTE: Acronyms are as follows: ACOs are accountable care organizations; ARRA is the American Recovery and Reinvestment Act; ASC VBP is ambulatory surgical center value-based purchasing; CAH VBP is critical access hospital value-based purchasing; EQROs are external quality review organizations; ESRD is End-stage Renal Disease; ESRD QIP is End-stage Renal Disease quality incentive program; HH is home health; HITECH is the Health Information Technology for Economic and Clinical Health Act; IQR is inpatient quality reporting; IRF is inpatient rehabilitation facility; LTCH is long term care hospital; OQR is outpatient quality reporting; PRQS is physician quality reporting system; QIOs are quality improvement organizations; SNF is skilled nursing facility; and VBP is value-based purchasing.
SOURCE: Ling, 2011.
addresses cultural competency and improving health literacy through better communication with Medicare beneficiaries in minority and underserved populations.
Ling concluded her presentation by saying that the attributes discussed in the commissioned paper provide an opportunity for moving the important health literacy agenda forward.
Roundtable member Benard Dreyer said that his hospital was recently surveyed by the Joint Commission. During the week that the surveyors spent in the hopsital, not once did anyone ask about anything related to health literacy or health communication, even though they asked about many other specific things. Unless the importance of health literacy is made explicit, he said, hospitals will not pursue it. Because hopsitals are under a variety of pressures, they are only going to respond to those who regulate or pay them. Those are the pressures that create change. How can health literacy be made explicit in the ways that CMS regulates and that the Joint Commission accredits health care organizations?
McKee said that the Joint Commission must achieve a balance between being too prescriptive and too nondirectional. One opportunity is provided by surveyor education and the need for a specific focus on health literacy training. The training should address not only what to look for and discuss with hospital staff, but also what to look for and discuss with patients.
Ling said that health literacy must be spoken about, particularly within the area of care transitions and patient safety. An actionable opportunity for CMS would be to examine its disparities data and to approach health literacy through its quality-improvement efforts.
Roundtable member Will Ross said that the relationship of health literacy to quality was not emphasized in the figure of implementation levers (Figure 6-2). Yet that is what health literacy is about—improving quality. Perhaps the discussion should be reframed, he said. George Isham, the roundtable chair, added that the figure is useful because it provides a guide to potential points of action or influence. Another action pathway to add to the figure would be access to health information technology and other resources for small private practices.
Ling said that the figure is meant to provide a framework of opportunities to think about. Reaching individual physicians and providers is challenging. Avenues in the past have included educational sessions in the context of the physician quality reporting program and electronic health record incentives. Operational health literacy definitions and action items would help tremendously.
Roundtable member Cindy Brach said that employers are important players in encouraging health literate practices and that their purchasing power offers them levels by which change can be encouraged. For example, employers make decisions about which insurance plans to offer and which providers to contract with. How would the attributes discussed in the paper help an employer think about information provided by a health plan and about its health literate practices? For CMS, will the information
in the commissioned paper help with developing surveyor training and checklists they might use?
Neuberger agreed that employers do have a major role to play in health literacy. Everyone has a stake in health literacy. Poor health literacy contributes significantly to the cost of care because if patients do not comprehend what they are supposed to do, they don’t do it, which results in poorer outcomes and greater costs. QuadGraphics has learned not to use acronyms when explaining health plan options, Neuberger said. Providing incentives for preventive care and wellness programs is another way to influence the options chosen.
Ling said that CMS values the concepts of health literacy. The difficulty comes at the operational level. How can the terms be defined in ways that are measurable? What criteria should be used in determining whether an organization is health literate? Is there a scale that could be used and implemented within one of the quality reporting programs? What are the sources of data? Having a data source would make it easier for CMS to achieve health literacy objectives through the survey process or the quality measurement, reporting, and improvement programs.
Brach said that the Agency for Healthcare Research and Quality has developed a health literacy supplement to the Consumer Assessment of Health Providers Survey.3 And the agency is about to finalize an HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) health literacy supplement and is currently working on one for health plans as well. Ling replied that these would be wonderful tools to have. Another thing that is needed, she said, is to demonstrate that health literacy interventions support affordability. Perhaps such efforts could be included in the health care innovation challenge.4
McKee said that there is opportunity to provide education in health literacy. The Joint Commission has sentinel event alerts that attract a great deal of attention. Health literacy might be a topic for an alert. Furthermore, Joint Commission Resources5 might expand its scope of services to include health literacy. Another opportunity is to assess health literacy as a potential contributing factor when conducting a sentinel event review
![]()
3 The supplement “focuses on assessing providers’ activities to foster and improve the health literacy of patients.” https://www.cahps.ahrq.gov/surveys-guidance/item-sets/healthliteracy.aspx (accessed February 5, 2012).
