
![]()
This chapter examines the effects of deployments to Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) on the mental, emotional, and social well-being of military family members, including spouses, children, and caregivers. It also discusses issues related to the availability of programs and services for military families. Military family members are an important part of the readiness and well-being of the military force. The care and support of military families is considered a top national security policy priority in recognition of the integral role family members have in supporting service members and, therefore, the mission of the military. With that priority, various challenges arise. Throughout this chapter, the committee presents evidence that military family members have to deal with additional relationship problems, impairments in psychologic and physical well-being, responsibilities as caregivers of children or wounded service members, and overwhelming household duties. The committee’s primary focus is on the impacts of deployment on military families, and not on the entire scope of experiences faced by military families. Given the exceptional demands that deployments to OEF and OIF have placed on military families and the impact that family concerns have on soldiers’ well-being, there continues to be a need for military leaders to gain a better understanding of the needs of families and to use that understanding to implement more-effective coordinated programs and services for the good of military families and, thus, for the military as a whole.
CHARACTERISTICS OF MILITARY FAMILIES
Military families are more diverse than most statistics or research might suggest. Many families do not meet the criteria used for official counts of military families and, therefore, are not included in the data (for example, common-law spouses). Because of that, this chapter reports information only about a subset of military families: those of service members in heterosexual marriages and parents with dependent children who live with them at least part of the time. The committee views the military’s definition of family as narrow and out of step with the diversity in family arrangements in modern society. The committee found little or no information about parents or siblings of service members (who are sometimes relied upon for important caregiving responsibilities), unmarried partners, stepfamilies, children who are not legal dependents (for example, stepchildren or nonresidential children), gay families, service members acting as substitute parents, or other nontraditional family configurations. Most published studies focus on active-duty male military personnel married to civilian wives.
Because women constitute a relatively small number of service members, they are sometimes excluded from studies. As the number of women in the military continues to increase, it becomes even more important that they be included in research studies.
Despite the apparent popularity of marriage among military members, nonmarital intimate relationships are likely to become a more prominent feature of the relationships of service members in the future, as they are in the population as a whole, and methods of counting relationships may need to be amended as a result. The general population has been characterized in recent decades by rising tendencies for individuals to delay marriage and to cohabit before marriage (Copen et al., 2012). Delays in and alternatives to marriage might become more evident in the military, especially as policies change in the aftermath of discontinuing the “Don’t Ask, Don’t Tell” policy (McKean et al., 2011). Thus, marital status might become an increasingly inaccurate index of relationship patterns, and useful information about the health of intimate relationships of military members might be overlooked if tabulation methods are not adjusted.
Defining Military Families
Multiple definitions of family are used in the Department of Defense (DOD), each tied to specific regulatory requirements. The most common definition uses eligibility for military identification cards, which are necessary for access to health care, military exchanges, and a variety of supportive services for families. Military identification cards are currently issued to spouses and unmarried children of service members—exceptions and additional categories are defined by children’s ages, student status, or special needs and by whether the marriage ends in divorce or in death of the service member while on active duty. Spouses and unmarried children of reserve-component members are covered while the service member is on active duty for more than 30 consecutive days (DOD, 2012d). Stepchildren may or may not qualify for military identification cards, depending on such factors as age, student status, and the circumstances of the biologic parents.
Single service members are not irrelevant in a chapter focused on the implications of deployment for family life. Single service members might have completed or be in the process of establishing families; for example, they might have cohabiting partners or they might be in close relationships that are precursors to marriage. The population of single service members also includes previously married individuals who might be in the process of establishing a second family. All service members, especially those who do not have spouses or partners, might rely on parents, siblings, or other family members for substantial emotional or tangible support, especially if they encounter hardships, such as illness, wounds, or other major life challenges. However, little research has examined family issues as they relate to single service members.
Demographic Characteristics of Military Families
This section describes the demographic characteristics of families of active-duty forces and selected reserve components. Because data presented here are derived from the DOD’s annual demographic profiles of the military community (DOD, 2011b, 2012a) and represent all service members—not only those who have been deployed—they will not be identical to the data presented in Chapter 3, which include only service members who have been deployed.
TABLE 6.1 Summary of Selected Demographic Characteristics for DOD Active-Duty and Selected Reserve Members
| Status | Percent of Active-Duty Membersa | Percent of Selected Reserve and National Guard Membersb |
| Percent married (enlisted, officers); (male, female) | 56.6 (54.0, 69.6); (58.5, 45.7) |
47.7 (43.7, 70.6); (50.1, 37.0) |
| Percent in dual-military marriages (sex of active-duty member: male, female) | 6.5c (3.9, 21.6) | 2.6d (1.3, 8.6) |
| Percent of married members in dual-military marriage (sex of active-duty member: male, female) | 11.5 (6.8, 47.3) | 5.5 (2.6, 23.3) |
aIncludes 1,411,425 members of the four DOD active-duty branches (Army, Navy, Marine Corps, and Air Force). Limited data are included for the active-duty Coast Guard (Department of Homeland Security).
bIncludes 855,867 members of the six reserve components (Army National Guard, Army Reserve, Navy Reserve, Marine Corps Reserve, Air National Guard, and Air Force Reserve) and the Coast Guard Reserve.
cOf these, 81.8% are enlisted members, and 18.2% are officers.
dOf these, 76.1% are enlisted members, and 23.9% are officers.
NOTE: Data are derived from a variety of sources, including the Active Duty Military Personnel Master File, the Active Duty Military Family File, the Reserve Components Common Personnel Data System, the Reserve Components Family File, and the Defense Enrollment and Eligibility Reporting System (DEERS).
SOURCE: DOD, 2012a.
Marital Status of Active-Duty and Selected Reserve Members
Marriage Patterns
Over two-thirds of active-duty and reserve officers are married, as are over half of enlisted active-duty service members and nearly half of those in the selected reserves (see Table 6.1). Reflecting the general makeup of the services, the great majority of both active-duty military (93.1%), and selected reserve (88.1%) spouses are female (DOD, 2011b). Male military members ages 18 to 41 are significantly more likely to have married at some point in their lives than are comparable civilians, particularly if they are black, Hispanic, or hold enlisted rank (Karney et al., 2012). On the basis of 1999 data from the Active Duty Survey of Military Personnel, Lundquist (2004) found that black service members in their early 20s were at least three times more likely to marry than their civilian counterparts and that the large marriage gap present between black and white civilians did not exist for those in the military.
Although less is known about the marital patterns of women serving in the military, they are less likely to be married than their male counterparts, a pattern not observed among civilians of similar age. Women in the military are also much more likely to be married to other service members: In 2011, female active-duty service members and women serving in the reserve component were more likely than their male counterparts to be married to a fellow service member. Nearly half of married women on active duty were married to another service member (DOD, 2012a).
In summary, military members are as likely or more likely to be married than their civilian counterparts, and this factor is particularly true for officers and members serving on active duty. Although the prevalence of marriage has been declining steadily in the civilian
population, in the military it has been essentially level, having some fluctuations, over the past two decades.
Divorce Patterns
An estimated 4.1% of married enlisted members and 2.1% of married officers divorced between September 2010 and September 2011. This percentage is a substantial increase over 2000 rates, when an estimated 1.4% of married officers and 2.9% of married enlisted members had divorced during the previous year. This increase was especially steep for married enlisted soldiers (2.3% in 2000 compared with 4.0% in 2011, a 74% increase) and sailors (2.6% in 2000 compared with 4.6% in 2010, a 77% increase).
Among the selected reserve, an estimated 2.8% of married enlisted members and 1.9% of married officers divorced during the 1-year period before September 2010. This percentage shows modest increases above the 2000 rates, which were 2.4% for married enlisted members and 1.6% for married officers.
Data analyses by Karney et al. (2012), however, suggest that the apparent increase in divorce rates in military relative to civilian populations is not statistically significant and does not reflect a widening gap between civilians and military members, at least during the 4 years before and after the start of combat operations in Afghanistan in 2001. In fact, male military officers and enlisted members reported being currently divorced at either the same or lower rates than civilian men with comparable education, age, race or ethnicity, and employment status both before (1998–2001) and during the war (2002–2005) (Karney et al., 2012).
Marriages of women in the military are more likely to fail than those of men (Karney and Crown, 2007; Lundquist, 2006). Karney and Crown (2007) examined military personnel records to track the marital status of service members over a 10-year period (1996 to 2005) and found that rates of marital dissolution for female service members were more than double those of their male counterparts. Regarding marital dissolution and race, Lundquist (2006) found that black service members were 53% less likely to divorce than whites, unlike in the civilian population, in which blacks were 30% more likely to divorce than whites. When only one partner was in the military, white dual-military couples were 40% more likely to divorce than black couples.
In summary, although overall divorce rates in the general population have been falling during the past decade, divorce rates in the military have risen noticeably. Nonetheless, on the basis of comparisons of matched civilian and military men, Karney et al. (2012) concludes that men serving in the military are no more likely than their civilian counterparts to divorce and that this gap did not widen between 1996 and 2004. A subsequent section about deployment and married couples examines research on the impact that deployment has on marital dissolution.
Family Responsibilities of Active-Duty and Selected Reserve Members
Information on the family status of service members is presented in Table 6.2.
TABLE 6.2 Family Status of DOD Active-Duty and Selected Reserve Members
| Status | Percent or Number of DOD Active-Duty Members | Percent or Number of Selected Reserve and National Guard Members |
| Percent with children (overall) | 44.2% | 43.3% |
| Percent married to civilian, with children | 36.1% | 32.5% |
| Percent dual-military with children | 2.8% | 1.5% |
| Percent single with children | 5.3% | 9.4% |
| Average number of children of members with children | 2.0 | 2.0 |
| Percent of children ages 0 to 5 | 42.6% | 28.8% |
| Percent married to civilian with no children | 14.0% | 12.7% |
| Percent dual-military with no children | 3.7% | 1.2% |
| Percent single with no children | 38.1% | 42.9% |
| Percent with family responsibilitiesa (enlisted, officers) | 59.0% (56.7%, 70.0%) | 56.4% (52.9%, 76.4%) |
| Average number of dependents of members with dependents | 2.4 | 2.4 |
aMembers are classified as having family responsibilities if they have a dependent (spouse, children, other dependents) registered in the Defense Enrollment and Eligibility Reporting System (DEERS).
NOTE: Children category includes minor dependents age 20 or younger or age 22 and younger enrolled as full-time students.
SOURCE: DOD, 2012a.
Over half of active-duty and selected reserve members have family responsibilities—that is, are married or have children or have another dependent registered in the Defense Enrollment and Eligibility Reporting System (DEERS)—as do over two-thirds of active-duty officers. Among active-duty enlisted service members, Army-enlisted soldiers are more likely to have family responsibilities than enlisted members of other active-duty service branches (63.5% for Army enlisted, compared with 53.0% for Navy, 46.3% for Marines, and 55.7% for Air Force enlisted). Approximately half to two-thirds of enlisted members of the selected reserve across reserve components have family responsibilities, the exception being Marine reserve families, in which just over a quarter (27.1%) have responsibilities. The majority (67.1%) of active-duty single parents are male service members. However, female service members are much more likely than males to be single parents (12.1% vs 4.2%, respectively).
The large minority of minor dependent children of active-duty members are 5 years old or younger (42.6%), followed by 6 to 11 years (30.7%), 12 to 18 years (22.4%), and 19 to 22 years old (4.3%; includes full-time students). The children of selected reserve members tend to be older than those of active-duty members, 28.8% being ages 5 or younger, 29.7% being ages 6 to 11, 29.6% being ages 12 to 18, and 11.8% being ages 19 to 22.
A study examining marital transitions among service members found that almost onethird of service members (30%) had nonresidential children, a strikingly high percentage in a population where 64.8% of the members were younger than age 30 (Adler-Baeder et al., 2006). Almost all of the service members with nonresidential children had only nonresidential children,
meaning that under military rules, they were defined as single, not as single parents. Among remarried respondents, 42.2% had children from a previous relationship.
In 2008, the Military Family Life project included two items related to marital transitions in a survey of a probability sample of 28,500 military spouses. The first item asked respondents, all of whom were married or separated, if they were currently living in a stepfamily; 20% indicated that they were. In addition, 35% of the participants indicated that they had a child from the service member’s or spouse’s prior relationship or were acting as parents for someone else’s child, such as a grandchild, niece, or nephew. Thus, a substantial proportion of service members are living in stepfamilies or are acting as parents for the children of others.
A small proportion of active-duty (0.7%) and selected reserve (0.2%) members are responsible for one or more adult dependents, such as a parent, grandparent, sibling, disabled older child, or other adult claimed as a dependent in the DEERS system. In the large majority of cases, the dependents are females age 51 or older.
DEPLOYMENT AND FAMILIES
Rewards and Challenges of Military Service for Families
Understanding the effects of wartime deployments on military families requires some understanding of the baseline conditions of military life. The demands of military service may characterize other occupations, but rarely with the prevalence and frequency of demands that occur in military life (Castro et al., 2006). However, military service offers tangible and intangible benefits and supports that other occupations might lack.
Rewards of Military Service
Research about military families tends to focus more on negative than beneficial aspects, but the latter are nonetheless important. Rewards of military service can include personal growth from surmounting difficult challenges, increased appreciation of personal relationships, increased earnings from hazardous duty pay, and a sense of purpose from performing an important mission for the country (Newby et al., 2005a).
A review of studies of appraisals by veterans from a variety of combat and peacekeeping operations (Schok et al., 2008) found that most veterans reported positive aspects of their experiences, primarily in three domains: self-image, such as self-discipline, self-confidence, and coping; in social relationships, such as cooperating better and becoming more tolerant; and in personal growth and priorities in life, such as valuing life, recognizing the importance of family, and strengthening of faith. In a focus group, data gathered by Hosek et al. (2006) showed that service members reported similar themes, including satisfaction from using the skills they had acquired in training and fulfillment of a sense of duty.
Family members also reported increased closeness, patriotism, pride, civic responsibility, and personal growth (Werber et al., 2008). Being in the military can also provide a sense of community for military families and a social support system of other military families who understand the demands of military life. Although relocations can be stressful, military life provides families with the opportunity to see and live in different parts of the country or the world that would not otherwise be available to them.
Challenges of Military Service
Military service includes a number of stressors related to the structure of work (Adams et al., 2006; MacDermid Wadsworth and Southwell, 2011; van Steenbergen et al., 2008). Military work is demanding, often requiring long hours and physically tiring tasks (Huffman and Payne, 2006; Kavanagh, 2005), and even nondeployed units must work to prepare for future deployments and support currently deployed units. Service members may be assigned with little advance notice to a variety of duties that require repeated episodes of time away from their families (for example, temporary duty assignments, training, disaster relief, humanitarian aid, and combat), all of which may expose service members to danger (Kavanagh, 2005).
Service members and their families are required to relocate much more frequently than civilian families (every 2 to 3 years), with little opportunity to influence the choice of the next duty station (DOD, 1998; GAO, 2001). In 2010, 31% of military members (excluding unmarried service members living in barracks) moved, compared with 13% of civilians (US Census Bureau, 2011c). Rates of international relocations, which can be more challenging than domestic moves, are four times higher among military families than their civilian counterparts (Reinkober Drummet et al., 2003). Frequent obligatory moves are associated with frustration and decreased satisfaction with military life (GAO, 2001). Lack of support and isolation in the new community is particularly mentioned as a concern by spouses (Burrell et al., 2006). In addition to their emotional consequences, frequent relocations disrupt the ability of spouses to achieve educational or career goals (Burrell et al., 2006; Eby et al., 1997; Harrell et al., 2004). Relocations can require spouses to transfer certifications and change jobs or retrain. Military spouses are less likely than their civilian counterparts to work full-time, to average fewer work hours and fewer days in the year, and to earn less than spouses of civilians (Hosek et al., 2002; Lim and Schulker, 2010).
Beyond dealing with the occupational demands of the service members, military life also may impose codes of conduct for family members as well as service members, especially when living in military housing, using military support services, or when the service member occupies a leadership position (Segal, 1986). Military scrutiny and expectations for good conduct on and off duty may lead service members and their families to perceive a lack of privacy. Furthermore, the behavior of spouses and children can impact service members and their careers. For example, spouses’ problematic behavior (e.g., traffic violations, financial problems, substance abuse) can come to official attention and result in pressure on service members to “control their family member” (Segal, 1986).
The high proportion of military women in dual-service marriages, when combined with the high rates of marital dissolution among military women, raises questions about the severity of the unique challenges faced by dual-military families in coordinating leaves between parents, arranging child care, and other challenges posed by dual commitments to military service (Bethea, 2007). As discussed by Huffman and Payne (2006), individuals in dual-military marriages have multiple roles—at the very least as spouse and as service member, and often as parent or active community member. In dual-military marriages, having multiple roles can have positive implications, but the difficulty of fulfilling obligations associated with each role can strain individuals, particularly for those with children. In addition, military-specific challenges, such as being in the presence of danger, working at a high pace, and frequent or long separations, are magnified in dual-military marriages.
Impact of Deployments on Families
Deployments are not single events but complex configurations of predictable and unpredictable experiences. Deployments are diverse, varying along several dimensions. The most obvious dimension is content, such as exposure to trauma, physical demands, harsh living conditions, access to resources, and the ability to communicate with family. The dimensions of deployment structure include duration and frequency of individual deployments, which also leads to consideration of “dwell time” or the interval between repeated deployments. As deployments accumulate, cumulative duration becomes relevant. Although every deployment comprises a before, during, and after period, there are differences in the amount of advance notice service members receive and when, where, and for how long they must receive training before departing or after they return. Deployments have been categorized as both normative and catastrophic. The former is characterized by adequate time to prepare, by predictable duration and content, and by relatively mild emotional distress; the latter is characterized by little advance warning, uncertainty and danger, and prolonged emotional distress (McCubbin and Figley, 1983; Wiens and Boss, 2006). To the extent that every deployment comprises before, during, and after deployment periods, they have a predictable structure. The duration and content of these phases vary widely, however—raising caution about the confidence with which predictions can be made about the implications for families.
Several scholars have constructed stage models to describe the emotional experiences and coping challenges that are thought to characterize the deployment and reunion periods (Wiens and Boss, 2006); see also Mateczun and Holmes (1996), Peebles-Kleiger and Kleiger (1994), and Pincus et al. (2001) for more information about stage models. Although these stage models are appealing in their clarity and appear to be consistent with the findings of some empirical studies, no longitudinal studies have documented that these stages occur, occur in the proposed sequence, incorporate the proposed experiences or challenges, or display the proposed durations.
Although the number of published peer-reviewed studies of the impact of OEF and OIF deployments is rapidly increasing, large knowledge gaps remain. For example, many studies do not incorporate family factors or gather data from family members. The studies that do incorporate that information focus mostly on spouses and to a lesser extent on children. Little attention is given to the parents or the “significant others” of service members, a particularly concerning gap for single service members. Similar to studies of military families in general, most OEF and OIF studies focus on male military personnel married to civilian women and serving in the Army (Kelley et al., 2002). Many studies focus on negative consequences, especially posttraumatic stress disorder (PTSD), rather than other potential sequelae of deployment.
Almost no studies have been conducted that include prospective data from the predeployment period. A few have gathered data during deployment but rarely from service members and even more rarely from both service members and family members. Most research—even of the period during deployment—has been conducted following return from deployment, and most studies are cross-sectional rather than longitudinal (de Burgh et al., 2011). Two large longitudinal studies, currently in the data-collection phase, are likely to generate important data about the effects of military service and deployments on families in the coming years. The family component of the Millennium Cohort Study is recruiting 10,000 spouses of service members participating in a 20-year prospective study of four cohorts totaling 150,000
service members. Data gathered from these spouses will permit comparisons of families of combat-deployed, noncombat-deployed, and nondeployed service members (Crum-Cianflone et al., 2012). The RAND Corporation is conducting a prospective, longitudinal study of approximately 2,000 military families who are expected to experience a deployment. This study will follow the cohort for 3 years; data will be gathered across a number of domains every 4 months. The design includes measures that will be repeated before, during, and after the deployment phases. One of the primary goals is to understand both risk and protective factors across the deployment phases in an effort to define family readiness. Other key elements of this study include data collection from multiple respondents per family, including one child 11 to 17 years old. Measures include physical health, behavioral health, marital relationship, parenting, use of services, career intentions, and deployment experience (RAND Center for Military Health Policy, 2012).
Theoretical Models
Several theoretical approaches have been presented to account for families’ experiences of deployment. Most of them take a systemic approach, recognizing that families have properties distinct from the characteristics of individual members. Systemic approaches also draw attention to patterns of information flow that can foster or impede adaptation to challenges within families.
The theoretical perspectives used to account for the impact of deployment on families focus on stress processes (see Karney and Crown, 2007; McCubbin, 1979; Patterson, 2002) or on patterns of family resilience (see Saltzman et al., 2011; Walsh, 2006; Wiens and Boss, 2006). Several approaches are based on the attachment theory, which posits that individuals develop internal working models for attachments to others during childhood that condition their responses not only to separations from primary attachment figures but also to interactions with future partners and children. Attachments vary in their characteristics and may be secure or insecure, the latter characterized by anxiety or avoidance. Deployment constitutes a significant challenge to attachment systems and, depending on the nature of attachment relationships among family members, can result in reactions ranging from adaptation that allows the family to function well during separation and incorporate the service member on his or her return and ranging to problematic arrangements that “close ranks” against the service member (Riggs and Riggs, 2011).
Finally, attention is being given to the conditions surrounding military families, including informal support from social networks of family, friends, colleagues, and others, as well as formal support from community agencies and programs. This perspective is prompted in part by greater recognition of the differences between the circumstances of active- and reservecomponent families (Bowen and Martin, 2011; MacLean and Elder, 2007; Wiens and Boss, 2006).
Characteristics of Deployments and Impact on Families
Families appear to experience greater stress and anticipate more difficulties when deployments are longer (Booth et al., 2007; Orthner and Rose, 2002). In a systematic review of studies of deployment length, Buckman et al. (2011) concluded that longer deployments are associated with adverse effects on service members and their families, deployments having a possible threshold of 6 months, beyond which negative effects are more likely to occur.
Several studies suggest that cumulative duration of deployments might be more important than frequency of deployment or the duration of a single deployment for certain family-related outcomes (Chandra et al., 2011; Hurley, 2011). For example, Lara-Cinisomo et al. (2011) found that caregivers who experienced more months of deployment of military members during the past 3 years (but not a larger number of deployments) reported lower relationship satisfaction, more relationship hassles, and poorer emotional well-being. Mansfield et al. (2010) found that the number of cases of depression was larger among wives whose husbands had been deployed longer. Franklin (2011), however, found that reports of psychologic symptoms on the Air Force Community Assessment rose with both frequency and duration of deployment. For length of deployment, but not for frequency, the connection to relationship quality was mediated by psychologic symptoms. These findings probably underestimate the impact of the frequency of deployment because most studies exclude deployments lasting less than 30 days or deployments not in support of war operations. Thus, the number of service members’ departures from and returns home are greatly underestimated, and the statistical effects associated with deployment frequency may be attenuated as a result.
There is considerable evidence that family-related concerns weigh heavily on service members during deployment. In each administration of the Army-led Mental Health Advisory Team (MHAT) surveys, concerns about being separated from family are among the foremost deployment concerns, as reported by about one-third of service members (MHAT-VII, 2011). Responses to the 2008 DOD Survey of Health-Related Behaviors indicated that service members who had been deployed recently were significantly more likely to report high family stress than were service members who had not been deployed; levels of these concerns did not change between 2002 and 2008 (Bray et al., 2010). In another study, British Forces service members surveyed during deployments to Iraq and Afghanistan reported poorer mental health when negative events occurred at home and when they perceived poor military support for their families. These findings were firm regardless of combat exposure but were somewhat weaker in the presence of strong military unit cohesion or military leadership (Mulligan et al., 2012). Skopp et al. (2011), in a large study that included pre- and postdeployment data from 2,583 Army soldiers, found that female soldiers with higher levels of combat exposure were significantly more likely to screen positive for PTSD if the strength of their intimate relationships had declined during deployment.
In their longitudinal study of more than 88,000 soldiers who served in Iraq, Milliken et al. (2007) found a fourfold increase in interpersonal problems from when they returned from deployment and a median of 6 months thereafter. The authors made special note of the cumulative burden of mental-health problems on family relationships and advocated greater mental-health resources for family members.
Baseline levels of perceived stress appear to have risen among Army spouses in recent years. The recent Army “Gold Book” indicated that more than half of all spouses reported experiencing stress in 2010 (56%, up from 46% in 2006) (Department of the Army, 2012). Supporting the notion of relatively high baseline rates of stressors, almost half of the spouses (44%) reported concern about finances, and two-thirds reported that they had less than $500 in savings accounts. More than half of the spouses were employed or were looking for work. Finally, 19% of spouses who responded indicated that they were in counseling, mostly for stress, family, and marital issues (Department of the Army, 2012).
Evidence assembled so far from both prior and current wars suggests that the likelihood of negative consequences for families rises with the amount of the service members’ exposure to traumatic or life-altering experiences. Thus, military service by itself does not appear to significantly raise the probability of negative outcomes (MacLean and Elder, 2007), and the same appears to be largely true for uneventful deployments lacking exposures to trauma (although traumatic exposures can occur not only with combat but also with duties related to peacekeeping and natural disasters (Allen et al., 2010). In contrast, deployment to combat zones has been found to significantly predict a variety of negative outcomes, including marital conflict and intimate partner violence (IOM, 2008). When service members display negative psychologic symptoms, the likelihood of negative consequences for families rises substantially (de Burgh et al., 2011), and families who experience the injury or death of service members are almost certain to experience at least some negative consequences.
