
Chapters 4-7 identified intriguing differences between the United States and other high-income countries that might plausibly contribute to the health gap:
• The U.S. health system suffers from a large uninsured population, financial barriers to care, a shortage of primary care providers, and potentially important gaps in the quality of care (Chapter 4).
• Americans have a higher prevalence of certain unhealthy behaviors involving caloric intake, sedentary behavior, drug use, unprotected sex, driving without seatbelts, and the use of firearms (Chapter 5).
• The United States lags in educational achievement, and it has high income inequality and poverty rates and lower social mobility than most other high-income countries (Chapter 6).
• Americans live in an obesogenic built environment that discourages physical activity, and they live in more racially segregated communities (see Chapter 7).
Although each of these unfavorable patterns could be examined in isolation, the panel was struck by a recurring theme: data compiled from unrelated sources show that the United States is losing ground to other high-income countries on multiple measures of health and socioeconomic well-being. This finding is true for the young and old and perhaps even for affluent and well-educated Americans. Other rich nations outperform the
United States not only on health status but also on protecting children from poverty, educating youth, and promoting social mobility.
It is highly likely that the U.S. health disadvantage has multiple causes and involves some combination of unhealthy behaviors, harmful environmental factors, adverse economic and social conditions, and limited access to health care.1 Although there are a number of explanations for the U.S. health disadvantage, the panel began to consider the possibility that this confluence of problems reflects more upstream, root causes. Is there a “common denominator” that helps explain why the United States is losing ground in multiple domains at once? This pattern began decades ago. As long ago as the 1970s and 1980s, the United States began losing pace with other high-income countries in preventing premature death, infant mortality, and transportation-related fatalities; in alleviating income inequality and poverty; and in promoting education.
More research is needed to determine if there is a common underlying cause, but the panel did discuss possibilities, such as characteristics of life in America that create material interests in certain behaviors or business models. For example, those characteristics include the typically pressured work and child care schedules of the modern American family, the strong reliance on automobile transportation, and delays created by traffic congestion often leave little time for physical activity or shopping for nutritious meals. Busy schedules create a market demand for convenient fast food restaurants.2 It is plausible, but as yet unproven, that societal changes in the United States in the post–World War II period set the stage for many of the deteriorating conditions that appeared in the 1970s and continue to this day.3
Certain character attributes of the quintessential American (e.g., dynamism, rugged individualism) are often invoked to explain the nation’s great achievements and perseverance. Might these same characteristics also be associated with risk-taking and potentially unhealthy behaviors? Are there health implications to Americans’ dislike of outside (e.g., government)
_________________
1Similarly, there are also probably multiple explanations for the health advantages the United States experiences relative to other countries, such as the potential dietary, medical, and policy explanations for the country’s below-average rate of stroke mortality.
2The panel notes the “chicken and egg” question of whether U.S. preferences—for fast foods, traveling in large automobiles, etc.—originated historically from consumer demand or from efforts by companies to create a market for these products and build an infrastructure for them (e.g., highways, drive-in restaurants) that is less prevalent in other rich nations. The currently strong market demand for these products in a society that has grown accustomed to a life-style that depends on these conveniences provides less incentive for businesses to change and strengthens the argument that they are providing products and services that consumers want.
3Some of these trends are increasingly observed in other countries as well.
interference in personal lives and in business and marketing practices? Few quantitative data exist to answer these questions or to assert that these characteristics actually occur more commonly among Americans than among people in other countries.4 Nor is it reasonable to apply a stereotype to an entire society, especially one with the demographic, geographic, and cultural diversity of the United States. Still, for a variety of social or historical reasons, these values have salience for a large segment of U.S. society and may be important in understanding the pervasiveness of the U.S. health disadvantage.
The nature of the interaction between the free market economy and consumer preferences may also be somewhat distinctive in the United States. Manufacturers and other businesses cater to consumer demand for products and services that may not optimize health (e.g., soft drinks and large portion sizes) or, as in the case of cigarettes, are dangerous (Brownell and Warner, 2009). The tobacco industry’s long success in manufacturing and marketing products that have been known for five decades to cause cancer and other major diseases (Kessler, 2001; Lovato et al., 2003) reflects, in part, a symbiotic interdependence between producers and consumers who want (or are addicted to) the products.
Another systemic explanation considered by the panel is whether there is something unique in how decisions are made in the United States, in contrast with other countries, which might produce different policy choices that affect health. Not all of the problems identified in this report are affected by policy decisions—many relate to individual choices or perhaps the inherent nature of life in America—but decisions by government and the private sector may play a role in shaping many of the health determinants discussed throughout this report.
THE ROLE OF PUBLIC- AND PRIVATE-SECTOR POLICIES
The relevance of public policy to health is perhaps most conspicuous in relation to recognized problems in the U.S. health care system—-limited access, especially for people who are poor or uninsured; fragmentation, gaps, and duplication of care; inaccessibility of medical records; and misalignment of physician and patient incentives (Institute of Medicine, 2001, 2010)—and the policies that are designed to address them. But the potential causes of the U.S. health disadvantage go beyond health care practice and policy. People are responsible for their individual behaviors, but individual life-styles are also influenced by the policies adopted by communities, states, and national leaders (Brownell et al., 2010). Cigarette
_________________
4However, there is qualitative evidence regarding these characteristics from research in political science, anthropology, and other social science disciplines.
smoking, second-hand smoke inhalation, and societal norms about smoking are influenced by the price of cigarettes, bans on indoor smoking, and advertising regulations (Brownson et al., 2006; Garrett et al., 2011). The obesogenic environment reflects decisions by the food industry and restaurants about the content and sizes of their offerings; business strategies about where to locate supermarket chains and fast food outlets; ballot decisions on parks, playgrounds, and pedestrian walkways; school board policies on high-calorie cafeteria menus and vending machine contracts; and the marketing of electronic devices to children (Brownell and Warner, 2009; Institute of Medicine, 2006, 2009b, 2009c, 2011c; Nestle, 2002).
Public- and private-sector policies affect drinking and driving, binge drinking, prescription and illicit drug abuse, and the use of contaminated needles by injection drug users. Policies can also influence access to contraceptives and firearms. Both the incidence and lethality of injuries are affected not only by personal choices, but also by decisions made by manufacturers, builders, lawmakers, and regulatory agencies that control product safety, road design, building codes, traffic congestion, law enforcement of safety regulations (e.g., use of seatbelts, blood alcohol testing), fire hazards, and the availability of firearms.
Policies also affect the social and economic conditions in which people live, and the quality of education—from preschool through college and professional schools (Bambra et al., 2010). Political and economic institutions, which help drive the economic success of nations, are subject to a range of public policies (Acemoglu and Robinson, 2012). Tax policy and decisions by employers, business leaders, government, and voters affect job growth, household income, social mobility, savings, and income inequality. They determine the strength of safety net and assistance programs and the quality of the environment, from its physical characteristics (e.g., pollution, housing quality) to social surroundings (e.g., crime, stress, social cohesion). The relevance of macroeconomic government policies on health was exhibited in a natural experiment when East and West Germany unified in 1989-1990: after unification, the mortality rates for the elderly in the eastern part of the country declined to those of the western part (Scholz and Maier, 2003; Vaupel et al., 2003).5
_________________
5The German experience also provides a useful reminder that interventions to improve health outcomes (and address the U.S. health disadvantage) can be effective among older adults. Notwithstanding the importance of addressing the causes of the U.S. health disadvantage among young people (e.g., violence, transportation-related accidents) and the influence of early life conditions on future health trajectories (see Chapter 3), policies to improve the health of middle-aged and older adults are also vitally important.