4 A new CMS initiative that “will invest up to $1 billion in support of local innovation in communities across the nation to achieve three-part aim outcomes: better care, better health and lower costs through continuous improvement.” http://innovations.cms.gov/ (accessed February 5, 2012).
5 Joint Commission Resources provides education, publications, consultation, and evaluation regarding accreditation, standards development, good practices, and health care quality improvement. http://www.jcrinc.com/About-JCR/ (accessed February 5, 2012).
or a review of any adverse event. One of the services that the Joint Commission provides to its accredited organizations is being able to review a sentinel event with the organization. There is a team of clinicians who dedicate 100 percent of their time to reviewing these events. Communication is the theme that runs through most of the 900 sentinel events reviewed each year. The traditional approach to a review does not get to the granular detail of the communication defect, but rather it defines the issue in general as a problem in communication. In general, the implications of health literacy may not be identified. If communication is the theme, what often occurs is that the patient misunderstood instructions. The defect is then assumed to be the responsibility of the patient, not the organization or the process. McKee said she would examine how these sentinel reviews could include a process that helps identify opportunities with the organizations to address systemic literacy defects.
Roundtable member Yolanda Partida asked Ling whether she thought there was an opportunity for CMS to create incentives for health promotion and health preservation. Ling responded that CMS can implement incentives within the limits of its authority. It can cover conditions and can pay for medical services for Medicare beneficiaries that include an annual wellness visit. Health risk assessment is still evolving. There is an increasing acknowlegment that behavior matters, yet any new thing proposed must go through rule making, which includes a requirement that CMS consider and respond to every comment. That discussion is an opportunity that plays out in a public forum during the course of rule making.
Roundtable member Clarence Pearson asked Neuberger what arguments could be advanced to employers to encourage them to support health literacy in an environment where employees stay with the same company for only 4 or 5 years on average. Neuberger responded that where turnover is very high, it is more difficult to see a postive return on investment (ROI). Yet for many employers wellness is a core strategy. For employers paying the bills, wellness is a much better investment than sickness.
Roundtable member Ruth Parker said that employers are key stakeholders to engage and are incredibly powerful drivers. What about these attributes is most useful in talking with employers? she asked Neuberger. Neuberger responded that over the past few decades health plans have mediated between the providers and the payers. As a result, employers lost the opportunity to talk with each other on a regular basis. But health care issues and costs are now so significant for employers that they are hungry for discussion. They reach out to hospitals and health systems around the country. Often the health care organizations think the entire discussion is about price. And sometimes it is, but more importantly it
is about outcomes, about creating and maintaining a healthy workforce. Employers want to talk with those providing the care, to work together to face key issues of improving care and outcomes.
Roundtable member Paul Schyve noted that the workshop discussion on how organizations can become health literate involved three different kinds of influences: the role of extrinsic requirements (such as those from regulators or accreditors), the role of intrinsic motivation, and the role of incentives. From the perspective of the Joint Commission, and probably also of CMS, the preference would be to not hear that an organization is doing something because it is required. These groups would rather receive a thank-you for reminding the organization what needs to be done, for evaluating how well it is doing, and for giving advice about how to do it better because only if there is the intrinsic motivation does one have a high level of success.
Either positive incentives (e.g., more pay) or negative incentives (e.g., less money) can be used to encourage the health literacy agenda. But there are also perverse incentives, that is, putting in place an incentive system that keeps an organization from doing what it intrinsically wishes to do. And that, Schyve said, is a major problem in health care today.
The roundtable fosters discussions aimed at developing intrinsic motivation. CMS and the accrediting bodies create extrinsic requirements. And industry is trying to produce incentives as well, although it also has extrinsic requirements in its contracting terms. But if these incentives continue to operate in separate silos the result will be inefficieny and ineffectiveness. All three things are important—intrinsic motivation, extrinsic requirements, and the incentives. At the same time, working collaboratively is needed in order to align these three influences.
Roundtable member Winston Wong agreed with the points that Schyve made in the discussion about extrinsic and intrinsic incentives. Benard Dreyer, while agreeing with the general discussion of intrinsic and extrinsic incentives, said that there are many organizations that do view health literacy as an intrinsic value, but they are under attack because of limited resources.
Ling, S. 2011. Centers for Medicare and Medicaid Services (CMS) Perspective. Presentation at the Institute of Medicine Workshop on Attributes of a Health Literate Organization, November 16. Washington, DC.
