Deployment and Married Couples
The health of marriages is typically assessed in research by two key indicators: marital quality and marital dissolution, which refers to the end of the marital relationship, typically via divorce (Karney and Bradbury, 1995). Although marital quality is difficult to measure, to date, measurements have focused primarily on the levels of satisfaction expressed by each partner (Knapp and Lott, 2010). Ideally, stable marriages have not only avoided dissolution, but also avoided separation or consideration of divorce, although studies vary in which of those elements are included (Karney and Bradbury, 1995). Dissolution, although relatively straightforward to measure, is a limited indicator of marital health because divorce is only the outcome of a lengthy and uncertain process.
In this section, we review research related to the impact of deployments on marital quality and marital dissolution.
Marital Quality Throughout the Deployment Cycle
The IOM (2008) found strong evidence that service members returning from deployments to combat zones were more likely to have marital problems, including intimate partner violence, than people who were not deployed and that this pattern was particularly strong when veterans had been diagnosed with PTSD. Evidence based on studies of Vietnam veterans was judged insufficient to conclude the existence of a causal relationship between deployment and marital conflict or marital dissolution.
On the basis of the perspectives of service members themselves, marital quality in the military population appears to have declined in the past decade. Data gathered from service members during deployments to Iraq and Afghanistan, as part of the MHAT research program, revealed a steady downward trend in marital satisfaction each year between 2003 and 2009, from 79% agreeing or strongly agreeing that they were satisfied with their marriages in 2000 to 57% giving similar reports in 2009 (MHAT-VII, 2011). The declines were limited to enlisted members and were largest among junior enlisted males (pay grades E1 to E4). Service members’ reports that they intended to seek a divorce also rose from 12.4% in 2003 to 21.9% in 2009, again being much more evident among junior enlisted members. The 2006 MHAT report (MHAT-IV, 2006) indicated that problems with infidelity rose from 4% to 15% between 2003 and 2006, and marital problems more than doubled—from 12% to 27%.
Several studies suggest that marital quality following deployment is in part a function of quality before deployment (Nelson Goff and Smith, 2005; Rosen et al., 1995). Nonetheless, reasons for declines in marital quality are complex, and research results so far are mixed, particularly with regard to which mediators and moderators are most consequential for which people under which conditions (de Burgh et al., 2011).
Researchers have articulated several concepts evident throughout the deployment cycle—ambiguity and uncertainty, relationship connection, and communication—that characterize the nature of the relationship between military service members and their spouses and that influence their experiences (Sahlstein et al., 2009; Wiens and Boss, 2006).
Ambiguity and uncertainty are dominant aspects in the lives of military couples. Before and following deployment, the service member may be physically present but psychologically absent at least to some extent, while during deployment he or she is physically absent but psychologically present (Sahlstein et al., 2009; Wiens and Boss, 2006). In a study of 50 Army wives with current or recent experience with deployment, Sahlstein et al. (2009) found that separations related to training before the deployment heightened concerns about relational uncertainties (for example, concerns for the future of the marriage), and wives often responded by either expressing support or distancing themselves communicatively from their husbands (for example, by being silent or starting arguments). In a longitudinal study of Army reservists by Faber et al. (2008), ambiguity led to worries about the safety of the service member, how to handle challenges at home, and how to react to one another following return.
Baptist et al. (2011) interviewed 30 soldiers and spouses (not married to each other) in Army couples who had experienced one deployment to OIF or OEF. They used both open-ended and quantitative measures of the perceived impact of deployment on their marriages. Because of ambiguity about how to reintegrate service members into household duties following deployment, spouses sometimes continued to manage tasks as they had during the deployment, suppressing their personal needs or preferences. The researchers labeled this a maladaptive process because it complicated reintegration. Both reservists and spouses in the Faber et al. (2008) study reported similar hesitancies.
Using a cross-sectional convenience sample of 220 service members living in 27 states who had returned from deployment in the past 6 months, Knobloch and Theiss (2011) examined relational uncertainty (lack of confidence in self, partner, or relationship) and interference from partners (perceptions that partners are making it harder to achieve goals by disrupting routines). Service members who were dissatisfied with their relationships were more likely to report symptoms of depression but only if they felt uncertain about their commitment to the relationship and perceived their partners as interfering with their plans and activities.
For military couples, preparing for deployment and deployment separation can affect feelings of closeness and connection, heightening feelings of relationship insecurity and feelings of a lack of connection to their partner that result in relationship distress. For example, in the Sahlstein et al. (2009) study, the primary tension that spouses experienced during deployment was between autonomy and connection, particularly as it related to parenting roles. Spouses needed to feel independent enough to assume primary responsibility for parenting but also needed to feel sufficiently connected to their partner for support.
Permeating almost all accounts of deployment-related experiences are themes related to communication. Before and during deployment, families reported dissatisfaction with the
communication they receive from the military about the logistics of deployment and the welfare of the deployed service members (SteelFisher et al., 2008). During deployment, service members may lack access to communication facilities, and service members and spouses must make difficult decisions about what information to share and, given the wide array of communication modalities now available, how and when (Mulligan et al., 2012). Following return, service members and their partners must negotiate reintegration of the service member into the daily operations of the family and renew their intimate relationships (Baptist et al., 2011).
In the following sections, we describe a range of concerns and impacts as they relate to different stages of the deployment cycle.
Marital Quality Predeployment Before deployment, families must make legal, logistical, and emotional preparations for separation and the possible injury or death of their service members (McCarroll et al., 2005). Although it is logical that families would find this period difficult, few prospective studies of family members have been published.
Studies of service members indicate that concerns about their families are an important element of their predeployment experience. Findings from a study of deployment during the first Gulf War (Kelley et al., 2001) suggested that Navy parents anticipating deployment suffered from separation anxiety, particularly mothers (whether married or single). Polusny et al. (2009) surveyed 522 service members in the Army National Guard about 1 month before deployment, comparing responses of soldiers who had or had not been previously deployed for OIF or OEF. Results showed that service members were on average in good mental health and that soldiers with or without prior deployments were similar in their levels of concern about the impact of the separation on their families. McCreary et al. (2003) surveyed 180 members of the Canadian military 48 hours before departure for a peacekeeping mission in Bosnia and found that selfreports of family concerns explained more than half the variability in measures of depression, hyper-alertness, anxiety, and somatic complaints.
Service members also worry about their partners’ ability to cope. The 2003 Air Force Community Assessment survey of over 30,000 Air Force members serving on active duty asked members to rate their spouses’ readiness to cope with deployment-related challenges. Approximately one-third of junior enlisted members and members married less than 3 years indicated that their spouses would have a serious or very serious problem coping with deployment. Protective factors included military-unit relationship quality, military leadership effectiveness, and tangible social support from community members (Spera, 2009).
Spouses themselves also reported elevated worries and psychologic symptoms prior to service members’ deployments, although baseline levels of these issues in the military spouse population are not well documented. For example, members of a sample of 295 Army active-duty-component spouses recruited from Family Readiness Groups shortly before departure of a Brigade Combat Team for deployment (response rate 33%) reported scores on the Perceived Stress Scale that were substantially above the community norm. One-quarter of the spouses reported scores consistent with mild depressive symptoms, another half reported scores consistent with depression, and one in 10 reported symptoms of severe depression. Almost all spouses (90% or more) reported two stressors: “feeling lonely” and concerns about the “safety of the deployed spouse.” Four additional stressors were reported by at least half the spouses:
“having problems communicating with my spouse,” “raising a young child while my spouse is not present,” “caring/raising/disciplining children with my spouse absent,” and “balancing between work and family obligations/responsibilities.” Levels of depression were not related to number of stressors or prior deployments or number of children at home (Warner et al., 2009).
During Deployment
Relationships are often a worry for military members during deployment. Since 2003, family separation has consistently been among the top concerns of service members stationed in Iraq and Afghanistan and has been more strongly related to mental health problems than to any other concern (MHAT-V, 2008). A study of Navy sailors assigned to carriers showed that concerns about the children, and especially the marriage and the spouse, were expressed by substantially more participants during deployment and following return than before deployment (McNulty, 2005).
Hurley (2011) observed in a study of 129 Army spouses that a substantial proportion developed heightened rejection sensitivity partway through deployment, fearful that their deployed partners had decided to leave the marriage. These fears were significantly and negatively related to relationship adjustment, even though participants could identify no precipitating reason for their fear; fears also appeared to increase with cumulative months of separation.
Hinojosa et al. (2012) delved into communication difficulties experienced by 20 reservecomponent members of the Army and Marine Corps during deployment, exposing specific challenges related to expressions of emotion. According to the participants, each partner’s worry about the other led them to withhold information because of fears about revealing their own vulnerability or exposing vulnerability in their partner. The diminished familiarity with one another’s day-to-day lives created a sense of disconnectedness and additional difficulties between spouses.
Baptist et al. (2011) observed many of the same patterns, including the tension between spouses who not only engaged in high levels of contact to maintain strong emotional connections but also limited information to insulate one another from stressors at home or in the war zone. When spouses chose not to disclose stressors they had experienced, they foreclosed the possibility of receiving support from their partners. Similarly, Lara-Cinisomo et al. (2011) found that at-home caregivers who experienced difficulty expressing feelings to their deployed partners reported lower satisfaction and more hassles in their relationship. Earlier, Bowling and Sherman (2008) suggested that service members and their family members coped with the stresses of deployment by suppressing their emotional responses and that this suppression could impede processes of reconnecting with one another after return. During the current conflicts, the prospect of possible future deployments and separations might complicate the reestablishment of intimate relationships.
Mulligan et al. (2012) and others have observed that access to immediate communication with home during deployment can present challenges. Although it offers a practical and immediate way for service members to participate in family life, it also might involve service members in solving problems that could be resolved without their attention. The authors suggested that service members and spouses be taught strategies to determine how to make the best choices of methods, content, and timing of communication. Carter et al. (2011) examined
the communication of 193 Army couples characterized on average by high levels of marital satisfaction during deployment, including both frequency and type of communication (interactive, such as instant messaging and telephone calls; and delayed, such as emails, letters, and care packages). Many of the couples exchanged emails, instant messages, and phone calls daily and typically exchanged letters and care packages once or twice per month. More than half also used video instant messaging once per month. Results showed that service members reported lower levels of PTSD symptoms following deployment when they had communicated more frequently with their spouses during deployment but only when marital satisfaction was high and only when delayed forms of communication, such as letters, emails, and care packages, were used.
In the MHAT studies, length of deployment was positively correlated with the percentage of deployed service members who indicated that they planned to obtain a divorce or to separate after their return; for example, the MHAT-V study estimated that about 6% of noncommissioned Army officers indicated plans to divorce at 1 month of deployment, compared with over 20% at 15 months of deployment (MHAT-V, 2008). Plans to divorce or separate also appeared to be inversely correlated with pay grade: The MHAT-V study reported that, in 2007, 17.0% of junior enlisted soldiers deployed for 9 months were considering getting a divorce, compared with 12.3% of noncommissioned officers and 3.6% of officers. Mulligan et al. (2012) studied 2,000 British service members during deployments to Iraq and Afghanistan. They found that both family problems (death or illness of a loved one, financial problems, or problems with children) and home and relationship breakdowns were negatively related to mental health by a large amount. Although high military-unit cohesion and effective military leadership fully mediated the relationship between relationship breakdown and mental health, family problems at home could not be completely compensated for by unit cohesion or military leadership. In addition, perceptions of poor military support for families at home were negatively related to mental health regardless of combat exposure, unit cohesion, or effective leadership.
Several studies have presented empirical data regarding the logistic, psychologic, and economic challenges experienced by marital partners during deployment. Logistic challenges include maintaining a household with only one adult present, such as management of maintenance, repair, and financial activity; providing all necessary care for children; maintaining employment; and arranging medical care or other services that are affected by military regulations (for example, reserve-component families may need to change medical providers when TRICARE coverage begins and ends) (SteelFisher et al., 2008). SteelFisher et al. (2008) conducted telephone interviews early in 2004 with 744 Army spouses associated with units that were deployed to the Persian Gulf during the first 4 years after the event on September 11, 2001 (9/11). Some of them had experienced an unexpected extension of their partners’ deployment. Deployment-induced logistic problems included difficulty in communication (sent and received) with the deployed members (41.0%), problems with household and car maintenance (29.0%), and problems finding child care (16.2%). Chandra et al. (2010a) and Lara-Cinisomo et al. (2011) surveyed over 1,000 at-home caregivers of children ages 7 to 17 who applied to have their children attend “Operation Purple” camps and conducted qualitative interviews with 50 participants. Baseline data were gathered during the summer of 2008; followups were conducted 6 and 12 months later. More than half of the caregivers surveyed reported one or more of the following logistic challenges associated with deployment: taking on more responsibilities at home; helping children deal with life without the deployed parent; spending more time with children on homework; and talking to teachers about children’s school performance. A
substantial proportion of spouses (30–50%) relocated during deployment. Proximity to extended family members increased, but it meant leaving local military services and causing children to change schools and living arrangements (Flake et al., 2009).
Psychologic challenges experienced by both service members and their spouses include fears for the safety of the service member, feeling anxious and overwhelmed by deploymentrelated challenges and responsibilities, worry about children, and concerns about military leadership, as well as vulnerability to additional stressors that might arise. In SteelFisher et al. (2008), the most common adverse effects of deployment on well-being that were reported by spouses were psychologic: loneliness (78.2%), anxiety (51.6%), depression (42.6%), and fears about personal safety (23.6%). A notable minority of the sample reported adverse perceptions of the military, the most commonly cited problem being lack of accurate information surrounding the timing of deployment, given that an unexpected extension had occurred (48.4%). According to Wright et al. (2006), fear of injury or death constituted major factors in the psychologic health of spouses throughout the deployment cycle, but especially before and during deployment. Existing data suggested that these concerns and fears tended to center on military training and leadership, the possible injury or death of service members, and concerns about managing on their own if that occurred.
In Chandra et al. (2010a), approximately half of the at-home spouses reported feeling that people in the community did not understand what life was like for them, particularly if they were affiliated with the reserve component. In addition, difficulties associated with new household duties were associated with increased anxiety and feelings of being overwhelmed (Lara-Cinisomo et al., 2011). Chandra et al. (2010a) also found that emotional well-being declined over time among caregivers who were experiencing deployment, but well-being improved if deployment ended during the course of the study. Overall, there were several indications in Lara-Cinisomo et al. (2011) of the same sample that reserve-component families were more likely than active-component families to experience deployment-related difficulties. For example, caregivers in both National Guard and reserve families reported significantly greater household and relationship hassles, and caregivers in National Guard families reported poorer emotional well-being.
Allen et al. (2011) studied 300 couples with active-duty Army husbands and civilian wives who experienced a deployment within the previous year. Top concerns during the year for both husbands and wives were exposure to combat and the effects of the deployment on children. Husbands’ other strongest concerns pertained to sexual frustration; wives’ other strongest concerns pertained to loneliness and staying in touch, injury and fear of death, and reintegration and fears about potential changes in the service member. Infidelity was not a major concern reported by either husbands or wives.
Economic challenges associated with deployment can include loss of spousal employment or difficulty paying for child care or other household services usually provided by the deployed family member. Reserve-component members experience small income increases on average, although some lose income during deployment (Angrist and Johnson, 2000). In the SteelFisher et al. (2008) study, spouses of service members experiencing a deployment extension were more likely to report problems with work and to have scaled back or left work; they were also more likely to report problems in their marriages than spouses who did not experience an extension. Reported problems with overall health (21%) and perceived effects on jobs (18%) were more prevalent than financial problems (12%) or problems with their marriage (10%).
Marital Quality on Return from Deployment
Many of the same adjustments and role reallocations that must be completed as deployments begin must be completed again when service members return home (Bowling and Sherman, 2008; Pincus et al., 2001). Studies conducted after return from deployment emphasize the implications of psychologic symptoms of service members, but many other aspects of the reintegration experience may be consequential for adults and children.
Following World War II, Hill (1949) recognized that families’ experiences following reintegration were partially a function of their experiences and behavior during deployment. Some families appeared to function exceptionally well during deployment, “closing ranks” as if the deployed service member was unneeded or irrelevant; other families had great difficulty continuing to perform even basic tasks in the absence of the service members. Families who seemed to function best were those that closed ranks only enough to fulfill important tasks but not so much that there was no place for the service member upon his return. Research conducted during the Vietnam era reinforced these observations, demonstrating that families who maintained the service members’ psychologic presence during deployment seemed to adapt more effectively when difficulties occurred (McCubbin et al., 1975).
Although most studies fail to measure positive consequences of deployment, the Rosen et al. (1995) study of Army couples who experienced deployments associated with Operation Desert Storm in Iraq found that the five most common reunion events were positive: the soldier was pleased with the spouse’s handling of finances or running of the household, the couple became closer, the spouse became more independent, and the soldier did more chores. All positive events were reported by at least one-third of the sample. The five least common reunion events reported by no more than 10% of the sample were the following: the spouse became more dependent, the soldier was critical of the spouse’s handling of finances, the soldier resented the spouse’s new friends, and the spouse resented the soldier’s new friends.
Following deployment, the couples in Baptist et al. (2011) who had been able to maintain the ability to exchange mutual support with their partners also were more likely to report closeness in their marriages. Religious faith and belief in the importance of the military mission also were helpful. However, participants also reported suppressing, avoiding, or restraining sexual behavior with their spouses, all of which interfered with marital closeness (Baptist et al., 2011).
In a review of existing literature about reintegration following war-related separations, Vormbrock (1993) found that longer separations were related to more distress, detachment, and damage to the attachment relationship. Although both service members and spouses tended to engage in contact-seeking behavior, home-based spouses were more likely than service members to display detachment and anger. Rosen et al. (1995) gathered data from 776 Army wives 1 year after deployments to Operation Desert Storm to test Vormbrock’s conclusions. Both Vormbrock and Rosen et al. found that separation distress was heightened by stressful events during the separation but lessened when adults had access to alternative attachment figures; however, revival of childhood attachments, such as those to parents, could undermine the marital relationship.
After deployment, Sahlstein et al. (2009) observed, “soldiers and spouses often found themselves struggling to know how, when, and what to communicate with one another.” Families who were able to achieve a quick “return to normal” had maintained open lines of
communication, working as a team throughout the deployment. In most couples, however, there were mismatches between the service member’s willingness to share and the spouse’s willingness to hear.
Baptist et al. (2011) also found that both husbands and wives reported withholding information from their spouses in efforts to protect them from distress. Wives reported continuing to perform household duties following husbands’ return from deployment when they would have preferred greater involvement by husbands, and both husbands and wives reported restraining sexual desires. Although well intentioned, these decisions usually were made without consulting the partner about his or her preferences. Nelson Goff and Smith (2005) also observed that couples who were unable to reconnect following deployment were a function of both prior marital problems, such as infidelity, and difficulties in sharing information, exchanging comfort, and supporting each other.
Although reintegration processes are typically described as occurring over time, few studies have empirically documented the sequence, durations, or content of these processes, particularly as they relate to families. In several studies, members of families affiliated with the National Guard and reserves have reported greater difficulties or poorer outcomes associated with deployment (Chandra et al., 2010a; Lara-Cinisomo et al., 2011). Faber et al. (2008) observed that reservists experienced prolonged ambiguity about their family roles and greater adjustment difficulties when return to the civilian workforce did not go smoothly. Civilian spouses and children might need to change medical providers, and civilian communities might be poorly prepared to serve military families (Huebner et al., 2009).
Summary of the Impact of Deployment on Marital Quality
In summary, as a result of deployment, marital quality is affected by psychologic challenges, including worry and uncertainty, that appear more prevalent than logistic issues (for example, managing the household) or economic difficulties (for example, loss of spousal employment). Some stressors are specific to a particular phase of the deployment cycle (that is, predeployment, during deployment, and postdeployment), and may dissipate as families move through the deployment cycle (for example, worries about a service member’s safety during deployment may lessen upon returning home). Others stressors are evident throughout (for example, communication issues) and may be a chronic symptom in a couple’s relationship. Male service members and their wives share many of the same concerns, such as concerns about the well-being of children and the service member’s safety, but also have separate ones. Dominant concerns among male service members include worries about the impact of separation on their families and worries about their spouses’ ability to cope with deployment-related challenges, including loneliness and household responsibilities. (The concerns of female service members are probably similar; however, there is a lack of studies of female service members to confirm the similarity.) The most common stressors among female spouses include feelings of loneliness, fears about their spouses’ death or injury, raising children alone, and problems communicating with their spouses. Spouses who are depressed and families that are members of the reserve component are more likely to experience deployment-related challenges. Families may also have positive experiences as a result of deployment, such as family bonding and increase competence in family functioning. Important to the understanding of the impact of deployment on marital quality is knowledge about what issues—individual or relational—may have been preexisting and not a symptom of deployment per se. Epidemiologic research that characterizes military
spouses irrespective of their experiences with deployment is lacking. Other gaps in the research base are related to the normative course, duration, and sequence of stressors experienced by military families as a result of deployment.
Marital Dissolution
Many media outlets have reported “skyrocketing” divorce rates as a result of deploymentrelated stressors (Alvarez, 2007; Crary, 2005; Parsons, 2008), and such an expectation seems reasonable given lengthy and repeated family separations. The empirical evidence so far is mixed, possibly because insufficient time has elapsed for the consequences of deployment to have become fully evident.
As noted earlier, military divorce rates have risen in the past decade. This section examines several investigations that have been conducted to determine the role of deployments in these increases. Two explanations have been proposed to explain divorce rates in the military. According to the stress hypothesis, the stressors of military life erode the stability of marriages, suggesting a positive relationship between deployment and the likelihood of divorce. In contrast, the selection hypothesis suggests that the likelihood of divorce is tied to characteristics of the partners and their relationships (Karney and Crown, 2007) and thus would not increase because of deployments.
Data from prior wars are inconsistent. For example, Ruger et al. (2002) studied 3,800 veterans of World War II and the conflicts in Korea and Vietnam using data from the National Survey of Families and Households. Veterans married prior to the Vietnam War were no more likely to divorce than those married after, failing to support the stress hypothesis at least with regard to deployment-related separation. A consistent finding across wars and robust to statistical controls, however, was that exposure to combat did increase the likelihood of marital dissolution, consistent with the stress hypothesis. More recently, a large representative survey of military members (59,631) showed that deployment to Operation Desert Storm was associated with a statistically significant increase, by 4.2 percentage points, in later divorce rates of female service members (Angrist and Johnson, 2000), but no association occurred among male service members.
Contrary to the view that longer deployments raise the risk of marital dissolution, (Karney and Crown, 2007, 2011) found in a study of personnel records of over 560,000 service members who married in 2002–2005 that the longer a service member was deployed, the lower the risk of divorce or separation. Risk was lowest for individuals who would normally be thought of as the most vulnerable—those who had married younger and who had children in the home. These results were not consistent with the hypothesis that the stress of deployment undermines otherwise healthy marriages. The findings were preliminary, however, because they focused only on relatively recent marriages that were followed for only a short period.
The most recent analyses were conducted by Negrusa and Negrusa (2012), who calculated the likelihood of marital dissolution as a function of deployment, using a military longitudinal dataset spanning from 1999 to 2008. They found that deployment substantially increased the risk of divorce, with the effect being stronger for female service members and for service members who were sent on hostile deployments (typically, to Iraq and Afghanistan).
In summary, results are mixed regarding the reasons for the rise in divorce rates in the military over the past decade. Both selection effects (preexisting characteristics of couples) and
stress effects (increasing operational tempo and more hostile deployments) appear to be relevant factors.
Spousal Abuse
Family violence, which includes spousal abuse1 as well as child maltreatment, has become a focus of concern in the military. This section covers spousal violence in terms of prevalence, types of abuse, risk factors, health consequences of abuse, and treatment.
Prevalence and Types
In 2011, the rate of substantiated incidents of spousal abuse was 11.1 per 1,000 couples (DOD, 2012c). This rate extends an upward trend that began in FY 2009. Before then, from FY 2001 to FY 2008, the rate had been declining (Figure 6.1). The data are compiled annually by DOD’s Family Advocacy Program (FAP), which was created in 1984 to identify, prevent, and treat family violence in the military. Because each report of spousal abuse reflects a single incident, there can be more than one report for a single victim. The abuser could have been an active-duty service member or a civilian. Finally, the data are not broken down by OEF or OIF; they are DOD-wide incidents.
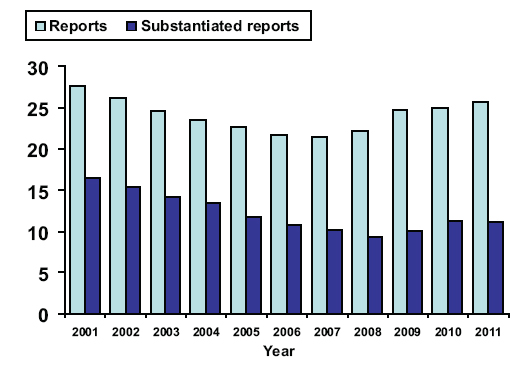
FIGURE 6.1 Rate of spousal-abuse reports per 1,000 couples to the Family Advocacy Program, 2001– 2011.
SOURCE: DOD, 2012c.
Spousal abuse is distributed as follows: physical abuse accounts for 90% of spousalabuse cases; emotional abuse, 6–8%; sexual abuse, 0.5%; and neglect, 0.4% (Rentz et al., 2006). Two-thirds (67%) of abusers are male and one-third (33%) are female (DOD, 2012c). In FY 2011, there were 18 fatalities tied to spousal abuse (DOD, 2012c). The occurrence of spousal abuse, as compiled by the FAP, is probably an underestimate: incidents often go unreported out of concern for career implications of the active-duty service member or for victims’ concerns
__________________
1In this chapter, spousal abuse is synonymous with intimate partner violence and domestic abuse.
about their physical safety.2 The overall rate of spousal abuse in the military is similar to that of civilians, although the only study to address the comparison dates back to the 1990s (Heyman and Neidig, 1999).
