
Suggested Citation:"Appendix H: Levels of Care." Institute of Medicine. 2013. Substance Use Disorders in the U.S. Armed Forces. Washington, DC: The National Academies Press. doi: 10.17226/13441.
×
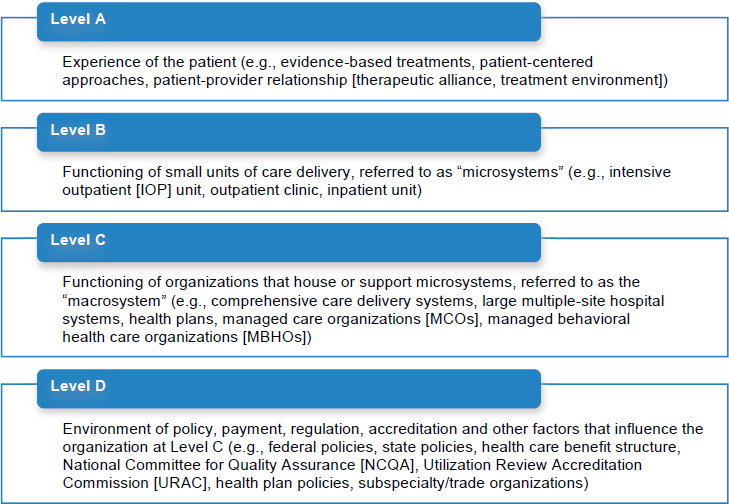
FIGURE H-1 Components of health care delivery systems.
SOURCE: Adapted from Berwick, 2002.
Figure H-1 depicts how the health care environment (i.e., policies, regulation, financing [Level D]), the organizational setting (i.e., health plans
Suggested Citation:"Appendix H: Levels of Care." Institute of Medicine. 2013. Substance Use Disorders in the U.S. Armed Forces. Washington, DC: The National Academies Press. doi: 10.17226/13441.
×
and health systems [Level C]), and the delivery of care (i.e., clinics [Level B]) combine to affect patient care (i.e., the patient experience [Level A]). The committee suggests that these four levels of care provide a blueprint applicable to the development of a 21st-century system of substance use disorder (SUD) prevention and treatment services within the U.S. military.
REFERENCE
Berwick, D. M. 2002. A user’s manual for the IOM’s “quality chasm” report. Health Affairs 21(3):80-90.