THE ROLE OF INSTITUTIONAL ARRANGEMENTS
ON POLICIES AND PROGRAMS
Policies that affect public health, education, and the economy are themselves shaped by the institutional arrangements in a society—the governmental and nongovernmental arrangements that organize social relations, rank people into social hierarchies, assign worth, structure employment and the labor market, and address working conditions (Bambra and Beckfield, 2012). As illustrated in Table 8-1, some studies of what has been described as the political economy of health (Muntaner et al., 2011) have demonstrated a positive association between styles of governance and health outcomes. Institutional arrangements in a society determine the population’s entitlement and access to housing, health care, education, pensions, unemployment insurance, collective bargaining, political incorporation, incarceration, and culture (Hall and Lamont, 2009; Krieger et al., 2008; Pinto and Beckfield, 2011). These influences are multilayered and complex. Figure 8-1 presents a model by Hurrelmann and colleagues (2011), which illustrates the multitude of social and political factors that contribute to population health and, by extension, to cross-national differences in health.
The U.S. approach to policies that relate to health and social programs is what sociologists classify as an Anglo-Saxon or liberal model
| Political Theme of Countries | Positive Association with Healtha N (%) | Inverse Association with Healthb N (%) | Mixed Resultsc N (%) | Total N |
| Democracy | 21 (81) | 3(12) | 2(8) | 26 |
| Globalization | 1(17) | 4(67) | 1(17) | 6 |
| Egalitarian political tradition | 9(90) | 1(10) | 0 | 10 |
| Welfare state generosity | 19(61) | 1(3) | 11 (36) | 31 |
| Total N (%) | 50 (69) | 9(14) | 14(19) | 73 (100) |
aPolitical variable demonstrates a positive, direct or indirect, association with a populationrelated health outcome.
bPolitical variable demonstrates a negative, direct or indirect, association with a populationrelated health outcome.
cPolitical variable is either unrelated or inconsistently related to a population-related health outcome.
SOURCE: Adapted from Muntaner et al. (2011, Table 2).
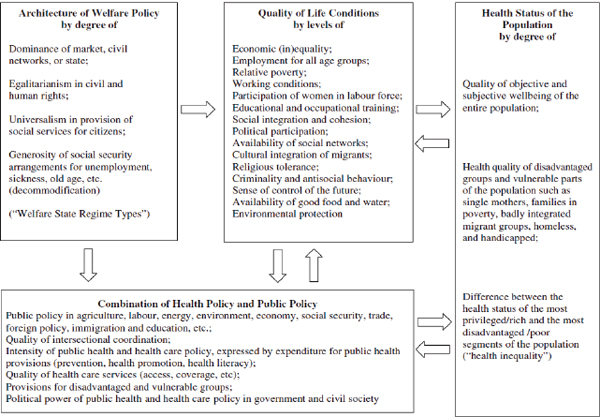
FIGURE 8-1 A model of structural and political influences on population health.
SOURCE: Hurrelmann et al. (2011, Figure 3).
(Esping-Andersen, 1990).6 In this terminology, “liberal” refers to the many English-speaking countries with economies that are more oriented to the free market (with relatively low levels of regulation, taxes, and government services) than other capitalist economies. Sociologists distinguish the Anglo-Saxon/liberal model of the United States and the United Kingdom from countries like Sweden, which operate under a social democratic model in which the state makes generous commitments to full employment, income protection, housing, education, health, and social insurance. Most European welfare programs came into existence after World War II with the goal of providing more universal access to assistance (Bambra and Beckfield, 2012). The social democratic model promotes social equality through wage compression, organized through strong collective bargaining by unions, and tax policies that direct resources to the social security system (Bambra and Beckfield, 2012).7
As detailed in Part I of the report, the Scandinavian (social democratic) countries generally have higher health rankings than the United States, along with more favorable measures of social and economic well-being. As a group, these social democratic countries report longer life expectancies, lower infant mortality rates, and better self-rated health than do liberal countries, including both the United States and the United Kingdom (Bambra, 2005, 2006; Chung and Muntaner, 2007; Coburn, 2004; Eikemo et al., 2008b; Lundberg et al., 2008; Navarro et al., 2003).8Figure 8-2 shows the high infant mortality rates that exist in liberal countries, especially the United States. Figure 8-3 shows that this pattern has existed for decades (Conley and Springer, 2001).
Sociological research is beginning to suggest that the style of governance in a country may exert its own influence on health outcomes, independent of individual-level variables. One study found that whether a country had a social democratic, Anglo-Saxon/liberal, or other sociopolitical model explained 47 percent of the variation in life expectancy between countries (Karim et al., 2010). Another study concluded that the model type predicted approximately 20 percent of the difference in infant mortality
_________________
6As distinct from the meaning of “liberal” as commonly used in the United States to describe left-leaning or progressive social or political ideology.
7A number of other typologies have been proposed: see, for example, Bonoli (1997); Castles and Mitchell (1993); Eikemo and Bambra (2008); Ferrera (1996); Korpi and Palme (1998); Leibfreid (1992); and Navarro and Shi (2001).
8There is substantial between-country variation within Scandinavia (Christensen et al., 2010), and health outcomes in Scandinavian countries are not always the best. For example, mortality rates in Denmark approach those of the United States, and Finland has high mortality rates for some conditions. Similarly, there is substantial between-country variations in Anglo-Saxon/liberal countries, such as the marked differences between the United States and England discussed in previous chapters.
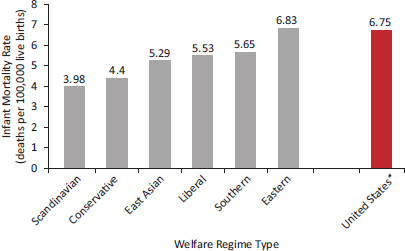
FIGURE 8-2 Infant mortality rate for the United States and 30 other countries, classified by welfare regime type.
*The United States is included in the group of countries classified as having “Liberal” regimes, but it is also presented here in isolation for comparison.
NOTE: Scandinavian countries: Denmark, Finland, Norway, Sweden; Conservative countries: Austria, Belgium, France, Germany, Luxembourg, the Netherlands, Switzerland; East Asian countries: Hong Kong, Japan, Korea, Singapore, Taiwan; Liberal countries: Australia, Canada, Ireland, New Zealand, United Kingdom, United States; Southern countries: Greece, Italy, Portugal, Spain; Eastern countries: the Czech Republic, Hungary, Poland, Slovenia.
SOURCE: Adapted from Karim et al. (2010, Table 5).
rates among countries and 10 percent of the difference in low birth weight (Chung and Muntaner, 2007).
However, the panel notes the limitations of current evidence on this topic, which relies heavily on cross-sectional associations. Such associations often provide only circumstantial evidence; they do not prove a causal effect, and population trends may not apply to individuals (the “ecological fallacy”). Controlled trials to produce more definitive evidence would be untenable, and all studies on this subject must cope with a variety of methodological challenges, such as the potential endogeneity of the political and social environments, as well as issues relating to aggregate efficiency, intertemporal dynamics, and macroeconomic effects. Typologies for regimes, such as welfare states, can be blunt measures that require further refinement to properly differentiate policy nuances across and within countries and to
track changes that affect countries over time.9 For these reasons, among others, research on the effect of welfare states on population health has often produced mixed results and has not fully explained cross-national health patterns. For example, social democratic countries like Sweden had low infant mortality rates early in the 20th century (Regidor et al., 2011), even before the introduction of their social welfare benefits, probably because of improved sanitation and other public health interventions (Burström et al., 2005).