Risk Factors
Deployment is perceived as the foremost stressor in the military, according to a 2005 DOD survey of some 16,000 male and female active-duty service members (Bray et al., 2006). Not surprisingly, deployment has been identified in the medical literature as a risk factor for spousal aggression in the aftermath of deployment. This finding was reported in a random sample of 26,835 deployed and nondeployed married active-duty members in the Army (McCarroll et al., 2000). The study also found that the likelihood of severe aggression rose with the length of deployment. With a short length of deployment (6 months), deployment was not found to be a risk factor in the first 10 months after return from deployment, but younger age was a risk factor (Newby et al., 2005b).
PTSD first emerged as a risk factor for intimate partner violence in Vietnam veterans. The National Vietnam Veterans Readjustment Study found that one-third of the males with PTSD exhibited violence, according to their female partners (Kulka et al., 1990). A similar rate of violence was found among veterans with PTSD seen at a Veterans Administration (VA) medical center from 2003 to 2008 (Taft et al., 2009). In a recent study of Navy recruits, PTSD also was identified as a risk factor, having an odds ratio of 2.05, compared with recruits without PTSD (Merrill et al., 2004). Having PTSD symptoms of arousal and feeling a lack of control were the most robust predictors of aggression (Taft et al., 2009).
Substance use also has been found to be a risk factor for spousal abuse, according to a study of two Army databases of offenders, the Army Central Registry and the Drug and Alcohol Management Information System. The study found that 25% of 7,424 service members were under the influence of substances during the abuse incident. They were more likely than nonsubstance abusers to be physically violent and to exert more severe spousal abuse (Martin et al., 2010). A separate study found that the odds ratios for spousal abuse were 1.90 for alcohol problems and 2.02 for drug use (Merrill et al., 2004). However, in another study, alcohol use was unrelated to intimate partner violence among 248 married enlisted female soldiers, regardless of whether they were perpetrators or victims (Forgey and Badger, 2010).
In the only study on spousal abuse specifically in OIF and OEF service members, experiential avoidance—a coping strategy that seeks to avoid emotionally painful events—was associated with physical aggression perpetration and victimization in a study of 49 male National Guard members who returned from deployment to Iraq (Reddy et al., 2011).
Consequences and Treatment
Although data on the consequences of spousal abuse specific to military families are not available, in civilian studies, spousal abuse has been found to be associated with numerous negative outcomes. In studies of sheltered female domestic-violence victims, PTSD prevalence ranged from 51% to 75% (Golding, 1999; Street and Arias, 2001), depression ranged from 35% to 70% (Golding, 1999; O’ Leary, 1999), and substance-abuse disorders occurred in about 10%
__________________
2The figures are also underestimated because DOD maintains another database of law-enforcement cases of abuse—the Defense Incident-Based Reporting System, which covers the minority of cases that rise to a crime.
of victims (Helfrich et al., 2008). Similar findings were reported in a community sample of 94 women who were evaluated by diagnostic interviews (Nathanson et al., 2012). In the latter study, psychologic abuse was more likely to be associated with a mental disorder than with physical abuse.
The committee found little information about treatment of spousal abuse, which is a service provided by the FAP itself or in conjunction with local treatment providers. In 2010, the Government Accountability Office (GAO) concluded that, despite some improvements subsequent to the mandate to establish a DOD Task Force on Domestic Violence that was included in the National Defense Authorization Act for Fiscal Year 2000, “DOD lacks the sustained leadership and oversight of its efforts to prevent and treat domestic abuse that would enable the department to accurately assess the effectiveness of these efforts” (GAO, 2010).
The DOD monitors spousal abuse treatment by this one metric: the percentage of abusers who are not reported for spousal abuse within 1 year of program completed. As noted elsewhere in this chapter, the DOD reported that 97% of abusers who completed the program in FY 2011 were not reported (DOD, 2012b). Yet, no information is given about the content of the treatment program, how programs are evaluated, and their impact on the mental health of victims. The civilian literature indicates that many treatment programs for spousal-abuse victims or perpetrators are only minimally effective (Babcock et al., 2004; Nelson et al., 2004).
Summary
In summary, a service member’s psychologic issues are related to increases in marital distress, divorce, and disruptions in family life. Findings also suggest that the reverse is true: family relationships, both before and after deployment, can influence how a service member experiences PTSD in terms of coping with symptoms and symptom severity. Moreover, relationship quality may have an impact on treatment seeking by a service member. A spouse’s perception of a service member’s psychologic health (for example, perceptions of the apparent cause for symptoms or of the service member’s control over symptoms) influences the level of personal and marital distress experienced by the spouse.
Service members’ deployment is associated with increases in mental-health problems, particularly depression and anxiety, among spouses. Length of deployment and cumulative months of deployment predict increases in the likelihood of distress, but the number of deployments does not. Pregnant women with deployed partners experience high levels of stress and depression, particularly if they have other children. Although overall rates of spousal abuse in the military do not appear to be higher than those in the civilian population, there is evidence that the risk of spousal physical violence is higher after deployment, the risk increasing with the length of deployment.
The impact that the presence of children has on the psychologic well-being of a parent with a deployed spouse is somewhat ambiguous. Some studies have found that a parent’s worry about the well-being of their children and concerns over the logistics of providing care add to deployment-related stress. Other studies indicate that mothers and female spouses without children experience similar levels of distress. At least one study found that the presence of children is protective against depression in the stay-at-home parent. More studies are needed to understand the specific stressors faced by single parents serving in the Armed Forces.
Single Service Members and Their Families
Little attention has been paid by researchers to single service members who have experienced deployment and the degree to which family formation processes have been delayed or disrupted as a result. However, some of the same themes relating to deployment and marital quality discussed above are evident in a study of single service members living with their parents following return from deployment. Worthen et al. (2012) conducted qualitative interviews of OEF and OIF veterans living with their parents on the basis of the finding that 60% of young people return home to live with parents at some point. In most cases, veterans described their experiences as positive, and parents were helpful in recognizing health and adjustment problems. Distinct from the experiences of couples, adult children sometimes struggled with feeling treated as a child by their parents. Some service members were motivated by conflict with their parents to pursue school, a relationship, or work with undue haste. Women veterans interviewed in the study, a substantial proportion of whom had experienced military sexual trauma, had mixed experiences in terms of parental support, some experiencing ideal support but others experiencing conflict with or “smothering” by their parents. Few programs were available to educate or support parents in their efforts to assist their adult children.
Psychologic Health of Family Members
Among service members whose deployment experiences result in personality changes or psychologic symptoms and diagnosis, particularly PTSD, there are consequences for marital quality as well as specific psychologic effects on spouses and children. These are discussed below.
Psychologic Health of Spouses
Several studies have examined the prevalence of psychologic symptoms among military spouses in relation to deployment-related stressors. Eaton et al. (2008) studied over 700 active-duty-component military spouses seeking primary care at military facilities. According to both broad and strict screening criteria, spouses and service members reported similar levels of major depression or generalized anxiety disorders (using broad screening criteria, 19.5% and 15.6%, respectively, for spouses and service members). Spouses were more likely than service members, however, to seek care (70% vs 40%) and less likely to be impeded in doing so by worries about stigma, although more than 25% reported one or more of the following barriers to obtaining care: arranging child care or time off from work, difficulty getting an appointment, or cost. About 20% of spouses received care only from primary care physicians rather than from mental-health specialists.
An analysis of medical records of over 250,000 military wives done by Mansfield et al. (2010) revealed similar patterns. After controlling for background characteristics (age, number of deployments, pay grade, and years of service of the military member) and mental-health history, there were 39.3 excess cases of depression per 1,000 population among spouses whose partners were deployed for longer than 11 months and 27.4 excess cases among women whose husbands had been deployed 1 to 11 months (compared with wives of nondeployed partners), and 30% of this group had higher rates of service use. Overall, wives whose husbands were deployed were significantly more likely to have diagnoses of depression, anxiety, acute stress reaction, adjustment disorders, and sleep disorders than wives whose husbands had not been deployed.
Spouses of deployed service members also used mental health services at higher rates, which increased with deployment length. The likelihood of any mental-health diagnosis was 19% higher among women whose husbands had been deployed 1 to 11 months (41.3 excess cases/1,0000) and 27% higher among women whose husbands had been deployed longer than 11 months (60.7 excess cases/1,000).
In a study by SteelFisher et al. (2008), spouses who experienced deployment extension reported increased levels of mental-health problems relative to those who did not. Half of the spouses reported frequent feelings of anxiety, and almost half reported frequent feelings of depression. In a sample of 332 National Guard members and 212 partners, Gorman et al. (2011) found that 40% and 34%, respectively, met screening criteria for one or more mental-health problems. In that group, 50% of service members and 61% of partners had attempted to obtain help. Barriers encountered by partners included cost, difficulty getting time away from work or scheduling appointments, and not knowing where to get help.
Across studies, most military spouses who reported psychologic symptoms also reported seeking care (Eaton et al., 2008; Gorman et al., 2011; Warner et al., 2009), but most encountered barriers to care, including difficulty in getting time off from work, arranging child care, difficulty getting an appointment, and cost. Barriers reported by active-duty and reserve-component spouses were similar.
Two small studies focused on spouses’ stress and coping with the demands of their service members’ military duties. In one, spouses evaluated their partners’ deployment as one of the most stressful experiences of recent years in their lives (Dimiceli et al., 2010). In turn, spouses’ perceived stress was positively related to their levels of well-being (Padden et al., 2011) and psychologic symptoms (Dimiceli et al., 2010). Consistent with the broader literature on stress, coping strategies focused on problem-solving, and taking action appeared to predict better psychologic health (Dimiceli et al., 2010; Padden et al., 2011).
Psychologic Health of Families with Children
Another topic that has received attention from researchers is the psychologic health of parents or caregivers of children in military families. Consistent with studies of civilian families (Luthar, 2006) and military families during the first Gulf War (Jensen et al., 1996), studies of military families during the current conflicts found that distress among parents and the children they care for are positively related. In addition, adults’ distress was found to be a function of cumulative exposure to deployment but not to number of deployments (Lara-Cinisomo et al., 2011; Lester et al., 2010)—but note that both of these studies focused exclusively on families still in military service.
In the Lara-Cinisomo et al. (2011) study of 1,337 mothers or caregivers (children ages 11 to 17) affiliated with the active and reserve components of the military, cumulative months of deployment in the past 3 years significantly predicted difficulties related to mental health, relationship with the service member, and household management. Current deployment was significantly and positively related to caregiver mental health and relationship difficulties. Caregivers of children affiliated with the National Guard reported significantly greater difficulties than caregivers of children affiliated with the reserves or the active component.
Similarly, in another study contrasting parents with currently deployed and recently returned military spouses in the Army and Marine Corps, distress—specifically, anxiety—was
significantly greater among parents whose partners were currently deployed. Emotional distress measured by global severity, depression, and anxiety scores on the Brief Symptom Inventory were significantly increased among both at-home civilians and active-duty parents. For example, global severity was 0.46 for civilians and 0.53 for active-duty parents compared with a community norm of 0.35. More than 25% of parents reported clinically significant global distress (26.4%), depression (30.1%), or anxiety (26.4%) (Lester et al., 2010).
It is not clear, however, that parenthood exacerbates stressors related to military service. Hopkins-Chadwick and Ryan-Wenger (2009) compared junior enlisted women serving in the Air Force with and without children (50 of each) younger than 5 living at home. Mothers and nonmothers reported similar levels of role strain, stress, health, and military career aspirations. Warner et al. (2009) found that the presence of children was protective in relation to depression.
Psychologic Health of Single Parents
The literature on stress and the military has focused primarily on two-parent families, and research on single parents is scare. What little does exist about single parents in the military was published approximately two decades ago, so it might not represent experiences from the more recent conflicts. Kelley et al. (2001) reported that, among Navy mothers, the level of separation anxiety was highest among single mothers anticipating deployment.
Spousal Physical and Psychologic Health During Pregnancy
A small number of studies have investigated the possible impact of deployment on the health of military spouses during pregnancy. To date, few differences in physical health have been found. For example, a cross-sectional survey of postpartum mothers at Camp LeJeune during 2003 revealed no differences in gestational age, likelihood of vaginal delivery, number of previous children, or weight gain between those with deployed or nondeployed partners. Mothers whose partners were deployed were more likely to report having changed their eating habits during pregnancy and had infants who were on average almost 300 grams heavier (Haas and Pazdernik, 2006).
Differences were found regarding the psychologic health of pregnant military spouses. For example, a survey of 525 pregnant women seeking services at the Naval Hospital at Camp LeJeune in 2005 revealed that women reported significantly higher levels of stress if their partners were deployed, if they themselves served on active duty, if they were farther along in their pregnancy, or had more than one child at home (Haas and Pazdernik, 2007). Robrecht et al. (2008) reviewed the medical records of 415 women who had recently given birth, finding that women whose spouses had been deployed during the pregnancy were 2.75 times more likely to screen positive for postnatal depression. Finally, an examination of screenings of 3,956 women with military spouses conducted at the first obstetrics visit during pregnancy, at the 28-week visit, and at 6 weeks postpartum between 2007 and 2009 revealed that mothers were significantly more likely to exceed clinical cutoffs for depression during the initial obstetrics visit if their spouses were preparing to deploy or had recently returned from deployment. At 28 weeks gestation, depression scores were higher for women whose partners were deployed or returning from deployment. Postpartum, depression scores were significantly higher for women whose partners were deployed (de Burgh et al., 2011; Smith et al., 2010). Note, however, that already having children at home was more strongly related to perceived stress among pregnant spouses than deployment of partners in most of these studies.
Psychologic Health of Surviving Spouses
Death is an inevitable accompaniment of war, and the OEF and OIF wars have left behind thousands of spouses, children, and other family members to mourn the loss of a loved one. To date, however, there are no comprehensive studies of bereavement in US military families. To address this gap, the Center for Traumatic Stress is currently undertaking a 5-year study of bereavement in about 3,000 family members, including spouses, parents, and siblings of deceased service members—the first scientific study of the impact of US military deaths on surviving family members. The focus will be not only on combat deaths but also on homicides, suicides, and accidents (Jowers, 2011).
Consequences of Service Members’ Psychologic Symptoms for Marital Quality
The largest area of research related to deployment and families pertains to the implications of service members’ combat- or deployment-related psychologic symptoms and diagnoses, particularly PTSD, for the quality and stability of relationships with intimate partners and children. Data collected from the 2004 through 2007 National Surveys on Drug Use and Health (SAMHSA, 2008), which surveyed veterans ages 21 through 39 (deployment history not known), showed that three-quarters of those who had experienced a major depressive episode the previous year reported being severely or very severely impaired in at least one of four role domains: home management, work, close relationships with others, and social life. Half reported severe or very severe impairment in role functioning with respect to close relationships with others.
Recent studies also are revealing ways in which relationship dynamics may influence vulnerability to and severity of psychologic symptoms among service members, and the likelihood of seeking treatment. In this section, we deal with the relationships between service members’ psychologic symptoms and marital quality; in a later section, we consider the implications of service members’ injuries for caregivers’ own well-being and functioning.
According to a review by Monson et al. (2009), studies of previous conflicts repeatedly found links between PTSD and relationship problems, including divorce. Specific symptom clusters might be linked to specific types of relationship problems. For example, the arousal cluster of symptoms is found to be related to greater hostility and violence directed by service members or veterans toward their partners, while the numbing and avoidance cluster is related to difficulties with intimacy, including sharing and receiving communication about emotions, as well as general relationship satisfaction. For male service members but less so for females, the effects of combat exposure are mediated through psychologic symptoms. Other possible mechanisms of influence include secondary traumatization and caregiver burden experienced by partners, but many research questions are yet to be answered.
Almost all studies have focused on the effects of PTSD on interpersonal relationships, but there also are reasons to expect that relationships can affect the occurrence of and prognosis for PTSD (Erbes, 2011; Monson et al., 2009). For example, social support, of which family relationships are a primary source, is negatively related to PTSD symptoms. In addition, relationship patterns among intimate partners may prolong or reduce avoidant behavior or support or discourage emotional expression, each of which can affect the course of PTSD. For example, intimate-relationship partners might be helpful in keeping service members engaged
with others rather than withdrawing. Conversely, strain or distance in intimate relationships might reinforce service members’ negative cognitions associated with PTSD (Erbes, 2011).
Several studies from both current and previous conflicts revealed positive relationships between service members’ deployment-related psychologic symptoms and disruptions in family life. Most of these studies were cross-sectional, and many were conducted with samples recruited from health clinics or hospitals. For example, Sayers (2011) studied 199 veterans of service during OEF and OIF who had been referred for behavioral health specialty care. Three of four of those who were married or living with a partner reported family problems in the past week, including feeling like a guest in their own home (40.7%). One of four reported that their children were acting afraid or distant. Among veterans who were currently or had recently separated from their partners, most reported that they had episodes of “shouting, pushing, or shoving” (54%) or that their partners were afraid of them (27.6%).
Johnson (2011) studied 60 spouses of veterans of OEF and OIF service in a mixture of branches and components, most of whom had been deployed multiple times. On average, the spouses reported significant negative change in 13 of 18 characteristics, including increases in veterans’ tendencies to be quick-tempered, irritable, unhappy, cold, lifeless, mean, cruel, unreasonable, insensitive, and changeable. When service members’ personalities had changed more, spouses reported higher levels of grief, which in turn were associated with more frequent arguments and less social support. These relationships appeared robust to a variety of demographic characteristics.
A group of studies using data from the Readiness and Resilience in National Guard Soldiers (RINGS) study documented interpersonal dynamics surrounding service members’ PTSD symptoms. Conducted as a partnership of the Minneapolis VA, the University of Minnesota, and the Minnesota National Guard, the studies’ participants were composed of members of the Minnesota Army National Guard and their partners. Erbes (2011) examined data provided by 522 RINGS participants before and after deployment, finding that 24% of the variability in postdeployment PTSD symptoms was accounted for by predeployment predictors, including psychologic symptoms at that time, prior exposure to trauma, concerns about occupational or family disruption, feeling insufficiently prepared or supported for the mission, and being younger or female.
In a factor analytic study, Erbes et al. (2011) examined the connection between specific PTSD symptom clusters and relationship adjustment. The dysphoria cluster appeared to be the most important factor explaining intimate-relationship adjustment within the 6 months following service members’ return from deployment and the only significant predicting relationship adjustment 1 year later. Thus, much of the impact of PTSD on couple adjustment may be because of the generalized distress that accompanies the disorder, rather than specific symptoms related to reexperiencing or arousal. The extent to which some PTSD symptoms predicted relationship disruption was substantially greater for female soldiers. There was a trend for PTSD avoidance symptoms to have a greater impact on couple relationships among female soldiers than male soldiers.
Evidence from both the Erbes (2011) study and others suggests that spouses’ attributions about their partners’ symptoms influence the spouses’ levels of personal and marital distress. Specifically, when spouses cannot see an obvious cause for their partners’ symptoms or when they perceive their partners as being able but choosing not to exert control over symptoms, they
may respond with less support and more distress. In two small studies of the OEF and OIF conflicts, wives were more distressed when they could not see an obvious cause for their husbands’ symptoms, whether because wives perceived symptoms that their husbands failed to acknowledge or husbands reported more severe symptoms than their wives expected, given what was known about their combat experience (Goff et al., 2007; Renshaw and Campbell, 2011; Renshaw and Caska, 2012; Renshaw et al., 2008). Pietrzak and Southwick (2011) observed similar patterns in a sample of 272 members of the National Guard and reserves, averaging 34 years of age, in that the group who experienced high exposure to combat and high levels of PTSD symptoms also reported the most problems in psychologic and social functioning, while the group of service members who experienced high exposure to combat but reported low levels of PTSD symptoms were significantly more likely than others to report receiving support and understanding from their families and to perceive a sense of purpose and control.
Erbes (2011) and Renshaw and Campbell (2011) concluded that generalized distress was a prominent feature of couples’ experiences related to PTSD. Erbes (2011) found that general dysphoria in service members, including irritability and numbing, was more strongly related to relationship adjustment than either reexperiencing or arousal, perhaps because dysphoria is less obviously connected to service members’ combat experiences than other symptom clusters. Renshaw and colleagues investigated the degree to which spouses’ psychologic symptoms reflected a form of secondary traumatization related to their partners’ symptoms, as opposed to a more generalized form of distress, and found greater support for the generalized form of distress among most spouses (Renshaw et al., 2011).
Using data from the RINGS project, Meis et al. (2010) examined processes that could be responsible for corroding relationship quality following return from deployment. Controlling for prior exposure to trauma and prior PTSD symptoms (but not prior relationship distress), levels of negative emotionality among service members before deployment significantly predicted levels of PTSD symptoms following return. In turn, the PTSD symptoms were significantly related to lower relationship quality. Service members with probable PTSD were more than half as likely as those without to experience relationship distress (33% vs 20%).
Symptom severity of PTSD and relationship quality may interact to influence the likelihood of seeking treatment and the nature of treatment sought. Buchanan et al. (2011) conducted a qualitative study with 34 wives or partners of combat veterans to learn their strategies for encouraging service members to seek treatment, as well as the barriers spouses perceived. Partners perceived the main barriers as service members’ denial, fear, and stigma about disclosing their symptoms. Partners’ strategies included offering support and patience, making suggestions that treatment be sought, initiating treatment themselves, or issuing ultimatums. Meis et al. (2010), in a sample of 223 coupled RINGS participants, found that the severity of PTSD symptoms interacted with relationship quality to predict the type of treatment sought, even though symptom severity predicted greater service use overall (to the exclusion of relationship quality when both were considered together as independent variables). At higher levels of relationship adjustment, more severe PTSD symptoms predicted use of individualoriented treatment, and relationship quality was unrelated to seeking couple or family care. At lower levels of PTSD symptoms, poorer relationship adjustment significantly predicted seeking couple or family care. These results suggest that once PTSD symptoms reach a certain (yet unknown) threshold, service members may be less willing to simultaneously deal with relationship issues and their symptoms. Or perhaps beyond this threshold, relationship
difficulties are such that couple-oriented treatment does not seem possible. Researchers are only beginning to sort out these issues as they pertain to returning veterans and their families.
MILITARY CHILDREN AND DEPLOYMENT
Children in military families have the advantage of a number of resources that help to buffer them from risks that many nonmilitary children might experience (Sheppard et al., 2010). In numerous respects, military families have a stronger socioeconomic safety net than many of their civilian contemporaries in the United States, where about 22% of children live in poverty and over a third (34%) live in a single-parent household (Annie E. Casey Foundation, 2012; Federal Interagency Forum on Child and Family Statistics, 2012). In 2010, 29% children lived in families where no parent had full-time, year-round employment (Federal Interagency Forum on Child and Family Statistics, 2012); that percentage is not a problem among military families. Although military children face the risk of traumatic events happening to their parents, so do many nonmilitary children. Military families have access to child care and health services that are often far superior to those available to civilian families at similar income levels. Housing is related to family size, and military installations tend to have good schools, good sports, and recreation facilities, and a system of support services, including ones targeted for the families of deployed or injured personnel.
On the other hand, military children may also have to cope with circumstances specific to military families, such as parents leaving for and returning from deployments (which can be unexpected, prolonged, and repeated), and the medical, psychologic, and economic consequences of deployment. The family may have to relocate frequently, either because the military member gets stationed at a new location, because the family members wish to relocate temporarily during a deployment (for example, to stay with relatives who can help with child care), or because the child of a single custodial military parent must go to live with another caretaker while the parent is deployed. Military families are more than four times as likely as civilian families to move to international locations, requiring them to adapt to unfamiliar cultures (Reinkober Drummet et al., 2003). Access to health care can also change if the family relocates during deployment, especially if they are no longer living near a military base. Relationships with peers, as well as local institutions (including schools), may also be disrupted. Parents may come back damaged, physically or psychologically. Or, tragically, they may not return at all.
These contrasts are part of the lives of children in families of OEF and OIF military personnel.
General Stressors for Military Children
Any review of military children and families dealing with deployment of a parent must take into account that these additional stressors occur against a background of exposure to the ordinary risks of daily life. Thus, before discussing the specific needs of children of parents deployed in OEF or OIF, it is useful to think about the stressors military children might experience (irrespective of whether their parent or parents have deployed) and the levels at which those stressors can occur in the general population. Stressors include parental absence, having to move multiple times, parental psychopathology, and death of a parent, as well as the effects on children of having to deal with the other parent’s reactions to such events. These stressors give a sense of the ordinary level of stress and strain that military families might experience, beyond which is the need to cope with the challenges presented by deployment.
Like children in military families, children in civilian families might experience the absence of a parent. Parental absence most often refers to the absence of the father; this is certainly true in military families, where—despite the increasing number of women in the military—the deployed service member is still much more likely to be male. According to 2011 US Census Bureau data, over 20 million children under age 18 live apart from their biologic fathers3; that is, just over a quarter (27%) of children in America (an additional 3% live apart from their mother, and 4% live apart from both parents) (US Census Bureau, 2011b). Absence of fathers, although an expected concomitant of military life during wartime, is thus not an uncommon experience for civilian children, although the nature of that absence may be different. Examples for children are temporary absence due to deployment to a war zone of fathers in intact households or in households where custody is shared after a divorce versus the ongoing absence of noninvolved fathers with whom the children have limited or no relationship.
Multiple Relocations
An estimated one-third of military families relocate annually, with families commonly moving every 3 years (Orthner and Rose, 2002). Just as periodic moves are an expected part of military life, it is also common for civilian families to move (NRC and IOM, 2010). From 2003 and 2004, about 14% of the US population moved—the rate for people living below the poverty level are higher (24%). Whether moving is for positive reasons (for example, relocation for a higher paying job or to be closer to family) or negative ones (for example, following eviction or foreclosure or breakup of a family), it is potentially disruptive for children. It can, for example, interrupt their learning in school, disrupt peer relationships, and disconnect children from important relationships with adults and institutions in the community (NRC and IOM, 2010). Impacts can also vary, depending on the age and developmental stage of the child, as brain development, capacities for dealing with stress, and behavior all change over time in ways that can affect a child’s ability to manage a move.
National longitudinal studies that examine the impact of relocation on school achievement are sparse, and it is difficult to disentangle the effects of mobility from other factors (for example, poverty and family characteristics). However, although the impact of a single move may be negligible overall, the negative impact on achievement is cumulative and increases with the number of moves (especially above a threshold of three to four or more moves). The impact is greater for some groups of children, especially certain ethnic minority groups, those at lower socioeconomic status levels, and those whose families are downwardly mobile (NRC and IOM, 2010). In the civilian population, multiple moves are thus positively associated with social disadvantage in a way that is not the case in military families who have both stable employment and guaranteed housing.
Parental Mental Illness and Substance Abuse
The number of children in either military or civilian families who live with a parent with a mental disorder is unknown. However, mental illness clearly occurs in both military and civilian families. Screening at the recruitment stage acts to limit the entry of individuals with serious mental illness into the military; however, mental illness can still develop later (for
__________________
3Includes children living with neither parent.
example, PTSD resulting from deployment experiences), and nonmilitary spouses may also have mental illness. National survey data on child exposure to parental mental illness are sparse, and most studies that look at children of people with mental illness focus only on clinical populations, making it difficult to estimate exposure in the general population. However, a Canadian study that extrapolated from the 2002 Canadian Community Health Survey and the 2006 Canadian census data (Bassani et al., 2009) found that approximately 12% of children under age 12 lived with a parent with a mental disorder (substance use disorder, 10.0%; mood disorder, 5.1%; and anxiety disorder, 4.6%). The National Survey on Drug Use and Health reported similar results for child exposure to parental alcohol-use disorder, finding that an average of approximately 7.5 million children each year in the United States (10.1% of all children) live with a parent with an alcohol-use disorder (Center for Behavioral Health Statistics and Quality, 2012).
Parental Death
The death of a parent is a highly traumatic event for any child. Like military deaths, civilian deaths may be sudden, such as in the case of a suicide or a car accident, or may follow long drawn-out illness or be the eventual consequence of a serious injury. Again, like military children, civilian children lose more fathers than mothers.
Although precise figures cannot be found, about 3.5% of children experience the death of a parent by the time they are 18 years of age (Haine et al., 2008). In December 2011, more than 1.2 million children under age 18 (approximately 1.6% of all children) were receiving Old-Age, Survivors, and Disability Insurance (OASDI) benefits because of the death of a parent (US Social Security Administration, 2012), and 1.1% of children were living with an unmarried widowed parent (US Census Bureau, 2011a). According to the report of the Census Bureau’s 2009 Survey of Income and Program Participation, 49,000 mothers and 36,000 fathers who were living with their children had been widowed in the previous year (Kreider and Ellis, 2011).
The Impact of Deployment on Children of OIF or OEF Families
As of February 2007, an estimated 700,000 children had experienced a parental absence because of deployment in OEF or OIF, sometimes for multiple periods (Engel et al., 2010). Since then, the number of children affected by the deployment of a parent has increased. Many parents, service providers, and policy makers are concerned about the implications of parental deployment for children. However, research evidence remains sparse, and the use of more powerful longitudinal or quasi-experimental designs has been rare. In this section, we review the literature on children from military families, with special reference to children with one or both parents deployed in OEF or OIF. This review is limited to adequately powered studies that use sound research methods. Two main methods are used in the research to date: examination of military records and in-person studies of selected individuals.
Deployment-Related Stressors and Children’s Mental Health
Most studies of prior conflicts have suggested that deployment is associated with a variety of internalizing (such as sadness, depression, and anxiety) and externalizing (such as aggressiveness and irritability) symptoms in children that in most cases are not clinically significant (Cozza et al., 2005; Lincoln et al., 2008; Sheppard et al., 2010). Studies from the current wars have generally been consistent with that earlier research. Studies have also been
consistent in finding that longer cumulative time spent deployed is associated with more problems.
Reviewing electronic medical records, Mansfield et al. (2011) compared rates of psychiatric diagnoses found in the records of over 300,000 children ages 5 to 17 of three groups of military personnel: those with up to 11 months of deployment in OIF or OEF; those with 12 or more months of deployment; and those with no deployment. Having a deployed parent was associated with an excess of all major diagnoses in comparison to being a child without a deployed parent. The excess was greater in older children and boys and those whose parent had been deployed for a year or more. As in most record-based analyses, it is not possible to conclude from this study whether children of deployed parents suffered more psychiatric disorders or whether (1) parents were more anxious or vigilant and more likely to bring their children to a medical provider and (2) medical care providers were more likely to diagnose disorders in children of deployed parents. However, the study does provide preliminary evidence that longer periods of deployment may put children at greater risk.
One of the largest studies of military parents and their children included interviews of over 1,500 caregiver-and-child pairs from military families in all branches of the military and reserve forces who were recruited from applicants for a military summer camp (Chandra et al., 2010a). Followup interviews were conducted at 6- and 12-month intervals. The study found that military children experienced significantly higher levels emotional and behavioral difficulties than those reported from the US Census Bureau’s 2001 National Health Interview Survey, a large national sample. Chandra et al. (2010a) also found that more time deployed was associated with increased prevalence of adjustment difficulties (such as school problems and anxiety) in children during both deployment and reintegration. Spouses of reserve-component service members were especially likely to report that their children were experiencing difficulties. Although the study was limited by using participants from a service-seeking group, it provides valuable insight into the concerns of children of deployed service members over the course of deployment and reintegration.
A cross-sectional study of a convenience sample of 272 children ages 6 to 12 from families with a deployed or recently returned parent found that anxiety scores were higher than community norms for both deployment groups (Lester et al., 2010). No mean differences were found in depressed mood or behavioral symptoms for the children in the study compared with population norms. In multivariate analyses, mood and behavioral symptoms were higher in children whose military parent was deployed for longer periods and for whom either parent reported higher levels of psychologic symptoms; the effects of long parental deployment were seen even after the parent returned.
Using input from parents and child care providers, a study of 169 preschoolers in child development centers at a large Marine Corps installation compared children of parents deployed in OIF or OEF with other military children and with national norms and found that children of deployed parents had significantly higher scores on both internalizing (mood) and externalizing (behavior) measures (Chartrand et al., 2008). Among the small number of children who scored in the clinical range, the only significant differences were in the area of internalizing problems. Although this study was cross-sectional and did not measure change from predeployment to deployment or postdeployment, it provides some evidence for an effect of parental deployment on children’s mood and behavior.
Impact of Parental Stress on Children’s Mental Health
Another concern is the effect on children of a custodial parent’s reaction to the other parent’s death, injury, disability, absence, or psychopathology. Studies during the first Gulf War demonstrated that children’s psychologic symptoms were more severe when their mothers’ own well-being was seriously compromised (Cozza et al., 2005). Similarly, parents who reported high levels of stress were much more likely to report symptoms in their children (Flake et al., 2009).
In research focused on deployments during the current wars, Chartrand et al. (2008) found that spouses of deployed service members who had children age 3 or older had significantly higher depression scores than spouses of nondeployed personnel; their children exhibited increased behavioral symptoms compared with peers who did not have a deployed parent. Another analysis of the psychosocial effects of deployment on military children found that families experiencing deployment identified one-third of the children at “high risk” for psychosocial morbidity and that parental stress was the most significant predictor of children’s psychosocial functioning (Flake et al., 2009). Lester et al. (2010) also found evidence that parental distress and length of parental deployment both increased anxiety levels in elementary-school-age children. However, the mean overall scores were not higher than those of the community samples on which the instruments were set at the norm. In another study of children of deployed parents (Chandra et al., 2011), 68% of youth reported that “helping the caregiver deal with life without deployed parent” was one of the most difficult aspects of the deployment. The study also found that youth whose nondeployed parent was doing worse emotionally reported having more difficulties during deployment; parents doing less well emotionally were likewise more likely to report that their children had greater emotional, social, and academic difficulties.
Parents who access military support services report less child psychologic morbidity. This finding suggests that use of services might ease parenting stress and underscores the necessity of providing military families with the support they need to cope with and adjust to deployment. Families considered more vulnerable to adjustment difficulties and in need of targeted outreach include families who are simultaneously undergoing other major transitions, such as relocation, pregnancy (Haas and Pazdernik, 2007), and bereavement, as well as families who have junior military personnel and families who have multiple needs and problems before deployment (Booth et al., 2007).
Deployment and Risk for Child Maltreatment
In FY 2011, there were 6,819 substantiated reports of child maltreatment among approximately 1,165,812 million children in military families. The number represents a rate of 5.8/1,000 children, a rate approximately half that in the US civilian population (DOD, 2012c). Still, the DOD rate is trending upward after having reached a nadir in FY 2009 (Figure 6.2).
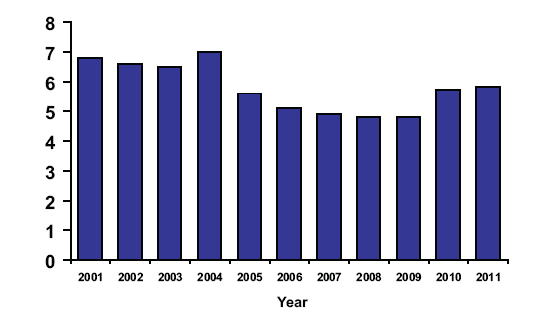
FIGURE 6.2 Rate of substantiated child abuse and neglect reports per 1,000 children to the Family Advocacy Program, 2001–2011.
SOURCE: DOD, 2012c.
Emotional abuse and neglect account for 71% of child maltreatment cases; physical abuse for 23%; and sexual abuse for 6%. Just over half (54%) of abusers are male, 45% being female. In FY 2011, there were 33 fatalities tied to child maltreatment (DOD, 2012c).
Risk Factors: Parental deployment might increase children’s risk for maltreatment. Although rates in general appear to be no higher than those in the civilian population, overall rates of child maltreatment (particularly neglect) by the nondeployed spouse appears to rise during deployment. A case series of substantiated child maltreatment by parents in 1,771 families of enlisted Army soldiers who were deployed at least once from September 2001 to December 2004 found that child maltreatment was more frequent during the times when the military parent was deployed than at other times, the most common perpetrators being civilian mothers (Gibbs et al., 2007). The incident records came from the Army Central Registry, which were merged with personnel records of the military parent, yielding information about entry to and exit from the Army as well as about deployment of the service member to OEF or OIF. The main type of maltreatment reported was neglect, which nearly quadrupled during deployment for civilian wives. Overall, the rate of child maltreatment was 42% higher during deployment than nondeployment; the rate of child neglect also rose during deployment, while the rate of physical abuse fell. Although information is missing in this study (for example, the psychologic status of the nondeployed parents before and during deployment), the large sample of substantiated abuse cases directs attention to the needs of the left-behind parents, especially those with preschool and grade-school-age children. This study is the only one of child maltreatment expressly in the OIF and OEF population.
Another study (Rentz et al., 2007) used time-series analysis to test the impact of operational deployments on maltreatment in military and nonmilitary families in Texas from 2000 to 2003, and the effect of deployment escalations after the September 2001 terrorist attacks in the United States. The study found that the rate of substantiated maltreatment reports for children of military families doubled, whereas the rate for civilian families was unchanged. About 90% of perpetrators were parents, with offenders being about equally divided between the military and the nonmilitary parent until October 2002, after which the nonmilitary parent was more often the offender, perhaps because more military parents were deployed. The study also
found that reintegration can be a high-risk period, as the increases in rates of child maltreatment observed as service members left for deployment also occurred when they returned.
Consequences and Treatment: It is not surprising that child maltreatment has negative consequences. Although data from military populations are not available, child maltreatment is associated in civilian studies with the development of depression, anxiety, alcohol abuse, attempted suicide, as well as chronic health conditions, such as heart disease, cancer, and chronic lung disease (Felitti et al., 1998; McCauley et al., 1997). A longitudinal study also found that nearly half of childhood physical or sexual abuse victims developed at least two mental disorders by age 21 (Silverman et al., 1996).
The committee was unable to find any information about the treatments rendered for child maltreatment victims by DOD’s Family Advocacy Program. The foremost evidence-based treatment for maltreated children is trauma-focused cognitive behavioral therapy (CBT) (Mannarino et al., 2012; Silverman et al., 2008). Trauma-focused CBT helps to alleviate posttraumatic stress, depressive symptoms, anxiety symptoms, and externalizing behavior problems.
Impact of Parental Injury on Children’s Mental Health
There is considerable concern about the impact of parental injury on children of returning OIF and OEF military members. Injured parents might have reduced capacity to respond sensitively to their children, and noninjured parents might provide less attention to children because of the demands of caring for their injured spouses (Cozza et al., 2005; Perlesz et al., 1999).
In a study in which 41 spouses of recently injured service members were interviewed, Cozza et al. (2010) reported on the relationship of child postinjury distress to preinjury deployment-related family distress and the family postinjury disruption. The main predictor of children’s distress was the emotional state of the family before deployment. As expected, children whose caregiver reported a high level of family distress before the injury were seen as having a high level of distress after the injury. This study is small and uses nonstandard measures, but it confirms a body of research showing that vulnerability to the impact of a major stressor is often influenced by the level of distress or family disruption before the stressor.
Impact of Parental Death on Children’s Mental Health
As of March 2008, over 3,400 children had experienced the death of a parent during the OEF and OIF conflicts (US House of Representatives, 2008). Although sparse, available data indicate that bereaved children are at increased risk for psychiatric disorders or behavioral or emotional problems (Cozza et al., 2005). However, little guidance is available to help children understand and adapt to the death or life-altering injury of a parent (Cozza, 2007).
Children of service members may struggle to understand the signature rituals of a military death, including formal notification, return of remains, and military funerals (Cohen and Mannarino, 2011). Death during deployment, when there has already been a long separation, can trigger children to develop maladaptive cognitions or omens, regret, and self-blame (for example, “If daddy hadn’t been so worried about me he would have been paying more attention and wouldn’t have gotten shot.”). Reactions to a military death can be magnified if the death is
by suicide. Both children and adults can feel a mixture of guilt, confusion, rejection, anger, and shame (Cohen and Mannarino, 2011; Shear, 2012).
One of the first studies to examine childhood reactions to a combat-related death of a parent was performed by Israeli researchers examining the impact of the 1973 October War. The researchers found that 70% of the children ages 2 to 10 whose father had died in the war experienced significant emotional symptoms and behavior problems, such as fear, separation anxiety, discipline problems, learning disabilities, and social withdrawal that might today be labeled as a type of traumatic grief. In a 4-year followup of this longitudinal sample of 25 children, the likelihood of a child developing traumatic grief was enhanced by such pretraumatic risk factors as poor impulse control, emotional lability, and explosive rage. Marital discord in parents before the death also increased the likelihood of traumatic grief, as did the mother’s mourning pattern. If the mother showed emotional restraint, it was difficult for children to express their feelings, and it heightened their sense of loneliness (Elizur and Kaffman, 1983). Children reacting to combat-related trauma also suffer from more conventional disorders, such as PTSD, depression, and anxiety (Smith et al., 2001), but the studies (for example, Mghir et al., 1995) focused on wartime stressors, not on the death of a parent who was a combatant.
Use of Health Care Services for Children
Data from TRICARE, the health care program for uniformed service members, retirees, and their families, provide the primary information on the needs of children, as reflected in their use of TRICARE-related services. Researchers have merged this information with deployment data to estimate the extent to which parental deployment affects medical and mental health service use.
Use of Medical Services for Children
Eide et al. (2010) used data on almost 170,000 children under the age of 2 enrolled in TRICARE and deployment data from the Defense Manpower Data Center to determine whether parental deployment influenced the rate at which parents used health care for their young children within the military health system. Overall, children made 7% more outpatient visits and 8% more well-child visits during periods of deployment. However, the increase was not consistent across marital status and age of the caregiving parent: children of younger single parents had fewer visits, and those of younger married parents had more visits. Both trends decreased as the parent’s age increased. The researchers suggested that younger married parents were more able to use TRICARE as a resource for their children than were single parents of children who might have been living with other relatives or caretakers with limited knowledge of or access to the military health system while their parent was deployed (because this study only captured health care visits within the military health system, it missed visits made with caretakers of those children to civilian health care settings). Because single-parent children experienced less frequent health care visits, the authors suggested that military social services should target families with young single parents.
Use of Mental-Health Services for Children
According to DOD records, military children’s use of mental-health care services rose substantially from 2003 to 2008: inpatient days rose by 50% or more, and appointments for mental-health problems rose by more than 85% per capita (IOM, 2010).
In one study, researchers Gorman et al. (2010) used data on over 600,000 children ages 3 to 8 enrolled in TRICARE; these data were merged with deployment data from the Defense Manpower Data Center to determine whether parental deployment influenced the rate at which parents used either medical or mental-health care for their children within the military health system. They found that mental health was the only clinical category for which visits increased when a parent was deployed. However, this finding was true only for children whose father was deployed. When the mother was deployed, mental-health-related visits fell. The older the child, the more likely it was that mental-health care would be sought, whether the deployed parent was male or female, married or single. This study underscores how central parents are in gaining access to mental health care for children. When mothers are in charge of getting services for their children, they seem to respond to their spouse’s absence with increased service-seeking. When fathers or other caregivers are in charge, help-seeking for mental and behavioral problems (but not for other areas of health care) drop.
Medicaid is an important supplement to TRICARE insurance for military children with special health care needs (CSHCN). Medicaid covers one in 9 military children with special health care needs. Among military CSHCN who are enrolled in Medicaid, 49% have low family incomes and 31% are nonwhite (Shin et al., 2005). Medicaid’s capacity to mitigate the needs of military children may be reduced by state-to-state mobility of military families, variations in coverage and health care resources across states, and the location of military bases outside of metropolitan areas. In 2005, TRICARE initiated the “Extended Care Health Option” (ECHO) program, which supplements TRICARE basic benefits for qualifying disabled or special needs family members of active duty service members (Shin et al., 2005). The committee is not aware of any data about the extent to which ECHO may reduce reliance on Medicaid among lower income military CSHCN.
Educational Achievement of Children
There are numerous ways in which parental deployment can have negative impacts on children’s school performance (Chandra et al., 2010b; Richardson et al., 2011). For example, children might have more difficulty completing homework assignments, particularly if the deployed parents were part of their children’s homework routine or if their children are saddled with more household responsibilities while their parents are absent. Schooling may be disrupted if families move during deployment to be closer to supportive family members, and the children must adjust to being in a new school and having to develop new peer relationships. Sadness or distress about parents’ deployment can also make it difficult for children to focus on school. Poor mental health of the nondeployed parents can likewise have a negative impact on school performance if, for example, the parents become disengaged from the school and from monitoring the children’s academic performance.
Children’s scores on academic achievement tests have been shown to drop slightly as a function of parental deployment. An examination of records from Texas that combined US Army personnel data with children’s standardized test scores found that parental absences adversely affected children’s test scores by a tenth of a standard deviation. Likewise, household relocations had modest negative effects on children’s test scores (Lyle, 2006). Both parental absences and household relocations had the greatest detrimental effect on test scores of children with single parents, children with mothers in the Army, and younger children. The study highlights the finding that deployment can have many consequences, including relocations, which can mean a
new school for children, the attendant risks being disrupted education and relationships. The impact on school achievement was modest overall, and no person-based analyses were carried out that could identify the children at greatest risk.
Another study, which looked at reading and math achievement for more than 44,000 students in North Carolina and Washington, found that elementary- and middle-school students with a parent who had been deployed for at least 19 months since 2001 had lower achievement scores than those of students with less or no parental deployment (Richardson et al., 2011). This association was not, however, present for high-school students. Although the total time deployed had a significant negative impact on achievement for younger students, the relationship between the number of deployments and performance was not significant.
Summary
The findings summarized here must be taken as suggestive rather than conclusive. Military databases are not designed primarily to examine the effects of deployment on children, and most studies of families and children suffer from a range of methodologic limitations that limit their generalizability (for example, convenience samples and small sample sizes). Nonetheless, an important conclusion of the extant research is that, in normal circumstances, military children enjoy good mental health; their scores on nationally standardized scales are equal to or exceed those of the general population. Second, studies underscore the importance of parental distress as a predictor of childhood symptoms. However, the TRICARE databases, as currently analyzed, do not permit researchers to distinguish parental distress as a predictor of child problems from parental distress as a predictor of increased help-seeking behavior. Treating distressed parents might be as important to child mental health as treating the children themselves.
It is important to understand more about how parental characteristics that predict selection for deployment also predict children’s response to parental deployment and parental reaction to returning home. From the viewpoint of the military-service system, it is critical to identify the small group of families at especially high risk of disruption during or after parental deployment. To answer these questions, researchers need a combination of integrated analyses of existing databases and larger, well-controlled studies of military personnel and their families, including studies that examine them over time.
FAMILY CAREGIVERS
As Chapter 4 illustrates, physical injuries, serious mental-health diagnoses, such as PTSD, are being reported at high rates for the OEF and OIF population. Brain injuries, polytraumatic injuries, and psychologic wounds of war can have a profound impact on the injured survivors in that these injuries can often lead to long-term residual deficits and the need for ongoing care. (See Chapter 4 for more details about the incidence, prevalence, and long-term outcomes of the leading physical and psychologic injuries of the OEF and OIF conflicts.)
Family members frequently assume a significant role in caring for injured service members and veterans. In addition to providing emotional support, spouses, adult children, and parents often provide assistance with their loved ones’ physical care. Family assistance, referred to as informal caregiving, is often unpaid and typically involves helping with basic self-care
tasks, such as getting out of bed, dressing, and bathing—known as “activities of daily living” (ADLs)—and with “instrumental activities of daily living” (IADLs), which involve complex skills needed to live independently, such as managing finances, shopping, and housework. In addition, family members might also aid with therapies, coordinate formal health care services, and help navigate health insurance and legal systems. Given the scope of assistance, the presence of an informal caregiver is an important resource facilitating a care recipient’s ability to stay at home (Griffin et al., 2012; Van Houtven et al., 2010).
This section examines research on the impact that caregiving of war-related injuries has on family caregivers. Although a significant body of research literature exists about civilian caregivers who support civilian patients with life-altering wounds and injuries, studies on caregivers of service members or veterans whose injury or illness is related to military service is sparse. Summarizing the civilian literature is beyond the scope of this report, but this section includes references to civilian literature where it is especially relevant and can possibly inform the understanding of the military population serving in OEF and OIF.
Nature of Service Members’ Injuries
In 2010, the National Alliance for Caregiving (NAC) reported findings from an online survey of 562 self-identified family caregivers, ages 19 or older, who provided care to a veteran whose injury, illness, or condition was related to military service. Of all respondents, 38% provided care to a veteran who served in the OEF or OIF conflicts. Although the report did not break out the findings separately for OEF and OIF veterans, it did show that conditions for which younger veterans (under the age of 45) needed care differed greatly from older veterans or typical civilian care recipients. Veterans under the age of 45 had mental illness, PTSD, or traumatic brain injury at rates much higher than those reported for veterans aged 65 or older (78% vs 56%, 79% vs 36%, and 61% vs 10%, respectively) or than those reported for national civilian populations, where 28% of caregivers reported that their care recipients had mental or emotional health problems. Older veterans, on the other hand, were more likely than younger veterans to have diabetes (36% vs 6%), cancer (27% vs 4%), or Parkinson’s disease (13% vs 1%). One in five (20%) veterans being cared for had a spinal-cord injury (age breakdown not reported) (National Alliance for Caregiving, 2010).
Demographic data about veteran care recipients from the NAC survey revealed that veterans tend to be much younger than care recipients nationally—41% being between the ages of 18 and 54 (18% were between the ages of 18 and 34)—a reflection of the growing numbers of young veterans from the OEF and OIF conflicts.
Nature of Care Provided by Family Caregivers
According to the 2010 NAC survey of caregivers providing assistance to veterans, the majority (64%) of caregivers reported helping the veteran with one or more ADLs, including help with getting dressed (48%), getting in and out of beds and chairs (45%), and bathing or showering (44%). Virtually all (98%) of the caregivers surveyed said they help with IADLs. Among these tasks were housework (88%), managing finances (87%), transportation (85%), grocery shopping (85%), and preparing meals (84%). Nearly three-quarters (73%) administer medications or injections, and 46% help to arrange or supervise paid services. The likelihood of helping with several IADLs increases as the veteran’s age increases; those over age 65 not
surprisingly need more assistance than those under age 45. Caregivers also reported that they assisted in coordinating medical care and rehabilitative services (85%) and administering physical therapy or medical or treatments (61%) (National Alliance for Caregiving, 2010).
Characterizing the level of burden experienced by caregivers on the basis of the number of ADLs and IADLs performed and the number of hours of care given, the NAC survey found that 65% of the veteran caregivers have a high burden of care, 15% have a medium burden, and 21% have a low burden (National Alliance for Caregiving, 2010). The survey also revealed that providing care for a veteran with a service-related health problem is a longer-term endeavor than family caregiving in the general population. As compared with caregivers in the general population, caregivers of veterans are twice as likely (30% vs15%) to have been in their role for 10 years or more (National Alliance for Caregiving, 2010).
Several studies involving veterans and their caregivers provided information about how much time caregivers spend supporting veterans in need of informal care. Generally, the nature and severity of the veterans’ problems are factors that influence the amount of caregiving time provided. Van Houtven et al. (2010) surveyed veterans referred to home health care or homebased primary care in 2007 and their informal caregivers. Findings indicated that patients received substantially more informal than formal care from the health care system: on average, patients received 5.6 hours of VA care and 47 hours of informal care per week. The 89 veteran respondents were older and more frail, having an average age of 75 and having an average of 2.7 problems. Movement limitations and diabetes affected the largest share of respondents.