There is little question that the European welfare model is effective in redistributing income and reducing poverty. More universal and generous welfare systems achieve greater income equality than other systems through more generous income transfers through taxes and services (Esping-Andersen and Myles, 2009). These entitlement benefits may buffer the health effects of material deprivation and thereby improve health outcomes but they may have other consequences that are not economically or politically viable in the United States.
Related characteristics of Scandinavian society, such as greater gender equality (Stanistreet et al., 2005) and social cohesion (Putnam, 2000), are also cited as potential explanations for the region’s relatively good health outcomes. Political empowerment of minority groups and women appears especially important to health (Beckfield and Krieger, 2009). As noted in Chapter 7, citizen engagement in the United States, such as voting in elections, is lower than in most other OECD countries (2011e), and the United States has one of the lowest rates of female participation in the national legislature (Congress) (Armingeon et al., 2012).
Scandinavian society is also known for having less income inequality than in the United States (see Chapter 6), a likely product of the welfare state. The Luxembourg Income Study provides evidence that social democratic policies have, over time, substantially reduced income inequality (Alderson and Nielsen, 2002). The Scandinavian welfare programs (universalism, generous wage replacement rates, extensive welfare services) may also narrow income inequalities and provide low-income individuals with greater access to services (Coburn, 2004). However, as discussed in Chapter 6, it remains unclear whether income inequality itself, or the policies that affect income inequality, bear more on the U.S. health disadvantage (Beckfield, 2004).
There is some evidence to suggest that aggregate spending on social programs is associated with better health. One study examined spending
_________________
9The categories assume that all the policies in a particular regime reflect a similar approach and that each category reflects a coherent set of principles, neither of which may be true (Kasza, 2002). No single country adheres to all aspects, and there is internal policy variation within individual welfare states and among the countries of each welfare state regime (Bambra, 2007).
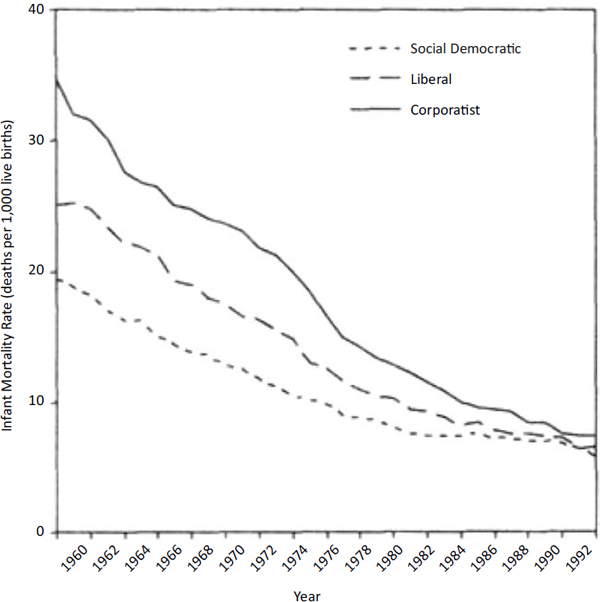
FIGURE 8-3 Infant mortality rates by welfare regime type, 1960-1992.
NOTE: In this study, corporatist countries included Austria, Belgium, France, Germany, and Italy.
SOURCE: Conley and Springer (2001, Figure 3).
on health care and social services in 30 OECD countries and found that U.S. spending on social services (13.3 percent of gross domestic product [GDP]) was less than the OECD average (16.9 percent) and less than that of all countries except Ireland, Korea, Mexico, New Zealand, and the Slovak Republic (Bradley et al., 2011).10 The ratio between spending on
_________________
10Social services expenditures included public and private spending on old-age pensions and support services for older adults, survivors benefits, disability and sickness cash benefits, family support, employment programs (e.g., public employment services and employment training), unemployment benefits, housing support (e.g., rent subsidies), and other social policy areas excluding health expenditures.
social services and health care was 0.91 in the United States and 2.00 in the OECD. More importantly, the study found a significant association between social spending and life expectancy, infant mortality, and potential years of life lost (Bradley et al., 2011).11 Another study also found an association between social spending12 and mortality in an analysis of 15 European countries (Stuckler et al., 2010). According to that study, each additional $100 per capita in social spending was associated with a 1.19 percent decrease in all-cause mortality (Stuckler et al., 2010).
In a commentary about the U.S. health disadvantage, Avendano and Kawachi (2011) noted a number of potentially important differences between the United States and Europe that may affect health: European tax systems are more progressive, child benefits are traditionally available for parents in many countries regardless of income, social programs are generally not restricted to the poor, employment protection is substantially higher, unemployment benefits are more generous, and labor standards for working parents are more extensive. Authors of another study also noted that the United States ranks poorly on measures of full-time employment, public child care, union representation, and parental leave (Pettit and Hook, 2009) (see Table 8-2). Many of these may be less acceptable in the United States because of related tax burdens and other implications.
In seeking a systemic cause for the U.S. health disadvantage, Avendano and Kawachi (2011, p. 4) noted the following:
We have suggested a potentially promising line of inquiry based upon differences in social policy contexts. However, the challenge is obviously to identify the particular social and labor policies that have a causal impact on health and that may contribute to cross-national health differences. For example, do the more generous parental leave policies in Europe contribute to their comparative health advantage? Have employment protection policies contributed to the better health of European workers compared with their U.S. counterparts? The great variation in policy reform during the last 50 years across Europe and the United States provides us with a potentially fruitful set of natural experiments to consider. Broadening the scope of our inquiry to include the social and policy context of nations might help to solve the puzzle of the U.S. health disadvantage.
_________________
11Social spending was also associated with low birth weight, a finding the authors speculated might reflect genetic factors or sociocultural features of the population that were not controlled for in the analysis.
12This study defined social spending as spending related to family support programs (such as preschool education, child care, and maternity or paternity leave), old-age pensions and survivors benefits, health care, housing (such as rent subsidies), unemployment benefits, active labor market programs (to maintain employment or help the unemployed obtain jobs), and support for people with disabilities.
TABLE 8-2 Macro-Level Conditions That Affect Work-Family Policy, by Country, Mid-1990s
| Country | Part-Time Workers* (%) | Children Aged 0–2 in Publicly Funded Child Care (%) | Union Membership of Workforce (%) | Parental Leave, Maximum Weeks* |
| Australia | 21 | 2 | 43 | 0 |
| Austria | 13 | 3 | 37 | 112 |
| Belgium | 14 | 30 | 60 | 67 |
| Canada | 19 | 5 | 33 | 25 |
| Denmark | 23 | 48 | 76 | 28 |
| Finland | 7 | 32 | 75 | 160 |
| France | 15 | 23 | 9 | 162 |
| Germany | 16 | 11 | 27 | 162 |
| Italy | 6 | 6 | 32 | 48 |
| Luxembourg | 8 | 3 | 50 | 16 |
| Netherlands | 36 | 8 | 23 | 68 |
| Norway | 27 | 20 | 53 | 64 |
| Spain | 5 | 5 | 9 | 162 |
| Sweden | 24 | 33 | 88 | 85 |
| United Kingdom | 22 | 2 | 34 | 18 |
| United States | 19 | 5 | 14 | 12 |
*Part-time employment was calculated from self-reports of usual hours worked. Employment was classified as part time when a respondent reported 1–30 hours of work per week. Parental leave represents the maximum number of weeks (paid or unpaid) available.
SOURCE: Data from Pettit and Hook (2009, Table A.2).