In 2009, Griffin et al. (2012) conducted a survey of 564 caregivers of service members with TBI (average age 30) who served in OEF or OIF and received care in a VA Polytrauma Rehabilitation Center from 2001 to 2009. After a median of 4 years since injury, about one in five (22%) patients still required help with ADLs and with IADLs, and nearly half (48%) required assistance with IADLs only. Nearly one-quarter (23%) of caregivers reported more than 40 hours per week of care. Among caregivers providing assistance with ADLs, half (49%) provided 80 hours or more of care per week. In addition to assisting with ADLs and IADLs, other types of tasks reported by caregivers included managing emotional issues (70%); navigating the health care (54%), benefits (53%), and legal (54%) systems; making medical appointments (44%); managing pain (36%); and aiding with therapies (37%) or assistive devices (33%) (Griffin et al., 2012).
The data provide estimates of the amount of time caregivers spend by the intensity of a care recipient’s needs, as well as insight into caregiving patterns over time. Among recipients with high-intensity needs, 49% of caregivers provided 80 hours or more of help per week, and 60% of caregivers of recipients with moderate-intensity needs provided less than 20 hours of help per week. Among recipients with low-intensity needs, 73% of caregivers provided less than 5 hours. The amount of time since injury did not affect the intensity of care recipients’ needs; even 7 or more years after the injuries, caregivers were still providing care (Griffin et al., 2012).
Robinson-Whelen and Rintala (2003) interviewed 348 veterans (average age 55) with a spinal-cord injury. Of the 130 participants who reported receiving informal unpaid care, 59% identified a spouse or partner as their primary caregiver; 17%, a parent; 9%, a sibling or spouse of a sibling; 8%, a child or spouse of a child; 2%, a friend; and 3%, some other person (for example, grandparent or niece). On average, informal caregivers provided all day care (11.6
hours per day)—the number of hours driven mostly by severity of injury (Robinson-Whelen and Rintala, 2003).
Characteristics of Family Care Providers
Demographic information from the 2010 NAC survey of caregivers of veterans whose illness, injury, or condition was service-related showed that the typical caregiver is a woman (96%) who is taking care of her husband or partner (70%). The majority (61%) of the caregivers are 50 years of age or older. Of the OEF and OIF veterans in need of care, over one-quarter (26%) are being cared for by their parents. One implication of this information is that caregiving responsibilities may need to be transitioned to others as their parents grow older (National Alliance for Caregiving, 2010).
The survey of caregivers of OEF and OIF service members with TBI conducted by Griffin et al. (2012) showed that, for this type of injury, parents were more likely to be the primary caregiver (62%) than the spouses (32%). Nearly half (48%) of the caregivers were a sibling, grandparent, other relative, or friend. These caregivers tended to be women (79%) and younger than age 60 (84%). A majority of the caregivers were solely responsible for the caregiving (59%) and were balancing both work and caregiving (55%); 31% were also caring for children or other dependent adults (Griffin et al., 2012).
Impact of Caregiving on Family Caregivers
Numerous studies of civilian populations have documented evidence that caregiving can have profound negative consequences for family caregivers in terms of burden, psychologic and physical health, emotional well-being, quality of life, employment, and financial status (for example, see Kreutzer et al., 2009; Pinquart and Sörensen, 2003; Schulz and Martire, 2004; Stenberg et al., 2010; van der Voort et al., 2007; Vitaliano et al., 2003; and Zarit, 2006). The focus of this section is on the few studies that assess caregiving effects specifically experienced by caregivers of veterans. Although there are common consequences of caregiving in the general population and those assisting veterans—for example, Griffin et al. (2009) cited evidence based on research on patients with TBI, stroke, dementia, and cancer that suggests that better functioning and supportive families are associated with improved patient outcomes—there are also differences. Even within the veteran-caregiver population, differences in caregiving are reported by type of war-related injury, for example, polytrauma versus TBI (Griffin et al., 2009).
Despite evidence for a preponderance of troublesome impacts, caregivers in the general population and caregivers of veterans also report positive aspects of caregiving. Research by Pinquart and Sörensen (2003) found that feeling useful or experiencing increases in closeness to the care recipient mitigated caregiver burden and depression. In the 2010 NAC survey of veteran caregivers, nearly all (94%) respondents reported feeling proud of the support they provide, and most felt a sense of reward from having gained new knowledge and skills from caregiving (78%) or feeling fulfilled by caregiving (67%).
The following discussion presents what is known about the impacts of caregiving, specifically experienced by caregivers of veterans.
Psychologic and Emotional Health of Caregivers
A study of caregivers of TBI patients who were 5 years or less postinjury found that, although about a third of the caregivers were experiencing increased levels of depression, anxiety, and somatic symptoms, most of the caregivers were coping adequately (Kreutzer et al., 2009). Higher caregiver distress was associated with caring for TBI patients who had worse functioning, who needed more supervision, who were less satisfied with life, and who abused alcohol. Respondents in the NAC survey of caregivers of veterans conveyed that providing care to their veteran took a toll on their psychologic and emotional health. Stress or anxiety was reported as the most prevalent health problem of caregivers (88%). When asked to indicate their level of emotional stress, two-thirds (68%) of caregivers reported that they were highly stressed. High emotional stress was most likely to be reported by caregivers for veterans with depression and anxiety, PTSD, or TBI. Depression was reported by 63% of the caregivers (National Alliance for Caregiving, 2010). However, caregivers also reported positive outcomes of caregiving. Nearly all (94%) agreed strongly or somewhat that they were proud of the support and assistance they provided, and 78% reported that gaining new knowledge and skills felt rewarding. Two-thirds agreed strongly or somewhat that caregiving had been fulfilling for them.
Caregiving puts strain on the caregivers’ personal relationships and can contribute to social isolation. Of those who were married, separated, or divorced, three-quarters (74%) of the respondents in the NAC survey said that caregiving placed strain on their marriage. A substantial share of caregivers reported a decline in time spent with family and friends (87%). Most (76%) felt that others did not understand what they are going through; this response was especially the case for those caring for a veteran with PTSD or TBI and for those caring for a younger veteran. Among the caregivers with children in their household, over two-thirds (69%) sacrificed the amount of time they spend with their children. More than half said that their children had experienced emotional or school problems (57%) (National Alliance for Caregiving, 2010). In a review of the civilian-caregiving literature, Blais and Boisvert (2005) similarly found the effect of increased social isolation and diminished social relationships among caregivers of spouses with TBI.
In another survey of 70 caregivers, Phelan et al. (2011) found that, for caregivers of veterans with TBI who did not serve during OEF or OIF, perceived discrimination and stigma were stressors that could lead to poor caregiver mental health outcomes. Specifically, there was a relationship between caregiver strain, social isolation, depression, and anxiety and the caregivers’ perceptions of being discriminated against and feelings of being stigmatized as a caregiver.
Physical Health of Caregivers
Caregivers are vulnerable to compromises in their physical health as a result of their caregiving responsibilities. Some of the physical effects reported by caregivers responding to the NAC survey of caregivers of veterans included sleep deprivation (77%), spending less time exercising (69%), delaying or skipping their own medical appointments (58%), poor eating habits (56%), and a high degree of physical strain (40%) (National Alliance for Caregiving, 2010). A meta-analysis of 23 studies comparing the physical health of 1,594 caregivers of family members with dementia and 1,478 demographically similar noncaregivers found that caregivers were at 9% greater risk of health problems, the size of the difference being moderated by the sex of the caregiver and the health category assessed (Vitaliano et al., 2003). This finding is
especially important in light of findings that a substantial proportion of providers of informal care face important health limitations themselves. In one study, one in four veteran patients reported that they expected their care providers to no longer be able to provide “the same level of care within 5 years” (Robinson-Whelen and Rintala, 2003). In the same study, almost one-third of the caregivers reported being in only fair or poor health themselves.
Employment and Financial Status of Caregivers
Caregivers often must make major life decisions related to their location of residence, employment, and education as a result of their caregiving role. In a random sample of 1,730 OEF or OIF active-duty component members, reserve component members, and retired veterans in 2007, 15% to 37% reported having a family member or friend who had relocated or left a job to provide care for a veteran, either temporarily or permanently (President’s Commission on Care for America’s Returning Wounded Warriors, 2007).
Among the respondents to the 2010 NAC survey of veteran caregivers, 59% of the caregivers were unemployed, 27% worked full time, and 14% worked part time. Of those who worked at some point since becoming a caregiver, 69% reported taking unpaid time off from work or stopping work temporarily, 62% reported cutting back the number of hours worked per week, and 47% stopped working entirely or took early retirement. Those more likely to stop working included caregivers of a veteran with depression and anxiety, diabetes, and paralysis or a spinal-cord injury. Other caregivers were compelled to continue working because of veteran’s condition and care needs. Of the caregivers aged 40 or older currently working, two-thirds (67%) said their own retirement plans were in question (National Alliance for Caregiving, 2010).
Studies examining the relationship between employment and caregiving in the general population found that caregiving affects labor-force participation and has both short-term and long-term economic consequences, particularly among women caregivers and those who are heavily involved in providing care (Lilly et al., 2007; Schulz and Martire, 2004). Other caregivers who are more likely to be out of the labor force, to work fewer hours, or to adjust their work hours to accommodate caregiving responsibilities include those in poor health, older caregivers, those with young children at home, those heavily involved in caregiving, those with less education or income, and those caring for persons with greater health limitations (Lilly et al., 2007).
The employment consequences reported by caregivers of veterans are also likely to be a major contributing factor to the serious financial strain experienced by families caring for veterans. Half (50%) of all caregivers responding to the 2010 NAC survey reported that caring for their veteran caused them a high degree of financial hardship. This percentage is a much higher proportion than the 13% of family caregivers nationwide reporting the same level of financial hardship (National Alliance for Caregiving, 2010). A survey of seriously wounded, ill, and injured service members about the economic impact of caregiving on their caregivers revealed that 37% of caregivers had unmet financial obligations, and 41% had new financial obligations. Those who provided more hours of assistance were more likely to have higher financial burdens (Christensen et al., 2009). The researchers estimated that the average loss in income and benefits for caregivers of seriously wounded, ill, and injured service members (assuming that care is needed for 19 months) is $60,300.
Factors Influencing Caregiver Experiences
Caregivers’ experiences vary considerably, and several variables, such as characteristics of the caregiver and the care recipient, are associated with the burden that caregivers experience. The following discussion largely reflects findings from the civilian literature but is not an exhaustive review.
Time since injury is not necessarily predictive of the need for care (Griffin et al., 2012; National Alliance for Caregiving, 2010; Vitaliano et al., 2003). In other words, care needs appear not to decline over time for some kinds of injuries. For example, Griffin et al. (2012) found that nearly a quarter (22%) of service members with TBI who had previously received inpatient rehabilitation care still required help with activities of daily living and instrumental activities of daily living about 4 years after injury; nearly half (48%) needed help only with instrumental ADLs. In addition, over half (56%) of caregivers in the 2010 National Alliance for Caregiving (2010) survey reported that they had been providing care to their veteran for 5 or more years; nearly a third (30%) had been providing care for a decade or longer.
Several characteristics of the care recipient were found to have an impact on caregiver burden. These included the presence of behavior problems (for example, aggression, agitation, and nighttime wandering) or dementia (Etters et al., 2008; Pinquart and Sörensen, 2003), as well as the severity of the care recipient’s symptoms, frequency of relapse, and hospitalization (van der Voort et al., 2007).
Characteristics of caregivers also were found to have an effect on caregiver burden. As reported in research with civilians, burden was positively related to living with the patient, difficulties in the relationship with the patient, an inability to cope with difficult behavior, stigma, and the caregiver’s belief that the patient was not making an effort to influence his or her symptoms (van der Voort et al., 2007). Caregivers who reported more self-efficacy, took time for themselves, and those who used more effective coping strategies had less burden (Etters et al., 2008). Ethnicity also plays a role; minority caregivers reported worse physical health than white caregivers, but findings were mixed for psychologic health (Pinquart and Sörensen, 2005).
The nature of the caregiver–recipient relationship was also associated with caregiver burden. Partners experienced more stress than parents, and young families with little social, financial, and psychiatric support or with medical problems were found to be the most vulnerable (Verhaeghe et al., 2005). Burden was higher for spouses who became caregivers than it was for adult children (Pinquart and Sörensen, 2011). There is also some research with the veteran population that informs understanding of caregiver burden. As discussed in the previous section, Psychologic Health of Family Members, research with spouses of combat veterans of OEF and OIF suggested that, in addition to the service members’ symptoms, spouses’ individual characteristics and perceptions of their partners’ symptoms might influence their levels of personal distress (Goff et al., 2007; Renshaw and Campbell, 2011; Renshaw and Caska, 2012; Renshaw et al., 2008). In particular, spouses might respond with less support and experience more distress when they cannot identify an obvious cause for their partners’ symptoms (for example, such as attributing their spouses’ emotional withdrawal to traumatic experiences during deployment) or when they perceive their partners as choosing not to exert control over symptoms.
Department of Veterans Affairs Caregiver Support Program
In recognition of the significant burden caregiving places on families, Congress passed and President Obama signed into law the Caregivers and Veterans Omnibus Health Services Act of 2010 (PL 111-163; 124 Stat. 1130), which authorizes the VA to provide new support services and benefits to caregivers of eligible veterans and service members seriously injured in the line of duty on or after September 11, 2001. Caregivers who qualify for the program are eligible to receive a monthly financial stipend, averaging about $1,600 a month, after completing a comprehensive caregiver training program. Other benefits available to caregivers include travel expenses associated with caregiving, access to health insurance (for caregivers not already entitled to health-plan coverage), mental-health services and counseling, and respite care that can help care for the veteran for a short time when the caregiver needs relief. As of August 30, 2012, nearly 6,000 primary family caregivers are receiving the monthly caregiver stipend (Gould, 2012).
Summary
In summary, although studies with civilian populations are helping to inform the understanding of the experiences of family caregivers, there is a paucity of evidence on the challenges and needs faced by families caring for patients with serious war-related injuries. The war-related care experience is complex, in part because of the severity of the injuries, the changing role from military to civilian family, and the stigma attached to disability and injuries (Griffin et al., 2009). Griffin et al. (2009) discussed the existence of “huge gaps in our understanding of the information, resources, and services families need to cope and function as their injured loved one recovers, rehabilitates, and reintegrates into the community.” Evidence suggested that providing caregivers with information they seek is an effective coping mechanism that can help reduce stress, anxiety, and uncertainty (Griffin et al., 2009).
PROGRAMS AND SERVICES FOR MILITARY FAMILIES
On the basis of the rationale that a well-served family is essential for retaining service members and force readiness, the DOD increased its support for military families with an everevolving catalog of programs aimed at meeting the needs of service members and their families. The wide-ranging programs cover such areas as psychologic health, child care, education, and personal finance. In this section, the discussion centers on programs and services for which there are data on implementation, utilization, or outcome research with military populations.
Programs and Services
Child Care
DOD has provided child care services to more than 200,000 military children from birth to age 12 at more than 900 child-development centers in over 300 locations worldwide and at 5,000 Family Child Care homes (DOD, 2012b). On the basis of demographic data, DOD estimated that an additional 37,000 military children still need child care but are not receiving it (DOD, 2010b). DOD (2012a) reported that it is continuing to build new child care facilities, both on and off base, to accommodate child care needs, concentrating on 13 states to expand
availability and the quality of child care services (DOD, 2012b). DOD also reported that 97% of its child care services are accredited by national accreditation agencies, thereby meeting standards for quality, and 100% are certified internally by DOD (2012b). All programs are inspected, unannounced, four times annually.
Regarding deployment-specific problems, in a 2009 survey of 802 spouses of active-duty Air Force airmen, the majority of respondents reported that their child care problems worsened following their spouses’ deployment. Parents who lived within 30 minutes of the base reported more problems finding child care than those who lived more than 30 minutes away, as did parents who were part of a dual-military family as compared with parents who were civilians. Spouses of enlisted airmen also reported more problems finding child care than did spouses of officers (Miller et al., 2011a).
Education
DOD Schools
Approximately 86,000 children of service members or DOD civilians attend 194 Department of Defense Education Activity (DODEA) schools in 14 school districts, 12 countries, 7 states, plus Guam and Puerto Rico. DODEA employs approximately 8,700 educators (DOD, 2012b). All DODEA schools are accredited by AdvancED (DOD, 2011a), an accreditation organization responsible for accrediting more than 30,000 public and private schools and districts in the United States (AdvancED, 2012).
DODEA tracks school performance with two standardized tests, the TerraNova and the Scholastic Aptitude Test (SAT). Both tests allow the DODEA to compare their students’ performance with national samples. For 2011, the DODEA’s goal was to have 75% of socialstudies students, 73% of students in reading and science, 72% of language arts students, and 70% of math students score at or above the 51st percentile on the TerraNova. The DODEA nearly met this goal; however, targets were missed by 1 percentage point in reading, science, and social studies, 2 percentage points in language arts, and 5 percentage points in math. In all subjects, DODEA schools failed to meet the goal of having no more than 7% of all students score below the 25th percentile (DOD, 2012b), rates for most subjects being 1 to 4 percentage points above the 7% benchmark (the highest rates were for math—11% of students scoring in the bottom 25%). For 2012, the DODEA goal is for 75% of students to score above the 51st percentile in all subjects, having no more than 7% fall into the bottom 25%.
On the SAT, the 2011 average critical reading score was 503, six points above the national average. In writing, the average was 489, the same as the national average. In math, the DODEA average was 495, which is 19 points below the national average (DOD, 2012b). When ethnicity was stratified, African American and Hispanic students scored significantly higher on the SAT in all three subjects in 2010 than was scored by African American and Hispanic students nationwide (DOD, 2011a).
To help improve student performance, DODEA has begun reducing class size in kindergarten to achieve a student-to-teacher ratio of 18:1 or better (DOD, 2011a). The DODEA has also launched an initiative to improve SAT math scores, which are lower than the national average. Program leaders reviewed and revised mathematics standards at all levels throughout the DODEA school system; the initiative also includes an extensive math program evaluation. In
the 2010–2011 school year, the DODEA began implementation of the new standards, which received top ratings from the Mid-continent Regional Educational Laboratory (DOD, 2011a).
In 2011, the DODEA announced plans to adopt the Common Core State Standards (CCSS), a research and evidence-based curriculum to replace its own curriculum standards in math and language arts. The new curriculum includes more progress assessments designed to help schools identify student achievement gaps. The CCSS is currently used in 46 states, so its use by the DODEA school system is expected not only to improve student performance but also to relieve problems arising from out-of-state school transfers (DOD, 2012b).
Disruptions in Children’s Education
Children from military families must relocate and change schools when a parent receives an order for what is called a “Permanent Change of Station” (PCS). A military child will attend, on average, six to nine schools from kindergarten to 12th grade (DOD, 2010b). Aside from the social disruptions associated with frequently switching schools, educational standards and requirements vary from state to state, creating administrative problems and delaying graduation and advancement. In response to problems with interstate school transfers, DOD developed the “Interstate Compact on Educational Opportunity for Military Children.” States that adopt the compact agree to provide uniform eligibility, enrollment, placement, and graduation policies with regard to military children. As of 2012, 40 states have adopted the compact, eliminating many of the problems associated with transferring from one state to another for 93% of all military children (DOD Education Activity, 2012). The DOD’s goal is for the compact to cover 100% of military school children by FY 2013 (DOD, 2012b).
Exceptional Family Member Program
Each military department has an “Exceptional Family Member Program” to work with the 120,000 enrolled military families with special-needs members (DOD, 2011a). DOD estimated that there are many more families with exceptional family members who have not enrolled, but it offered no estimate of how many (DOD, 2012b). The DOD provides, through TRICARE, basic medical services to exceptional family members at military installations within the United States. DOD will also provide in-home care and respite care when needed. However, the Government Accountability Office (GAO) found that DOD is not always equipped with the needed specialists, forcing some families to seek specialist services from neighboring installations or civilian providers (GAO, 2007). The GAO could not determine the scope and extent of the problem.
The National Defense Authorization Act FY 2010 established the Office of Community Support for Military Families with Special Needs (OSN) and requires military branches to expand community support for families with special-needs members to include referral assistance, assistance in obtaining services, and providing oversight (DOD, 2011a). The Act also requires DOD to report annually on gaps in service and to recommend ways to help fill those gaps (DOD, 2012b).
The OSN is currently collaborating with land-grant university faculty to complete several studies related to improving support for exceptional family members. A benchmark study will establish a uniform family support policy across the four services. The autism review study, conducted in two phases, is examining access in 15 states to evidence-based educational services for military children with autism. A Medicaid study—a collaboration with West Virginia
University—will assess the accessibility of Medicaid to military families with exceptional family members and assess how interstate relocation may be a barrier to receipt of Medicaid benefits. Finally, a functional analysis study will look at the support and services that each military service provides to families with exceptional family members. The findings are expected to help inform recommendations for a DOD-wide policy (DOD, 2012b).
Financial Readiness
DOD offers an array of financial management education programs, available both online and in person, aimed at all military personnel. The “Financial Readiness Campaign,” launched in 2003, is a DOD-wide program designed to provide additional financial readiness education and resources to complement existing efforts by individual services (DOD, 2010b).
The Status of Forces Survey, conducted by the Defense Manpower Data Center, provided a portrait of financial issues from junior enlisted soldiers in pay grades E1–E4. In general, respondents indicated fewer problems today than in 2002. About 15% of respondents in 2011, compared with about 26% in 2002, reported that it was “tough to make ends meet, but keeping your head above water” or “in over your head” (DOD, 2012b). Likewise, about 25% of respondents in 2010, compared with 47% in 2002, reported “one or more bill paying problems in the previous 12 months” (DOD, 2011a). In a separate 2010 survey of military spouses, however, 41% reported concerns about their personal finances (Defense Manpower Data Center, 2011). DOD did not undertake an assessment of its own financial readiness programs, so the disparity across surveys cannot be reconciled. Regarding deployment and its effect on finances, 29% of Air Force spouses surveyed reported that their financial problems worsened during the last deployment (Miller et al., 2011a). The committee was unable to find examples of DOD targeting financial problems specifically associated with deployment. Metrics to assess financial readiness programs are “currently being considered,” but no other information was provided over 3 consecutive years (DOD, 2010b).
Nonmedical Counseling
Nonmedical counseling refers to short-term, problem-focused counseling designed to address general conditions of living; it addresses such issues as stress management, marital problems, parenting issues, grief, and crisis intervention. (Medical counseling, on the other hand, is designed to address long-term, medically diagnosable issues, such as substance abuse, mental illness, or PTSD.) DOD offers confidential, free nonmedical counseling sessions to all activeduty, National Guard, and reserve members and their families. Services are available through Military OneSource and the Military and Family Life Counselor (MFLC) program. In FY 2009, Military OneSource provided over 133,000 in-person counseling sessions (DOD, 2010b). In FY 2010, it provided nearly 270,000 in-person counseling sessions (DOD, 2011a) and nearly 313,000 in 2011 (DOD, 2012b). Data regarding the number of telephone or online counseling sessions completed by Military OneSource were not reported. The MFLC program provides services to active-duty service members and families on or off military installations. Support is provided to the reserve components for mobilization, deployment, and reunion activities as requested by reserve unit commands. In FY 2009, the MFLC program completed almost 470,000 face-to-face contacts with military children and adults (DOD, 2010b). The number rose dramatically in FY 2010 to 5.5 million face-to-face contacts (DOD, 2011a) and 6.9 million face-to-face contacts in FY 2011 (DOD, 2012b). DOD sources did not give an explanation for the
striking rise in contacts from FY 2009 to FY 2010 and FY 2011, although it might be explained in part by some base commanders requiring returning troops to complete counseling with a Military and Family Life Counselor, additional staffing to increase capacity, expanded services for units returning from combat (“surge support”), and enhanced outreach capabilities (DOD, 2010b, 2012b).
DOD sponsored two evaluation and assessment studies to improve effectiveness measures of the counseling (DOD, 2012b). In one study, conducted in collaboration with Virginia Polytechnic University in 2010, researchers collected data from an assessment tool completed by counseling participants to measure the impact of counseling through the MFLC program. The study found that 98% of respondents reported the counseling sessions helped them deal more effectively with their problems and that they would use the service again. Virtually all (99%) reported that they received the kind of counseling service they wanted and that they would recommend MFLC services to a friend (DOD, 2012b). In the second study, DOD included questions on the use of nonmedical counseling in the May 2010 “Military Family Life Survey” for military spouses and a paired subset of active-duty personnel. Spouses reported that MilitaryOne Source counseling is the second most utilized source of counseling. Over half found it to be “very useful” (Defense Manpower Data Center, 2011). (The most utilized source is medical counseling sponsored under TRICARE.)
Despite the positive reviews from individuals using available counseling, the 2010 Military Family Life Survey found that many military spouses had concerns that deterred them from seeking counseling. Concerns included the following: “it would be difficult to get time off work or child care for counseling” (47%), “it would harm my spouse’s career” (45%), “don’t know where to get help” (40%), and “it is difficult to get help” (43%). In all, 78% of spouses surveyed reported that they had at least some concern discouraging them from seeking counseling. More than half of spouses reported they were more stressed than usual at the time of the survey, and 17% reported that they had talked to a counselor in the previous 6 months (Defense Manpower Data Center, 2011).
Couples Education
The “Prevention and Relationship Enhancement Program (PREP) for Strong Bonds” is a scientifically based education-program manual for couples designed to address the stress on military couples posed by long separations, frequent relocations, and deployment. Its goal is to strengthen the family and prevent divorce by teaching couples skills, principles, and strategies associated with healthy relationships. The program, which is led by trained Army chaplains, includes a 1-day weekday training on post, followed by a weekend retreat at a hotel off post. Program modules address such topics as communication and effective management skills, deployment and reintegration issues, fun and friendship, and relationship dynamics. A randomized controlled trial found that the divorce rate for Army couples assigned to participate in PREP for Strong Bonds was one-third of that for control couples (2.03% for Army couples vs 6.2% for the control group) when assessed 1 year after the intervention. The study authors concluded that couples education—at least in the short run—can reduce the risk of divorce (Stanley et al., 2010).