Research to date “has far too many black boxes,” note Bambra and Beckfield (2012, p. 29). “Surprisingly, despite vast cross-national variation in population health, and vast cross-national variation in institutional arrangements, very little work connects the two.” It is doubtful that any single aspect of the welfare model could be responsible for the better health outcomes observed in certain countries. Even the reduction in income inequality achieved by this form of capitalism probably results from the interaction and combination of multiple policies (e.g., universal access to welfare services) (Bambra and Beckfield, 2012; Chung and Muntaner, 2007; Navarro et al., 2006).
Nor is the social democratic model a panacea for public health. In what Hurrelmann and colleagues (2011) describe as the “Scandinavian
welfare paradox of health,” social democratic countries that have favorable aggregate health statistics—e.g., average disease rates or life expectancy for the population as a whole—sometimes have steeper within-population health gradients (i.e., larger health inequalities) than do countries governed by other models (Bambra, 2007; Bambra and Eikemo, 2009; Dahl et al., 2006; Eikemo et al., 2008a; Huijts and Eikemo, 2009; Kunst et al., 1998; Lahelma and Lundberg, 2009; Mackenbach et al., 1997, 2000, 2008; Stirbu et al., 2010). Compared with Scandinavian countries, health gradients tend to be lower in Bismarkian countries (e.g., Austria, France, Germany) and Southern Europe (e.g., Italy, Spain) and highest in Eastern European and Baltic countries (Eikemo et al., 2008a). As discussed in Box 8-1, a variety of explanations for the paradox have been proposed (Bambra, 2011; Dahl et al., 2006; Huijts and Eikemo, 2009; Hurrelmann et al., 2011; Mackenbach, 2012).
The United States can take little comfort in debates about why some European countries do better than others in reducing health gradients, because it is still the case that the United States and the United Kingdom generally fare worse than all of them—on both aggregate health status and the steepness of the health gradient (Avendano et al., 2010; Eikemo et al., 2008a). As noted in Chapter 6, at least one study has reported that the health gradient by education is steeper in the United States than in Western European countries (Avendano et al., 2010). These cross-national comparisons certainly shed light on the U.S. health disadvantage, but other factors unique to the United States may also be important in understanding the relatively poor health of Americans, as discussed in the next section.
Social, economic, and public health policies are often an expression of societal values, set against the backdrop of other exigencies (e.g., economic turmoil). For example, the emergence of social democratic regimes in post–World War II Scandinavia was driven in part by their shared values, including a belief in the obligation of society to promote equity and guarantee universal access to assistance as a right of citizenship, regardless of one’s economic means (Esping-Andersen, 1987, p. 86). Social rights were extended at minimal cost to the entire population in a social contract that sought to eliminate status privilege (Bambra and Beckfield, 2012).13
_________________
13Even now, the ministers of the G20 (the group of 19 countries with major economies and the European Union) have been discussing plans to extend “social protection floors” to ensure their populations expanded social protection systems amid current fiscal constraints (International Labour Office, 2011).
BOX 8-1
Explanations for the Scandinavian Welfare Paradox
One proposed explanation for the paradox of greater health inequalities in many Scandinavian welfare states is that lower social strata may have a higher relative concentration of individuals at increased risk of disease. Decades of upward intergenerational social mobility may have increased opportunities for social selection and created more homogenous disadvantaged social groups with such characteristics as low cognitive ability and less favorable personality profiles. The increase of intergenerational social mobility is due primarily to changes in the economy that have led to an expansion of higher education, but to the extent that welfare policies have contributed to making the education system more merit based, they may paradoxically have contributed to a widening of health inequalities (Mackenbach, 2012).
Another proposed explanation is that some European welfare states happen to be further in their epidemiological development, and have now reached the fourth stage of the epidemiological transition in which health improvement depends largely on behavior change (Olshansky and Ault, 1986). This explanation increases the importance of nonmaterial factors—including cultural capital and such personal characteristics as cognitive ability in relation to health—that have become more socially differentiated because they have largely been untouched by the welfare state. To the extent that welfare policies have contributed to making an affluent life-style widely affordable, they may have paradoxically contributed to a widening of health inequalities (Mackenbach, 2012).
Hurrelmann and colleagues raised the following hypothesis in their call for further research on the paradox (2011, p. 16):
If public social expenditures are accompanied by decreased responsibility and influence of private actors and informal corporate institutions, then the social system disincentivises and devaluates the social activities of closely knit social networks and diminishes individual’s perception that they can help themselves. In economic terms, this is tantamount
Conversely, the limited state welfare assistance that exists in East Asian countries (Hong Kong, Singapore, South Korea, Taiwan, and sometimes Japan)—which rely instead on the family and voluntary sector for the social safety net—reflect Confucian social ethics, such as obligation for immediate family members, thrift, diligence, and a strong education and work ethic (Aspalter, 2006; Bambra and Beckfield, 2012; Croissant, 2004; Walker and Wong, 2005).
As in all countries, institutional arrangements in the United States are
to a “crowding out” of informal health institutions. As a consequence, health-promoting strategies within the family, leisure and work settings may be neglected or deemphasized in the social democratic countries. In this respect, conservative countries* with their somewhat stronger reliance on informal social networks may have an advantage vis-à-vis the Scandinavian countries.
Some of these international patterns can probably be explained by between-country variations in the social patterning of health-related behaviors, such as smoking and alcohol consumption. In the Scandinavian countries, inequalities in mortality from smoking-related causes (such as lung cancer and chronic lung disease) and from alcohol-related causes tend to be larger than in many other Western European countries (Mackenbach et al., 2008; Van der Heyden et al., 2009). Survey data show that inequalities in smoking are larger in the north and west of Western Europe than in the south (Cavelaars et al., 2000; Huisman et al., 2005). These geographic patterns reflect differences between countries in the progression of the smoking epidemic: countries in Southern Europe tend to be at an earlier stage in the progression, in which smoking is not yet as strongly socially patterned as in later stages (Lopez et al., 1994).
There is also some evidence to suggest that cross-national variations in inequalities in access or quality of health care may play a role. Socioeconomic inequalities in mortality from conditions that are amenable to medical intervention are particularly large in Eastern Europe (Mackenbach et al., 2008; Stirbu et al., 2010), where inequalities in utilization of health care services also tend to be large (Plug et al., 2012). This proposed explanation would also need further confirmation.
_____________________
*By “conservative,” the authors refer to European political systems such as those in Austria, Belgium, France, Germany, and Italy.
affected by social values and the nation’s historical legacy. On issues that pertain directly to the U.S. health disadvantage—ranging from government regulation to attitudes toward contentious issues, such as firearms or birth control—the policy of the U.S. government and of states and localities often reflect societal priorities and beliefs.
The United States ranks poorly on a number of factors that could explain its health disadvantages. As detailed in Chapters 4-7:
• The public health and medical care systems are more fragmented, and greater barriers exist in access, affordability, and some measures of quality than those in other high-income countries.
• Certain important unhealthy or injurious behaviors are more common in the United States than peer countries, including high-caloric intake, drug misuse, unsafe driving practices, high-risk sex, and the use of firearms.
• Poverty, unemployment, and income inequality are more prevalent than in comparable countries, education has not kept pace with other countries, and social mobility is more limited.
• Land use, the built environment, and the transportation model are less conducive to physical activity; food availability, distribution, and marketing discourage healthy diets; and communities are more heavily segregated by income and race than in other high-income countries.
These conditions reflect multiple factors, including history, governance models, societal values, and priorities that cannot be ignored in trying to understand the U.S. health disadvantage. For example, as discussed in Chapter 4, the lack of universal health insurance coverage sets the United States apart from most high-income nations, but there are reasons this situation has existed for generations. At the same time that countries in Europe were establishing universal access to health services, attempts to do so in the United States, beginning with the Truman administration in the 1940s, met with political resistance, as it still does today (Altman and Shachtman, 2011; Starr, 2011). The resistance has been shaped not only by interest groups, such as medical organizations and health insurance companies, but also by societal beliefs about the proper role of government and the private sector in health care (Freeman and Marmor, 2003). Similarly, to make sense of why Americans are more likely to engage in certain unhealthy behaviors or injurious practices (see Chapter 5), the role of societal values in enacting or resisting countermeasures cannot be ignored.
Yet there is little empirical evidence to prove that values in the United States differ substantially from those in other high-income countries.14 Some evidence on the subject has been gathered from the World Values Survey (World Values Survey Association, 2012) and polling organizations (e.g., World Gallup Poll). The internal and external validity of the indicators and sampling techniques used in such surveys is less than ideal.
_________________
14It is also true that cultural values are not uniform, either within the United States or within other countries, and that such values are dynamic and shift over time (Byrne, 2004; McKee, 2002; Staley, 2001).
However, the panel believes that the individual behaviors and policies of Americans in relation to public health and socioeconomic issues are, to at least some extent, influenced by prevailing values and priorities (Goldberg, 2011). For example, five iconic American beliefs seem especially relevant: individual freedom, free enterprise, self-reliance, the role of religion, and federalism.
Individual Freedom Strong beliefs in individual freedom, as expressed in the Declaration of Independence and Bill of Rights, remain powerful drivers in modern America (Fairchild et al., 2010). As in other countries, Americans struggle with the natural tension between the state’s responsibility to safeguard public health (Institute of Medicine, 2011d) and the rights of people to freely make their own decisions about eating habits, tobacco or alcohol use, and other health-related risky behaviors (Nathanson, 2009). Some personal freedoms carry special significance in the United States, such as the right to bear arms, a constitutional protection that does not exist in most other countries (Glantz and Annas, 2009).
Free Enterprise American society is committed to free-market capitalism and generally eschews restrictions on industries, especially when they impede economic activity or involve an expansion of governmental regulatory authorities. Many aspects of the political process, including the campaign finance system in the United States, give large donors and special interests a degree of influence over the formulation of policy than may exist in other countries (Mann and Ornstein, 2008). Whether regulations are meant to protect public health, assist vulnerable populations, or meet other needs, a popular refrain in the United States is that effective solutions for social and economic problems are best achieved through the free market and more directly by families and their communities (see discussion on self-reliance, below). It is also true that a vibrant and growing economy is good for public health and for the health of the population, that anything that impedes economic growth and flexibility can have detrimental population health effects, and that strategies to boost employment and raise levels of income and wealth can yield important health benefits.
Self-Reliance In a nation founded by pioneers, many Americans believe in the responsibility of individuals, not the state, to solve personal problems: dependency on government welfare programs or “handouts” is discouraged. Thus, raising taxes for state-financed social or health programs is often unpopular with a large proportion of American voters.
In contrast, there is a consensus in many other high-income countries around shared responsibility, solidarity, and the principle that a certain standard of living is a right of citizenship (Bambra and Beckfield, 2012; Esping-Andersen, 1990); this consensus that may not be as pervasive in the United States.
Role of Religion Although the separation of church and state is a core principle in the United States, the United States is less secular than most other high-income countries (Taylor, 2003; World Values Survey Association, 2012), and religious beliefs are often raised in public discourse. Sensitive public health policies, such as those related to contraception or adolescent sexuality, may not be as contentious in other countries (Darroch et al., 2001; Hofstede, 1998; Inglehart and Welzel, 2005; cited by Santelli and Schalet, 2009).15
Federalism The United States originated with a revolution against an overbearing government, and Americans continue to seek limits on the size and budget of government, including agencies responsible for social services, safety, and even health itself. The federalist principles adopted by the nation’s founders reserved limited authorities for the federal government and divided the remainder across the states, which in turn have delegated many authorities to counties and municipalities. Although this decentralized model is an ingenious strategy for separation of powers and is of growing appeal in other countries (Charbit, 2011), the resulting fragmentation complicates attempts to set national policy priorities that many smaller countries with more centralized governments can pursue more easily. It also creates an uneven distribution of resources that might not exist in countries with more centralized models and that often affect the neediest. For example, because authority for so many services rests with the states, the poorest Americans often live in states (e.g., Louisiana, Mississippi) with low tax revenue and small budgets for Medicaid, public schools, and social services.
The potential relevance of these societal values cannot be ignored in attempting to explain the findings documented in this report. Values and priorities create configurations of policies that can act as an upstream underlying cause, or as a systemic explanation for downstream health consequences, as the following examples illustrate:
_________________
15However, sexual content is increasingly prominent in U.S. entertainment media, such as film, television, music, and advertising.
• Constitutional law: The Second Amendment provides an essential context for understanding why civilian firearm ownership is so common in the United States.
• Deregulation: The dramatic rise in the consumption of high-fructose corn syrup in the United States—climbing from zero in 1950 to 63.8 pounds per capita in 2000 (U.S. Department of Agriculture, 2003)—did not occur solely because of consumer demand. The placement of such products on store shelves and restaurant menus was also influenced by business decisions by the food industry, and the reluctance of government to impose regulatory limits on commercial marketing practices (Brunello et al., 2008; Nestle, 2002).
• Taxation: Failed attempts in some U.S. jurisdictions to discourage caloric consumption by applying a tax on carbonated beverages reflects, at least in part, the political influence of strong industry lobbies and consumer resistance to government taxation (Wang et al., 2012).
• Free markets: For years, tobacco companies have defended their right to market and profit from a product that customers purchase and that supports tobacco farmers, despite the major health risks associated with tobacco.
As Box 8-2 discusses in more detail, the policies that may be responsible for the high rate of traffic fatalities in the United States offer a case study of this phenomenon and of the combined impact of social-ecological influences (from individual behavior to public policy) in producing unfavorable health patterns in the United States.
POLICIES FOR CHILDREN AND FAMILIES
Just as the high rate of traffic fatalities could arise from multiple causes, other areas of health disadvantage in the United States are equally complex, both in origin and policy solutions. Many of the problems, such as obesity and diabetes, can be addressed by policies directed at middle-aged or older adults, but a life-course perspective becomes important to fully analyze underlying causes.
Consider the example of childhood obesity. Figure 8-4 shows that energy imbalances that cause weight gain and obesity-related health outcomes originate as early as the prenatal period. While scientists study the responsible physiological mechanisms, such as effects on mood, metabolism, appetite, genes, and the hypothalamic-pituitary-adrenal (HPA) axis
BOX 8-2
The Role of Public Policies on U.S. Traffic Fatalities
In 2011, the National Academies’ Transportation Research Board (TRB) issued a special report, Achieving Traffic Safety Goals in the United States: Lessons from Other Nations. The report was of great interest to this panel both because it examined a major cause of death that sets the United States apart from other high-income countries and because it provides a powerful example of how an in-depth cross-national study can shed light on potential strategies to address an important aspect of the U.S. health disadvantage. As noted in Chapter 1, transportation-related accidents account for 18 and 16 percent for men and women, respectively, of the excess years of life lost before age 50 in the United States.