TRICARE is the health care plan that serves approximately 9.7 million beneficiaries, including active-duty personnel, their families, eligible reserve-component populations, and retirees (DOD, 2012b). User satisfaction is captured through two questions on the Health Care Survey of Department of Defense Beneficiaries (HCSDB). The questions are based on the Consumer Assessment of Healthcare Providers and Systems (CAHPS), a widely used tool to measure client satisfaction with health care. In 2011, 62% of eligible beneficiaries (active-duty, families, and retirees) rated their care an 8, 9, or 10 of 10 (10 being the best). When stratified by group, retirees and their families were most satisfied (72%), followed by active-duty families (62%), and then active-duty personnel (50%) (DOD, 2012b). Respondents reported similar levels of satisfaction for their military health care plan (as opposed to actual care). Overall, 65% of eligible beneficiaries were satisfied with their plan. Retirees and their families were most satisfied (72%); 69% of active-duty families were satisfied, and 56% of active-duty personnel were satisfied. However, no information was provided about HCSDB’s response rates or the survey population (DOD, 2012b).
In September 2009, DOD adopted the Patient-Centered Medical Home (PCMH) model for implementation throughout its health care system. The model is designed to lower hospital visits and admissions and lower the cost of care by fostering a stronger relationship between a patient and primary care provider. Early data from the PCMH within the military health system indicated improved access to care, higher-quality health outcomes, better patient satisfaction, and reduced health costs per patient (DOD, 2011a).
DOD recognizes the shortage of mental-health providers that accept TRICARE and that the shortfall must be addressed in the next 5 years to meet the demand (DOD, 2010b). DOD is working through TRICARE but also with the US Department of Health and Human Services to help increase community capacity for mental-health care for military families. DOD does not offer specifics regarding these activities in the “family readiness” reports to Congress.
DOD also established the Office of Wounded Warrior Care and Transition Policy to help streamline care coordination for wounded service members and their families as they receive care (DOD, 2010b).
Family Advocacy
Every military installation has a Family Advocacy Program (FAP) in place to provide an array of services dealing with sexual, physical, or emotional abuse of a family member (DOD, 2010b). One prominent service, the New Parent Support Program (NPSP), is a voluntary home visitation program targeting active-duty parents with children under age 3 identified as being at risk for family violence. Families can self-refer or be referred by a health provider. From 2005, when the program assessment began, to 2011, at least 85% of families who received intensive NPSP services for at least 6 months were not reported for child abuse or neglect within 1 year of completing the program (DOD, 2011a, 2012b). No control group data were presented.
In regard to spousal abuse in FY 2009, 90% of service members who completed FAP treatment were not reported for spousal abuse (physical, sexual, or emotional) within 1 year of program completion (DOD, 2010b). In FY 2010, the figure rose to 96% of service members who completed a FAP treatment program and were not reported for spousal abuse within 1 year (DOD, 2011a). In FY 2011, the figure rose to 97% of participating service members (DOD,
2012b). Again, no control group data were presented, but DOD cited evidence indicating that abusers who complete a treatment program are less likely to repeat abuse compared with those who drop out of the program (DOD, 2012b). DOD noted, however, that spousal abusers are a heterogeneous group (for example, men or women who are emotional or physical abusers) and that treatment for each type of abuser differs greatly. The outcome data do not stratify by treatment type, so some treatments may be more effective than others (DOD, 2010b). The FAP is working toward capturing treatment-specific outcome data, but DOD did not report on the specifics of those efforts (DOD, 2010b).
Family Caregivers
As described above in the section about family caregivers, the Comprehensive Assistance for Family Caregivers program provides support for severely injured post-9/11 veterans and their family caregivers (VA, 2011). Although the program is designed to provide some economic relief to family caregivers of injured veterans, the committee is unaware of any plans to evaluate program outcomes or participant satisfaction.
Bereavement
There are a variety of interventions to help families cope with their grief, ranging from counseling by military chaplains to trauma-focused CBT. Trauma-focused CBT is an evidencebased treatment for children and parents that often includes a mixture of psychoeducation to help patients understand and cope with their loss, relaxation skills, cognitive coping, trauma narration, and emotional processing (Cohen and Mannarino, 2011). Despite many DOD-sponsored programs serving bereaved military families, such as the Army’s Survivors Outreach Services, a DOD (2010a) Task Force on the Prevention of Suicide by Members of the Armed Forces found that no programs expressly meet the needs of family members whose loved one died by suicide.
Program Evaluation
The committee was unable to find evidence of evaluation efforts of DOD programs beyond what is presented above. The evidence base for understanding the needs of military families is thus lacking, as is the evidence base for measuring the performance of military family readiness programs (Miller et al., 2011b). The committee is aware of an evaluation tool developed by Miller and her colleagues at the RAND Corporation and sponsored by the Under Secretary of Defense for Personnel and Readiness (Miller et al., 2011b). Rather than develop program-specific evaluation instruments, they developed an adaptable survey instrument to measure (1) the problems and needs of service members and their families; (2) the actions families take to address their needs; (3) their satisfaction with the resources they use to meet their needs; (4) why certain resources were used and others were not (either military, civilian, formal, or informal resources); and (5) the effectiveness of the resources on retention and readiness. The authors noted that, by measuring these issues rather than focusing on the individual programs, service providers and military leadership at all levels can better understand the needs of their service members, identify unmet needs among specific demographic groups and locations, and adjust service provision as needed to more effectively meet their needs (Miller et al., 2011b). The committee is unaware if the DOD has used or plans to use the survey instrument in any capacity.
The RAND Corporation compiled a list of about 200 DOD programs that address psychologic health and traumatic brain injury, of which 120 serve families. RAND likewise
concluded that there is no centralized mechanism to catalog these programs and track which are effective, whether they meet the needs of families, whether there are any gaps, and whether programs need more resources (Weinick et al., 2011). It is possible that greater attention will be paid to evaluate family needs and program effectiveness in response to an initiative by President Obama on “Strengthening Our Military Families: Meeting America’s Commitment,” which strives to improve the quality of life among service members and their families. Although the initiative seeks to have a monitoring and evaluation component (Interagency Policy Committee et al., 2011), the committee could not find any descriptions of performance measures or any information regarding evaluation schedules for the initiative’s outlined activities.
What little program information is available is largely contained in DOD’s annual reports to Congress on “Plans for the Department of Defense for Support of Military Family Readiness” (DOD, 2011a, 2012b). However, what is reported there focuses primarily on program capacity, frequency of delivery, and utilization rather than on program performance and effectiveness in meeting the needs of families. It is important to emphasize, however, that the majority of programs compiled by RAND are not mentioned in the reports to Congress.
Summary
Assuring the health and welfare of military families is both an obligation for DOD and a necessity for retaining and supporting service members. DOD thus has in place hundreds of programs to support military families that address a wide range of needs—from child care and financial readiness to counseling and health care services. Despite the growth in programs that serve families, the committee found that DOD does not maintain a complete list of programs, describe their scope, or assess whether they have been evaluated, and if evaluated, by what metrics. As a consequence, a comprehensive catalog of programs for which there is empirical evidence of effectiveness cannot be compiled.
TREATMENT AND MEDICAL COUNSELING FOR FAMILIES
In 2006, family participation in treatment and other mental-health services was declared to be a national priority for veterans (VA, 2006) and active-duty military members (Interagency Policy Committee et al., 2011). Their mental-health problems not only deserve treatment in their own right, but family-based care also carries the advantage of ameliorating psychiatric illness in the service member (Makin-Byrd et al., 2011). Further, service members wisely prefer and express the desire for family participation in treatment (Batten et al., 2009; Khaylis et al., 2011). This preference is no surprise for personal reasons, but for complex mental-health problems, family participation leads to better outcomes. Mental-health-service needs for military family members span a broad continuum—from education about mental illness to inpatient and resident treatment services. There is also a need for a range of additional services, including behavioral management services, psychopharmacologic management, and family and individual psychotherapy. Many evidence-based treatments for individuals and families have been developed in civilian communities, and mental-health providers often adapt these services to the special needs of a military or veteran population, whether informally or formally. These treatments often take the form of “new programs” that might or might not be as effective for military families as they are for civilians.
Many of the family programs are psychoeducational, a generic term for evidence-based interventions aimed at teaching problem solving and other crucial skills families need to deal with serious mental illness. More than 30 randomized trials in the civilian literature attest to its capacity to enhance psychosocial and family outcomes, in addition to reducing relapse and improving symptoms in the ill family member (Murray-Swank and Dixon, 2004).
Family Education
Understanding the symptoms, diagnosis, causes, and treatments for a particular condition can help to improve family selection of and adherence to treatment programs. There are a number of models of family educational programs, most of which are intended to assist families of individuals who have a serious psychiatric illness, such as severe depression, schizophrenia, or PTSD.
The Support and Family Education (SAFE) program was developed at the Oklahoma City Veterans Affairs Medical Center (Sherman, 2006). It works with groups of families to provide them with information about the symptoms, causes, and treatment of mental illness, and about various resources available to them. They also receive information to help them better understand what their family member with mental illness is experiencing, and skills that they can use to work more effectively with their family member, such as how to set boundaries or manage violent behavior. The SAFE program also helps families to cope with their own stresses related to the illness, while teaching them how to relate more effectively to other family members, friends, community resources, and professionals. SAFE consists of a series of 18 90-minute confidential workshops that include didactic presentations and group discussions. Workshops are scheduled to take place once or twice a month and are facilitated by two mental-health professionals, such as a psychologist and a social worker or psychiatric nurse; a psychiatrist also attends at the end of the workshop to address questions about medications. A 5-year evaluation that gathered information from participants in the SAFE program found that attending more sessions was associated with lower levels of caregiver distress, having a better understanding of mental illness, being more aware of VA resources, and being better able to engage in self-care activities. The evaluation also reported high levels of participant satisfaction and retention (Sherman, 2006).
The Family-to-Family Education Program (FFEP) is similar to SAFE but uses trained family members rather than mental-health professionals as group leaders. FFEP, which was developed by the National Alliance on Mental Illness (NAMI), consists of 12 weekly group sessions designed to help families address the challenges they face in dealing with an ill family member. Sessions teach problem solving, listening, and communication skills to enhance relationships with the family member as well as service providers. FFEP also focuses on addressing issues related to the mental-health service systems and on dealing with problems related to social or financial support. The goal of FFEP is to teach family members to become better advocates for the care of their ill family member. The VA offers FFEP in at least one Veterans Health Administration (VHA) facility in each state; the program is also provided by NAMI chapters around the country (Makin-Byrd et al., 2011).
After Deployment: Adaptive Parenting Tools (ADAPT) is a relatively new program for returning military parents that focuses on helping children with behavioral and adjustment problems, using role-playing exercises and audiovisual materials to teach parenting skills. It is
based on the well-validated program known as the Parent Management Training Oregon-Model (PMTO); however, materials and curriculum were modified to make them more applicable to military and veteran families. The program focuses on providing parents with specific skills in five distinct areas: (1) contingency management, (2) limit setting, (3) positive involvement, (4) monitoring children’s activities, and (5) effective family problem solving. ADAPT is currently undergoing evaluation (Gewirtz et al., 2011).
The VA has trained a number of VHA clinicians in both behavioral family therapy (BFT) and multifamily group therapy (Makin-Byrd et al., 2011). BFT is a form of behavior therapy in which a clinician meets with one patient and his or her family members to change specific maladaptive behavior patterns. This process is done by enhancing awareness and then teaching specific skills to enhance communication and problem solving. In the VHA, BFT is tailored to veterans with PTSD and their families. After initial orientation and assessment sessions, the program offers two sessions on education, three on communication training, two on anger management, and the remaining six to eight sessions on problem solving that is specific to the veteran and his or her family (Glynn et al., 1995).
In contrast to BFT, multifamily group therapy (MFGT) operates in a large group setting with several families who typically meet biweekly in 90-minute sessions that can continue for 12 months or longer. A therapist uses a structured problem-solving format to discuss relapse prevention, provide support for social and vocational rehabilitation, build relationship skills, and foster interdependence among the families. Targeted areas for intervention include increasing family coping skills and providing education about the course of illness and its treatment. The sessions also provide an opportunity to meet other families with similar struggles, thus helping families to feel less isolated (Sherman et al., 2012). Families are typically invited to participate in the MFGT sessions after participating in two to three individual family sessions and an educational session about the family member’s illness. In the civilian literature, MFGT has been demonstrated to increase family-member quality of life and lessen family-member burden (McFarlane et al., 1995).
A version of MFGT adapted for veterans with PTSD includes additional education in an extended family workshop and more attention to relationship building, which focuses on the common problems that veterans with PTSD have with trust, intimacy, and communication. The problem-solving component of this form of MFGT also focuses on the specific PTSD symptoms of avoidance and emotional numbing (Sherman et al., 2012). MFGT has been adapted for veterans with TBI (Perlick et al., 2011) by adding information about the military experience and the pathophysiology and treatment of TBI and comorbid conditions, such as depression and PTSD. The workshop is divided over 2 days to minimize overload for veterans with TBI who have memory impairment. The group therapy phase is modified in three ways: (1) it addresses reduced or impaired communication, parenting conflicts, and partner frustration associated with cognitive deficits of TBI; (2) it includes problem solving related to forgetfulness; and (3) it focuses on loss of identity and difficulty accepting cognitive limitations. No information is available regarding efficacy for OIF and OEF veterans, but a pilot study has shown that TBIadapted MFGT is helpful for civilians and families with spinal-cord injury and TBI. Reduced family burden was also reported in a pilot study of civilians (Rodgers et al., 2007).
Couples therapy can be useful for various problems, such as communication, maritalstability, sexuality, and joint-parenting issues. Couples therapy does not preclude the use of other forms of therapy, including group and individual therapies.
Behavioral couples therapy (BCT) has been adapted for a variety of purposes, including work with veterans who have PTSD and their partners. BCT encourages acceptance, tolerance, and expression of emotions, such as fear and sadness, both of which characterize PTSD. Adaptations for PTSD include a shorter length of treatment, incorporation of motivational interviewing, trauma education, and emphasis on scheduling activities during treatment that increase couples’ shared experiences (Erbes et al., 2008). The VHA is also training its clinicians to add parenting and domestic violence to their content (Makin-Byrd et al., 2011). No evaluation of PTSD-adapted BCT has been reported.
Cognitive behavioral conjoint therapy (CBCT) is another form of couples therapy directed at PTSD and associated disruptions in the functioning of couples. CBCT is a 15-session structured treatment that includes family psychoeducation, behavioral interventions to enhance approach behaviors and communication, and cognitive interventions aimed at the maladaptive cognitions that are associated with PTSD and that create relationship distress. Glynn et al. (1999) compared a version of CBCT along with exposure therapy in a controlled clinical trial of 42 combat-exposed Vietnam veterans and their partners. As compared with wait-list controls, veterans and partners who received both therapies experienced improved interpersonal problemsolving and reduced symptoms of PTSD, such as reexperiencing and hyperarousal. A subsequent uncontrolled clinical trial of CBCT alone in veterans found posttreatment reductions in PTSD symptoms and partner reports of improved relationship satisfaction and mental-health functioning (Monson et al., 2005). Another small uncontrolled trial yielded similar findings (Monson et al., 2011).
A related couples therapy, strategic approach therapy, is designed to ameliorate PTSD symptoms, specifically avoidance and emotional numbing. One study found reductions in selfreported, clinician-rated, and partner-rated avoidance, emotional numbing, and overall PTSD symptoms; however, there were no measures for its effect on relationship functioning (Sautter et al., 2009).
Alcohol and Substance-Abuse Treatment for Dependents
The TRICARE benefit pays for certain SUD services for military dependents, including assessment and diagnosis by SUD professionals. In addition, there are a few programs that provide SUD screening, diagnosis, or treatment for military spouses or children in the direct care system, but data on the effectiveness of these programs is scarce. “Military Pathways” includes a self-assessment/self-screening component that can serve as a secondary prevention mechanism for military members or spouses who self-identify as being at personal risk for SUD and subsequently seek help. This intervention reaches more than 305,000 active-duty service members and their families each year and appears to follow evidence-based principles (IOM, 2012). The Adolescent Substance Abuse Counseling Program is focused on children of military families in grades 6–12 who are considered at risk for substance use and who are authorized to use military treatment facilities. Services include treatment, identification and referral, and prevention education in community settings. The effectiveness of the program is unknown as no
formal outcome evaluations have been conducted with the target population (IOM, 2012). Military OneSource provides a confidential means for service members and their families to be screened for SUDs and referred to resources; however, the program is not designed to provide actual treatment for SUD or other mental health issues (IOM, 2012).
Prevention Intervention for Families
Although effective treatments are essential for military families with mental-health, behavioral, and marital problems, preventing the initiation of such problems is ideal. Many prevention programs for military populations are adaptations of preventive interventions designed for civilian populations. There is a need for preventive intervention strategies addressing the needs of military families facing deployment. Of special note is the Families Over Coming Under Stress (FOCUS) intervention, which shows great promise for prevention. This treatment is a relatively new family-centered resiliency training program developed for military families by the University of California, Los Angeles (UCLA), and Harvard researchers. FOCUS has been delivered since 2008 to thousands of military families who experienced stress associated with multiple deployments. Designed to enhance resiliency (defined as “engagement in adaptive behaviors and achieving developmental milestones in the face of stressful or traumatic life events”), FOCUS involves eight structured family-training sessions that are targeted at increasing resiliency skills in the domains of communication, emotional regulation, managing trauma or loss, problem solving, and goal setting (Lester et al., 2011). A program evaluation that examined 331 families with a mean of 4.5 service-member deployments found improved family function and adaptation for those who participated in FOCUS. Parents reported that they had fewer symptoms of anxiety and depression, as well as healthier family functioning; lower than expected behavioral and emotional problems were also reported for children (Lester et al., 2012).
Summary
In summary, although there are many family-based interventions for individuals who have or are at risk for psychiatric disorders, few are adapted or readily available for use with military and veteran families. When they are available, trained clinicians who can provide the interventions are not always accessible. There is clearly a need for new evidence-based programs, including prevention interventions, that are specifically designed to meet the needs of military families. Evaluation of these programs must be multifaceted and multimodal so that not only individual psychopathology and marital relationships are studied but also overall family function, parent–child interactions, and child functioning are studied.
CONCLUSIONS
Military service members are also members of families, and their families can provide essential support to them as well as—at times—be a source of stress and concern. Families have a crucial, although sometimes unrecognized, role to play in military readiness, helping to ensure the well-being and functioning of service members so that they can be effective in their jobs. Family members are an essential asset to the military; they help to prepare service members for their deployments, provide emotional support and motivation, assist with readjustment and
reintegration after deployment, and provide hands-on informal care and management for service members who return from war with physical or psychologic injuries. When families are doing poorly, service members also function worse. Quite simply, it is in the best interests of the military to work to ensure that families are also doing well, including before, during, and after deployments. The demographics of the military have changed, however, and it is important that the military consider the full spectrum of family configurations instead of limiting its focus to married heterosexual couples and their children; excluding the nontraditional families misses key opportunities to enhance military readiness. Although a wide array of services are available to families, few have been evaluated for effectiveness, and most are focused solely on married couples and their children—a family configuration that no longer captures the full diversity of military families.
FUTURE RESEARCH DIRECTIONS
The committee identified a number of areas for future research and direction based on its reviews of the literature and the federally funded research on military families with service members who had deployed with OEF or OIF (see Appendix D). Although the committee found that research attention to military families (including the impact of deployments) is growing, many of the findings are limited by poor sampling strategies (for example, the use of nonrandom convenience samples) and small sample sizes. Certain populations, including women, reserve, and National Guard families, are also understudied. Few studies have examined military families over time, and none of those reviewed by the committee used inclusive definitions of family beyond traditional marriage. The committee recommends that research be supported to increase understanding of the following:
• Research is needed to better understand the nature of deployment. Although several emotional stages of adjustment to deployment have been proposed and are widely used, they have not been empirically validated longitudinally. Furthermore, the interaction between chronic military challenges and deployment-related stressors is not well understood and should be studied. More knowledge is needed about the impact of different characteristics of deployment, such as timing, duration, and frequency. Research should also be done on the impact of multiple short (for example, under 30 days) deployments on families; these deployments are usually not included in research, and better understanding is needed particularly of the impact of multiple parental departures on children.
• Although healthy and stable marital and other romantic partner relationships provide important supports for service members, there are many knowledge gaps regarding how these relationships influence military readiness and how they are affected by deployments. There is evidence, for example, that deployment erodes marital quality, but the factors that moderate these processes are not well understood; therefore, knowledge is insufficient about the best way to prevent such erosion in association with military service. Although patterns of marital formation and dissolution in the military have been studied repeatedly, little information is available about the accumulation of marital transitions among military members and the implications of such accumulation for family needs. Young military members marry at much higher rates than civilians of similar age, and such marriages have been demonstrated to be susceptible to divorce; military policies might unintentionally promote such marriages. Studies should be undertaken to determine how best to minimize both the threats to marital
stability posed by military service and the likelihood of premature marriage. Finally, in the context of relationships, deployment-related wounds and injuries and PTSD, particularly with regard to the impact on prognoses and recovery, is not well understood. Social isolation is, however, a risk factor for poor outcomes. Therefore, greater understanding of relationship dynamics is needed in regard to wounds and injuries in both nuclear and extended families.
• Research is needed to improve understanding of which children in military families are at highest risk, whether their mental-health needs are different from those of nonmilitary children, and of effective treatments that work within the context of military life.
• Despite now representing a significant minority of the armed forces, female military members are understudied. Studies should be conducted that focus on the specific characteristics, needs, and experiences of female service members and their families (including single female heads of households, members of dual-military couples, and military women with civilian partners). There is a need for better understanding of dual-military families, particularly as they relate to the needs of female service members and their ability to pursue their military careers.
In addition, the committee calls for the following to improve the quality of research and to increase the availability of research findings on military service members and their families:
• Although there are important longitudinal studies under way that examine the impact of deployments on service members and their families, they do not fully represent the diversity of military families. DOD should conduct longitudinal studies that include the full range of family configurations and support systems (for example, grandparents and unmarried partners). Studies are especially needed to quantify the value and impact of families on military readiness, including helping to prepare service members for deployment, supporting them during deployment, and providing physical and psychologic care for them upon their return.
• DOD collects large amounts of data about military members and families. However, most of these data remain unanalyzed. Large military data sets should be anonymized and made publicly available to researchers. Such availability will greatly increase the capacity of DOD to reap benefits from the vast amount of data it already collects. Access to unpublished DOD data is needed to identify current trends in child maltreatment; the last data were published in 2007.
• Many large, nationally representative population studies deliberately exclude individuals living in institutions, including military installations (for example, the National Longitudinal Survey of Youth). Service members and their families should be included in these large national surveys wherever feasible, both to expand knowledge about them and to allow comparisons of comparable population groups within studies.
RECOMMENDATIONS
The committee found that DOD has many programs and policies to support families. However, DOD policies, programs, and practices typically do not take into consideration the full spectrum of military families. By focusing almost exclusively on traditional families (married heterosexual spouses and their children), DOD is missing critical opportunities to support the readjustment needs of many service members’ nontraditional families. To be able to support all families, DOD will need data on the full constellation of service members’ families.
The committee recommends that the Department of Defense ensure that policies, programs, and practices aim to support and strengthen all military families, including nontraditional ones.
Healthy families help service members to do their jobs effectively and readjust after deployment. The demands placed on military family members call for support in the areas of relationship building, family and individual function, and reduction of risk of psychologic and physical-health problems. The committee found that little information is available on the potential effectiveness of broad-based, universal prevention efforts aimed at military children and their families. In addition, most treatment interventions for family members have been developed and tested in civilian communities and lack evidence of their effectiveness for military families. The committee concludes that military families would benefit from increased efforts to identify, develop, and test new prevention and treatment interventions targeted toward military families, including interventions directed at children and adolescents.
The committee recommends that the Department of Defense use evidence-based primary prevention programs and treatments that have been specifically evaluated in service members and their families and that are focused on preventing and treating mental-health and relationship problems.
The committee concludes that there are substantial gaps in knowledge about the effects of deployment on military families that hinder DOD’s ability to meet the needs of military service members and their families effectively. The committee found that—although some important large-scale, well-designed studies are under way—much of the research heretofore has been methodologically flawed, suffering, for example, from the use of small convenience samples, use of cross-sectional designs, and the like. The committee concludes that well-designed studies that use rigorous and diverse methods (both qualitative and quantitative) are needed to increase understanding of the challenges faced by military service members and their families.
The committee recommends that the Department of Defense and other relevant federal agencies fund methodologically rigorous research on the social, psychologic, and economic effects of deployments on families, including nontraditional families.
Studies of families of service members deployed to OEF and OIF have documented a rise in domestic violence (typically including abuse of spouses or neglect of children). In the FY 2000 National Defense Authorization Act (PL 106-65, Section 591), Congress directed the secretary of defense to establish a Defense Task Force on Domestic Violence to make recommendations for reducing the prevalence of domestic violence in military families. The task force submitted a report in 2003 that identified multiple shortcomings in the current systems and recommended many improvements. The Government Accountability Office, in 2006 and 2010, issued reports concerning progress in implementing the nearly 200 recommendations made by the task force. Both reports described progress on some recommendations but little on others, including a recommendation for reliable documentation of violent events.
The committee recommends that the Department of Defense place high priority on reducing domestic violence because it degrades force readiness and the well-being of military family members.
REFERENCES
Adams, G. A., S. M. Jex, and C. J. L. Cunningham. 2006. Work-family conflict among military personnel. In Military Life: The Psychology of Serving in Peace and Combat, Vol. 3. Edited by C. A. Castro, A. B. Adler and T. W. Britt. Westport, CT: Praeger. Pp. 169-192.
Adler-Baeder, F., J. F. Pittman, and L. Taylor. 2006. The prevalence of marital transitions in military families. Journal of Divorce and Remarriage 44(1-2):91-106.