The TRB study clearly documents how motor vehicle injury is influenced by many different factors:
• economic conditions (traffic fatalities increase with economic growth and higher employment levels);
• traffic characteristics (such as traffic congestion and the mix of pedestrians, cyclists, and vehicle types);
• demographic characteristics (younger populations have higher crash rates);
• alcohol abuse;
• land use (such as miles of road and urban-rural balance) and geographic context, which can influence the success of regulatory measures on traffic accidents;
• vehicle characteristics (such as fleet age and passenger restraints);
• road design and maintenance standards;
• driver behaviors (such as the prevalence of drunk driving, seatbelt use, speeding, and compliance with speed limits and other traffic laws);
• the timeliness and quality of medical care; and
• government safety policies (including those that affect vehicle and road design standards, traffic regulations, enforcement practices, and education and communication activities).
It is worth noting how this list spans multiple health determinants covered in this part of the report—including medical care (Chapter 4), personal/driver behaviors (Chapter 5), environmental factors (Chapter 7), and governmental policies (Chapter 8). Despite this complex array of causal factors, the panel was struck by how closely the TRB committee’s overall findings parallel those documented in Part I of this report. Indeed, the TRB report’s opening paragraph could have been used (with only minor changes) for this report (Transportation Research Board, 2011, p. 7):
The United States is missing significant opportunities to reduce traffic fatalities and injuries.The experiences of other high-income nations and of the U.S. states with the best improvement records indicate the benefits from more rigorous safety programs. Most high-income countries are reducing traffic fatalities and fatality rates (per kilometer of travel) faster than is the United States, and several countries that experienced higher fatality rates 20 years ago now are below the U.S. rate. From 1995 to 2009, annual traffic fatalities declined by 52 percent in France, 39 percent in the United Kingdom, 25 percent in Australia, and 50 percent in total in 15 high-income countries (excluding the United States) for which long-term fatality and traffic data are available, but by only 19 percent in the United States. Some U.S. states have fatality rates comparable to those of the countries with the safest roads; however, no state matches the typical speed of improvement in safety in other countries.
The TRB report’s findings relating to alcohol, seatbelts, and speeding are presented below, followed by the report’s findings on cross-national differences in road design, and finally, the report’s observations about differences in policy making and enforcement.
Alcohol-Related Fatalities
According to the TRB report (p. 150):
[I]n the past decade almost no reduction has been achieved in the annual numbers of fatalities in alcohol-related crashes in the United States…. Although differences in measurement methods complicate comparisons, Germany, Great Britain, Sweden, and Australia all appear to have attained lower rates of alcohol-involved traffic fatalities, per vehicle kilometer of travel and as a fraction of all fatalities, than the United States.
The report went on to identify public policy as the way forward in addressing the problem (pp. 150-151):
Getting progress started again in the United States apparently will require more widespread and systematic application of the proven countermeasures and greater coordination of strategy among law enforcement agencies, the court system, and public health programs aimed at alcohol abuse. […] In countries that have introduced sustained, high-frequency programs of random sobriety testing, including Australia, Finland, and France, reductions of 13 to 36 percent in the frequency of alcohol-involved fatal injury crashes have been achieved. Evaluations
of intensive campaigns of selective testing at sobriety checkpoints in U.S. jurisdictions (following procedures now legal in most states) have reported reductions of 20 to 26 percent in alcohol fatal injury crashes (Shults et al., 2001, 76; Fell et al., 2004, 226). In the United States in 2008, 12,000 persons were killed in crashes involving a driver who was alcohol-impaired (National Highway Traffic Safety Administration, 2009). Therefore, widespread implementation of sustained, high-frequency sobriety testing programs in the United States could be expected to save 1,500 to 3,000 lives annually.
Seatbelts
The TRB report noted that almost every high-income country requires the use of seatbelts, but the share of front seat occupants who use seat-belts is lower in the United States than in many of these countries (see Table 5-1, in Chapter 5). The report noted the effects of decentralized safety regulation (a major theme of the report) and political opposition (p. 181):
The cases of seat belts and of motorcycle helmets … provide clear illustrations of how public and political attitudes can restrain risk-reducing measures despite the availability of effective and well-managed countermeasure programs in many states. The effectiveness of seat belts in reducing casualties and of specific interventions (primary laws and high-visibility enforcement) in increasing usage are well established by research and by the experience of many states. The interventions are not complex or expensive compared with the efforts required for speed control or impaired-driving control. Nonetheless, some jurisdictions have chosen not to apply these measures.
Speed Control
Speeding may contribute to as many as one-third of fatal accidents (Aarts and van Schagen 2006, pp. 220, 223), and speed is an aggravating factor in the severity of all accidents. In light of these findings, the results of a survey by the Governors Highway Safety Association (2005, p. 5) are especially troubling: “[S]tates are becoming increasingly concerned that gains made in the areas of safety restraint usage and impaired driving have been offset by increased fatalities and injuries due to higher speeds.” In addition, the TRB report noted (p. 151):
[I]n contrast, in several of the countries that are making the greatest progress in highway safety, speed control is one of the interventions receiving the greatest attention and resources. If speed control is weakening in the United States, this trend may explain part of the safety performance gap between the United States and other countries.
The TRB report documented how U.S. failures in addressing this problem span research, planning, practice, and policy: see table below. In comparing U.S. policy with efforts in benchmark countries, the report concluded (p. 233):
Successful speed management initiatives in other countries are of high visibility (through publicity and endorsement of elected officials), are long term (sustained for periods of years), target major portions of the road system, use intensive enforcement (e.g., automated enforcement and high penalties), sometimes use traffic-calming road features (such as narrow lanes and traffic circles that cause drivers to reduce speed), and monitor progress toward publicly declared speed and crash reduction objectives. No U.S. speed management program today is comparable in scale, visibility, and political commitment to the most ambitious programs in other countries.
Driving Speed Management in Selected Countries
|
|
||
|
Speed Management Strategy |
France, United Kingdom, and Australia |
United Statesa |
|
|
||
|
Management and Planning |
Focused program with goals, strategy, and budget Timely monitoring and publication of relevant speed and crash data Long-term, multiyear, or permanent perspective |
Routine, low-level activity; reactive management; no long-term plan No speed data; no meaningful crash data Episodic attention; occasional enforcement crackdowns |
|
Technical Implementation of Countermeasures |
Major portions of national or state road network targeted Automated plus traditional enforcement Penalties designed as part of the integrated program |
Haphazard or spot enforcement Automated enforcement not authorized or rarely used Little attention to effectiveness of penalties |
|
Political and Public Support |
Active support and leadership of elected officials; management held accountable for results |
Politically invisible except when speed limits altered or automated enforcement proposed |
|
|
||
aDoes not necessarily include all states.
SOURCE: Transportation Research Board (2011, Table 4-3).
The role of societal values is central in a striking observation by the AAA Foundation for Traffic Safety: “[C]urrent methods for controlling speed are virtually powerless in the face of this [U.S.] speeding culture” (Harsha and Hedlund, 2007, p. 1). This report notes that a successful nationwide program to reduce speeding will require political leadership at the federal, state, and local levels, starting with congressional action, as well as a staged approach to speed control campaigns that includes efforts to increase public awareness and support for these efforts.
Safe Road Design and Highway Network Screening
The TRB report found that definitive studies and data linking highway screening to safety improvements are still missing, but it also found that all countries have design standards for new construction and reconstruction that are intended to improve safety.* The TRB report noted a shift in some benchmark countries’ road programs, which emphasize research on the relationship of design to crash and casualty risk, give higher priority and earlier attention to risk reduction in the design of projects and in project programming, and are more willing to trade a degree of traveler convenience for the sake of safety. Road designers in these countries are expected to quantify the predicted crash frequency and to justify the level of risk in the design.
Political Factors and Public Attitudes
Interestingly, just as the TRB report’s opening paragraph parallels the cross-national mortality patterns observed by this panel, the committee that wrote that report also looked upstream in search of explanations
_________________
*Unlike laws that proscribe risky individual behaviors (such as speeding), highway screening and safe road design aim to make roads inherently safer. Highway screening programs use data to identify places with frequent crashes and then modify these locations to reduce accident risk. The changes can include adjusting alignment, widening shoulders, removing roadside obstacles, improving signage and pavement markings, changing intersections, installing barriers, and increasing traffic law enforcement. When new roads are built or old ones rehabilitated, various design standards can be used to introduce safer road characteristics, including alignment; lane, shoulder, and median widths; sight distance; superelevation (i.e., banking on curves); pavement surface; number of lanes; intersection design; and the roadside environment.
for the U.S. poor performance on traffic safety. The committee noted the following obstacles (p. 14):
• Decentralization: in most benchmark countries, regulation and enforcement are highly centralized, often the responsibility of a single national authority, whereas in the United States, 50 states and thousands of local jurisdictions are responsible for traffic safety and the operation of the highway system;
• Public attitudes that oppose measures common elsewhere: for example, in the United States, motorcycle helmet laws and speed enforcement using automated cameras often encounter active public opposition;
• Weak support for or opposition to rigorous enforcement in legislatures and among the judiciary;
• The constitutional prohibition of unreasonable searches, which prevents police from conducting driver sobriety testing without probable cause, a common practice in some other countries; and
• Resource limitations that prevent enforcement of the intensity common in other countries.
The obstacles are, to an extent, the product of differences in political systems and in the physical characteristics of transportation systems, and possibly of other social and cultural factors.
Many of these underlying explanations are not only applicable to traffic fatalities but also may contribute to other health and injury risks that are more prevalent in the United States than elsewhere (as detailed in this and other chapters). For example, decentralization contributes to lapses in traffic safety, to fragmented public health, and medical care systems in the United States (Institute of Medicine, 2011d). Opposition to rigorous enforcement applies to speed control, life-style choices, and restrictions on industry. Constitutional prohibitions restrict not only unreasonable searches but also proscribe interventions on gun possession. Resource limitations apply not only to law enforcement but also explain deficiencies in public health programs (Institute of Medicine, 2012), the foods chosen for school lunch menus (Institute of Medicine, 2010b), and weakness in social and safety net services.
(portrayed in the bottom of the diagram), policy solutions occupy the diverse domains at the top: macro issues, such as the built environment that enables children to engage in outdoor physical activity and farm subsidies for corn-based food products, as well as other obesogenic influences, such as cultural norms about body image, commercial messaging, local food environments, and the effects of material deprivation and psychological stresses.
A key finding of this report is the alarming scale of health disadvantage among children and adolescents in the United States compared with their peers in other high-income countries. This finding has major implications not only for public health (especially when today’s children become tomorrow’s older adults), but also for the economy and national security (World Economic Forum, 2011). The spectrum of problems that disproportionately affect youth in the United States relative to other countries covers virtually every aspect of their lives: the risk of infant mortality and low birth
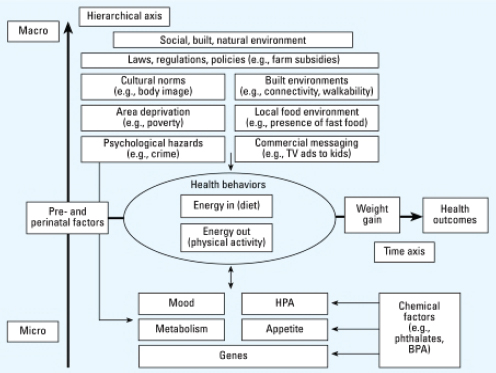
FIGURE 8-4 A life-course perspective on childhood obesity.
NOTES: BPA: bisphenol A; HPA: hypothalamic-pituitary-adrenal axis. The life span is depicted horizontally; factors are depicted hierarchically, from the individual level at the bottom of the figure to the community level at the top of the figure.
SOURCE: Trasande et al. (2009, Figure 1).
weight; injuries and homicide; behavioral health problems involving drug use, high-risk sex, and depression; high rates of childhood disease (e.g., obesity, diabetes, asthma); high rates of child poverty; lower educational achievement; and lower social mobility. This list is a powerful signal for greater attention and investment in policies and programs for children and families (National Research Council and Institute of Medicine, 2008) but, historically and even now, the United States has made greater investments in assisting the elderly than the nation’s youth. Some analysts have concluded that the underinvestment in children and adolescents may be the product of their limited political power compared with older voters (Isaacs et al., 2012; Preston, 1984). Those investments in older adults have produced important social and public health benefits for older Americans and offer an important avenue for addressing the U.S. health disadvantage, but the problems that affect the nation’s youth deserve greater investment.
Maternal and child well-being are clearly important to any nation’s health, and a comprehensive review of this component of population health in the United States is beyond the scope of this panel. However, the areas of disadvantage among U.S. children and adolescents relative to other rich nations that we document point to a number of important areas that should be considered. These include environmental factors—at home, school, and elsewhere—that promote obesity and limit physical activity; the need for child care and early childhood education; reducing barriers that children and mothers face in obtaining essential preventive services and health care; providing a range of supports for youth, especially around sexual health and preventing tobacco, alcohol, and other drug use; and interventions to prevent car crashes and fatalities that involve children or young drivers. Child protection policies would also be important to reduce children’s exposure to family violence, crime, and the risk of violent deaths (especially from firearms), to unhealthy air and housing, to the material deprivations of poverty, and to schools and home environments that compromise learning, educational opportunities, and social mobility.
The life-course perspective is a reminder that adverse exposures during childhood—from fetal life through other critical periods of children’s physical, sexual, and emotional development—have profound implications in shaping health outcomes later in life and, increasingly, the chances of even surviving to old age. Investing in today’s youth is thus an investment in all age groups.
The familiar adage to “follow the money” is a reminder that a society’s policy priorities are often reflected in budget decisions. The panel’s review of data on the U.S. health disadvantage and its potential causes shows that
the United States often spends less per capita in many of the areas in which its performance is lagging, with the obvious exception of health care. Levels of spending should be interpreted with caution because they say little about the efficiency or effectiveness of programs, but the spending patterns of the United States stand in contrast to those of other high-income countries with better health outcomes. Examples include early childhood education, family and children’s services, education, and public health.
• Early childhood education: In 2007, the United States spent only 0.3 percent of its GDP on formal preschool programs (for children aged 3-5 years), less than that of seven peer countries and even some emerging economies in Eastern Europe (OECD, 2012i).
• Family and children’s services: Total public spending by the United States on services for families and young children places the United States last among the 13 peer countries studied. In 2004, the most recent year reported by the OECD, the United States devoted only 0.78 percent of GDP to public services for families and young children, whereas Nordic countries spent approximately 4 percent (OECD, 2006). Only Korea ranked lower than the United States on the proportion of its economy devoted to public services for families and young children.
• Public health: According to many analyses, public health is systematically underfunded in the United States (Institute of Medicine, 2012; Mays and Smith, 2011), for a variety of reasons (Hemenway, 2010), but valid data for international comparisons are lacking. The OECD does measure the proportion of public expenditures devoted to health and to public health, but classification schemes are too variable by country to draw meaningful inferences.
• Social services: Compared with other countries, the United States spends less on social programs, subsidies, and income transfers than do other countries (see Figure 8-5). As noted above, U.S. spending on social services (13.3 percent of GDP) was less than the OECD average (16.9 percent) and that of all 30 countries except Ireland, Korea, Mexico, New Zealand, and the Slovak Republic (Bradley et al., 2011). A recent report found that the United States spent less on public social protection (as a percentage of GDP) than any peer country but Australia and less than some emerging economies, including Russia and Brazil (International Labour Office, 2011).