AdvancED. 2012. Advanced Company Overview. http://www.advanc-ed.org/company-overview (accessed July 9, 2012).
Allen, E. S., G. K. Rhoades, S. M. Stanley, and H. J. Markman. 2010. Hitting home: Relationships between recent deployment, posttraumatic stress symptoms, and marital functioning for Army couples. Journal of Family Psychology 24(3):280-288.
Allen, E. S., S. M. Stanley, G. K. Rhoades, H. J. Markman, and B. A. Loew. 2011. Marriage education in the Army: Results of a randomized clinical trial. Journal of Couple and Relationship Therapy 10(4):309-326.
Alvarez, L. 2007. Long Iraq tours can make home a trying front. New York Times, February 23.
Angrist, J. D., and J. H. Johnson. 2000. Effects of work-related absences on families: Evidence from the Gulf War. Industrial and Labor Relations Review 54(1):41-58.
Annie E. Casey Foundation. 2012. Kids Count Data Book: State Trends in Child Well-Being. Baltimore, MD: Annie E. Casey Foundation.
Babcock, J. C., C. E. Green, and C. Robie. 2004. Does batterers' treatment work? A meta-analytic review of domestic violence treatment. Clinical Psychology Review 23(8):1023-1053.
Baptist, J. A., Y. Amanor-Boadu, K. Garrett, B. S. Goff, J. Collum, P. Gamble, H. Gurss, E. Sanders-Hahs, L. Strader, and S. Wick. 2011. Military marriages: The aftermath of Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF) deployments. Contemporary Family Therapy: An International Journal 33(3):199-214.
Bassani, D. G., C. V. Padoin, D. Philipp, and S. Veldhuizen. 2009. Estimating the number of children exposed to parental psychiatric disorders through a national health survey. Child and Adolescent Psychiatry and Mental Health 3(1):6.
Batten, S. V., A. L. Drapalski, M. L. Decker, J. C. DeViva, L. J. Morris, M. A. Mann, and L. B. Dixon. 2009. Veteran interest in family involvement in PTSD treatment. Psychological Services 6(3):184-189.
Bethea, M. C. 2007. Long War and the Forgotten Families: Dual-Military Couples. Carlisle Barracks, PA: US Army War College.
Blais, M. C., and J. M. Boisvert. 2005. Psychological and marital adjustment in couples following a traumatic brain injury (TBI): A critical review. Brain Injury 19(14):1223-1235.
Booth, B., M. W. Segal, and D. B. Bell. 2007. What We Know About Army Families: 2007 Update. Arlington, VA: Department of the Army, Family and Morale, Welfare and Recreation Command.
Bowen, G. L., and J. A. Martin. 2011. The resiliency model of role performance for service members, veterans, and their families: A focus on social connections and individual assets. Journal of Human Behavior in the Social Environment 21(2):162-178.
Bowling, U. B., and M. D. Sherman. 2008. Welcoming them home: Supporting service members and their families in navigating the tasks of reintegration. Professional Psychology: Research and Practice 39(4):451-458.
Bray, R. M., L. L. Hourani, K. L. Rae Olmsted, M. Witt, J. M. Brown, M. R. Pemberton, M. E. Marsden, B. Marriott, S. Scheffler, R. Vandermaas-Peeler, B. Weimer, S. Calvin, M. Bradshaw, K. Close, and D. Hayden. 2006. 2005 Department of Defense Survey of Health Related Behaviors Among Military Personnel. Research Triangle Park, NC: RTI international.
Bray, R. M., M. R. Pemberton, M. E. Lane, L. L. Hourani, M. J. Mattiko, and L. A. Babeu. 2010. Substance use and mental health trends among US military active duty personnel: Key findings from the 2008 DOD health behavior survey. Military Medicine 175(6):390-399.
Buchanan, C., J. Kemppainen, S. Smith, S. MacKain, and C. W. Cox. 2011. Awareness of posttraumatic stress disorder in veterans: A female spouse/intimate partner perspective. Military Medicine 176(7):743-751.
Buckman, J. E. J., J. Sundin, T. Greene, N. T. Fear, C. Dandeker, N. Greenberg, and S. Wessely. 2011. The impact of deployment length on the health and well-being of military personnel: A systematic review of the literature. Occupational and Environmental Medicine 68(1):69-76.
Burrell, L. M., G. A. Adams, D. B. Durand, and C. A. Castro. 2006. The impact of military lifestyle demands on well-being, army, and family outcomes. Armed Forces and Society 33(1):43-58.
Carter, S., B. Loew, E. Allen, S. Stanley, G. Rhoades, and H. Markman. 2011. Relationships between soldiers’ PTSD symptoms and spousal communication during deployment. Journal of Traumatic Stress 24(3):352-355.
Castro, C. A., A. B. Adler, and T. W. Britt. 2006. Future directions. In Military Life: The Psychology of Serving in Peace and Combat. Edited by C. A. Castro, A. B. Adler and T. W. Britt. Westport, CT: Praeger. Pp. 245-248.
Center for Behavioral Health Statistics and Quality. 2012. National Survey on Drug Use and Health (NSDUH) Data Spotlight: More Than 7 Million Children Live with a Parent with Alcohol Problems. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Chandra, A., S. Lara-Cinisomo, L. H. Jaycox, T. Tanielian, R. M. Burns, T. Ruder, and B. Han. 2010a.
Children on the homefront: The experience of children from military families. Pediatrics 125(1):16-25.
Chandra, A., L. T. Martin, S. A. Hawkins, and A. Richardson. 2010b. The impact of parental deployment on child social and emotional functioning: Perspectives of school staff. Journal of Adolescent Health 46(3):218-223.
Chandra, A., S. Lara-Cinisomo, L. H. Jaycox, T. Tanielian, B. Han, R. M. Burns, and T. Ruder. 2011. Views from the Homefront: The Experiences of Youth and Spouses from Military Families. Santa Monica, CA: RAND Corporation.
Chartrand, M. M., D. A. Frank, L. F. White, and T. R. Shope. 2008. Effect of parents’ wartime deployment on the behavior of young children in military families. Archives of Pediatrics and Adolescent Medicine 162(11):1009-1014.
Christensen, E., P. Netzer, E. Schaefer, C. Hill, D. Farr, and J. McMahon. 2009. Economic Impact on Caregivers of the Seriously Wounded, Ill, and Injured. Alexandria, VA: Center for Naval Analyses.
Cohen, J. A., and A. P. Mannarino. 2011. Trauma-focused CBT for traumatic grief in military children. Journal of Contemporary Psychotherapy 41(4):219-227.
Copen, C. E., K. Daniels, J. Vespa, and W. D. Mosher. 2012. First marriages in the United States: Data from the 2006–2010 National Survey of Family Growth. National Health Statistics Reports 49:1-21.
Cozza, S. J. 2007. Proceedings: Workgroup on intervention with combat injured families. Paper read at Workgroup on Intervention with Combat Injured Families, December 11–12, 2007, Bethesda, MD.
Cozza, S. J., R. S. Chun, and J. A. Polo. 2005. Military families and children during Operation Iraqi Freedom. Psychiatric Quarterly 76(4):371-378.
Cozza, S. J., J. M. Guimond, J. B. A. McKibben, R. S. Chun, T. L. Arata-Maiers, B. Schneider, A.
Maiers, C. S. Fullerton, and R. J. Ursano. 2010. Combat-injured service members and their families: The relationship of child distress and spouse-perceived family distress and disruption. Journal of Traumatic Stress 23(1):112-115. Crary, D. 2005. As deployments increase, so does Army’s divorce rate. USA Today. http://usatoday30.usatoday.com/news/nation/2005-06-29-army-divorces_x.htm (accessed April 20, 2011).
Crum-Cianflone, N. F., J. Fairbank, C. Marmar, W. Schlenger, and H. McMaster. 2012. Millennium Cohort Family Study. Paper presented at Annual Review Meeting, Military Operational Medicine Research Program, Fort Detrich, MD.
de Burgh, H. T., C. J. White, N. T. Fear, and A. C. Iversen. 2011. The impact of deployment to Iraq or Afghanistan on partners and wives of military personnel. Internal Review of Psychiatry 23(2):192-200.
Defense Manpower Data Center. 2011. 2010 Military Family Life Project. Arlington, VA: Department of Defense.
Department of the Army. 2012. Army 2020: Generating Health and Discipline in the Force. Washington, DC: Department of Defense.
Dimiceli, E. E., M. A. Steinhardt, and S. E. Smith. 2010. Stressful experiences, coping strategies, and predictors of health-related outcomes among wives of deployed military servicemen. Armed Forces and Society 36(2):351-373.
DOD (Department of Defense). 1998. Selected Manpower Statistics, MO1 (Directorate for Information, Operations, and Reports). Washington, DC: US Government Printing Office.
———. 2010a. The Challenge and the Promise: Strengthening the Force, Preventing Suicide and Saving Lives. Washington, DC: Department of Defense.
———. 2010b. Plans for the Department of Defense for the Support of Military Family Readiness: Report to the Congressional Defense Committees Pursuant to Section 1782b of Title 10, United States Code. Washington, DC: Department of Defense.
———. 2011a. Annual Report to Congress on Plans for the Department of Defense for the Support of Military Family Readiness. Washington, DC: Department of Defense.
———. 2011b. Demographics 2010: Profile of the Military Community. Washington, DC: Department of Defense.
———. 2012a. 2011 Demographics Profile of the Military Community. Washington, DC: Department of Defense.
———. 2012b. Annual Report to Congress on Plans for the Department of Defense for the Support of Military Family Readiness. Washington, DC: Department of Defense.
———. 2012c. Department of Defense Family Advocacy Program Child Abuse/Neglect (CAN) Data FY11 Report. Washington, DC: Department of Defense.
———. 2012d. TRICARE. http://www.tricare.mil/mybenefit/ProfileFilter.do;jsessionid=PQ2hM96Jx9ybGG8xnbhCwqnvK331Lxql3d5vQgcLjC1pNv21J2ND!349025571?puri=%2Fhome (accessed March 2, 2012).
DOD Education Activity. 2012. Interstate Compact on Educational Opportunity for Military Children. http://www.dodea.edu/teachers/interstate.cfm (accessed June 28, 2012).
Eaton, K. M., C. W. Hoge, S. C. Messer, A. A. Whitt, O. A. Cabrera, D. McGurk, A. Cox, and C. A. Castro. 2008. Prevalence of mental health problems, treatment need, and barriers to care among primary care-seeking spouses of military service members involved in Iraq and Afghanistan deployments. Military Medicine 173(11):1051-1056.
Eby, L. T., J. S. DeMatteo, and J. E. A. Russell. 1997. Employment assistance needs of accompanying spouses following relocation. Journal of Vocational Behavior 50(2):291-307.
Eide, M., G. Gorman, and E. Hisle-Gorman. 2010. Effects of parental military deployment on pediatric outpatient and well-child visit rates. Pediatrics 126(1):22-27.
Elizur, E., and M. Kaffman. 1983. Factors influencing the severity of childhood bereavement reactions. American Journal of Orthopsychiatry 53(4):668-676.
Engel, R. C., L. B. Gallagher, and D. S. Lyle. 2010. Military deployments and children’s academic achievement: Evidence from Department of Defense Education Activity schools. Economics of Education Review 29(1):73-82.
Erbes, C. R. 2011. Couple functioning and PTSD in returning OIF soldiers: Preliminary findings from the readiness and resilience in National Guard soldiers project. In Risk and Resilience in US Military Families, edited by S. MacDermid Wadsworth and D. Riggs. New York: Springer. Pp. 47-67.
Erbes, C. R., M. A. Polusny, S. Macdermid, and J. S. Compton. 2008. Couple therapy with combat veterans and their partners. Journal of Clinical Psychology 64(8):972-983.
Erbes, C. R., L. A. Meis, M. A. Polusny, and J. S. Compton. 2011. Couple adjustment and posttraumatic stress disorder symptoms in National Guard veterans of the Iraq war. Journal of Family Psychology 25(4):479-487.
Etters, L., D. Goodall, and B. E. Harrison. 2008. Caregiver burden among dementia patient caregivers: A review of the literature. Journal of the American Academy of Nurse Practitioners 20(8):423-428.
Faber, A. J., E. Willerton, S. R. Clymer, S. M. MacDermid, and H. M. Weiss. 2008. Ambiguous absence, ambiguous presence: A qualitative study of military reserve families in wartime. Journal of Family Psychology 22(2):222-230.
Federal Interagency Forum on Child and Family Statistics. 2012. America's Children in Brief: Key National Indicators of Well-Being. Washington, DC: US Government Printing Office.
Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M. Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. American Journal of Preventive Medicine 14(4):245-258.
Flake, E. M., B. E. Davis, P. L. Johnson, and L. S. Middleton. 2009. The psychosocial effects of deployment on military children. Journal of Developmental and Behavioral Pediatrics 30(4):271-278.
Forgey, M. A., and L. Badger. 2010. Patterns of intimate partner violence and associated risk factors among married enlisted female soldiers. Violence and Victims 25(1):45-61.
Franklin, K. 2011. The impact of deployment and psychological well-being on family relationships: A secondary analysis of Air Force community assessment data. Dissertation Abstracts International Section A: Humanities and Social Sciences 72(4-A):1441.
GAO (US Government Accountability Office). 2001. Military Personnel: Longer Time Between Moves Related to Higher Satisfaction and Retention. Washington, DC: US Government Accountability Office.
———. 2007. Military Personnel: Medical, Family Support, and Educational Services Are Available for Exceptional Family Members. Washington, DC: US Government Accountability Office.
———. 2010. Sustained Leadership and Oversight Needed to Improve DOD's Prevention and Treatment of Domestic Abuse. Washington, DC: US Government Accountability Office.
Gewirtz, A. H., C. R. Erbes, M. A. Polusny, M. S. Forgatch, and D. S. Degarmo. 2011. Helping military families through the deployment process: Strategies to support parenting. Professional Psychology Research and Practice 42(1):56-62.
Gibbs, D. A., S. L. Martin, L. L. Kupper, and R. E. Johnson. 2007. Child maltreatment in enlisted soldiers' families during combat-related deployments. Journal of the American Medical Association 298(5):528-535.
Glynn, S. M., S. Eth, E. T. Randolph, D. W. Foy, G. B. Leong, G. G. Paz, J. D. Salk, G. Firman, and J. W. Katzman. 1995. Behavioral family therapy for Vietnam combat veterans with posttraumatic stress disorder. Journal of Psychotherapy Practice and Research 4(3):214-223.
Glynn, S. M., S. Eth, E. T. Randolph, D. W. Foy, M. Urbaitis, L. Boxer, G. G. Paz, G. B. Leong, G. Firman, J. D. Salk, J. W. Katzman, and J. Crothers. 1999. A test of behavioral family therapy to augment exposure for combat-related posttraumatic stress disorder. Journal of Consulting and Clinical Psychology 67(2):243-251.
Goff, B. S. N., J. R. Crow, A. M. J. Reisbig, and S. Hamilton. 2007. The impact of individual trauma symptoms of deployed soldiers on relationship satisfaction. Journal of Family Psychology 21(3):344-353.
Golding, J. M. 1999. Intimate partner violence as a risk factor for mental disorders: A meta-analysis. Journal of Family Violence 14(2):99-132.
Gorman, G. H., M. Eide, and E. Hisle-Gorman. 2010. Wartime military deployment and increased pediatric mental and behavioral health complaints. Pediatrics 126(6).
Gorman, L. A., A. J. Blow, B. D. Ames, and P. L. Reed. 2011. National Guard families after combat: Mental health, use of mental health services, and perceived treatment barriers. Psychiatric Services 62(1):28-34.
Gould, M., House Committee on Veterans Affairs. 2012. Veterans Affairs in the 112th Congress: Reviewing VA’s Performance and Accountability. September 20, 2012.
Griffin, J. M., G. Friedemann-Sanchez, C. Hall, S. Phelan, and M. van Ryn. 2009. Families of patients with polytrauma: Understanding the evidence and charting a new research agenda. Journal of Rehabilitation Research and Development 46(6):879-892.
Griffin, J. M., G. Friedemann-Sanchez, A. C. Jensen, B. C. Taylor, A. Gravely, B. Clothier, A. B. Simon, A. Bangerter, T. Pickett, C. Thors, S. Ceperich, J. Poole, and M. van Ryn. 2012. The invisible side of war: Families caring for US service members with traumatic brain injuries and polytrauma. Journal of Head Trauma Rehabilitation 27(1):3-13.
Haas, D. M., and L. A. Pazdernik. 2006. A cross-sectional survey of stressors for postpartum women during wartime in a military medical facility. Military Medicine 171(10):1020-1023.
———. 2007. Partner deployment and stress in pregnant women. Journal of Reproductive Medicine 52(10):901-906.
Haine, R. A., T. S. Ayers, I. N. Sandler, and S. A. Wolchik. 2008. Evidence-based practices for parentally bereaved children and their families. Professional Psychology: Research and Practice 39(2):113.
Harrell, M. C., N. Lim, L. Werber Castaneda, and D. Golinelli. 2004. Working Around the Military: Challenges to Military Spouse Employment and Education. Santa Monica, CA: RAND Corporation.
Helfrich, C. A., G. T. Fujiura, and V. Rutkowski-Kmitta. 2008. Mental health disorders and functioning of women in domestic violence shelters. Journal of Interpersonal Violence 23(4):437-453.
Heyman, R. E., and P. H. Neidig. 1999. A comparison of spousal aggression prevalence rates in US Army and civilian representative samples. Journal of Consulting and Clinical Psychology 67(2):239.
Hill, R. 1949. Families Under Stress. New York: Harper and Brothers.
Hinojosa, R., M. S. Hinojosa, and R. S. Hognas. 2012. Problems with veteran-family communication during Operation Enduring Freedom/Operation Iraqi Freedom military deployment. Military Medicine 177(2):191-197.
Hopkins-Chadwick, D. L., and N. Ryan-Wenger. 2009. Stress in junior enlisted Air Force women with and without children. Western Journal of Nursing Research 31(3):409-427.
Hosek, J., B. Asch, C. C. Fair, C. Martin, and M. Mattock. 2002. Married to the Military: The Employment and Earnings of Military Wives Compared with Those of Civilian Wives. Santa Monica, CA: RAND Corporation.
Hosek, J., J. Kavanagh, and L. Miller. 2006. How Deployments Affect Service Members. Santa Monica, CA: RAND Corporation.
Huebner, A. J., J. A. Mancini, G. L. Bowen, and D. K. Orthner. 2009. Shadowed by war: Building community capacity to support military families. Family Relations 58(2):216-228.
Huffman, A. H., and S. C. Payne. 2006. The challenges and benefits of dual-military marriages. In Military Life: The Psychology of Serving in Peace and Combat (Vol 3): The Military Family. Westport, CT: Praeger Security International. Pp. 115-137.
Hurley, E. C. 2011. Rejection sensitivity as a predictor of marital adjustment among military spouses during military deployments. Dissertation Abstracts International: Section B: The Sciences and Engineering 72(5-B):3096.
Interagency Policy Committee, Presidential Study Directive, and The White House. 2011. Strengthening Our Military Families. Washington, DC: The White House.
IOM (Institute of Medicine). 2008. Gulf War and Health: Volume 6. Physiologic, Psychologic, and Psychosocial Effects of Deployment-related Stress. Washington, DC: The National Academies Press.
———. 2010. Returning Home from Iraq and Afghanistan: Preliminary Assessment of Readjustment Needs of Veterans, Service Members, and Their Families. Washington, DC: The National Academies Press.
———. 2012. Substance Use Disorders in the US Armed Forces. Washington, DC: The National Academies Press.
Jensen, P. S., D. Martin, and H. Watanabe. 1996. Children’s response to parental separation during Operation Desert Storm. Journal of the American Academy of Child and Adolescent Psychiatry 35(4):433-441.
Johnson, A. J. 2011. Examining partner experiences of returning Operation Enduring Freedom and Iraqi Freedom Veterans. Dissertation Abstracts International: Section B: The Sciences and Engineering 71(11-B):7118.
Jowers, K. 2011. Bereavement Study to Focus on 3,000 Survivors. http://militarytimes.com/news/2011/10/military-ausa-bereavement-study-3000-survivors-101111w (accessed October 25, 2012).
Karney, B. R., and T. N. Bradbury. 1995. The longitudinal course of marital quality and stability: A review of theory, method, and research. Psychological Bulletin 118(1):3-34.
Karney, B. R., and J. S. Crown. 2007. Families Under Stress: An Assessment of Data, Theory, and Research on Marriage and Divorce in the Military. Santa Monica, CA: RAND Corporation.
———. 2011. Does deployment keep military marriages together or break them apart? Evidence from Afghanistan and Iraq. In Risk and Resilience in US Military Families. New York: Springer. Pp. 23-45.
Karney, B. R., D. S. Loughran, and M. S. Pollard. 2012. Comparing marital status and divorce status in civilian and military populations. Journal of Family Issues 33(12):1572-1594.
Kavanagh, J. 2005. Stress and Performance: A Review of the Literature and Its Applicability to the Military. Santa Monica, CA: RAND Corporation.
Kelley, M. L., E. Hock, J. F. Bonney, M. S. Jarvis, K. M. Smith, and M. A. Gaffney. 2001. Navy mothers experiencing and not experiencing deployment: Reasons for staying in or leaving the military. Military Psychology 13(1):55-71.
Kelley, M. L., E. Hock, M. S. Jarvis, K. M. Smith, M. A. Gaffney, and J. F. Bonney. 2002. Psychological adjustment of Navy mothers experiencing deployment. Military Psychology 14(3):199-216.
Khaylis, A., M. A. Polusny, C. R. Erbes, A. Gewirtz, and C. M. Rath. 2011. Posttraumatic stress, family adjustment, and treatment preferences among National Guard soldiers deployed to OEF/OIF. Military Medicine 176:126-131.
Knapp, S. J., and B. Lott. 2010. Forming the central framework for a science of marital quality: An interpretive alternative to marital satisfaction as a proxy for marital quality. Journal of Family Theory and Review 2(4):316-333.
Knobloch, L. K., and J. A. Theiss. 2011. Depressive symptoms and mechanisms of relational turbulence as predictors of relationship satisfaction among returning service members. Journal of Family Psychology 25(4):470-478.
Kreider, R. M., and R. Ellis. 2011. Living arrangements of children: 2009. Current Population Reports (June):P70-126.
Kreutzer, J. S., L. J. Rapport, J. H. Marwitz, C. Harrison-Felix, T. Hart, M. Glenn, and F. Hammond. 2009. Caregivers' well-being after traumatic brain injury: A multicenter prospective investigation. Archives of Physical Medicine and Rehabilitation 90(6):939-946.
Kulka, R. A., W. E. Schlenger, J. A. Fairbank, R. L. Hough, B. K. Jordan, C. R. Marmar, D. S. Weiss, and D. A. Grady. 1990. Trauma and the Vietnam War Generation: Report of Findings from the National Vietnam Veterans Readjustment Study. New York: Routledge.
Lara-Cinisomo, S., A. Chandra, R. Burns, L. Jaycox, T. Tanielian, T. Ruder, and B. Han. 2011. A mixedmethod approach to understanding the experiences of non-deployed military caregivers. Maternal and Child Health Journal 16(2):374-384.
Lester, P., K. Peterson, J. Reeves, L. Knauss, D. Glover, C. Mogil, N. Duan, W. Saltzman, R. Pynoos, K.
Wilt, and W. Beardslee. 2010. The long war and parental combat deployment: Effects on military children and at-home spouses. Journal of the American Academy of Child and Adolescent Psychiatry 49(4):310-320.
Lester, P., C. Mogil, W. Saltzman, K. Woodward, W. Nash, G. Leskin, B. Bursch, S. Green, R. Pynoos, and W. Beardslee. 2011. Families overcoming under stress: Implementing family-centered prevention for military families facing wartime deployments and combat operational stress. Military Medicine 176(1):19-25.
Lester, P., W. R. Saltzman, K. Woodward, D. Glover, G. A. Leskin, B. Bursch, R. Pynoos, and W.
Beardslee. 2012. Evaluation of a family-centered prevention intervention for military children and families facing wartime deployments. American Journal of Public Health 102(Suppl1):S48-S54.
Lilly, M. B., A. Laporte, and P. C. Coyte. 2007. Labor market work and home care's unpaid caregivers: A systematic review of labor force participation rates, predictors of labor market withdrawal, and hours of work. Milbank Quarterly 85(4):641-690.
Lim, N., and D. Schulker. 2010. Measuring Underemployment Among Military Spouses. Santa Monica, CA: RAND Corporation.
Lincoln, A., E. Swift, and M. Shorteno-Fraser. 2008. Psychological adjustment and treatment of children and families with parents deployed in military combat. Journal of Clinical Psychology 64(8):984-992. Lundquist, J. H. 2004. When race makes no difference: Marriage and the military. Social Forces 83(2):731-757.
———. 2006. The black-white gap in marital dissolution among young adults: What can a counterfactual scenario tell us? Social Problems 53(3):421-441.
Luthar, S. S. 2006. Resilience in development: A synthesis of research across five decades. In Developmental Psychopathology: Risk, Disorder, and Adaptation, edited by D. Cicchetti and D. J. Cohen. New York: Wiley. Pp. 740-795.
Lyle, D. S. 2006. Using military deployments and job assignments to estimate the effect of parental absences and household relocations on children's academic achievement. Journal of Labor Economics 24(2):319-350.
MacDermid Wadsworth, S., and K. Southwell. 2011. Military families: Extreme work and extreme “work-family.” Annals of the American Academy of Political and Social Science 638(1):163-183.
MacLean, A., and G. H. Elder. 2007. Military service in the life course. Annual Review of Sociology 33:175-196.
Makin-Byrd, K., E. Gifford, S. McCutcheon, and S. Glynn. 2011. Family and couples treatment for newly returning veterans. Professional Psychology—Research and Practice 42(1):47-55.
Mannarino, A. P., J. A. Cohen, E. Deblinger, M. K. Runyon, and R. A. Steer. 2012. Trauma-focused cognitive-behavioral therapy for children sustained impact of treatment 6 and 12 months later. Child Maltreatment 17(3):231-241.
Mansfield, A. J., J. S. Kaufman, S. W. Marshall, B. N. Gaynes, J. P. Morrissey, and C. C. Engel. 2010. Deployment and the use of mental health services among US Army wives. New England Journal of Medicine 362(2):101-109.
Mansfield, A. J., J. S. Kaufman, C. C. Engel, and B. N. Gaynes. 2011. Deployment and mental health diagnoses among children of US Army personnel. Archives of Pediatrics and Adolescent Medicine 165(11):999-1005.
Martin, S. L., D. A. Gibbs, R. E. Johnson, K. Sullivan, M. Clinton-Sherrod, J. L. Walters, and E. D. Rentz. 2010. Substance use by soldiers who abuse their spouses. Violence Against Women 16(11):1295-1310.
Mateczun, J. M., and E. K. Holmes. 1996. Return, readjustment, and reintegration: The three R's of family reunion. In Emotional Aftermath of the Persian Gulf War: Veterans, Families, Communities and Nations, edited by R. J. Ursano and A. E. Norwood. Washington, DC: American Psychiatric Press, Inc. Pp. 250-282.
McCarroll, J. E., R. J. Ursano, X. Liu, L. E. Thayer, J. H. Newby, A. E. Norwood, and C. S. Fullerton. 2000. Deployment and the probability of spousal aggression by US Army soldiers. Military Medicine 165(1):41-44.
McCarroll, J. E., K. J. Hoffman, A. Grieger, and H. C. Holloway. 2005. Psychological aspects of deployment and reunion. In Military Preventive Medicine: Mobilization and Deployment Vol. 2, edited by P. W. Kelley. Washington, DC: Office of the Surgeon General, Department of the Army and Borden Institute. Pp. 1395-1426.
McCauley, J., D. E. Kern, K. Kolodner, L. Dill, A. F. Schroeder, H. K. DeChant, J. Ryden, L. R. Derogatis, and E. B. Bass. 1997. Clinical characteristics of women with a history of childhood abuse. Journal of the American Medical Association 277(17):1362-1368.
McCreary, D. R., M. M. Thompson, and L. Pasto. 2003. Predeployment family concerns and soldier wellbeing: The impact of family concerns on the predeployment well-being of Canadian forces personnel. Canadian Journal of Police and Security Services 1:33-40.
McCubbin, H. I. 1979. Integrating coping behavior in family stress theory. Journal of Marriage and the Family 41(2):237-244.
McCubbin, H. I., and C. R. Figley. 1983. Bridging normative and catastrophic family stress. In Stress and the Family, Volume I: Coping with Normative Transitions, edited by H. I. McCubbin and C. R. Figley. New York: Brunner/Mazel. Pp. 218-228.
McCubbin, H. I., B. B. Dahl, G. R. Lester, and B. A. Ross. 1975. The returned prisoner of war: Factors in family reintegration. Journal of Marriage and the Family 37(3):471-478.
McFarlane, W. R., B. Link, R. Dushay, J. Marchal, and J. Crilly. 1995. Psychoeducational multiple family groups: Four-year relapse outcome in schizophrenia. Family Process 34(2):127-144.
McKean, D., J. Goodman, B. Bodnar, H. Warden, E. Shirey, Z. Stokes, A. Scheideberg, and A. Searvis. 2011. Freedom to Serve: The Definitive Guide to LGBT Military Service. Washington, DC: Servicemembers Legal Defense Network.
McNulty, P. A. F. 2005. Reported stressors and health care needs of active duty Navy personnel during three phases of deployment in support of the war in Iraq. Military Medicine 170(6):530-535.
Meis, L. A., C. R. Erbes, M. A. Polusny, and J. S. Compton. 2010. Intimate relationships among returning soldiers: The mediating and moderating roles of negative emotionality, PTSD symptoms, and alcohol problems. Journal of Traumatic Stress 23(5):564-572.
Merrill, L. L., J. L. Crouch, C. J. Thomsen, and J. M. Guimond. 2004. Risk for intimate partner violence and child physical abuse: Psychosocial characteristics of multirisk male and female Navy recruits. Child Maltreatment 9(1):18-29.
Mghir, R., W. Freed, A. Raskin, and W. Katon. 1995. Depression and posttraumatic stress disorder among a community sample of adolescent and young adult Afghan refugees. Journal of Nervous and Mental Disease 183(1):24-30.
MHAT-IV. 2006. Mental Health Advisory Team IV (MHAT- IV): Operation Iraqi Freedom 05-07 Final Report. Washington, DC: Office of the Surgeon General, United States Army Medical Command, Office of the Surgeon Multinational Force-Iraq.
MHAT-V. 2008. Mental Health Advisory Team V (MHAT-V) Operation Iraqi Freedom 06-08: Iraq; Operation Enduring Freedom 8: Afghanistan. Washington, DC: Office of the Surgeon General, United States Army Medical Command, Office of the Surgeon Multinational Force-Iraq.
MHAT-VII. 2011. Joint Mental Health Advisory Team 7 (J-MHAT 7) Operation Enduring Freedom 2010. Washington, DC: Office of the Surgeon General, United States Army Medical Command, Office of the Command Surgeon HQ, USCENTCOM, Office of the Command Surgeon U.S. Forces Afghanistan.
Miller, L. L., S. O. Meadows, L. M. Hanser, and S. L. Taylor. 2011a. Year of the Air Force Family: 2009 Survey of Active-Duty Spouses. Santa Monica, CA: RAND Corporation.
Miller, L. L., B. D. Rostker, R. M. Burns, D. Barnes-Proby, S. Lara-Cinisomo, and T. R. West. 2011b. A New Approach for Assessing the Needs of Service Members and Their Families. Santa Monica, CA: RAND Corporation.
Milliken, C. S., J. L. Auchterlonie, and C. W. Hoge. 2007. Longitudinal assessment of mental health problems among active and reserve component soldiers returning from the Iraq war. Journal of the American Medical Association 298(18):2141-2148.
Monson, C. M., S. P. Stevens, and P. P. Schnurr. 2005. Cognitive-behavioral couple’s treatment for posttraumatic stress disorder. In Focus on Posttraumatic Stress Disorder Research, edited by T. A. Corales. Hauppauge, NY: Nova Science Publishers, Inc. Pp. 250-274.
Monson, C. M., C. T. Taft, and S. J. Fredman. 2009. Military-related PTSD and intimate relationships: From description to theory-driven research and intervention development. Clinical Psychology Review 29(8):707-714.
Monson, C. M., S. J. Fredman, K. C. Adair, S. P. Stevens, P. A. Resick, P. P. Schnurr, H. Z. MacDonald, and A. Macdonald. 2011. Cognitive-behavioral conjoint therapy for PTSD: Pilot results from a community sample. Journal of Traumatic Stress 24(1):97-101.
Mulligan, K., N. Jones, M. Davies, P. McAllister, N. T. Fear, S. Wessely, and N. Greenberg. 2012. Effects of home on the mental health of British forces serving in Iraq and Afghanistan. British Journal of Psychiatry.
Murray-Swank, A. B., and L. Dixon. 2004. Family psychoeducation as an evidence-based practice. CNS Spectrums 9(12):905-912.
Nathanson, A. M., R. C. Shorey, V. Tirone, and D. L. Rhatigan. 2012. The prevalence of mental health disorders in a community sample of female victims of intimate partner violence. Partner Abuse 3(1):59.
National Alliance for Caregiving. 2010. Caregivers of Veterans—Serving on the Homefront. Bethesda, MD: National Alliance for Caregiving.
Negrusa, B., and S. Negrusa. 2012. Home Front: Post-Deployment Mental Health and Divorces. Santa Monica, CA: RAND Corporation.
Nelson, H. D., P. Nygren, Y. McInerney, and J. Klein. 2004. Screening women and elderly adults for family and intimate partner violence: A review of the evidence for the US Preventive Services Task Force. Annals of Internal Medicine 140(5):387-396.
Nelson Goff, B. S., and B. D. Smith. 2005. Systemic traumatic stress: The couple adaption to traumatic stress model. Journal of Marital and Family Therapy 31(2):145-157.
Newby, J. H., J. E. McCarroll, R. J. Ursano, Z. Fan, J. Shigemura, and Y. Tucker-Harris. 2005a. Positive and negative consequences of a military deployment. Military Medicine 170(10):815-819.
Newby, J. H., R. J. Ursano, J. E. McCarroll, X. Liu, C. S. Fullerton, and A. E. Norwood. 2005b. Postdeployment domestic violence by US Army soldiers. Military Medicine 170(8):643-647.
NRC (National Research Council) and IOM. 2010. Student Mobility: Exploring the Impact of Frequent Moves on Achievement: Summary of a Workshop. Washington, DC: The National Academies Press.
O’Leary, K. D. 1999. Psychological abuse: A variable deserving critical attention in domestic violence. Violence and Victims 14(1):3-23.
Orthner, D. K., and R. Rose. 2002. Relocation Adjustment Among Army Civilian Spouses. Washington, DC: Army Research Institute for the Behavioral and Social Sciences.
Padden, D. L., R. A. Connors, and J. G. Agazio. 2011. Stress, coping, and well-being in military spouses during deployment separation. Western Journal of Nursing Research 33(2):247-267.
Parsons, C. 2008. US Military Marriages Strained by Long Deployments. http://www.reuters.com/article/2008/05/06/us-usa-military-marriage-idUSN2228946820080506 (accessed August 22, 2012).
Patterson, J. M. 2002. Integrating family resilience and family stress theory. Journal of Marriage and Family 64(2):349-360.
Peebles-Kleiger, M. J., and J. H. Kleiger. 1994. Re-integration stress for Desert Storm families: Wartime deployments and family trauma. Journal of Traumatic Stress 7(2):173-194.
Perlesz, A., G. Kinsella, and S. Crowe. 1999. Impact of traumatic brain injury on the family: A critical review. Rehabilitation Psychology 44(1):6-35.
Perlick, D. A., K. Straits-Troster, D. G. Dyck, D. M. Norell, J. L. Strauss, C. Henderson, J. Close, N.
Berger, E. R. Bonuck, K. H. Taber, C. Kalvin, T. Dolber, and A. Cristian. 2011. Multifamily group treatment for veterans with traumatic brain injury. Professional Psychology—Research and Practice 42(1):70-78.
Phelan, S. M., J. M. Griffin, W. L. Hellerstedt, N. A. Sayer, A. C. Jensen, D. J. Burgess, and M. van Ryn. 2011. Perceived stigma, strain, and mental health among caregivers of veterans with traumatic brain injury. Disability and Health Journal 4(3):177-184.
Pietrzak, R. H., and S. M. Southwick. 2011. Psychological resilience in OEF-OIF veterans: Application of a novel classification approach and examination of demographic and psychosocial correlates. Journal of Affective Disorders 133(3):560-568.
Pincus, S. H., R. House, and J. Christenson. 2001. The emotional cycle of deployment: A military family perspective. Army Medical Department Journal 4/5/6:15-23.
Pinquart, M., and S. Sörensen. 2003. Differences between caregivers and non-caregivers in psychological health and physical health: A meta-analysis. Psychology and Aging 18:250-267.
———. 2005. Ethnic differences in stressors, resources, and psychological outcomes of family caregiving: A meta-analysis. Gerontologist 45(1):90-106.
———. 2011. Spouses, adult children, and children-in-law as caregivers of older adults: A meta-analytic comparison. Psychology and Aging 26(1):1-14.
Polusny, M. A., C. R. Erbes, P. A. Arbisi, P. Thuras, S. M. Kehle, M. Rath, C. Courage, M. K. Reddy, and C. Duffy. 2009. Impact of prior Operation Enduring Freedom/Operation Iraqi Freedom combat duty on mental health in a predeployment cohort of National Guard soldiers. Military Medicine 174(4):353-357.
President’s Commission on Care for America’s Returning Wounded Warriors. 2007. Serve, Support, Simplify: Report of the President’s Commission on Care for America’s Returning Wounded Warriors. Washington, DC.
RAND Center for Military Health Policy. 2012. The Deployment Life Study. http://www.rand.org/multi/military/deployment-life.html (accessed October 17, 2012).
Reddy, M. K., L. A. Meis, C. R. Erbes, M. A. Polusny, and J. S. Compton. 2011. Associations among experiential avoidance, couple adjustment, and interpersonal aggression in returning Iraqi war veterans and their partners. Journal of Consulting and Clinical Psychology 79(4):515-520.
Reinkober Drummet, A., M. Coleman, and S. Cable. 2003. Military families under stress: Implications for family life education. Family Relations 52(3):279-287.
Renshaw, K. D., and S. B. Campbell. 2011. Combat veterans’ symptoms of PTSD and partners’ distress: The role of partners’ perceptions of veterans’ deployment experiences. Journal of Family Psychology 25(6):953-962.
Renshaw, K. D., and C. M. Caska. 2012. Relationship distress in partners of combat veterans: The role of partners’ perceptions of posttraumatic stress symptoms. Behavior Therapy 43(2):416-426.
Renshaw, K. D., C. S. Rodrigues, and D. H. Jones. 2008. Psychological symptoms and marital satisfaction in spouses of Operation Iraqi Freedom veterans: Relationships with spouses' perceptions of veterans’ experiences and symptoms. Journal of Family Psychology 22(4):586-594.
Renshaw, K. D., E. S. Allen, G. K. Rhoades, R. K. Blais, H. J. Markman, and S. M. Stanley. 2011. Distress in spouses of service members with symptoms of combat-related PTSD: Secondary traumatic stress or general psychological distress? Journal of Family Psychology 25(4):461-469.
Rentz, E. D., S. L. Martin, D. A. Gibbs, M. Clinton-Sherrod, J. Hardison, and S. W. Marshall. 2006. Family violence in the military: A review of the literature. Trauma Violence and Abuse 7(2):93-108.
Rentz, E. D., S. W. Marshall, D. Loomis, C. Casteel, S. L. Martin, and D. A. Gibbs. 2007. Effect of deployment on the occurrence of child maltreatment in military and nonmilitary families. American Journal of Epidemiology 165(10):1199-1206.
Richardson, A., A. Chandra, L. T. Martin, C. M. Setodji, B. W. Hallmark, N. F. Campbell, S. Hawkins, and P. Grady. 2011. Effects of Soldiers’ Deployment on Children’s Academic Performance and Behavioral Health. Santa Monica, CA: RAND Corporation.
Riggs, S. A., and D. S. Riggs. 2011. Risk and resilience in military families experiencing deployment: The role of the family attachment network. Journal of Family Psychology 25(5):675-687.
Robinson-Whelen, S., and D. H. Rintala. 2003. Informal care providers for veterans with SCI: Who are they and how are they doing? Journal of Rehabilitation Research and Development 40(6):511-516.
Robrecht, D. T., J. Millegan, L. L. Leventis, J. B. Crescitelli, and R. N. McLay. 2008. Spousal military deployment as a risk factor for postpartum depression. Journal of Reproductive Medicine 53(11):860-864.
Rodgers, M. L., A. D. Strode, D. M. Norell, R. A. Short, D. G. Dyck, and B. Becker. 2007. Adapting multiple-family group treatment for brain and spinal cord injury intervention development and preliminary outcomes. American Journal of Physical Medicine and Rehabilitation 86(6):482-492.
Rosen, L. N., D. Durand, D. J. Westhuis, and J. M. Teitelbaum. 1995. Marital adjustment of Army spouses one year after Operation Desert Storm. Journal of Applied Social Psychology 25(8):677-692. Ruger, W., S. E. Wilson, and S. L. Waddoups. 2002. Warfare and welfare: Military service, combat, and marital dissolution. Armed Forces and Society 29(1):85-107.
Sahlstein, E., K. C. Maguire, and L. Timmerman. 2009. Contradictions and praxis contextualized by wartime deployment: Wives’ perspectives revealed through relational dialectics. Communication Monographs 76(4):421-442.
Saltzman, W. R., P. Lester, W. R. Beardslee, C. M. Layne, K. Woodward, and W. P. Nash. 2011. Mechanisms of risk and resilience in military families: Theoretical and empirical basis of a familyfocused resilience enhancement program. Clinical Child and Family Psychology Review 14(3):213-230.
SAMHSA (Substance Abuse and Mental Health Services Administration). 2008. Results from the 2007 National Survey on Drug Use and Health: National Findings: Major Depressive Episode and Treatment for Depression Among Veterans Aged 21 to 39. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Sautter, F. J., S. M. Glynn, K. E. Thompson, L. Franklin, and X. Han. 2009. A couple-based approach to the reduction of PTSD avoidance symptoms: Preliminary findings. Journal of Marital and Family Therapy 35(3):343-349.
Sayers, S. L. 2011. Family reintegration difficulties and couples therapy for military veterans and their spouses. Cognitive and Behavioral Practice 18(1):108-119.
Schok, M. L., R. J. Kleber, M. Elands, and J. M. P. Weerts. 2008. Meaning as a mission: A review of empirical studies on appraisals of war and peacekeeping experiences. Clinical Psychology Review 28(3):357-365.
Schulz, R., and L. M. Martire. 2004. Family caregiving of persons with dementia: Prevalence, health effects, and support strategies. American Journal of Geriatric Psychiatry 12(3):240-249.
Segal, M. W. 1986. The military and the family as greedy institutions. Armed Forces and Society 13(1):9-38.
Shear, M. K. 2012. Grief and mourning gone awry: Pathway and course of complicated grief. Dialogues in Clinical Neuroscience 14(2):119-128.
Sheppard, S. C., J. W. Malatras, and A. C. Israel. 2010. The impact of deployment on US military families. American Psychologist 65(6):599-609.
Sherman, M. D. 2006. Updates and five-year evaluation of the S.A.F.E. Program: A family psychoeducational program for serious mental illness. Community Mental Health Journal 42(2):213-219.
Sherman, M. D., D. A. Perlick, and K. Straits-Troster. 2012. Adapting the multifamily group model for treating veterans with posttraumatic stress disorder. Psychological Services 9(4):349-360.
Shin, P., S. Rosenbaum, and D. R. Mauery. 2005. Medicaid’s Role in Treating Children in Military Families. Washington, DC: George Washington University SPHHS Center for Health Services Research and Policy.
Silverman, A. B., H. Z. Reinherz, and R. M. Giaconia. 1996. The long-term sequelae of child and adolescent abuse: A longitudinal community study. Child Abuse and Neglect 20(8):709-723.
Silverman, W. K., C. D. Ortiz, C. Viswesvaran, B. J. Burns, D. J. Kolko, F. W. Putnam, and L. Amaya-Jackson. 2008. Evidence-based psychosocial treatments for children and adolescents exposed to traumatic events. Journal of Clinical Child and Adolescent Psychology 37(1):156-183.
Skopp, N. A., M. A. Reger, G. M. Reger, M. C. Mishkind, M. Raskind, and G. A. Gahm. 2011. The role of intimate relationships, appraisals of military service, and gender on the development of posttraumatic stress symptoms following Iraq deployment. Journal of Traumatic Stress 24(3):277-286.
Smith, D. C., M. L. Munroe, L. M. Foglia, P. E. Nielsen, and S. H. Deering. 2010. Effects of deployment on depression screening scores in pregnancy at an Army military treatment facility. Obstetrics and Gynecology 116(3):679-684.
Smith, P., S. Perrin, W. Yule, and S. Rabe-Hesketh. 2001. War exposure and maternal reactions in the psychological adjustment of children from Bosnia-Herzegovina. Journal of Child Psychology and Psychiatry 42(3):395-404.
Spera, C. 2009. Spouses’ ability to cope with deployment and adjust to Air Force family demands. Armed Forces and Society 35(2):286-306.
Stanley, S. M., E. S. Allen, H. J. Markman, G. K. Rhoades, and D. L. Prentice. 2010. Decreasing divorce in Army couples: Results from a randomized controlled trial using prep for strong bonds. Journal of Couple and Relationship Therapy 9(2):149-160.
SteelFisher, G. K., A. M. Zaslavsky, and R. J. Blendon. 2008. Health-related impact of deployment extensions on spouses of active duty Army personnel. Military Medicine 173(3):221-229.
Stenberg, U., C. M. Ruland, and C. Miaskowski. 2010. Review of the literature on the effects of caring for a patient with cancer. Psycho-Oncology 19(10):1013-1025.
Street, A. E., and I. Arias. 2001. Psychological abuse and posttraumatic stress disorder in battered women: Examining the roles of shame and guilt. Violence and Victims 16(1):65-78.
Taft, C. T., R. P. Weatherill, H. E. Woodward, L. A. Pinto, L. E. Watkins, M. W. Miller, and R. Dekel. 2009. Intimate partner and general aggression perpetration among combat veterans presenting to a posttraumatic stress disorder clinic. American Journal of Orthopsychiatry 79(4):461-468.
US Census Bureau. 2011a. America’s Families and Living Arrangements: 2011, Table C2: Household Relationship and Living Arrangements of Children Under 18 Years, by Age and Sex: 2011. http://www.census.gov/population/www/socdemo/hh-fam/cps2011.html (accessed October 25, 2012). ———. 2011b. America’s Families and Living Arrangements: 2011, Table C3: Living Arrangements of Children Under 18 Years and Marital Status of Parents, by Age, Sex, Race, and Hispanic Origin and Selected Characteristics of the Child for all Children: 2011. http://www.census.gov/population/www/socdemo/hh-fam/cps2011.html (accessed October 25, 2012). ———. 2011c. Current Population Survey, 2010 Annual Social and Economic Supplement. www.census.gov/hhes/migration/files/cps/cps2010/tab02.xls (accessed June 1, 2012).
US House of Representatives. 2008. National Month of the Military Child. H. Res. 265. 110th Congress.
US Social Security Administration. 2012. Office of Retirement and Disability Policy. http://www.ssa.gov/policy/docs/statcomps/supplement/2012/5f.html#table5.f4 (accessed October 25, 2012).
VA (Department of Veterans Affairs). 2006. VHA directive 2006-041: Veterans Health Care Service Standards. Washington, DC: Veterans Health Administration, Department of Veterans Affairs.
———. 2011. New Services for Family Caregivers of Post-9/11 Veterans. http://www.caregiver.va.gov/support_benefits.asp (accessed July 9, 2012).
van der Voort, T. Y., P. J. Goossens, and J. J. van der Bijl. 2007. Burden, coping and needs for support of caregivers for patients with a bipolar disorder: A systematic review. Journal of Psychiatric and Mental Health Nursing 14(7):679-687.
Van Houtven, C. H., E. Z. Oddone, and M. Weinberger. 2010. Informal and formal care infrastructure and perceived need for caregiver training for frail US veterans referred to home and community-based services. Chronic Illness 6(1):57-66.
van Steenbergen, E. F., N. Ellemers, S. A. Haslam, and F. Urlings. 2008. There is nothing either good or bad but thinking makes it so: Informational support and cognitive appraisal of the work-family interface. Journal of Occupational and Organizational Psychology 81(3):349-367.
Verhaeghe, S., T. Defloor, and M. Grypdonck. 2005. Stress and coping among families of patients with traumatic brain injury: A review of the literature. Journal of Clinical Nursing 14(8):1004-1012.
Vitaliano, P. P., J. Zhang, and J. M. Scanlan. 2003. Is caregiving hazardous to one's physical health? A meta-analysis. Psychological Bulletin 129(6):946-972.
Vormbrock, J. K. 1993. Attachment theory as applied to wartime and job-related marital separation. Psychological Bulletin 114(1):122-144.
Walsh, F. 2006. Strengthening Family Resilience, 2nd ed. New York: Guilford.
Warner, C., G. N. Appenzeller, C. Warner, and T. Grieger. 2009. Psychological effects of deployments on military families. Psychiatric Annals 39(2):56-63.
Weinick, R. M., E. B. Beckjord, C. M. Farmer, L. T. Martin, E. M. Gillen, J. D. Acosta, M. P. Fisher, J. Garnett, G. C. Gonzalez, T. C. Helmus, L. H. Jaycox, K. A. Reynolds, N. Salcedo, and D. M. Scharf. 2011. Programs Addressing Psychological Health and Traumatic Brain Injury Among US Military Servicemembers and Their Families. Santa Monica, CA: RAND Corporation.
Werber, L., M. C. Harrell, D. M. Varda, K. Curry Hall, and M. K. Beckett. 2008. Deployment Experiences of Guard and Reserve Families: Implications for Support and Retention. Santa Monica, CA: RAND Corporation.
Wiens, T. W., and P. Boss. 2006. Maintaining family resiliency before, during, and after military separation. In Military Life: The Psychology of Serving in Peace and Combat, Volume 3: The Family, edited by C. A. Castro, A. B. Adler, and T. W. Britt. Westport, CT: Praeger.
Worthen, M., R. Moos, and J. Ahern. 2012. Iraq and Afghanistan veterans’ experiences living with their parents after separation from the military. Contemporary Family Therapy:1-14.
Wright, K. M., L. M. Burrell, E. D. Schroeder, and J. L. Thomas. 2006. Military spouses: Coping with the fear and the reality of service member injury and death. In Military Life: The Psychology of Serving in Peace and Combat. Volume 3: The Family, edited by C. A. Castro, A. B. Adler, and T. W. Britt.
Westport, CT: Praeger.
Zarit, S. 2006. Assessment of family caregivers: A research perspective. In Caregiver Assessment: Voices and Views from the Field. Report from a National Consensus Development Conference (Vol. II), edited by Family Caregiver Alliance. San Francisco, CA: Family Caregiver Alliance. Pp. 12-37.










































