In contrast, however, the United States ranks high on public spending on education. In 2008, U.S. spending per student on public education (primary through tertiary levels) was equaled only by Switzerland. Among all
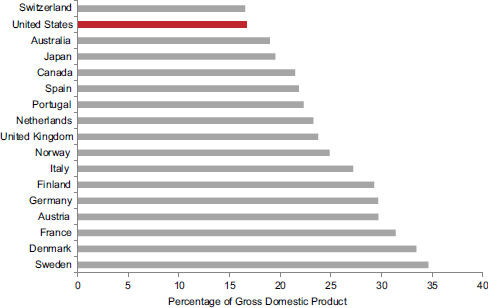
FIGURE 8-5 Social benefits and transfers, 17 peer countries, 2000.
NOTES: Social benefits reflect current transfers to households in cash or in kind to provide for the needs that arise from certain events or circumstances (e.g., sickness, unemployment, retirement, housing, education, family circumstances) that may adversely affect the well-being of households either by imposing additional demands on resources or by reducing incomes. Transfers are typically made by governments.
SOURCE: Data from National Accounts at a Glance: 5. General Government, OECD(2012l).
OECD countries, the United States had the fifth highest public expenditure per student on primary education, the fourth highest for secondary education, and the highest for tertiary education (OECD, 2011a). Measured as a percentage of GDP, U.S. public expenditures on education ranked eighth (tied with France, Ireland, Israel, the Netherlands, Switzerland, and the United Kingdom) (OECD, 2012h).
Many of the programs discussed above are financed in other countries by taxes, an approach with limited political support in the United States. Of the 17 peer countries that are the focus of Part I of this report, 11 report a higher tax burden than the United States (U.S. Census Bureau, 2008).16 Since the 1980s, no country in this peer group except Switzerland has spent less than the United States (as a percentage of employee-employer payroll
_________________
16Tax burden is defined as the percentage of gross wage earnings of the average production worker that is spent on income tax plus employee social security contributions less cash benefits.
taxes) on social security programs such as old-age, disability, and survivors insurance; public health or sickness insurance; workers’ compensation; unemployment insurance; and family allowance programs (U.S. Census Bureau, 1995).
Nine areas of health disadvantage are documented in Part I of this report:
• adverse birth outcomes;
• injuries, accidents, and homicides;
• adolescent pregnancy and sexually transmitted infections;
• HIV and AIDS;
• drug-related mortality;
• obesity and diabetes;
• heart disease;
• chronic lung disease; and
• disability.
There are policy implications for each of these. Although much is still to be learned, for many of these public health issues there are evidence-based policies that could address them at the national, state, and local levels.
Policy is also relevant to the unfavorable social, economic, and environmental conditions identified in this report as potential contributors to the U.S. health disadvantage. A variety of policies can contribute to high poverty rates, unemployment, inadequate educational achievement, low social mobility, and the absence of safety net programs to protect children and families from the consequences of these problems. However, identifying and implementing policy solutions is a formidable challenge. For example, national health objectives to address many of the conditions listed above were adopted decades ago by the federal government but only some have been achieved, a problem that global initiatives to improve public health have also encountered. Although there have been important public health successes in the United States and elsewhere, such as the remarkable progress in reducing the rate of tobacco use (Brownson et al., 2006), a variety of barriers have impeded progress on other fronts, such as stemming the obesity epidemic or reducing smoking among adolescents.
Other high-income countries with better health status, lower rates of poverty, and more impressive advances in education may owe their success to creative policies or strategies that could find application in the United States. These suppositions, however, amount only to informed speculation and are without empirical evidence. This panel did not undertake a systematic
review of the policies and outcomes in other countries, but we believe that such an exercise would be worthwhile to identify useful lessons (see Chapter 9). Reports like the Transportation Research Board study (see Box 8-1) would be valuable for each of the leading causes of the U.S. health disadvantage. However, there are valid questions about the generalizability of “imported” models from overseas, and comparisons with other countries—even other high-income countries—may be seen as less applicable if the comparison countries are much smaller, have a more homogenous population, or have very different social or political systems.
The Measurement and Evidence Knowledge Network (Kelly et al., 2007, pp. 31-32) examined these issues in its final report to the World Health Organization Commission on the Social Determinants of Health. Its conclusions included the following challenges to implementation of such policies:
• [Social factors and other nonmedical determinants of health (SDH)] are multifaceted phenomena with multiple causes. [Although] conceptual models of SDH are useful, they do not necessarily provide policy makers with a clear pathway towards policy development and implementation. As specific policy initiatives tend to be targeted to a specific (population) group in certain circumstances and for prescribed time-periods, they can neglect the wider context within which the social and other determinants are generated and re-generated.
• … [R]ecent studies of SDH have emphasized the significance of the life-course perspective (Blane, 1999). Such a perspective poses serious challenges to policy-making processes whose time-scales are rarely measured over such long periods. The tenure of elected or appointed officials is measured in months and years rather than decades. Moreover, coalitions of interests in support of [these policies] may be unsustainable over the time periods necessary to [achieve] significant change. There have been some exceptions to this [general finding], especially in the field of public pension policies, but the general problem of time-scales remains important.
• … SDH necessarily imply policy action across a range of different sectors. It is increasingly recognized that action beyond health-care is essential and, as such, intersectoral partnerships are critical to formulating and implementing effective … [policies]. However, there is a significant body of evidence which shows that partnerships are hampered by cultural, organizational, and financial issues (Sullivan and Skelcher, 2002).
• Traditionally, government agencies have been organized vertically according to service delivery (Bogdanor, 2005; Ling, 2002) and
such “silo” or “chimney” approaches are not well equipped to tackle issues that cut across traditional structures and processes.
The report notes that silos within and across agencies make it difficult for leaders who address one social factor (e.g., education) to interact with health agencies. With the exception of some success stories (e.g., school health), meetings across agencies occur only occasionally except the Cabinet level. Looking at policies on social factors and other nonmedical determinants of health, the report notes:
• [They] must be viewed as only one of several competing priorities for policy makers’ attention and resources. Economic policy or foreign affairs [often] take precedence over health concerns. More specifically, SDH may be over-shadowed … by [concerns over] health-care itself. However, this health care focus is often to the neglect of health and [its broader determinants].
The report further notes that a focus on health care also ignores the important connection between health and the economy: nonhealth policies that reduce disease burden and thus the costs of health care have enormous implications for medical spending and the economy itself (Milstein et al., 2011; Woolf, 2011). Unfortunately, the report notes, political realities often limit attention to “short-term [returns] rather than the long-term [ramifications] and on discrete interventions rather than coordinated, collaborative initiatives….” Lastly, the report notes that globalization has been changing the role of national governments in shaping policy making:
• Governments’ ability to shape and mould SDH with the goal of improving their population’s health is becoming limited as many of the [upstream causes] no longer fall within their responsibility. There is a parallel argument that decentralization [of authority] to regions and cities has had a similar effect on the policy-making capacity of national governments.
Ultimately, meaningful initiatives to address the underlying causes of the U.S. health disadvantage may have to address the distribution of resources that are now directed to other categorical priorities—a change that is likely to engender political resistance. Is a shift in priorities warranted? This report documents that the United States is not keeping pace with other high-income countries in many areas of health and socioeconomic well-being, and the consequences to the nation can be measured not only in lives, but also in dollars. Understanding why this is occurring and identifying policies that could reverse these unfavorable trends are clearly important for the nation’s future.
































